Ocd is real
Are OCD Thoughts Real? | Intrepid Detox
According to the National Institute of Mental Health, more than 1% of adults in America have obsessive-compulsive disorder (OCD). It is estimated that almost 30% of people who have OCD also have a substance use disorder. Unfortunately, many people with mental health disorders look to substances to numb their symptoms. Learning about OCD and how it is expressed can be the first step to better managing its symptoms.
So, what does OCD feel like and how can a person get help for the disorder? Learn more below.
Jump to Section
Is OCD a Real Disorder?
Yes, OCD is a real disorder. Obsessive-compulsive disorder is characterized by irrational fears and thoughts that lead to compulsions. Fears and thoughts are often referred to as obsessions, while compulsions are compulsive behaviors. OCD looks different in each individual. The OCD experience, or how OCD is expressed, can range greatly from person to person. OCD may center around fear of germs or arranging objects in a specific manner.
The mental disorder is not limited to those obsessions and compulsions, though.
What Does OCD Feel Like?
Though OCD can vary, one thing about the disorder is somewhat consistent: Overwhelming thoughts are often at the root of the OCD experience. These thoughts can be so powerful to some that they can convince them otherwise on a subject they were certain about. For example, let’s say you leave the house and lock the door. On your ride to work, you begin having thoughts that you left the door unlocked. These thoughts can become so powerful that you begin to believe that you left the door unlocked.
In this case, someone with OCD may even turn around because the urge to check the door becomes so overwhelming. Someone with severe OCD will experience this type of feeling several times a day, interrupting their daily life.
Intrusive thoughts can be hard to ignore, especially for someone with obsessive-compulsive disorder. Someone with OCD can lose control of their thoughts entirely. In this case, the mind becomes completely absorbed by obsessions.
In this case, the mind becomes completely absorbed by obsessions.
What Are 5 Symptoms of OCD?
What does OCD feel like? OCD symptoms can be classified into five themes. These themes do not cover every single obsession. However, most forms of OCD fall within these themes:
- Fear of dirt or contamination
- Difficulty tolerating uncertainty; constant doubting
- Requiring things to be symmetrical or orderly
- Awful thoughts about the loss of control or potentially harming yourself or others
- Unwanted and unreasonable thoughts, including sexual, religious, or aggressive subjects
Potential examples of these obsessions include:
- Not wanting to touch objects other people have touched due to contamination
- Doubts that you turned off the stove, locked the door, or similar scenarios
- Severe stress when particular objects aren’t facing a certain way
- Cognitive images of you driving your car into people
- Urges to act inappropriately in public, thoughts about shouting vulgarities
- Sexual images
- Avoiding situations that may trigger OCD, including shaking hands or touching certain things
What Is the Vicious Cycle of OCD?
The OCD experience involves having thoughts or impulses occur unwillingly. You likely do not want to be having these thoughts or ideas, but you can’t stop them. As mentioned, these thoughts can disrupt daily life and cause issues at home or work.
You likely do not want to be having these thoughts or ideas, but you can’t stop them. As mentioned, these thoughts can disrupt daily life and cause issues at home or work.
Naturally, people tend to deal with obsessive thoughts by using compulsions, also known as behaviors or rituals, to make the obsessions go away. The vicious cycle of OCD roots itself deeply since these compulsions can sometimes work temporarily. Therefore, you may find yourself acting out through rituals over and over again. For example, to avoid the fear of contamination, you may construct cleaning rituals that you perform elaborately. Though it may feel like you are acting on your obsession, you ensure that the obsessive thoughts come back even stronger.
This situation can cause someone to be riddled with anxiety. Anxiety plays a large role in OCD and is often the reason OCD can be so disruptive and time-consuming. The vicious cycle of OCD generally works in this order:
- Obsessive thought
- Anxiety
- Compulsive behavior
- Temporary relief
What Does OCD Do To A Person?
The OCD experience can manifest itself in many ways. One individual’s OCD experience may differ completely from another’s. Regardless, people with severe OCD deal with obsessions and compulsions that may take up hours of their day. This can be an obvious detriment on family and social relationships, education, and employment.
One individual’s OCD experience may differ completely from another’s. Regardless, people with severe OCD deal with obsessions and compulsions that may take up hours of their day. This can be an obvious detriment on family and social relationships, education, and employment.
As obsessions and compulsions become more severe, avoidance also becomes an issue. OCD can make an individual attempt to avoid any scenario that may trigger their OCD. For some, this could result in them staying within the boundaries of their home indefinitely.
Obsessive fears can make it difficult for people with OCD to eat, shop, drink, read, and perform normal daily responsibilities. In many cases, OCD is compounded by symptoms of other mental health disorders, such as depression, anxiety, panic disorder, and more.
If someone becomes embarrassed of their symptoms, they may go to great lengths to hide them. Many family members of people suffering from OCD can become distressed and involved in their loved one’s rituals.
Are OCD Thoughts Real or Not Real?
Intrusive thoughts are a key component of OCD. Just because you are having thoughts does not mean they are real. Intrusive thoughts are not only limited to words that show up in your mind. These thoughts can take the form of sensations, ideas, memories, urges, and images.
Even though some of these thoughts can be “blamed” on OCD, it does not make them less distressing. People with OCD may have a difficult time realizing their thoughts are just thoughts. Uncertainty leads to a strong distress response. Tolerating the distress and when the mind and body go on high alert is difficult. At this point in the OCD cycle, the individual feels the need to act on these thoughts, attempting to make sure the thoughts do not come to fruition. Though the thoughts may not be “real,” it is easy for someone with OCD to get “stuck” by fighting the thoughts and protecting against them.
What Can Trigger OCD?
The cause of OCD is still unknown. Scientists continually investigate the cause of OCD, other than it being passed on genetically. One scientific journal found links between inflammatory biomarkers and OCD. This evidence requires further investigation before it can be solidified. If this were the case, some form of anti-inflammatory medication could treat OCD.
Scientists continually investigate the cause of OCD, other than it being passed on genetically. One scientific journal found links between inflammatory biomarkers and OCD. This evidence requires further investigation before it can be solidified. If this were the case, some form of anti-inflammatory medication could treat OCD.
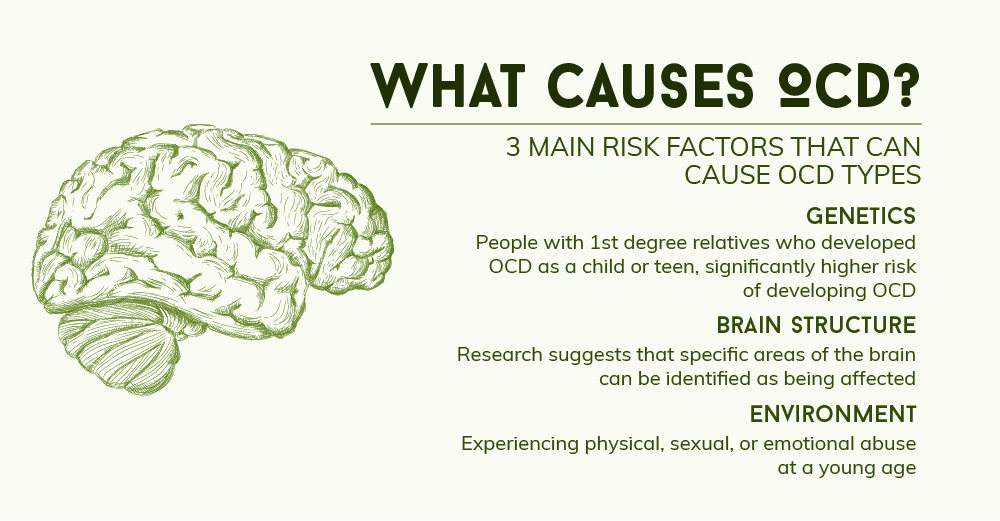
Some theories about the causes of OCD include:
- People experiencing anxiety begin using compulsions as a learned behavior. Once associated with relief from anxiety, the behavior becomes repetitive and looks like an expression of OCD.
- Hereditary and genetic factors pass on OCD.
- People with OCD have functional and structural abnormalities in the brain.
- Symptoms associated with OCD stem from distorted beliefs that are continually reinforced.
OCD likely stems from several factors. Since each person’s OCD experience is different, that theory is more than likely. The underlying expression and functions of OCD may be influenced by personality traits, hormonal changes, and life events.
The underlying expression and functions of OCD may be influenced by personality traits, hormonal changes, and life events.
Treatment For OCD
Another study found that mice with a higher level of Immuno-moodulin (an immune protein) exhibited OCD-like behaviors. During the study, scientists gave the mice an antibody that blocked Immuno-moodulin, and their repetitive behaviors decreased.
Though there is no absolute cure for OCD, many treatments can help manage even the most intense symptoms. Treatments may include individualized therapy, such as cognitive behavioral therapy (CBT) or exposure and response therapy (ERP). For some, medications like SSRIs (serotonin reuptake inhibitors) are an option. The best option is to talk to a mental health professional.
There are even support groups that people with OCD can benefit from. Support groups consist of individuals dealing with similar issues that act as a communication and support system.
Cognitive Behavioral Therapy
CBT helps by changing the individual’s patterns of behaviors, beliefs, and thinking. Clinical professionals help their clients by promoting control over their symptoms. During therapy sessions, the specialist may even expose their client to situations that trigger their obsessions. While doing so, the therapist will help them develop tools that reduce their avoidance and compulsion behaviors.
Clinical professionals help their clients by promoting control over their symptoms. During therapy sessions, the specialist may even expose their client to situations that trigger their obsessions. While doing so, the therapist will help them develop tools that reduce their avoidance and compulsion behaviors.
The process is often gradual, and it begins with less intensive triggers. Consistent exposure can help prevent compulsions and reduce the anxiety that surrounds the triggers. This process is called exposure and response therapy.
What Happens If OCD Is Left Untreated?
People with mild OCD may find that they can adapt to their condition. The symptoms that they experience may only interfere with their life in inconsiderable ways. However, symptoms of OCD tend to worsen over time if untreated. As people with OCD get older, they may find that they are altering certain aspects of their life to avoid certain triggers.
Compulsions can drive individuals subconsciously. As OCD compulsions worsen, you may find that you:
As OCD compulsions worsen, you may find that you:
- Avoid gatherings
- Avoid going outside unnecessarily
- Stop visiting particular friends or family members
- Have difficulty focusing on work because you are consumed by thoughts
- Isolate yourself
- Engage in compulsions that interfere with hobbies and other activities
- Miss school or work due to avoiding triggers
OCD and addiction are common co-occurring disorders that require professional intervention. In severe cases, some people with OCD look to substances to numb their symptoms. Treatment centers like Intrepid Detox Residential offer dual diagnosis programs explicitly designed to deal with OCD and addiction.
Find Help With Intrepid Detox Residential
Here at Intrepid, we strive to offer treatments that target co-occurring disorders. We provide a range of mental health services designed to help our clients develop tools to manage their mental health while recovering from addiction.
If you would like to learn more about what OCD feels like and what we offer at Intrepid Detox Residential, please contact us today.
Real Event OCD: Symptoms, Treatments, and More
Obsessive-compulsive disorder (OCD) is a condition that is characterized by a cycle of recurring and intrusive thoughts and behaviors. These thoughts, or obsessions, can lead to uncontrollable behaviors, or compulsions.
In the mind of a person with this mental health condition, the compulsions should help alleviate the obsessions. However, they rarely do.
Instead, the person performs the compulsions over and over again without resolution. The thoughts and compulsions can interfere with the person’s ability to:
- perform daily tasks
- hold a job
- leave their home
In most cases, these intrusive thoughts are worries or anxieties about things that might happen. You might leave the oven on and start a fire.
Sometimes, however, these obsessions may come from thinking about something that already happened.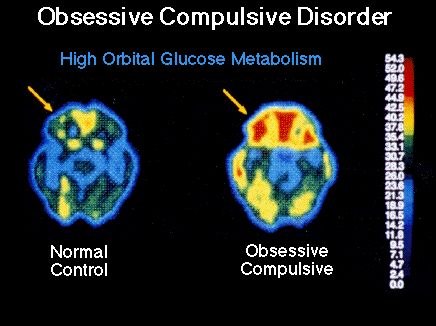 This type of OCD is called real event OCD.
This type of OCD is called real event OCD.
According to the Anxiety and Depression Association of America, real event OCD is not a unique diagnosis. It is OCD that develops when responding to actual events.
Real event OCD occurs when you have obsessive thoughts about an event that occurred in your life. This obsession-compulsion cycle of real event OCD may look a bit different from other types.
Primarily, the compulsion is an inability to stop thinking about the event. You play it over and over again in your mind, seeking answers that you cannot find.
But like other forms of OCD, real event OCD can often be treated if it is recognized and addressed. Keep reading to learn the symptoms of real event OCD and who can help treat it.
The driving force behind OCD is doubt. You may ask yourself questions such as:
- Did you turn the stove off?
- Will the stove start a house fire if you didn’t turn it off?
- Did you lock the door before you got into bed?
- Will you be robbed (or worse) in your sleep?
- Is the door handle to your apartment dirty?
- Can you even clean the door handle well enough to avoid germs?
These are a few types of obsessive thoughts. They typically deal with theoretical situations, or something that might arise.
They typically deal with theoretical situations, or something that might arise.
With real event OCD, however, the recurring thoughts are of a specific event that happened to you. That means the obsessive thoughts and compulsions are typically related to something you did or did not do.
Symptoms of real event OCD include:
- Mental review. People with real event OCD spend excessive time replaying events in their minds. They analyze them from every angle and perspective. They play every word, action, and event back in their minds. Often, they try to decide something black and white about the event: Do their actions make them a bad person? Did they make the right choice?
- Reassurance seeking. People with real event OCD cannot answer their worries. So, they may bounce the events and their feelings off other people in their lives to seek reassurance that the worst things they’re thinking aren’t going to come true or haven’t happened.
- Catastrophizing. People with real event OCD create cognitive distortions. In other words, they take something that would quickly pass through the mind of another individual and sit on it for longer than they should. They often twist or change it, so they find problems with it. From that, they draw the worst conclusions about what happened and about themselves.
- Emotional reasoning. People with real event OCD confuse feelings for facts. People with this condition might convince themselves that because they feel guilty, they must have done something bad.
- Urgency. To people experiencing this cycle of intrusive thoughts, finding resolution to situations can be increasingly important. They may feel that they have to find the answer now. This may make the compulsions worse.
- Magnification. People with this condition may have a difficult time separating themselves from the significance of an event because of the intense focus on the event.
 In other words, an inconsequential choice becomes highly significant and meaningful because of the distortions caused by OCD.
In other words, an inconsequential choice becomes highly significant and meaningful because of the distortions caused by OCD.
It’s unclear why some people develop real event OCD and others don’t. Even two people who experience the same event together may have different responses. One may develop OCD, while the other doesn’t.
For that reason, it’s hard to know precisely what types of events trigger real event OCD, but anecdotal evidence suggests that these situations may play a role:
- abuse
- neglect
- family disruption
- relationship changes or interpersonal issues
- traumatic events
Then again, the event may not amount to a single significant life event. It may result from a chronic stressful situation, or a stressful life event like moving.
Although events like these are ordinary, for someone with OCD the stress may be so significant that it triggers the obsessive thoughts and compulsions.
For example, someone with real event OCD may focus on an interaction they had as a student, decades before the time the obsessive thoughts begin. This focus may be the result of a similar experience.
This focus may be the result of a similar experience.
It may also come back up if you see the other person again or if something happens to them.
OCD is a persistent state of doubt. Everyone has doubts from time to time, but people with this mental health condition face doubts and anxieties that are obsessive and intrusive.
Indeed, they feel that they cannot manage them. That, in turn, can interfere with daily life.
Your doubts and worries about something that happened in your life could indicate symptoms of real event OCD if you:
- feel “stuck” thinking about the same event(s) over and over
- cannot control the thoughts
- cannot find resolutions
- seek reassurance but don’t find the support sufficient
- experience significant problems in your daily life due to these thoughts
- have trouble focusing or being productive at school or work
- have strained relationships from your obsessive thoughts and doubts
- have previously experienced OCD
Real event OCD can be treated. As with other types of OCD, it may require a combination of treatments to find something that helps you. But you do not have to live in this cycle.
As with other types of OCD, it may require a combination of treatments to find something that helps you. But you do not have to live in this cycle.
The most common treatments for real event OCD include:
- Medication. Serotonin reuptake inhibitors (SRIs) and selective serotonin reuptake inhibitors (SSRIs) are sometimes prescribed for people with OCD. These medicines impact the brain’s natural chemistry to help stop or slow the overactive thoughts.
- Psychotherapy. Therapies such as cognitive behavioral therapy (CBT) and habit reversal training are used for OCD treatment. These types help people with real event OCD learn how to stop and redirect the intrusive thoughts before the compulsive cycle begins.
- Exposure and response (ERP) therapy. This type of psychotherapy is used often with OCD. With this therapy, a mental health professional will develop ways to expose you to your triggers. Together, you will learn to unpair the real event from the feelings that have caused so much doubt and anxiety.
Online therapy options
Read our review of the best online therapy options to find the right fit for you.
In addition to traditional treatments, other practices may help you eliminate obsessive thoughts. These include:
- Mindfulness. Blocking or stopping thoughts may not work. The practice of mindfulness encourages people to experience thoughts and feelings, and “sit” with them. They can experience thoughts as they happen, and usher them out.
- Mental exercises. With a mental health professional, you can try mental health exercises to stop your compulsive examinations. They might include refocusing or negotiating with your mind. It will take time and attention to make this work, but recognizing the compulsive thoughts helps stop them.
- Take care of yourself. A tired mind may be difficult to manage. Get adequate sleep, eat a balanced diet, and exercise regularly. These practices can help your overall health and treatments.
If you think you’re experiencing real event OCD, consider talking with a healthcare professional to determine next steps. These resources can help:
- Your healthcare provider. Talk with a doctor, nurse practitioner, or other clinician to find a mental health professional in your area that may be able to help you answer questions and find treatment.
- Substance Abuse and Mental Health Services Administration (SAMHSA). Their treatment referral hotline (1-800-662-HELP or 1-800-662-4357) can connect you with resources in your area. Their Behavioral Health Treatment Locator can also be a good resource.
- National Institute of Mental Health (NIMH). The NIMH Help for Mental Illnesses page lists a variety of resources that can guide you to the best providers.
Many people experience these feelings because of past events:
- regret
- shame
- stress
That’s typical. But what isn’t typical is an inability to stop thinking about those feelings.
People with real event OCD cannot always manage their obsessive thoughts and compulsive actions. They often seek to clarify what happened and find a “resolution.” But that’s not always possible.
However, with treatment and continuing mental health exercises, people with real event OCD can find relief from their obsessive thoughts.
And they may manage their daily lives without the worry of these doubts and anxieties overrunning their minds.
symptoms, how to get rid of and treat
Olya Selivanova
struggles with obsessive-compulsive disorder
Author profile
Since childhood, I have suffered from obsessive thoughts.
When I was nine years old, I was reading a book, when suddenly the thought occurred to me: “If you don’t finish reading today, your mother will die.” The thought frightened me, I put down the book and cried, but I had to return to reading so that my mother would not die.
From that moment on, the frightening thoughts were different. I could suddenly change the route, because the thought came to my mind: “It is not safe to go further. Get around." There were thoughts to harm loved ones: push, hit, pour over. At such moments, I thought that an evil force had entered into me, and I began to count to myself, imagined how the numbers increased in order in size and knocked bad thoughts out of my head.
I could suddenly change the route, because the thought came to my mind: “It is not safe to go further. Get around." There were thoughts to harm loved ones: push, hit, pour over. At such moments, I thought that an evil force had entered into me, and I began to count to myself, imagined how the numbers increased in order in size and knocked bad thoughts out of my head.
By the time I was twelve, it all came to naught, and as a teenager, I decided that it was just childish oddities. But seven years later, the obsessive thoughts returned, and the doctor at the neuropsychiatric dispensary diagnosed me with Obsessive-Compulsive Disorder. I'll tell you how I was treated and how I live now.
Go see a doctor
Our articles are written with love for evidence-based medicine. We refer to authoritative sources and go to doctors with a good reputation for comments. But remember: the responsibility for your health lies with you and your doctor. We don't write prescriptions, we make recommendations. Relying on our point of view or not is up to you.
Relying on our point of view or not is up to you.
What is obsessive-compulsive disorder
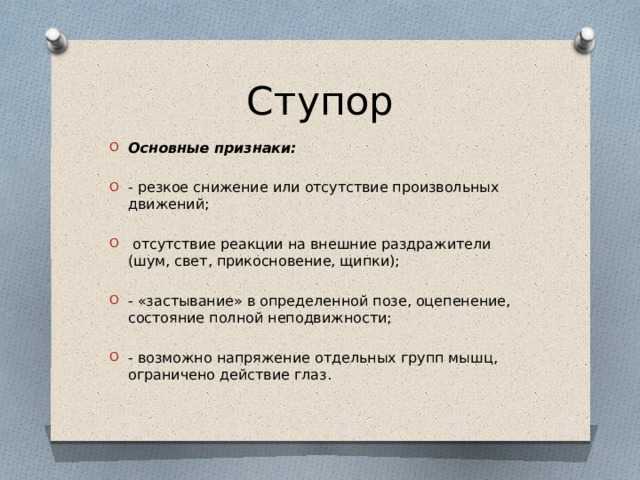
Obsessive-compulsive disorder is a mental illness in which a person has obsessive thoughts and compulsive actions.
What is Obsessive-Compulsive Disorder - Mayo Clinic
Obsessive thoughts - obsessions - usually revolve around certain topics: fear of harming yourself and others, fear of germs and toxic substances, the need to organize everything. They appear suddenly or are provoked by external circumstances, such as a sharp object or the word "last".
Intrusive thoughts cannot be ignored, they cause anxiety or disgust. In response to them, a person has compulsions - a strong desire to perform certain actions that, according to his feelings, will get rid of such thoughts. Compulsions are difficult to resist: the anxiety will grow until the person gives up.
For example, the obsessive thought that a person will become infected after touching a doorknob will provoke compulsive actions - repeated washing of hands, sometimes for several hours in a row.
/shizofreniya/
How much does it cost to support a relative with a mental disorder
I try not to touch doorknobs in public places and always make sure the door is closed. Do I have OCD?
Sergey Divisenko
psychotherapist
If a person's condition does not interfere with himself or others, then everything is in order, if it interferes, a disorder can be suspected. In the case of checking the door, one can say that checking if the door is closed once is not a problem, rechecking the door several times in a row and doing it systematically is already a problem.
To understand whether or not there is OCD, the doctor pays attention to how often the patient has obsessive thoughts and compulsive actions and how they affect his life. If symptoms occur more frequently in two weeks than in seven days and interfere with daily activities, it is probably OCD.
In this case, the symptoms should have the following characteristics:
- The person should evaluate them as his own thoughts and desires.
- There must be at least one thought or action that the person unsuccessfully resists.
- The thought of a person performing a compulsive action should not in itself be pleasurable. The fact that an action will help reduce anxiety is not considered pleasant in this sense.
- Thoughts or actions must be repeated.
How obsessive-compulsive disorder is treated
OCD is considered a lifelong disorder, but with treatment it is possible to achieve remission: to get rid of obsessive thoughts and compulsive actions for a long time or to reduce their number.
Medical treatment. The main drugs for the treatment of OCD are antidepressants of the SSRI group. They increase serotonin levels in the brain, making OCD symptoms less likely to occur.
Treatment options for OCD - NHS
Depending on the course of the disease and symptoms, along with antidepressants, the doctor may prescribe other drugs: tranquilizers, neuroleptics or mood stabilizers.
Cognitive behavioral therapy. This is a type of psychotherapy during which a person learns to control their emotional response to intrusive thoughts. As a result of therapy, obsessive thoughts cease to cause anxiety and compulsive actions.
Cognitive behavioral therapy - NHS
Order of the Ministry of Health of the Russian Federation of September 16, 2003 No. 438 "On psychotherapeutic care"
Psychiatrists, psychotherapists and psychologists are involved in the treatment of OCD in Russia. Psychiatrists prescribe prescription drugs. Psychotherapists and psychologists conduct psychotherapy sessions.
How I was diagnosed
At the age of 19, the development of the disease took a new turn. I was washing the kitchen knife and I had an obsessive thought that I was losing control and could cut myself and the guy who was nearby at that moment. So I began to avoid sharp objects, there was an irresistible desire to hide or throw them away.
Obsessive thoughts revolved around the topic of death: drinking nail polish remover, bleach, vinegar, throwing yourself under a vehicle or jumping out of a window. Because of this, I removed all dangerous liquids from the house and stayed away from open windows, highways and train station platforms. I didn’t sleep well at night, suffered from anxiety, considered myself crazy and dangerous, and began to move away from everyone.
I also doubted everything. Even if I just performed an action, it seemed to me that it was not completed. I opened the door to make sure that it had been closed before, closed it again, pulled the handle, asked those around me if the door was exactly closed. I could wake up at night and see if the stove was turned on, although before going to bed I went up to it and stared without blinking - so that it would crash into my memory that it was definitely turned off. My young man, seeing all this, insisted that we try to see a psychologist.
In Irkutsk, where I live, psychiatric care can be obtained free of charge at the regional psycho-neurological dispensary. I turned to the psychotherapeutic department of the dispensary for a consultation with a psychologist. At the reception, they brought me a card and said that there was no appointment with a psychologist for the next few days, but I could get to a psychiatrist: there are fewer people who want to see him.
I turned to the psychotherapeutic department of the dispensary for a consultation with a psychologist. At the reception, they brought me a card and said that there was no appointment with a psychologist for the next few days, but I could get to a psychiatrist: there are fewer people who want to see him.
/spravka/
How to get a certificate from the PND
At the appointment with the psychiatrist, I told about what was happening to me. The doctor was not surprised and said that it was an obsessive-compulsive disorder. It was the first time I heard my diagnosis, but I didn't believe it. On the Internet, I came across information that OCD is only pedantry, handwashing, fear of germs and perfectionism, and not the creepy things that come to my mind. The psychiatrist said that OCD was treated with antidepressants and offered to write a prescription, but I refused treatment because I thought they were serious drugs that would do more harm than help.
How a visit to a neuropsychiatric dispensary with OCD will affect later life
Sergey Divisenko
psychotherapist
The patient could move freely, drive a car, use weapons and work.
With an OCD diagnosis, you can still work in any job, there are no legal barriers to this. With regard to cars and weapons, the situation has changed. In 2014 and 2015, government decrees appeared, according to which OCD became a contraindication for driving and owning weapons.
However, from a psychiatrist's point of view, a person diagnosed with OCD can drive a car and use a weapon. Doctors of the psycho-neurological dispensary still give a certificate about this, but they do it through a medical commission.
Treatment
First hospitalizationMy condition worsened, I tried to ignore obsessive thoughts. But the more I resisted them, the stronger they became. In addition, anger, irritability and constant fatigue appeared.
With new symptoms, I decided to see an endocrinologist, because I heard that this happens with problems with the thyroid gland. According to the results of ultrasound and hormone tests, the thyroid gland was in order. Then I made an appointment with a neurologist, but he also said that this was not his profile. Both doctors suggested that my constant fatigue, anger and irritability were symptoms of depression and advised me to seek psychiatric help.
According to the results of ultrasound and hormone tests, the thyroid gland was in order. Then I made an appointment with a neurologist, but he also said that this was not his profile. Both doctors suggested that my constant fatigue, anger and irritability were symptoms of depression and advised me to seek psychiatric help.
Symptoms of clinical depression - NHS
I researched information about depression and realized that antidepressants could help, all I had to do was get a prescription. I came to the psychotherapeutic department again, but there was already another psychiatrist there. Since my condition worsened, instead of a prescription, he wrote out a referral for hospitalization in a day hospital. I had prejudices about a psychiatric hospital, so I did not want to visit the hospital. But there was no strength to argue with the psychiatrist.
This is how a referral for hospitalization to a day hospital looks like The next day I was already in the hospital. During the registration, the psychiatrist on duty asked what I was complaining about, measured the pressure and examined whether there were injuries on the body. It turned out to be difficult for me to talk about the symptoms: there was a feeling that they would not believe me, or vice versa, they would believe me so much that they would put me in a round-the-clock hospital. But everything was fine, the psychiatrist wrote down the data on the card, gave it to the orderly, and together with him sent me to the head.
It turned out to be difficult for me to talk about the symptoms: there was a feeling that they would not believe me, or vice versa, they would believe me so much that they would put me in a round-the-clock hospital. But everything was fine, the psychiatrist wrote down the data on the card, gave it to the orderly, and together with him sent me to the head.
The manager looked at the card, confirmed the diagnosis of OCD and depression, and prescribed treatment: an antidepressant, an antipsychotic, a mood stabilizer, tranquilizer tablets, and injections of B vitamins.
/guide/vitamins/
Vitamins: what foods contain and how to take supplements
The routine in the hospital was as follows: I arrived at eight in the morning, had breakfast and took the prescribed pills, took injections, dined and went home. Tablets were issued immediately for one day, but they could also be issued for two days, for example, before the weekend. Once after the injection, I went to an appointment with a clinical psychologist, he gave various tests and questionnaires that tested logic and intelligence.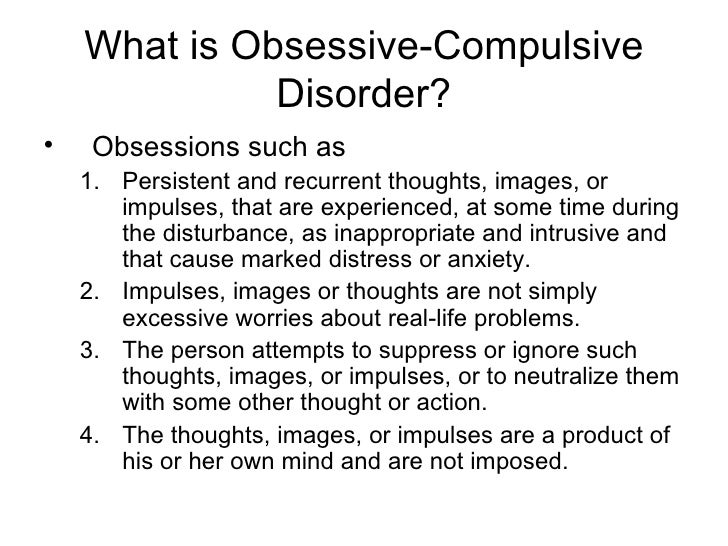
About three times a week I went to see a psychiatrist in the same hospital. I told her about my condition and asked questions. I thought that as soon as I start taking medication, my mood will rise and my anxiety will go away. But this did not happen, so it seemed that everything was in vain and the treatment had to be abandoned. The psychiatrist explained to me that not all drugs begin to act instantly, she assured me that we were on the right track and we had to wait. These conversations made it easier. In my case, antidepressants began to work only on the third month of admission, when I no longer visited the day hospital.
Treatment at the day hospital lasted a month. All medications, medical consultations and meals were free. I spent money only on the road to the hospital and back - 600 R by public transport for the whole time.
/bye-depression/
“It reminded me of a strict regime sanatorium”: how much I spent on treating depression
After treatment, the symptoms of depression remained, but obsessive thoughts began to bother me less often: I stopped being afraid of open windows and was able to ride the escalator. Treatment had to be continued on an outpatient basis. Before I was discharged, the psychiatrist said that she would transfer my data to the psychiatric department. Now I will need to come to the local psychiatrist for prescriptions for medicines, and turn to him if the condition worsens or questions arise.
During the treatment in the hospital, I doubted everything. Even in being sick. Not only the psychiatrist, but also relatives helped to cope. They noticed the changes, but my young man did not let me stop the treatment
They noticed the changes, but my young man did not let me stop the treatment Treatment
Visiting a local psychiatristAfter I was discharged from the hospital, I came to the registration office of the psychiatric department with a passport and I was immediately sent to the district police officer. The doctor did not change the treatment and wrote out a prescription for the same medicines that were given in the day hospital. In the future, a referral to the district police officer was also not required. I just came to the appointment when I needed to update the prescription.
Government Decree of July 30, 1994 No. 890 with a list of categories of beneficiaries who are entitled to free medicines
District psychiatrists were different: some were polite, some were rude and rude. Using the brute force method, I found two normal specialists - when I made an appointment at the reception, I began to ask to be directed to them. Usually the registrar complied with my request.
Spent in six months of outpatient treatment — 8895 Р
| Preparation | Spending |
|---|---|
| Antidepressants | 5988 R |
| Normotimics | 2384 P |
| Antipsychotics | 419 P |
| Tranquilizers | 104 Р |
Antidepressants
5988 R
Normotimics
2384 R
neuroleptics
419 R
Transquilizers
104 R
Free medicines for the treatment of OCD are provided to certain privileged categories of people. I’m not a beneficiary, so I bought everything with my own money. Pharmacies don’t require a passport, but they put the date of issue of the medicine on the back and don’t sell more than prescribed by prescription. For example, according to a prescription for three months, I was given only three packs of an antidepressant. When I wanted to buy one more to have a supply, the pharmacist refusedTreatment
Second hospitalization and psychotherapy After six months of outpatient treatment, the district psychiatrist recommended to be treated again in the hospital. Antidepressants helped: my mood improved, I got energy and I wanted to live, but I felt a side effect from antipsychotics. I was terribly sleepy, my handwriting changed, it was difficult to write in class and generally follow the train of thought of the teacher. In addition, there were more intrusive thoughts.
Antidepressants helped: my mood improved, I got energy and I wanted to live, but I felt a side effect from antipsychotics. I was terribly sleepy, my handwriting changed, it was difficult to write in class and generally follow the train of thought of the teacher. In addition, there were more intrusive thoughts.
In the day hospital, I was treated by the same psychiatrist as the first time. She adjusted the drug treatment so that I was not bothered by intrusive thoughts. She also said that a psychotherapist had appeared in the hospital and referred me to her for a consultation.
Unlike the psychiatrist's consultations during the first hospitalization, we did not discuss drugs and their effects with the psychotherapist. We talked about what is happening to me and what other methods can be used to combat this, in addition to drugs. At the first appointment, I briefly talked about my lifestyle, obsessive thoughts, compulsive actions, and how I tried to resist them even before the treatment. Then the doctor explained to me what obsessive-compulsive disorder is and how it manifests itself, why my struggle only worsened the condition and led to depression.
Then the doctor explained to me what obsessive-compulsive disorder is and how it manifests itself, why my struggle only worsened the condition and led to depression.
/psychotherapy-search/
How to choose a psychotherapist
We agreed that I would try to keep the number of compulsive acts to a minimum, and I would cope with anxiety from intrusive thoughts with the help of techniques.
Speak key phrases. Thoughts in themselves mean nothing, they can come to mind automatically. We agreed that when I had an obsessive thought, I would simply tell myself that it was a manifestation of OCD. Here are the two phrases that I used: “This is just my thought that…”, “I know that this thought is a manifestation of OCD…” So gradually I stopped identifying myself with my thoughts and realized that thinking about the bad is does not mean to be a bad person.
Separately, we discussed the issue of the materialization of thoughts. When terrible things are spinning in your head, and you hear from everywhere that thoughts are material, you get very worried. We discussed the fact that thoughts are intangible and you can’t invite trouble with them. This made it easier and the degree of emotions decreased.
When terrible things are spinning in your head, and you hear from everywhere that thoughts are material, you get very worried. We discussed the fact that thoughts are intangible and you can’t invite trouble with them. This made it easier and the degree of emotions decreased.
Observe how the body reacts to anxiety. Every time I had anxiety from obsessive thoughts, I did not run away from it, but watched my body. I was shaking, my heartbeat increased, my breathing quickened, but I continued to live it. The psychotherapist said that I would not die from this. Yes, it is unpleasant and scary, but when you live emotions, you gradually learn to cope with them.
Keep a diary. In the course of the sessions, I became convinced that I cannot control the thoughts themselves - it is impossible, but I can control the reaction to them. So I started keeping a diary.
/psychotherapy/
How psychotherapy works
It was necessary to take notes according to the formula: A - situation, B - my thoughts, C - my emotions. Using such records, it is easier to track the thoughts that cause negative emotions and work them out. For example, when I could not fall asleep for a long time, I began to think that something was going wrong, and this caused anxiety. Then I wrote down the whole situation in a diary and instead of negative thoughts I formulated new ones: "My sleep does not depend on my will, and this is normal." It helped to get rid of anxiety, stop trying to sleep and go about your business. About half an hour later I went to bed and fell asleep peacefully.
Using such records, it is easier to track the thoughts that cause negative emotions and work them out. For example, when I could not fall asleep for a long time, I began to think that something was going wrong, and this caused anxiety. Then I wrote down the whole situation in a diary and instead of negative thoughts I formulated new ones: "My sleep does not depend on my will, and this is normal." It helped to get rid of anxiety, stop trying to sleep and go about your business. About half an hour later I went to bed and fell asleep peacefully.
| I also kept a mood diary. Before treatment, there was no point in monitoring the mood: it always turned out to be bad or indifferent | On antidepressants, I began to make entries in a diary every day and could track what affects my mood |
I also kept a mood diary. Before treatment, there was no point in monitoring the mood: it always turned out to be bad or indifferent. On antidepressants, I began to make entries in a diary every day and could track what affects my mood
Before treatment, there was no point in monitoring the mood: it always turned out to be bad or indifferent. On antidepressants, I began to make entries in a diary every day and could track what affects my mood
In the day hospital, I was treated for a month and a half, during which time I had only five sessions with a psychotherapist. All sessions, meals and drugs, as in the first hospitalization, were free. The only thing I had to spend money on was the road to the hospital and back, as well as the original antidepressant instead of the analogue provided in the dispensary. The doctor recommended the original, it suited me better.
3202 Р
spent on medicines and transport for a month and a half of treatment in the hospital
When I was discharged, the doctor told me that I was in a stable condition, the treatment helped me. I myself felt it: the mood was consistently good, and I quickly coped with obsessive thoughts. I was canceled all the drugs, except for antidepressants, then I had to continue taking them, be observed by the district psychiatrist and monitor my condition.
I was canceled all the drugs, except for antidepressants, then I had to continue taking them, be observed by the district psychiatrist and monitor my condition.
Spent one and a half months of treatment in a hospital — 3202 Р
| Expenditures | Spending |
|---|---|
| Antidepressants | 2422 R |
| Transport | 780 Р |
Antidepressants
2422 R
Transport
780 R
How do I feel after treatment
I stopped taking antidepressants a year and a month after discharge I spent another 14,640 R on them. Sometimes I have obsessive thoughts and compulsive actions, but I do not scold myself for this. I know that if I get upset, the symptoms will become more frequent. The psychiatrist warned me that OCD symptoms may appear periodically, but this is normal.
14,640 Р
spent on antidepressants for a year and one month
Coronavirus last spring was a test of strength for me. The condition worsened, compulsive actions resumed, I stopped leaving the house, I began to choke on the street, obsessive thoughts about death appeared. But I managed it on my own with the help of techniques taught to me by the therapist. I kept in my head the idea that if it worked then, it will work now.
The condition worsened, compulsive actions resumed, I stopped leaving the house, I began to choke on the street, obsessive thoughts about death appeared. But I managed it on my own with the help of techniques taught to me by the therapist. I kept in my head the idea that if it worked then, it will work now.
Before treatment, it was difficult for me to talk about my disorder. And now I openly talk about it and I can even joke about random manifestations of OCD. Almost everyone in my circle knows that I was being treated for OCD and depression. They help me notice compulsive actions and stop in time, treat me with understanding when I ask obvious things just in case - for example, did I close the door.
How often do people with OCD need to take drugs for life
Sergey Divisenko
psychotherapist
With the help of treatment, you can achieve remission - for a long time to get rid of the symptoms of OCD or reduce their number. Remission can occur both against the background of taking medications, and without them, against the background of psychotherapy.
Approximately 80% of patients with OCD stop taking medication sooner or later.
How much does OCD treatment cost?
In total, I treated OCD for one year and nine months. Of these, she was treated in a day hospital for two and a half months, and for a year and seven months - on an outpatient basis.
In the hospital, I only spent money on transport to and from the dispensary. Even during the second hospitalization, on the recommendation of the doctor, she bought antidepressants at the pharmacy and took them instead of those given in the hospital. The rest of the drugs, consultations and meals were free.
6 useful services for finding a psychotherapist
Most of the expenses are medicines during outpatient treatment.
Spent on OCD treatment for 1 year and 9 months — 27,337 R
| Expenditures | Spending |
|---|---|
| Antidepressants | 23 050 Р |
| Normotimics | 2384 P |
| Antipsychotics | 419 P |
| Tranquilizers | 104 Р |
| Transport during hospitalization | 1380 Р |
Save
- Obsessive Compulsive Disorder or OCD is a mental illness in which a person experiences obsessive thoughts and compulsive actions.
- OCD is considered a lifelong disorder, but remission can be achieved with the help of psychotherapy and drugs.
- OCD is treated in Russia by psychiatrists, psychotherapists and psychologists. Psychiatrists prescribe prescription drugs. Psychotherapists and psychologists conduct psychotherapy sessions.
- A visit to a neuropsychiatric dispensary will not prevent people with OCD from moving freely, driving a car, using weapons, or getting a job.
- Patients with OCD can receive care free of charge in state neuropsychiatric dispensaries or at their own expense in private clinics.
Did you also have an illness that affected your lifestyle or attitude? Share your story.
Tell
Obsessive Compulsive Disorder Treatment
Great Thought is an obsessive compulsive disorder treatment program. We will relieve you of obsessive thoughts, movements and rituals. Let's get back to life!
Symptoms of obsessive-compulsive disorder
- Frightening images and drives
- Compulsive acts (rituals)
- Intrusive check of one's own actions
- Fear of trouble, pollution or contamination
- Inexplicable desire to count something
- Excessive organization and pedantry
- Perfectionism in relationships, work and even leisure
- "Stuck", "looping" on one's thoughts
You feel that over time your mood becomes worse: apathy, depression, obsessions increase, and rituals begin to fill all your free time or harm your physical health.
You may have had more than one meeting with psychologists, psychotherapists and psychiatrists. You are not given the "scary" psychiatric diagnoses of Schizophrenia or Bipolar Disorder, but are prescribed medication and psychotherapy nonetheless. However, such treatment cannot be called effective - the symptoms persist and only aggressive pharmacotherapy temporarily reduces anxiety.
What is obsessive-compulsive disorder?
Obsessive-compulsive disorder is a syndrome characterized by the presence of obsessive thoughts (obsessions) to which a person reacts with certain actions (compulsions). The causes of the disorder are rarely superficial. The syndrome is also accompanied by the development of obsessive memories and various pathological phobias. May be chronic, episodic or progressive.
Obsession - obsessive thought, persistent desire for something, uncontrollable and accompanied by anxiety and intense anxiety. In an attempt to cope with such thoughts, a person resorts to committing compulsions.
Compulsion - an irresistible need to perform certain actions (rituals), which can be assessed by the person himself as irrational or meaningless, and the internal need to perform them is forced and is the result of obsessive ideas.
Common examples of OCD manifestations
- An exaggerated sense of danger. Fear of the materiality of thoughts:
- "now I will lose control and hurt my loved ones"
- "something terrible is about to happen, I can feel it"
- "I shouldn't think like that, all this will come true because of me"
- Pathological fear of pollution. Thirst for Purity
- Excessive perfectionism, exaggerated responsibility - "everything must be done perfectly", "everything depends on me, mistakes are unacceptable"
How does this painful algorithm work?
Most people have unwanted or obsessive thoughts quite often, but all sufferers of the disorder greatly exaggerate their importance. Fear of one's own thoughts leads to attempts to neutralize the negative feelings that arise from obsessions, for example by avoiding thought-provoking situations or by engaging in "rituals" of excessive self-cleansing or prayer.
Fear of one's own thoughts leads to attempts to neutralize the negative feelings that arise from obsessions, for example by avoiding thought-provoking situations or by engaging in "rituals" of excessive self-cleansing or prayer.
As we noted earlier, repetitive avoidance behavior can "get stuck", "loop", that is, have a tendency to repeat. The cause of obsessive-compulsive disorder is the interpretation of intrusive thoughts as catastrophic and true.
If you periodically experience over the years:
- Constant or fluctuating anxiety
- The need to perform certain ritualized actions
- A persistent decline in the quality of life due to the need to avoid certain thoughts and actions, places and events
And you are also persecuted:
- Significant problems in studies and career
- Failure to establish a serious relationship
- Constant criticism and pressure from relatives
- Many senseless activities
- Excessive involvement in computer games and the Internet, alcohol
- Loneliness and isolation
We strongly recommend that you do not delay seeking help and that you complete a remedial program.
Consultations and psychotherapeutic sessions according to the program are held several times a week, until the relief of severe symptoms, then the frequency of meetings with specialists is reduced to 2–3 per month. Count on the fact that in the end we will deal with your problem together.
Treatment of obsessive-compulsive disorder in Neuro-Psi
Every day, the specialists of the NEURO-PSI clinic analyze the world practice in the field of psychiatry and psychotherapy. The goal is the impartial selection and implementation of those methods of treatment and psychological assistance, the effectiveness of which has been convincingly proven in independent studies.
We are guided by the principles of evidence-based medicine and use as a basic method of treatment a psychotherapeutic paradigm, the effectiveness of which has been widely recognized by the professional community.
1. What is the essence of the obsessive-compulsive disorder treatment program?
A comprehensive work is carried out with the client, taking into account the main factors that create well-being.
The main emphasis is on teaching the client how to properly respond to his thoughts, emotions, inner feelings and interpretation of external events.
All types of psychotherapeutic and drug treatments serve the same goal: to achieve the best result in the shortest possible time. At the same time, by coordinating the efforts of specialists in various fields, the most complete coverage of all types of mental illnesses, disorders and disorders is possible.
2. What treatments are used
- Priority:
- Cognitive-Behavioral Therapy.
- Schema Therapy.
- Reality Therapy.
- Choice Theory.
- Rational pharmacotherapy.
- Psychopharmacotherapy (if indicated)
- Biofeedback Therapy
- Rational psychocorrection of stress
- Jacobson progressive muscle relaxation.
- Traditional and modern gymnastic systems, relaxation techniques.
- Breathing techniques .

- Stress exposure.
- Self-control training.
- Lifestyle modification
- Work with bad habits.
- Diet correction.
- Professional and social adaptation.
3. How is the treatment under the program
Each treatment program at the NEURO-PSI clinic consists of four stages:
- diagnostics,
- work with disease symptoms,
- work with the causes of the disease,
- consolidation of the achieved results.
Work efficiency is increased by dividing the treatment process into a predetermined number of sessions, at convenient times and without hospitalization. This means that each program is adapted to the problem that the client has addressed.
The program method of treatment is predictable, time-limited, productive, and, most importantly, understandable for the client.
Of course, the treatment takes place in a comfortable mode without interruption from work, study or family. Specialists of various profiles will work with you (team method). This is necessary to minimize the risk of diagnostic errors that could lead to the adoption of a suboptimal treatment plan.
Specialists of various profiles will work with you (team method). This is necessary to minimize the risk of diagnostic errors that could lead to the adoption of a suboptimal treatment plan.
Improvements in well-being and mood (healing) occur in stages: after the decrease in emotional problems, bodily symptoms decrease. Working with the causes (etiology) of obsessive-compulsive disorder helps to avoid relapses in the future.
4. What are the results and prognosis?
Upon completion of the program, you get rid of obsessive thoughts and rituals, fear of pollution, unmotivated fears, panic attacks and multiple vegetative symptoms (sudden jumps in blood pressure, heart palpitations, dizziness, nausea).
According to statistics, the effectiveness of the methods used approaches 100% if all recommendations of specialists are followed.
Skills you acquire during the program:
- self-control and self-regulation
- constructive analysis of the state of the body
- understanding one's own mental and emotional sphere
- ability to control one's attention
- ability to act consciously in stressful situations
Significantly improves the emotional and physical condition, gaining self-confidence, in the future.