Witnessing domestic violence the effect on children
Witnessing Domestic Violence: The Effect on Children
MELISSA M. STILES, M.D., University of Wisconsin-Madison Medical School, Madison, Wisconsin
Am Fam Physician. 2002;66(11):2052-2067
Domestic violence is an ongoing experience of physical, psychologic, and/or sexual abuse in the home that is used to establish power and control over another person.1 Although awareness about the rate of domestic violence in our society is increasing, the public health ramifications have only recently been recognized in the medical community.
The majority of the medical literature to date has focused on the effect of domestic violence on the primary victim. What effect does witnessing domestic violence have on secondary victims, such as children who live in homes where partner abuse occurs? It is estimated that 3.2 million American children witness incidents of domestic violence annually.2
Witnessing domestic violence can lead children to develop an array of age-dependent negative effects. Research in this area has focused on the cognitive, behavioral, and emotional effects of domestic violence. Children who witness violence in the home and children who are abused may display many similar psychologic effects.3,4 These children are at greater risk for internalized behaviors such as anxiety and depression, and for externalized behaviors such as fighting, bullying, lying, or cheating. They also are more disobedient at home and at school, and are more likely to have social competence problems, such as poor school performance and difficulty in relationships with others. 5–9 Child witnesses display inappropriate attitudes about violence as a means of resolving conflict and indicate a greater willingness to use violence themselves.3,4,10
5–9 Child witnesses display inappropriate attitudes about violence as a means of resolving conflict and indicate a greater willingness to use violence themselves.3,4,10
Although there is general agreement that children from violent homes have more emotional and behavioral problems than those from nonviolent homes, the research in this area has a number of limitations. The sample sizes are generally small, usually composed of shelter participants, and the studies generally have a retrospective design. A number of variables are not well controlled, such as gender, socioeconomic status, intelligence, cultural background, and social support. Many of these children also experience abrupt school and home changes and parental separation that can have a significant effect on their development.
Another potential confounding variable is that many of these children undergo direct abuse. How can the effects of witnessing violence be distinguished from the effects of direct abuse? Research in this area has focused on the cognitive, behavioral, and emotional effects of witnessing domestic violence. More research is needed to develop appropriate screening tools and intervention strategies for children who are at risk.
7,8
More research is needed to develop appropriate screening tools and intervention strategies for children who are at risk.
7,8
Age Span Differences
The potential negative effects vary across the age span (Table 1).3,5 In infants from homes with partner abuse, the child's needs for attachment may be disrupted. More than 50 percent of these infants cry excessively and have eating and sleeping problems. Infants are also at a significantly increased risk for physical injury.
Preschool-aged children who witness intimate violence may develop a range of problems, including psychosomatic complaints such as headaches and abdominal pain. They also can display regressive behaviors such as enuresis, thumb sucking, and sleep disturbances. During the preschool years, children turn to their parents for protection and stability, but these needs are often disrupted in families with partner abuse. Increased anxiety around strangers and behaviors such as whining, crying, and clinging may occur. Nighttime problems such as insomnia and parasomnias are more frequent in this age group. Children in this age group who have witnessed domestic violence also may show signs of terror, manifested by yelling, irritability, hiding, and stuttering.5,8,11
Nighttime problems such as insomnia and parasomnias are more frequent in this age group. Children in this age group who have witnessed domestic violence also may show signs of terror, manifested by yelling, irritability, hiding, and stuttering.5,8,11
| Age | Potential effects |
|---|---|
| Infants | Needs for attachment disrupted |
| Poor sleeping habits | |
| Eating problems | |
| Higher risk of physical injury | |
| Preschool children | Lack feelings of safety |
| Separation/stranger anxiety | |
| Regressive behaviors | |
| Insomnia/parasomnias | |
| School-aged children | Self-blame |
| Somatic complaints | |
| Aggressive behaviors | |
| Regressive behaviors | |
| Adolescents | School truancy |
| Delinquency | |
| Substance abuse | |
| Early sexual activity |
School-aged children also can develop a range of problems including psychosomatic complaints, such as headaches or abdominal pain, as well as poor school performance. They are less likely to have many friends or participate in outside activities. Witnessing partner abuse can undermine their sense of self-esteem and their confidence in the future. School-aged children also are more likely to experience guilt and shame about the abuse, and they tend to blame themselves.4,5
They are less likely to have many friends or participate in outside activities. Witnessing partner abuse can undermine their sense of self-esteem and their confidence in the future. School-aged children also are more likely to experience guilt and shame about the abuse, and they tend to blame themselves.4,5
Adolescent witnesses have higher rates of interpersonal problems with other family members, especially interparental (parent-child) conflict. They are more likely to have a fatalistic view of the future resulting in an increased rate of risk taking and antisocial behavior, such as school truancy, early sexual activity, substance abuse, and delinquency.5,10,12,13
Resilience
It is important to note that many children who witness domestic violence do not have adverse cognitive, behavioral, and emotional effects. Several variables may lessen the effects of witnessing violence. These variables include female gender, intellectual ability, higher levels of socioeconomic status, and social support for the children.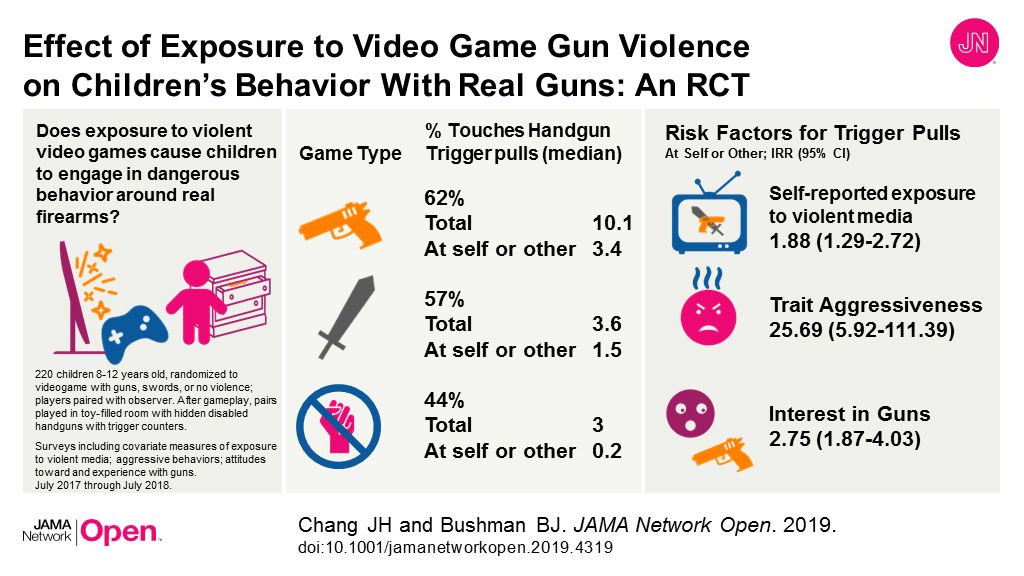 The studies on resilience also have been limited by small sample sizes but show promise in identifying potential protective factors that mediate the negative effects of witnessing domestic violence.14
The studies on resilience also have been limited by small sample sizes but show promise in identifying potential protective factors that mediate the negative effects of witnessing domestic violence.14
Prevention and Screening
Primary care physicians can address the issue of domestic violence on multiple levels. Medical schools should educate physicians about the potential negative effects in children who witness domestic violence. Although a recent effort has been made to educate physicians about domestic violence, the focus has been on the primary victim. Medical education must broaden the view of domestic violence to include effects on silent witnesses and to encourage physicians to screen for and help prevent violence.
Physicians can begin violence prevention measures in the clinic. Because violence is, in large part, a learned behavior, physicians should assess the parents' methods of resolving conflict and their responses to anger.15 Optimally, this discussion should begin when a couple is contemplating having a child or during prenatal examinations. Couples should be educated about the negative effects that arguments and fights have on children. They should be encouraged to be consistent with discipline and to keep children out of their disagreements. Physicians can also discuss nonviolent forms of discipline, such as time-outs and removal of privileges.16,17
Couples should be educated about the negative effects that arguments and fights have on children. They should be encouraged to be consistent with discipline and to keep children out of their disagreements. Physicians can also discuss nonviolent forms of discipline, such as time-outs and removal of privileges.16,17
Parents should be educated about the negative consequences of watching violence on television and should be encouraged to limit their children's television viewing to no more than two hours per day. In addition, because the presence of guns and other weapons in the home is associated with an increased risk of homicide and suicide among family members, parents should be asked if weapons are kept in the home.18,19 If so, parents should be advised to store guns unloaded in a locked case. Children should be told that if they see a gun they must not touch it and should leave the area immediately and tell an adult.20–22
Posters and information about family violence issues and resources can be displayed in waiting rooms, examination rooms, and office restrooms (Table 2). 15,16,20–22
15,16,20–22
| Counsel parents about developmentally appropriate means of disciplining their children. |
| Counsel parents about nonviolent ways to resolve conflict. |
| Educate parents about the negative consequences of arguments on children and each other. |
| Ask about the presence of guns or other weapons in the home. |
| Advise parents to limit their children's television viewing. |
| Screen for domestic violence. |
| Display resource materials in the office. |
During well-child and adult health maintenance examinations, physicians should routinely screen for family violence by asking open, nonjudgmental questions. The discussion should begin with a statement regarding the importance of the topic, such as, “Because I am concerned about the health effects of domestic violence, I ask all patients about violence in the home. ” Specific questions that address the various forms of domestic abuse should follow (Table 3).1 According to experts, screening during well-child examinations should be performed privately with the mother.23
” Specific questions that address the various forms of domestic abuse should follow (Table 3).1 According to experts, screening during well-child examinations should be performed privately with the mother.23
The rightsholder did not grant rights to reproduce this item in electronic media. For the missing item, see the original print version of this publication.
If a child presents with emotional or behavioral problems, an inquiry about family violence should be made. Because such symptoms are not specific for witnessing domestic violence, the physician also should inquire about other etiologies, such as child abuse, marital discord, peer relationships, sexual violence, and community violence. Depression and alcohol and drug abuse also should be considered. Age-specific screening questions can be incorporated into well-child examinations and sports physicals (Table 4).1,15–20,24,25
| Fighting: When was your last pushing-shoving fight? How many fights have you been in during the past month? The past year? |
| Injuries: Have you ever been injured in a fight? Do you know anyone who has been injured or killed? |
| Sexual violence: What happens when you and your boyfriend (or girlfriend) have an argument? Have you ever been forced to have sex against your will? |
| Threats: Have you ever been threatened with a knife? A gun? |
| Self-defense: How do you avoid getting in fights? Do you carry a weapon for self-defense? |
Identification of Domestic Violence
If domestic violence is identified, a number of actions may be taken by the primary care physician. First, the patient should be assured that confidentiality will be maintained. It is also important to express concern for the patient's safety and to acknowledge that violence is not an appropriate behavior. Physicians should avoid expressing outrage toward the perpetrator, implying that the patient is responsible for the abuse, or directing the patient to leave the relationship. In addition, medical records must be accurate and thorough because they may become an important element in any legal action.
First, the patient should be assured that confidentiality will be maintained. It is also important to express concern for the patient's safety and to acknowledge that violence is not an appropriate behavior. Physicians should avoid expressing outrage toward the perpetrator, implying that the patient is responsible for the abuse, or directing the patient to leave the relationship. In addition, medical records must be accurate and thorough because they may become an important element in any legal action.
Of note, a mother's disclosure during a well-child examination should not be recorded in the child's medical record, because the perpetrator may have access to that record. Rather, documentation should be placed in the mother's medical record. Because child abuse is often present in homes where partner abuse occurs, the risk for both types of violence should be assessed.
State laws require physicians to report a diagnosis or impression of probable child abuse or neglect to the authorities. Witnessing domestic violence is not defined as a mandatory reportable form of child abuse. Reporting requirements for domestic violence vary by state, so physicians should be aware of their own state laws. Five states have mandatory reporting (California, Kentucky, New Hampshire, New Mexico, and Rhode Island). Community and national resources for victims of domestic violence should be offered to the patient (Table 5). Many shelters also provide services for children who have witnessed violence. Safety assessment and planning for patients and children are paramount (Table 6).1,23 A follow-up appointment or telephone call should be scheduled to ensure that the patient will have access to a primary care provider.1,23–26
Witnessing domestic violence is not defined as a mandatory reportable form of child abuse. Reporting requirements for domestic violence vary by state, so physicians should be aware of their own state laws. Five states have mandatory reporting (California, Kentucky, New Hampshire, New Mexico, and Rhode Island). Community and national resources for victims of domestic violence should be offered to the patient (Table 5). Many shelters also provide services for children who have witnessed violence. Safety assessment and planning for patients and children are paramount (Table 6).1,23 A follow-up appointment or telephone call should be scheduled to ensure that the patient will have access to a primary care provider.1,23–26
| National Domestic Violence Hotline: 800-799-SAFE (7233) |
| National Resource Center on Domestic Violence: 800-537-2238 |
Family Violence Prevention Fund: www. fvpf.org fvpf.org |
| American Medical Association: www.ama-assn.org |
| American Academy of Pediatrics: www.aap.org |
| American Academy of Family Physicians: www.familydoctor.org |
| Minnesota Center Against Violence and Abuse: www.mincava.umn.edu |
| Do you feel safe going home? If not, where could you go? |
| Are you aware of your local resources? |
| Can you keep money, important papers, and telephone numbers in a safe place? |
| Are there weapons in the home? Can they be removed or placed in a safe, locked area? |
| Do you have a friend or family member with whom you can stay? |
| Where would you go in an emergency? How would you get there? |
Community Advocacy
Physicians can be community advocates and leaders with regard to violence prevention issues. Many communities have formed coordinated community response teams for cases of domestic violence that require physician input. Physicians may serve as consultants to schools on issues such as conflict resolution and anger management programs. Physicians also may foster links between physician societies and local community groups to develop programs for the management and prevention of domestic violence.27
Many communities have formed coordinated community response teams for cases of domestic violence that require physician input. Physicians may serve as consultants to schools on issues such as conflict resolution and anger management programs. Physicians also may foster links between physician societies and local community groups to develop programs for the management and prevention of domestic violence.27
Witnessing domestic violence can have significant short- and long-term effects on a child. Primary care physicians should be aware of the possible cognitive, behavioral, and emotional effects of witnessing domestic violence. Physicians can play a key role by developing curricula for medical schools, screening in the office, and serving as advocates for their community on this important public health topic.
Effects of domestic violence on children
Many children exposed to violence in the home are also victims of physical abuse.1 Children who witness domestic violence or are victims of abuse themselves are at serious risk for long-term physical and mental health problems. 2 Children who witness violence between parents may also be at greater risk of being violent in their future relationships. If you are a parent who is experiencing abuse, it can be difficult to know how to protect your child.
2 Children who witness violence between parents may also be at greater risk of being violent in their future relationships. If you are a parent who is experiencing abuse, it can be difficult to know how to protect your child.
What are the short-term effects of domestic violence or abuse on children?
Children in homes where one parent is abused may feel fearful and anxious. They may always be on guard, wondering when the next violent event will happen.3 This can cause them to react in different ways, depending on their age:
- Children in preschool. Young children who witness intimate partner violence may start doing things they used to do when they were younger, such as bed-wetting, thumb-sucking, increased crying, and whining. They may also develop difficulty falling or staying asleep; show signs of terror, such as stuttering or hiding; and show signs of severe separation anxiety.
- School-aged children. Children in this age range may feel guilty about the abuse and blame themselves for it.
 Domestic violence and abuse hurts children’s self-esteem. They may not participate in school activities or get good grades, have fewer friends than others, and get into trouble more often. They also may have a lot of headaches and stomachaches.
Domestic violence and abuse hurts children’s self-esteem. They may not participate in school activities or get good grades, have fewer friends than others, and get into trouble more often. They also may have a lot of headaches and stomachaches. - Teens. Teens who witness abuse may act out in negative ways, such as fighting with family members or skipping school. They may also engage in risky behaviors, such as having unprotected sex and using alcohol or drugs. They may have low self-esteem and have trouble making friends. They may start fights or bully others and are more likely to get in trouble with the law. This type of behavior is more common in teen boys who are abused in childhood than in teen girls. Girls are more likely than boys to be withdrawn and to experience depression.4
What are the long-term effects of domestic violence or abuse on children?
More than 15 million children in the United States live in homes in which domestic violence has happened at least once. 5 These children are at greater risk for repeating the cycle as adults by entering into abusive relationships or becoming abusers themselves. For example, a boy who sees his mother being abused is 10 times more likely to abuse his female partner as an adult. A girl who grows up in a home where her father abuses her mother is more than six times as likely to be sexually abused as a girl who grows up in a non-abusive home.6
5 These children are at greater risk for repeating the cycle as adults by entering into abusive relationships or becoming abusers themselves. For example, a boy who sees his mother being abused is 10 times more likely to abuse his female partner as an adult. A girl who grows up in a home where her father abuses her mother is more than six times as likely to be sexually abused as a girl who grows up in a non-abusive home.6
Children who witness or are victims of emotional, physical, or sexual abuse are at higher risk for health problems as adults. These can include mental health conditions, such as depression and anxiety. They may also include diabetes, obesity, heart disease, poor self-esteem, and other problems.7
Can children recover from witnessing or experiencing domestic violence or abuse?
Each child responds differently to abuse and trauma. Some children are more resilient, and some are more sensitive. How successful a child is at recovering from abuse or trauma depends on several things, including having:8
- A good support system or good relationships with trusted adults
- High self-esteem
- Healthy friendships
Although children will probably never forget what they saw or experienced during the abuse, they can learn healthy ways to deal with their emotions and memories as they mature. The sooner a child gets help, the better his or her chances for becoming a mentally and physically healthy adult.
The sooner a child gets help, the better his or her chances for becoming a mentally and physically healthy adult.
How can I help my children recover after witnessing or experiencing domestic violence?
You can help your children by:
- Helping them feel safe. Children who witness or experience domestic violence need to feel safe.9 Consider whether leaving the abusive relationship might help your child feel safer. Talk to your child about the importance of healthy relationships.
- Talking to them about their fears. Let them know that it’s not their fault or your fault. Learn more about how to listen and talk to your child about domestic violence (PDF, 229 KB).
- Talking to them about healthy relationships. Help them learn from the abusive experience by talking about what healthy relationships are and are not. This will help them know what is healthy when they start romantic relationships of their own.

- Talking to them about boundaries. Let your child know that no one has the right to touch them or make them feel uncomfortable, including family members, teachers, coaches, or other authority figures. Also, explain to your child that he or she doesn’t have the right to touch another person’s body, and if someone tells them to stop, they should do so right away.
- Helping them find a reliable support system. In addition to a parent, this can be a school counselor, a therapist, or another trusted adult who can provide ongoing support. Know that school counselors are required to report domestic violence or abuse if they suspect it.
- Getting them professional help. Cognitive behavioral therapy (CBT) is a type of talk therapy or counseling that may work best for children who have experienced violence or abuse.10 CBT is especially helpful for children who have anxiety or other mental health problems as a result of the trauma.
 11 During CBT, a therapist will work with your child to turn negative thoughts into more positive ones. The therapist can also help your child learn healthy ways to cope with stress.12
11 During CBT, a therapist will work with your child to turn negative thoughts into more positive ones. The therapist can also help your child learn healthy ways to cope with stress.12
Your doctor can recommend a mental health professional who works with children who have been exposed to violence or abuse. Many shelters and domestic violence organizations also have support groups for kids.13 These groups can help children by letting them know they are not alone and helping them process their experiences in a nonjudgmental place.14
Is it better to stay in an abusive relationship rather than raise my children as a single parent?
Children do best in a safe, stable, loving environment, whether that’s with one parent or two. You may think that your kids won’t be negatively affected by the abuse if they never see it happen. But children can also hear abuse, such as screaming and the sounds of hitting. They can also sense tension and fear. Even if your kids don’t see you being abused, they can be negatively affected by the violence they know is happening.
Even if your kids don’t see you being abused, they can be negatively affected by the violence they know is happening.
If you decide to leave an abusive relationship, you may be helping your children feel safer and making them less likely to tolerate abuse as they get older.15 If you decide not to leave, you can still take steps to protect your children and yourself.
How can I make myself and my children safe right now if I’m not ready to leave an abuser?
Your safety and the safety of your children are the biggest priorities. If you are not yet ready or willing to leave an abusive relationship, you can take steps to help yourself and your children now, including:16
- Making a safety plan for you and your child
- Listening and talking to your child and letting them know that abuse is not OK and is not their fault
- Reaching out to a domestic violence support person who can help you learn your options
If you are thinking about leaving an abusive relationship, you may want to keep quiet about it in front of your children.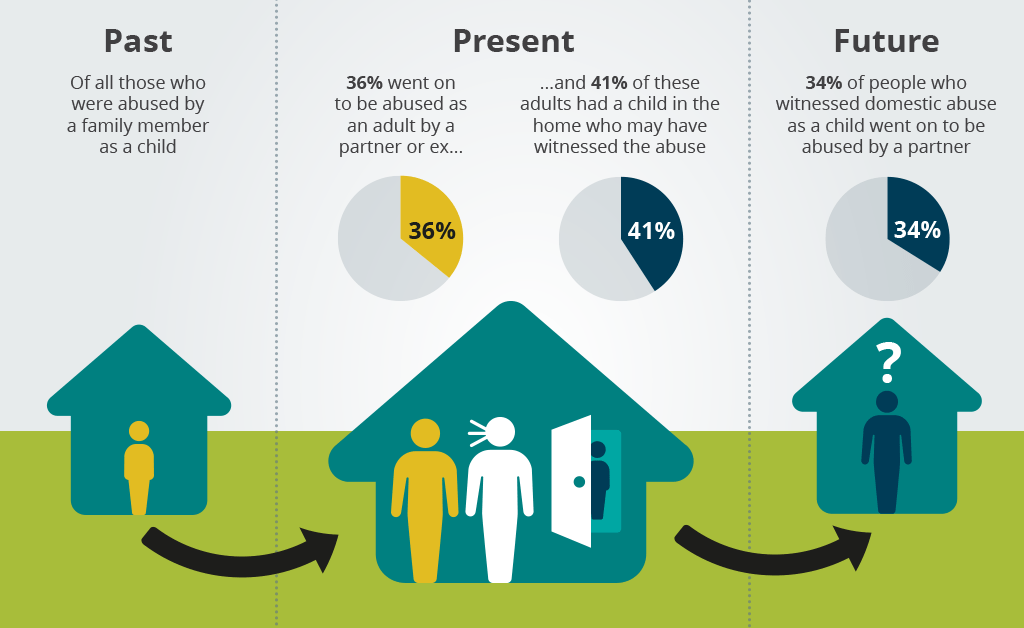 Young children may not be able to keep a secret from an adult in their life. Children may say something about your plan to leave without realizing it. If it would be unsafe for an abusive partner to know ahead of time you’re planning to leave, talk only to trusted adults about your plan. It’s better for you and your children to be physically safe than for your children to know ahead of time that you will be leaving.
Young children may not be able to keep a secret from an adult in their life. Children may say something about your plan to leave without realizing it. If it would be unsafe for an abusive partner to know ahead of time you’re planning to leave, talk only to trusted adults about your plan. It’s better for you and your children to be physically safe than for your children to know ahead of time that you will be leaving.
Did we answer your question about the effects of domestic violence on children?
For more information about the effects of domestic violence on children, call the OWH Helpline at 1-800-994-9662 or check out the following resources from other organizations:
- About the Issue: What is child abuse? — Fact sheet from the Joyful Heart Foundation.
- Behind Closed Doors: The Impact of Domestic Violence on Children (PDF, 1.8 M) — Publication from the United Nations Children’s Fund (UNICEF).
- Child Abuse — Information from KidsHealth.org.
- Childhood Domestic Violence — Information from the Childhood Domestic Violence Association.
- Help for Families — Information about Temporary Assistance for Needy Families from the Office of Family Assistance.
- Safety for Parents — Information from the Rape, Abuse & Incest National Network (RAINN) for parents about getting a child to safety.
- Help for Parents of Children Who Have Been Sexually Abused by Family Members — Information from RAINN.
Sources
- Modi, M.N., Palmer, S., Armstrong, A. (2014). The Role of Violence Against Women Act in Addressing Intimate Partner Violence: A Public Health Issue. Journal of Women’s Health; 23(3): 253-259.
- Gilbert, L.K., Breiding, M.J., Merrick, M.T., Parks, S.E., Thompson, W.W., Dhingra, S.S., Ford, D.C. (2015). Childhood Adversity and Adult Chronic Disease: An update from ten states and the District of Columbia, 2010. American Journal of Preventive Medicine; 48(3): 345-349.
- Domestic Violence Roundtable. (n.d.). The Effects of Domestic Violence on Children.
- Child Welfare Information Gateway.
 (2014). Domestic Violence and the Child Welfare System. Washington, DC: Children’s Bureau, Administration for Children and Families, U.S. Department of Health and Human Services.
(2014). Domestic Violence and the Child Welfare System. Washington, DC: Children’s Bureau, Administration for Children and Families, U.S. Department of Health and Human Services. - McDonald, R., Jouriles, E.N., Ramisetty-Mikler, S., Caetano, R., Green, C.E. (2006). ). Estimating the Number of American Children Living in Partner-Violent Families. Journal of Family Psychology; 20(1): 137-142.
- Vargas, L. Cataldo, J., Dickson, S. (2005). Domestic Violence and Children. In G.R. Walz & R.K. Yep (Eds.), VISTAS: Compelling Perspectives on Counseling. Alexandria, VA: American Counseling Association; 67-69.
- Monnat, S.M., Chandler, R.F. (2015), Long Term Physical Health Consequences of Adverse Childhood Experiences. The Sociologist Quarterly; 56(4): 723-752.
- Child Welfare Information Gateway. (2014). Protective Factors Approaches in Child Welfare. Washington, DC: Children’s Bureau, Administration for Children and Families, U.S. Department of Health and Human Services.

- National Child Traumatic Stress Network. (n.d.). Interventions for Children Exposed to Domestic Violence: Core Principles.
- Caffo, E., Belaise, C. (2003). Psychological aspects of traumatic injury in children and adolescents. Child and Adolescent Psychiatric Clinics of North America; 12(3): 493-535.
- Deblinger, E., Mannarino, A. P., Cohen, J. A., & Steer, R. A. (2006). A follow-up study of a multisite, randomized, controlled trial for children with sexual abuse-related PTSD symptoms. Journal of the American Academy of Child and Adolescent Psychiatry; 45(12): 1474-84.
- Kidshealth.org. (2013). Taking Your Child to a Therapist.
- National Child Traumatic Stress Network. (n.d.). Interventions for Children Exposed to Domestic Violence: Core Principles.
- Vargas, L., Cataldo, J., Dickson, S. (2005). Domestic Violence and Children. In Walz, G.R., Yep, R.K. (Eds.), VISTAS: Compelling Perspectives on Counseling. Alexandria, VA: American Counseling Association; 67-69.

- Center for Domestic Peace. (2016). Calling the Police.
- Loveisrespect.org (n.d.). I Have Children with My Abuser.
The Office on Women's Health is grateful for the medical review by:
- Kathleen C. Basile, Ph.D., Lead Behavioral Scientist, Division of Violence Prevention, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention (CDC)
- Kathryn Jones, M.S.W., Public Health Advisor, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention (CDC)
- Sharon G. Smith, Ph.D., Behavioral Scientist, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention (CDC)
- Rape, Abuse & Incest National Network (RAINN) Staff
All material contained on these pages are free of copyright restrictions and maybe copied, reproduced, or duplicated without permission of the Office on Women’s Health in the U.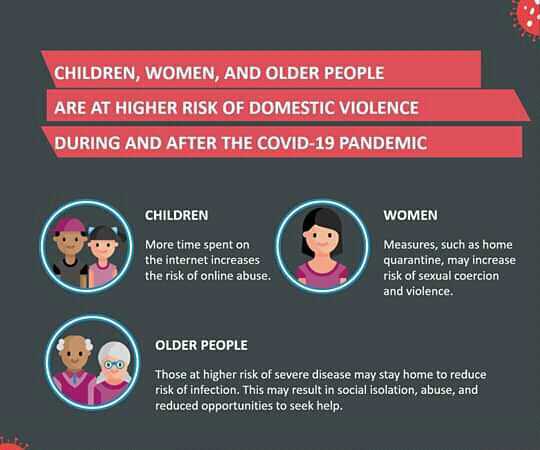 S. Department of Health and Human Services. Citation of the source is appreciated.
S. Department of Health and Human Services. Citation of the source is appreciated.
Page last updated: February 15, 2021
Child abuse
Child abuse- Healthcare issues »
- A
- B
- B
- G
- D
- E
- and
- 9000 O
- P
- R
- S
- T
- U
- F
- X
- C
- H
- W
- W
- B
- S
- B
- E
- S
- I
- Popular Topics
- Air pollution
- Coronavirus disease (COVID-19)
- Hepatitis
- Data and statistics »
- Newsletter
- The facts are clear
- Publications
- Find a country »
- A
- B
- in
- G
- D
- E
- С
- and
- L 9000 P
- C
- T
- U
- Ф
- x
- h
- Sh
- 9
- WHO in countries »
- Reporting
003
- Regions »
- Africa
- America
- Southeast Asia
- Europe
- Eastern Mediterranean
- Western Pacific
- Media Center
- Press releases
- Statements
- Media messages
- Comments
- Reporting nine0005
- Online Q&A
- Developments
- Photo reports
- Questions and answers
- Update
- Emergencies "
- News "
- Disease Outbreak News
- WHO Data »
- Dashboards »
- COVID-19 Monitoring Dashboard
- Highlights "
- About WHO »
- General director
- About WHO
- WHO activities
- Where does WHO work?
- Governing Bodies »
- World Health Assembly
- Executive committee
- Main page/
- Media Center /
- Newsletters/
- Read more/
- Child abuse
WHO/S. Becker
Becker
© Photo
\r\n
Magnitude of the problem
\r\n
\r\nChild maltreatment is a global problem with serious life-long consequences. Although studies have recently been carried out in some low- and middle-income countries, much data is still lacking.
\r\n
\r\nChild maltreatment is a complex and difficult issue to study. Available estimates vary widely depending on the country and the research method used. Grades depend on the following aspects:
\r\n
- \r\n
- applicable definitions of child abuse;\t \r\n
- type of child abuse being studied; \r\n
- statistical coverage and quality of official statistics; \r\n
- coverage and quality of surveys that require reports from victims themselves, parents or caregivers. \r\n
\r\n
\r\nHowever, international studies show that one quarter of all adults were physically abused as children, and that 1 in 5 women and 1 in 13 men were sexually abused as children. abuse. In addition, many children are victims of emotional (psychological) abuse and neglect. nine0285
abuse. In addition, many children are victims of emotional (psychological) abuse and neglect. nine0285
\r\n
\r\nAn estimated 41,000 murders of children under the age of 15 occur each year. This figure underestimates the true extent of the problem, as a significant proportion of child abuse deaths are incorrectly attributed to falls, burns, drowning, and other causes.
\r\n
\r\nIn armed conflict and refugee camps, girls are particularly vulnerable to sexual violence, exploitation and abuse by the military, security forces, other members of their communities, humanitarian workers and others. nine0285
\r\n
Consequences of child abuse
\r\n
\r\nChild abuse hurts children and families and can have long-term consequences. Abuse leads to stress, which is associated with impaired early brain development. Extreme stress can disrupt the development of the nervous and immune systems. As a result, in adulthood, people who were abused as children are at increased risk of behavioral and physical and mental health problems, such as:
As a result, in adulthood, people who were abused as children are at increased risk of behavioral and physical and mental health problems, such as:
\r\n
- \r\n
- committing or being a victim of violence;\t \r\n
- depression; \r\n
- smoking; \r\n
- obesity;\r\n \r\n
- high risk sexual behavior; \r\n
- unplanned pregnancy; \r\n
- Harmful use of alcohol and drugs. \r\n
\r\n
\r\nAs a result of these behavioral and mental health consequences, abuse can lead to heart disease, cancer, suicide, and sexually transmitted infections. nine0285
\r\n
\r\nIn addition to the health and societal impacts, child abuse also has economic impacts, including hospitalization costs, mental health care, child care, and long-term health costs.
\r\n
Risk factors
\r\n
\r\nRisk factors for child abuse have been identified. These risk factors are not present in all social and cultural settings, but they give a general idea when trying to understand the causes of child abuse. nine0285
These risk factors are not present in all social and cultural settings, but they give a general idea when trying to understand the causes of child abuse. nine0285
\r\n
Child
\r\n
\r\nIt is important to emphasize that children are victims and should never be blamed for abuse. Some individual characteristics of a child may increase the likelihood of abuse:
\r\n
- \r\n
- child under 4 years of age or adolescent;\r\n \r\n
- unwanted or not living up to parental expectations child; \r\n
- a child who has special needs, who cries constantly, or who has abnormal physical features. nine0005 \r\n
\r\n
Parents or caregivers
\r\n
\r\nSome characteristics of parents or caregivers may increase the risk of child abuse. Among them are the following:
\r\n
- \r\n
- difficulties associated with the newborn;\r\n \r\n
- leaving the child unattended; \r\n
- childhood abuse; \r\n
- ignorance of child development or unrealistic expectations; nine0005 \r\n
- harmful use of alcohol or drugs, including during pregnancy; \r\n
- involvement in criminal activity; experiencing financial difficulties friends and peers may increase the risk of child abuse, for example:
\r\n
- \r\n
- problems in the field of physical or mental health or development of any family member;\r\n \r\n
- discord in the family or violence between other family members; \r\n
- isolation from the community or lack of a supportive circle; \r\n
- lack of support in raising a child from other family members.
 \r\n
\r\n
\r\n
Community and social factors
\r\n
\r\nA number of characteristics of individual communities and communities can increase the risk of child abuse. They include:
\r\n
- \r\n
- gender and social inequality; \r\n
- lack of adequate housing or family support services and institutions; \r\n
- high levels of unemployment and poverty; \r\n
- easy access to alcohol and drugs; \r\n
- inadequate policies and programs to prevent child abuse, child pornography, child prostitution and child labor;\r\n \r\n
- social and cultural norms that support or glorify violence against others, favor the use of corporal punishment, require rigid gender roles, or diminish the status of the child in parent-child relationships; \r\n
- social, economic, health and educational policies that lead to poor living standards or socioeconomic inequality or instability.
 \r\n
\r\n
\r\n
Prevention
\r\n
\r\nChild maltreatment prevention requires a multisectoral approach. Effective programs are those that support parents and instill positive parenting skills. These include:
\r\n
- \r\n
- nurse home visits to parents and children for support, education and information;\r\n \r\n
- parent education, usually in groups, to improve skills raising children, increasing knowledge about child development and encouraging strategies for positively dealing with children; and \r\n
- multi-component activities, usually including parent support and education, early childhood education and childcare. \r\n
\r\n
\r\nOther prevention programs are also promising in some respects.
\r\n
- \r\n
- Abuse Head Injury Prevention Programs (also called Shaken Baby Syndrome and Inflicted Traumatic Brain Injury).
 These are usually hospital-level programs targeting young parents prior to their discharge, educating them about the dangers of shaken baby syndrome and recommending interventions for inconsolably crying babies. nine0005 \r\n
These are usually hospital-level programs targeting young parents prior to their discharge, educating them about the dangers of shaken baby syndrome and recommending interventions for inconsolably crying babies. nine0005 \r\n - Child sexual abuse prevention programs. They are usually held in schools and teach children about the following areas: \r\n
- ownership of one's body;\t \r\n
- the difference between good and bad touch; \r\n
- how to recognize threatening situations; \r\n
- how to say \"no\"; \r\n
- how to tell a trusted adult about abuse. nine0005 \r\n
- \r\n
\r\n
\r\nSuch programs are effective in enhancing protective factors against child sexual abuse (for example, knowledge about sexual abuse and protective behaviors), but data on whether such programs contribute to the reduction of other types of violence are not available.
\r\n
\r\nThe earlier in a child's life such activities are carried out, the more beneficial they are for the child (e.
 g. cognitive development, behavioral and social competence, educational training) and society (e.g. reduced delinquency) and crimes). nine0285
g. cognitive development, behavioral and social competence, educational training) and society (e.g. reduced delinquency) and crimes). nine0285 \r\n
\r\nIn addition, early recognition of cases, combined with ongoing care for child victims of abuse and their families, can help reduce re-abuse and its consequences.
\r\n
\r\nFor maximum impact, prevention and care interventions are recommended by WHO as part of a four-pronged public health approach:
\r\n
- \r\n
- identifying the problem;\r\n \r\n
- identifying causes and risk factors; \r\n
- development and testing of measures aimed at minimizing risk factors; \r\n
- disseminate information on the effectiveness of interventions and scale up proven effective interventions.\r\n \r\n
\r\n
WHO activities
\r\n
\r\nWHO in collaboration with a number of partners in the following areas:
\r\n
- \r\n
- provides evidence-based technical and normative guidance on child maltreatment prevention;\r\n \r\n
- calls for greater international support for child maltreatment prevention evidence-based children and investment in this area; \r\n
- provides technical support for evidence-based child abuse prevention programs in certain low- and middle-income countries.
 nine0005 \r\n
nine0005 \r\n
","datePublished":"2022-09-19T19:00:00.0000000+00:00","image":"https://cdn.who.int/media/images/default- source/imported/children-running-jpg.jpg?sfvrsn=50512cc9_2","publisher":{"@type":"Organization","name":"World Health Organization: WHO","logo":{"@ type":"ImageObject","url":"https://www.who.int/Images/SchemaOrg/schemaOrgLogo.jpg","width":250,"height":60}},"dateModified":" 2022-09-19T19:00:00.0000000+00:00","mainEntityOfPage":"https://www.who.int/ru/news-room/fact-sheets/detail/child-maltreatment","@context ":"http://schema.org","@type":"Article"}; nine0285
Key facts
- One in 5 women and 1 in 13 men report being sexually abused as children.
- The consequences of child maltreatment include lifelong physical and mental health damage, and its social and professional consequences can ultimately slow down the economic and social development of a country.
- Child maltreatment can be prevented - this requires a multisectoral approach.
 nine0005
nine0005 - Effective prevention programs can support parents and teach them positive parenting skills.
- Continued care for children and families can help reduce the risk of re-abuse and minimize its consequences.
Child abuse is the mistreatment and neglect of children under the age of 18. It covers all types of physical and/or emotional abuse, sexual abuse, neglect, neglect and commercial or other exploitation that results in actual or potential harm to the health, survival, development or dignity of the child in the context of a relationship of responsibility, trust or power. . Intimate partner violence is also sometimes considered a form of child abuse. nine0285
Magnitude of the problem
Child abuse is a global problem with serious lifelong consequences. Although studies have recently been carried out in some low- and middle-income countries, much data is still lacking.
Child abuse is a complex and difficult issue to study. Available estimates vary widely depending on the country and the research method used.
 Grades depend on the following aspects:
Grades depend on the following aspects: - applicable definitions of child abuse;
- type of child abuse being studied;
- coverage and quality of official statistics;
- coverage and quality of surveys that require reports from victims themselves, parents or caregivers.
However, international studies show that one quarter of all adults were physically abused as children, and that 1 in 5 women and 1 in 13 men were sexually abused as children. In addition, many children are victims of emotional (psychological) abuse and neglect. nine0285
An estimated 41,000 murders of children under the age of 15 occur each year. This figure underestimates the true extent of the problem, as a significant proportion of child abuse deaths are incorrectly attributed to falls, burns, drowning, and other causes.
In armed conflict and refugee camps, girls are particularly vulnerable to sexual violence, exploitation and abuse by the military, security forces, other members of their communities, humanitarian workers and others.
 nine0285
nine0285 Consequences of abuse
Child abuse causes suffering to children and families and can have long-term consequences. Abuse leads to stress, which is associated with impaired early brain development. Extreme stress can disrupt the development of the nervous and immune systems. As a result, in adulthood, people who were abused as children are at increased risk of behavioral and physical and mental health problems, such as:
- committing violence or becoming a victim of violence;
- depression;
- smoking;
- obesity;
- high risk sexual behavior;
- unplanned pregnancy;
- harmful use of alcohol and drugs.
As a result of these behavioral and mental health consequences, abuse can lead to heart disease, cancer, suicide, and sexually transmitted infections. nine0285
In addition to health and societal impacts, child maltreatment also has economic impacts, including the cost of hospitalization, mental health treatment, child care, and long-term health costs.
Risk factors
Risk factors for child abuse have been identified. These risk factors are not present in all social and cultural settings, but they give a general idea when trying to understand the causes of child abuse. nine0285
Child
It is important to emphasize that children are victims and should never be blamed for abuse. Certain individual characteristics of a child may increase the likelihood of abuse:
- child under 4 years of age or adolescent;
- an unwanted child or a child that does not live up to the expectations of the parents;
- a child with special needs, constant crying or abnormal physical features.
Parents or caregivers
Certain characteristics of parents or caregivers may increase the risk of child abuse. Among them are the following:
- difficulties associated with the newborn;
- leaving a child unattended;
- childhood abuse;
- ignorance of child development or unrealistic expectations;
- harmful use of alcohol or drugs, including during pregnancy; nine0005
- involvement in criminal activity;
- experiencing financial difficulties.
Relationships
A number of factors in family relationships or between sexual partners, friends and peers can increase the risk of child abuse, for example:
- a family member's physical or mental health or developmental problems;
- discord in the family or violence between other family members; nine0005
- isolation in the community or lack of a support circle;
- lack of support in raising a child from other family members.
Community and social factors
A number of characteristics of individual communities and communities can increase the risk of child abuse. They include:
- gender and social inequality;
- Lack of adequate housing or family support services and institutions; nine0005
- high levels of unemployment and poverty;
- easy access to alcohol and drugs;
- inadequate policies and programs to prevent child abuse, child pornography, child prostitution and child labor;
- social and cultural norms that support or glorify violence against others, favor the use of corporal punishment, require rigid gender roles, or degrade the status of the child in parent-child relationships; nine0005
- social, economic, health and educational policies that lead to poor living standards or socioeconomic inequality or instability.
Prophylaxis
A multisectoral approach is needed to prevent child maltreatment. Effective programs are those that support parents and instill positive parenting skills. These include:
- home visits by nurses to parents and children for support, education and information; nine0005
- Parent education, usually in groups, to improve child-rearing skills, increase knowledge of child development, and encourage positive child-care strategies; and
- multi-component activities, usually including parent support and education, early childhood education and childcare.
Other prevention programs are also promising in some respects.
- Abuse head injury prevention programs (also called shaken baby syndrome and traumatic brain injury). These are usually hospital-level programs targeting young parents prior to their discharge, educating them about the dangers of shaken baby syndrome and recommending interventions for inconsolably crying babies.
 nine0005
nine0005 - Child sexual abuse prevention programs. They are usually held in schools and educate children in the following areas:
- ownership of one's body;
- difference between good and bad touches;
- how to recognize threatening situations;
- how to say "no";
- how to talk about abuse to a trustworthy adult.
Such programs are effective in increasing protective factors against child sexual abuse (eg, knowledge about sexual abuse and protective behaviours), but there is no data on whether such programs reduce other types of violence. nine0285
The earlier in a child's life such interventions are, the more beneficial they are for the child (eg cognitive development, behavioral and social competence, educational training) and society (eg reduction in delinquency and crime).
In addition, early recognition of cases, combined with continued care for child victims of violence and families, can help reduce re-abuse and its consequences.
 nine0285
nine0285 For maximum impact, prevention and care interventions are recommended by WHO as part of a four-step public health approach:
- problem definition;
- determination of causes and risk factors;
- development and testing of measures aimed at minimizing risk factors;
- disseminate information on the effectiveness of interventions and scale up proven effective interventions. nine0005
WHO activities
WHO is collaborating with a number of partners in the following areas:
- provides evidence-based technical and normative guidance on child maltreatment prevention;
- calls for increased international support for and investment in evidence-based child abuse prevention;
- provides technical support for evidence-based child abuse prevention programs in selected low- and middle-income countries. nine0005
Consequences of child abuse
Child abuse can have various types and forms, but their consequences are always: serious damage to the health, development and communication of the child, often a threat to his life up to death.
Define 4 types of child abuse :
- neglect of the basic needs of children;
- emotional (or psychological) abuse; nine0755 - physical abuse;
- sexual assault.
Neglect is the chronic failure of a parent to provide for a child's basic needs of food, clothing, shelter, medical care, education, protection and supervision. Children are characterized by: developmental delay, learning problems, low self-esteem, passivity, low social intelligence.
Emotional (or psychological) abuse of a child is any action that causes a state of emotional stress in a child. Emotional abuse includes:
- rejection of the child, rejection and constant criticism;
- insult or humiliation of his human dignity;
- threats, accusations against the child;
- social isolation, i.e. coercion to loneliness;
- prolonged deprivation of the child of parental love, care.
This type of violence also includes constant lying, deception of a child, making demands on a child that do not correspond to his age capabilities.
Most often, children from families for whom violence is a lifestyle experience emotional abuse; from families with authoritarian parents; with such a parenting style as overprotection. nine0749
In preschoolers and younger schoolchildren, emotional abuse leads to a delay in psychoverbal development and growth, to sleep and appetite disorders, and may manifest itself in the presence of bad habits. Often there are skin rashes, allergic pathology. Neuropsychiatric diseases often develop: tics, stuttering, enuresis. Adolescents may experience: leaving home, chronic academic failure, low self-esteem, neurosis, deviant behavior, depression.
Physical abuse - any non-accidental injury, bodily harm to a child.This type of abuse can manifest itself in the form of beatings, concussions, blows, slaps, bites, intentional burns, grinding, trauma.
 It also includes the involvement of the child in the use of drugs, alcohol.
It also includes the involvement of the child in the use of drugs, alcohol. The effects of physical abuse are always visible on the child's body. These can be: inexplicably occurring bruises, scars, traces of binding and blows, burns, hemorrhages, grinding of bones, dislocations. nine0749
Physical abuse can cause serious disorders not only of physical but also mental health, developmental delays.
Sexual abuse - an illegal act, forcing a child into any sexual relationship against his will and will. Sexual abuse committed against a child is one of the most severe psychological traumas in terms of its consequences.In the case of sexual abuse, both physical signs of what happened (bruising, abdominal pain, headache, venereal disease, pregnancy) and changes in the behavior of the child can be detected. Some children become withdrawn, depressive, others are characterized by hysterical behavior, outbursts of anger. But everyone has difficulties in communicating with peers.