Worst cases of reactive attachment disorder
A parent's worst nightmare | Salon.com
According to Renee Polreis, the bruises that blackened her son's body at the
time of his death were self-inflicted. Her adopted son David apparently
suffered from reactive attachment disorder (RAD), a condition marked by
violent fits of rage, inappropriate emotional responses, severe emotional
detachment and an inability to feel pain.
Last week, a Greeley, Colo., judge sentenced her to 22 years in prison for
abuse resulting in David's death. Investigators found a broken, bloody wooden spoon wrapped in a diaper in
the Polreis home; Polreis had called her attorney and her therapist before
calling "911" to report her son's death. U.S. News and World Report reported that Polreis'
defense characterized David's behavior as violent and out of control --
David banged his head on the floor, became rigid and smashed his face on
the ground and tugged his penis until it bled. Despite the defense's focus
on David's uncontrollable behavior, at least two witnesses for the
prosecution testified to the mother's loss of control. According to the New
York Times, one of the Polreis' family's two therapists, Byron Norton,
stated that Renee Polreis called him at 4:30 a.m. on the day David died and
told him that she'd hurt David. "I just lost it," Polreis told Norton.
While casting the national spotlight on reactive attachment disorder, the
Polreis case may have further muddied the waters around a condition that
many have never heard of and few understand. Although recognized by the
American Psychiatric Association as legitimate, attachment
disorder is controversial because of the therapeutic community's
disagreement on the most effective course of treatment. Some doctors advocate
"holding therapy," during which the patient is physically restrained until
he/she can exhibit appropriate emotions, while others advocate more traditional psychotherapy that involves both
parents and children.
Salon recently asked Dr. Alicia Lieberman, director of the Child Trauma Research Project
at San Francisco General Hospital and an expert on attachment disorders, to
discuss the diagnosis, symptoms and treatment of reactive attachment disorder.
What is attachment disorder?
It is a disorder that occurs when children have not had the opportunity to
become emotionally connected to a primary caregiver, particularly in the
absence of a biological or adopted mother figure. It is most notable in
children who have not had a consistent caregiver for the first three years of
life. If the child is not given the opportunity to form a deep emotional
connection with an adult who takes care of him, then it becomes a lifelong
personality disorder that consists of an inability to form intimate
connections with others. Often this manifests itself in a very aggressive,
exploitative pattern of relationships or in a withdrawn, scared, unconnected
pattern.
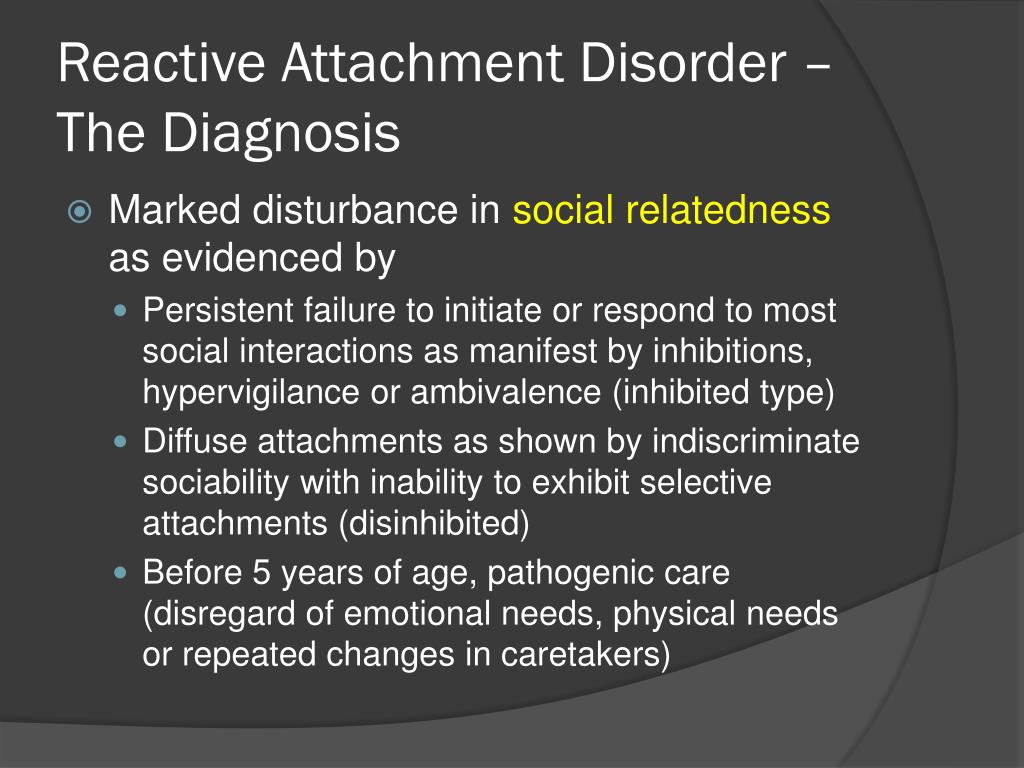
How do infants with the disorder act?
"Infant" is defined here as babies ages 0 through 5 years. There
are two major patterns in infants. In one, the child is overly
gregarious, does not seem to see the difference between one person and
another, even between their parent and a stranger. This happens when a
This happens when a
child lives in an orphanage for years and has many, many different
caregivers and then is adopted. The adoptive parents will complain that the
child will follow a stranger who smiles at him. You also see this in
children who were raised in institutions; whatever stranger comes into the
room becomes the novelty, the attractive person, and the child might want to
follow that person out of the room only to turn to the next person they see
and follow them. There is an indiscriminate search for connection without
any emotional preference. It can be very chilling to see.
The second pattern is withdrawal. Children seem to be afraid of the
world. These children are lethargic, apathetic and do not explore or reach
out to anybody and seem uniformly afraid of people.
In the Polreis case, the little boy was apparently abusive to
himself. He apparently banged his head against the wall.
There can also be a component of aggression -- and that includes aggression
toward the self -- but that is much rarer.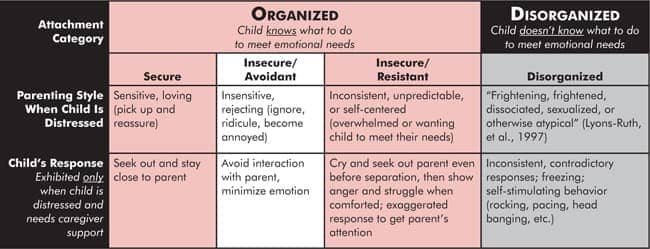
Why is there so much controversy around the treatment of attachment
disorder?
First of all, there is very little controversy over the fact that this
is a real disorder. It is very well documented and nobody who knows
anything about children doubts that it is real.
There is an established approach to treating disorders of attachment
that emphasizes the importance of giving these children precisely what they
have lacked. The research on what makes for a secure attachment and what
makes for a disordered one emphasizes the mother's ability to be responsive
to the child, to be sensitive. The research has shown what really works is
maternal empathy, maternal responsiveness, the ability of the mother to put
herself in the child's position and to be sensitive to the child's signals.
The form of treating attachment disorders that I do is called
infant-parent psychotherapy. It involves understanding the
meaning of the signals a child gives off and helping the mother respond
appropriately. I have done research showing that children
I have done research showing that children
who were treated this way do much better in terms of their social and
emotional functioning, and their mothers become much more competent and
sensitive and less angry and less aggressive.
What does this therapy entail?
We can start the first day of life, prenatally even. The whole point is to
help the mother recognize the meaning of the child's behavior. When a child
is signaling distress, joy or need, we help the mother identify the kinds
of behavior that would meet the child's needs. So essentially what we do is
awaken a sense of nurturance or love for the child. Many of the mothers who
have children with these disorders have been abused or neglected during their own childhoods.
So they are not familiar with the things that you and I might take for
granted -- to go to children when they are crying, to reassure them when
they are scared, to feed them when they are hungry.
It often takes being sensitive to the mother to change the situation
with the child. It is only when the mother feels protected and supported by
It is only when the mother feels protected and supported by
us that she in turn can reconnect with her pain, the pain of not having
grown up with this security and caring that she longed for terribly.
What is your opinion of holding therapy?
I've had some mothers call me and say they've gone through it and are
having a hard time. I've heard hearsay about it, but I haven't seen it. One
thing I think is very important to ask is: "What is developmentally appropriate
for children?" One thing we do in our therapy is to try not to exacerbate the
symptoms, not to retraumatize the child. Many of these children not only
have attachment disorder but also post-traumatic stress disorder because of
punishment and loss. We are working with terrified children.
From what I understand, part of the holding therapy is to physically
hold the children down until they "break through," finally
expressing their true emotions.
These children are already having trouble regulating intense emotions.
The best way you can best help them regulate their emotions is to provide
a self-container, where you are the person they can rely on to soften their
emotions, rather than exacerbate them.
The Polreis case highlighted the situation of an adopted child with
attachment disorder. But it sounds like you mostly work with kids and their
natural mothers.
Eighty percent of the women I see are biological mothers.
Why then do we seem to hear only about the cases of attachment
disorder among adopted children, mostly those adopted from the Soviet Union and
Romania?
I think it's because the parents that adopt them are very articulate in
explaining the difficulties that these children have. But the disorders of
attachment are a rampant problem for infants in our foster-care system.
The disorder occurs often in children who are born to mothers who are
addicted to drugs and therefore cannot provide consistent care, and the children often have a
string of caregivers. Those parents are often not aware of the difficulties
Those parents are often not aware of the difficulties
their children are enduring and they feel too guilty to talk about it,
whereas adopted parents don't feel the disorder is their fault
so they seek help. They also have more resources to pay for the help
privately.
Is the level of frustration Renee Polreis exhibited something that you
often see in parents who are dealing with this illness?
Yes, I think that there are parents who find themselves unable to get
through to their child, so that their efforts to get the child to obey,
to get the child to mind, to get the child to love them, to be loving and
affectionate with them, seem to go nowhere. That's where I think it is
very important to seek therapy that looks at the meaning of the behavior. I
think it is very important to remember that these behaviors are defenses
that the child engages in. These are children who have no reason to trust
human relations. Every human relation that these children have had have
been disappointing, frightening or confusing. So in a way you have to
So in a way you have to
say to these children, I am going to give you a totally different experience
from anything you have experienced until now. And I am going to show you
that no matter how much you push me away, how much you make me angry, how
much you defy me, I will not hurt you.
Adopting family tortured by girl's RAD illness
Estimated read time: 4-5 minutes
This archived news story is available only for your personal, non-commercial use. Information in the story may be outdated or superseded by additional information. Reading or replaying the story in its archived form does not constitute a republication of the story.
ALPINE -- A Utah County family has been living through a nightmare for five years. It's a child-raising scenario so disturbing and so challenging they decided to share their story to help others.
It took Jay and Jodi Bean of Alpine years to figure out why their new daughter brought anger and fear into the family and triggered maternal hate instead of love. Jodi has written a book to help others who may, unknowingly, be struggling with a rare condition called RAD.
Jodi has written a book to help others who may, unknowingly, be struggling with a rare condition called RAD.
The emotional puzzle began five years ago. That's when Jay and Jodi welcomed 4-year-old Victoria into their family, adopted from an orphanage in the former Soviet Republic of Belarus.
Jodi Bean talks to her daughter, Victoria, during a horseback riding therapy session"As far as her emotional needs, I honestly thought I just had to bring her here and give this girl all the love that she never had," Jodi said.
The orphanage seemed nice, but it wasn't long before they knew something horrible was wrong with their adopted daughter.
"She was lying, and she was sneaky, and she was destructive," Jodi said. "She would break her toys, she would rip her clothes, pull her hair out. She'll bite on her lips until they bleed."
Victoria even threatened, in detail, how she would kill her new mom. She would hit, bite and spit on Jodi.
After raising three boys, Jodi considered herself a nurturing parent, but she just couldn't break through to Victoria.
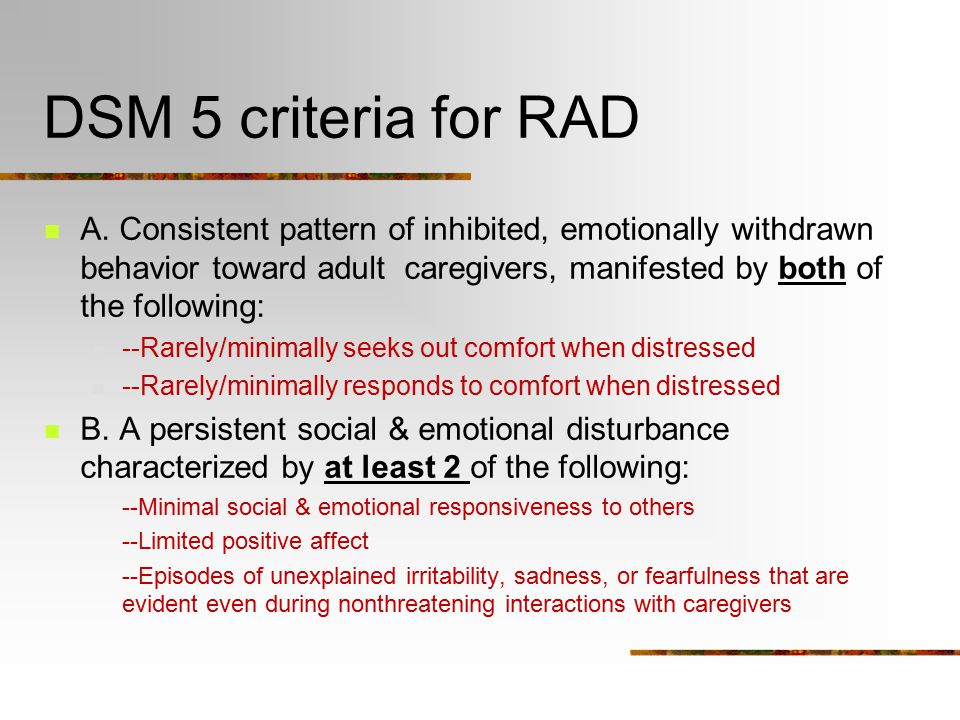
**What is... Reactive attachment disorder?**
Reactive attachment disorder (RAD) is a rare but serious condition in which infants and young children don't establish healthy bonds with parents or caregivers. A child with reactive attachment disorder is typically neglected, abused, or moved multiple times from one caregiver to another. Because the child's basic needs for comfort, affection and nurturing aren't met, he or she never establishes loving and caring attachments with others. This may permanently alter the child's growing brain and hurt their ability to establish future relationships. It is a lifelong condition, but can be treated with psychological counseling and parent or caregiver education.-*Mayo Clinic*
"Her emotions have been so shut down that the only emotions that I knew for sure she knew how to feel were anger and fear," Jodi said. Through five years of therapy, including therapeutic horseback riding, Jodi finally fit the pieces of the puzzle together. The key was those first four years in the orphanage.
The key was those first four years in the orphanage."She never had a consistent caregiver," Jodi said. "She didn't believe her needs were going to be met. She literally thought she was going to die. There's no doubt. I have no doubts of that."
It turns out that Victoria suffers from a rare psychiatric illness called RAD, or reactive attachment disorder.
"These are kids who, biologically, are feeling stressed all the time," explained Doug Goldsmith of the Children's Center.
RAD kids actually endure chemical changes and physical damage to the brain. It happens in their first couple of years when there's a shifting succession of caregivers, and the kids fail to form a parental bond. They avoid seeking assistance from adults even when they have a childhood crisis.
"They don't go seek out mom," Goldsmith said. "In fact, they don't even look up when they're cut, and they're hurt because they've learned that there's no reason to go to adults for care."
In the United States, RAD children are sometimes born to drug-addicted parents. Families adopting internationally are at especially high-risk if the kids are older than perhaps 2 or 3 years old.
Families adopting internationally are at especially high-risk if the kids are older than perhaps 2 or 3 years old.
"Most of these kids we're talking about are being raised in institutions outside the U.S." Goldsmith said.
Victoria BeanThere's often a tragic undercurrent of abuse and neglect in the orphanage. Jodi now suspects Victoria suffered serious abuse at the orphanage in Belarus.
"I have to think there was definitely trauma, some intense trauma there," Jodi said.
Goldsmith says many dubious treatments have been promoted over the years; none of them proven scientifically, some of them outright dangerous. But professional psychologists are beginning to come to grips with it.
"We've seen many, many wonderful successes," Goldsmith said. "The earlier we treat it, the better off we are."
Jodi is self-publishing her book called "Love Lessons," and she has a website to help other families.
She admits she sometimes hated Victoria in their first few years together. Hate sometimes gave way to indifference, which Jodi said is worse.
Hate sometimes gave way to indifference, which Jodi said is worse.
But for mother and daughter, love slowly arrived through counseling, horse therapy and intensely focused, highly-structured parenting.
"In the beginning, obviously for the first three years, it was hard to love anything about her. But now I honestly can say I love everything about her because I've seen who she is," Jodi said.
E-mail: [email protected]
Related links
Most recent Utah stories
Related topics
UtahJohn Hollenhorst
Attachment Disorder: 8 Tips for Parents and Carers
Photo from army.mil
It is human nature to seek another person, establish close relationships, become attached to someone who shows warmth and care. It is in the nature of a child to become attached to parents, grandparents, brothers and sisters, or to those who in their lives replace blood relatives.
Man is a social being, and therefore, even in conditions when parents neglect their duties, not satisfying the basic needs of the baby for food, comfort, affection, in the overwhelming majority of cases, he still loves a cruel mother or a father who drinks heavily and does not want to be separated with them.
But it happens in a different way. The difficult conditions in which the early development of the child proceeds can lead to a disease that is difficult to treat.
Most often, this problem is faced by adoptive parents whose child has experienced trouble in the birth family, and then ended up in an orphanage. The situation is even more difficult when the child has already been adopted by the family and then returned back to the children's institution.
However, there are cases of RRS in families with many children, where no one helps the mother and some of the children receive very little attention and care. The disorder can develop if the child was separated early from the parents for a long time as a result of a long hospital stay, or if the child spent most of the time with a mother suffering from depression or other serious illness that prevented her from properly caring for the child.
What is reactive attachment disorder?

Photo courtesy of phillypsychology.com
This is a condition in which a child does not form an emotional attachment to parents or persons acting in their stead. Symptoms of the disorder appear before the age of 5 years, often as early as infancy. This is lethargy, refusal to communicate, self-isolation. A small child is indifferent to toys and games, does not ask to be held, does not seek solace in physical pain. He rarely smiles, avoids eye contact, and appears sad and apathetic.
As they grow older, signs of self-isolation can manifest themselves in two seemingly opposite types of behavior: disinhibited and inhibited.
With disinhibited behavior, the child seeks to attract the attention of even strangers, often seeks help, performs acts that are inappropriate for his age (for example, comes to bed with his parents).
Misunderstanding, lack of patience, severe negative reaction to the child's behavior on the part of a significant adult can cause irritation, anger or an outburst of aggression on the part of the child, and if the violation persists in adolescence, alcohol abuse, drug addiction and other types of antisocial behavior.
With inhibited behavior, the child avoids communication and refuses help. In some cases, both types of behavior, both disinhibited and inhibited, are alternately observed in him.
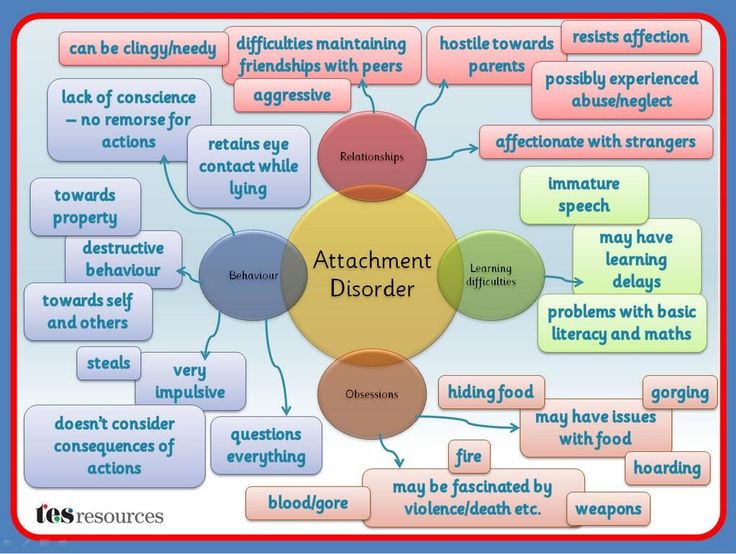
Reactive attachment disorder can manifest in forms that sometimes cause despair in adoptive parents: the child constantly lies, steals, behaves impulsively, shows cruelty to animals and a complete lack of consciousness. He does not express regret or remorse after unacceptable behavior.
Diagnosing RRP is not an easy task. Some features of this disorder can be seen in attention deficit hyperactivity disorder (ADHD), anxiety disorder, autism, and post-traumatic stress disorder. In order to make an accurate diagnosis, it is necessary to observe the child's behavior in various situations over a certain period of time, analyze his biographical data, and evaluate the interaction of parents with the child.
In order to make an accurate diagnosis, it is necessary to observe the child's behavior in various situations over a certain period of time, analyze his biographical data, and evaluate the interaction of parents with the child.
Even harder to treat him
Photo from helpguide.org
Psychiatrists sometimes prescribe drugs to children with RAD, but in some cases they can only slightly improve the background against which the therapeutic interaction with the child will take place.
A child's parents or guardians play a key role in treatment. It is they who, with the help of doctors and psychologists, will have to create such an environment in which he can experience a healthy addiction, believe that an adult can be relied upon, and begin to trust him.
Experts believe that the therapeutic environment has 3 essential components: safety, stability and sensitivity.
In order to overcome the consequences of those events that caused the child's inability to form close and warm relationships, an adult must have enough time and patience to listen and hear the child with an open mind and without trying to judge him.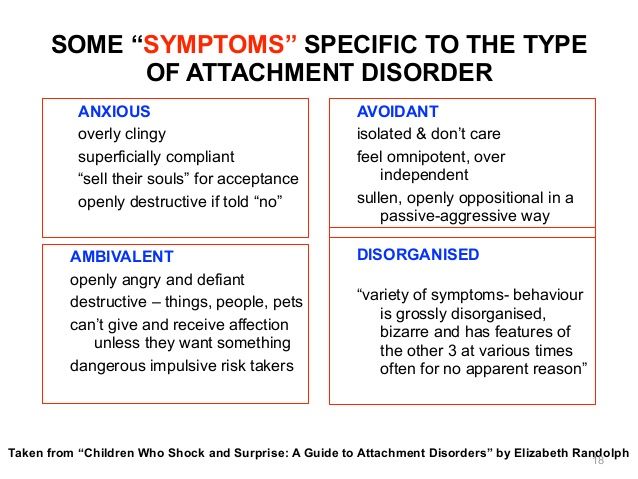
The child needs boundaries, but they must be set in a context of understanding and empathy. Only if the child feels emotional safety , that is, he understands that his story about himself will not cause a negative assessment from an adult, he will be filled with confidence and tell his foster mother or psychologist about the difficult experiences of his early childhood.
The second component after security is stability . The figure of an adult for the formation of a primary attachment must remain the same. It takes a long time to establish trust between a significant adult and a child with RAD. Changing such a figure, moving from one foster family to another, not only slows down the process, but also aggravates the disorder.
Having gone through the painful experience of ignoring his needs, the child must re-learn to be aware of them, as well as the fact that the same person can satisfy them over and over again: feed, give clean clothes, put in a warm bed, play, listen and comfort, help with the performance of tasks. Such children are often afraid that the new mother will abandon them or die, and only after a long period of stability do these fears subside.
Such children are often afraid that the new mother will abandon them or die, and only after a long period of stability do these fears subside.
Some children need at least a year of stability to begin to trust their significant adult, others become imbued with trust in foster parents after a few months. It depends on the temperament of the child (it is important, for example, whether he is an extrovert or an introvert), as well as how well the child and his new parent fit together in various ways.
Photo from wisegeekhealth.com
Long separations between a foster child and mother are undesirable: they can activate his defensive reaction, which is self-isolation.
And finally sensitivity . This is the emotional availability of an adult, his attentiveness to the needs of the child. Adoptive parents should be informed by specialists that while the mental development of a child with RAD may be age appropriate, his emotions often remain immature, which means that during the process of attachment formation, the need for an adult may be greater than that of a healthy child of the same age.
During this transitional period, parents must be very patient, be prepared for unexpected behaviors that are signals that the child is going through some earlier stages of development and attachment.
For example, a child who behaved suspiciously and aloofly suddenly begins to obsessively follow his mother, constantly report his fears, climb on his knees or come to sleep in his parent's bed - in a word, behave as if he suddenly stood on 2-3 years younger. In this case, parents should accept the situation and meet the child's need for greater dependence on them.
It is important for adoptive parents to understand the logic of changes happening to the child. Some adopted children initially seem emotionally cold, as experience has taught them that it is not safe for them to express their feelings and communicate their desires. At the same time, the child gives the impression of being completely obedient, because he does not show any irritation or discontent, does not talk about his needs.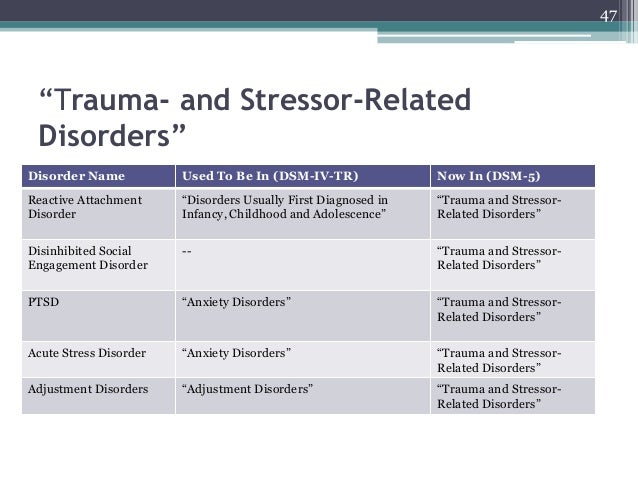
Feeling safe, he intuitively feels that adults accept him and will not refuse him, which means that it is quite safe to declare your desires in any form, up to whims and tantrums.
If earlier the child remained indifferent to whether the mother was at home or she had gone somewhere, now he may burst into tears, cling to her and not let her go if she was about to leave without him. This is not easy for parents, but such behavior should be seen as a positive sign: attachment is gradually formed, the child overcomes the destructive consequences of his difficult early childhood.
In the case of RAD, the task of the psychologist is primarily to educate the parents and support them in creating a safe and stable environment for the child at home, but activities with the child can also be useful. Play therapy and other techniques can help the child to realize their own needs, to build trusting relationships with a new significant adult.
Photo courtesy of drpokea. com
com
At the same time, parents should be wary of offerings to work with their child using methods that are collectively called Attachment Therapy.
Not only does this therapy lack scientific evidence and documented efficacy, it is also not safe.
Attachment therapy combines a number of violent methods, the most famous of which are holding therapy (holding) and rebirthing (“rebirth”).
In "rebirth", the baby's body is wrapped in a blanket and forced to crawl through compressed pillows, simulating passage through the birth canal. It is assumed that "having been born again", he overcomes past negative experiences and is ready for intimacy with his mother. In 2000, a 10-year-old girl suffocated during such a procedure in Colorado (USA), and this therapy has since been banned in the state.
Until now, there are quite a few adherents of holding therapy for the treatment of autism and RRP, among them the well-known psychologists in our country, Dr. OS Nikolskaya and M. M. Liebling.
M. Liebling.
The essence of therapy is that the mother forcibly holds the child in her arms and, despite his resistance, tells him how much she needs him and how much she loves him. It is assumed that after a period of resistance, when the child tries to escape, scratches and bites, relaxation occurs, during which contact is established between mother and child.
Critics of the method argue that it is not ethical, as it is based on physical coercion, and can provoke a regression in the development of the child. Indeed, how can trust be established on the part of a child in an adult who uses physical violence against him?
Raising a child with a reactive disorder is associated with enormous emotional costs, sometimes with stress for parents who blame themselves if they do not see positive changes in the child's condition and behavior for a long time.
If your child is diagnosed with RDD
Photo from helpyourteennow.com
- Remember that there are no miracle cures to achieve a breakthrough in a child's condition in a short time.
 There is no substitute for a therapeutic home environment, security, stability, and your willingness to respond emotionally to your child's needs.
There is no substitute for a therapeutic home environment, security, stability, and your willingness to respond emotionally to your child's needs. - Be sure to find an opportunity and a way to restore your own emotional balance. A child with RAD is already stressed, and your anxiety or irritability can make it worse. To feel safe, the child must feel your calmness and firmness.
- Set boundaries for what is permitted. The child must understand what behavior is unacceptable and what consequences await him in case of violation of the rules. It is important to explain to the child that your rejection does not apply to him, but to certain of his actions.
- After a conflict, be ready to quickly reconnect with your child to let him feel that the reason for your dissatisfaction was a particular behavior, but you love him and cherish the relationship with him.
- If you were wrong about something, don't be afraid to admit your mistake. This will strengthen your bond with your child.
- Set a daily routine for your child and monitor his performance. This will reduce the level of anxiety in the child.
- If possible, show your love for your child through bodily contact: rocking, hugging and holding. However, keep in mind that if a child has been abused or traumatized, he will initially resist being touched, so you will need to work slowly.
- Set aside time that you will completely devote to the child, you will play, talk, walk with him, without being distracted by other activities or other people. This is a very important part of your relationship.
You have a difficult task ahead of you, but it can be done. Do not rush things, be patient and do not lose hope.
Sources:
Reactive attachment disorder in childhood
Psychological and Behavioral Interventions
Attachment Issues and Reactive Attachment Disorder
Rebirthing therapy banned after girl died in 70 minute struggle
The Dangers of Holding Therapy Source: LETIDOR
Let's figure out what threatens a child to lose a secure attachment to a significant adult.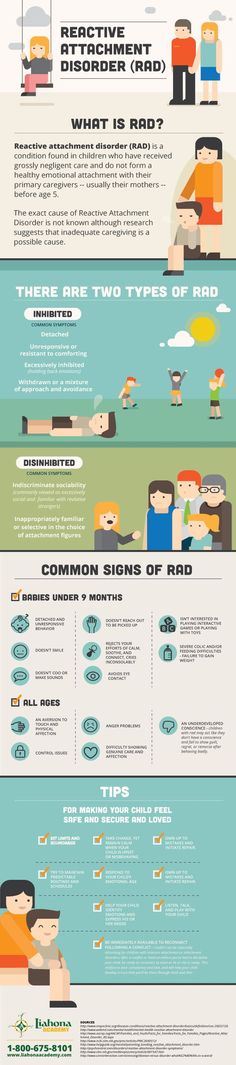
Our regular author Diana Mashkova, writer, journalist, head of the “Enlightenment” direction of the Arithmetic of Kindness Foundation, mother of 4 children, 3 of which are adopted, has already told us about the correct hierarchy in the foster family, and about the stages of adaptation of the adopted child in the family , and about relationships with blood relatives of the adopted child. In a new article, Diana explains the importance of maintaining attachment and the dangers of breaking it.
A large number of modern adults - scientists say the figure is 45% - did not develop a reliable attachment to their parents in childhood. Unfortunately, this is not just a fact from their past. This is something that affects a person all his life: affects health, relationships with other people, resilience, self-confidence and many other issues.
People who are deprived of “secure attachment” in the first years of life often unconsciously reproduce the broken model in their own family, with their children, passing on the broken relationship code from generation to generation. Can this vicious circle be broken?
Can this vicious circle be broken?
What is attachment? If we turn to the definition, this is a mutual process of forming emotional bonds between people that persist indefinitely, even if people are separated.
For adults, this is a useful thing that unites the closest people. For children, it is a vital need and a vital necessity.
For an infant, a mother or a person who constantly replaces her is a natural source of food, warmth, security, comfort, joy and other emotions. The kid is not able to feed himself, or calm, or captivate. Therefore, the development of the child stops in loneliness, the subconscious setting turns on: “nobody needs me”, which is one of the reasons for the high infant mortality in institutions for orphans.
Attachment is not given to a child by the fact of birth, it arises gradually, in the daily interaction of an adult and a child.
The baby experiences a natural need - hunger, thirst, discomfort, which he cannot satisfy on his own, and therefore cries. A significant adult comes to the call - feeds, waters, changes diapers, and at the same time gently sentences, kisses and cuddles. Out of this healthy circle of relationships—the need, the call, the coming of the adult, the satisfaction of the need involved—is born the basis for development.
A significant adult comes to the call - feeds, waters, changes diapers, and at the same time gently sentences, kisses and cuddles. Out of this healthy circle of relationships—the need, the call, the coming of the adult, the satisfaction of the need involved—is born the basis for development.
He learns to trust an adult who is reliable and not indifferent, and through trust in a loved one, trust in other people and in the whole world is born. A secure future is born.
An excellent basis for understanding the essence and mechanisms of attachment can be a book by the classic of developmental psychology by the outstanding English scientist John Bowlby. It's called "Attachment".
An even easier way to get acquainted with the basics is to read the book by the famous Russian psychologist Lyudmila Petranovskaya “Secret support. Attachment in a child's life.
The main thing is to realize that a healthy attachment instills in a child the ability to love, understand their own feelings and the feelings of others, control their emotional outbursts, learn and gain knowledge, think logically, have self-respect and build relationships with other people. It protects against many psychosomatic diseases and reduces the risks of possible developmental delays.
It protects against many psychosomatic diseases and reduces the risks of possible developmental delays.
This is the indisputable value of secure attachment in a child's life.
“From World War II onwards,” writes world-famous psychologist and therapist Nils Peter Rygaard in his book Attachment Disordered Children, “with acceleration into the 1960s, we undertook the largest social experiment ever was held in the western world: mothers of toddlers and preschool children went to work outside the home, away from their babies... The conditions for learning how to become human through relationships during early childhood were turned on their head. To date, we are probably the only mammalian species in which mother and infant do not remain inseparable for at least the first two to three years after birth."
In maternity hospitals, newborns begin to be separated from their mothers immediately after birth, supposedly giving the woman in labor time to recover, but in reality traumatizing both and causing anxiety, insecurity and guilt in women.
In the Soviet Union, babies are sent to a nursery from the age of four months, and sometimes even earlier, separated from their mothers despite the vital needs for breastfeeding, caress, tactile contact and love. There are kindergartens - five days, which allow parents to work, arrange their personal lives and earn money, and doom children to severe experiences of loss and pain of separation.
Deprivation, the inevitable and eternal companion of orphans in state institutions, suddenly seizes family children as well.
Parents are forbidden to take babies in their arms so that they “do not get used to”, they are ordered to feed them by the hour, and not on demand, they do not allow mothers to be with small children in hospitals and other “health” institutions.
Many of us today's adults have fallen victim to these rash actions. It is in them that the reason for those same 45% of people with insecure attachment.
An attachment disorder can manifest itself in many ways. Much depends on the individual characteristics of the child - his psychological structure, temperament, hardiness. What is quite easily tolerated by some children turns out to be a deep trauma for others.
Much depends on the individual characteristics of the child - his psychological structure, temperament, hardiness. What is quite easily tolerated by some children turns out to be a deep trauma for others.
The book The Boy Who Was Raised Like a Dog by the famous psychotherapist Bruce Perry tells the story of a teenage rapist, an asocial type, whose cruel crimes horrify even specialists. But most of all - his own parents, who do not understand what is happening to their youngest son.
The eldest child grew up to be a fine boy, and the youngest turned out to be a criminal, although both were brought up by the same parents.
How could this happen? Gradually, in the course of working with the family, the therapist gets to the bottom - it turns out that the youngest son developed a severe attachment disorder in infancy.
Immediately after his birth, the family moved to a new area, where my mother had no relatives, no friends, no support. Due to a slight mental retardation, she could not cope with two children at once, besides, the youngest turned out to be extremely restless and irritated the woman. She fed him in the morning, swaddled him and left him in the crib for the whole day, and she herself went for a walk with her eldest son. She returned only in the evening, when her husband came home from work.
She fed him in the morning, swaddled him and left him in the crib for the whole day, and she herself went for a walk with her eldest son. She returned only in the evening, when her husband came home from work.
So the boy grew up - in a family, but without a mother, who had no one to replace. And all further violations started in that period of life, which he did not even remember.
If a less sensitive child were in this guy's place, he could get out of the situation differently, he could get the love of close adults at an older age. But it was for this child that neglect of needs had fatal consequences.
There are no common "event-consequence" schemes for all. There is a unique set of impairments and injuries that lead to unpredictable outcomes.
One child may show aggression, another may have depression, a third may have a psychosomatic illness, a fourth may have suicidal tendencies, a fifth may be unsociable, a sixth may have extremely low self-esteem, a seventh may lack empathy, and so on. And for someone - all at once. This is impossible to predict.
And for someone - all at once. This is impossible to predict.
Therefore, for comparison, I will just give one more real example.
Saniya Ispergenova was brought up in an orphanage from birth to the age of 18. In her book “I am Sania. The Story of an Orphan, published with the support of the Arithmetic of Kindness charity foundation, traces the influence of deprivation and attachment violations on the entire path of becoming a person.
The girl talks about health disorders (nervous enuresis, multiple pneumonias and bronchitis in childhood), about a terrible fear of people, about sensory deprivation, about social deprivation, about the inability to build close relationships, about the lack of empathy and much more.
“Haptic contact was the most difficult for me ,” she shares with readers. - I got used to every fleeting touch for a long time, entered into relationships, as if into cold water. She moved forward in small, barely perceptible steps.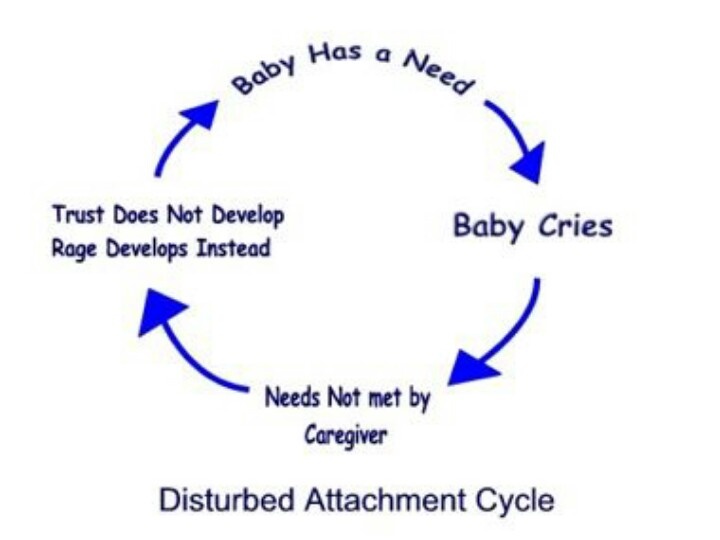
After life without a mother, without a family, it was difficult to learn hugs, kisses, touches - all this seemed too complicated a science.
Lack of attention and care in childhood interfered with the formation of emotional intelligence.
“Then it never occurred to me,” says Sania, “that inside an adult, his own emotions are seething. Who and when spoke to us about feelings? Who taught to recognize joy or sadness, fun or despair, pleasure or pain? There was nothing. I could not name my own experiences and, like a blind man, did not pay attention to the feelings of others. The people around me never seemed upset or, conversely, happy. Frightened or, conversely, calm. To be honest, I didn't care about them at all. Years of inattention to my own feelings returned in adolescence as a boomerang of indifference.
Sanya's story is a prime example of a serious attachment disorder. And yet he is life-affirming: Sania proves to readers that a person is able to change his future. The main thing is not to give up, to wish for change and look for support in life.
The main thing is not to give up, to wish for change and look for support in life.
What helps to cope with the consequences of attachment violation?
Of course, the first step is to discover the problem and become aware of it. Do not write off all the difficulties of relations with the child on children's whims, "bad" heredity or bad character, but try to understand the essence of what is happening.
Parents themselves are often the first people to see problems. In the case of orphans, adoptive parents.
And then the main task is to build a trusting and warm relationship with the child. At any price. It is on this - not on study, circles or sports - that all efforts in the family should be directed. Just to build a bond.
Specialists working with cases of such a disorder confirm that the efforts of parents are primary, and the efforts of psychologists and psychotherapists for success are secondary. A trusting relationship with a significant adult is precisely the foundation on which the whole life of a child is built: it develops, talents are revealed, and physical and mental health is formed.