Most current dsm
Diagnostic Criteria, Inclusivity, and Racial Equity
- The DSM-5 released updates to its diagnostic and taxonomic criteria in March 2022 as the DSM-5-TR, including the addition of prolonged grief disorder.
- Codes for clinicians have been altered, which may improve the insurance claims process for certain mental health conditions.
- Cultural, racial, and ethnic factors, as well as gender inclusivity, have been intentionally reviewed and updated in the new DSM-5-TR.
As the stigma around mental health continues to fade, the field itself is changing — some might say for the better.
In March 2022, American Psychiatric Association (APA) Publishing released a Text Revision (TR) to the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) to add clarity around certain mental health conditions and diagnostic criteria and codes.
Highlights in the newly updated DSM-5-TR include the addition of prolonged grief disorder as a condition, as well as symptom codes for suicidal behavior and nonsuicidal self-injury.
The APA also consulted culture and equity professionals to acknowledge the historical role of racial discrimination in clinical diagnoses. Language throughout the DSM-5-TR was updated to promote inclusivity for People of Color and marginalized groups.
The DSM-5-TR has refined some of its diagnostic criteria and codes, which may better inform how mental health professionals work with their clients and how they file claims with insurance companies.
Although the DSM-5-TR cannot fully address the unique experiences and situations of every individual, improved diagnostic criteria may help clinicians identify their clients’ disorders or conditions with more accuracy.
“For the [clients] whose symptoms are not fully represented in the present DSM-5, this is a start to treatment planning and more thoughtfully diagnosing,” said Kendra Kubala, PsyD, a trauma psychologist in Pennsylvania and New York and Psych Central Advisory Board member, in an email.
Prolonged grief disorder
The DSM-5-TR added symptoms associated with prolonged grief disorder to its list of diagnostic criteria..jpg) Now, clinicians can make a formal diagnosis for those who have faced difficulty coping with loss for an extended period of time.
Now, clinicians can make a formal diagnosis for those who have faced difficulty coping with loss for an extended period of time.
Still, everyone’s grieving process is different, and there’s some controversy among clinicians when it comes to linking a person’s experiences of loss to a mental health disorder.
“I think these [clients] would generally get lumped into adjustment disorders or depression diagnoses,” said Karin Gepp, PsyD, a clinical psychologist in New York and Psych Central Advisory Board member, said in an email.
“But studies have shown that 1 in 10 adults may experience prolonged grief — especially now, with this pandemic having killed so many people suddenly, this is a really important addition,” she said.
Diagnostic criteria
According to the DSM-5-TR, the diagnostic criteria for prolonged grief includes:
- a persistent grief response for a duration of longer than 12 months (6 months for a child)
- symptoms that significantly interrupt a person’s day-to-day functioning
- experiences that can’t be attributed to another condition, such as major depressive disorder (MDD) or post-traumatic stress disorder (PTSD)
Unspecified mood disorder
The DSM-5 removed “unspecified mood disorder” as a diagnosis in its 2013 update, which meant that clinicians had to diagnose their clients with a specific mood disorder instead.
The DSM-5-TR has reverted to the “unspecified” diagnosis to include a range of possible mood disorders, which may help clinicians avoid potential misdiagnoses.
“Unspecified mood disorder has been reinstated to provide diagnosis to someone whose presenting symptoms do not fit neatly under bipolar or depressive disorders,” Kubala said.
According to Gepp, distinguishing between bipolar disorder and depressive disorders takes time. Often, symptoms concurrent with bipolar disorder are not always noticeable at the onset.
“When a patient is misdiagnosed with depression and prescribed an SSRI, this could push that person into a manic episode,” Gepp explained.
According to Gepp, the DSM-5-TR reinstating unspecified mood disorder allows practitioners more time to observe a client’s symptoms to provide a more accurate diagnosis and subsequent prescription.
Nonsuicidal self-harm
The DSM-5-TR has added self-harm without the presence of suicidality to its list of diagnoses.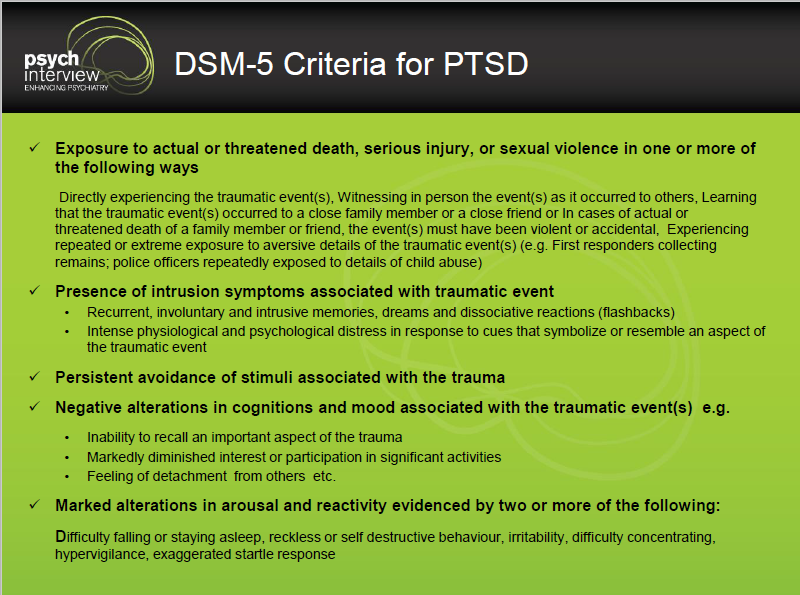
Because not everyone who has engaged in self-harm may do so with the intent of ending their life, lumping it into suicidality could blur assessments made by clinicians.
“It’s good to differentiate those, as there [are] many people who self-harm without an intention of suicide,” Gepp said. “The intent of the injury is the focus, which makes it easier to track the behaviors for us and assess risk.”
In addition, diagnostic codes for suicidal behavior without the presence of other mental health disorders have been included in the new updates.
The DSM-5-TR includes changes to its language around gender and gender identity to help reduce stigma by clarifying that these aspects of a person are not selected by choice.
This includes the more accurate and inclusive changes of:
- “desired gender” to “experienced gender”
- “cross-sex medical procedure” to “gender-affirming medical procedure”
- “natal male/native female” to “individual assigned male/female at birth”
Roberto Lewis-Fernandez, MD, a professor of clinical psychiatry at Columbia University and chair of the DSM-5-TR Cross-Cutting Culture Review Group, told Psych Central that reviewing the DSM through a lens of equity and inclusion and making appropriate changes were high on the committees’ priority list.
Debra Rose Wilson, PhD, MSN, RN, a professor, holistic healthcare practitioner, and Psych Central Advisory Board member, said the addition of racial and cultural perspectives in the DSM-5-TR is beneficial.
“If we’re going to be talking about this, then we should talk about social norms and cultural norms and how they’re going to be different depending on race and where you live, and I think that’s worth identifying,” Wilson said by phone.
According to Lewis-Fernandez, future iterations of the DSM-5 will likely incorporate further changes, specifically around how social, sociocultural, and genetic disorder causations intersect, all with the goal of enabling clients to be seen within a more holistic framing.
“The role of social determinants of mental health has been increasingly recognized in recent years,” he said. “DSM-5-TR started to incorporate this information but there is still more that needs to be done in this area.”
The DSM-5-TR’s acknowledgment of how race and discrimination have historically impacted mental health care is a step forward in creating more safe and inclusive environments for People of Color and marginalized groups.
But barriers to quality mental health care still exist, such as cost factors, health insurance, and enough access to culturally competent counselors and therapists.
According to Kubala, the varied opinions and shifting cultural dynamics within the mental health field speak to the necessity of ongoing updates to the DSM. As research in the field continues to evolve, so will the manual.
“It’s always beneficial to have an open dialogue between [clients], providers, and the public regarding mental illness, and ways in which the field is continually evolving in an effort to provide the most comprehensive, sensitive, research-based, compassionate, appropriate treatment,” Kubala said.
What Are the New Classifications in the DSM-5?
Diagnosis is the cornerstone of any mental health clinician’s patient care. To make an accurate diagnosis of any mental health disorder, you need the most up-to-date inf
ormation available in the DSM. The most recent DSM is the fifth edition, which introduced a host of changes from the previous version. Understanding the updates is essential to providing correct diagnoses and selecting appropriate treatment in clinical practices.
Understanding the updates is essential to providing correct diagnoses and selecting appropriate treatment in clinical practices.
Table of Contents
- What Is the DSM?
- What Have Been the Major Changes of DSM-5?
- New and Updated Diagnoses
- Classifications With New DSM-5 Criteria
- DSM-5 Codes and ICD-10-CM
- Strengths and Weaknesses of DSM-5
- Viability for Research
- Developments for the Next DSM
- Updates to Intellectual Disability
- ICANotes: Your Source for DSM Information
What Is the DSM?
The Diagnostic and Statistical Manual of Mental Disorders, fifth edition, also known as DSM-5, is the handbook currently used by U.S. behavioral and mental health professionals to make diagnoses. Many people consider the DSM the “Bible” of the mental health field, providing descriptions and classifications of mental disorders, including their symptoms and other criteria required for diagnosis. The DSM gives clinicians a common language to use when communicating information about patients, and researchers a shared basis to study disorders and recommend potential revisions. The DSM has been instrumental in driving advanced research on every aspect of mental and behavioral health. The first DSM came out in 1952 and has undergone several revisions as researchers’ knowledge of mental disorders has evolved. DSM-5 arrived in 2013, bringing multiple updates to mental illness classification that have, in some cases, stirred controversy in the field. The revision process that created DSM-5 lasted nearly a decade and involved nearly 400 scientists and more than 160 renowned clinicians and researchers from around the world. The American Psychiatric Association approved all proposed changes, and a Scientific Review Committee reviewed the strength of the evidence of each modification with a template of validators.
The DSM has been instrumental in driving advanced research on every aspect of mental and behavioral health. The first DSM came out in 1952 and has undergone several revisions as researchers’ knowledge of mental disorders has evolved. DSM-5 arrived in 2013, bringing multiple updates to mental illness classification that have, in some cases, stirred controversy in the field. The revision process that created DSM-5 lasted nearly a decade and involved nearly 400 scientists and more than 160 renowned clinicians and researchers from around the world. The American Psychiatric Association approved all proposed changes, and a Scientific Review Committee reviewed the strength of the evidence of each modification with a template of validators.
What Have Been the Major Changes of DSM-5?
Broadly, the DSM’s overhaul entails five overarching changes meant to make diagnostics easier and more accurate for clinicians. These changes for mental and behavioral disorders include the following.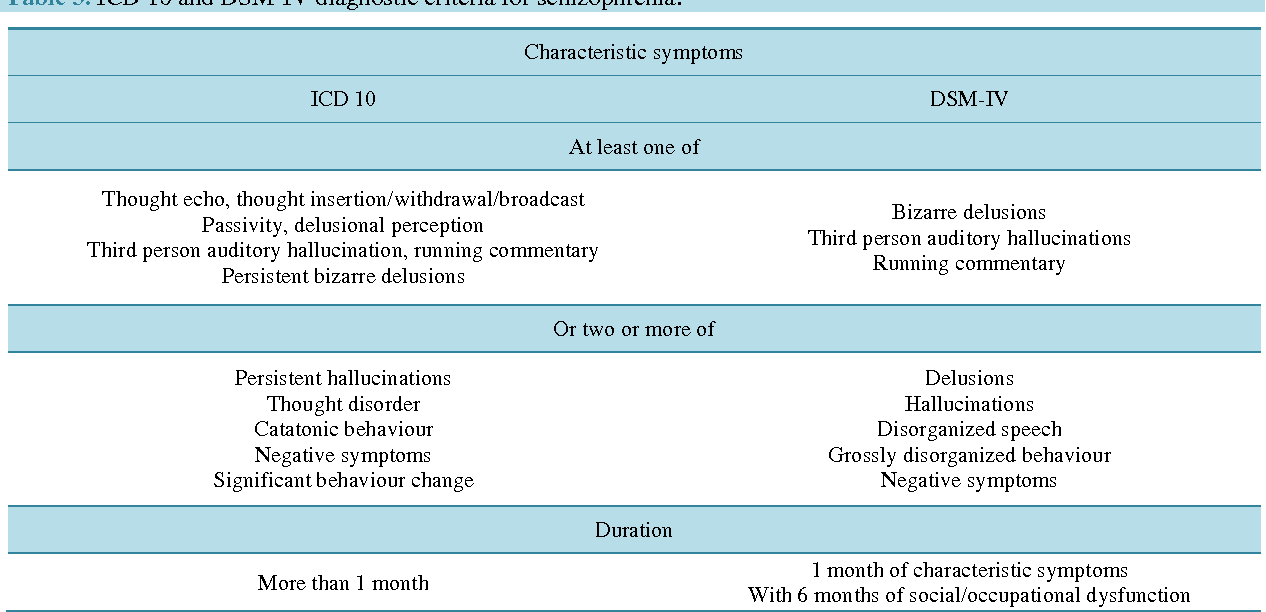
- Developmental focus: DSM-5 places disorders according to the age at which they are most likely to appear, starting in childhood and ending with disorders that usually occur in old age. Descriptions of disorders also include the different ways they might present according to age.
- New diagnostic criteria: Criteria for some disorders will change, including the addition of new disorders and removal of subtypes of schizophrenia.
- Dimensional measures: DSM-5 includes measures of a disorder’s severity to help clinicians think about what dimensions of disorders are similar. These measures aim to benefit patients with multiple diagnoses by providing more nuanced insight into their continuum of symptoms.
- Culture and gender emphasis:
A multitude of cultural and social factors can impact diagnosis. DSM-5 has a new section describing cultural syndromes, their potential causes and how people express them.
- Further research: The DSM now contains a section that describes conditions that need further research. Future editions of the DSM may or may not add these conditions based on the results of ongoing research. They currently do not have ICD codes clinicians can use to diagnose patients and receive reimbursement from insurance companies.
New and Updated Diagnoses
The DSM-5 classifications include updates and additions for many mental disorders. Clinicians and researchers have eliminated some classifications and combined others. The following 17 mental disorders are new or updated in DSM-5.
- Social communication disorder: This addition allows clinicians to diagnose speech and language issues that aren’t symptoms of reduced cognitive ability or autism.
- Disruptive mood dysregulation disorder: This diagnosis applies to children under 18 who display extreme rages and frequent outbursts, eliminating the classification of childhood bipolar disorder.
- Premenstrual dysphoric disorder: This extremely controversial addition affects up to 5% of premenopausal women.
- Hoarding disorder: This condition, depicted in multiple TV shows, is now an official diagnosis listed under obsessive-compulsive disorders.
- Caffeine withdrawal: Another divisive addition, caffeine withdrawal has moved from the appendix of DSM-IV to “Caffeine-Related Disorders” in DSM-5.
- Cannabis withdrawal: The proliferation of legal cannabis led to a pronounced increase in people experiencing cannabis withdrawal, which now falls under “Substance-Related and Addictive Disorders.”
- Excoriation disorder: This diagnosis addresses chronic scratching and picking at the skin, and is under “Obsessive-Compulsive and Related Disorders.”
- Binge eating disorder: Binge eating even once a week now qualifies a patient for this diagnosis, rather than biweekly.
- Rapid eye movement sleep behavior disorder: This disorder causes people to act out dreams in potentially dangerous ways, and is now separate from the parasomnia category it occupied in the previous DSM.
- Restless leg syndrome: Previously classified as a form of dyssomnia, restless leg syndrome now has full DSM status as a separate diagnosis.
- Major neurocognitive disorder with Lewy body disease: This classification differentiates major and mild neurocognitive disorders, allowing for more specific treatment.
- Disinhibited social engagement disorder: This classification previously fell under reactive attachment disorder, but is now under a separate category because children with it do not necessarily lack attachment.
- Additional eating disorders: In addition to recognizing binge eating disorder, the newest edition of the DSM adds rumination, pica and avoidant/restrictive food intake disorder.

- Gender dysphoria: Individualswhose gender at birth is contrary to the one they identify with will now receive a diagnosis of gender dysphoria instead of gender identity disorder. The shift in language intends to represent these individuals’ experiences more accurately and reduce stigma. Gender dysphoria will also now have a dedicated chapter separate from sexual dysfunctions and paraphilic disorders.
- Specific learning disorder: Specific learning disorder is now a single, stand-alone category. It contains different specifiers to indicate more narrowly defined types of learning disorders, such as dyslexia, that affect reading, writing or math. It also replaces the IQ-achievement discrepancy requirement with characteristic-based criteria.
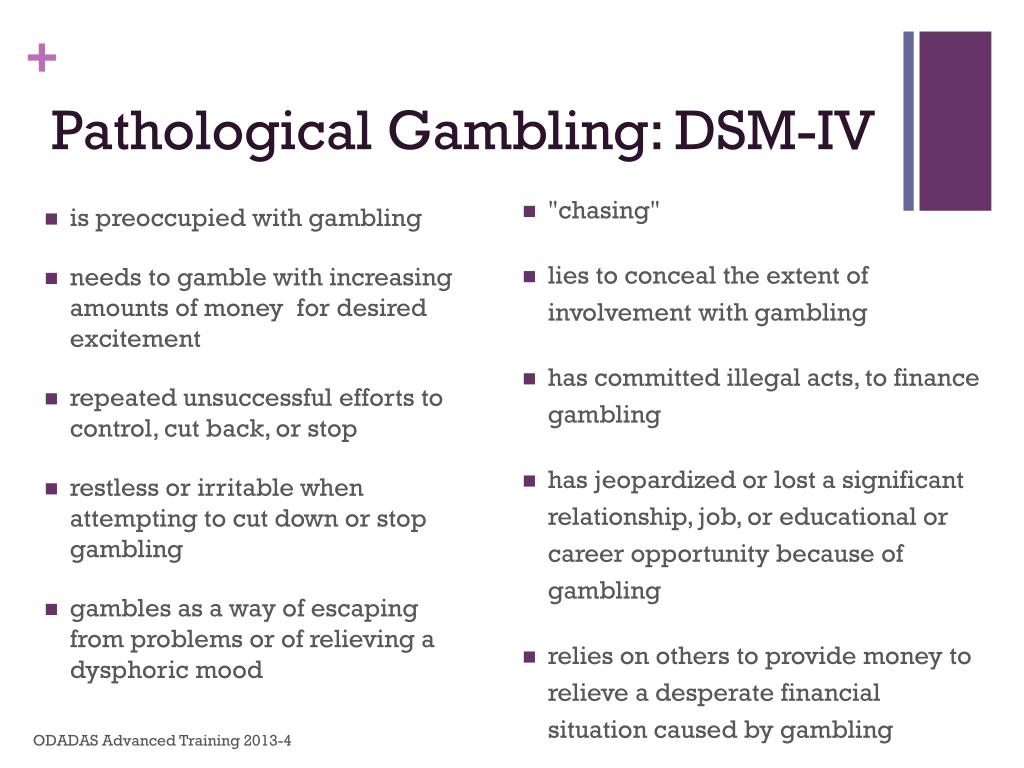
- Gambling disorder: The chapter on addictive disorders now includes gambling disorder as a diagnosable condition. The DSM-IV included a section on pathological gambling but did not classify it as an official addictive disorder.
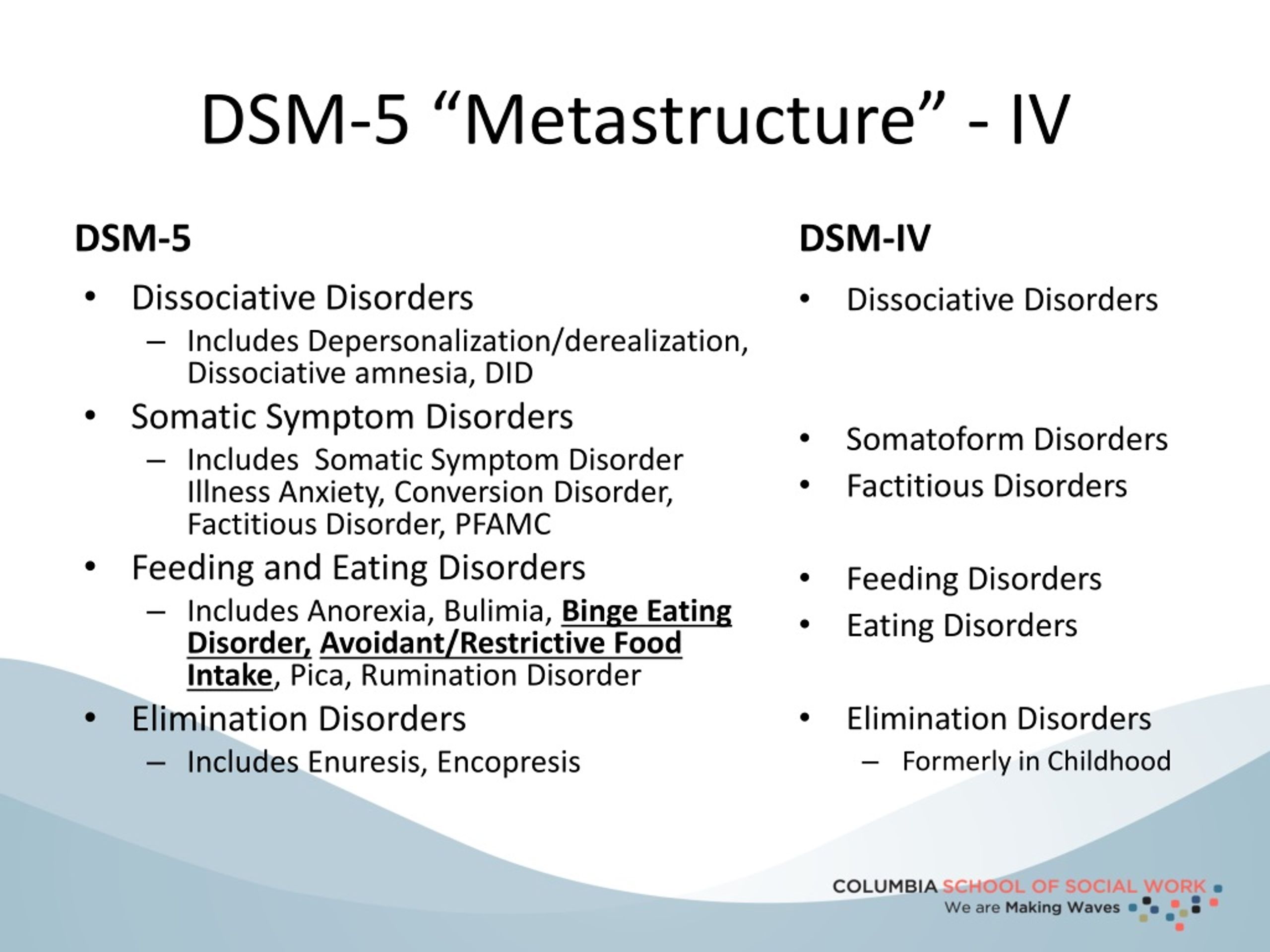
- Somatic symptom disorder: DSM-5 replaces the old somatoform disorders — such as somatization disorder, hypochondriasis, pain disorder and undifferentiated somatoform disorder — with somatic symptom disorder. It makes substantial changes to the disorder criteria to clarify the distinctions between similar conditions and minimize overlap.
Classifications With New DSM-5 Criteria
In addition to the diagnoses added to DSM-5, several mental disorders in the fifth edition have new criteria, including:
- Autism spectrum disorder: One of the most crucial changes involving collapsing diagnoses deals with autism spectrum disorder. In DSM-IV, there were four categories: autism, Asperger’s, childhood disintegrative disorder and pervasive developmental disorder. DSM-5 collects all four under the umbrella of autism spectrum disorder.
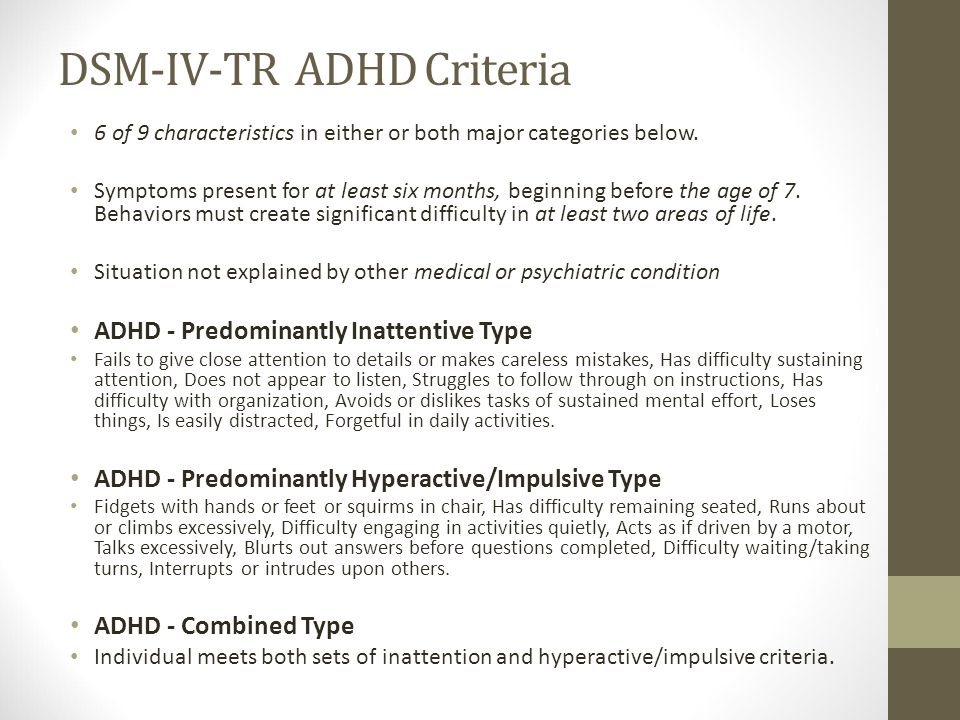
- ADHD: Revisions to the ADHD diagnosis have broadened the criteria to allow for adult-onset cases.
 Because adult brains are more developed and adults have better impulse control, clinicians can diagnose them with fewer symptoms than children.
Because adult brains are more developed and adults have better impulse control, clinicians can diagnose them with fewer symptoms than children. - PTSD: Due to the new research on PTSD available, DSM-5 has expanded detail on this diagnosis. The new criteria add more information on diagnosing children and create four separate classes of symptoms: arousal, avoidance, flashbacks and negative impacts on mood and thought patterns.
- Mental retardation: Asa result of DSM-5’s new focus on cultural relevance, it has reclassified the collection of issues called “mental retardation” as “Intellectual Development Disorder” to reflect changes in everyday language. The criteria for diagnosis have also shifted to focus more on level of function, instead of relying so heavily on IQ score.
- Major depressive disorder: The new addition removes the exclusion that prevented many recently bereaved individuals from receiving a major depressive disorder diagnosis.
- Conduct disorder: The update to conduct disorder adds a descriptive features specifier to the diagnosis. The specifier identifies symptoms, such as limited empathy and little concern for others’ feelings and well-being, that extend beyond the general presence of negative behavior. It will help clinicians identify and diagnose individuals who experience a more severe form of this disorder and require more individualized, intensive treatment.
- Minor neurocognitive disorder: Minor neurocognitive disorder previously required only a single criterion —neuropsychological testing results — for diagnosis. DSM-5 defines this disorder using several cognitive and related criteria instead. The revision will enable early detection and treatment of cognitive decline before it develops into major neurocognitive disorder, or dementia.
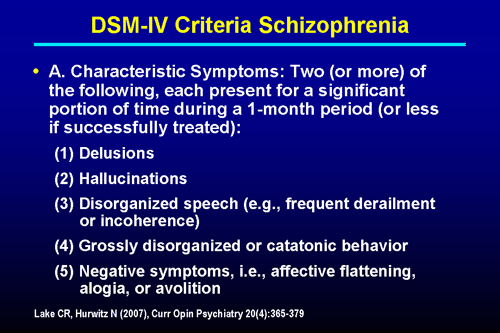
- Schizophrenia: For schizophrenia, DSM-5 raises the symptom threshold for diagnosis. An individual must now exhibit at least two of the potential symptoms to receive a diagnosis.
 The diagnostic criteria for schizophrenia also no longer identify subtypes, since these predominant symptoms tended to shift throughout the patient’s life. Some of the subtypes, such as catatonia, have now become specifiers for schizophrenia and other disorders.
The diagnostic criteria for schizophrenia also no longer identify subtypes, since these predominant symptoms tended to shift throughout the patient’s life. Some of the subtypes, such as catatonia, have now become specifiers for schizophrenia and other disorders. - Sleep-wake disorders: The sleep-wake disorders in the DSM have undergone a few diagnostic updates, many of which remove the distinction between primary and secondary disorders.
DSM-5 Codes and ICD-10-CM
The DSM and the World Health Organization’s International Classification of Disease are companion publications. The DSM contains diagnostic criteria, while the ICD codes monitor mortality and morbidity statistics and are necessary for insurance reimbursement. There are no DSM codes. Instead, the numbers you will find next to diagnoses in the manual are ICD codes. The manual contains ICD-9 codes in bold and new ICD-10 codes in parentheses. Many codes stayed the same between ICDs, but it is vital to note any changes between ICD codes, as clinicians switched to using ICD-10 in 2015. Several disorders have recently received coding updates. The following disorders or conditions initially had no ICD-10-CM codes in DSM-5. They have now had recommended codes since October 2020.
Several disorders have recently received coding updates. The following disorders or conditions initially had no ICD-10-CM codes in DSM-5. They have now had recommended codes since October 2020.
- Alcohol withdrawal, uncomplicated, with mild use disorder: F10.130
- Alcohol withdrawal, delirium, with mild use disorder: F10.131
- Alcohol withdrawal, with perceptual disturbance, with mild use disorder: F10.132
- Alcohol withdrawal, with mild use disorder: F10.139
- Alcohol withdrawal, uncomplicated, with use disorder: F10.930
- Alcohol withdrawal, delirium, without use disorder: F10.931
- Alcohol withdrawal, with perceptual disturbance, without use disorder: F10.932
- Alcohol withdrawal, without use disorder: F10.939
- Opioid withdrawal, with mild use disorder: F11.13
- Cannabis withdrawal, with mild use disorder: F12.
 13
13 - Sedative, hypnotic or anxiolytic withdrawal, uncomplicated, with mild use disorder: F13.130
- Sedative, hypnotic or anxiolytic withdrawal, delirium, with mild use disorder: F13.131
- Sedative, hypnotic or anxiolytic withdrawal, with perceptual disturbance, with mild use disorder: F13.132
- Sedative, hypnotic or anxiolytic withdrawal, unspecified, with mild use disorder: F13.139
- Cocaine withdrawal, with mild use disorder: F14.13
- Cocaine withdrawal, without use disorder: F14.93
- Amphetamine or other stimulant withdrawal, with mild use disorder: F15.13
- Other (or unknown) substance withdrawal, uncomplicated, with mild use disorder: F19.130
- Other (or unknown) substance withdrawal, delirium, with mild use disorder: F19.131
- Other (or unknown) substance withdrawal, with perceptual disturbance, with mild use disorder: F19.
 132
132 - Other (or unknown) substance withdrawal, unspecified, with mild use disorder: F19.139
Strengths and Weaknesses of DSM-5
There is always some disagreement between professionals on the best diagnostic and treatment approaches, and continuing research brings more information that drives revisions to the DSM. Some clinicians have enthusiastically greeted many new classifications in DSM-5, while others insist the same changes are detrimental. Some of the most significant controversies and problems with DSM-5 include the following.
1. Grief and Major Depression
The previous DSM had a bereavement exclusion for major depressive disorder. Using DSM-IV, clinicians could not diagnose people who had recently experienced a loved one’s death with depression unless:
- Symptoms lasted longer than two months.
- Symptoms produced functional impairment.
- The patient had a morbid preoccupation with worthlessness.
- There was suicidal ideation, psychotic symptoms or psychomotor retardation.
DSM-5 has replaced the bereavement exclusion with a note that provides further guidance on how to tell grief apart from major depression. There is now another guide for recording reactions to a loved one’s death, found in the chapter “Other Conditions That May Be a Focus of Clinical Attention.” Clinicians who oppose eliminating the bereavement exclusion are concerned that removing it will lead to people with normal grief receiving an inappropriate depression diagnosis.
2. Oppositional Defiant Disorder
Oppositional defiant disorder was highly controversial when added to DSM-IV, and the outcry has continued, as it remains a diagnosis in DSM-5. The condition has these characteristics:
- Using obscene language
- Angry outbursts
- Frequent resentment
- Intentionally irritating or hurting others
- Being easily angered
- Refusing to follow instructions or rules
- Throwing temper tantrums repeatedly
The DSM-5 stipulates that these behavioral patterns must last for six months or more and not result from a different mental health issue.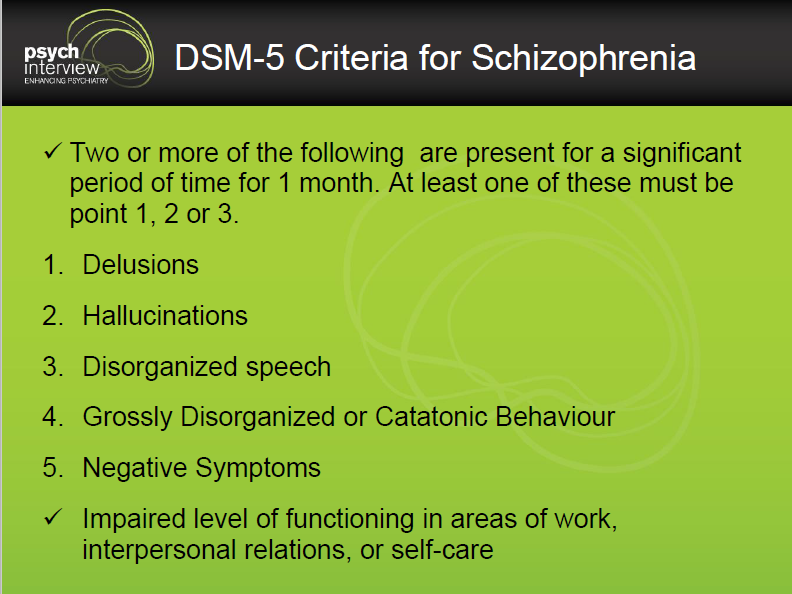 The controversy here is that the relatively lax criteria may lead to over-diagnosis of what may only be bad behavior. It can be severely damaging to label a child or teen “mentally ill” when they may not be.
The controversy here is that the relatively lax criteria may lead to over-diagnosis of what may only be bad behavior. It can be severely damaging to label a child or teen “mentally ill” when they may not be.
3. Pediatric Bipolar Disorder
While ODD remained in the DSM, a diagnosis some clinicians have been asking for is still missing. Rather than adding a diagnosis for pediatric bipolar disorder, also known as child-onset bipolar disorder, DSM-5 introduced disruptive mood dysregulation disorder. DMDD focuses on temper tantrums and general anger rather than addressing all the symptoms of pediatric bipolar disorder, so clinicians must create a workaround. The closest thing to a diagnosis of pediatric bipolar disorder is a combination of DMDD diagnosed alongside major depression. These two diagnoses can occur together, but clinicians cannot combine DMDD and bipolar.
Viability for Research
While the DSM’s creators intended it to function as a common language for researchers to use, it seems the manual has not accomplished part of its mission. According to many experts, DSM-5 does not provide a strong foundation for studying mental illnesses. The National Institute of Mental Health has rejected DSM-5 for research purposes and has shifted its funding away from DSM categories to more neuroscience-based sources. However, this announcement was not a rejection of the DSM outright. Instead, NIMH clarified that while the DSM may no longer be sufficient for researchers, it remains the gold standard for clinical diagnosis.
According to many experts, DSM-5 does not provide a strong foundation for studying mental illnesses. The National Institute of Mental Health has rejected DSM-5 for research purposes and has shifted its funding away from DSM categories to more neuroscience-based sources. However, this announcement was not a rejection of the DSM outright. Instead, NIMH clarified that while the DSM may no longer be sufficient for researchers, it remains the gold standard for clinical diagnosis.
Developments for the Next DSM
One of the most substantial changes for the next DSM is the shift in revision processes. The APA recognizes the need to make more timely updates to the DSM in response to breakthroughs in research. The change from the Roman numerals used through DSM-IV to the Arabic numerals in DSM-5 reflects the intention to publish incremental updates. We may soon be seeing a DSM-5.1, DSM-5.2 and more until enough cumulative updates necessitate a whole new edition.
The eight conditions identified as needing further study in DSM-5 are:
- Attenuated psychosis syndrome
- Caffeine use disorder
- Depressive episodes with short-duration hypomania
- Internet gaming disorder
- Neurobehavioral disorder associated with prenatal alcohol exposure
- Non-suicidal self-injury
- Persistent complex bereavement disorders
- Suicidal behavior disorder
Though these conditions do not have formal diagnoses in DSM-5, they will be the first up for consideration in updates to mental illness classification.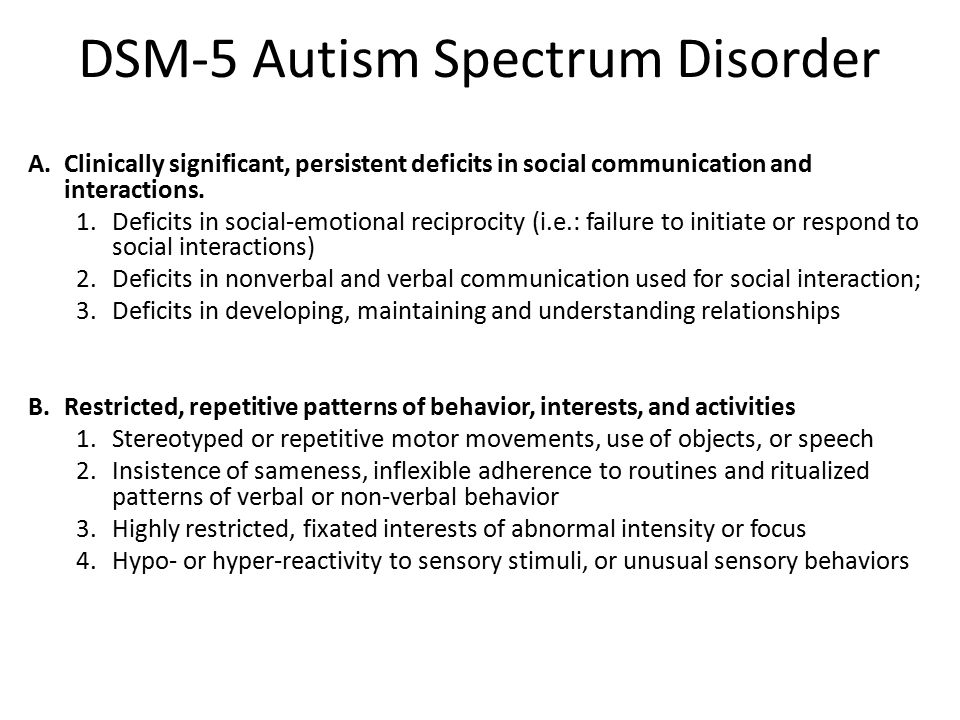 The information on them is in the DSM to give clinicians more details that may influence the diagnosis of other conditions. For example, someone addicted to caffeine can only receive a diagnosis of a substance-related and addictive disorder, but the diagnosing clinician can gain more insight into the situation by reading the caffeine use disorder section.
The information on them is in the DSM to give clinicians more details that may influence the diagnosis of other conditions. For example, someone addicted to caffeine can only receive a diagnosis of a substance-related and addictive disorder, but the diagnosing clinician can gain more insight into the situation by reading the caffeine use disorder section.
Updates to Intellectual Disability
One of the formally proposed DSM-5 updates regards the diagnostic features section of intellectual developmental disorder. At present, the criteria for diagnosing an intellectual disability are:
- Deficiency in adaptive daily life skills or functioning.
- Deficits in intelligence.
- Onset during childhood.
DSM-5 requires that the intellectual impairments must directly relate to the deficiency in adaptive functioning. However, the APA has recommended replacing this with a criterion that specifies a lack of adaptive functioning is due to intellectual deficits. One example given by the American Association on Intellectual and Developmental Disabilities is the case of the state of Texas seeking to execute a man with an intellectual disability. According to the state, the man’s adaptive functions likely resulted from a lack of learning opportunities and were unrelated to his intellectual function. Therefore, he did not have any intellectual disability. In 2016, the Supreme Court ruled against the state, found that the man does have an intellectual disability, then disallowed his execution. The CEO of AAIDD, Margaret Nygren, says that experts agree it is inaccurate to connect or conflate intellect and adaptive behavior because it is impossible to determine which elements of behavior result from mental health issues, IQ or a lack of educational opportunities. The use of the current DSM-5 language in Moore v. Texas is a clear indicator that the DSM is not perfect and needs updates in this area.
One example given by the American Association on Intellectual and Developmental Disabilities is the case of the state of Texas seeking to execute a man with an intellectual disability. According to the state, the man’s adaptive functions likely resulted from a lack of learning opportunities and were unrelated to his intellectual function. Therefore, he did not have any intellectual disability. In 2016, the Supreme Court ruled against the state, found that the man does have an intellectual disability, then disallowed his execution. The CEO of AAIDD, Margaret Nygren, says that experts agree it is inaccurate to connect or conflate intellect and adaptive behavior because it is impossible to determine which elements of behavior result from mental health issues, IQ or a lack of educational opportunities. The use of the current DSM-5 language in Moore v. Texas is a clear indicator that the DSM is not perfect and needs updates in this area.
Understanding the latest DSM classifications is crucial to providing accurate diagnoses and the most appropriate course of treatment for your patients. The most recently updated ICD codes, ICD 11, became available in June 2018, and clinicians will also need to become familiar with those since they will be a reporting requirement starting in 2022. Keeping up with crucial information on the DSM and ICD codes can be time-consuming and confusing, which is why ICANotes works hard to provide up-to-date resources and information for mental and behavioral health clinicians. For additional information on DSM-5 updates and ICD changes, contact ICANotes today.
The most recently updated ICD codes, ICD 11, became available in June 2018, and clinicians will also need to become familiar with those since they will be a reporting requirement starting in 2022. Keeping up with crucial information on the DSM and ICD codes can be time-consuming and confusing, which is why ICANotes works hard to provide up-to-date resources and information for mental and behavioral health clinicians. For additional information on DSM-5 updates and ICD changes, contact ICANotes today.
Watch a Live Demo
Start a Free Trial
Related Posts
Mental & Behavioral Healthcare Billing: How to Maximize Your Reimbursement Rate
Understanding the Mental Health Crisis Facing Young People
CPT Code Basics: What You Should Know
What Is Evidence-Based Health Care?
What You Need to Know About MIPS in 2019
Sources:
- https://www.psychiatry.org/psychiatrists/practice/dsm/feedback-and-questions/frequently-asked-questions
- https://www.
 apa.org/monitor/2013/04/dsm
apa.org/monitor/2013/04/dsm - https://ajp.psychiatryonline.org/doi/10.1176/appi.ajp.2012.11081302
- https://www.naswma.org/page/ICD10andDSM5
- https://www.aafp.org/afp/2014/1115/p690.html
- https://www.apa.org/monitor/2013/07-08/nimh
- https://www.psychiatry.org/psychiatrists/practice/dsm/proposed-changes
- https://www.disabilityscoop.com/2019/08/12/psychiatrists-considering-change-intellectual-disability-criteria/27000/
- https://www.oyez.org/cases/2018/18-443
- https://www.who.int/news-room/detail/18-06-2018-who-releases-new-international-classification-of-diseases-(icd-11)
Last updated May 21, 2021.
October Boyles, MSN, BSN, RN
Clinical Director October has been a Registered Nurse for over 15 years. She is board certified in Mental Health and Psychiatric Nursing. She holds a Bachelor of Arts from the University of North Carolina at Greensboro. She also graduated with bachelor and master degrees in Nursing from Western Governors University.
ICD-10 and DSM-V: differences in the diagnosis of eating disorders
“Today there are 2 main guidelines that specialists from different countries rely on to classify and diagnose all existing diseases, including eating disorders. These are ICD (International Statistical Classification of Diseases and Related Health Problems) and DSM (Diagnostic and Statistical Manual of Mental Disorders).
Of course, there are also national guidelines and classifications. For example, in Soviet psychiatry, such a type of schizophrenia as sluggish schizophrenia was separately distinguished, although such a diagnosis is generally absent in international classifications.
Nevertheless, qualified specialists are guided by the ICD or DSM in their work.
The ICD has more than three hundred years of history and is currently the official regulatory document of the World Health Organization.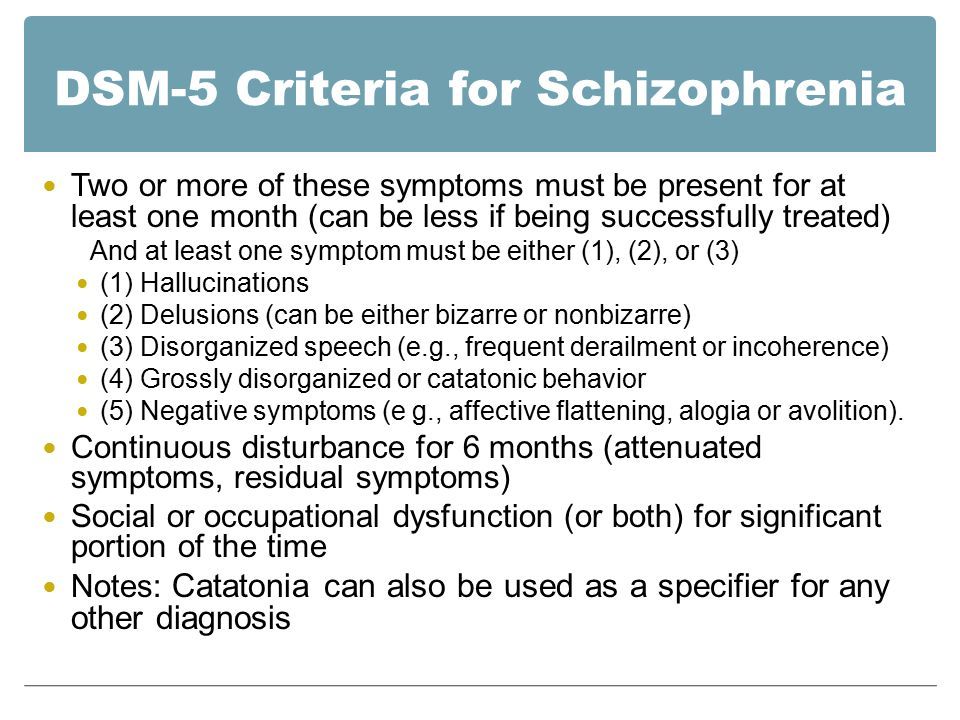
ICD went through 10 editions. The current ICD-10 is used, which has been in use in WHO Member States since 1994. And work is already underway on the ICD-11, which is planned to be introduced after 2018.
It is important to note that in ICD-10 represents all diseases. Mental and behavioral disorders are presented there only as a separate chapter. Eating disorders are not a separate rubric in this chapter, but are included under the broader rubric Behavioral Syndromes Associated with Physiological Disorders and Physical Factors.
This heading has a subheading "Eating Disorders" (code F50), which includes:
- anorexia nervosa
- bulimia nervosa
- overeating associated with other psychological disorders
- vomiting associated with other psychological disorders
- other eating disorders
- Eating disorder, unspecified
The fundamental point - in ICD-10 there is only a classification and key features of eating disorders.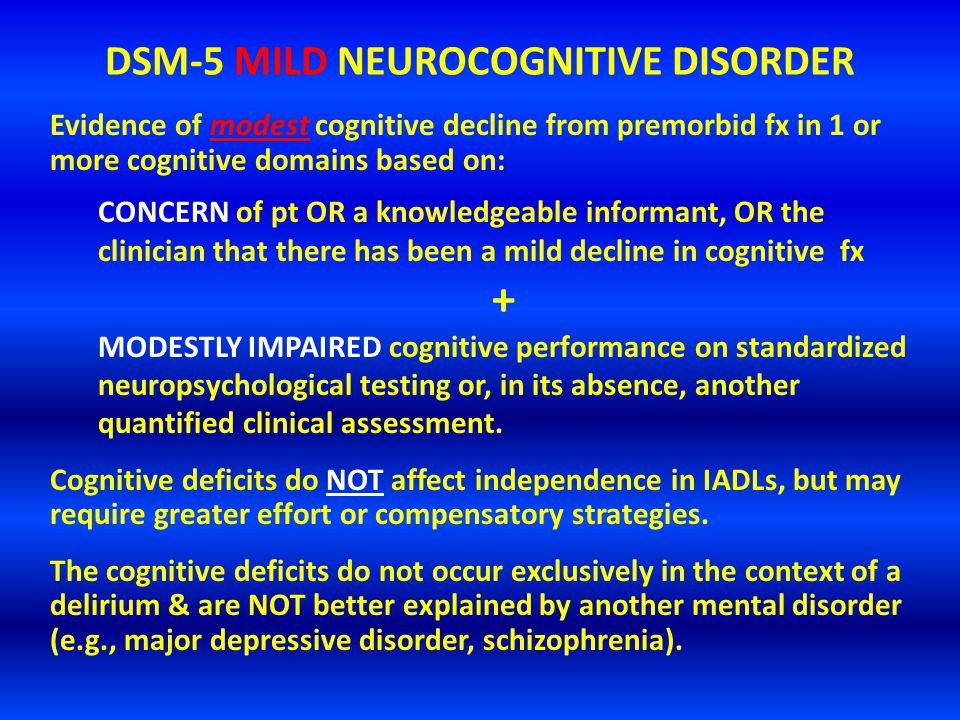 And that's it! Details of criteria, prevalence, differential diagnosis, etc. in the ICD, unfortunately, you will not find.
And that's it! Details of criteria, prevalence, differential diagnosis, etc. in the ICD, unfortunately, you will not find.
Regarding the DSM, this guide was originally developed by the American Psychiatric Association. The first edition (DSM-I) was in 1952. Now the 5th edition (DSM-V), released in 2013, is already in use. This edition is not available in Russian.
This manual features detailed classification and, most importantly, the description of specifically mental disorders (hence the name).
In particular, there is a separate section devoted to eating disorders.
The following eating disorders are distinguished in it:
- "peak" (perverted appetite)
- chewing disorder
- avoidant/restrictive eating disorder
- anorexia nervosa
- bulimia nervosa
- overeating
- other specific eating or eating disorders
- non-specific eating or eating disorders
An important difference of the DSM-V is that, unlike the ICD-10, for each of the major eating disorders are given:
- criteria for diagnosing eating disorders
- extended explanation for each criterion
- subtypes or severity of the disorder
- diagnostic features
- data on the prevalence of the disorder
- information on the course and development of the disease
- risk factors
- specific diagnostic markers
- suicide risk data
- consequences of an eating disorder
- differential diagnosis
- relationship with other psychiatric disorders (not related to eating disorders).
In addition, DSM-V is the most current version of released in 2013. It presents the latest data on the criteria for mental disorders, some of which differ from those in earlier versions of the guide.
This also applies to eating disorders.”
The author of the article is Sergei Leonov, source https://www.b17.ru/article/mkb10-i-dsm5-otlichiya-v-diagnostike/
* — required fields
By submitting an application, you agree to the terms
of the privacy policy
Read also
Live Healthy Program on Channel One On October 13, the program “Live Healthy” was released, with the participation of a psychiatrist of the Center …
Read more »
Program “Beyond” on NTV channel
In October, psychiatrist Marina Evgenievna Kotik took part in the filming of the program “For …
Read more” Our daughter was 12 years old when she was diagnosed with anorexia and it turned our world upside down…
Read more »
Specialized therapeutic massage for patients with eating disorders
Read more »
Never use eating disorder language to object to an eating disorder
The day I was diagnosed with anorexia, the nutritionist told me: “Don't worry, you can…
Read more »
All-Russian scientific and practical conference with international participation "Diagnosis, treatment and prevention of eating disorders"
From June 1 to June 3, Moscow hosts the All-Russian Scientific and Practical Conference with an international …
Read more »
Directory and catalog of organizations in Russia and other republics
Da Vinci School
Bargain
Russia, Irkutsk, st. Gornaya, 24
Gornaya, 24
+73952725412
Read more
Network of veterinary pharmacies IP Kasyanenko V.V.
Veterinary clinics
Russia, Birobidzhan, Sovetskaya st. 111 V
84262270120
Read more
OOO PROEKTOR24
Audio / Video
Moscow, Altufevskoe shosse 41
+7(925)575-78-19
Read more
Hydraulics SpecKomplekt, OOO
Spare parts for special equipment
Moscow, Butovsky dead end, 1B
+79771040123
Read more
Law Center Lawers
Bargain Purchases
Moscow, Nagatinskaya st., 22, building 1
+7-916-826-50-00
Read more
AutoPrime - Autocomplex
Car washes
Chita, Olympic 2
8 (3022) 72-72-77
Read more
ArtTravel - bus tours from Ufa
Travel agencies
Russia, Ufa, Komsomolskaya 37
89177828666
ansoyuz@gmail.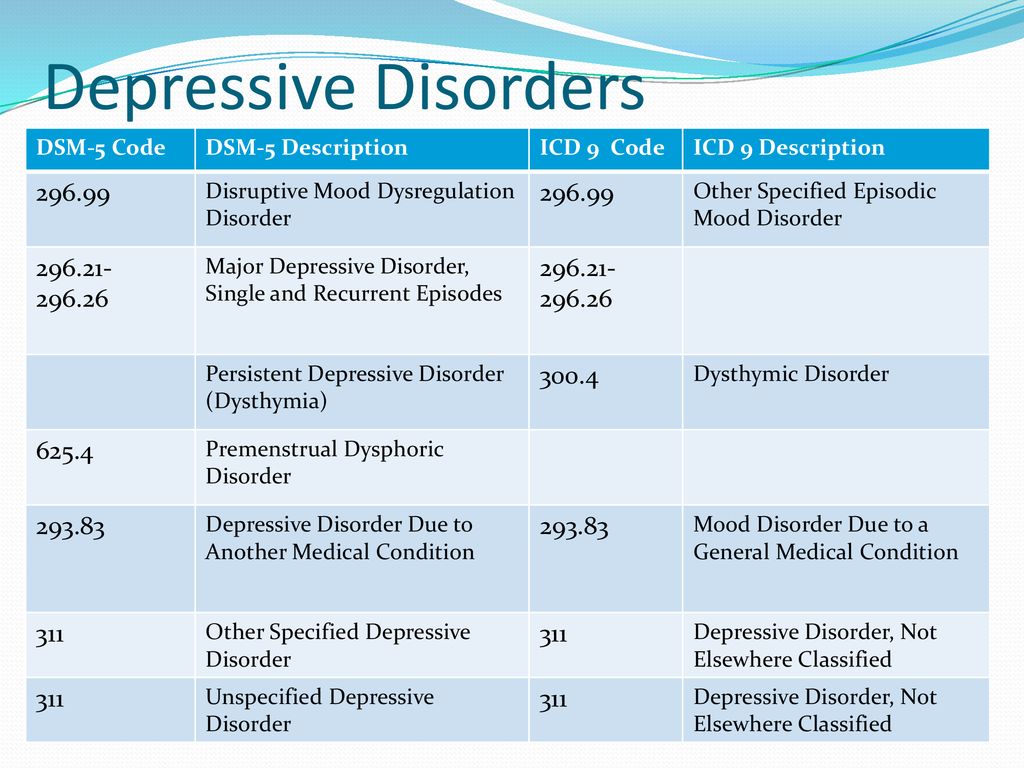 com
com
Read more
PhotoMania
Bargain shopping
Biysk, Merlin street, 51
+79237
09237
[email protected]Read more
Photokeramik - pottery workshop
Monuments and ritual accessories
Moscow,
+74952310927
Read more
WWW-OKNA.RU
Bargain shopping
Moscow, Garibaldi d. Read more
SPASIMOBILE
Car heating services
St. Petersburg,
+7 812 443 87 64
Read more
Avantis Specialized Center for Orthodontics
Bargain Shopping
Russia, Novosibirsk, st. Dusi Kovalchuk
+7(383)331-08-08
Read more
Facade and roofing systems
Bargain shopping
Russia, Angarsk, st. Tchaikovsky, shopping center StroyMir, 2nd floor, pavilion 28
+79249950888
mail@spec38. ru
ru
Read more
Avantis
Dental centers
st. Dusi Kovalchuk d.250, office 12/1
83833310808
Read more
SkolService
Installation and repair of auto glass
Kirov, Moskovskaya 1E
+79128261600
Read more
Barsuk
Night clubs
Tyumen, Krasina 7a
+7 963 067 67 67
Read more
LLC ALZA-NEFT
Trade automation
603152, Nizhny Novgorod region, Nizhny Novgorod, st. Shaposhnikova, 13, office 402, room 2
+7 926 463 48 67
Read more
LLC PKF ORGKROVLIA
Cemeteries
Stary Oskol, Olympic 62
8
02344Read more
MicroEM Technologies
Radio electronic devices
Pine alley, 6A
+74997000990
microemtechnology@yandex.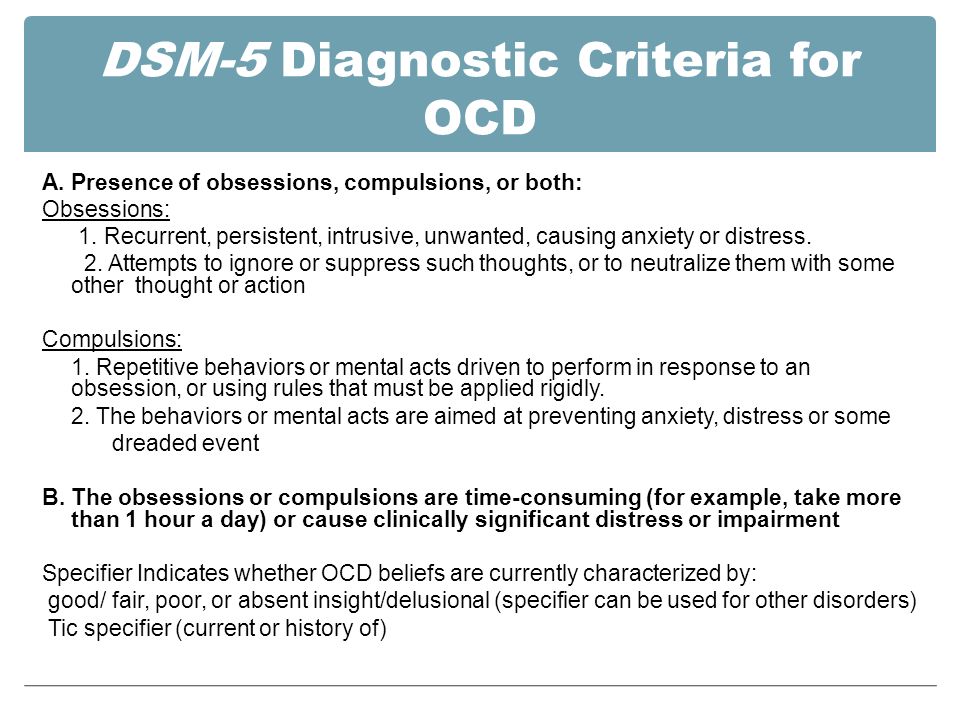 ru
ru
Read more
MAXIMEDIA
Full service advertising agencies
Almaty, Shevchenko 90
+77273271375
Read more
Elba LLC
Equipment / tools rental
Labor Avenue, 63
+7 (473) 254-31-10
Read more
Company order printing.rf
Bargain purchases
Moscow, Rusanova passage, 2c1
+7 (495) 142 - 87 - 18
Read more
Build a dacha
Construction of dachas / cottages
Russia, Yaroslavl, Leskova, 28
89154172983
Read more
Web Studio - Video filming and online broadcasting
Video studios
Yamasheva Ave. 94
+79934118920
Read more
Anticafe Come in If What
Bargain shopping
Saint-Petersburg, Prospect Engels, 139/21
+78123896160
pvkzec@mail. ru
ru
Read more
Creative Production (IP Matveev A.O.)
Profitable purchases
Bryansk, Kostycheva 3
+79155369495
Read more
Koi sushi
Sushi bars
Russia, Krasnodar street named after the 40th anniversary of the Victory, 143
+7 (999) 633-36-30
Read more
LLC NPO PMP Ventilation
Ventilation / heating equipment
123298, Moscow, st. Marshal Biryuzova, 4, office 2
+74997555751
Read more
Flower delivery
Flower delivery
123100, Moscow, st. Mantulinskaya, 2
+7
65785Read more
Angelika.rf
Cosmetics / consumables for beauty salons
Novosibirsk, Pisareva st. Read more
Hanler Tver
Automatic gates / barriers
Russia, Tver Oktyabrsky prospect, 99
+7 (482) 231-91-20
tver@hanler.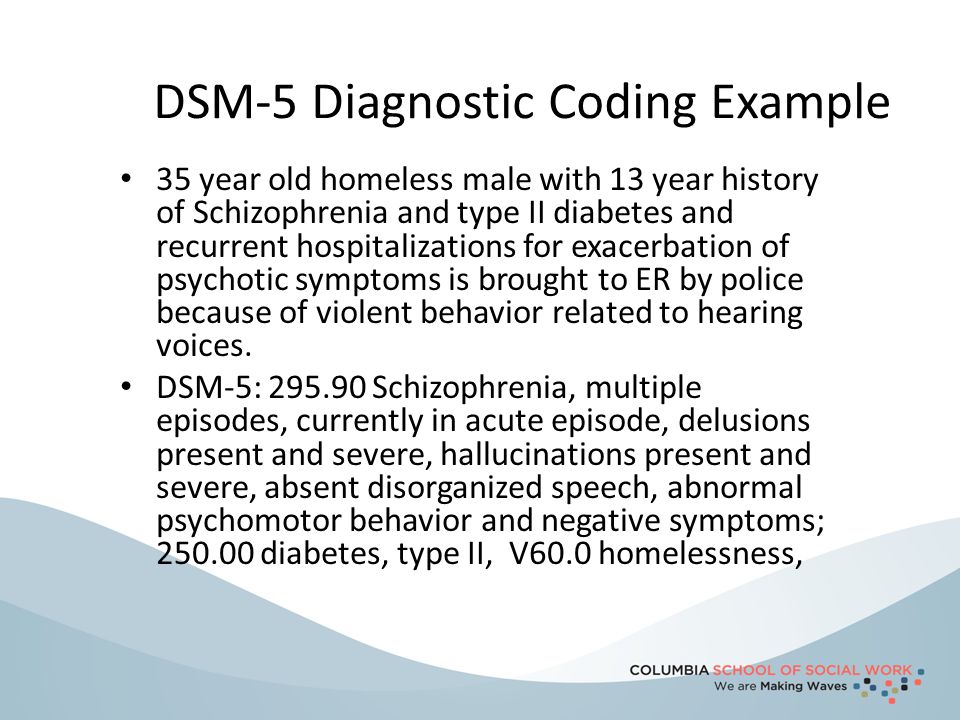 ru
ru
Read more
New solution
Bargain shopping
Moscow Startovaya, 1, building 6
+7 925 055-58-66
Shabanov73@mail. en
Read more
Atmosphere
Dental centers
Chernyakhovsky, 6
+74812515638
Read more
Men's club "Barsuk"
Night clubs
Tyumen, st. Krasina 7A
+7 (963) 067-67-67
Read more
Shop Ivanovskiy textile
Bedding / Home textiles
Dmitrovskoe highway, 169k1
+79645222575
Read more
Trading and manufacturing company EMITEKS
Building materials
Russia, Nizhny Novgorod, Shcherbakova, 37I
8-800-600-09-50
Read more
Emily Group
Construction Materials
Nizhny Novgorod, Soyuzny Prospekt, 13, apt. Read more
Read more
Emily Group
Construction Materials
Nizhny Novgorod, Soyuzny Prospekt, 13, apt. Read more
Emily Group
Construction materials
Nizhny Novgorod, Soyuzny Prospekt, 13, apt. Read more
CARDDEX
Safety and security systems
Russia, Oryol region, Orlovsky district, town Znamenka, st. Zarechnaya, 16a St. Petersburg,
8-800-333-93-36
Read more
Binar
Computer repair
Astrakhan,
88512666539
Read more
Contract manufacturing and assembly of AXIOMA electronics
Electronic components
Tolyatti, st. Communal, 39
+7(846)300-41-18
Read more
GoldikWhite
Jewelry
Moscow, Schelkovskoe highway, 90
89647016237
Read more
GoldikWhite
Jewelry
Moscow, Schelkovskoe highway, 90
89647016237
goldikwhite@gmail.