Causes of stupor
Stupor: Symptoms, Causes, and Diagnosis
Stupor: Symptoms, Causes, and DiagnosisMedically reviewed by George Krucik, MD, MBA — By Rachel Nall, MSN, CRNA — Updated on November 1, 2019
What Does Stupor Mean?
Stupor can be a serious mental state where people don’t respond to normal conversation. Instead, they respond only to physical stimulation, such as to pain or rubbing on their chest, which is known as a sternal rub.
Another word for stupor is “obtunded.” Stupor can be considered a very serious symptom because it’s associated with disorders like drug overdose, stroke, lack of oxygen, meningitis, or brain swelling. It’s important to seek immediate medical attention when someone shows signs of stupor.
Someone experiencing stupor can be aroused or woken up with vigorous stimulation. They may be considered unconscious, but may respond somewhat to stimuli. This is different from someone in a coma because people in a coma can’t be woken up or aroused at all.
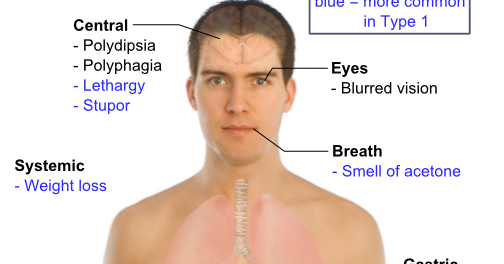
Stupor can cause the following physical symptoms in addition to mental symptoms:
- abnormal breathing, such as breathing too slow or fast
- muscles contracted in abnormal ways
- pupils that are wider or smaller than normal
- pupils that don’t react or change with exposure to light
There can be other, disease-specific symptoms associated with stupor as well.
There are many causes of stupor, most of which are severe diseases. Examples of possible causes of stupor include:
- alcohol intoxication
- brain aneurysm
- brain tumor
- carbon monoxide poisoning
- cardiac arrest
- delirium
- dementia
- drug overdose
- encephalitis (brain infection)
- head injury
- hyperglycemia
- hypernatremia
- hyperthermia
- hyperthyroidism
- hypoglycemia
- hyponatremia
- hypothermia
- hypothyroidism
- hypoxia or lack of oxygen
- kidney failure
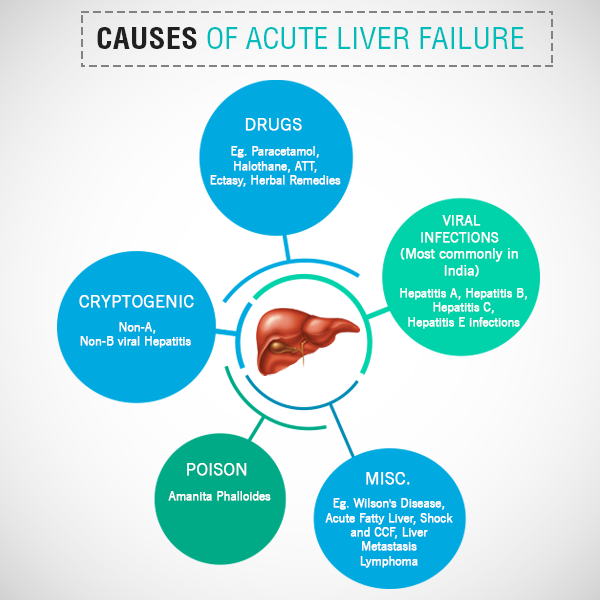
- liver failure
- meningitis
- respiratory arrest
- seizure
- sepsis, a serious bloodstream infection
- stroke
Stupor is always considered a medical emergency. Call 911 immediately if a person around you is experiencing stupor. It’s vital to get fast care in order to diagnosis the cause of stupor.
Call 911 immediately if a person around you is experiencing stupor. It’s vital to get fast care in order to diagnosis the cause of stupor.
Someone with stupor is unable to provide a medical history. If a loved one or eyewitness is available, a doctor may ask about their symptoms or any relevant medical history, if available.
The next step is to do a physical examination of the person. This includes taking vital signs, such as:
- heart rate
- respirations
- blood pressure
- temperature
- oxygen saturation
Each of these can provide important information if the problem is related to the lungs or heart.
The doctor will evaluate how the person is breathing and any visible injuries that could be causing stupor. This includes head injuries as well as signs of bleeding on the body. The person’s posture or body positioning could also indicate stroke.
A neurological or brain examination is next. This can include testing the person’s reflexes, include pupil reflexes and light movements. The doctor may provide stimuli, including noise, pressure on the fingernails, or a sternal rub, to test their response.
The doctor may provide stimuli, including noise, pressure on the fingernails, or a sternal rub, to test their response.
The doctor might also do blood testing. This can help determine:
- blood sugar levels
- blood counts
- blood clotting
- electrolyte levels
The doctor may order an arterial blood gas (ABG) test. This test determines the pH of a person’s blood, which can indicate if too much acid or base is present and causing symptoms.
Imaging tests, especially those to view the brain, are also often conducted. An example is a computed tomography (CT) scan that doctors can use to pinpoint bleeding signs.
How someone is treated for stupor depends on the underlying cause or causes. Because the causes can range from infection to heart-related to lung-related to all of the above, stupor requires careful and fast treatment to keep the condition from worsening.
Last medically reviewed on May 15, 2015
How we reviewed this article:
Healthline has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical associations. We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
- Depression of consciousness. (2008)
dartmouth.edu/~dons/part_2/chapter_17.html - Rajagopal, S. (2007). Catatonia. Advances in Psychiatric Treatment, 13, 51-59
apt.rcpsych.org/content/aptrcpsych/13/1/51.full.pdf - Stupor and coma. (2014, August)
merckmanuals.com/home/brain_spinal_cord_and_nerve_disorders/coma_and_impaired_consciousness/stupor_and_coma.html - Young, G. (2011). Stupor and coma in adults
ncbi.nlm.nih.gov/books/NBK380/
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
Share this article
Medically reviewed by George Krucik, MD, MBA — By Rachel Nall, MSN, CRNA — Updated on November 1, 2019
Read this next
Autonomic Dysfunction
Medically reviewed by Judith Marcin, M.
 D.
D.Autonomic dysfunction occurs when the autonomic nervous system is damaged. This is the system of nerves that controls functions that help you survive.
READ MORE
Bruce Willis’ Family Say He’s Living With Aphasia. Here’s What That Means.
The family of Bruce Willis shared that the actor is retiring following a diagnosis of aphasia. There are several types of aphasia, and each may affect…
READ MORE
Understanding Oppositional Defiant Disorder
A pattern of anger and defiance against authority could be a sign of oppositional defiant disorder (ODD). Learn more about symptoms and treatment for…
READ MORE
Understanding Bradyphrenia
Medically reviewed by Timothy J. Legg, PhD, PsyD
Bradyphrenia is a medical term for slowed thinking and processing of information.
 It sometimes affects people with neurological conditions, including…
It sometimes affects people with neurological conditions, including…READ MORE
What Is Miosis?
Medically reviewed by Ann Marie Griff, O.D.
Miosis means excessive dilation (shrinking) of your pupil. It's not a disease in and of itself, but rather a symptom of some other cause or underlying…
READ MORE
How a Simple ‘Thank You’ from Your Partner Can Reduce Holiday Stress
New research suggests that people who feel appreciated by their partners are more resilient during stressful times and are less likely to engage in…
READ MORE
Grace Gaustad on Mental Health, Trauma, and Finding Purpose
From early anxiety to founding a nonprofit, Grace Gaustad is on a mission.
READ MORE
Why Rooting for Your Favorite Team May be Boosting Your Mental Health Too
New research suggests that fans experience lower rates of depression and loneliness than non-fans.
 Here's why.
Here's why. READ MORE
Therapy for Every Budget: How to Access It
Medically reviewed by Karin Gepp, PsyD
Finding a therapist is a huge step in caring for your mental health. To help get you started, here’s a list of affordable mental health care options.
READ MORE
The Top 8 Online Psychiatry Services in 2022
If you’re considering meeting with a psychiatrist but prefer remote visits, online psychiatry may be right for you. Here are our top picks for online…
READ MORE
Structural Causes of Stupor and Coma | Plum and Posner's Diagnosis of Stupor and Coma
Navbar Search Filter Oxford AcademicPlum and Posner's Diagnosis of Stupor and Coma (4 edn)Contemporary Neurology SeriesNeurologyBooksJournals Mobile Microsite Search Term
Close
Navbar Search Filter Oxford AcademicPlum and Posner's Diagnosis of Stupor and Coma (4 edn)Contemporary Neurology SeriesNeurologyBooksJournals Microsite Search Term
Advanced Search
-
Cite Icon Cite
-
Permissions
-
Share
- More
Cite
Posner, Jerome B. and others,
and others,
'Structural Causes of Stupor and Coma'
,
Plum and Posner's Diagnosis of Stupor and Coma
, 4 edn
, Contemporary Neurology Series
(
2008;
online edn,
Oxford Academic
, 1 Apr. 2013
), https://doi.org/10.1093/med/9780195321319.003.0145,
accessed 4 Dec. 2022.
Select Format Select format.ris (Mendeley, Papers, Zotero).enw (EndNote).bibtex (BibTex).txt (Medlars, RefWorks)
Close
Navbar Search Filter Oxford AcademicPlum and Posner's Diagnosis of Stupor and Coma (4 edn)Contemporary Neurology SeriesNeurologyBooksJournals Mobile Microsite Search Term
Close
Navbar Search Filter Oxford AcademicPlum and Posner's Diagnosis of Stupor and Coma (4 edn)Contemporary Neurology SeriesNeurologyBooksJournals Microsite Search Term
Advanced Search
Abstract
Two major classes of structural brain injuries cause coma (Table 3–1): (1) Compressivelesions may impair consciousness either by directly compressing the ascending arousal system or by distorting brain tissue so that it moves out of position and secondarily compresses components of the ascending arousal system or its forebrain targets (see herniation syndromes, page 95). These processes include a wide range of space-occupying lesions such as tumor, hematoma, and abscess. (2) Destructive lesions cause coma by direct damage to the ascending arousal system or its forebrain targets. To cause coma, lesions of the diencephalon or brainstem must be bilateral, but can be quite focal if they damage the ascending activating system near the midline in the midbrain or caudal diencephalon; cortical or subcortical damage must be both bilateral and diffuse. Processes that may cause these changes include tumor, hemorrhage, infarct, trauma, or infection. Both destructive and compressive lesions may cause additional compression by producing brain edema.
These processes include a wide range of space-occupying lesions such as tumor, hematoma, and abscess. (2) Destructive lesions cause coma by direct damage to the ascending arousal system or its forebrain targets. To cause coma, lesions of the diencephalon or brainstem must be bilateral, but can be quite focal if they damage the ascending activating system near the midline in the midbrain or caudal diencephalon; cortical or subcortical damage must be both bilateral and diffuse. Processes that may cause these changes include tumor, hemorrhage, infarct, trauma, or infection. Both destructive and compressive lesions may cause additional compression by producing brain edema.
Subject
Neurology
Series
Contemporary Neurology Series
Disclaimer
Oxford University Press makes no representation, express or implied, that the drug dosages in this book are correct. Readers must therefore always …
More
Oxford University Press makes no representation, express or implied, that the drug dosages in this book are correct.
Readers must therefore always check the product information and clinical procedures with the most up to date published product information and data sheets
provided by the manufacturers and the most recent codes of conduct and safety regulations. The authors and the publishers do not accept responsibility or
legal liability for any errors in the text or for the misuse or misapplication of material in this work. Except where otherwise stated, drug dosages
and recommendations are for the non-pregnant adult who is not breastfeeding.
Readers must therefore always …
More
Oxford University Press makes no representation, express or implied, that the drug dosages in this book are correct.
Readers must therefore always check the product information and clinical procedures with the most up to date published product information and data sheets
provided by the manufacturers and the most recent codes of conduct and safety regulations. The authors and the publishers do not accept responsibility or
legal liability for any errors in the text or for the misuse or misapplication of material in this work. Except where otherwise stated, drug dosages
and recommendations are for the non-pregnant adult who is not breastfeeding.
You do not currently have access to this chapter.
Sign in
Get help with access
Get help with access
Institutional access
Access to content on Oxford Academic is often provided through institutional subscriptions and purchases. If you are a member of an institution with an active account, you may be able to access content in one of the following ways:
If you are a member of an institution with an active account, you may be able to access content in one of the following ways:
IP based access
Typically, access is provided across an institutional network to a range of IP addresses. This authentication occurs automatically, and it is not possible to sign out of an IP authenticated account.
Sign in through your institution
Choose this option to get remote access when outside your institution. Shibboleth / Open Athens technology is used to provide single sign-on between your institution’s website and Oxford Academic.
- Click Sign in through your institution.
- Select your institution from the list provided, which will take you to your institution's website to sign in.
- When on the institution site, please use the credentials provided by your institution. Do not use an Oxford Academic personal account.

- Following successful sign in, you will be returned to Oxford Academic.
If your institution is not listed or you cannot sign in to your institution’s website, please contact your librarian or administrator.
Sign in with a library card
Enter your library card number to sign in. If you cannot sign in, please contact your librarian.
Society Members
Society member access to a journal is achieved in one of the following ways:
Sign in through society site
Many societies offer single sign-on between the society website and Oxford Academic. If you see ‘Sign in through society site’ in the sign in pane within a journal:
- Click Sign in through society site.
- When on the society site, please use the credentials provided by that society. Do not use an Oxford Academic personal account.
- Following successful sign in, you will be returned to Oxford Academic.
If you do not have a society account or have forgotten your username or password, please contact your society.
Sign in using a personal account
Some societies use Oxford Academic personal accounts to provide access to their members. See below.
Personal account
A personal account can be used to get email alerts, save searches, purchase content, and activate subscriptions.
Some societies use Oxford Academic personal accounts to provide access to their members.
Viewing your signed in accounts
Click the account icon in the top right to:
- View your signed in personal account and access account management features.
- View the institutional accounts that are providing access.

Signed in but can't access content
Oxford Academic is home to a wide variety of products. The institutional subscription may not cover the content that you are trying to access. If you believe you should have access to that content, please contact your librarian.
Institutional account management
For librarians and administrators, your personal account also provides access to institutional account management. Here you will find options to view and activate subscriptions, manage institutional settings and access options, access usage statistics, and more.
Purchase
Our books are available by subscription or purchase to libraries and institutions.
Purchasing information
causes, symptoms, diagnosis, treatment, prevention
This is one of the severe types of movement disorders, which is caused by complete immobility, accompanied by mutism and a decrease in reactions to external stimuli, including pain.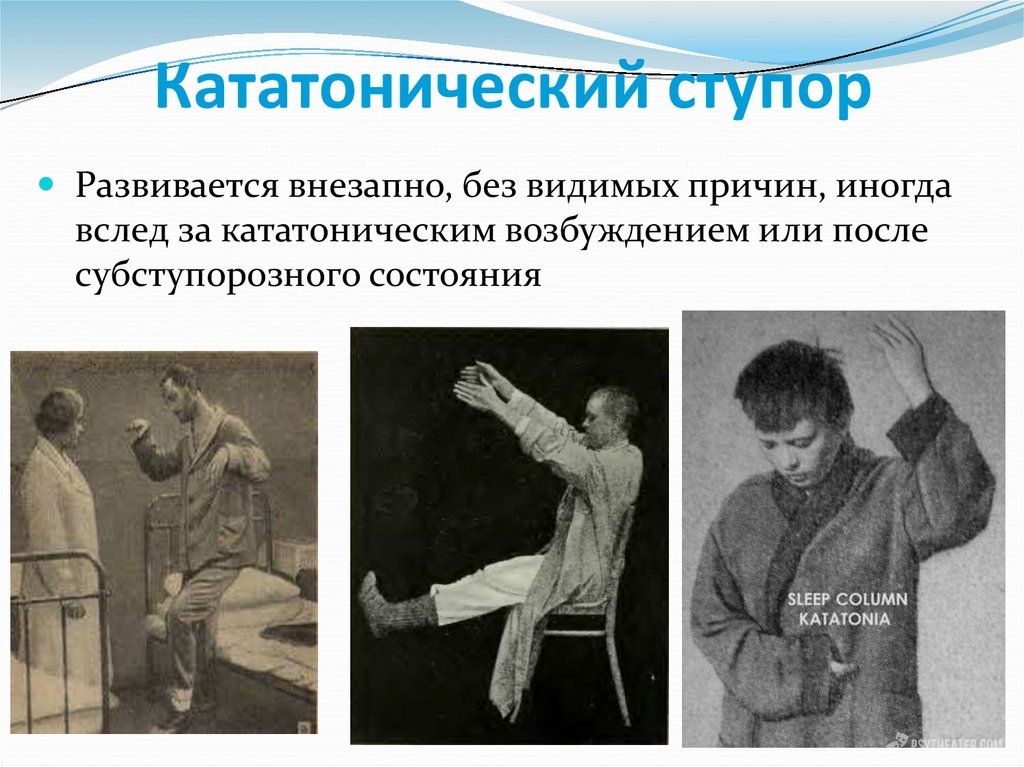
Causes
Among both sexes, the development of emotional stupor is much more common in women. The occurrence of this state occurs against the background of strong psycho-emotional shocks, accompanied by a blockage of motor and mental activity, affective activity. Sometimes this disorder may disappear on its own. Sometimes stupor is accompanied by depression. Women who have witnessed an accident, catastrophe or someone else's suffering are subject to this type of violation. The occurrence of stupor sometimes occurs in soldiers on the battlefield or in children during examinations.
Symptoms
In severe cases, a person experiences total immobility, accompanied by the absence of any reaction to any external stimuli, even pain. Muscle tone in such patients is increased or, conversely, reduced. In some types of stupor, waxy flexibility may develop.
Depending on the causes that caused the violation, there may be a different combination of symptoms, decrease and distortion of motor and volitional functions.
Stupor is sometimes a symptom of reactive psychoses, schizophrenia and organic lesions of the central nervous system.
There are several types of stupor:
Wax-flexible stupor is due to the patient's mutism, immobility, and the ability to maintain a certain posture for a long time. Patients do not want to communicate, but at night they can eat, answer questions or take care of themselves.
Negativistic stupor is manifested by the fact that a person refuses to eat, talk, and attempts to change the position of his body cause sharp resistance.
Stupor with muscle torpor is manifested by the patient assuming the fetal position, the muscles in such patients are tense, the lips are slightly extended, and the eyes are closed. Such patients may refuse to eat, in connection with this they receive food through a tube.
Depressive stupor is due to complete immobility, such patients have a pained expression on their faces, if you manage to make contact with them, they give monosyllabic answers.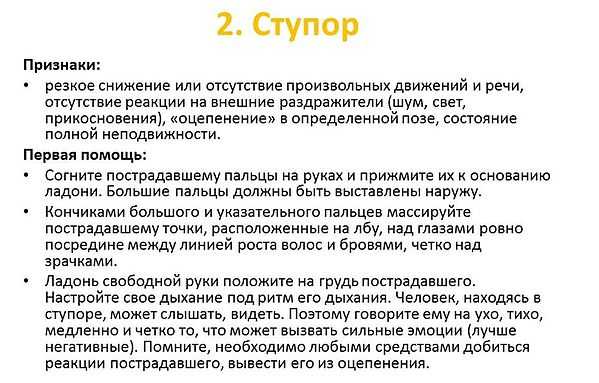 Sometimes this type of stupor is replaced by a sharp excitement or a melancholic raptus, in which the patients are apt to inflict severe injuries on themselves.
Sometimes this type of stupor is replaced by a sharp excitement or a melancholic raptus, in which the patients are apt to inflict severe injuries on themselves.
Apathetic stupor is expressed by the fact that patients lie on their backs, they are detached from the outside world, they answer all questions in monosyllables with some delay. This type of stupor occurs with psychosis or with Wernicke's disease.
Catatonic stupor is associated with freezing in fear or numbness with fear, freezing in fear. Such patients refuse to talk and eat and tend to freeze in one position for a long time.
Diagnostics
When diagnosing stupor, the presence or absence of a state of immobility in a patient, a decrease or lack of response to external stimuli is taken into account. Also, when making a diagnosis, it is necessary to take into account whether the patient has recently suffered a stressful event.
Treatment
Barbamyl-caffeine disinhibition is used in a hospital, thanks to which it is possible to find out the characteristics of a person's experiences and determine the type of stupor.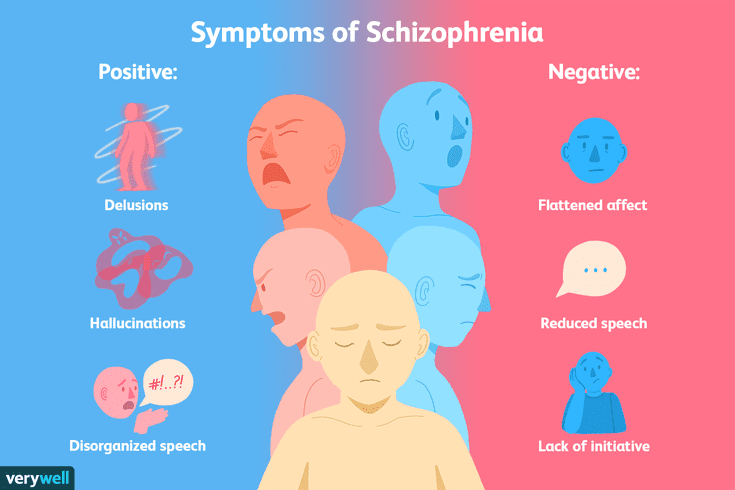 At the initial stage, patients are given 1 or 2 ml of a 20% caffeine solution, and after 3 or 5 minutes, by intravenous injection of 5 to 10 ml of a 5 or 10% solution of barbamyl, with constant monitoring of the patient's condition.
At the initial stage, patients are given 1 or 2 ml of a 20% caffeine solution, and after 3 or 5 minutes, by intravenous injection of 5 to 10 ml of a 5 or 10% solution of barbamyl, with constant monitoring of the patient's condition.
Also, to eliminate stupor, patients are shown the introduction of frenolon, the intake of mazheptil or drugs of the barbamilcaffeine series.
Prevention
Prescribing the correct treatment when the first signs of a disorder occur.
causes, symptoms, types, treatment, how to get out of stupor
Stupor in a person is a stupor in literal translation. In psychiatry, stupor is a type of movement disorder. The stuporous state is a total immobility combined with mutism (muteness or an absolute refusal to communicate) and weakened responses to all kinds of stimulus stimuli. An individual suffering from a psychological stupor does not react to ongoing events, and there are also no reactions to common negative messages, such as pain, noise or cold. Such a patient may not eat for a relatively long period, not talk, and often even freeze in one position.
Such a patient may not eat for a relatively long period, not talk, and often even freeze in one position.
A stupor can be the end result of depression, various mental disorders, severe stress or fear. Often, some stuporous patients lie without changing position, refusing to eat, not responding to questions, for days or even weeks. Other patients sit or stand, often as if petrified in a strange position, wrapped in a blanket with their heads or turned to the wall, absolutely motionless until they are forcibly transferred to a different position.
Causes of stupor
Stupor is a psychopathological disorder, which manifests itself in the form of suppression of various mental operations, primarily motor skills, mental activity and speech. Patients who find themselves in this state are characterized by immobility. Left to themselves, sick individuals stay in one position for a long time. They may not respond at all to addressed interrogative phrases, or they answer, but after a pause, at a slow pace, with interjections, in separate words, or only occasionally in short phrases.
In some cases, the disease may occur in combination with a variety of psychopathological symptoms, such as delirium, hallucinosis, clouding of consciousness, altered affect. In other situations, more rare, the stuporous state is limited exclusively to motor immobility and speech retardation. In other words, this state is also called "empty" stupor.
Stupor accompanied by clouding of consciousness is called receptor stupor. The stuporous state observed in conditions of clear consciousness is called lucid or effector.
The main factors provoking the occurrence of a stuporous state include severe psycho-traumatic events, stressful situations, mental disorders, emotional negatively colored situations, organically determined damage to brain structures, various bruises or concussions, intoxication, and an infectious disease. However, to this day, with one hundred percent probability, it cannot be argued that the listed list of reasons is complete.
World-famous specialists in the field of psychiatry enter into discussions about the possible causes that provoke the development of the disease. So, among the numerous assumptions, there are several most characteristic for the formation and formation of a fixed type of catatonic stupor. Deficiency in the brain of gamma-aminobutyric acid, which is its key inhibitory neurotransmitter. The lack of this acid can become a cause that causes disorders of the musculoskeletal system. And this is the main symptom of catatonia.
So, among the numerous assumptions, there are several most characteristic for the formation and formation of a fixed type of catatonic stupor. Deficiency in the brain of gamma-aminobutyric acid, which is its key inhibitory neurotransmitter. The lack of this acid can become a cause that causes disorders of the musculoskeletal system. And this is the main symptom of catatonia.
Catatonic stupor can occur due to an unexpected stop in the production of dopamine by the body.
In 2004, specialists began to consider the formation of catatonic syndrome as a genetic reaction that occurs in situations of stress or under life-threatening circumstances in animals before an encounter with a predator. The whole body is paralyzed due to fear, as a result of which the animal's body is reconfigured for a quick death. Such a reaction of fear on a subconscious level has been preserved in humans and to this day is manifested during exacerbations of psychosomatic diseases or intense attacks of schizophrenia.
Catatonic stupor, according to this assumption, is expressed in the characteristic reaction of individuals to the inevitable death that haunts him from the onset of the disease. Thus, the above hypotheses cause the onset of a catatonic syndrome as a consequence of the presence of schizophrenia and other psychosomatic diseases.
Symptoms of stupor
While in stupor, people are not in contact with the environment, they have no reactions to ongoing events or uncomfortable conditions, various inconveniences (eg noise, dirty bed).
Patients in stupor may not move even in case of fire, earthquake or other natural disasters. They often lie without changing position, the muscles are in good shape. Usually, tension begins with the masticatory muscles, then descends to the cervical region, and later is distributed over the back, arms and legs. In this state, there is no emotional and pupillary response to pain.
Symptoms of stupor include: clouding of consciousness, absolute immobility, partial or complete silence (mutism), increased muscle tone, negativism, depression of reflex reactions, lack of verbal communication with others and response to external stimuli.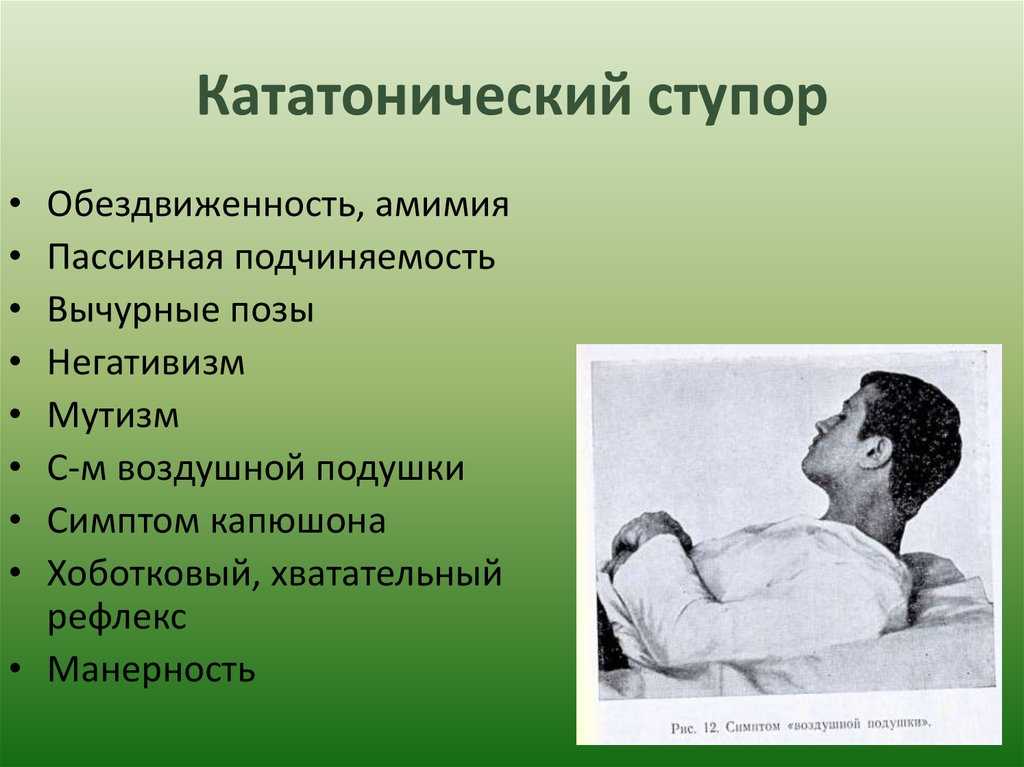
Falling into an emotional stupor is more characteristic of the female part of the population. Emotional stupor often occurs as a result of intense mental shocks (for example, experienced horror or grief). It is characterized by a blockage of motor activity and emotional-affective activity, in addition, the mental function also slows down. Such an attack, in most cases, passes without specific treatment, but sometimes it can lead to a state of panic, during which the patient will tend to perform chaotic actions. This can result in depression.
This type of stupor can be observed in women who have witnessed some catastrophe or accident. There may also be stupor in children due to passing exams or during the battle of the soldiers.
Depressive stupor is equally characteristic of the female part of the population and the strong half of humanity. It occurs against the background of deep depression and, as a rule, is accompanied by a hunched posture, a grimace of suffering on the face of the subjects, and a lowered gaze.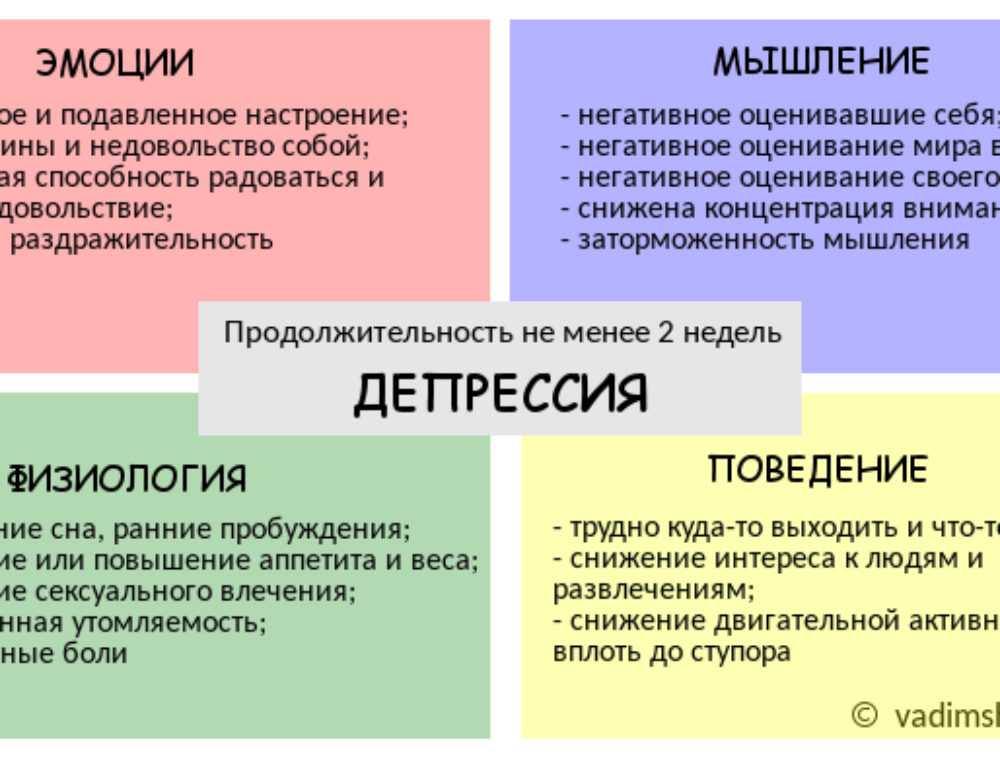 Patients in this condition may respond to interrogative statements with monosyllabic phrases in a whisper. This variation of the stuporous state can be observed for a couple of hours, and sometimes for weeks. People in this condition may refuse food.
Patients in this condition may respond to interrogative statements with monosyllabic phrases in a whisper. This variation of the stuporous state can be observed for a couple of hours, and sometimes for weeks. People in this condition may refuse food.
Overly receptive, emotional, vulnerable people and creative individuals, characterized by a fine internal organization, are characterized by a mental stupor. It is expressed in the form of apathy, laziness, melancholy, creative crisis, inability to think, feel and inability to act differently. In such a state, a kind of spiritual “ossification” sets in.
Hysterical stupor is more often observed in overly emotional ladies. It usually manifests itself as affective inconstancy, the cause of which may be a changed environment. This type of stuporous condition in difficult conditions that threaten the health, life or well-being of a woman can be a defensive reaction. It can manifest itself either in absolute immobility, or in active emotionality and psychomotor agitation.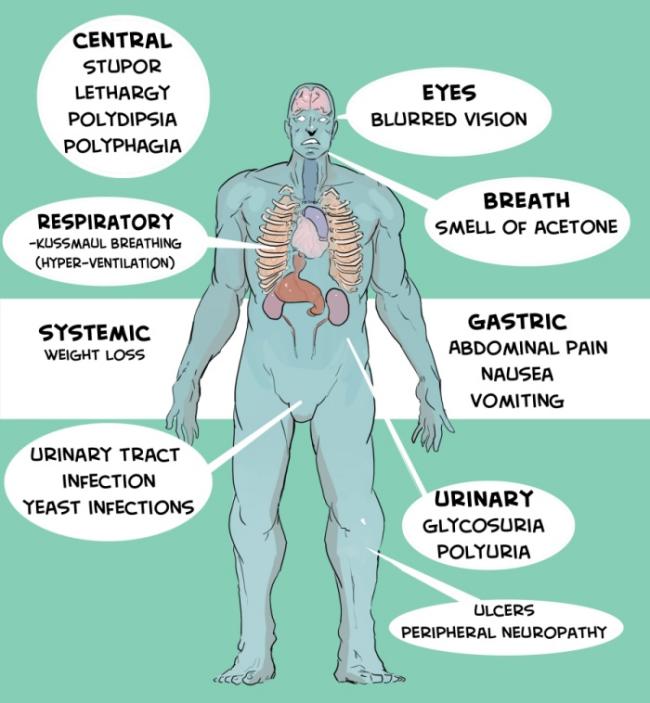 Patients suffering from this type of stupor are characterized by increased facial expressions. So, for example, patients can senselessly goggle their eyes, grimace, cry.
Patients suffering from this type of stupor are characterized by increased facial expressions. So, for example, patients can senselessly goggle their eyes, grimace, cry.
Apathetic stupor manifests itself in passivity and immobility, absence of aspirations and interests.
Types of stupor
There are several types of stupor: negativistic, depressive, apathetic and catatonic, as well as a stuporous state with waxy flexibility or with muscle numbness.
Negativistic stupor is expressed in mutism and absolute immobility, but at the same time, any action aimed at changing the patient's posture provokes a sharp opposition and resistance. A sick individual is not easy to get out of bed, but then, having lifted him, it is impossible to put him down again. Often, active opposition is added to passive opposition. For example, if a doctor extends his hand to the patient, then he, in turn, hides behind his back, when asked to open his eyes, closes their eyes, etc.
Depressive stuporous state is characterized by almost complete immobility along with a depressive facial expression and a pained grimace. When you manage to establish contact with them, you can get a monosyllabic response statement.
When you manage to establish contact with them, you can get a monosyllabic response statement.
A person's depressive stupor may suddenly give way to an agitated state in which the patient jumps up and hurts himself, may injure himself or roll on the floor howling (melancholic raptus). In severe depression of an endogenous nature, a depressive stupor may occur.
Patients suffering from apathetic stupor usually lie on their backs. They also do not react to what is happening around them, and their muscle tone is reduced. Answer questions in monosyllables and with a long delay. However, during interaction with relatives, an adequate emotional reaction is observed. Sleep disturbances and appetite disturbance are noted. Often the bed is untidy. Catatonic stupor is a kind of freezing in fright, numbness in fear and helplessness along with the most severe suffering of the inner "I". Patients with catatonia, sometimes, do not understand whether they are still alive, whether they are able to perform actions, they are not sure of the integrity of their own personality.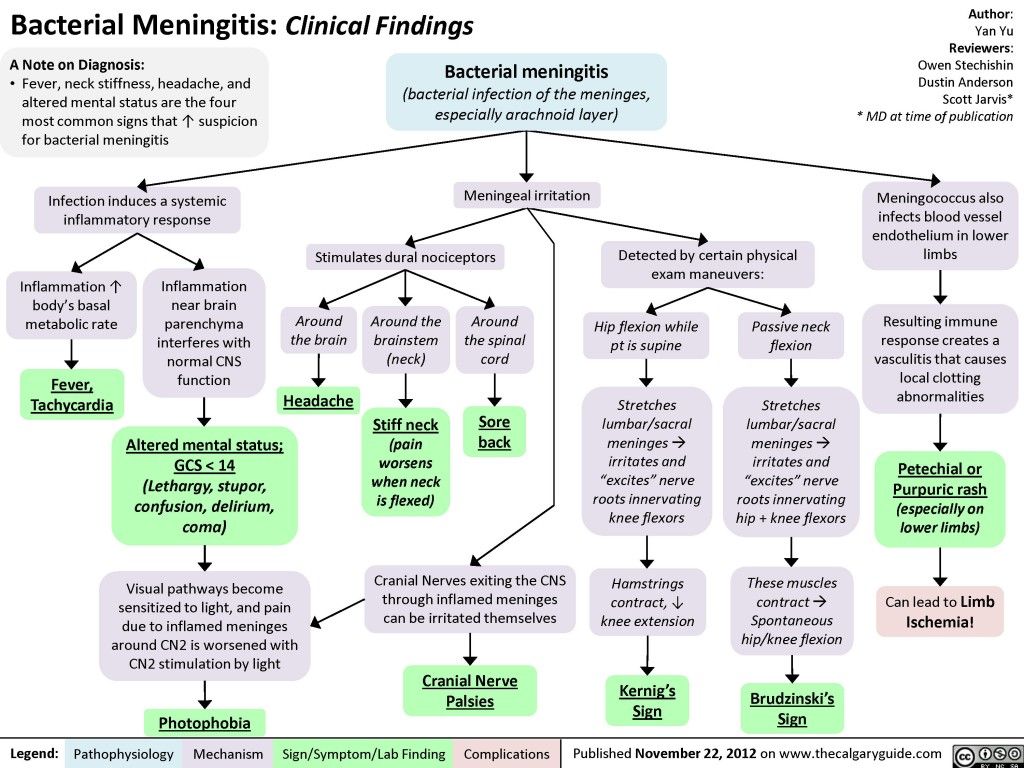 Therefore, everything that can lead to the reconstruction of the authenticity of the I-experience will play a therapeutic role for the patient.
Therefore, everything that can lead to the reconstruction of the authenticity of the I-experience will play a therapeutic role for the patient.
For example, in case of loss of self-identity, sometimes it is enough just to call by name to improve the patient's condition. How to get out of a stupor? In the severe course of the disease, a purely verbal therapeutic approach is often insufficient. Other types of catatonic stupor appear when loaded with delusional experiences, for example, when the individual is in a state of ecstasy.
In a stuporous state with waxy flexibility, in addition to mutism and immobility, the patient holds the dowry for a long time. For example, freezes with a raised hand or freezes in an uncomfortable position. Often, the presence of Pavlov's symptom is noted, which consists in the absence of a reaction in patients to interrogative phrases set in a normal voice, but at the same time responds to a whisper. At night, sick individuals can walk, sometimes eat and contact the environment.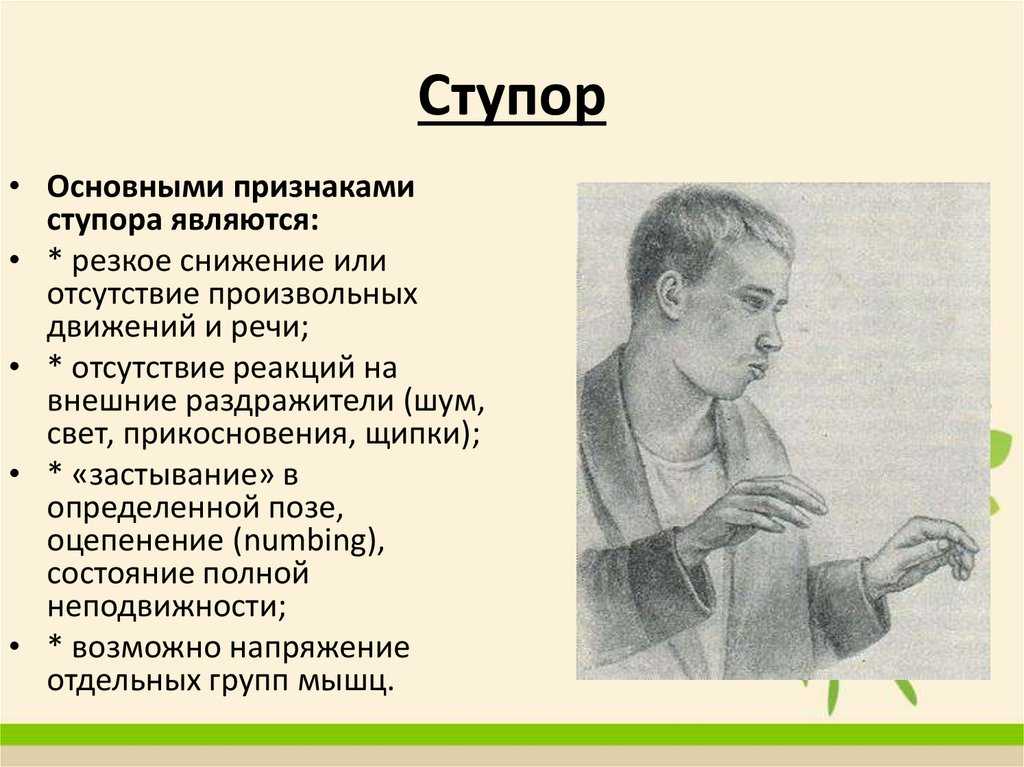
Stupor state with muscular torpor is being in the fetal position. In such patients, the muscles are tense, the eyes are closed, the lips are stretched forward. Often, individuals suffering from this type of stupor have to be fed through a probe, as they refuse food. It is not uncommon for physicians to perform amytal-caffeine disinhibition, and after the muscle numbness subsides or disappears, they feed the patients.
Treatment of stupor
Many people are concerned about the question: "how to get out of stupor"? Naturally, only specialists - psychotherapists and psychologists - can help in this. However, one should still know how to help a loved one or someone in the environment if there are signs that the subject intends to fall into a stupor or has already entered such a state and needs help.
So, first of all, massage of special points, located exactly in the middle above the pupils, equidistant from the brow ridges and the hairline, will help relieve tension. These points should be massaged with the pads of the index finger and thumb. In addition, it is recommended to try to provoke strong emotions in an individual who is in a stuporous state, whether positive or negative (preferably negative). For example, you can give a slap in the face.
These points should be massaged with the pads of the index finger and thumb. In addition, it is recommended to try to provoke strong emotions in an individual who is in a stuporous state, whether positive or negative (preferably negative). For example, you can give a slap in the face.
Flexing the fingers of the hands and pressing them firmly against the palms, while the thumbs remain straight, can help to get out of the stupor. So, the answer to the question: "how to get out of a stupor" is hidden in the emotional shake-up of the body and the synchronization of the breathing of the sufferer with the subject helping him. To this end, you can put your hand on the chest of an individual who has fallen into a stupor and adjust to his respiratory rate.
In stupor, emergency care is limited to ensuring the safety of subjects and preventing dangerous actions on their part. For example, in a catatonic stuporous state, emergency care will be a willingness to stop unexpected impulsive agitation.
In depressive stupor - prevention of the likelihood of sudden development of depressive arousal with a focus on suicide, as well as the elimination of food refusal. In addition, it must be borne in mind that stupor can suddenly be replaced by excitement.
Treatment often takes place in a hospital setting. Use barbamil-caffeine disinhibition. Thanks to which it is possible to detect the features of the patient's experiences and anxieties, which helps to determine the nature of the stuporous state. This disinhibition is also a therapeutic method that helps with persistent refusal of food.
A stuporous condition that occurs against the background of severe somatic ailments requires treatment of the underlying disease.
In stupor accompanied by hallucinations and delusions Stelazin, Trisedal is used as well as in the treatment of hallucinatory and delusional states. In a depressive stuporous state, disinhibition is also carried out and Melipramin is used up to 300 mg per day orally or intramuscularly.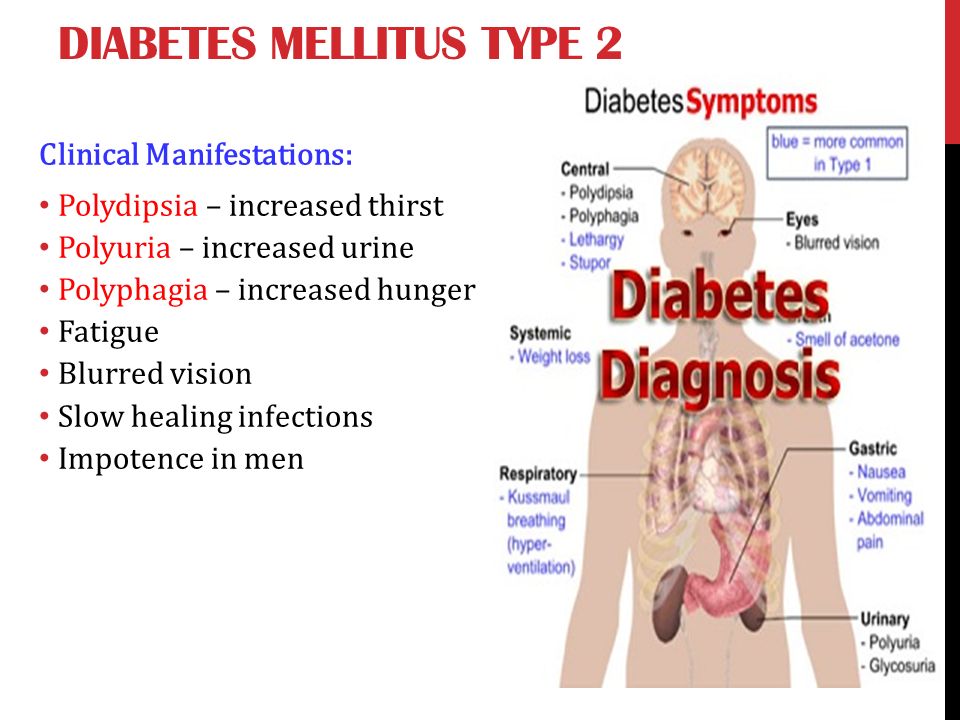 In a psychogenic stuporous state - Diazepam up to 30 mg per day orally or intramuscularly, Elennium or Phenazepam.
In a psychogenic stuporous state - Diazepam up to 30 mg per day orally or intramuscularly, Elennium or Phenazepam.
Catatonic stupor
A psychopathological syndrome, the main manifestation of which is movement disorders, is called catatonic stupor.
Catatonic stupor was first described by Kahlbaum as an independent mental illness, later classified by Kraepelin as schizophrenia. Catatonic stupor is a form of schizophrenia characterized by psychomotor disorders. Such a stuporous state can last for several months, and in a more serious course - several years. It manifests itself in the preservation by the subject of an uncomfortable, unnatural posture for a rather long period and mutism. At the same time, being in a similar position, a person does not feel tired. A stuporous state may be accompanied by increased plastic tone or extreme tension of the entire musculature.
Catatonic stupor is a form of schizophrenia characterized by a condition in which individuals refuse food, defecate on their own.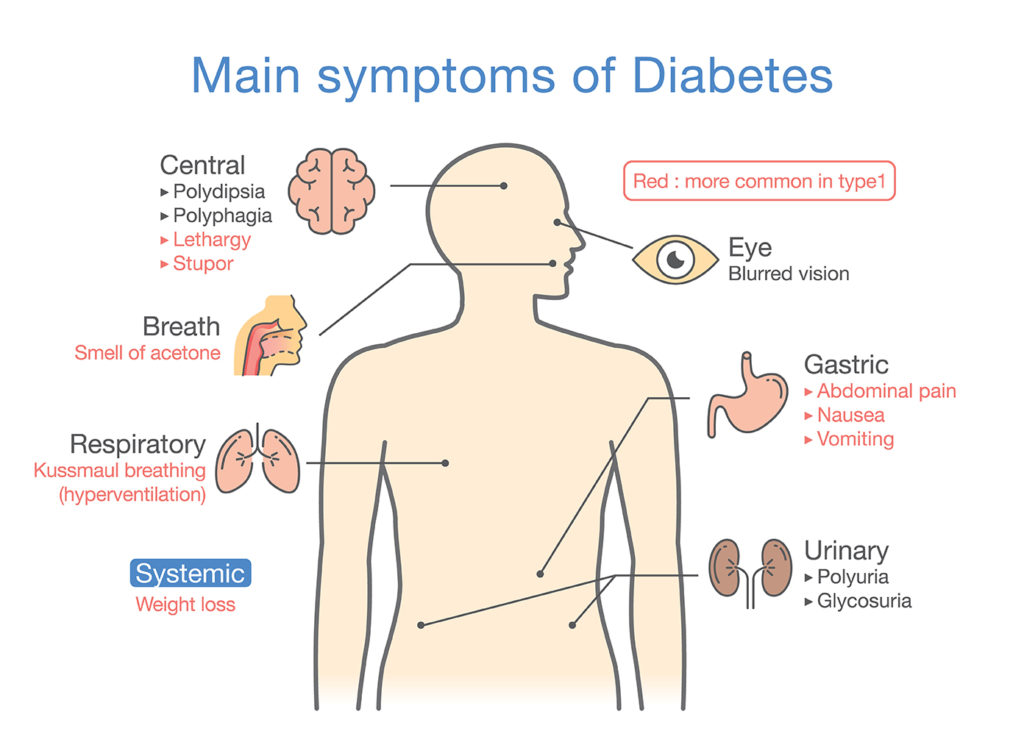 However, at the same time, their consciousness is preserved, as a result of which the patients, having come to their senses, can describe in detail the incidents that occurred during the stupor around them.
However, at the same time, their consciousness is preserved, as a result of which the patients, having come to their senses, can describe in detail the incidents that occurred during the stupor around them.
At the beginning of the twentieth century, the catatonic syndrome was considered mainly as a subspecies of schizophrenia. Today, catatonia is understood as a syndrome that develops with affective and other mental disorders, somatic ailments, and poisoning. The catatonic syndrome is an alternation of stupor with periods of catatonic excitation.
Catatonic stupor is expressed in motor inhibition, mutism, muscle hypertonicity. In a clamped state, patients can sometimes stay even for several months. In such a state, all forms of activity, including instinctive ones, are violated. The following types of catatonic stupor are distinguished: with waxy flexibility, negativistic and with stupor.
Catatonic stupor often develops as a manifestation of the catatonic syndrome. Being in a stuporous state, patients do not come into contact with the environment, they do not react to ongoing phenomena or various inconveniences (for example, a wet bed). They completely refuse to eat, they do not have pupil dilation as a response to pain.
Being in a stuporous state, patients do not come into contact with the environment, they do not react to ongoing phenomena or various inconveniences (for example, a wet bed). They completely refuse to eat, they do not have pupil dilation as a response to pain.
Patients suffering from catatonic stupor initially become silent, may repeat phrases uttered by another individual (echolalia) or not answer questions at all, but still perform the necessary daily (domestic) activities. Then they stop moving, freeze in a strange position, for example, resembling the posture of a fetus in the mother's womb (catalepsy), remain in the position given during examination, and show negativism.
Against this background, short-term excited states may occur, and other psychopathological manifestations are also detected: delusional ideas of persecution, auditory hallucinations. Impulsive actions can be observed, which manifest themselves in the form of sudden aggressiveness towards the environment.