How to deal with manic bipolar spouse
You, Me & Bipolar Disorder Makes 3: Marriage Tips
In sickness and in health, right? Well, mania and maybe episodes of depression, too, are putting your vows to the test. With the right tools, you can cope with whatever comes your way.
You and your spouse may have knock-down, drag-out verbal matches. They might go from feeling sad to feeling elated; from wanting loads of sex to having none; from having fun times filled with energetic activities to being unable to take out the trash.
Maybe they talk your ear off at one point, yet don’t speak to you for days at other times. Or perhaps they go from saving money to wild spending sprees.
This is what a marriage to someone living with bipolar disorder can look like.
Or, with transparency, strong mutual intimacy, and having routines and a solid treatment plan, it could look like a smooth-running train: Yes, there are departures and arrivals, but you’ll both know the signs, act accordingly, and keep things moving forward.
Bipolar disorder, previously called manic depression, is a mental health condition known for sudden or intense changes in mood.
Someone with bipolar disorder may experience highs — mania or hypomania — that involve high energy, an increased sex drive, impulsivity, agitation, and even anger or irritability. Some people may also have lows, known as depressive episodes.
There are three types of bipolar disorder: bipolar I, bipolar II, and cyclothymic disorder. Each type comes with its own set of similar symptoms, patterns, and cycling phases. A diagnosis may also include features or additional specifiers to better describe your spouse’s condition.
What might bipolar disorder look like? In an episode of mania, your partner may drive too fast or recklessly, overspend, act out sexually, or even become emotionally or physically abusive. On the other end, in a depressive episode they may be too depressed to get out of bed, work, or just perform everyday tasks around the house.
A small study in 2019 found a significant increase in marital distress among partners of people with bipolar disorder, including issues like:
- family finances
- career or job decisions
- household tasks
The good news is that if your partner is diagnosed with bipolar disorder and moves forward with treatment, you can work together to make your marriage healthy and successful.
Since people with bipolar disorder may have different types, severity, and particular features, each person’s condition will be unique.
For example, an analysis in 2009 observed how someone’s symptoms and condition can change in type and the length of episodes as they age.
Educating yourself on bipolar disorder can help you learn what to expect from your relationship and your partner’s mood episodes.
Being in contact with your spouse’s healthcare team is also a great idea, according to Nicole Nina, a therapist in Aurora, Colorado.
If your partner agrees to include you as a contact on their medical release forms and share information access, it can:
- provide 2-way communication between you and their treatment team, in case of emergency
- help you know their particular diagnosis so you know what to expect in general
- keep you in the loop on their treatment plan, therapy, and medication routine so you can be an advocate in their journey
Sasha Jackson, therapist in Brooklyn, New York, says that psychoeducation is crucial to helping your marriage.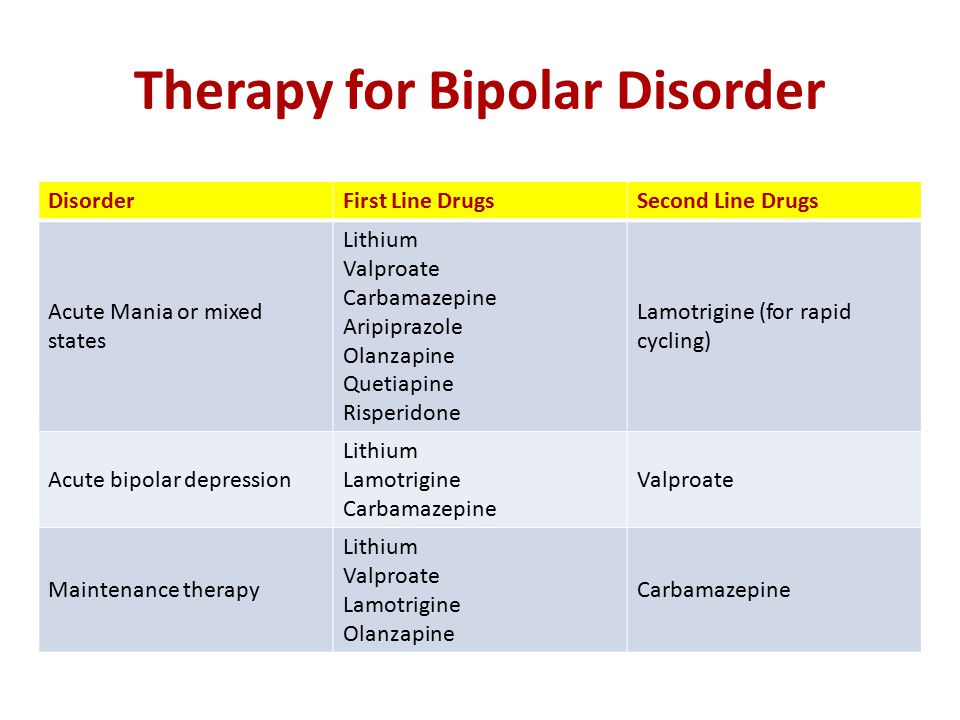
Other ways you can help your spouse, yourself, and your marriage
Make a plan together
As a spouse, you may be the most in tune with how symptoms occur in your loved one. “Over time, you will likely be able to pinpoint when your spouse is getting ready to enter either a cycle of mania or a cycle of depression,” says Nina.
You may not be able to stop the cycle, but you can develop plans to ride them out together.
For instance, you can have a plan in place to prevent your partner from making large purchases or engaging in harmful behaviors when they’re having a manic episode.
You can also weather depressive episodes by helping them get their tasks completed or giving them a pass on the garbage or yard work when you know they’re not up for it.
Even just having plans in place for when an episode comes on can give you a sense of control and help you prepare.
Talk about impulsive and reckless behaviors
Since impulsivity and reckless behaviors can be symptoms of bipolar disorder that affect marital life, addressing them openly when your partner is in a stable state — called euthymia (you-thigh-me-uh) — can make a difference.
“Create a plan with your partner to help reduce damage from behaviors,” says Jackson. An example would be agreeing to limit access to credit cards if they have a history of impulsive spending or gambling when experiencing mania or hypomania.
Likewise, agree to opt for the passenger seat or a rideshare, or reschedule a long road trip if they have trouble with speeding or reckless driving during mania.
Don’t take mood changes personally
“It’s difficult to not take your partner’s mood dysregulation (depression, irritability, anger, or [ill-timed] happiness) as a personal attack,” says Jackson. “However, mood swings are a symptom of bipolar disorder and have to do with a chemical imbalance.”
Even though it’s hard, instead of taking it personally, communicate with your partner about ways you can help them cope and ways you’d like them to try and communicate their needs so they can avoid escalations like raised voices, the silent treatment, or personal attacks.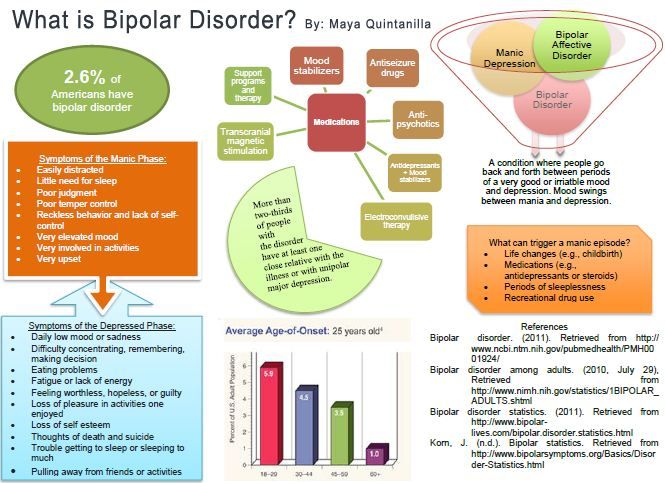
Ensure they have the resources they need
“Bipolar disorder is primarily managed through medication to stabilize the [mood],” says Nina.
If they ask you to hold them accountable, you can remind your partner to take their meds, keep their supply current, attend their therapy and medication appointments, and prioritize their health — eating right, exercising, and sleeping well. Lifestyle habits are known to help reduce severity of episodes.
Psychotherapy can also be a vital tool for managing the emotions that come with the condition.
Nina says helping your partner find the right therapist for them can ensure they have a trusted relationship with an objective party to help maintain and build on their progress.
Remember to enjoy time with each other
It’s easy to forget the pleasurable memories you’ve had with your spouse when managing health conditions takes so much of your time and energy. But it’s important to stay present, create space to enjoy each other’s company, have fun together, and continue to build your life.
“Every couple experiences highs and lows — spouses of those with bipolar disorder just get more heights and canyons to see,” says Nina.
Take care of yourself
Whether it’s a mental health or physical condition, taking care of a spouse, parent, or child can be taxing.
When supporting someone, you’ll want to have a self-care plan in place, where you put yourself first and make sure you get proper sleep, exercise, and downtime you need. Otherwise, you’ll burn out — or worse, feel resentful.
Choose activities that increase your energy and calm your emotions:
- Do an exercise you love like hiking, swimming, meditation.
- Find a hobby like reading or doing puzzles.
- Get away for me-time.
- Spend time in nature or with friends.
Ask for help when you need it
“Being in a relationship with someone who has bipolar disorder may be overwhelming at times,” says Nina. It’s OK — scratch that — vital to get an assist from online support groups, a therapist, or your spouse’s family if they’re privy to the diagnosis, whenever needed.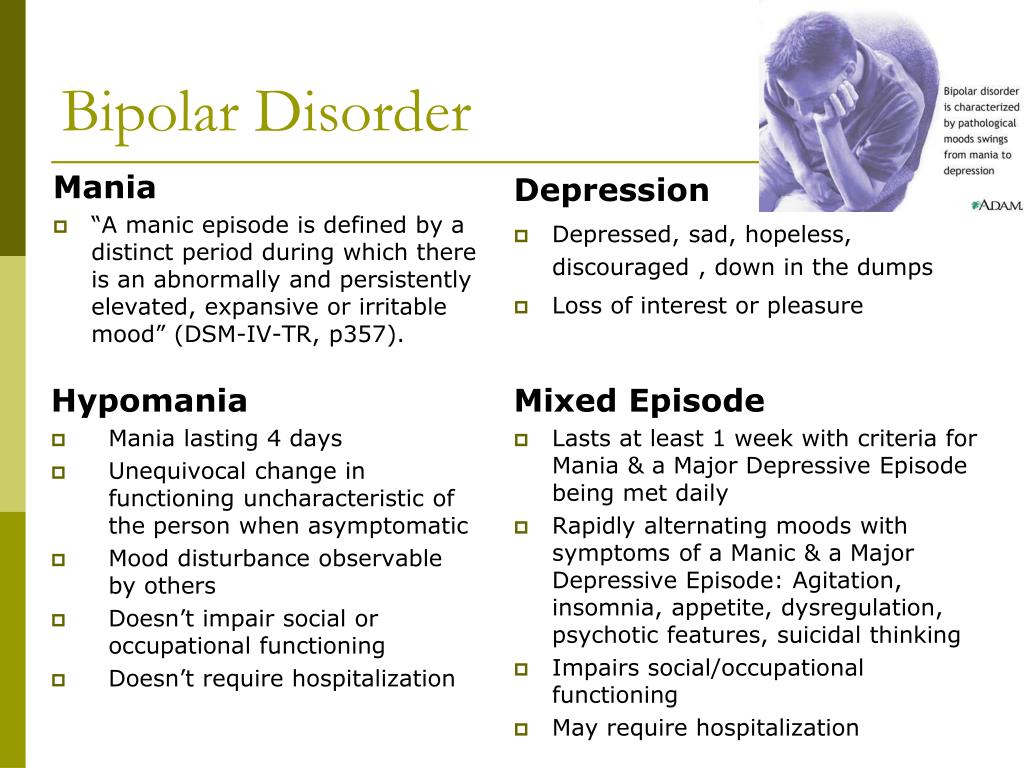
You may even consider marriage counseling to help you two meet the challenges and rise above them.
Marriage is less of a static institution and more of a living, breathing, organism: It grows healthy when we nourish and nurture it.
There may come a time when you need similar support, grace, and a proactive investment from your partner who’s also managing a chronic condition. Stay encouraged. A healthy bond is adaptable — physically, emotionally, and mentally.
10 Tips for Living with a Bipolar Spouse
If you’re married to someone living with bipolar disorder, you already know it’s a rough ride sometimes. The mood swings can make your days together sometimes exhilarating and other times frustrating. Yet you and your bipolar spouse can beat the dire statistics that predict the end of many of these marital unions.
New Orleans resident “Mary” has been married to her husband for 25 years. Almost halfway through their marriage, he was hospitalized at age 42 and received a diagnosis of bipolar disorder. The diagnosis was not surprising due to a strong family history — but it helped to clarify the situation, says Mary, age 51.
The diagnosis was not surprising due to a strong family history — but it helped to clarify the situation, says Mary, age 51.
“The diagnosis made it easier, because you know the reason, but it doesn’t change anything. It is a roller coaster. You can have months that are perfectly fine and then all of a sudden it will come from nowhere,” she says.
Mary says she knows the statistics showing higher rates of divorce and abuse in marriages that include one spouse with bipolar disorder. She describes her husband as a “rapid cycler” (“On a day to day basis you never know what it’s going to be,” she explains) and says there are many days and weeks when she is tired, frustrated, and wondering why she is still married. After so many years of marriage and successfully raising a daughter together, she has developed a philosophical and compassionate view of her husband and her relationship.
Coping with Bipolar Spouse Mood Swings
Here are some tips for surviving and thriving in your relationship:
Breathe. When things are tough, take a deep breath and step back. “It’s a disease — it’s not the person. So you try to remember that,” advises Mary.
When things are tough, take a deep breath and step back. “It’s a disease — it’s not the person. So you try to remember that,” advises Mary.
Build support. Caring for someone with a disease can keep you focused on his needs, but you also need your own sources of support. Joining a support group for family members of bipolar patients can help. Working with your own therapist may also be a good idea. Support from understanding family and friends is also invaluable. Mary has never joined a support group — and says she probably could have benefited from one — but she does find support in her friends.
Get away. Mary says part of what keeps her sane is her job, for which she occasionally travels. Despite the fact that her business trips often coincide with times when her husband stops taking his medications, she values her time away. At home, when her husband’s moods are out of control, Mary acknowledges, “I try to avoid him.”
Laugh. Whether you can insert humor into the situation and get a good response is highly individual, but Mary says this tactic works for her. “I try to make him laugh, to get him out of it,” she says.
Whether you can insert humor into the situation and get a good response is highly individual, but Mary says this tactic works for her. “I try to make him laugh, to get him out of it,” she says.
Enforce meds. Mary has made it clear to her husband that taking his medication is non-negotiable. “If you can keep them on the meds, you’re okay. It’s a fight. It’s like having another child,” she says. If he refuses to take his meds (as he often does when he is manic), she leaves, even if only to spend the night at a friend’s house to make her point. That usually gets him back on track.
Recall your love. There are hard times in marriage to a bipolar spouse, acknowledges Mary. But she prefers to see the man she fell in love with, even when his moods are unpredictable.
Know (or grow) your philosophy of marriage. Mary believes in the commitment she made when she married her husband. “You know, I married a man for better or for worse.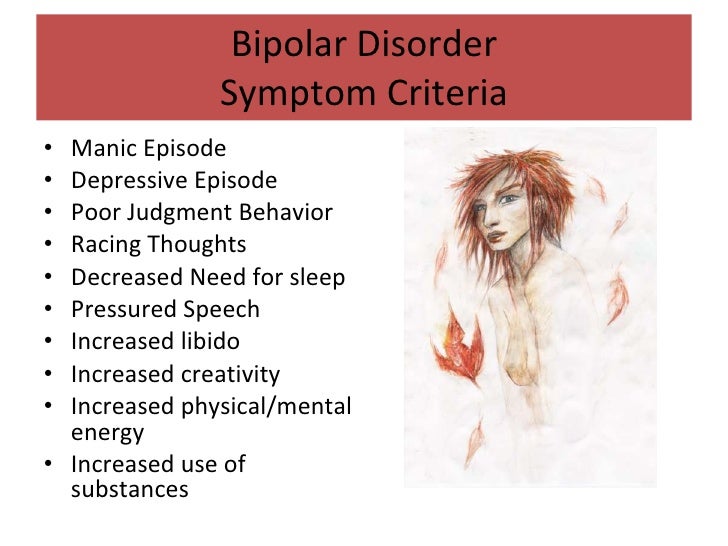 I did not marry a disease." While she acknowledges bipolar disorder is difficult, she also notes, "The person I fell in love with is still there. Would I want someone to leave me? I don’t think so,” she explains.
I did not marry a disease." While she acknowledges bipolar disorder is difficult, she also notes, "The person I fell in love with is still there. Would I want someone to leave me? I don’t think so,” she explains.
Look for triggers. “When your spouse is in a stable or more favorable mood, pay close attention to what environmental triggers precipitated and are maintaining the stability. Often there are specific environmental stressors or soothers — including relationship issues — that influence mood swings. Use the soothers to help maintain the mood that both of you are desiring,” advises marriage and family therapist Tracy Todd, PhD, based in Alexandria, Va.
Ask. Despite the mood swings, your spouse can tell you what he needs. “Have an honest discussion about what is helpful to your spouse when he is in an undesirable mood. Incorporate ideas, plans, and strategies so that there can be a minimization of harmful effects,” advises Todd.
Keep talking. There may be days and weeks when it is not easy, but communication is essential. “Communication during and between mood swings is critical to managing the accompanying stressors,” says Todd.
There may be days and weeks when it is not easy, but communication is essential. “Communication during and between mood swings is critical to managing the accompanying stressors,” says Todd.
Ultimately, Mary’s experience has given her a unique depth of compassion, both for family members whose loved ones have bipolar disorder and for people who live with bipolar disorder. “[I've said before] that I would hate to be in his head — I can’t even imagine how he feels,” she says.
People with bipolar disorder tell how to properly support them
March 30 is celebrated as Bipolar Day around the world. With this disease, it is important to monitor mood changes, which can be difficult to do alone. The founder of the Bipolar Association, Masha Pushkina, has collected stories of people who are helped by treatment partners.
At the initiative of public organizations bringing together scientists, doctors and activists, every year on March 30, World Bipolar Day is celebrated.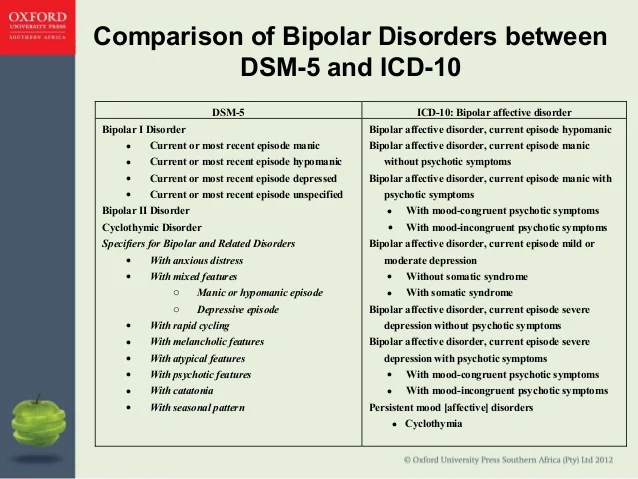 The date chosen was the birthday of Vincent van Gogh, an artist who, according to researchers, was the embodiment of a "bipolar genius." nine0003
The date chosen was the birthday of Vincent van Gogh, an artist who, according to researchers, was the embodiment of a "bipolar genius." nine0003
With bipolar disorder, a person lives either in a state of high emotional uplift and excitement (mania), or in depression. According to world statistics, about 2% of people suffer from bipolar disorder in various forms. This means that in Russia there are at least three million bipolar people - this is about half of St. Petersburg.
In most cases, this condition responds well to medication. But, unfortunately, many do not seek help or do not know how to find it. Without treatment, the disease progresses and ultimately leads to sad consequences: loss of family, job, disability in general, and in almost every seventh case, suicide. nine0003
These consequences can be avoided. The peculiarity of bipolar disorder is that the onset of remission depends not only on the doctor and medications, but also on the behavior of the patient himself.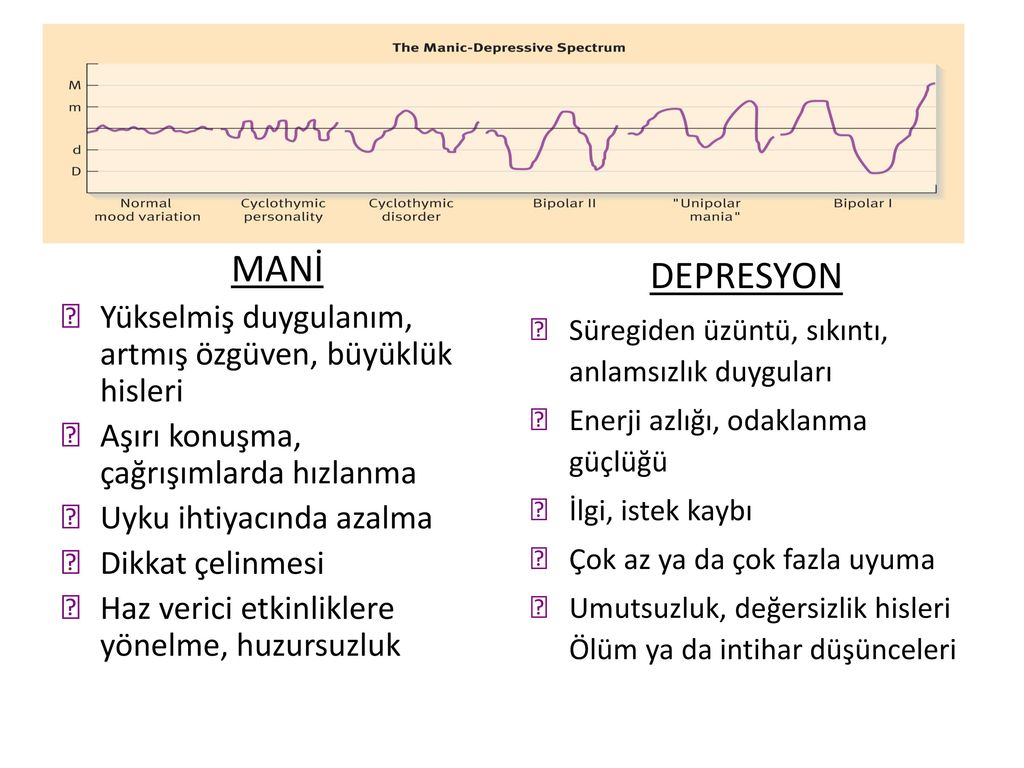 Very often, bipolar people provoke seizures "with their own hands." The mood of people with BAD (bipolar affective disorder. - Note ed. ) is very unstable, the balance is fragile, and mania or depression can be “started” in dozens of ways: the psyche is easily shaken by psychoactive substances, alcohol, lack of sleep, too intense work, travel and even love. So, a short time after the next course of treatment with powerful drugs, the person again ends up in the hospital. And each new attack reduces the chances of a long remission, affects social status, and even more painfully - self-esteem. nine0003
Very often, bipolar people provoke seizures "with their own hands." The mood of people with BAD (bipolar affective disorder. - Note ed. ) is very unstable, the balance is fragile, and mania or depression can be “started” in dozens of ways: the psyche is easily shaken by psychoactive substances, alcohol, lack of sleep, too intense work, travel and even love. So, a short time after the next course of treatment with powerful drugs, the person again ends up in the hospital. And each new attack reduces the chances of a long remission, affects social status, and even more painfully - self-esteem. nine0003
The experience of people with mental disorders around the world has proven that you are much more likely to cope with difficulties when you are supported by people who understand your problems and condition, but do not look at you as a patient. As practice shows, such a person can be not only a partner or close relative. An old friend, and even a person with whom you have never met in person, can help you get through the darkest times. Masha Pushkina, especially for Afisha Daily, spoke with several bipolar people about those in whom they found their support. The result is a story not about illness, but about friendship and trust, which can defeat even madness. nine0003
Masha Pushkina, especially for Afisha Daily, spoke with several bipolar people about those in whom they found their support. The result is a story not about illness, but about friendship and trust, which can defeat even madness. nine0003
Yana, 31 years old
Housewife, collects books and is fond of confectionery
Purposefully, I didn't find out about the ways of support anywhere, everything turned out quite naturally. I have been sick for 15 years. The first person who looked after me was my best friend, and now it's my husband.
When my hypomania (a mild degree of mania, which is characterized by a constantly high mood. - Approx. ed. ) accelerated into a full-fledged mania (this state is also characterized by a one-sided attraction to some topic, sometimes accompanied by delirium. - Note ed. ), it became clear that I needed to be looked after. A friend began to pay attention to repetitive patterns of behavior in one phase or another, and we decided together to find out what helps in such cases.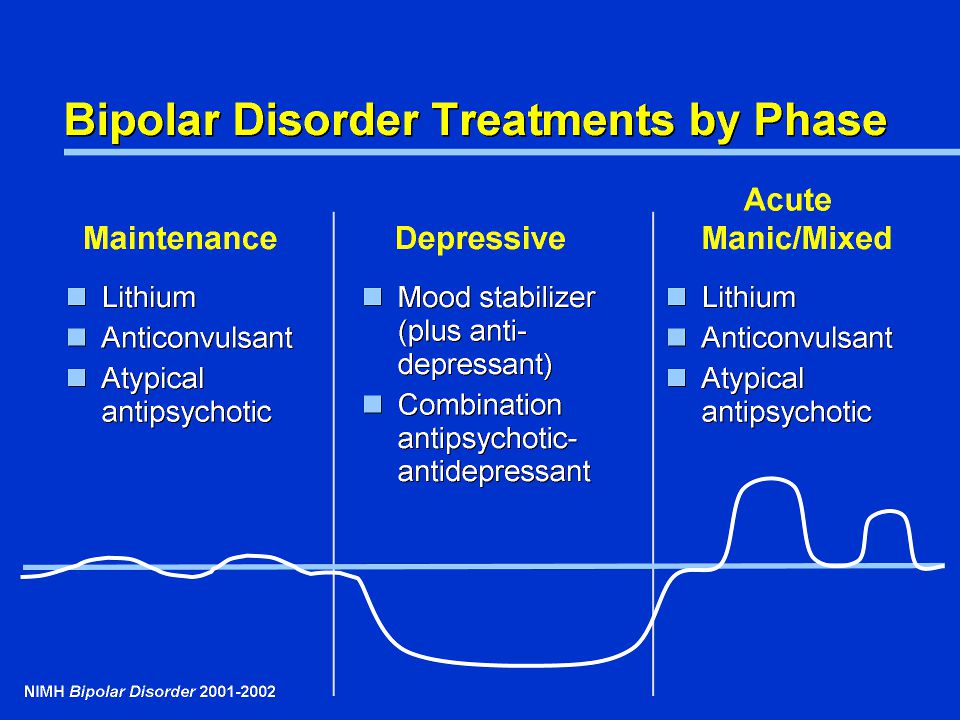 I think my friend was afraid to take responsibility for my condition, but she turned out to be generous and selfless. When I got married, a friend passed this knowledge on to her husband, and he already supplemented it, based on his own experience. The husband initially knew with whom he connects his life. He says it didn't scare him. nine0003
I think my friend was afraid to take responsibility for my condition, but she turned out to be generous and selfless. When I got married, a friend passed this knowledge on to her husband, and he already supplemented it, based on his own experience. The husband initially knew with whom he connects his life. He says it didn't scare him. nine0003
I have obsessions during my manic episodes. My husband does not argue with me at this time, but he also does not feed them, trying to redirect my stormy energy in a different direction. You can’t argue, because the result will be the opposite: I will finally get stuck on the idea, I will consider that I must prove it at all costs, even if the whole world is against me, and there are enemies and conspiracies around. If this does not help, the husband agrees to discuss all these things, but at the same time tries to slow down their implementation by offering to draw up a specific and detailed plan. Sometimes it takes me a long time. nine0003
For example, I always want to move somewhere. Right now, and why aren't we packing our things yet? My husband tries to make me write down what are the pros and cons of different cities, what attracts us to them. As a result, I sit for hours on different forums, make lists, think about how we will arrange our life, calculate the budget for different countries of the world. There is also a manic passion for travel, but after preparation, we usually implement these plans. And many years ago, in a fit of mania, I bought an apartment - with a mortgage, with hellish payments. Then it took a long time to resolve this situation, but, fortunately, everything worked out well. nine0003
Right now, and why aren't we packing our things yet? My husband tries to make me write down what are the pros and cons of different cities, what attracts us to them. As a result, I sit for hours on different forums, make lists, think about how we will arrange our life, calculate the budget for different countries of the world. There is also a manic passion for travel, but after preparation, we usually implement these plans. And many years ago, in a fit of mania, I bought an apartment - with a mortgage, with hellish payments. Then it took a long time to resolve this situation, but, fortunately, everything worked out well. nine0003
My husband began to chart my mood. I also manage it, and we check the results so that they are objective. Quarrels due to the fact that the husband takes on the role of the elder often arise in the manic phase (never in depression). Then I become very suspicious, any attempts at control cause rage. But now the husband has learned from experience, so he does not react to attempts to unleash a conflict. With obvious attacks of rage and auto-aggression, he uses holding therapy (long strong hugs. - Note ed. ). We have seen this in autistic children, this is how their parents influence them.
With obvious attacks of rage and auto-aggression, he uses holding therapy (long strong hugs. - Note ed. ). We have seen this in autistic children, this is how their parents influence them.
When I'm depressed, he doesn't comfort me because it's pointless, but he tries to give reasonable arguments that this period has always ended and this time will also pass soon. We look at mood charts for the past months, discuss the duration of the attacks: two weeks have already passed and, judging by past experience, it should get better in a couple of weeks.
Such support from the husband helps in many ways. When I was being treated by two doctors, taking all the medicines, I didn’t have such support, everything was very bad. Over time, I stopped disappearing from home in a manic state and inflicting serious injuries on myself. All my super-ideas remain on paper in the form of graphs and tables, I don’t even have time to start putting them into practice, so that later I don’t have to deal with the consequences with the whole family. nine0003
nine0003
Alisa, 27 years old
Biologist
To be honest, I don't always find understanding from my healthy environment, I often faced condemnation, devaluation of problems. But from a person who has a similar experience, you won’t hear “don’t invent”, “you can’t feel so bad”, “take a walk and it will pass”.
It just so happens that my best friend also suffers from bipolar disorder. I did not look for support in specialized communities where patients communicate, we met by chance. My friend is much older, he has much more life experience, and he was able to become a real mentor for me. Not once did his actions worsen my condition - I hope that he can say the same about me. nine0003
When I'm on the rise, I feel uncomfortable when he tries to slow me down and reduce my passions. But as soon as this state passes and I again take a sober look at the situation, each time I thank him for trying to stop the revelry and disgrace. My friend himself is currently not being treated, but he never imposed his position on me, and when I turn to doctors, he supports me in this.
I told the doctor about this source of support - he is all for it. Before meeting a friend, I had suicidal attempts, but during the entire time of our communication I never tried to say goodbye to life. When you know that there is a person who will understand everything and share warmth (while even my own family repels me), that there is a place where you can come in any condition and where they will accept me without unnecessary questions and teachings, this is a source of great strength. and hope. nine0003
When I was expecting my second child, I was depressed. My husband did not yet fully understand the features of the disease and did not want to admit obvious things - this added problems, and my emotional state became extremely difficult. It seems that only thanks to the participation of my friend, I did not do anything to myself and successfully endured the pregnancy. The child was named after him.
Sergey, 49 years old
Freelancer
At the height of the depression, I was looking for any available support and ended up in an online group of anonymous debtors (people who have taken on large loans). One of the participants drew attention to my condition and said that I urgently need medical help. Despite the fact that she lives in the USA, we began to communicate regularly via Skype. Olga literally brought me to the hospital and helped me prepare for the treatment. nine0003
One of the participants drew attention to my condition and said that I urgently need medical help. Despite the fact that she lives in the USA, we began to communicate regularly via Skype. Olga literally brought me to the hospital and helped me prepare for the treatment. nine0003
Americans are a pragmatic people, many young and healthy people have folders with wills and instructions in case of their death. They also approach mental difficulties calmly and thoroughly. It is common practice for the patient to draw up detailed instructions in advance. In the United States, there is a practice of issuing Treatment Agreements for people with mental illness (Treatment Contract). This document is needed so that family, friends and doctors recognize the symptoms of deterioration in time and take into account your experience and wishes in the treatment. Typically, such a document contains: a list of trusted people; signs of a normal state; signs of an approaching episode; symptoms of mania and depression; actions that trusted people should take to help a person get better and keep him from destructive acts; plan of action in case of an emergency (for example, a suicide attempt). who and what will be done in case of his hospitalization, so that he can be treated without anxiety for household chores. nine0003
who and what will be done in case of his hospitalization, so that he can be treated without anxiety for household chores. nine0003
In a period of severe depression, there is a struggle inside a person between the craving for death and the desire to live - and many external things can outweigh in one direction or another. Every clue is important to help you get out. It is very difficult for one to cope with all this.
I madly didn’t want to go to the hospital and wouldn’t have made up my mind myself, until the last I hoped that somehow everything would go away on its own. But under the supervision of a friend, I drew up a preparation plan: warn the customer at work, arrange to look after my cats. Reported to her about every step. But then he could no longer simply “escape” [from hospitalization], because he felt obliged to both her and the doctor. During depression, one's own life has no value, but the people dear to me, the promises made to them, do. nine0003
At the most difficult moment, Olga became my “outer brain”, which told me what to do when I didn’t understand anything myself. After I was discharged from the hospital, I turned to four friends for support. Usually we call each other once a week, I tell what my condition is. It is important not only to chat online, but also to hear the voice, you can understand a lot from it. Friends immediately pay attention, if I suddenly disappear and stop calling, then something is wrong.
After I was discharged from the hospital, I turned to four friends for support. Usually we call each other once a week, I tell what my condition is. It is important not only to chat online, but also to hear the voice, you can understand a lot from it. Friends immediately pay attention, if I suddenly disappear and stop calling, then something is wrong.
I think it is possible to find such a person if you set yourself such a goal. Take a closer look at people in support groups, religious or other communities - those who understand what compassion and mutual assistance are. This must be an internally mature person, ready to take responsibility for you in a difficult situation. If this person has similar problems, then he will better understand your experiences. For this reason, relatives are far from always suitable: they themselves can panic, seeing how bad you feel, choke you with their anxiety, overprotection. nine0003
It is necessary to establish the frequency of communication and observe it. And of course, in no case should you parasitize on someone else's kindness. The support system works when you yourself take responsibility for your life, and do not outweigh it completely on another.
And of course, in no case should you parasitize on someone else's kindness. The support system works when you yourself take responsibility for your life, and do not outweigh it completely on another.
Anna and Valeriya, 21 years old
Students
Anna: After a major depressive episode four years ago that almost ended in a suicide attempt, I started looking for information on [support]. I managed to find a guide in English for relatives and friends on how to behave with such a person. I have sent this list to all my friends so that they have an idea of what is happening to me. For the past few years, Lera has been monitoring my emotional state on a daily basis, and if, in her opinion, it goes beyond the norm, she tells me about it. Lera just asks every day how I'm doing, and if she sees that I'm reacting strangely, she wonders if something happened. At first, it was very difficult, because, in principle, I did not like to regularly share personal experiences. But by regularly receiving feedback, I can imagine the dynamics: do the pills help, how long do the side effects last, does the depressive phase go into a moderate and severe degree, do I lose my critical thinking during hypomania. nine0003
But by regularly receiving feedback, I can imagine the dynamics: do the pills help, how long do the side effects last, does the depressive phase go into a moderate and severe degree, do I lose my critical thinking during hypomania. nine0003
Valeria: We gradually established a very trusting relationship. Anya studied the topic of bipolar disorder up and down, and I read the articles that she sent me. The diagnosis did not change anything for me, because it remained the same. After that, we already discussed some formalities (for example, who to call in case of an emergency).
Anna: I asked Lera to watch for hypomanic manifestations in which I lose an adequate assessment of my actions: impulsive night walks, alcohol begin. nine0003
Valeria: My friend is a very responsible and conscious girl who takes care of herself, her health and her wallet. Before buying something expensive, she asks for my advice - and then we are already sorting out the situation.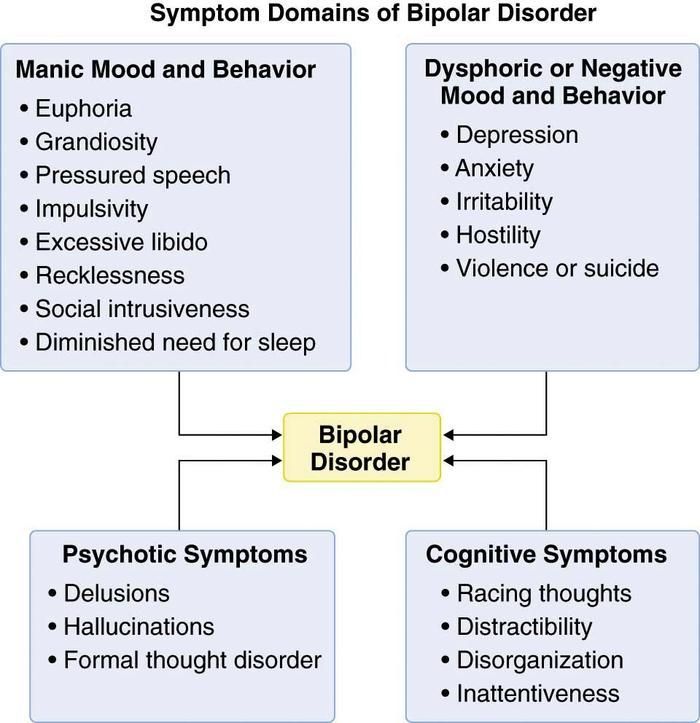 We can entrust accounts to each other and not worry. I also know where and to whom to run in cases of exacerbation.
We can entrust accounts to each other and not worry. I also know where and to whom to run in cases of exacerbation.
Anna: I react badly to prohibitions and reminders of illness. Yes, I periodically have to turn to relatives for help, change treatment or take long breaks, but I expect mutual respect so that they don’t look at me through the prism of the disease. nine0095 When the mood is unstable, harsh phrases like “the disease speaks in you”, “these are not your real emotions” cause persistent rejection, even when they are true. The line between accepting a loved one's illness and identifying him with a diagnosis for healthy people is extremely thin. Therefore, those who were able to grope it deserve great respect.
Anna: In the last year, I go to see the doctor with my parents. When the doctor notices that I may not be able to do it alone, she duplicates the instructions and advice for them. I, in turn, am a friend. The doctor has repeatedly emphasized that the change of episodes is more noticeable from the outside.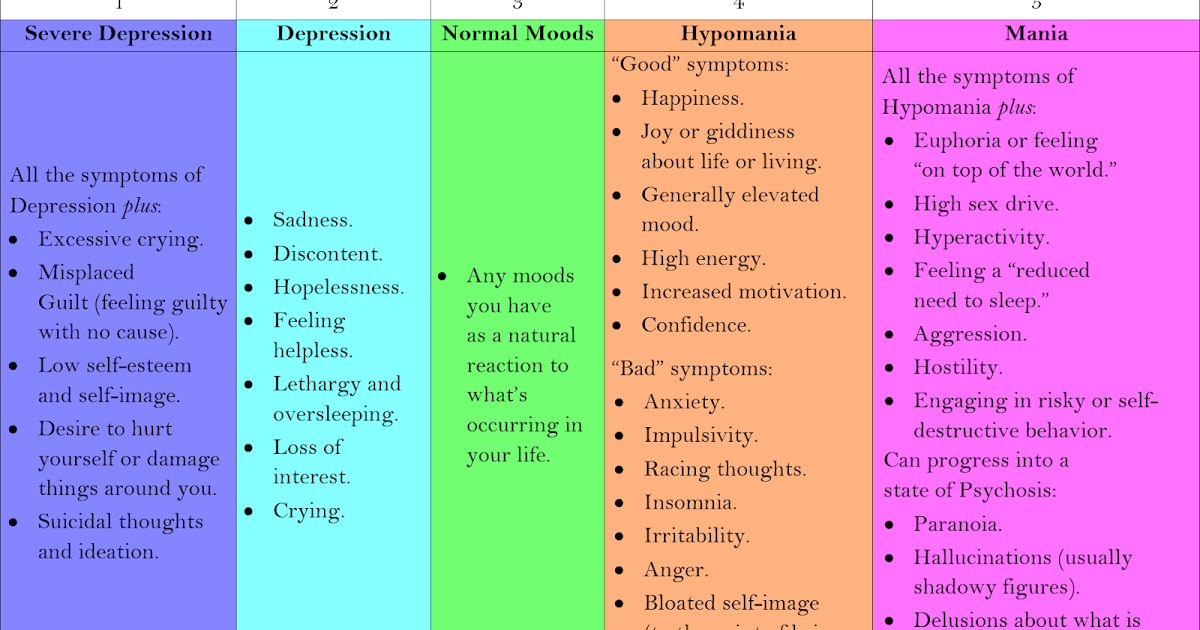 nine0003
nine0003
Valeria: We don't have any kind of hierarchy in relationships, so there is no pressure when one makes decisions for another. This is not eating each other's emotional resources, but complementing and supporting.
Anna: The main danger in a relationship with a person with a serious illness is to fall into codependency. This format is equally bad for both the "controller" and the "subordinate". Unfortunately, I have been in such relationships before. It is worth maintaining mutual respect and treating each other as equals. Illness should not dominate a relationship. In difficult episodes, it temporarily comes to the fore, but you should always remember that you are not a disease. nine0003
Anna: I have memory problems: I don't remember some episodes. In such cases, I can ask Lera for help. If you remember the last weeks, then these are regular reminders to call the doctor. In mixed episodes, this becomes an acute problem, because I can suddenly change my mind or forget. Against the backdrop of a severe episode, I may develop psychosis, and this is the most dangerous thing in the disease. Thanks to our format, I manage to avoid such exacerbations almost always.
Against the backdrop of a severe episode, I may develop psychosis, and this is the most dangerous thing in the disease. Thanks to our format, I manage to avoid such exacerbations almost always.
The advantages of observation from a loved one are an early response and the fact that he knows the patient's usual behavior very well and can notice even small changes. The main disadvantage is that normal friendly communication risks turning into constant monitoring of symptoms. Not every mentally healthy person is able to remain within the boundaries of reason. nine0003
It is important to agree in advance, before an attack, what is an undoubted sign of a worsening condition (for example, persistent insomnia), and what you do not need to pay special attention to (for example, loud indignation at something that you do not like). In a difficult situation, often a loved one begins to behave not as an equal, but as a “healthy” and “knowledgeable”. Not all relationships stand this test.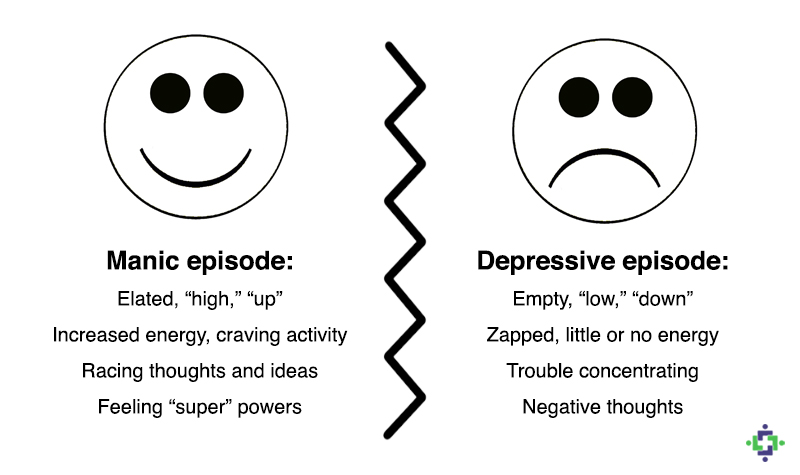
There is also a variant of "buddy" (when two people with mental disorders look after each other. - Note ed. ) - it is good precisely because it is the true request of the patient and more equal relations without mixing roles. But I don't know the buddy support system.
To choose a person you can rely on in a critical situation, take a closer look at your surroundings. Above all, a high level of trust is needed. Your assistant should be open to nonjudgmental and open dialogue and at the same time emotionally stable and resistant to stress.
Support is essential for every person - very often we as mental health professionals need it. And with bipolar disorder, this problem is especially acute. At the initial stages, those closest to you often ignore the presence of the disease, and friends advise you to either "pull yourself together" or, conversely, "relax", sometimes with the help of alcohol. When it becomes obvious to everyone that the “condition” will not go away on its own, urgent hospitalization is already required.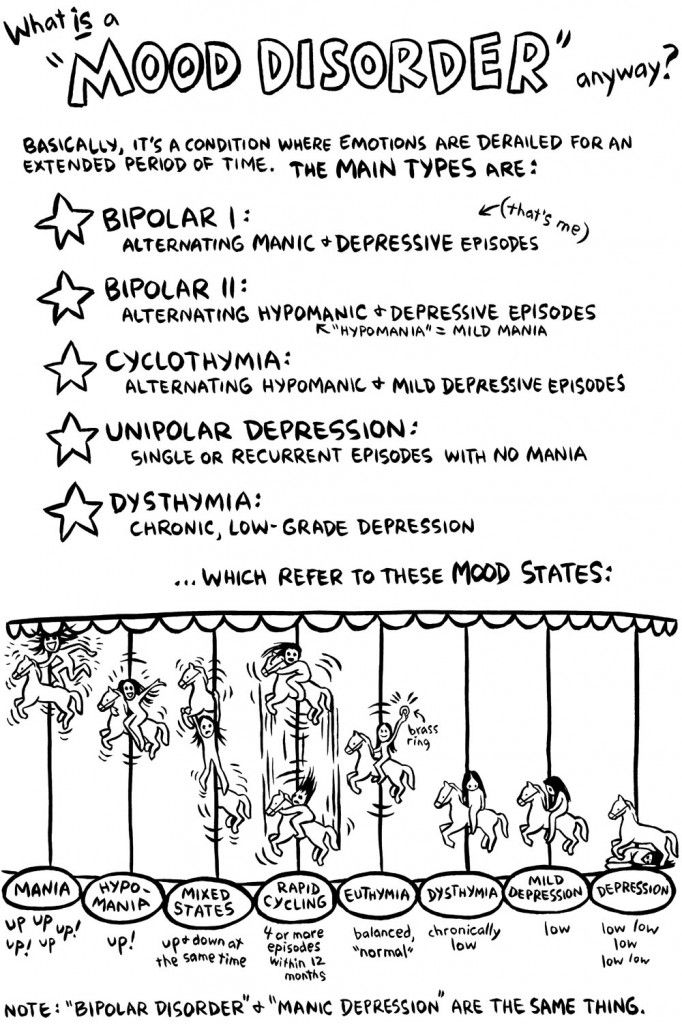 The saved patient receives the "stigma". nine0003
The saved patient receives the "stigma". nine0003
Psychiatrists then make it the responsibility of the uninitiated next of kin (parent or spouse) to monitor any changes in the patient, and they really try to do so. At the level of "laughing out loud - hypomania has begun, upset - depression." As a result, psychiatrists begin to treat quite normal human emotions based on complaints from relatives... and the circle closes.
For this to change, mental health literacy must play a major role. Relatives, in order to be able to help, need to understand well what is happening with a loved one. In many, including state clinics, groups for training relatives either already exist or are being created. nine0003
The support of loved ones in case of emergency is especially important. In deep depression or mania, a person is not able to independently control his behavior, this decision is made by relatives, sometimes without his consent. In the case of bipolar disorder, this should be the last option when all others have been exhausted.
symptoms of bipolar disorder, how it proceeds, how to find a psychiatrist, diagnosis and treatment
Victoria K.
lives with bipolar disorder
The first signs of the disease appeared in my teenage years, and the psychiatrist diagnosed BAD at the age of 26. nine0003
According to WHO, 45 million people worldwide suffer from bipolar disorder. This disease greatly reduces the quality of life: in some periods you are overly energetic and do things that you can regret, in other periods you are not able to get off the couch to do everyday things.
I will tell you how I have BAD and what I do to cope with the disorder and live like all ordinary people.
Go see a doctor
Our articles are written with love for evidence-based medicine. We refer to authoritative sources and go to doctors with a good reputation for comments. But remember: the responsibility for your health lies with you and your doctor. We don't write prescriptions, we make recommendations. Relying on our point of view or not is up to you. nine0003
Relying on our point of view or not is up to you. nine0003
What is Bipolar Affective Disorder?
Bipolar Affective Disorder, or BAD, is a mental disorder with alternating emotional ups and downs in mood. It is affective just because it is associated with violations of the emotional state, that is, mood - in psychiatry, the manifestation and experience of emotions is called affect. Previously, this disease was called manic-depressive psychosis.
Bipolar Disorders - A Physician's Handbook MSD
Why BAD develops is not exactly known. Among the reasons are heredity, traumatic events, violations of the production of neurotransmitters - substances due to which signals are transmitted between brain neurons. The disease often manifests itself in adolescence or in the period between 20 and 30 years.
How Bipolar Disorder Manifests
BAD usually begins abruptly, followed by periods without signs of illness and periods of exacerbations. The peculiarity of the disease is that during periods of exacerbations there are episodes, or phases, with different emotional states that can replace each other in an arbitrary order. nine0003
nine0003
Bipolar Disorder - Mayo Clinic Blog Article
For example, when the illness escalates, the following conditions may occur.
Mania - a state of elevated or irritable mood. The person feels energetic, actively engaged in something, such as finding a new hobby or even trying to open a business. As a rule, he sleeps little, is self-confident, talkative, he has a lot of ideas, often crazy. Risk sensitivity may decrease - for example, a person invests all the money in a hopeless business or gets into a loan. Hobbies for gambling, extreme sports are not uncommon. At the same time, a person feels great, but often cannot concentrate on one thing, work productively. nine0003
The extreme degree of mania is manic psychosis, when delusions of persecution, hallucinations, excessive activity develop, a person can become dangerous to himself or others.
Hypomania is a kind of mild mania. A person is in a state of emotional uplift, but this uplift is not so pronounced. However, the mood still improves, the need for sleep decreases, the person is creative, relaxed, feels euphoric, and his productivity increases. Although in some people such periods may be accompanied by irritability and a decrease in concentration. nine0003
However, the mood still improves, the need for sleep decreases, the person is creative, relaxed, feels euphoric, and his productivity increases. Although in some people such periods may be accompanied by irritability and a decrease in concentration. nine0003
Depression - low mood, loss of interest in life, fatigue, guilt, indecision, decreased concentration. Sleep and appetite disturbances may occur. Sometimes there are thoughts of suicide, the futility of one's own life.
/bye-depression/
“It reminded me of a strict regime sanatorium”: how much I spent on treating depression
Between exacerbations, a person can return to normal, although it happens that his performance is still reduced. nine0003
Manifestations of the phases of bipolar disorder, according to the National Institute of Mental Health USA
| Parameter | Mania | Depression |
|---|---|---|
| Mood | Excitement, joy, irritability, resentment | Sadness, depression, emptiness, anxiety, hopelessness |
| Sleep | Reduced need for sleep | Trouble falling asleep, getting up early or sleeping too much |
| Appetite | Loss of appetite | Often increased appetite, weight gain |
| Communication | Talkativeness | Slow speech, forgetfulness |
| Concentration | Sensation of jumping thoughts, multitasking | Problems with attention and decision making, distraction |
| Behavior | Risk appetite, runaway spending, promiscuous sex | Lack of pleasure and interest in anything, decreased libido |
| Subjective feelings | Feeling of self-importance, talent and power | Feelings of worthlessness, suicidal thoughts, suicide attempts |
Mood
Excitement, joy, irritability, resentment
Sleep
Decreased need for sleep
Appetite
Loss of appetite
Communication
Talking
Concentration
The feeling of jumping of thoughts, multitasking
behavior
Risk, unbridled sex
Subjective sensations
Feeling and power
9000 Depression 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 MoodSadness, depression, emptiness, anxiety, hopelessness
Sleep
Trouble falling asleep, getting up early or sleeping too much
Appetite
often increased appetite, weight gain
Communication
Slow speech, forgetfulness
Concentration
Problems with attention and making decisions, Dispersibility
behavior
Lack of pleasure and interest in something, decrease in libido
Subjective feelings
Feelings of worthlessness, suicidal thoughts, suicide attempts
There are two main types of bipolar disorder according to how the disease manifests itself:
- When there has been at least one manic episode and depressive episodes recur.
- When there are periods of depression and at least one episode of hypomania, but without full mania.
Bipolar Disorder - National Institute of Mental Health USA
I just have bipolar affective disorder type 2. This means that there are no full-fledged manias, but there are hypomanias and severe depressions.
Hypomania is a very cool time for me. You can do everything: get a second degree, run a marathon, learn English, go on an unplanned trip. And so for several months during which you do not sleep, do not eat, acquire new friends, start novels, end old relationships. You feel all sensations in the maximum range. During the day, it can throw several times from tears and the desire to die to incredible happiness. nine0003 This is what mania looks like in BAD. Source: Twitter
After hypomania comes depression. And immediately there is not enough strength not only for what was started during the previous phase, but also for ordinary things. The most understandable image of depression for me is “pressed down by a concrete slab.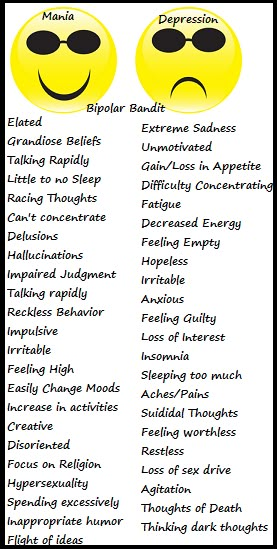 ” It becomes hard to do the simplest things: wash the dishes, change clothes, go to the store.
” It becomes hard to do the simplest things: wash the dishes, change clothes, go to the store.
Unfortunately, the brighter the hypomania goes, the worse the depression gets later — that's why, with experience, I stopped enjoying the active phase. nine0333 Now it's even more difficult for me: I understand what is happening with my brain, but I can't control it.
As I remember now, my first hypomania happened at the age of 12. Then there were periods of exacerbations clearly in a year and a half: hypomania lasts 2-3 months, usually May - July, depression - 5-6 months, usually in October - March, in between remission occurs when I feel normal. If I am in a long-term remission, then I hardly notice phase changes: mood swings are smoothed out with the help of medications or psychotherapy. nine0003
10 podcasts about health and medicine
The usual course of bipolar affective disorder
Viktor Lebedev
psychiatrist, science journalist
During an exacerbation of bipolar disorder, episodes of mania or hypomania and depression may alternate.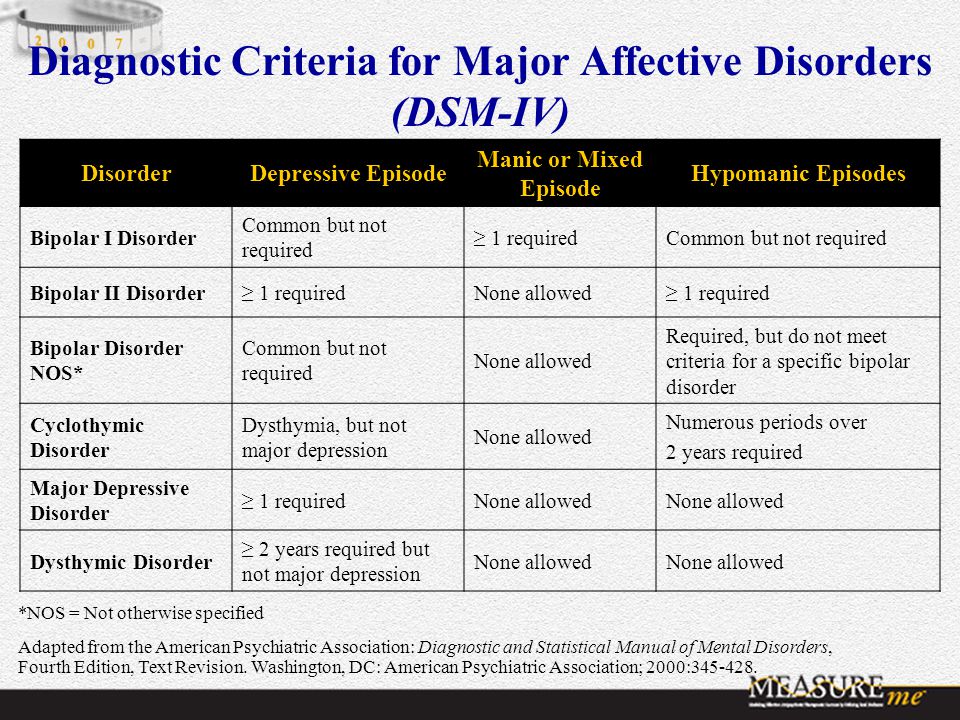 There is a clear separation of phases: first a hypomanic or manic episode, then a depressive episode, it happens that there are recurring episodes of depression, then hypomania. In the latter case, hypomanic phases are sometimes not noticed, a person may be diagnosed with recurrent, that is, recurring depression, and may be prescribed the wrong treatment. nine0003
There is a clear separation of phases: first a hypomanic or manic episode, then a depressive episode, it happens that there are recurring episodes of depression, then hypomania. In the latter case, hypomanic phases are sometimes not noticed, a person may be diagnosed with recurrent, that is, recurring depression, and may be prescribed the wrong treatment. nine0003
In fact, in BAD, the phases can alternate in any order, the diagnosis is made if there is any combination of manic and depressive episodes. The first time the disease usually begins with an episode of mania or hypomania, which develops into depression. Less commonly, it starts with depression, then mania or hypomania occurs. But in any case, there must be affective disturbances, that is, mood disturbances.
The exacerbation of the disease lasts from several weeks to several months. This also depends on whether the person is receiving medical treatment. If you respond quickly to an exacerbation, you can sometimes return to normal health in a week. If not treated, the exacerbation can last for several months - especially the depressive phases, episodes of hypomania and mania usually pass faster. nine0003
If not treated, the exacerbation can last for several months - especially the depressive phases, episodes of hypomania and mania usually pass faster. nine0003
Seasonality of phases, when there is a connection between the manifestations of the disease and the change of seasons, occurs, but not all patients with bipolar disorder notice it.
How I suspected I had BAD
The first time I thought I was going crazy was when I was 18 years old. Painful relationships ended, obsessive thoughts and images swirled in my head, I listened to the same song in the player, walked for hours and could not stop. This went on for so long and was so unbearable that I almost decided to go to a psychiatrist. However, they didn’t talk about mental disorders then, so I didn’t even know where to turn. Then this state passed by itself. nine0003
I did not see a psychiatrist until seven years later, when I again had a similar severe condition: obsessive thoughts, inability to control emotions, self-harm, sleep and appetite disturbances. Before that, I had three episodes of hypomania every two years, but after them there was no severe depression, and therefore no reason to seek help.
Before that, I had three episodes of hypomania every two years, but after them there was no severe depression, and therefore no reason to seek help.
Then I just went to the district polyclinic - it turned out that a psychotherapist was there. She checked my symptoms on the Beck scale, diagnosed me with an anxiety-depressive disorder, and prescribed a common antidepressant that is often prescribed for depression. nine0003
Beck Depression Scale - online test
It seemed to me that antidepressants helped me immediately: my mood improved, I got energy, I talked a lot with friends, hung out, worked. Now I know this is a bad sign. Antidepressants usually take a long time to work: it takes about three weeks for the effect to appear, and I got better after a few days. In addition, in bipolar affective disorder, antidepressants can cause hypomania if not mitigated by other drugs. nine0003 This meme is well understood by those who were not immediately given the correct diagnosis. If you add Mentos to Coca-Cola, you get a foamy fountain that will splash out of the bottle. Antidepressants, in particular SSRIs - selective serotonin reuptake inhibitors - have the same effect on the mood of people with BAD
If you add Mentos to Coca-Cola, you get a foamy fountain that will splash out of the bottle. Antidepressants, in particular SSRIs - selective serotonin reuptake inhibitors - have the same effect on the mood of people with BAD
I went to this psychotherapist several more times, but she did not track my sharp mood swings, and I had one of the most severe hypomanias . I drank and smoked a lot, I had incredible emotional swings, I ruined my relationship with my best friend, I stopped eating and sleeping. nine0003
After a couple of months, my condition stabilized a little, but I continued to take antidepressants: I knew that they should not be stopped abruptly. Before canceling, I went for a consultation with another doctor, already at a paid clinic. She turned out to be a good specialist: she asked questions about mood swings, found out if I had previously had mood swings, ups and downs, depressions. Then everything was fine because of taking antidepressants, so I denied everything.
A year later, as the doctor ordered, I smoothly stopped taking antidepressants, and a few months later I was overcome by one of the most severe depressions. If last time I could attribute depression to circumstances - burnout, relationship difficulties, fatigue - now there was no reason for it. I had a job I loved, a great relationship with my husband, financial stability, a new city. And I wanted to die. nine0003
/psychotherapy-search/
How to choose a psychotherapist
This moment became a turning point in the diagnosis. I already knew that there is such a disease as bipolar affective disorder, what are its symptoms and features. Information about BAR appeared in the media field: I read articles and blog posts, watched videos on YouTube.
I was able to describe the last 10 years of my life in phases: there was a strong rise, followed by a decline. For example, in the hypomania of 2012, I worked two jobs, passed the state exams, wrote a diploma, hung out with friends until the middle of the night and completely took care of the life of the family.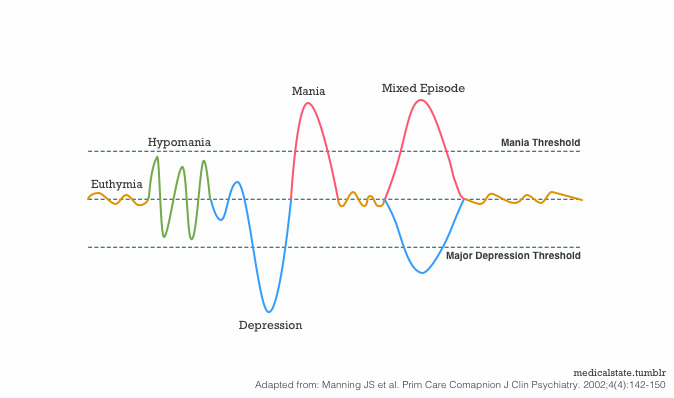 In hypomania in 2014, she entered the magistracy, graduated from a driving school, traveled, and also ran a marathon. nine0003
In hypomania in 2014, she entered the magistracy, graduated from a driving school, traveled, and also ran a marathon. nine0003
Every upswing was followed by a downturn: I stopped running, didn't pass the exam in the traffic police, and dropped out of the master's program. Each such exacerbation generally lasts a year and a half, and then repeats.
How I searched for a suitable psychiatrist
After collecting information about BAD, I decided to find a psychiatrist to confirm or deny my diagnosis. It didn't happen right away.
First I went to a psychiatrist on the advice of a friend, he helped her with depression. The doctor saw me in a paid clinic, the appointment cost about 3000 R. The consultation was unsuccessful: the doctor was clearly not interested in my condition, he indifferently asked questions about depression and prescribed antidepressants. And not the ones that were assigned to me last time, but others. I was too depressed to stand my ground, so I just started looking for another doctor.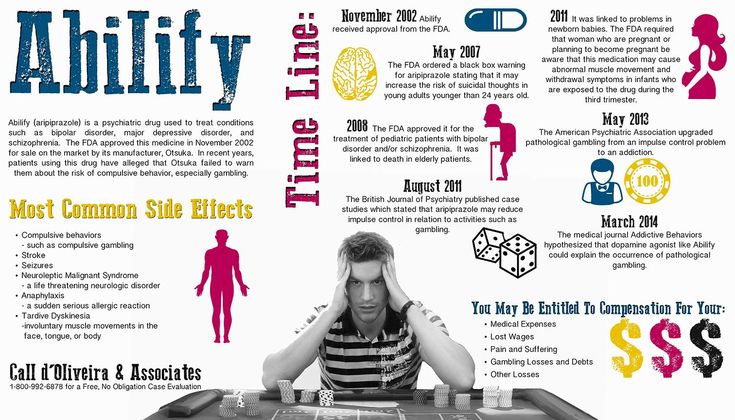 nine0003
nine0003
6 useful services for finding a psychotherapist
The second doctor was in a state clinic, she was recommended to me on Facebook. At first, I waited a long time for an appointment - the doctor was half an hour late, then I started asking about birth injuries and vascular dystonia. This consultation didn't work for me either. I paid 2,000 rubles for her.
The third appointment was successful: I found a psychiatrist, whom I still go to. She works at the State Institute of Psychiatry, but I see her for a fee. One consultation costs 2500 R.
2500 Р
I pay a psychiatrist for one appointment
The institute where the doctor sees, I was advised somewhere in the comments on the Internet. I called the reception and asked to sign me up for a doctor specializing in affective disorders as soon as possible.
The search for a suitable psychiatrist took about a month, so I went to see a doctor in a completely crushed state, in tears and hysteria.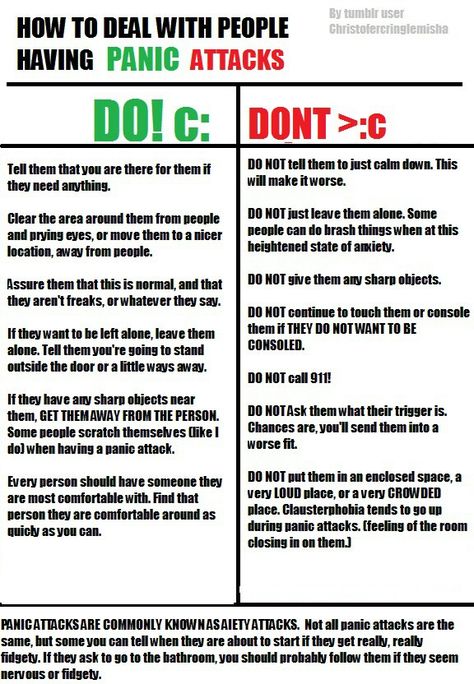 The psychiatrist asked me about the illness, listened to me and offered free hospitalization. However, I refused: I felt that I was controlling myself so as not to commit suicide, and my husband was also nearby, who understood the seriousness of the situation. As a result, I continued the treatment at home. nine0003
The psychiatrist asked me about the illness, listened to me and offered free hospitalization. However, I refused: I felt that I was controlling myself so as not to commit suicide, and my husband was also nearby, who understood the seriousness of the situation. As a result, I continued the treatment at home. nine0003
When hospitalization is needed for bipolar disorder
Viktor Lebedev
psychiatrist, science journalist
Hospitalization for bipolar affective disorder may be necessary if during a manic episode the patient develops strong arousal, he completely loses a critical attitude to his condition, and hallucinations appear rave. Such a condition can end badly for the patient himself or his relatives. In a depressive episode, indications for hospitalization will be suicidal thoughts or suicide attempts. nine0003
Inpatient treatment may also be needed in case of a severe decrease in working capacity.
If you suspect you have bipolar disorder, but are not in the acute phase of the disease, help is not urgent, it is better to spend time looking for a psychiatrist who specializes in bipolar disorder or affective disorders in general. Such a doctor is likely to quickly make the correct diagnosis and select the best treatment.
Such a doctor is likely to quickly make the correct diagnosis and select the best treatment.
Before taking, it is worth writing down all the symptoms that bother you, and also, if possible, make a retrospective graph of the expected phases - mania and depression, write down when they occurred and how long they lasted. This will help the doctor understand if this is BAD or something else. nine0003 This is how the BAR phase sequence looks like in my case
BAD treatment
Consultations with a psychiatrist and drug therapyThe psychiatrist first wrote me a prescription for several drugs: antidepressants and mood stabilizers. They are usually prescribed to people with affective disorders.
As explained to me, treatment is, among other things, checking for the correctness of the diagnosis, a way to distinguish depression from bipolar disorder. If the prescribed drugs help, the diagnosis is correct. nine0333 About two months later, my diagnosis was officially confirmed: bipolar affective disorder type 2.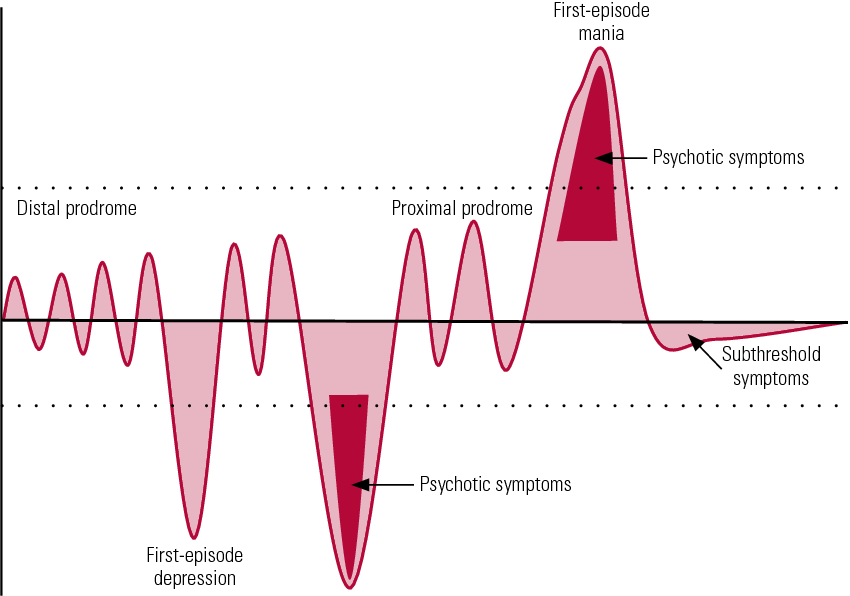
How bipolar disorder is diagnosed
Viktor Lebedev
psychiatrist, science journalist
Bipolar affective disorder is diagnosed by the problems that bother a person. His story should contain a description of typical mood and behavioral disorders, usually there is an alternation of phases of the disease.
Complaints and a history of the disease are enough for diagnosis, sometimes the testimonies of relatives are also taken into account, which can tell about a person's behavior. It happens that a doctor can send you to a clinical psychologist for a psychological examination, but usually an ordinary psychodiagnostic conversation is enough. nine0003
You can suspect the disease on your own, although with hypomania or mania, criticality to one's condition often decreases, that is, a person does not understand that something is wrong with him. Sometimes relatives of the patient come for help, and not he himself. It is better to apply for a diagnosis to a specialist who has worked with BAD, knows what the manifestations of the disease look like.
In general, drug therapy for bipolar disorder consists of several types of drugs that relieve different manifestations of the disease. These are normotimics that stabilize mood, antidepressants that help to cope with depression, antipsychotics that relieve excessive arousal. nine0003
Medication for Bipolar Disorders - MSD Handbook
Bipolar Disorder in Adults: Choice of Therapy - Article for Physicians Uptodate
The doctor selects the type of medication and dosage based on the phase the patient is in. Antidepressants are usually used in depressive phases and in combination with mood stabilizers. Antipsychotics - only in manic episodes and also together with normotimics.
In severe cases, a person with bipolar disorder may take up to six different drugs. But you need to strive to get by with one or two. nine0003
I started taking prescribed antidepressants and mood stabilizers immediately after seeing a psychiatrist. This time, the process of getting out of depression was long and smooth.
How therapy is selected for bipolar affective disorder
Viktor Lebedev
psychiatrist, scientific journalist
The psychiatrist selects treatment individually, taking into account the clinical picture: in the depressive phase - some drugs, in the hypomanic phase - others, in mania - still others.
It is important to combine drugs correctly. So, if a patient with bipolar disorder is prescribed only antidepressants, this can worsen the situation, even if he is depressed. Antidepressants can "disperse" his condition to hypomania or even mania. It is necessary to normalize a person’s well-being, and not throw him into a state with the opposite sign, so therapy includes normotimics. nine0003
The fact is that depression in BAD is not the same depression as usual, they are not always similar even in external manifestations, there are differences from a biological point of view, that is, in how processes in the brain change.
I visit my psychiatrist regularly: she adjusts the doses of drugs and monitors my condition.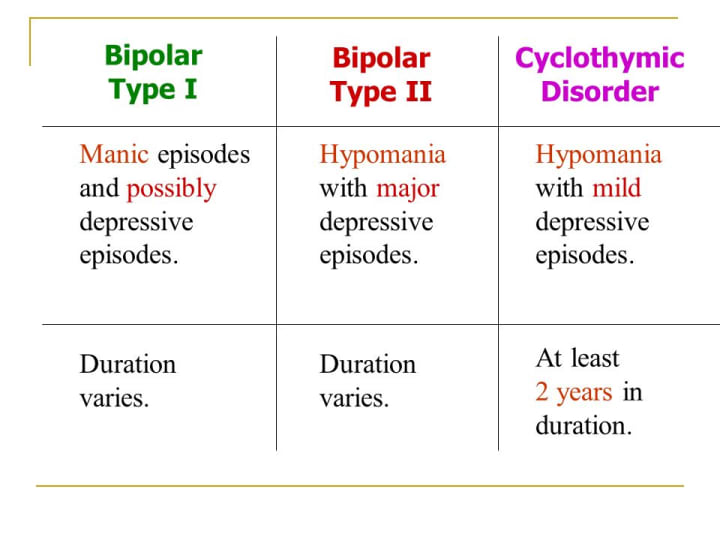 In the first year, I visited her six times - it cost me 15,000 R. Now I go to the doctor only during an exacerbation or a presumptive phase change - about four times a year, once every three to four months. It costs 10,000 R per year. In total, I have been seeing a doctor for three years now. nine0003
In the first year, I visited her six times - it cost me 15,000 R. Now I go to the doctor only during an exacerbation or a presumptive phase change - about four times a year, once every three to four months. It costs 10,000 R per year. In total, I have been seeing a doctor for three years now. nine0003
For two years, until recently, I took antidepressants and mood stabilizers in the minimum dosage. A pack of antidepressants for a month cost about 400 R, mood stabilizers - 600 R. That is, during the period of remission, the pills took 1000 R per month.
1000 R
I spend on pills per month in remission
My prescriptions for drugs However, a few months ago I had an exacerbation, I went into hypomania, so the regimen and dose of drugs had to be changed on the go. Within two weeks, my psychiatrist and I canceled antidepressants, significantly increased the dose of mood stabilizers - 2.5 times, and added antipsychotics. During the exacerbation, which lasted two months, 4000 R per month was spent on tablets. Now 2000 R will go away - the dose of mood stabilizers has been reduced by one and a half times and neuroleptics by half, antidepressants have been removed. nine0003
Now 2000 R will go away - the dose of mood stabilizers has been reduced by one and a half times and neuroleptics by half, antidepressants have been removed. nine0003
It is interesting to observe how quickly drug therapy changes the state of the body and how it then returns to normal. Often, drugs do not fit the first time, so you need to regularly visit a psychiatrist and monitor your well-being. But after choosing the right therapy, you can live almost as before, except that you need to be more attentive to yourself.
/obsessive-compulsive-disorder/
How I live with obsessive-compulsive disorder
BAD treatment cannot be found once and for all
Each patient who is responsible for the treatment of bipolar disorder and is in contact with the doctor has his own scheme for changing the dosage or types of medications, taking into account well-being. For example, if you cannot sleep for more than a few days and stop eating, you add an antipsychotic. If you fall into an abyss of self-hatred and don’t swim for more than a week, an antidepressant will help.
If you fall into an abyss of self-hatred and don’t swim for more than a week, an antidepressant will help.
Of course, this does not cancel regular meetings with a psychiatrist, because the process of choosing drugs and dosages is very complicated. Now I can regulate a lot myself, depending on how I feel, but I still see a specialist. nine0003
At the same time, bipolar affective disorder cannot be cured once and for all - you can only go into a long remission. As my doctor told me, this is five years without pronounced phases. In my case, I lasted two years without episodes, and now I need to start the countdown again.
Also, as far as I know from my experience and the experience of people with the same diagnosis, at some point there is an illusion that everything is cool, there is no illness, it seemed to you that you are doing great. At this point, people stop taking pills - this is a bad decision, never do this. If you feel good, first of all, you should check if this is the beginning of hypomania.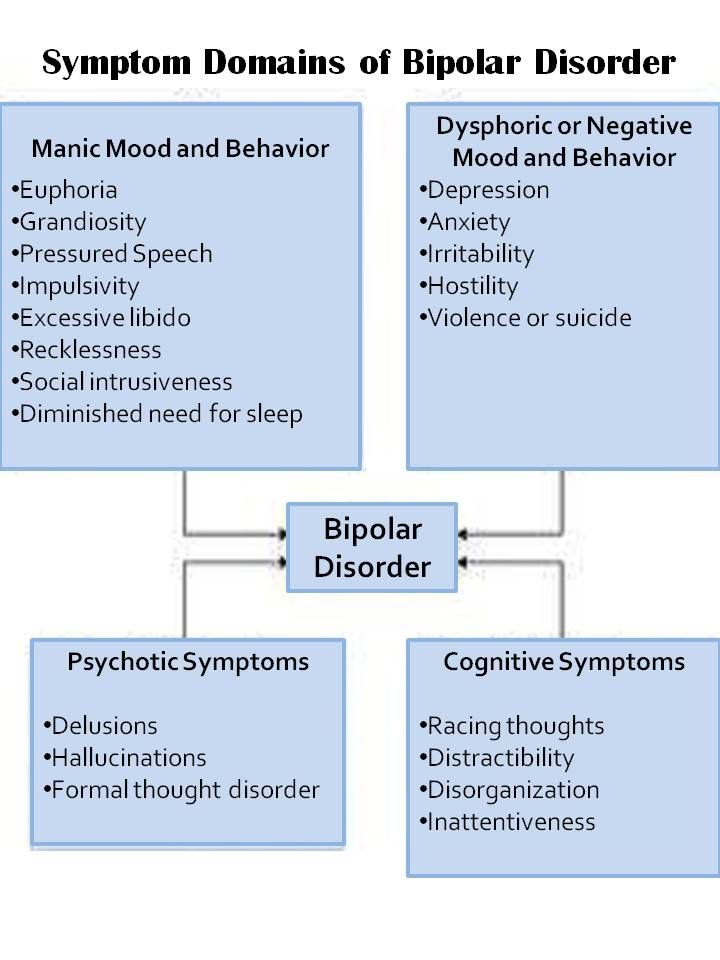 And secondly, be glad that you have entered remission. nine0003
And secondly, be glad that you have entered remission. nine0003
During these three years, I once stopped drinking pills - I got depressed, once I did not pay attention to the symptoms - I got severe hypomania, now I'm trying to go into remission again.
BAD treatment
PsychotherapyThe effectiveness of bipolar affective disorder treatment can be improved by combining drug therapy with psychotherapy. Cognitive behavioral therapy is often used for bipolar disorder. It teaches you how to cope with stress factors, monitor your condition, manage the symptoms of the disease. Even during the sessions, together with the doctor, they work out trigger situations, that is, what can provoke an exacerbation of the disease. nine0003
Bipolar affective disorder and supportive psychotherapy - article on the Uptodate physician website
For example, I have trouble admitting my own mistakes. Every mistake for me is a tragedy, and it seems to me that those around her will never forget.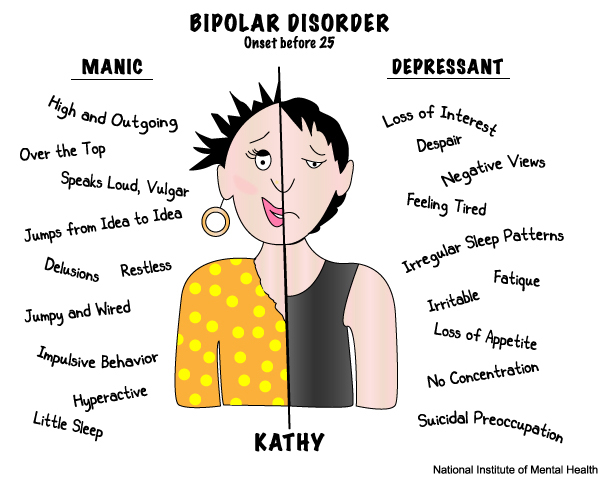 It is difficult for me to admit my own mistakes, oversights cause great anxiety. I also have an ideal image of what I should be: read a lot, earn money, keep my house perfectly clean, have six-packs, study, know two foreign languages, go to exhibitions. Obviously, this is impossible, but a persistent desire to reach an unattainable height is also stressful. I work through all this with a psychotherapist. nine0003
It is difficult for me to admit my own mistakes, oversights cause great anxiety. I also have an ideal image of what I should be: read a lot, earn money, keep my house perfectly clean, have six-packs, study, know two foreign languages, go to exhibitions. Obviously, this is impossible, but a persistent desire to reach an unattainable height is also stressful. I work through all this with a psychotherapist. nine0003
I started therapy only six months ago, on the advice of a doctor, before that I thought that I could cope on my own. At first she was in therapy with a psychotherapist, whom she found through the Inhale project, which helps burnt out employees from the charitable field. I worked with her on this project, then continued after completion.
We looked at situations that increase my anxiety, including fear of making mistakes and being judged, as well as difficulties in life in general. The cost within the project was 400 R per meeting, there were about ten of them in total, then, already outside the project, the price increased to 2400 R.
/prl/
How much does it cost to treat borderline personality disorder
Now I went to another psychotherapist - she has a more applied approach, we look for my cognitive distortions and try to remove them. For example, we work with my excessive anxiety about the impression I make on other people, and the fear that I cannot control it.
The cost of sessions with this specialist is 2500 R per visit. Now I go to her every 10-14 days, that is, 2-3 times a month. In general, I have been working with my condition on my own for quite a long time, so the therapist only directs me in the right direction. nine0003
Is psychotherapy mandatory for bipolar disorder
Viktor Lebedev
psychiatrist, science journalist
Cognitive behavioral therapy is most often prescribed for bipolar disorder. This is an optional therapy, that is, an auxiliary method of treatment, you only need to take medication. However, psychotherapy can greatly improve the quality of life: it complements the action of drugs well, helps to control and change those things that pills do not work on.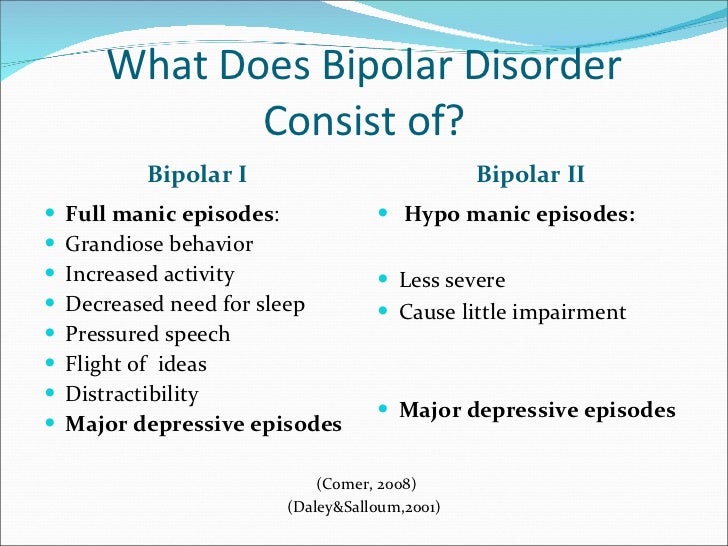 First of all, cognitive-behavioral therapy helps to control emotions, better cope with your illness. nine0003
First of all, cognitive-behavioral therapy helps to control emotions, better cope with your illness. nine0003
Many also benefit from support groups for people with bipolar disorder. I tried to go to such a meeting, but it didn’t work for me: I don’t want to define myself through illness, this is part of my life - but not me.
The largest project holding such meetings is Sunday BAR. They support not only people with bipolar disorder, but also their loved ones. Meetings are held online and offline.
List of support groups in different cities for people with BAD and other disordersPDF, 275 KB
BAD treatment
LifestyleUniversal advice given for bipolar disorder and more includes: sleep and work-life balance, eat right, avoid alcohol, exercise.
All this really helps, but in fact, organizing your life is difficult: meetings with friends, vacations, unexpected work do not fit into the routine, you want to work more, and alcohol looks like a great way to cope with anxiety, although in fact it can lead to depression. nine0003
nine0003
I try to keep the correct regimen to the best of my ability. True, according to my feelings, depression comes by itself, without any triggers from the outside, and I cannot influence it. But hypomania is fueled by new projects, loves, and other emotions. For example, even a small amount of falling in love causes hypomania, which, in turn, increases falling in love. It doesn't end well.
/shizofreniya/
How much does it cost to support a relative with a mental disorder
I lived in St. Petersburg for quite a long time, there during the white nights you don’t feel like sleeping at all - and this provokes hypomania. One of the psychiatrists even forbade me to go to St. Petersburg for some time.
Now I have an established sleep and eating regime, I quickly notice its violation - this is a signal that an exacerbation has begun. Unfortunately, sometimes the regime is knocked down by external circumstances, then it is more difficult to notice the exacerbation of BAD.
Sleep is very important to me, it is my priority. I try not to hang out until the middle of the night, and if I didn’t manage to get enough sleep, then I try to sleep in the afternoon. I usually go to bed around midnight, get up at 8-9hours of the morning is a comfortable mode for me and my work. I very rarely stay awake at night or wake up later than 10 am.
I have a fitness bracelet that tracks the phases and amount of sleep - it helps to see the dynamics and notice deviations. When I see a sleep disorder, I start drinking light tranquilizers and antipsychotics to return to a comfortable mode.
| Sleeping less than seven hours on pills indicates an episode of hypomania, without drugs in this phase I would sleep less than four hours | And sleep for more than seven hours is already the normalization of the state after the addition of other tablets |
It’s getting more and more difficult with food: I have a difficult relationship with my own body, so I perceive a decrease in appetite with enthusiasm.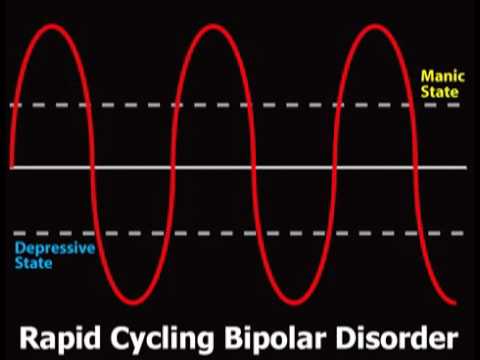 I am working on the problem with a psychotherapist, how to solve it, until I figured it out. My psychiatrist believes that first sleep, and then everything else, and my experience confirms this: sleep disturbances have a stronger effect on well-being. I also keep a record of alcohol consumption in the Alcogram application - abuse negatively affects my condition. When I see how many sober days there were, it motivates me to control myself. nine0003
I am working on the problem with a psychotherapist, how to solve it, until I figured it out. My psychiatrist believes that first sleep, and then everything else, and my experience confirms this: sleep disturbances have a stronger effect on well-being. I also keep a record of alcohol consumption in the Alcogram application - abuse negatively affects my condition. When I see how many sober days there were, it motivates me to control myself. nine0003
I am lucky that I take my job seriously: it is responsible and resource-intensive, it is important for me to be productive, it disciplines and helps me to keep the regime.
What to do to reduce the frequency of exacerbations
Viktor Lebedev
psychiatrist, science journalist
In BAD, it is important to have a daily routine that allows you to maintain normal behavior. This reduces the frequency of exacerbations, sometimes helps to completely avoid the recurrence of episodes of the disease. In addition to quality sleep and proper nutrition, you need to avoid overwork, work in an exhausted state, give yourself a rest. Doctors usually insist on the exclusion of alcohol, drugs are also dangerous, especially stimulants, which can cause psychosis in a healthy person. nine0003
Doctors usually insist on the exclusion of alcohol, drugs are also dangerous, especially stimulants, which can cause psychosis in a healthy person. nine0003
Exacerbations of the disease can occur on their own, without the influence of external factors, or they can be caused by external events, both tragic, such as the death of a loved one or a break in relationships, and joyful. Therefore, it is important to learn to recognize your emotions, to identify in time what provokes a new episode, both independently and with the help of psychotherapy.
How I live with BAD now
Accepting the diagnosis was not easy: on the one hand, it finally became clear what was happening to me and that it could be regulated. On the other hand, this is a diagnosis for life. You need to constantly monitor your condition, take pills, consult with doctors. nine0003
The most difficult thing for me was the inability to separate myself as a person from the disease. What of what I did in life was the result of my choice, and what was a symptom of the disease? Moving from city to city, changing jobs, partners, hobbies - what if all this is just a disease, and I'm not behind it? Three years have passed - and I still cannot separate myself from BAD, it seems impossible.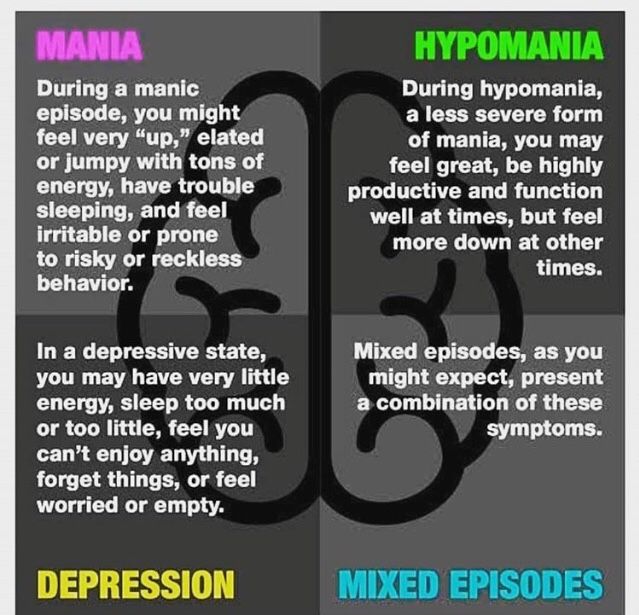
Now life has become easier: now I know what to expect in the near future, because the phase schedule is still respected. It is clear when to slow down with the pace of life, and when to add antidepressants. nine0003
My work is related to people. Of course, the disease affects my mood and state: in depression I have less strength and the ability to give out emotions, in hypomania, on the contrary, there are a lot of emotions, but there is not enough concentration. It's good that work allows you to vary the load depending on the phase: in depression I can work a little less, and in hypomania - a little more.
At the time of my first diagnosed depression, I had an unloved job, it took the entire resource. I cried in the mornings, afternoons and evenings because it was difficult for me to keep working. Now I really love my job, it gives me more resources than it takes. nine0003
I continue to take medication, see a psychiatrist several times a year and a psychotherapist several times a month.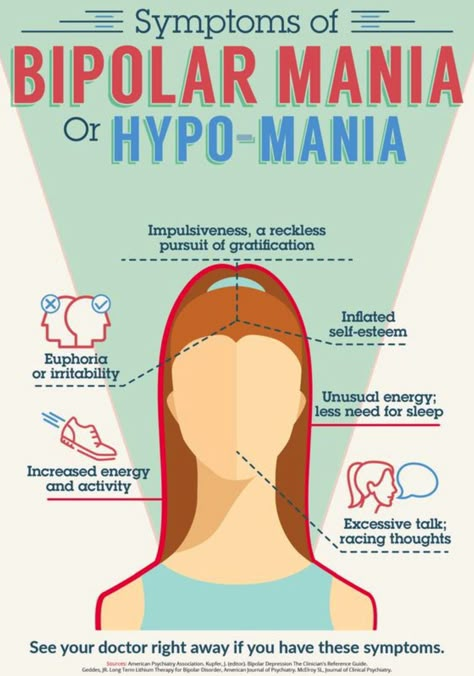 In March, at the most difficult moment of the exacerbation, I spent on medicines, an appointment with a psychiatrist and three meetings with a psychologist 13,000 R.
In March, at the most difficult moment of the exacerbation, I spent on medicines, an appointment with a psychiatrist and three meetings with a psychologist 13,000 R.
13,000 R
I go into remission and spend about 8,000-10,000 R per month on medications, a psychologist, and periodic appointments with a psychiatrist. A significant amount, but it allows me to remain in a resourceful and efficient state. nine0003
The unobvious difficulty of living with bipolar disorder is the need to strictly control one's financial situation. In hypomania, money flies away easily, you make decisions instantly - for example, you can decide in a minute to fly to Spain and buy tickets. When you are depressed, you spend less, but it is also difficult to earn money. I try to keep a financial cushion in case of an aggravation, and also take into account all expenses in the application so as not to get into debt. Fortunately, so far my financial anxiety is stronger than bipolar, so there has never been a credit card debt.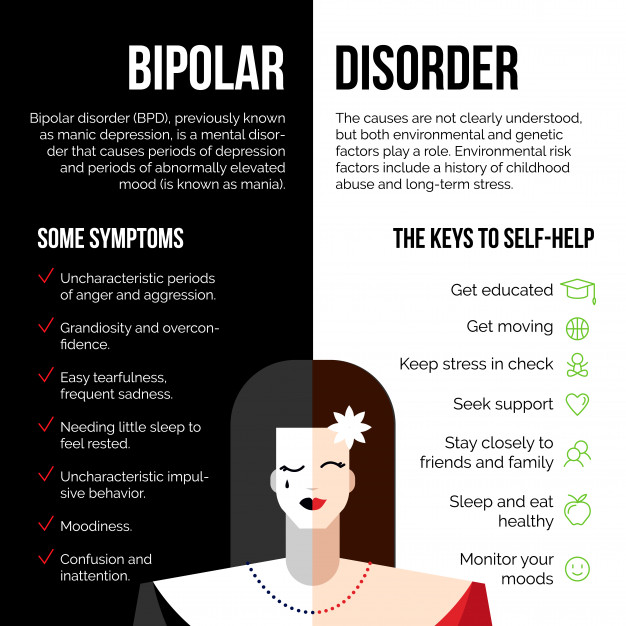 nine0003
nine0003
I spent 58,800 rubles on BAD treatment in a year
| Treatment | Price |
|---|---|
| Psychiatric appointment | 10 000 R, total 4 receptions of 2500 R |
| Psychotherapist appointment | 25 000 R, total 10 receptions of 2500 R |
| Antidepressants | 4800 R, 12 packs of 400 R |
| Antipsychotics | 7000 R, 7 packs of 1000 R |
| Normotimics | 12000 R, 15 packs of 800 R |
Reception of a psychiatrist
10 000 R, total 4 receptions of 2500 r
Reception of a psychotherapist
25 000 R, total 10 doses of 2500 R
antidepressants
4800 r, 12 packages of 400 p
neuroleptic neuroleptic
7000 R, 7 packs of 1000 R
Normotimics
12000 R, 15 packs of 800 R
Books I recommend reading about bipolar affective disorder
The most famous book about living with bipolar disorder is The Restless Mind.