Dealing with schizophrenic parent
Top 3 Tips for Balancing Support With Self-Care – BrightQuest Treatment Centers
September 20, 2017, Elisabet KvarnstromBrightQuest Treatment Centers
Growing up with a parent with schizophrenia can have a profound impact on how you see yourself and the world around you. The challenges faced by the adult children of people with schizophrenia are myriad, but by educating yourself, seeking support for yourself, and finding treatment for you parent, you can create new paths toward healing and realize that you are not alone.
Many adult children who have a parent with schizophrenia fear their own potential for developing the same disorder. They may even blame their parent for their illness, believing that if they were stronger, more resilient, they might not have become ill in the first place.
Of course, the truth is that schizophrenia is not a result of weakness or a fault in character. It is a disease of the brain, one that requires compassionate support to cope with—and if you are the child of a parent with schizophrenia, you are one of the most important potential sources of the very love and understanding your parent needs in order to heal.
The Challenges of Having a Parent with Schizophrenia
As a child of a parent with schizophrenia, it is likely that you were profoundly affected by your experience of growing up with a sick parent. Now, as an adult, you are not only left grappling with the wounds the illness inflicted during your formative years, but you must now negotiate the complex dynamics of being the adult child of someone with a severe mental health disorder.
Learning how to balance support with self-care can be a challenging process that can drain your emotional resources and leave you feeling disoriented and isolated, particularly if your parent’s illness remains untreated. But you are not alone in your struggle, and with the right resources you can find the support that you need to nurture both yourself and your parent. Using the following three tips, you can start to formulate a plan for moving toward a healthier future for both of you.
1. Educate Yourself
When you grow up with a parent with schizophrenia, it’s easy to feel as if you know everything you need to know about the disorder. When you’ve spent your life witnessing the embodiment of the illness firsthand, what could someone possibly tell you that you don’t already know?
When you’ve spent your life witnessing the embodiment of the illness firsthand, what could someone possibly tell you that you don’t already know?
The truth is that even people who living in the presence of mental illness sometimes don’t fully understand what their loved one is experiencing, particularly when their observations are clouded by their own complicated emotional reactions to their parents’ symptoms. By learning more about schizophrenia with the help of experts, you can come to more fully understand how the illness functions and develop a more accurate perception of your parent’s experience as well as your own. This can be essential to cutting through the anger, shame, fear, and sadness that is so common amongst children of schizophrenic parents. It also gives you an opportunity to identify what both of you truly need in order to heal.
For instance, many children of parents with schizophrenia experience anger and frustration if their parent refuses to take medication, seeing non-adherence as a sign that the parents doesn’t care enough about them try to get better. However, in many cases, non-adherence arises out of a condition called anosognosia, or “lack of insight”, a neurological deficit that prevents people from recognizing that they are ill. About 50% of people with schizophrenia experience anosognosia, often resulting in treatment refusal. By understanding that nonadherence is the product of the illness itself—not a comment on the quality of your parents’ love for you—you can let go of blame, identify the true source of the problem, and work toward resolution.
However, in many cases, non-adherence arises out of a condition called anosognosia, or “lack of insight”, a neurological deficit that prevents people from recognizing that they are ill. About 50% of people with schizophrenia experience anosognosia, often resulting in treatment refusal. By understanding that nonadherence is the product of the illness itself—not a comment on the quality of your parents’ love for you—you can let go of blame, identify the true source of the problem, and work toward resolution.
2. Seek Support for Yourself
Having a parent with schizophrenia can have a profound impact on your sense of self and your place in the world, deeply influencing your emotions, beliefs, behaviors, and relationships. As Herbert, Manjula, and Philip write:
[Children with mentally ill parents] tend to have social deficits characterized by emotional instability, aggressiveness, and social isolation, difficulties in work, marriage, and struggle with issues related to poor self-esteem, and social adjustment.
Studies showed that […] they reported having inadequate parenting, excessive care giving to the mentally ill parents, stigma, and lack of support from others.
At the same time, having a parent with schizophrenia heightens the risk of developing a mental illness yourself; according to some preliminary estimates, children of parents with schizophrenia have a 50% chance of developing a mental health disorder in their lifetime, although most will not develop schizophrenia specifically. If you have one parent who has schizophrenia, your chance of developing the illness yourself is 12%. That number jumps to 39% if you have two parents with schizophrenia. Research shows also shows a strong correlation between schizophrenia and substance abuse. While there is no conclusive evidence that substance abuse can
cause schizophrenia, it may be particularly dangerous for people with increased risk of schizophrenia, such as children of people with the illness, to abuse drugs and alcohol.
It is essential to seek out a support network for yourself in order to cope with the effects of having a parent with schizophrenia, help you process and heal from your experiences, and address any mental health issues you may be experiencing yourself. Ideally, this support network should include a therapist with experience working with the adult children of people with schizophrenia.
You may also wish to seek out a support group designed specifically for people in your situation to benefit from the guidance and understanding of peers who have been where you are, free from stigma and shame. This not only helps you to cope with the effect your parent’s illness has had on your life, it also allows you to better support them in the future while keeping yourself safe.
3. Find Help for Your Parent
Today there are more treatment options available for schizophrenia than ever before, including pharmacological, psychotherapeutic, holistic, and experiential modalities that can open up the door to profound transformation. Helping your parent connect to caring and compassionate treatment providers can be a vital step toward finding a resolution to psychiatric distress.
Helping your parent connect to caring and compassionate treatment providers can be a vital step toward finding a resolution to psychiatric distress.
However, if your parent has failed to respond to various forms of treatment over the years there it may seem like there are few places to turn. Indeed, the outpatient therapy, hospitalizations, and short-term treatment programs that your parent has cycled in and out of may not offer them the kind or quality of care they need to make progress toward a more stable and independent life. In these cases, long-term residential treatment for schizophrenia may be the best option. Long-term residential care facilities can offer the structure and therapies necessary to help your parent gain the skills necessary to effectively manage their illness and their life. By engaging in a comprehensive array of therapies within a therapeutic community, they can come to develop the emotional and behavioral regulation they need to minimize symptoms and augment self-sufficiency.
Because schizophrenia affects the entire family, it is essential to find a long-term treatment program that will work with your family to support you individually and collectively and give you a safe space to heal. Through family therapy, psychoeducation, and family support groups, you can participate in your parent’s care while simultaneously addressing your own unique challenges and working to resolve painful conflicts. You will also be a part of continuing care planning to ensure that the gains you and your parent have made in treatment are preserved once residential care is complete.
Begin Your Recovery Journey Today.
619-466-0547Our Unique Treatment Model can Help
Visit Our Program Page
You Are Not Alone
Having a parent with schizophrenia can be an isolating, sad, frustrating, and disorienting experience. However, there are resources out there to help you both understand and cope with the impact of mental illness and create a strong foundation for ongoing wellness. Don’t be afraid to reach out to ask for support; there is a community of people who have been where you are and who can give you the guidance you need to move forward with love, compassion, and dignity.
Don’t be afraid to reach out to ask for support; there is a community of people who have been where you are and who can give you the guidance you need to move forward with love, compassion, and dignity.
Treatment at BrightQuest
BrightQuest Treatment Centers provide world-class residential treatment for schizophrenia and other complex mental illnesses. We know that choosing the right treatment option for yourself or a loved one is difficult. We believe our unique model of care gives our clients the best chance at success.
- Family Integration in Treatment
- Inclusive Therapeutic Community
- Focus on Lasting Behavioral Change
We offer clients the tools, skills, and support necessary to attain greater stability and independence with the confidence and courage to live a healthy, happy, and productive life.
Here's How to Live with a Mother Who Has Schizophrenia
Schizophrenia is a serious mental health condition that can present challenges for family members.
A mental health diagnosis affects not only the individual but their loved ones, too. If you’re the child of a mother who lives with schizophrenia, there are several specific challenges you may face.
Language matters
Sex and gender exist on a spectrum. We use “women,” “mother,” and “mom” in this article to reflect the terms assigned at birth or what you might call them. However, your parent’s gender is solely about how they identify themself, independent of their physical body.
Schizophrenia is a mental health condition that distorts a person’s thoughts, behaviors and perceptions. Because it causes a detachment from reality, its symptoms can be very debilitating, making it hard to accomplish everyday tasks.
A person with schizophrenia may experience the world completely differently from others, which could create distance between them and their loved ones.
Schizophrenia is also one of the most misunderstood and stigmatized mental health conditions.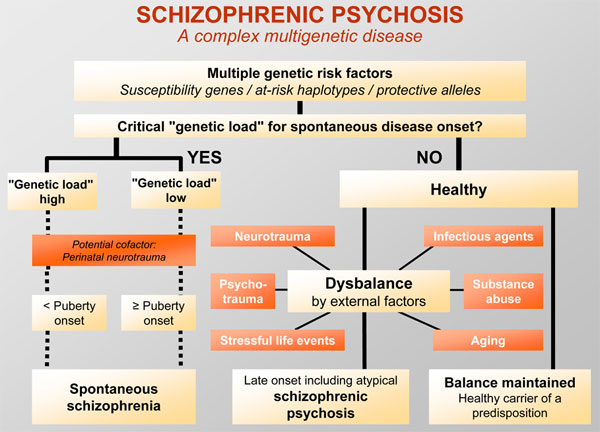 The myths surrounding the illness can create additional challenges for the person and their family.
The myths surrounding the illness can create additional challenges for the person and their family.
If your mom has schizophrenia, it’s natural to find yourself overwhelmed by all kinds of feelings. You may feel scared, sad, or angry. You might resent her for not being like other parents, or try to avoid spending time together. You may even fall into the role of the caregiver, trying to “fix” them.
There’s no right or wrong way to respond to your situation, all your emotions are natural and you’re not the only one. But there are some sound strategies you can use to help navigate your parent’s diagnosis.
Schizophrenia affects roughly 1% of people in the United States. It develops later in women than men, on average – typically during the late teens to early 20s for men and during the late 20s to early 30s for women.
Schizophrenia can look very different from one person to the next. But getting familiar with the broad symptoms can help you to understand your parent’s behavior.
According to the DSM-5, a diagnosis of schizophrenia requires at least 2 of the following symptoms for a period of at least one month:
- Hallucinations: Hearing, seeing or experiencing things that aren’t really there. Auditory and visual hallucinations are both common in schizophrenia, but other senses can also be involved.
- Delusions: A strongly-held belief in something that is provably false. Some people believe they are being pursued, targeted or influenced by outside forces, while others may think that they have superpowers or have been chosen for a special purpose.
- Disorganized speech: Incoherent, rambling speech that moves quickly from one subject to another and may be hard for others to follow. This is sometimes called “word salad.”
- Disorganized behavior: This can include catatonic symptoms, and problems with motor function.
- Negative symptoms: The absence of a trait that would otherwise be present, such as emotions, speech, engagement with others, and motivation.
Schizophrenia is an incredibly complex condition which can manifest in various ways. Having schizophrenia does not mean someone can’t be a loving and functional parent, particularly if the condition is being treated.
But because the condition impacts a person’s functioning, moods and emotional well-being, it will inevitably affect their children too.
In a 2021 study, researchers at the University of Manchester examined the “emotional climate” of families where one parent has schizophrenia.
They did this by focusing on emotional expression and parenting practices in parents with schizophrenia versus parents without serious mental health conditions.
The study showed that parents with schizophrenia displayed more hostility toward their children, and were more critical and blaming of their children.
An older study from 2013 focused on the experiences of a small group of adults who had grown up with a parent with schizophrenia.
While most of the participants (70%) were satisfied with the parenting they’d received, many reported that the condition had affected their lives.
In particular, 66% of the participants said they’d felt burdened by their parent’s condition, and 40% said that they experienced a lack of support from their parent with schizophrenia.
It’s important to know that you shouldn’t have to take responsibility for your parent’s mental health – especially if you’re a minor.
If your parent has schizophrenia or is exhibiting symptoms of the condition and is unwilling or unable to seek help, it’s a good idea to speak to a trusted adult about the situation.
This could be:
- another parent or relative
- a teacher
- a guidance counselor
- a therapist
When you have a parent with mental illness, it’s natural to feel protective of them and perhaps even feel under pressure to keep their condition a secret.
The stigma around schizophrenia can make it feel very scary. But the reality is that there are very effective treatments available which can help your mom to live a fulfilling and productive life:
Medications: Antipsychotic drugs are the first-line treatment for schizophrenia. They can reduce or eliminate symptoms like delusions and hallucinations and can also reduce the likelihood of relapse.
They can reduce or eliminate symptoms like delusions and hallucinations and can also reduce the likelihood of relapse.
Therapy: Psychotherapy can reduce stress and help to address negative thought patterns. Cognitive behavioral therapy (CBT) has been shown to be effective for schizophrenia because it can help a person to gain perspective on their thoughts and reduce the power of symptoms like delusions.
These are things they’d be introduced to by a doctor and mental health team after a diagnosis or hospitalization.
What you can manage is how you educate yourself about the condition and the support system you create. You can benefit from creating a mental health crisis plan either with your parent or a trusted adult.
You might also bookmark our schizophrenia hub for all sorts of insight.
Like many mental health conditions, schizophrenia is hereditary to some extent. The lifetime chances of developing the condition is:
- 1% for the general population
- 6.
 5% in people who have a first-degree relative with the condition — such as a parent
5% in people who have a first-degree relative with the condition — such as a parent
However, this still means that most people who have a parent with schizophrenia don’t develop the condition.
A note on genetic predispositions
Your genes play a role in whether you will develop some mental or physical health conditions, but they’re only one piece of the puzzle.
Epigenetics is the study of how the DNA you inherit does or does not manifest in you. This means that any genetic predispositions that run in your family can stay inactive or can even be reversible when signs show up early.
Research from 2016 suggests that the condition is often caused by a combination of genetic and environmental factors. It’s possible, for example, that the stress of taking care of a parent with mental illness could play a role in activating the condition, rather than genetic predisposition alone.
Schizophrenia can be an incredibly isolating condition for the person who has it and for their loved ones. And because of how stigmatized the condition is, you may find it difficult to know where to turn or find support.
And because of how stigmatized the condition is, you may find it difficult to know where to turn or find support.
The National Alliance on Mental Illness (NAMI) is a great resource for the families of those with mental health conditions. There are support groups nationwide where relatives can gather and support each other.
Teen Line is another great resource for young people –— it’s a hotline staffed by teenage counselors and provides a safe, confidential space to talk about anything on your mind.
Many children with a parent who has mental health conditions fall into the role of the caretaker. But it’s also important to take care of yourself –— ensuring that you get enough sleep, eat well, and prioritize your mental health.
What worries the relatives of people with schizophrenia
Pharmaceutical company Gedeon Richter, together with VTsIOM, presented a study on how relatives of people with schizophrenia feel. The study is timed to coincide with World Mental Health Day, which is celebrated on October 10.
Evgenia Fedorova Health, Human Rights 08.10.2019
Photo: Jack Finnigan, UnsplashBack in the summer, on June 4, VTsIOM published data from a survey on mental disorders and schizophrenia, conducted in partnership with a pharmaceutical company. Then 90% of respondents reported that they are aware of schizophrenia: among them, 83% believe that it is difficult for relatives of people with schizophrenia to tell others about the diagnosis, 75% - that such families lack support and mutual assistance, and 73% - that caring for loved ones with schizophrenia takes a lot of time and effort. 20% of respondents said that there are people with schizophrenia in their environment.
Then Gedeon Richter and VTsIOM conducted another study in the form of an online forum, in which residents of several large Russian cities took part anonymously.
“Hurt and ashamed”
According to this survey, people whose loved ones were diagnosed with schizophrenia felt “pained and ashamed” because of prejudices and ambiguous attitudes towards the topic of mental health in society. Every third respondent of the VTsIOM survey (38%) felt that people with schizophrenia “should stay away from others.”
Every third respondent of the VTsIOM survey (38%) felt that people with schizophrenia “should stay away from others.”
“Prejudices are in the air: that such patients can harm themselves and others, that they should be kept in psychiatric hospitals, preferably in straitjackets, that they should be isolated from society, since it is not known what to expect from them. That they have a constant grimace on their face, and their appearance is repulsive, ”writes one of the participants in an anonymous online forum.
Relatives of people with schizophrenia also noted changes in their lifestyle: due to caring for a person with schizophrenia, they were forced to adjust their work schedule, change jobs (or leave them) and control their free time.
“My life is at a standstill. And the control of taking the pills required my presence strictly and without gaps. In general, I spent all my free time at home. No entertainment and no personal life, ”says another participant in the online forum.

Among the difficulties noted by relatives of people with schizophrenia were also emotional changes: they needed to learn to be patient with their loved ones, not to give up.
“All of us in the family live according to our son's daily routine. Eating at a certain time, you have to watch the programs that he watches. If he asks to turn on the radio, and at this time someone wants to listen to something else, then we cede the right to choose to him. The schedule of the second child is also drawn up taking into account the daily routine of the son, ”says the mother of a child with schizophrenia.
Relatives need support
Relatives of people with schizophrenia need support, information, legal and medical measures to improve their quality of life. 45% report difficulties with medications.
“Relatives of patients with schizophrenia expect comprehensive support from the professional community, including their expectations from pharmaceutical companies to develop effective and safe drugs and ensure their availability. Today, in partnership with the expert community, we are working on the creation of information and educational projects to improve the quality of life of patients' relatives,” says doctor Attila Varadi , authorized representative of Gedeon Richter in Russia.
Today, in partnership with the expert community, we are working on the creation of information and educational projects to improve the quality of life of patients' relatives,” says doctor Attila Varadi , authorized representative of Gedeon Richter in Russia.
Relatives of people with schizophrenia agreed that the difficulties they face are largely due to the stigmatization of mental disorders.
“A person lives life, not a disease”
ASI asked Svetlana Beilezon , vice-president of the Interregional public organization for helping children with psychoverbal developmental disabilities and their families “Road to the World”, what could help avoid stigmatization .
“We need open information that catches the eye of people everywhere - like advertising on TV or information leaflets in public places, clinics, schools and social services, on the Internet: they say, if you have such and such problems (indirectly describe signs of mental disorders), remember that you are not alone! Call the hotline or visit a support club in your area, or you can consult a doctor at a dispensary or a private clinic,” Beileson said.
But, in her opinion, this will not be limited to one call, because these prevention and support programs should really appear at the place of residence - accessible and not intimidating with an official sign with scary words about psychiatry, complex paperwork and white coats. At this stage, probably, clinical psychologists can be the main supporting specialists, who will assess the likelihood of the disease and risks, calm the person or his anxious relatives and give the first recommendations on where to turn.
According to Beileson, people without an official diagnosis could also come to such places so that the stigma does not arise and the person begins to be treated.
For those who cannot work or study now, leisure programs or useful daytime employment are needed, and also at the place of residence: a person lives a life, not a disease, and as soon as the disease recedes a little, he should have the opportunity to be with people and engage in interesting or necessary work.
Relatives of people with schizophrenia benefit from "social respite" programs, according to Beileson.
“Someone could sit or take a walk with a person with a mental disorder if he is sad, so that his relatives can go to visit, to the doctor, to the theater. A person may be in a state that is not dangerous to health and to others, but his relatives may be ashamed to leave him, ”the expert says. “The most important thing is that such programs appear close to home and be available without a long formalization.”
Help
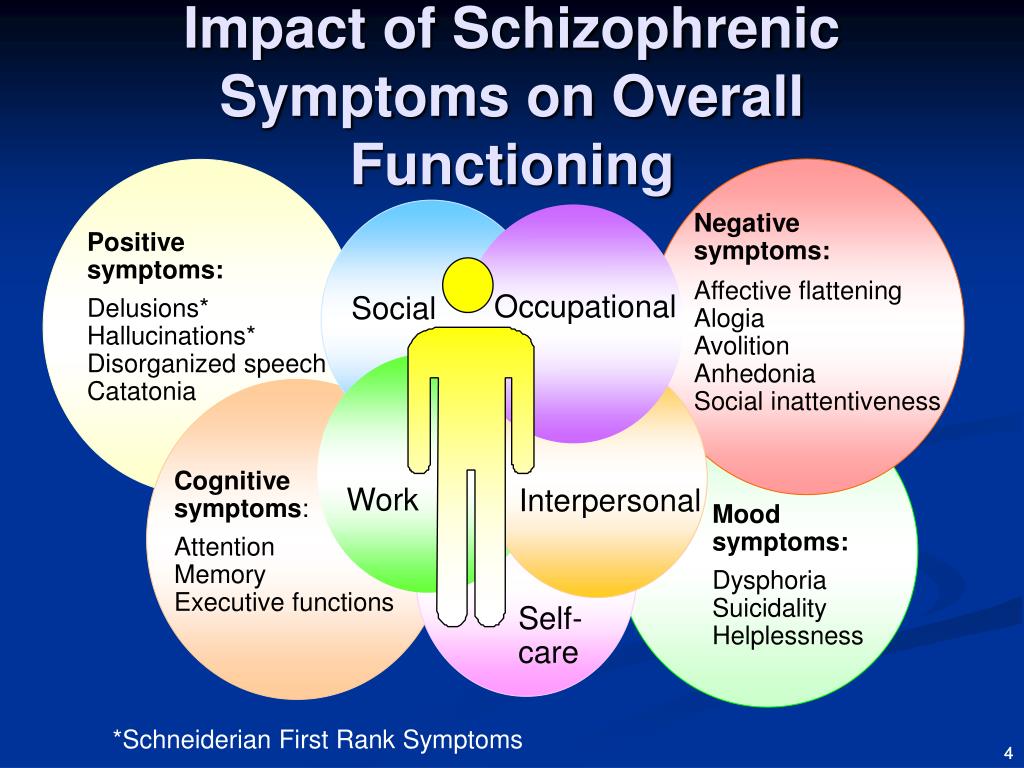
Schizophrenia is a chronic and disabling mental illness characterized by impaired thinking and perception. According to statistics, about 1% of the world's population suffers from it, both men and women are equally susceptible to it. Symptoms of the disease fall into three main categories. These are positive - hallucinations, delusions, mental and motor disorders; negative - loss of motivation, apathy, scarcity of speech, asociality. There are also cognitive symptoms - disorders of thinking, perception, memory and attention.
There are also cognitive symptoms - disorders of thinking, perception, memory and attention.
Subscribe to telegram channel ASI .
Dear readers, colleagues, friends of ASI.
Your support is very important to us. Together we can make the news better and more interesting.
Contribute
Recommended
Don't be left out of life
Tatyana Safyannikova, founder of the Russian House Center for Social Initiatives, talks about how to help a person with a mental illness make their life more complete and why it is important…
Cope with fear: four projects to help Muscovites
Hotlines, psychological counseling and support groups: ASI has compiled a selection of non-profit organizations that provide emergency psychological assistance to those who need it.
Recommended
Newsletter subscription
The latest news and our best materials in your mailbox
Subscribe by email
Announcements
-
South Ural Civil Forum
Tue, 29.
 11.2022, 08:00 Chelyabinsk
11.2022, 08:00 Chelyabinsk -
Telekino competition "Native paths-2022"
Tue, 29.11.2022, 13:30 Moscow
-
Training "Environmental journalism: simple about the complex"
Wed, 11/30/2022, 09:30 Moscow
-
Webinar “Development of social fashion photography. Social project Soul Gohar»
Wed, 30.11.2022, 12:00 Online
-
VII National Forum of the Rehabilitation Industry and Universal Design "Hope for Technology"
Wed, 30.11.2022, 10:30 Moscow
All events
Send news
Editor's choice
Communication in schizophrenia //Psychological newspaper
The description of schizophrenia, like any other mental illness, is a description of its symptoms that develop into their more complex complexes - syndromes that follow each other with a certain sequence, giving us the opportunity to talk about a particular diagnosis. It is possible to talk about certain objectively detectable symptoms of mental disorders by describing the patient's behavior in the context of a particular situation, communication with a particular person. From the point of view of communication theory, communication can be recognized as a symptom of a mental disorder if two criteria are met: a) the person's behavior must be unusual in a given situation for a given culture, and b) it occurs involuntarily. It should also be noted that in any act of communication there is both a verbal component (what is specifically said) and a non-verbal component - facial expressions, gestures, features of voice intonation, as well as the context of communication, and information about the content of communication is transmitted simultaneously through all these channels. Of great importance in communication is the fact whether the information transmitted through all these channels is uniform (for example: a girl who invited a young man to her home greets him with an affectionate voice, smiles, and in response to his hug clings to him) - this the option is called congruent communication, in which the attitude towards the interlocutor is determined unambiguously, or different (in response to the young man's attempt to hug the girl in this situation, she says that she does not want this, but does it in a gentle voice and her body rushes to him).
From the point of view of communication theory, communication can be recognized as a symptom of a mental disorder if two criteria are met: a) the person's behavior must be unusual in a given situation for a given culture, and b) it occurs involuntarily. It should also be noted that in any act of communication there is both a verbal component (what is specifically said) and a non-verbal component - facial expressions, gestures, features of voice intonation, as well as the context of communication, and information about the content of communication is transmitted simultaneously through all these channels. Of great importance in communication is the fact whether the information transmitted through all these channels is uniform (for example: a girl who invited a young man to her home greets him with an affectionate voice, smiles, and in response to his hug clings to him) - this the option is called congruent communication, in which the attitude towards the interlocutor is determined unambiguously, or different (in response to the young man's attempt to hug the girl in this situation, she says that she does not want this, but does it in a gentle voice and her body rushes to him). The second option is called incongruent communication, and the young man has to guess what is really meant: whether to accept the girl’s verbal message that she does not want more intimate communication as truth, or, neglecting her words, behave even more insistently, considering that it is the intonation and movement of the body, as well as the context of the situation - after all, the girl herself invited him to visit - are more significant (118).
The second option is called incongruent communication, and the young man has to guess what is really meant: whether to accept the girl’s verbal message that she does not want more intimate communication as truth, or, neglecting her words, behave even more insistently, considering that it is the intonation and movement of the body, as well as the context of the situation - after all, the girl herself invited him to visit - are more significant (118).
It should be emphasized here that no kind of communication occurs by chance. In psychology, as in economics, only those processes are preserved that bring some kind of, way and perverted, benefit. Both congruent and incongruent communication pursue their goals to achieve some specific behavior from the interlocutor (even if this intention is not realized by the person himself). For example, it can be assumed that in the second case, the true goal of the girl is to inflame the feelings of the young man. In addition, in the process of communication, information about the internal state of a person is always transmitted - valuable feedback, without which no systematic interaction is possible. Working with severe personality disorders and schizophrenia, we very often see how the whole process of intra-family communication is permeated with “double binds”. Selvini Palazzolli described the style of communication in such families as follows: “Everyone is desperate to seize the right to determine the relationship, and everyone keeps testing his position again and again, thus constantly exposing himself to the risk of defeat. However, arrogance, this hypertrophied pride, nests in each of the spouses and cannot accept defeat. Failure (or even the possibility of it) is utterly unbearable and must be prevented at all costs. Avoiding the conflict does not solve the problem in itself, in this case it is tantamount to admitting defeat. The fight must continue, but without risk to the opponents. And they find the only way out - avoiding any definition of relationships. Each must disqualify his definition of relationship before the other gets a chance to do so.” (122).
Working with severe personality disorders and schizophrenia, we very often see how the whole process of intra-family communication is permeated with “double binds”. Selvini Palazzolli described the style of communication in such families as follows: “Everyone is desperate to seize the right to determine the relationship, and everyone keeps testing his position again and again, thus constantly exposing himself to the risk of defeat. However, arrogance, this hypertrophied pride, nests in each of the spouses and cannot accept defeat. Failure (or even the possibility of it) is utterly unbearable and must be prevented at all costs. Avoiding the conflict does not solve the problem in itself, in this case it is tantamount to admitting defeat. The fight must continue, but without risk to the opponents. And they find the only way out - avoiding any definition of relationships. Each must disqualify his definition of relationship before the other gets a chance to do so.” (122).
Thus, any psychiatric symptom that manifests itself in any behavior can also be considered as a way of unconscious manipulation of others. Neurotic symptoms in this respect are built more simply, and it is not for nothing that one of the signs of neurosis is the situational secondary benefit from neurotic behavior that is relatively easily detected by a psychiatrist (for example, the widespread headache of wives, which helps, while maintaining their status as a wife, to avoid intimate relationships with an unloved husband). With schizophrenic symptoms, the situation is more complicated.
Neurotic symptoms in this respect are built more simply, and it is not for nothing that one of the signs of neurosis is the situational secondary benefit from neurotic behavior that is relatively easily detected by a psychiatrist (for example, the widespread headache of wives, which helps, while maintaining their status as a wife, to avoid intimate relationships with an unloved husband). With schizophrenic symptoms, the situation is more complicated.
J. Haley described the essence of schizophrenic behavior as the avoidance of a clear definition of one's behavior and intentions in order, on the one hand, to make one's communication more effective using unconscious mechanisms, on the other hand, to avoid responsibility for one's actions and in any case remain innocent and good for all.
Any appeal of one person to another can be schematically described as follows:
1. I am
2. report something
3. you
4. in this situation
There are many ways to avoid defining your behavior when addressing someone. For example:
For example:
1. In order to deny that it is this person who is addressing the interlocutor, you can call yourself by some other name, for example, introduce yourself as Stalin or a Martian, or say that God (and not himself) speaks through his mouth. It can also be said that the statement was made involuntarily when a person could not control himself - under the influence of alcohol or by order of "voices". In addition, the conversion can be performed in the form of some symbolic physiological action (for example, urination, defecation, or yawning), as if in fact it was not a conversion at all, but the manifestation of some physiological process.
2. The easiest way to deny that a person said something is amnesia. In addition, for this it can be stated that he misunderstood the interlocutor and had in mind something completely different. It is also possible to invent your own language, or communicate in such a way that verbal and non-verbal communication contradict each other (for example, saying "I'm glad to see you" in a dull tone with a wistful expression). In addition, to deny your behavior, you can plunge into a trance state. When a hypnotic in a trance is suggested that his hand becomes lighter and begins to rise higher and higher on its own, and this happens, then later on the question of how this happened, the patient will answer with sincere surprise that the hand really did rise on its own in addition to his will. However, on the other hand, who could raise a hand except the patient himself?
In addition, to deny your behavior, you can plunge into a trance state. When a hypnotic in a trance is suggested that his hand becomes lighter and begins to rise higher and higher on its own, and this happens, then later on the question of how this happened, the patient will answer with sincere surprise that the hand really did rise on its own in addition to his will. However, on the other hand, who could raise a hand except the patient himself?
Similar phenomena occur in schizophrenia. Even Pavlov, in his article "A Trial Excursion of a Physiologist into the Field of Psychiatry", noted the extreme similarity from the point of view of physiologists between schizophrenic psychosis and hypnotic trance: "it can hardly be doubted that schizophrenia in certain variations and phases really represents chronic hypnosis" (167 ). The same point of view is expressed by Ericksonian hypnotherapists, for example, M. Erickson (9), S. Gilligan (10). It is worth remembering that the hypnotic trance differs from the waking state precisely in the focus of consciousness. In the waking state, it is focused outward, and in trance it is focused on the inner world of a person, his feelings, sensations and visual images. Deep, persistent withdrawal into oneself, one's experiences during the devaluation (i.e., refusal to define the relationship) of the real things of the outside world is one of the characteristic signs of schizophrenia.
In the waking state, it is focused outward, and in trance it is focused on the inner world of a person, his feelings, sensations and visual images. Deep, persistent withdrawal into oneself, one's experiences during the devaluation (i.e., refusal to define the relationship) of the real things of the outside world is one of the characteristic signs of schizophrenia.
3. In order to deny that a person is addressing any particular interlocutor, you can start talking aloud to yourself, or call the interlocutor by a different name. In addition, you can say that the interlocutor (let's say a neighbor) is not the one he claims to be, but a secret FSB officer, and, accordingly, start talking to him not as a neighbor, but as a secret FSB officer, which, again However, it excludes the possibility of determining the true nature of the relationship.
4. You can deny the situation in which the conversation is being conducted by violating the orientation in place, time and situation. In addition, you can begin to transfer past experiences into the present and future ("no one could help me - and you will not help").
In addition, you can begin to transfer past experiences into the present and future ("no one could help me - and you will not help").
In studies by G. Bateson's group (46), this kind of communication, built according to the type of "double bind" (double bind), was qualified as "schizophrenogenic". For this kind of relationship, G. Bateson identified three qualifying signs:
1. Communication should be important for this person.
2. During communication, two contradictory messages are simultaneously transmitted (the term “incongruence” was used to define this - for example, words and facial expressions, pantomime, intonation do not correspond to each other).
3. It is forbidden by the rules of communication to clarify what exactly is meant.
It was found that schizophrenogenic communication itself is often found not only in patients with schizophrenia. However, in other cases, it is temporary - alcohol is excreted from the body, headache and anger pass, the traumatic situation ends, and the person begins to communicate congruently. The fundamental difference in communication between patients with schizophrenia and neuroses, as Jung and Haley (118) pointed out, is quantitative - how consistently a person communicates incongruently and how deep this incongruence goes. The pathopsychologists come to the same conclusions: it is important not only that in the experiment, in principle, there are slips of thinking or the patient's lack of interest in performing one or another test, but how often these phenomena occur in various tests (168). While the neurotic simply uses incongruence to deny his message (for example, annoyedly says "Sit down!" to an unwanted visitor at the end of the working day - this still allows the visitor to guess that he is not particularly welcome here), the schizophrenic patient strengthens his incongruence to such an extent that the very fact of denying the definition of one’s behavior is denied in behavior: for example, when an unwanted visitor enters the room, the patient not only remains silent and pretends not to notice him - this is already, albeit incongruently, but would already show an attitude towards a person, but begins to behave as if he is extremely busy with something in the room or in his thoughts - this allows him to avoid communication and at the same time not define his behavior as avoidant.
The fundamental difference in communication between patients with schizophrenia and neuroses, as Jung and Haley (118) pointed out, is quantitative - how consistently a person communicates incongruently and how deep this incongruence goes. The pathopsychologists come to the same conclusions: it is important not only that in the experiment, in principle, there are slips of thinking or the patient's lack of interest in performing one or another test, but how often these phenomena occur in various tests (168). While the neurotic simply uses incongruence to deny his message (for example, annoyedly says "Sit down!" to an unwanted visitor at the end of the working day - this still allows the visitor to guess that he is not particularly welcome here), the schizophrenic patient strengthens his incongruence to such an extent that the very fact of denying the definition of one’s behavior is denied in behavior: for example, when an unwanted visitor enters the room, the patient not only remains silent and pretends not to notice him - this is already, albeit incongruently, but would already show an attitude towards a person, but begins to behave as if he is extremely busy with something in the room or in his thoughts - this allows him to avoid communication and at the same time not define his behavior as avoidant. The same purpose is served by symbolic statements, actions, as well as the expression of one's true feelings as metaphors - in words and behavior. In a lighter version, this will be a statement: “I feel as if the world has collapsed and everyone has betrayed me” - with the corresponding suicidal behavior, in a more difficult version - sewing up the mouth with threads in protest that the patient’s opinion was not heeded, even more severe - the fragmentation of speech and thinking as an expression of fear of life, which allows you to safely hide from this life behind the walls of a psychiatric clinic.
The same purpose is served by symbolic statements, actions, as well as the expression of one's true feelings as metaphors - in words and behavior. In a lighter version, this will be a statement: “I feel as if the world has collapsed and everyone has betrayed me” - with the corresponding suicidal behavior, in a more difficult version - sewing up the mouth with threads in protest that the patient’s opinion was not heeded, even more severe - the fragmentation of speech and thinking as an expression of fear of life, which allows you to safely hide from this life behind the walls of a psychiatric clinic.
In addition, the refusal to clearly define one's intentions guarantees the absence of defeats, because whoever does nothing never loses. And this circumstance for our patient, brought up in the spirit of the double bind: “you must always be a winner and make only accurate decisions, but at the same time you are forbidden in the fight to cause inconvenience to others and make mistakes, gaining experience through them” turns out to be extremely important. After all, it is possible to clearly fulfill this parental instruction only by going into a schizophrenic type of reaction: “I am generally good and talented, but I could not fulfill everything entrusted to me because I fell ill with an incurable disease, which is also complicated by the fact that I cannot realize what I am ill, and I am not capable of purposeful actions in order to cope with the disease. Now, if someone (God forbid!) cured me, I would certainly be able to justify my parental hopes.
After all, it is possible to clearly fulfill this parental instruction only by going into a schizophrenic type of reaction: “I am generally good and talented, but I could not fulfill everything entrusted to me because I fell ill with an incurable disease, which is also complicated by the fact that I cannot realize what I am ill, and I am not capable of purposeful actions in order to cope with the disease. Now, if someone (God forbid!) cured me, I would certainly be able to justify my parental hopes.
In the Old Testament, it was established: “If your brother, a Jew, or a Jewess, sells himself to you, then for six years he should be your slave, and in the seventh year let him go free from you ... If he says to you: “I will not go away from you, because I love you and your house”, because it is good for him with you, then take an awl and pierce his ear to the door; and he will be your servant forever” (Deuteronomy 15:12-17). Why was the share of a slave so pleasant that Moses had to specifically prescribe such a law? Only one: the slave is spared the burden of taking responsibility. How sweet, despite the constant humiliation and obligation to do the hardest work, is the share of an irresponsible person that even his own ears turned out to be not a pity!
How sweet, despite the constant humiliation and obligation to do the hardest work, is the share of an irresponsible person that even his own ears turned out to be not a pity!
In the same way, a person who avoids determining his behavior, attitudes and intentions through unconscious mechanisms also avoids responsibility, falling under the category of insanity.
Certainly, a significant role in the patient's transition to a schizophrenic style of response is also played by the specific vulnerability of the personality, which, as modern studies show, is based on a decrease in the function of the frontal cortex against the background of autoimmune, toxic and mediator disorders. It is erroneous to oppose the biological and psychological mechanisms of pathogenesis to each other.
They, as practice shows, always go hand in hand, and the strengthening of biological disorders always leads to aggravation of psychological and family problems. At the same time, regular stresses to which patients are exposed due to the psychological weakness and vulnerability of their personality, as well as constant family problems, according to all the laws of the development of stress reactions, are guaranteed to lead to a violation of the biological functioning of the brain. Therefore, in parallel with the described psychological methods of influence, and often ahead of them, scientifically based biological therapy should always be carried out.
Therefore, in parallel with the described psychological methods of influence, and often ahead of them, scientifically based biological therapy should always be carried out.
Another weighty reason to use a schizophrenic type of communication for a patient is narcissistic rage - a powerful charge of destructive negative emotions that invariably manifests itself in the psyche of a patient with schizophrenia during psychoanalytic therapy.
It arises as a reactive formation due to a deep sense of one's own weakness, the inferiority of the patient and the corresponding fear of annihilation by the outside world. This rage is restrained by libido - the energy of love for loved ones. Spotnitz describes this process as follows: “The integrity of the psyche and the fate of the external object become the stake in the battle between the aggressive object cathexis, fighting for motor control, and the libidinal cathexis, controlling motor skills to prevent aggressive actions. In these states of high tension, the energy of the libido is sufficient to restrain hostile behavior, but not enough to be the organizing force of the psychic apparatus. The outcome of this battle is a foregone conclusion in favor of a more powerful opponent.
The outcome of this battle is a foregone conclusion in favor of a more powerful opponent.
The patterning of the schizophrenic reaction reduces the tension sufficiently to preserve the object, but disorganizes the psychic apparatus, resulting in psychosis... To clarify the unconscious operation, I will emphasize again that the patient is constantly under the pressure of a strong desire to kill and defends himself from it by deducing out of order their mental apparatus with its high potential for destructive actions.
To destroy a potentially destructive self in order to prevent dangerous actions directed against other people is like smashing a rifle to smithereens so as not to pull the trigger” (1).
Going into the world of symbols, the patient must spend somewhere the energy that should have been spent on social adaptation and development of his personality, and also at least somehow explain to himself the meaning of what is happening (despite the fact that the true goals of his behavior, according to the rules of the subconscious games are not subject to clarification). This is where initiation comes to the rescue using the endogenous mechanisms of the myth-ritual complex "death-rebirth", described by Zaitseva-Pushkash and other authors who studied traditional cultures (2) (39). The patient does not just move away from communication with people and work - he is busy comprehending important, unknown to the uninitiated knowledge and performing actions under the guidance of higher forces that capture his will. After that, a completely new life awaits him - sometimes filled with a new meaning, incomprehensible to others, and sometimes just living out his life exhausted and weak-willed, like a squeezed lemon. But now this lack of will has an explanation: “Everything that happened completely exhausted me, it’s not me running away from life, it’s my illness. I can’t do anything myself, but I hope that everything will work out somehow (that is, someone will solve my problems for me).” In both of these cases, as Yalom shows, a person refuses to take responsibility for his actions and his life, entrusting it to the "ultimate savior" (40).
This is where initiation comes to the rescue using the endogenous mechanisms of the myth-ritual complex "death-rebirth", described by Zaitseva-Pushkash and other authors who studied traditional cultures (2) (39). The patient does not just move away from communication with people and work - he is busy comprehending important, unknown to the uninitiated knowledge and performing actions under the guidance of higher forces that capture his will. After that, a completely new life awaits him - sometimes filled with a new meaning, incomprehensible to others, and sometimes just living out his life exhausted and weak-willed, like a squeezed lemon. But now this lack of will has an explanation: “Everything that happened completely exhausted me, it’s not me running away from life, it’s my illness. I can’t do anything myself, but I hope that everything will work out somehow (that is, someone will solve my problems for me).” In both of these cases, as Yalom shows, a person refuses to take responsibility for his actions and his life, entrusting it to the "ultimate savior" (40).
In addition, we constantly see that communication in the families of patients with schizophrenia, as noted above, is built on "double binds". The difference between the patient and his family members is that, firstly, they use "double binds" periodically, refusing them where it interferes with social and labor adaptation, and, secondly, the patient is a less important member of the family, than one of the parents or siblings, and despite the fact that this other family member turns out to be even more mentally ill than our patient, the latter, according to the unconscious mechanisms of the functioning of the family system, is sacrificed to family stability. Declaring him sick allows others to sigh sadly: “Oh, how good we would live if Vasya did not suffer from schizophrenia,” and calm down, forgetting about their own intrapsychic problems and difficulties in communication. The love of the parents is gone (or it never was), and it’s scary to get a divorce and start life over again. To realize this for them is to plunge into the abyss of despair, and here again Vasya's illness comes to the rescue: “We are honest, decent, responsible people. How can we part when our son is so seriously ill! We are together to save him." Experienced psychiatrists know that often the biggest problems in a family begin when a mentally ill family member suddenly goes into pure remission.
To realize this for them is to plunge into the abyss of despair, and here again Vasya's illness comes to the rescue: “We are honest, decent, responsible people. How can we part when our son is so seriously ill! We are together to save him." Experienced psychiatrists know that often the biggest problems in a family begin when a mentally ill family member suddenly goes into pure remission.
However, to go into pure remission does not mean to recover forever. After all, our patient spent his whole life in the little world of his family, who communicated in “double bonds” and hid their true feelings and intentions from themselves and from each other. And to recover means to enter the big world, where people communicate in a completely different way and where “double binds” are used relatively rarely, and successful people (oh, horror!) openly tell each other about their feelings, desires and intentions, and at the same time are not afraid make new mistakes, guided by the dictum of W. Churchill: “Success is the ability to go from defeat to defeat without losing optimism!” Our patient has never lived in such conditions, and, in the absence of psychosocial rehabilitation, he simply does not know how to act in such a way. He tries, with the best of intentions, to communicate the way he learned in his family, but he is not understood and rejected, considering him a ridiculous eccentric. Social and labor maladaptation is growing, and soon, like a prisoner released after a long term of imprisonment and unable to adapt to the freedom that he dreamed of for so long, our patient returns to the world of his family, which causes him the most negative feelings, but the style of communication which is more familiar to him. And to start communicating differently usually means becoming a stranger to your parental family in conditions where new social ties are made with great difficulty and, due to the inability to develop them, are not stable, which is fraught with chronic loneliness.
Churchill: “Success is the ability to go from defeat to defeat without losing optimism!” Our patient has never lived in such conditions, and, in the absence of psychosocial rehabilitation, he simply does not know how to act in such a way. He tries, with the best of intentions, to communicate the way he learned in his family, but he is not understood and rejected, considering him a ridiculous eccentric. Social and labor maladaptation is growing, and soon, like a prisoner released after a long term of imprisonment and unable to adapt to the freedom that he dreamed of for so long, our patient returns to the world of his family, which causes him the most negative feelings, but the style of communication which is more familiar to him. And to start communicating differently usually means becoming a stranger to your parental family in conditions where new social ties are made with great difficulty and, due to the inability to develop them, are not stable, which is fraught with chronic loneliness.
Thus, the refusal to define one's relationship and the withdrawal into a schizophrenic style of response has a number of great advantages for the patient:
1. Avoiding leaving for an independent life and taking responsibility for your actions.
2. Keeping your loved ones safe by keeping them from venting their narcissistic rage.
3. Stabilization of the mental state of their loved ones and relationships in the parental family.
4. Avoiding mistakes and defeats.
5. Maintaining relationships with parents.
6. Prevention of complete loneliness.
7. Finding the meaning of one's life through the development of the mythological-ritual complex "death-rebirth".
As pointed out by N.P. Bekhterev (116), any long-term neurological or psychiatric disease leads to the formation of a stable pathological state of the brain, in which the psyche resists doctors' attempts to cure the patient, and exit from which is possible only through the decompensation phase (if possible, controlled). Psychoanalysis also affirms the same, one of the most important tools of which is work with the patient's unconscious resistance. Therefore, as Hayley (118), Minukhin (121), Whitaker (50), Selvini Pallazzolli (122) and others rightly pointed out, the first step in working with a patient with schizophrenia is “uprooting” him from the “ecological niche” occupied by him, refusing to relationship definitions. This can be done in two ways. The first is the most common way of a direct attack, when the patient is removed from his intra-family environment to a psychiatric hospital, where his relationships are determined by the directive of the medical staff (and therefore it is impossible to avoid their definition), and the symptoms of mental disorders, with the help of which the patient manipulated the environment, are cut off with the help of psychopharmacotherapy or comatose treatments, forcing the patient to look for other ways of communicating and behaving in the world. However, the results of using this method are reminiscent of the situation common in modern politics, when a major developed power undertakes to urgently civilize a neighboring country that is in a barbaric state, using the method of a major military operation, hoping that in the future the neighbors will hold civilized democratic elections and finally live as people.
Psychoanalysis also affirms the same, one of the most important tools of which is work with the patient's unconscious resistance. Therefore, as Hayley (118), Minukhin (121), Whitaker (50), Selvini Pallazzolli (122) and others rightly pointed out, the first step in working with a patient with schizophrenia is “uprooting” him from the “ecological niche” occupied by him, refusing to relationship definitions. This can be done in two ways. The first is the most common way of a direct attack, when the patient is removed from his intra-family environment to a psychiatric hospital, where his relationships are determined by the directive of the medical staff (and therefore it is impossible to avoid their definition), and the symptoms of mental disorders, with the help of which the patient manipulated the environment, are cut off with the help of psychopharmacotherapy or comatose treatments, forcing the patient to look for other ways of communicating and behaving in the world. However, the results of using this method are reminiscent of the situation common in modern politics, when a major developed power undertakes to urgently civilize a neighboring country that is in a barbaric state, using the method of a major military operation, hoping that in the future the neighbors will hold civilized democratic elections and finally live as people. At first, everything goes brilliantly: the neighboring country is quickly occupied, all its leaders swear allegiance to the democratic ideals of their pale-faced brothers, humanitarian aid is sent to the country in a wide stream. However, the latter is quickly being stolen, which for some reason is only helped by democratically elected authorities, in the poor provinces the guerrilla movement is rearing its head and strengthening, which is becoming increasingly difficult to cope with, new and new military operations bring less and less results at ever greater costs, and gradually a major developed power is discovering that the cost of keeping its barbarian neighbors from ultimate chaos is getting ever higher. At a certain moment, a major developed country develops a syndrome of psychotherapeutic burnout, it spits on the problems of its neighbors and leaves, having come to terms with all the reputational and economic losses, regarding the situation as incurable in principle, when the best way would be to isolate yourself from your neighbors with the highest possible fence in order to never see them again.
At first, everything goes brilliantly: the neighboring country is quickly occupied, all its leaders swear allegiance to the democratic ideals of their pale-faced brothers, humanitarian aid is sent to the country in a wide stream. However, the latter is quickly being stolen, which for some reason is only helped by democratically elected authorities, in the poor provinces the guerrilla movement is rearing its head and strengthening, which is becoming increasingly difficult to cope with, new and new military operations bring less and less results at ever greater costs, and gradually a major developed power is discovering that the cost of keeping its barbarian neighbors from ultimate chaos is getting ever higher. At a certain moment, a major developed country develops a syndrome of psychotherapeutic burnout, it spits on the problems of its neighbors and leaves, having come to terms with all the reputational and economic losses, regarding the situation as incurable in principle, when the best way would be to isolate yourself from your neighbors with the highest possible fence in order to never see them again. Will it just work?
Will it just work?
Wise politicians know that in order to cultivate a barbarian country, one should first of all establish close ties with the ruling elites and, first of all, slowly cultivate them by educating the rulers and their children in their universities, providing these elites with military and economic assistance so that they themselves bring order, and to create economic conditions so that it would be more profitable and easier for the inhabitants of the country to engage in peaceful labor than to rob. Then begins delicate diplomatic work, full of cunning, imperceptible from the outside, but accurately calculated moves. This process turns out to be much longer and less brilliant at the beginning than the frontal attack method described earlier, but it gives much better and more stable long-term results.
In a similar way, the principle of community-based treatment of mental illness, which has recently become increasingly popular, operates when the goals of a team of specialists working with the patient and his relatives is to build an adequate hierarchical structure among the latter, trained to independently successfully cope with all emerging problems.
There is another important point that is characteristic not only for patients with schizophrenia, but for personally immature people in general. If for a mature person the words that he speaks and which are spoken to him are important (the second signal system according to Pavlov), then for an immature person words in themselves are unimportant and significant are the external expressions of mental life: actions and gestures (the first, phylogenetically older signal system ). Humanity faced this even during the collapse of Ancient Rome, when the coherent system of Roman laws, based on the logic and evidence of the word, gave way to the laws of gestures and actions. Instead of a speech or a logically composed statement, the Frankish legislation "Salic Truth" (169) to lay part of his debt on relatives, he ordered to invite 12 jurors - witnesses from the closest relatives, go out onto the porch of his house, stand facing inside the house - civilization of the gesture, stand up like that, then it will be according to the law - and throw this handful with your right hand, necessarily right, over their shoulders to the next three relatives, on the father, then on the mother, etc. , and then they must pay half of what is not enough to pay the fine. If these next of kin have already paid - even for the next relatives. Then he must, without shoes, without a belt, with a stake in his hand, jump over the wattle fence, and then the requirement of the law to pay relatives for the debtor came into force. If, on the contrary, a person wanted to renounce kinship in order not to pay off other people's debts, then he had to come to the judge and there scatter sticks a cubit long over his head to all parts of the world. Among immature people, it was the act, the gesture that reigned and reigns, and it is on them that the psychotherapist should rely in the first stages of his work, paying more attention to working with action and experiencing feelings than with a logical discussion of what is happening, the turn of which comes much later. This idea is one of the core ones in justifying the use of body-oriented psychotherapy for schizophrenia, based on the use of dance, gestures, and movement.
, and then they must pay half of what is not enough to pay the fine. If these next of kin have already paid - even for the next relatives. Then he must, without shoes, without a belt, with a stake in his hand, jump over the wattle fence, and then the requirement of the law to pay relatives for the debtor came into force. If, on the contrary, a person wanted to renounce kinship in order not to pay off other people's debts, then he had to come to the judge and there scatter sticks a cubit long over his head to all parts of the world. Among immature people, it was the act, the gesture that reigned and reigns, and it is on them that the psychotherapist should rely in the first stages of his work, paying more attention to working with action and experiencing feelings than with a logical discussion of what is happening, the turn of which comes much later. This idea is one of the core ones in justifying the use of body-oriented psychotherapy for schizophrenia, based on the use of dance, gestures, and movement. K.-H. Leiner, in turn, describing his method of symbol-drama (42), emphasized that at the first stages of working with visualized images, their analysis and interpretation are possible, but undesirable, which also reflects the difficulties of our patients in logical comprehension of the world and the greater importance of action. and experiences, even imaginary ones.
K.-H. Leiner, in turn, describing his method of symbol-drama (42), emphasized that at the first stages of working with visualized images, their analysis and interpretation are possible, but undesirable, which also reflects the difficulties of our patients in logical comprehension of the world and the greater importance of action. and experiences, even imaginary ones.
In the practice of a psychiatrist, periodically there are patients whose thinking and emotional-volitional response, according to the data of an experimental psychological study (EPI), are greatly altered by the current endogenous process, while these patients turn out to be remarkably adapted in society, have good families or personal relationships, and come to the attention of a psychiatrist about moderately severe problems of a neurotic nature. An important question for us was: what exactly compensatory mechanisms help them, with a sufficiently pronounced schizophrenic pathological symptom complex, to avoid social and labor maladjustment and live a fairly happy, full life?
For this purpose, we conducted clinical examinations in combination with EPI of 32 similar patients. All of them showed signs of a schizophrenic pathopsychological symptom complex from mild to moderate severity with a change in both the motivational and operational spheres of thinking according to the schizophrenic type. At the same time, clinically, it was impossible to confidently speak about the presence of the current endogenous process in its progredient form: structurally and dynamically, they were confidently kept at the neurotic level, neither autism nor social and labor maladaptation was noted. The reason for visiting a psychiatrist was moderate anxiety and psychosomatic disorders.
All of them showed signs of a schizophrenic pathopsychological symptom complex from mild to moderate severity with a change in both the motivational and operational spheres of thinking according to the schizophrenic type. At the same time, clinically, it was impossible to confidently speak about the presence of the current endogenous process in its progredient form: structurally and dynamically, they were confidently kept at the neurotic level, neither autism nor social and labor maladaptation was noted. The reason for visiting a psychiatrist was moderate anxiety and psychosomatic disorders.
In the process of studying compensation mechanisms, it was noted that this group of patients was characterized by high intelligence and high values on the scales of "hysteria" and "psychopathy" in SMIL (i.e., personality traits that compensate for schizoid and depressive traits gradually developing against the background of the disease, thanks to which, at some stages of the disease, they themselves and their relatives sometimes noted that their character had become even better than before the disease). To a lesser extent than in other patients, they had facial expression disorders; they were able to understand quite well the true meaning of the mimic reactions of the interlocutors. All of them, thanks to their high intelligence and ability to establish harmonious object relations, managed to develop an interesting way of adaptation: in the conditions of the unevenness and inconsistency of the process of generalization with the equalization of the significance of the main and secondary features of objects and concepts, they were trained to solve these issues by asking interlocutors in detail about about what exactly should be done and according to what criteria the right decision should be made, after which, having received the necessary instructions and following them exactly, they acted very effectively, including during testing. If, during the EPI, they were given a test with a “deaf” instruction (when the psychologist refused to give detailed explanations on how to perform the test correctly, limiting himself to the standard setting of the task), significant thinking disorders were immediately reflected in the results in the form of a tendency to equalize the significance of the main and secondary signs of objects and concepts, semantic slips with the actualization of non-standard properties and relationships, a clear tendency to overgeneralize when defining concepts, manifestations of diverse thinking.
To a lesser extent than in other patients, they had facial expression disorders; they were able to understand quite well the true meaning of the mimic reactions of the interlocutors. All of them, thanks to their high intelligence and ability to establish harmonious object relations, managed to develop an interesting way of adaptation: in the conditions of the unevenness and inconsistency of the process of generalization with the equalization of the significance of the main and secondary features of objects and concepts, they were trained to solve these issues by asking interlocutors in detail about about what exactly should be done and according to what criteria the right decision should be made, after which, having received the necessary instructions and following them exactly, they acted very effectively, including during testing. If, during the EPI, they were given a test with a “deaf” instruction (when the psychologist refused to give detailed explanations on how to perform the test correctly, limiting himself to the standard setting of the task), significant thinking disorders were immediately reflected in the results in the form of a tendency to equalize the significance of the main and secondary signs of objects and concepts, semantic slips with the actualization of non-standard properties and relationships, a clear tendency to overgeneralize when defining concepts, manifestations of diverse thinking.
In addition, well-established object relations were also a source of motivation for constructive activity for patients. At the same time, it should be emphasized once again that personal relationships in all examined patients of this group were quite structurally clearly built, with an established intra-family hierarchy and feedback. All of them worked and were valued as specialists or even heads of organizations, and the occasional emotional and volitional decompensation was quickly smoothed out by those around them who knew the personal characteristics of the patients well: “The boss is not in a good mood today, come tomorrow or let us decide everything ourselves.”
Often, to solve their problems, patients in this group spontaneously used the method of image visualization: “I work somehow at the machine, and then “voices” appear. Well, I understand that this is a potentially dangerous business, I turn off the machine, sit next to me and imagine a beautiful garden, apple trees, a stream, how I relax there - the voices gradually disappear. I'll take a break and get back to work."
I'll take a break and get back to work."
In this way, the main mechanisms of spontaneous personal compensation that prevent the development of social and labor maladjustment and reduce the severity of emotional and volitional disorders in patients with schizophrenia turned out to be high intelligence, the severity of excitable and hysterical radicals in the personality, clearly structurally built, with an established intra-family hierarchy and feedback, object relationships (which, in turn, is impossible without sufficient integration of the Super-Ego, the ability to take responsibility for oneself and one's life) and the ability to overcome decompensation with the help of visualization of images. These observations of ours confirm Kernberg's opinion that the prognosis of psychotherapeutic treatment for severe personality disorders largely depends not on the severity of the disease, but on the quality of object relations and the degree of Super-Ego integration (20).
What should be the strategy for solving the problems of a patient with schizophrenia and his microsocial environment? As we have already shown above, it should be based on moves that render ineffective the usual strategy of the patient's problem-solving behavior, based on the manipulation of the environment with the help of his symptoms, disguised as a refusal to determine his behavior and intentions. These moves fall into a number of categories:
These moves fall into a number of categories:
1. Creation in the microsocial environment of the patient of a harmonious hierarchical structure with clearly defined rights and obligations of all its members, responsibility for failure to fulfill their duties, and a head capable of enforcing all these laws, as well as a working feedback that allows each family member to correctly understand the consequences of their actions. In such a structure, there is no room for the uncertainty of relations.
2. Effective biological therapy aimed at correcting mediator, toxic and autoimmune disorders leading to a specific schizophrenic vulnerability of the individual and the development of psychosis. In addition, biological therapy leads to a limitation of the patient's ability to maintain the previous style of intra-family response, which also creates conditions for changing the nature of intra-family relations and the patient's search for new opportunities for self-realization in the outside world.
3. Contrasting communication based on "double binds" with the psychotherapist's paradoxical actions aimed at prescribing the patient in a disguised form of his own schizophrenic style of response. It also destroys the unconscious game of the patient and his loved ones: the continuation of the previous behavior and response now begins to mean submission to the psychotherapist and, accordingly, a clear definition of the relationship.
4. Given the inclination of patients with schizophrenia to trance functioning, hypnotherapy can also be used to gain access to their experiences and correct their personality, which, among other things, has a pronounced positive effect on biological processes that are also the driving forces of the disease - intoxication, autoimmune disorders, mediator metabolism disorders. However, most of these patients are less receptive to conventional hypnotic induction techniques due to negativism, impaired concentration, and thought disorders. Therefore, in these cases, hypnotic work should be preceded by cognitive training aimed at correcting these problems.
5. The schizophrenic initiation of the myth-ritual complex "death-rebirth" (35) with the shifting of all one's problems and responsibility to the "ultimate savior" (40) should be replaced with the initiation of the development of a mature, a successful person, strong enough to, unlike many other people, successfully cope with all his difficulties both in the internal and external world (the script of his own exceptionalism) (40). This is especially necessary because schizophrenic patients, due to the dysfunctionality of their families, have many more examples of life failures and dead ends around them than successes, and in order to win, they often really need to become an exception to the general rule of life failures established in their family.
6. At the first stages of work with the patient, priority should be given not to the logical analysis of existing difficulties, but, first of all, to the patient's relatives performing specific actions demonstrating compliance with the new laws based on the principles of hierarchy and feedback.
These actions lead to the destruction of previous stereotypes in relationships, response style and behavior. But for the final solution of the issue, the patient and his relatives must be trained to act differently and accumulate sufficient experience in the harmonious expression of their feelings and problem-solving behavior both in matters of internal and external life. This also turns out to be important goals for further individual and family psychotherapy, as well as social and labor readaptation. This book "Practical Psychotherapy of Schizophrenia" is devoted to the presentation of practical ways to achieve these goals.
“This book is not a textbook. These are rather travel notes of a person who for 13 years, together with his colleagues, explored the field at the intersection of psychiatry and psychology, which seemed interesting to him - psychotherapy and rehabilitation of patients with schizophrenia.
We cannot say that we were the first here.