Rapid cycle bipolar 1
Rapid Cycling Bipolar Disorder Symptoms, Treatments, Causes, and More
Written by Matthew Hoffman, MD
In this Article
- What Is Rapid in Cycling Bipolar Disorder?
- Who Gets Rapid Cycling Bipolar Disorder?
- What Are the Features of Bipolar Disorder?
- How Is Rapid Cycling Bipolar Disorder Identified?
- How Is Bipolar Disorder with Rapid Cycling Treated?
- What Are the Risks of Rapid Cycling Bipolar Disorder?
What Is Rapid in Cycling Bipolar Disorder?
Rapid cycling is a pattern of frequent, distinct episodes in bipolar disorder. In rapid cycling, a person with the disorder experiences four or more episodes of mania or depression in one year. It can occur at any point in the course of bipolar disorder, and can come and go over many years depending on how well the illness is treated; it is not necessarily a "permanent" or indefinite pattern of episodes.
Who Gets Rapid Cycling Bipolar Disorder?
Virtually anyone can develop bipolar disorder. About 2.5% of the U.S. population suffers from some form of bipolar disorder - nearly 6 million people. A rapid cycling pattern may occur in about 10% to 20% of people with the disorder. Women, and people with bipolar II disorder, are more likely to experience periods of rapid cycling.
Most people are in their late teens or early 20s when symptoms of bipolar disorder first start. Nearly everyone with bipolar disorder develops it before age 50. People with an immediate family member with bipolar disorder are at higher risk.
What Are the Features of Bipolar Disorder?
The major features of bipolar disorder include:
- At least 1 episode of mania or hypomania in the patient's lifetime
- Episodes of depression (major depressive disorder), which are often recurrent
Mania is a period of abnormally elevated mood and high energy, usually accompanied by erratic behavior lasting at least seven days at a time. Hypomania is an elevated mood not reaching full-blown mania and lasting a minimum of four days.
A few people with rapid cycling bipolar disorder alternate between periods of hypomania and major depressive disorder. Far more commonly, though, repeated and distinct episodes of depression dominate the picture. Repeated periods of depression are punctuated by infrequent, shorter periods of elevated or normal mood.
How Is Rapid Cycling Bipolar Disorder Identified?
Bipolar disorder is diagnosed after someone experiences a hypomanic or manic episode along with multiple additional episodes of either mania, hypomania or depression. Rapid cycling in itself is not a diagnosis, but rather a "course specifier" or descriptor of the course of illness. In bipolar disorder rapid cycling is identified when four or more distinct episodes of depression, mania, or hypomania occur during a one year period.
Rapid cycling bipolar disorder can be difficult to identify, because a single mood episode can sometimes simply wax and wane without resolving. As a result, they don't necessarily represent multiple separate and distinct episodes. Rapid cycling may seem to make the changing mood states of bipolar disorder more obvious, but because most people with rapid cycling bipolar disorder spend far more time depressed than manic or hypomanic, they are often misdiagnosed with unipolar depression.
Rapid cycling may seem to make the changing mood states of bipolar disorder more obvious, but because most people with rapid cycling bipolar disorder spend far more time depressed than manic or hypomanic, they are often misdiagnosed with unipolar depression.
For example, in one study of people with bipolar II disorder, the amount of time spent depressed was more than 35 times the amount of time spent hypomanic. Also, people often don't take note of their own hypomanic symptoms, mistaking them for a period of unusually good mood.
How Is Bipolar Disorder with Rapid Cycling Treated?
Because symptoms of depression dominate in most people with a rapid cycling course of bipolar disorder, treatment is usually aimed toward stabilizing mood, mainly by relieving depression while preventing the comings-and-goings of new episodes.
Antidepressants such as fluoxetine (Prozac), paroxetine (Paxil,) and sertraline (Zoloft) have not been shown to treat the depression symptoms of rapid cycling bipolar disorder, and may even increase the frequency of new episodes over time.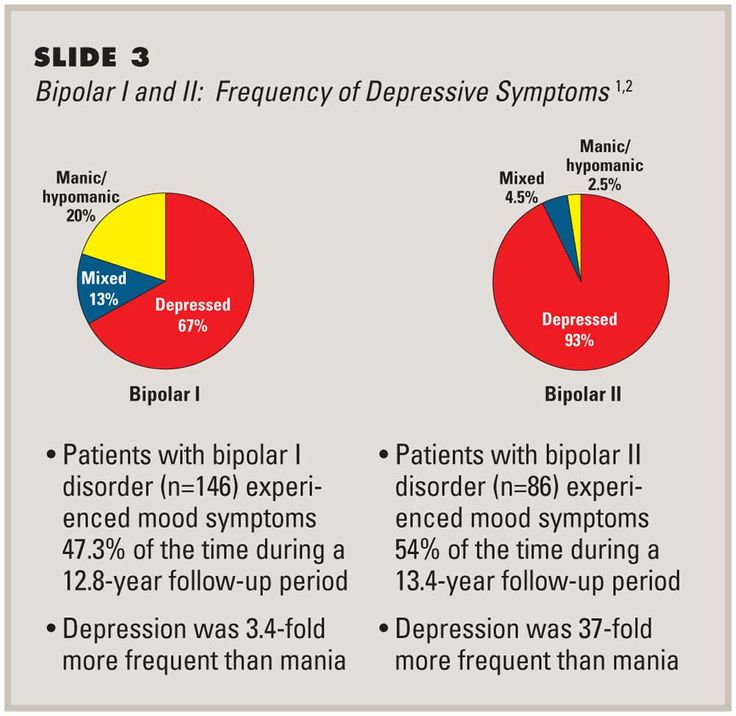 Many experts therefore advise against the use of antidepressants (especially long term) in bipolar patients with rapid cycling.
Many experts therefore advise against the use of antidepressants (especially long term) in bipolar patients with rapid cycling.
Mood-stabilizing drugs -- such as carbamazepine (Tegretol), lamotrigine (Lamictal ), lithium (Lithobid), and valproate (Depakote)-- are the core treatments of rapid cycling. Often, a single mood stabilizer is ineffective at controlling episode recurrences, resulting in a need for combinations of mood stabilizers. Several antipsychotic medicines such as olanzapine (Zyprexa) or quetiapine (Seroquel) also have been studied in rapid cycling and are used as part of a treatment regimen, regardless of the presence or absence of psychosis (delusions and hallucinations).
Treatment with mood stabilizers is usually continued (often indefinitely) even when a person is symptom-free. This helps prevent future episodes. Antidepressants, if and when used, are generally tapered as soon as depression is under control.
What Are the Risks of Rapid Cycling Bipolar Disorder?
The most serious risk of a rapid cycling course in bipolar disorder is suicide. People with bipolar disorder are 10 times to 20 times more likely to commit suicide than people without bipolar disorder. Tragically, 8% to 20% of people with bipolar disorder eventually lose their lives to suicide.
People with bipolar disorder are 10 times to 20 times more likely to commit suicide than people without bipolar disorder. Tragically, 8% to 20% of people with bipolar disorder eventually lose their lives to suicide.
People with a rapid cycling course may be at even higher risk for suicide than those with nonrapid cycling bipolar disorder. They are hospitalized more often, and their symptoms are usually more difficult to control long term.
Treatment reduces the likelihood of serious depression and suicide. Lithium in particular, taken long term, has been shown to reduce the risk.
People with bipolar disorder are also at higher risk for substance abuse. Nearly 60% of people with bipolar disorder abuse drugs or alcohol. Substance abuse is associated with more severe or poorly controlled bipolar disorder.
Bipolar Disorder Guide
- Overview
- Symptoms & Types
- Treatment & Prevention
- Living & Support
Rapid Cycling Bipolar Disorder - DBSA
Bipolar disorder with rapid cycling is diagnosed when a person experiences four or more episodes of mania, hypomania, or depressive episodes in any 12-month period.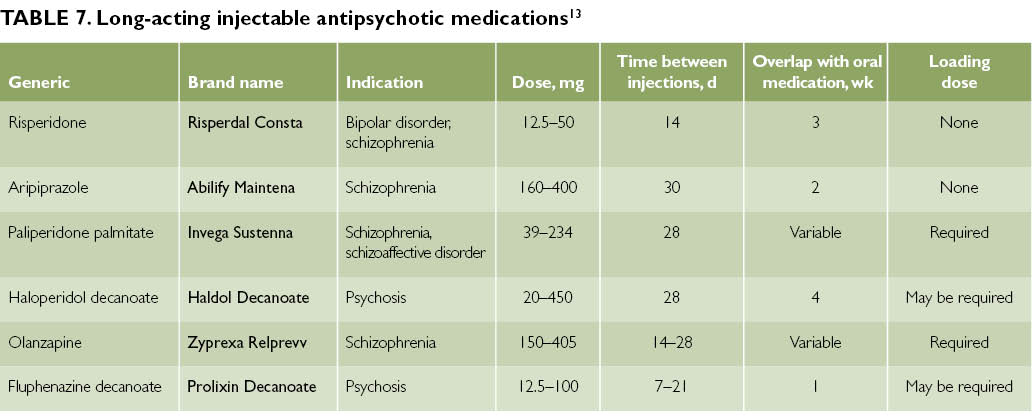 Rapid cycling can occur with any type of bipolar disorder, and maybe a temporary condition for some people.
Rapid cycling can occur with any type of bipolar disorder, and maybe a temporary condition for some people.
People who live with bipolar experience the “highs” that come with mania or hypomania, they also experience “lows” that come with depression. When Rapid Cycling occurs, it means that four or more manic, hypomanic, or depressive episodes have taken place within a twelve-month period. Changes in mood here can happen quickly and occur over a few days or even over a few hours. If there are four mood changes within a month, it is called ultra-rapid cycling. While the phrase “rapid cycling” may make it seem that there is a regular cycle to these shifts in mood, most cycles do not follow a pattern.
Who develops rapid cycling?As many as half of all individuals who live with bipolar may develop rapid cycling at some time. For most, rapid cycling is a temporary occurrence. For a small number of individuals, the pattern of cycling can continue indefinitely. While there are no hard rules for who will develop rapid cycling, it may be more likely to develop in women. Bipolar is equally common in both genders.
While there are no hard rules for who will develop rapid cycling, it may be more likely to develop in women. Bipolar is equally common in both genders.
The cause of rapid cycling is unknown however, there are several theories that have been posed:
KindlingThe kindling theory proposes that early episodes are triggered by actual or anticipated life events. Stressful circumstances such as loss of a job or of a loved one may become ‘triggers’ for that individual. Again, this can be actual or anticipated. Perceived or actual stress associated with these circumstances may result in the cycling of mood seen in rapid cycling. As the triggers continue to present themselves an individual can experience the increase of cycling.
Circadian or Biological RhythmsThis theory proposes that individuals who experience rapid cycling are “out of sync” with their typical biological rhythms. Circadian rhythms represent the 24-hour cycle that people experience each day. This rhythm keeps people in sync with dusk and dawn, sleep, and activity. While it is uncertain if inconsistency with circadian rhythms can cause rapid cycling, it is understood that good sleep hygiene can mitigate symptoms associated with bipolar.
Circadian rhythms represent the 24-hour cycle that people experience each day. This rhythm keeps people in sync with dusk and dawn, sleep, and activity. While it is uncertain if inconsistency with circadian rhythms can cause rapid cycling, it is understood that good sleep hygiene can mitigate symptoms associated with bipolar.
Hypothyroidism means that the thyroid is underactive in the system and is not producing enough of the thyroid hormone for the brain. Some with rapid cycling have responded to treatment with the thyroid hormone.
Anti-DepressantsIt has been found that anti-depressants can increase the frequency of cycling. Some experts have advised against the use of anti-depressants in individuals living with bipolar, especially for the long term. More commonly individuals living with bipolar are prescribed mood-stabilizing drugs which can be a treatment for rapid cycling. Before changing medication, talk to your physician. Do not stop medication without first consulting with your physician.
Do not stop medication without first consulting with your physician.
Rapid cycling is not its own diagnosis, rather a specifier that defines how the course of a bipolar diagnosis is experienced. It can be difficult to treat rapid cycling, however, people may find benefit in talk therapy and tracking their mood.
Mood TrackingKeeping track of your mood may help you understand patterns that cause stress. By keeping records of mood changes, as well as lifestyle factors such as sleep, diet, exercise you can better understand what may trigger mood shifts.
Talk TherapyTalk therapy can help people to identify and stick to a specific treatment plan. Collaborating with a therapist can help people who are experiencing rapid cycling. Feelings such as irritability, sadness, and racing thoughts can interfere with day to day life. By talking to a therapist those feelings can be explored in a “judgment free zone. ” Establishing a treatment plan with a therapist can help you keep track of what improves or worsens symptoms.
” Establishing a treatment plan with a therapist can help you keep track of what improves or worsens symptoms.
What are "quick cycles"? - Bipolar.su
The rapid cycling course of bipolar disorder (from the English - `rapid cycling`) means frequent mood swings, when a person experiences at least four (or more) manic, hypomanic or depressive episodes during the year. Why is this happening and why is it dangerous?
In a person with fast cycling bipolar disorder, mood rises and falls, up and down, and back again, and such fluctuations can occur over several days and even hours. The person feels like on a roller coaster, with powerful shifts in mood and activity that are out of control. For some, rapid cycling is manifested by intense irritability, anger, impulsiveness, and sudden outbursts of aggression. In fast-cycling bipolar disorder, episodes follow each other in a random order.
Some patients may experience true mania, hypomania, or depression in just one day.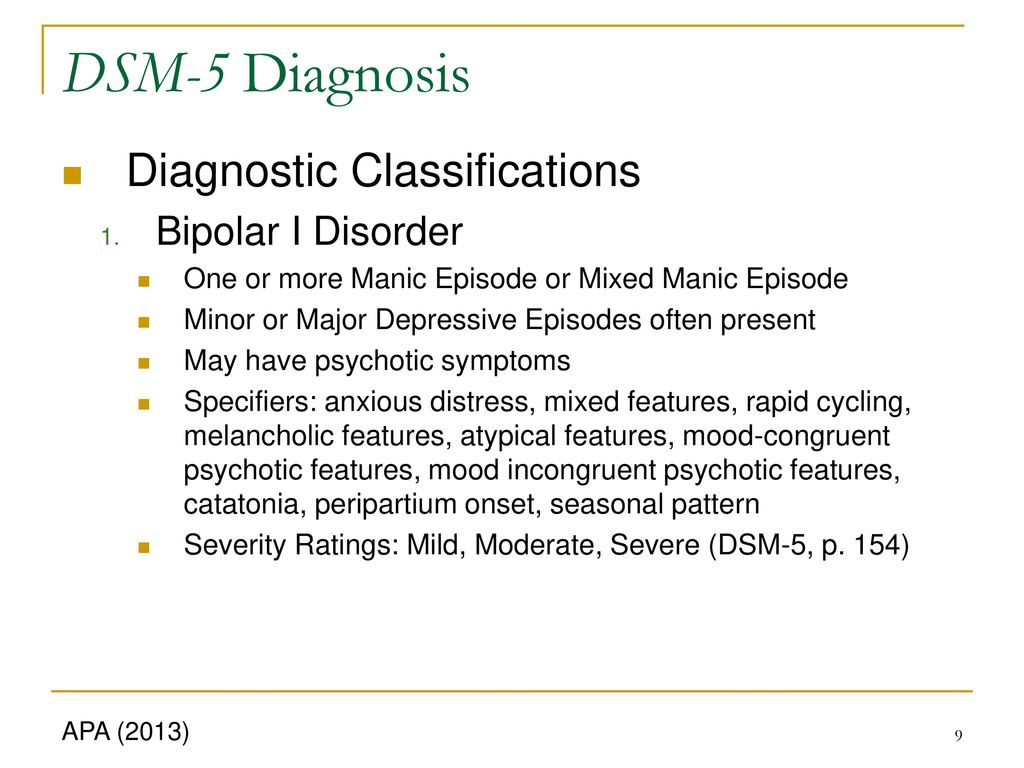 The fast-cyclic course of BAD has several subspecies. If there are 4 mood swings in a month, this is called "ultra-rapid cycling", if several alternations of episodes occur in one day or for several days in one week, this is "ultra-ultra-rapid cycling", or "ultra-range cycling".
The fast-cyclic course of BAD has several subspecies. If there are 4 mood swings in a month, this is called "ultra-rapid cycling", if several alternations of episodes occur in one day or for several days in one week, this is "ultra-ultra-rapid cycling", or "ultra-range cycling".
In general, those with bipolar disorder have a low range of mood swings and experience longer episodes. In some "bipolar" BC (rapid cycles) are observed from the beginning of the course of the disease, but in many the disease takes on this form over time.
Most people with bipolar disorder, in fact, begin to experience shorter and more frequent episodes over the course of the illness if not properly treated. For some people, the appearance of BC is a temporary phenomenon. It is possible to experience a rapid alternation of episodes for a while, and then return to longer states and less frequent swings, and at best, to a stabilized mood with treatment. Only a few people have bipolar disorder with a fast-cycling form for a long time.
It is important to see a doctor right away to find the most appropriate and effective treatment for this form of bipolar disorder, because the longer a person goes without treatment, the more drug-resistant the disease becomes.
Who develops rapid cycling bipolar disorder?
Almost half of people with bipolar disorder may develop BC at some point. There is no definite answer as to who is more likely to have them, but women are more prone to rapid cycles than men, although the disease is equally common among both sexes. An increase in the frequency of episodes can be triggered by taking certain antidepressants. Fast cycles often go away when they are stopped, but be aware of the possibility of recurrence of depressive episodes, so you need to work with your doctor to find a more effective combination of drugs, and never stop medication or change the dosage without first discussing with a specialist.
Undoubtedly, there is an indisputable relationship between the appearance of BC and the use of drugs or alcohol. Substance abuse makes a person more prone to rapidly cycling bipolar disorder. According to the results of the research, it was revealed that alcohol and drug addiction is more common in families of patients with BAD with a fast-cycle form than in families of patients with BAD without fast cycles. Whether this is the result of a genetic link between substance abuse or a consequence of self-medication is unknown.
Substance abuse makes a person more prone to rapidly cycling bipolar disorder. According to the results of the research, it was revealed that alcohol and drug addiction is more common in families of patients with BAD with a fast-cycle form than in families of patients with BAD without fast cycles. Whether this is the result of a genetic link between substance abuse or a consequence of self-medication is unknown.
Causes of rapid cycling bipolar disorder
The underlying cause of rapid cycling remains unknown, but there are three theories.
Sensitization
Sensitization is an increase in the sensitivity of nerve centers under the influence of a stimulus. The theory is that early episodes occur due to various triggers. These can be different events: from the death of a loved one to the upcoming interview. Over time, a person with bipolar disorder becomes increasingly sensitive to small triggers or stressors and is more likely to experience episodes in response to stressful situations.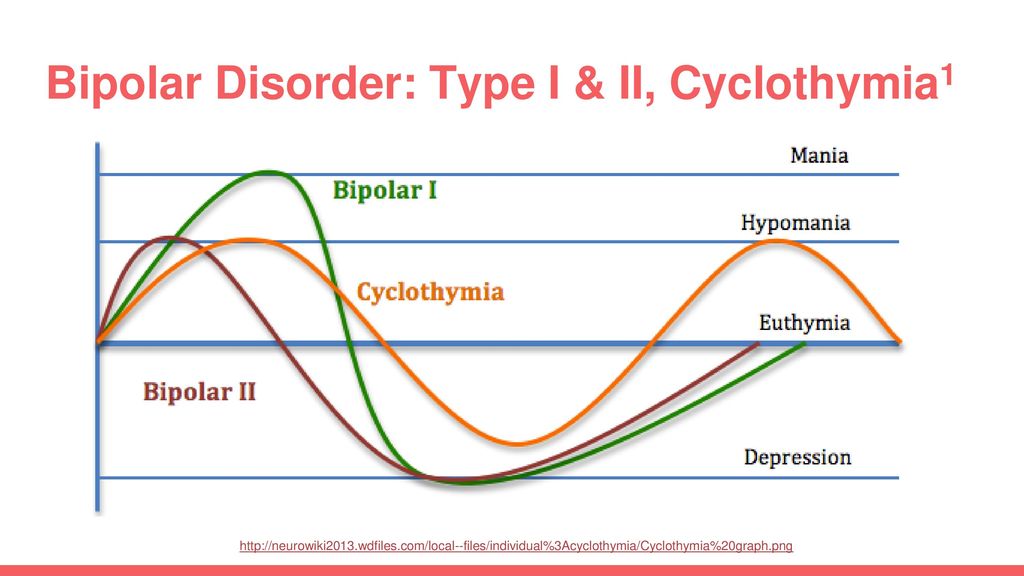 In the end, the person begins rapid cycles without any "triggers". The episodes become more frequent and the end result, if the disease is not properly treated, may be rapid, ultra-rapid or ultra-range cycling.
In the end, the person begins rapid cycles without any "triggers". The episodes become more frequent and the end result, if the disease is not properly treated, may be rapid, ultra-rapid or ultra-range cycling.
Biorhythm disorders
This theory states that in patients with CD, daily biorhythms are not synchronized with such phenomena as dawn and dusk. The disruption of jet lag leads to the sleep disturbances characteristic of mania and depression, as well as other symptoms. There may also be an association between BC and seasonal affective disorder. Abnormal circadian biological rhythms do not cause illness but contribute to the duration and severity of a manic or depressive episode. Therefore, it is better to treat insomnia in a timely manner.
Hypothyroidism
The rapid alternation of episodes of mania, hypomania and depression may be caused by a lack of thyroid hormone in the brain. Most fast cycling people have normal thyroid levels but may respond well to thyroid hormone treatment regardless of the thyroid level.
Are there effective treatments for the rapid cycling course of bipolar disorder?
Yes, although it is difficult to find the right treatment. People with bipolar disorder should not despair if the first few medications or drug combinations prescribed are not successful. There are many different treatment options. Keep track of what works for you and what doesn't or doesn't work to help your doctor decide on future medications. Be sure to discuss adding any medications to your treatment, including natural herbal supplements, with your doctor.
Psychotherapy should be an important part of your treatment plan. In addition to being at risk for another manic or depressive episode, people with bipolar disorder may also have difficulty coping with the effects of past episodes. Feelings such as irritability, tearfulness, racing thoughts or impulsiveness lead to social problems. Because people with bipolar disorder are often unfairly judged, they may lose the opportunity to develop friendships or romantic involvement, or have difficulty achieving their career goals. These factors contribute to self-esteem issues. That is why people with bipolar disorder should work with psychotherapists, in person with a doctor, or with family members. It is important to have a treatment plan that works and stick to it, and to work on preventing suicidal thoughts as it is vital.
These factors contribute to self-esteem issues. That is why people with bipolar disorder should work with psychotherapists, in person with a doctor, or with family members. It is important to have a treatment plan that works and stick to it, and to work on preventing suicidal thoughts as it is vital.
Diagnosing your condition can help you and your doctor identify what is causing your stress, track which medications are working for you, and prevent new episodes. You can try keeping a personal mood calendar, writing down the medications you take, keeping track of mood changes, and noting stressful situations, side effects, and other symptoms.
Conclusion
Research shows that the rapid cycling course of bipolar disorder differs from other forms of it. Patients with fast cycling may respond differently to standard and experimental treatments than people with standard bipolar disorder. With sudden and unpredictable mood changes, episodes are more difficult to bear. It is highly recommended to interact with your doctor, stick to a suitable treatment plan and not give up hope.
It is highly recommended to interact with your doctor, stick to a suitable treatment plan and not give up hope.
Translation: Nadya Abramova
Source: http://www.dbsalliance.org/site/PageServer?pagename=education_brochures_bipolar_disorder_rapid_cycling
Bipolar affective disorder (BAD), its signs, types and treatments
Manifestations of various emotions, mood changes of a person, manifestations of both sadness and joy are normal and depend on many factors - from temperament and character to ongoing events that influence from the outside. However, when these changes are excessive, often unexpected and for no apparent reason, emotions get out of control, or a person remains in a radically positive or negative mood for a long time, it is very likely that bipolar disorder can be diagnosed. This disease was first described at the end of 19century, the famous German psychiatrist Emil Kripelin, calling it manic-depressive psychosis. Many world famous personalities such as Vincent van Gogh, Isaac Newton, Ludwig van Beethoven, Abraham Lincoln suffered from this disease.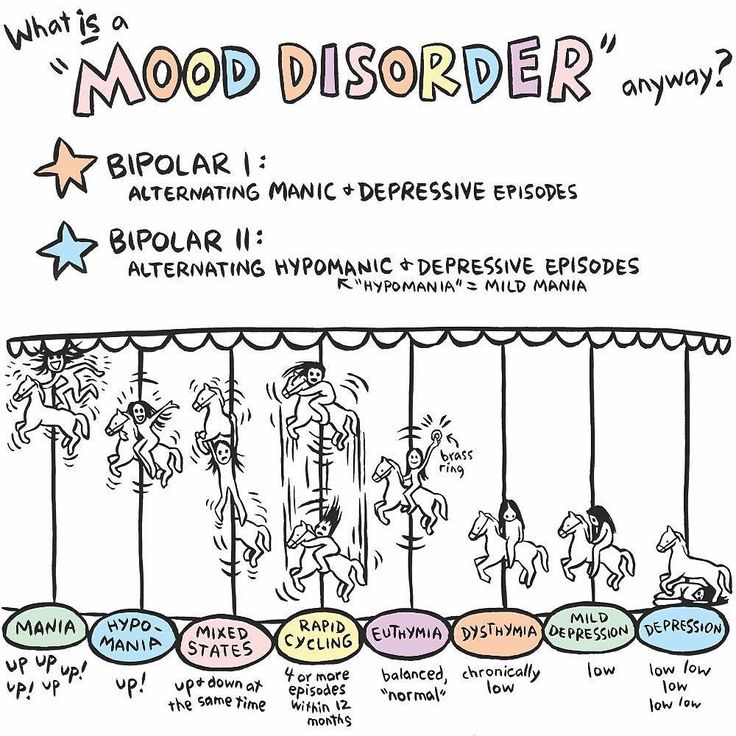 The pronounced form of this disease, which in the international classification of diseases is called bipolar affective disorder (BAD), is detected in 3% of the world's population.
The pronounced form of this disease, which in the international classification of diseases is called bipolar affective disorder (BAD), is detected in 3% of the world's population.
TABLE OF CONTENTS
- 1. Bipolar Personality Disorder - Overview
- 2. Symptoms and signs
- 3. Types of Bipolar Disorder
- 4. Phases of Bipolar Disorder
- 5. Bipolar disorder in women
- 6. Treatment of Bipolar Personality Disorder
It is not uncommon for women to be treated with a combination of drug therapy and cognitive behavioral or interpersonal therapy with a psychotherapist.
Bipolar personality disorder - general information
According to statistics, bipolar disorder affects people between 14 and 44 years of age. Unlike adults, children and adolescents experience more frequent mood swings from mania to depression, sometimes several times a day. 90% of young people make their debut precisely from the phase of depression or melancholy. Another feature of bipolar disorder is that, due to the low level of diagnosis, the patient can live with this disease for 5-10 years without knowing the cause of the painful symptoms.
Another feature of bipolar disorder is that, due to the low level of diagnosis, the patient can live with this disease for 5-10 years without knowing the cause of the painful symptoms.
Most often, bipolar disorder is diagnosed in people whose immediate family members have had a similar problem. The causes of this disease are unknown, but stress, overstrain, and various diseases can provoke the manifestation of its symptoms. However, having fenced off a person from the influence of these factors, it is impossible to get rid of the problem, you need to seek help from a psychotherapist.
Bipolar disorder is a disease that cannot be completely cured. But with properly selected medication and psychotherapy, the quality of life is significantly improved and the periods between phases are lengthened. The person remains socialized and able to work.
Symptoms and signs
From the name it is clear that we are talking about two different poles of affective manifestations, that is, mood manifestations.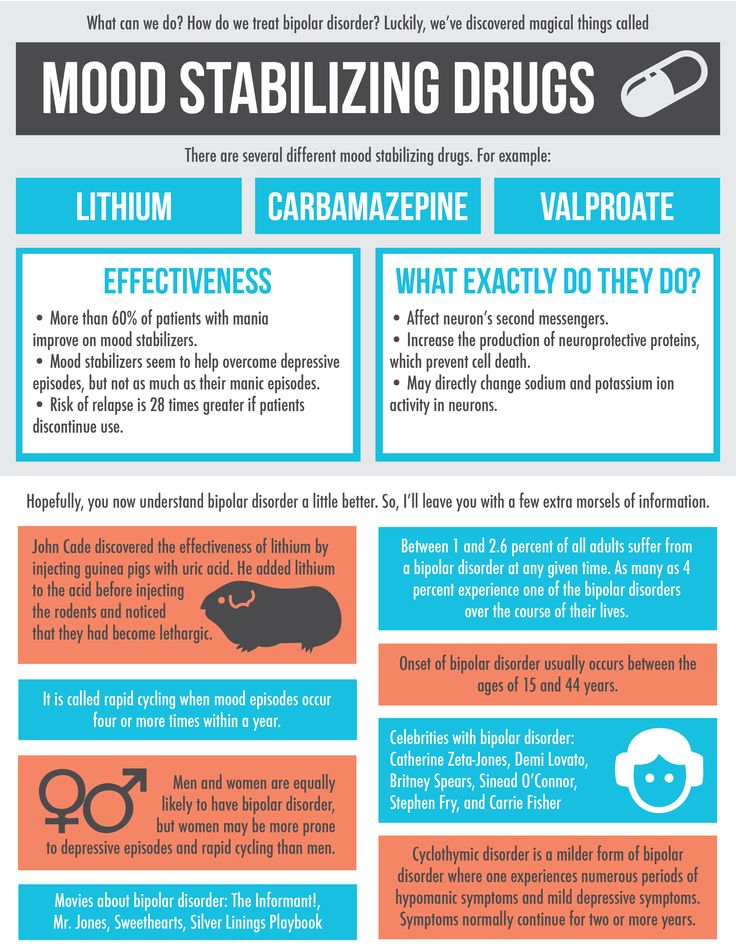 One of these conditions is depression. Depression in bipolar disorder is pronounced, with vivid symptoms. It can last up to a year and is manifested not only by low mood, lack of ability to enjoy and interest in ongoing events, but also by psychosis, when ideas of self-accusation arise, the patient feels inferior, unnecessary, poisoning the life of others. There are also nihilistic thoughts about suffering from some kind of severe illness, despite medical evidence to the contrary. There may be delusional thoughts, as well as suicidal thoughts and even attempts.
One of these conditions is depression. Depression in bipolar disorder is pronounced, with vivid symptoms. It can last up to a year and is manifested not only by low mood, lack of ability to enjoy and interest in ongoing events, but also by psychosis, when ideas of self-accusation arise, the patient feels inferior, unnecessary, poisoning the life of others. There are also nihilistic thoughts about suffering from some kind of severe illness, despite medical evidence to the contrary. There may be delusional thoughts, as well as suicidal thoughts and even attempts.
The other pole of bipolar disorder is a hypomanic state or hypomania, the characteristic features of which are an increased euphoric emotional background, the patient is constantly on the move, hyperactive, and is distinguished by very fast, associative speech. The patient is constantly cheerful, often hypersexual, almost always awake or sleeping 2-3 hours a day.
Hypomania is often followed by a manic bipolar state with psychotic manifestations. The patient develops convictions in his own greatness, he believes that he is capable of anything, feels that he has a special calling in this world or that he is a descendant of great people. In extended manic episodes of mania with psychotic manifestations, anger, irritability, and direct aggression often occur. This condition leads the patient into extremely unpleasant and sometimes dangerous situations.
The patient develops convictions in his own greatness, he believes that he is capable of anything, feels that he has a special calling in this world or that he is a descendant of great people. In extended manic episodes of mania with psychotic manifestations, anger, irritability, and direct aggression often occur. This condition leads the patient into extremely unpleasant and sometimes dangerous situations.
In addition to the typical symptoms of the disease, there are a large number of comorbid mental disorders. Comorbid mental disorders are those that accompany the underlying disease. The most common disorder of this kind is anxiety, which is manifested, among other things, by nonspecific autonomic symptoms, including sweating, palpitations, tremors of the limbs, various disorders of the gastrointestinal tract, dizziness, headaches, suffocation, and many others. In the case when these symptoms occur suddenly, mainly in public places, they are called panic attacks.
Types of bipolar disorder
Bipolar disorder can be of Ι and ΙΙ types.
Bipolar I disorder is a condition in which the patient has persistent manias, i.e. overexcitation, enthusiastic inappropriate behavior, manic psychosis, as well as severe depressions. Symptoms of this type are more severe, so hospitalization is indicated in most cases.
Bipolar I disorder is characterized by short periods of hypomania followed by periods of deep depression. Hypomania is a pre-manic state with less active manifestations. Hypomania lasts a very short period of time - from several days to several hours, so sometimes patients do not even notice them and do not inform the doctor about it. Only careful, painstaking work with the patient makes it possible to identify hypomania, make the correct diagnosis and prescribe treatment.
Phases of bipolar disorder
There are several phases of bipolar personality disorder:
- Depressive (unipolar depression). People experience a depressed mood, despair and despondency, complain of a lack of energy and mental concentration, they can either eat too much or too little and sleep.

Depersonalization and derealization may occur at the peak of bipolar depressive disorder. The boundaries of their own "I" and the world around them become blurred, patients experience difficulties in perceiving what is happening. Familiar places seem new, the colors of the surrounding world change, the patient constantly experiences a feeling of "déjà vu". Sounds become muffled, even if someone is talking very close, it seems to the patient that the voice is coming from afar.
- Manic (hypomanic). In this state, patients are full of energy, overly happy or optimistic, euphoric, and have extremely high self-esteem. At first glance, these are positive signs, but when a person experiences large-scale manic episodes, these symptoms and such an emotional state can reach dangerous extremes. A patient in this phase may indiscriminately spend huge amounts of money or behave carelessly, not realizing the full danger. In conversation, people may choke on words, speak at a high speed, or jump from one thought to another.
 These episodes may also be accompanied by delusions of grandeur or the adoption of serious decisions without thinking about the further consequences.
These episodes may also be accompanied by delusions of grandeur or the adoption of serious decisions without thinking about the further consequences.
In the development of the manic phase, the following stages of development can be distinguished:
- Hypomania - increased excitement, emotional upsurge.
- Mania - all signs are more pronounced, aggression, irritability, irascibility and rage are possible.
- Phase peak. The patient constantly experiences nervous excitement, he cannot relax. All his emotions are "heated" to the limit, coordination of movements is disturbed, thoughts are illogical and abrupt, in speech he constantly jumps from one sentence to another.
- Relief of symptoms. The patient gradually calms down. Movement disorders are on the decline. The speed of thinking and increased emotional mood remain unchanged.
- Return to normal.
- Mixed. Sometimes people have complaints that are characteristic of both depression and mania at the same time.
 They may also experience frequent phasing—4 or more episodes in one year.
They may also experience frequent phasing—4 or more episodes in one year.
In the intervals between depressive and manic phases in bipolar disorder, there is a light period during which the general background of mood becomes relatively stable, the person continues to adequately respond to certain events, the emotional sphere is under his control. This is the main criterion for remission of bipolar disease.
Bipolar disorder in women
Statistically, type Ι bipolar disorder occurs with the same frequency in men and women, and type ΙΙ disease is more often diagnosed in women. It is also known that the female course of the disease is characterized by rapid cycles and mixed episodes. Comorbidities often include eating disorders, borderline personality disorder, alcohol or drug addiction, and psychotropic drug abuse. Women are more susceptible to such somatic diseases as migraine (intense headaches), thyroid pathologies, diabetes, and obesity.
For women, a special technique is being developed to alleviate this disorder, since from adolescence to menopause there are specific changes in hormonal levels that must be taken into account. In addition, psychotropic substances, which are supposed to stabilize the condition, can adversely affect the intrauterine development of the fetus if the woman is in position. It is noted that in the first trimester of pregnancy this disorder is milder, but after childbirth they often have to deal with postpartum depression. Thus, at each stage of the development of the female body, a competent doctor must review and adjust the treatment regimen. Often in the treatment of women, a complex method is used that combines drug therapy and cognitive-behavioral or interpersonal therapy with a psychotherapist. This approach gives the fastest results.
In addition, psychotropic substances, which are supposed to stabilize the condition, can adversely affect the intrauterine development of the fetus if the woman is in position. It is noted that in the first trimester of pregnancy this disorder is milder, but after childbirth they often have to deal with postpartum depression. Thus, at each stage of the development of the female body, a competent doctor must review and adjust the treatment regimen. Often in the treatment of women, a complex method is used that combines drug therapy and cognitive-behavioral or interpersonal therapy with a psychotherapist. This approach gives the fastest results.
Treatment for bipolar disorder
Attempts to get rid of bipolar disorder on your own do not bring the desired result and, ultimately, lead to an aggravation of the situation, including the development of drug or alcohol addiction. In the diagnosis of the disease, keeping a mood diary can help, where the patient records all his thoughts, emotions, feelings, changes in mood. Such records will help the doctor to assess the mental state in detail and make the correct diagnosis. If you suspect bipolar disorder, you should consult a doctor, and the sooner a person realizes that he has a disease and comes to the clinic for help, the sooner professional help will be provided to him and painful symptoms will be replaced by a stable condition. It is impossible to get rid of the disease on your own, since a person cannot fully adequately assess not only his actions, but also the alternation of the phases of the disease.
Such records will help the doctor to assess the mental state in detail and make the correct diagnosis. If you suspect bipolar disorder, you should consult a doctor, and the sooner a person realizes that he has a disease and comes to the clinic for help, the sooner professional help will be provided to him and painful symptoms will be replaced by a stable condition. It is impossible to get rid of the disease on your own, since a person cannot fully adequately assess not only his actions, but also the alternation of the phases of the disease.
Bipolar disorder is one of the few mental disorders in which medication is indicated in 100% of cases, and psychotherapy is an auxiliary tool. This disease is incurable, but its diagnosis and treatment is extremely important. Treatment can reduce the number of episodes, their severity and intensity, as well as prevent negative life events, help prevent relationship breakups, job loss, and even suicidal attempts. Thus, the quality of life of a patient with bipolar disorder who is undergoing treatment will be several times higher than that of a person who neglects treatment.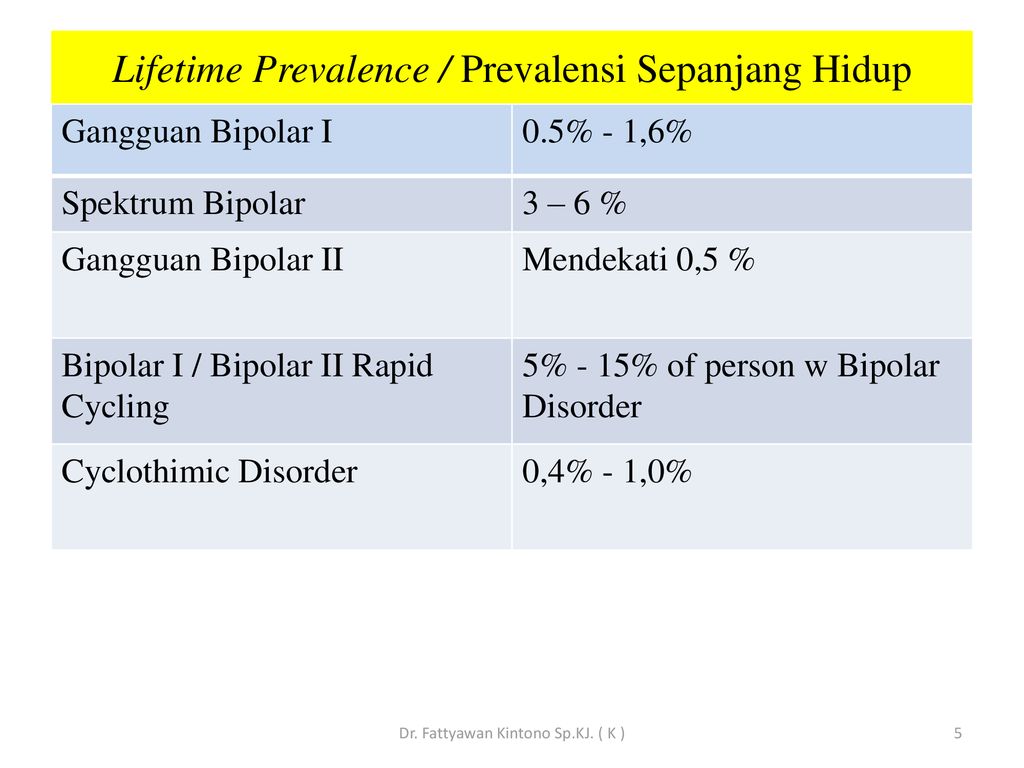 If the patient loses touch with reality and harms himself and others, he is subject to hospitalization, outpatient treatment in this case is not permissible.
If the patient loses touch with reality and harms himself and others, he is subject to hospitalization, outpatient treatment in this case is not permissible.
If you have a disease, it is recommended to exclude coffee, strong tea, alcoholic and energy drinks from your diet in order not to provoke an overexcited state. If possible, you should stop smoking and in no case should you take even soft drugs. It is also very important to establish a sleep pattern, sleep at least 8 hours a day and try to go to bed at about the same time. You should learn to recognize mood swings and notice the early manifestations of new episodes.
If you suspect that you have bipolar personality disorder, there is no need to panic, only a doctor can diagnose the disease, so you need to make an appointment with a psychotherapist with extensive experience in managing such patients at our MedAstrum clinic. If the diagnosis is confirmed, the doctor will make the necessary medication, if necessary, prescribe psychotherapeutic sessions and give recommendations for further lifestyle adjustments.