Therapy for hocd
HOCD: How to Identify and Manage It
HOCD is the abbreviation for homosexual obsessive-compulsive disorder. It’s also known as SO-OCD (sexual orientation) or “gay OCD.” It is a variant of OCD, and can have a profound impact on the lives of those living with it.
HOCD — The Basics
How Common Is It?
HOCD affects less than 1% of the population. OCD, the broader category in which HOCD falls, affects 1.2% of Americans — approximately 3.95 million people. Of those 3.95 million, estimates are that 8% of them have sexual orientation obsessions. So a reasonable estimate of the number of Americans suffering from sexual orientation-themed OCD would be 315,000. This a large number for such an infrequently discussed phenomenon! It’s similar to the numbers estimated for Americans living with multiple sclerosis, and more than the number of people living in Cincinnati, Ohio.
One factor that perhaps makes HOCD more torturous than other types of OCD is its relative obscurity. Therapists who specialize in OCD are typically familiar with HOCD, but most other therapists are not. If you ask most people what OCD is, their answers will likely involve a preoccupation with order, being excessively neat, or washing your hands. These can indeed be symptoms of OCD, but for some people, OCD can look completely different.
Is HOCD a Real Thing?
HOCD is poorly understood outside of the OCD community. For this reason, many people misunderstand it to be “repressed” homosexuality. Others mistakenly interpret it as an early part of the coming out process. HOCD has been around for a long time and, to those in the know, is an established and well-understood sub-type of OCD.
Note: HOCD can affect people of any sexual orientation. For simplicity’s sake, this article describes the experience of a straight person with obsessions about being gay. Everything written here can be applied to a gay person with obsessions about being straight; just swap the words “gay” and “straight. ”
”
The core symptoms of HOCD are intrusive thoughts about being gay. These can lead to any of the following:
- Difficulty setting aside thoughts about your sexual orientation
- Diminished attraction to the opposite sex
- Reviewing your day or week to feel sure that at no time did you feel attracted to someone of your own sex
- Preoccupation with one’s level of arousal toward either sex
- Avoidance of people of the same sex
- Construing any positive reaction to a member of the same sex as evidence of being gay
- Checking one’s response to opposite- or same-sex images of attractive people
- An urgent need to decide whether one is gay or straight
- Spending time in anxious rumination about one’s reaction to members of the same or opposite sex, looking for proof that one is gay/straight
- Looking at pornography, not because of enjoyment but because it is an opportunity to check one’s responses to men vs. women
Common Intrusive Thoughts in HOCD
- What if I’m gay?
- Did my noticing that man/woman just now mean I’m gay?
- Did my childhood interest in rugby/dance as a kid mean I’ve always been gay and missed the signs?
- Do my friends think I’m gay? If so, are they right?
- How can I continue in this relationship if I’m actually gay? That’s dishonest!
- What if these thoughts never go away?
- How much am I *really* enjoying this stereotypically straight man/woman activity? Maybe not enough!
- Why did I slow my pace a little when I walked by the LGBT community center the other day?
HOCD Compulsions
Claire WeekesCompulsions in HOCD run the gamut from the unnoticeable and subtle all the way to the life-altering. People with HOCD feel a strong temptation to eliminate uncertainty about whether they are straight or gay. This has some parallels to Claire Weekes‘ metaphor of swimming rather than floating; you want the anxiety to go away, and assume that hard work is needed to make that happen. Paradoxically, the healthiest thing we can do in these situations is… nothing.
People with HOCD feel a strong temptation to eliminate uncertainty about whether they are straight or gay. This has some parallels to Claire Weekes‘ metaphor of swimming rather than floating; you want the anxiety to go away, and assume that hard work is needed to make that happen. Paradoxically, the healthiest thing we can do in these situations is… nothing.
The Role of Tolerating Uncertainty
The more someone with HOCD seeks certainty, the more they weaken their innate ability to tolerate uncertainty. We all have the ability to tolerate uncertainty. We can tolerate not knowing what we’ll wear tomorrow, we can tolerate not knowing exactly where we’ll be in a year. So why are obsessive thoughts so hard to tolerate?
Partially, they’re hard to tolerate because they run counter to our well-rehearsed habits of eliminating that uncertainty. People with HOCD are tempted by the prospect of “figuring out” if they’re gay or straight, either by checking in some fashion or by mental exercise. There is no comparable temptation to “figure out” where we’ll be in a year because we know we can’t. That temptation makes the HOCD thought hard to tolerate.
There is no comparable temptation to “figure out” where we’ll be in a year because we know we can’t. That temptation makes the HOCD thought hard to tolerate.
For people with HOCD, tolerating anxiety around their sexual orientation is analogous to acquiring a taste for healthier foods if you’re used to eating junk food. If you’re used to pork chops and macaroni every day, your first taste of broccoli might not be appealing. However, the more you work it into your diet, the more you can tolerate it. You might even come to enjoy it!
Similarly, if someone with HOCD has never tried anxiety tolerance as a means of coping, it will be difficult at first. It may feel pointless, painful, and unproductive. Over time, however, with continued effort, it will feel easier and more natural.
There are two options for those who would like to improve their HOCD symptoms. You can work with a professional or try to make changes on your own.
How You Can Battle HOCD on Your Own
If you have HOCD, The good news is that there are a lot of things you can do to help yourself. Several strategies are listed below that have been helpful for many suffering from HOCD. One challenge in implementing them is that the obsessive thoughts are hard to shake, and feel very convincing.
Several strategies are listed below that have been helpful for many suffering from HOCD. One challenge in implementing them is that the obsessive thoughts are hard to shake, and feel very convincing.
The HOCD Thoughts Feel Real
People with HOCD are often thrown by their obsessions, and explain that the thoughts “feel so real.” Why is that?
The answer involves fear, repetition, and the power of mental habits. People with HOCD focus excessively on their reaction to men vs. women. The fearful intensity of that focus makes it impossible to distinguish between real desire and fear of real desire. (Similar phenomena happen in other anxiety disorders – for example, people who suffer from panic disorder also become very focused on a feared internal experience. In their case, it’s a sensation and not a desire, but the situations are similar.) When this inability to discern real sexual preferences repeatedly meets with fear and pessimism, there are consequences.
Sometimes people with HOCD go from being anxious because they’re unsure if they’re gay to being convinced that they’re gay. Instead of feeling horrified that they might have been wrong about being straight, they start to feel horrified that they are certainly wrong about being straight. This shift in thinking reduces the questioning of one’s sexual orientation; the belief that one has been masquerading as straight becomes strong and solid. This is sometimes referred to as overvalued ideation.
Instead of feeling horrified that they might have been wrong about being straight, they start to feel horrified that they are certainly wrong about being straight. This shift in thinking reduces the questioning of one’s sexual orientation; the belief that one has been masquerading as straight becomes strong and solid. This is sometimes referred to as overvalued ideation.
This is a difficult problem to address, but two strategies can be helpful: mindfulness and creating uncertainty.
Mindfulness
The traditions of meditation and mindfulness offer a valuable perspective for those struggling with upsetting thoughts about one’s sexual orientation. From the mindfulness perspective, no thoughts are real, regardless of how they feel. They are all temporary experiences without any inherent substance or profound meaning.
Mindfulness practice helps us maintain a healthy relationship with thoughts (and emotions). It helps us remember that even beliefs we take for granted — e. g., that I’m reading an article on HOCD right now — are not reality. They may be factually based and accurate, but are still just beliefs. This is a useful perspective for someone with HOCD to have as they cope with thoughts and beliefs around their sexual orientation.
g., that I’m reading an article on HOCD right now — are not reality. They may be factually based and accurate, but are still just beliefs. This is a useful perspective for someone with HOCD to have as they cope with thoughts and beliefs around their sexual orientation.
What makes a thought feel real is the attention we bring to it.
Nancy Colier LCSW, Rev.
The “Lloyd Christmas” Technique
This is ideally used in the context of exposure and response prevention therapy, with the assistance of a trained therapist, but is presented here in the hopes that it might be useful to others.
Typically in OCD treatment, the emphasis is on learning to tolerate uncertainty. With the “Lloyd Christmas” technique, the person with HOCD strives to manufacture uncertainty. (Lloyd Christmas was the name of the character played by Jim Carrey in the film “Dumb and Dumber” who succeeded in creating doubt where there had been none — see video below. ) This technique is appropriate for when you’re feeling completely convinced that you’re gay (or straight!). A therapist using the Lloyd Christmas technique helps an HOCD patient who is quite convinced that he or she is gay to create some doubt about their sexual orientation. You can try this on your own by briefly contemplating any of the following:
) This technique is appropriate for when you’re feeling completely convinced that you’re gay (or straight!). A therapist using the Lloyd Christmas technique helps an HOCD patient who is quite convinced that he or she is gay to create some doubt about their sexual orientation. You can try this on your own by briefly contemplating any of the following:
- past sexual relationships as possible evidence you might be straight
- hobbies or interests you have that are stereotypically heterosexual
- perhaps your friends think you’re straight
- past aversive reactions to same-sex flirting, touching, or erotic material
- past serious and long-lasting romantic relationships with someone of the opposite sex
Granted, none of the above factors prove that someone is straight or gay. However, they are not intended to convince you that you’re straight. Their job is to create some doubt! If you can see how one of the above factors might reduce the “odds” of your being gay from 100% to 80%, then this technique has been a success.
It’s important not to use this technique for too long. If one overindulges in it, it becomes simply a form of reassurance and can become compulsive. The key with the Lloyd Christmas technique is to only use it as long as needed to create some doubt, and then to stop.
How Can I Get Rid of HOCD Thoughts?
Understandably, the most common impulse of someone with HOCD is to try to get rid of the obsessive thoughts. In many ways, this impulse is the root of the problem.
The more we try not to think about something specific, the more it tends to crop up in our minds. The effect of the phenomenon is clear for those suffering from intrusive thoughts about sexual orientation or any other common obsessive topic. The more we try to get rid of an undesirable thought, the more it will come up! The lesson is clear: abandon efforts to get rid of the thoughts.
The more we try to get rid of an undesirable thought, the more it will come up! The lesson is clear: abandon efforts to get rid of the thoughts.
The 4-Step ERP Technique for HOCD Obsessions
When an intrusive thought strikes, be ready. The following four-step technique will help you practice precisely the skills necessary to reduce your HOCD symptoms. It’s based on the components of exposure and response prevention therapy, which is described below.
How to cope with HOCD thoughts when they arise:
- “Maybe I’m gay.”
Acknowledge to yourself the possibility that you may be gay. After all, nobody knows for 100% sure, and neither do you.
- “Maybe I’m not.”
Similarly, acknowledge that it’s also absolutely possible that you may be straight.
- “I don’t know.”
Admit to yourself that you just aren’t sure right now whether you’re gay or straight, and rest in that without trying to fix it.

- “I’m not going to try to figure it out right now.”
This is the “response prevention” step. Resolve to yourself that for the next few minutes, you will refrain from efforts to determine whether you’re gay or straight. Allow the question to remain unanswered.
Knowing Which Strategy to Use and When
Remember, it is possible to feel 100% certain of something and to be wrong about it. When symptoms are severe, some straight people with HOCD describe feeling 100% sure that they are gay. One helpful step in combatting HOCD anxiety is to ask yourself: how certain am I that I’m gay vs. straight?
If you’ve spent most of the past few days feeling certain that you are gay, then use the Lloyd Christmas technique described above. Then try to use the 4-step ERP technique.
If, on the other hand, HOCD symptoms have not dominated the past few days, then try the 4-step ERP technique. Go through those four steps each time an intrusive thought arises, and be prepared to do it a million times. Be relentlessly patient in your battle against OCD; be willing to use these techniques forever if necessary.
Be relentlessly patient in your battle against OCD; be willing to use these techniques forever if necessary.
Generally speaking, it’s always helpful in battling HOCD to keep the following points in mind:
- Thoughts are just thoughts, they are not reality. The same goes for feelings. If you’re feeling completely sure at times that you’re gay, remember this quote from the movie Doubt: “Certainty is a feeling, not a fact.”
- If you’re able to confront the possibility that you may indeed be gay, but also may be straight, try to rest in that uncertainty without resolving the question. It’s not easy, but the more you can do that, the more you will weaken OCD.
HOCD Treatment With a Professional
The treatment of choice for sexual orientation obsessions is a form of cognitive-behavioral therapy called exposure and response prevention (ERP). Improving your ability to tolerate intrusive thoughts is an excellent way to reduce HOCD symptoms. Another way is to reevaluate the meaning you attribute to HOCD thoughts, images and impulses. ERP therapy helps you develop both of these skills.
Another way is to reevaluate the meaning you attribute to HOCD thoughts, images and impulses. ERP therapy helps you develop both of these skills.
What Does ERP Therapy Involve for HOCD?
The first stage of ERP is informational. You will learn about OCD and about how obsessions and compulsions work. Your therapist will teach you different ways of understanding the thoughts and feelings you’ve been having. (Check out our post with examples of how HOCD presents and how treatment can help.) This way of understanding your symptoms is a critical framework for what comes next.
Next, your therapist and you will develop a list of people, places, situations, images, etc. that trigger the anxiety that comes with HOCD thoughts. Your therapist will then teach you how to do exercises called exposures. In these exercises, you purposefully “expose” yourself to something that will evoke a little bit of HOCD anxiety. Following that, you practice responding differently than you have been; you refrain as best you can from efforts to seek reassurance about your sexual orientation. You also refrain from ruminating about the possibility that you might be gay. If you’re able to refrain from doing these things for a long enough time, you will weaken your HOCD.
You also refrain from ruminating about the possibility that you might be gay. If you’re able to refrain from doing these things for a long enough time, you will weaken your HOCD.
Under the therapist’s guidance, the more you do the exposure exercises, the more you will improve.
Mindfulness as Part of HOCD Treatment
More and more psychotherapy (cognitive-behavioral and otherwise) in recent years has included an emphasis on mindfulness. Mindfulness derives from ancient traditions of meditation. Mindfulness is an awareness that we all have at times — an awareness that is relaxed, focused on the present, and not caught up in distracting thoughts. Some folks incorrectly think of mindfulness as a fad — in reality, mindfulness is an innate capacity of mind that we all have to one degree or another. By doing certain practices we can cultivate this awareness so that it becomes easier to access. This informs our experience of anxiety and other emotions, and in some cases, even how we live our lives.
Importantly for those with intrusive thoughts, mindfulness helps us relate to our thoughts as they actually are: insubstantial and much less important than they feel in the moment.
Does Traditional Therapy Help?
Traditional insight-oriented therapy is unlikely to help someone with HOCD. This type of therapy aims to — as the name suggests — produce insight. Typically, the desired insight is around the origin of the problem. However, for people with obsessive thoughts, the origin of the problem is 1) usually impossible to find and 2) not helpful even if you do find it. For these reasons, as well as the lack of emphasis on concrete strategies to navigate the symptoms, traditional therapy is typically unhelpful for HOCD.
This is a major problem in access to effective HOCD treatment in the United States. If you have HOCD and see a random therapist, you are not likely to find someone who recognizes and understands HOCD. Consider doing a consultation with an OCD specialist if at all possible.
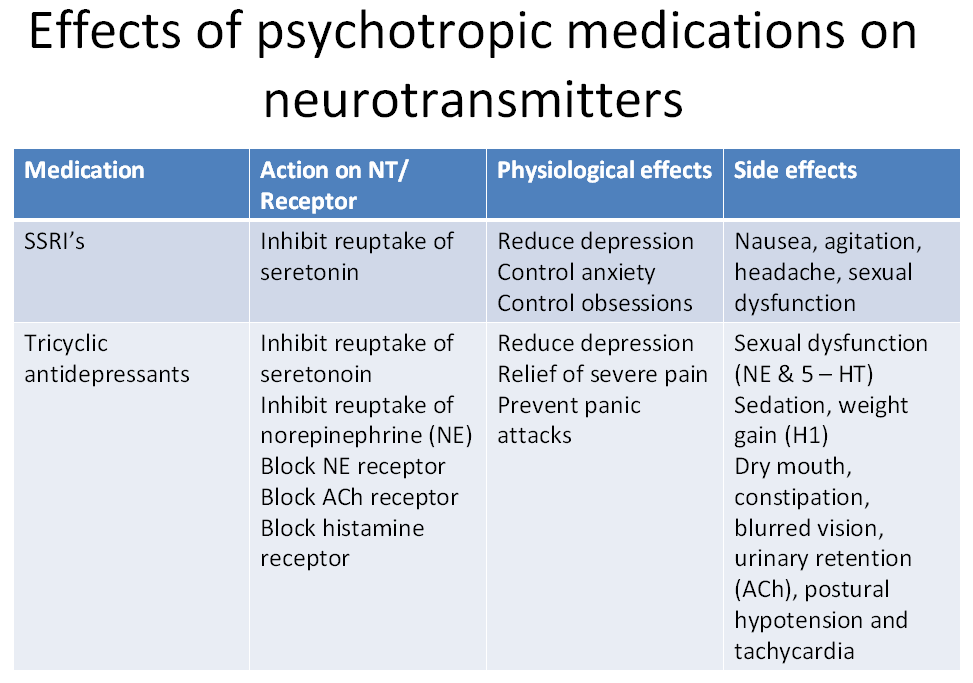
Do Medications Help?
Medications can be part of the solution for someone suffering from intrusive thoughts about their sexual orientation.
Selective serotonin reuptake inhibitors (SSRIs) are often prescribed in high doses to address symptoms of OCD. Anafranil (clomipramine) is also used in some cases. These medications can help bring down the severity of the HOCD symptoms. However, in our experience, it is quite unusual for someone to make significant and lasting progress against HOCD without learning, to some extent, how to understand and cope with the intrusive thoughts.
HOCD Frequently Asked Questions
What causes HOCD?
Remember that HOCD is not distinct from OCD. We know that several factors increase the risk of having OCD, including genetics and learning history.
How is HOCD treated?
The primary recommended treatment is a form of therapy called exposure and response prevention. This therapy helps people develop their ability to tolerate obsessive thoughts so their impact lessens over time.
This therapy helps people develop their ability to tolerate obsessive thoughts so their impact lessens over time.
Can you have HOCD without OCD?
No. If you have HOCD, you have OCD.
Can HOCD change your sexuality?
No. There are no known instances of HOCD or anxiety changing anyone’s sexual orientation.
When will HOCD go away?
The more you interpret HOCD thoughts and impulses as evidence of your sexual orientation, the longer HOCD will stick around. The more you are able to practice tolerating the thoughts without ascribing meaning to them, the sooner HOCD will subside.
How can you tell if you have HOCD or if you’re in denial about your sexual orientation?
HOCD is characterized by an urgent needing to know about whether one is gay or straight. People who have not yet come to terms with a given sexual orientation do not feel any such urgency.
Let’s Hear From You
Let us know about your experience in the comments below. If you have questions this page did not address, please mention them and we will try to address them as the page is updated over the years.
Please contact us if we can help you in your efforts to find anxiety therapy here in New York. Our CBT therapists are doctoral-level psychologists. We also have student therapists who offer reduced-fee services. Our offices are in midtown Manhattan, but we offer teletherapy services to people elsewhere in New York State, New Jersey, and Florida. If you’re looking for CBT therapy in another part of the country or world, please contact us, we are happy to help!
Contact Us
Treatment for HOCD | Sheppard Pratt
Obsessive-compulsive disorder is treated with a form of psychotherapy called cognitive behavioral therapy. It is a present-focused therapy that addresses how you are responding to your thoughts and feelings and how these responses can be modified to improve your mental health. Treatment for HOCD is no different from treatment for other forms of OCD. You identify the obsession, identify the compulsions, stop the compulsions, and starve the obsession. To achieve this, you attack the OCD from three angles:
Treatment for HOCD is no different from treatment for other forms of OCD. You identify the obsession, identify the compulsions, stop the compulsions, and starve the obsession. To achieve this, you attack the OCD from three angles:
- Exposure,
- Recognition of distorted thinking, and
- Mindfulness
ERP for HOCD
Exposure with Response Prevention (ERP) is a way of overcoming fears by gradually confronting things that cause the fear state while (and this is key) resisting the compulsive response. It’s not enough to look at weights at the gym. You have to pick them up and resist gravity’s objection.
Working with an OCD specialist, you will want to identify what it is about your HOCD that really compels you to ritualize. For some, it’s a straightforward discomfort with gay imagery (or imagery of another orientation than your own, recall my note above) and for that, you might do exposure to gay-themed pictures and videos of gradually increasing intensity while resisting the urge to convince yourself that you are straight. It’s extremely important that these exposures are done without any covert testing or analysis. In other words, looking at triggering pictures while reassuring yourself that you are not attracted to them is sending the signal to the brain that it should remain afraid of unwanted attractions instead of simply observe them.
It’s extremely important that these exposures are done without any covert testing or analysis. In other words, looking at triggering pictures while reassuring yourself that you are not attracted to them is sending the signal to the brain that it should remain afraid of unwanted attractions instead of simply observe them.
For others, the fear is more abstract, having less to do with unwanted sexual imagery and more to do with a loss of identity or a fear of emotionally scarring your loved ones by “coming out” to everyone’s dismay. For this, exposure to sexual material is less relevant because you may not be fighting a fear or disgust with gay sexual imagery, but instead are grappling with a fear of being an imposter. Exposures for this type of HOCD may focus more on being in environments where the thoughts are likely to be active and resisting checking or reassurance-seeking behaviors. You may also use imaginal exposure, such as writing narratives about your fears possibly coming true and the consequences therein. Many HOCD sufferers benefit from a combination of these two forms of exposure.
Many HOCD sufferers benefit from a combination of these two forms of exposure.
In both cases, it will also mean identifying what you are avoiding and gradually reintroducing yourself to those things. This doesn’t mean having you have to engage in unwanted sexual behaviors to overcome your fear. You presumably weren’t avoiding that before HOCD started. You just weren’t doing it. But you may have started to avoid other valued behaviors, such as reading a magazine if there happens to be an article about a gay celebrity in it, or listening to a piece of music performed by a gay person, or having conversations with someone you think may be gay. So, a lot of ERP is really about gradually returning to a life of behaviors totally unrelated to sexual orientation that got thrown off course by the HOCD.
Dealing with the HOCD Thoughts
Recognizing when a pattern of thought is leading you toward compulsive behavior and then challenging that way of thinking can be helpful. This may be addressed in therapy with something called cognitive restructuring, a way of identifying mistaken assumptions and responding to intrusive thoughts without doing compulsions. A good example of distorted thinking is the tendency in all forms of OCD to look at things in black-and-white terms. For example, equating the presence of one gay-themed thought with the self-identification of “being gay.”
A good example of distorted thinking is the tendency in all forms of OCD to look at things in black-and-white terms. For example, equating the presence of one gay-themed thought with the self-identification of “being gay.”
There is also a powerful tendency toward disqualifying the positive, in this case of a life history of being one orientation in the face of fear over being another. In other words, though you may have always pursued members of the opposite sex, your obsessive thoughts about being gay seem to make that seem irrelevant – or worse, like a desperate attempt to deny the truth! Another common distortion in HOCD is equating the presence of any gay thoughts or feelings with being less “you” (i.e. less masculine or feminine).
Though it is important to identify and challenge distorted thinking in all forms of OCD, you want to be very careful not to use logic as your main weapon against the disorder. You can’t fight OCD illogic for very long with logic. You have to fight it with better illogic in the form of exposure. In other words, by leaning in to your fears and getting better at embracing uncertainty, rather than trying to convince yourself your fears are untrue and reinforcing the idea that the content of your obsession is a threat.
In other words, by leaning in to your fears and getting better at embracing uncertainty, rather than trying to convince yourself your fears are untrue and reinforcing the idea that the content of your obsession is a threat.
Mindfulness Skills and HOCD
Accepting thoughts, feelings, and physical sensations as they are is all mindfulness really means. It is noticing and accepting without judgment. Hey, look at that, another thought. All right then. But in HOCD, accepting thoughts, feelings, and sensations may feel like accepting a death sentence. If I accept a thought like, “Maybe I would love kissing that guy” then what’s to stop me from making out with my best buddy? Well, nothing really, except that you are basically only going to do it if and when you both want to. You cannot control the thoughts and feelings and random physical sensations that happen to occur in you. No one can. You just choose what to do with them. Consider what are likely a number of highly disturbing thoughts you have that you simply disregard as irrelevant because they don’t relate to your obsessive theme.
Mindfulness for HOCD often means allowing yourself to incorporate unwanted sexual thoughts, feelings, and sensations into the larger picture of whatever you are experiencing in that moment. So, rather than attend to wishing that you could have a conversation with a same-sex friend without “gay thoughts,” actively embrace the experience of having both the conversation and the thoughts simultaneously. The experience you are having involves both of those things. When you focus your attention only on the unwanted thoughts, their origins, and when you imagine they will leave, then you are depriving yourself of the other experience, a nice conversation with a friend. If, on the other hand, you can allow yourself to stop “minding” that the thoughts are there and commit to having whatever experience you are having, you not only get to enjoy more of your life, but you send a powerful message to your OCD mind that these thoughts are not particularly important and not worthy of intruding so aggressively.
Working with Uncertainty in HOCD
In the end, because certainty does not truly exist, we only ever have two choices in life. One choice is to take the risk and stand up to your OCD. Get treatment from an OCD specialist, do the exposure with response prevention, practice mindfulness, and possibly spend the rest of your life happily engaged in whatever you pursue. It may end up well, it may not. You may live the life of one sexual orientation and right at the very end decide it was all a sham. That would be really disappointing I imagine.
But compare it to the alternative. The alternative is you don’t treat the OCD and you spend the rest of your life devoted to the futile pursuit of certainty, ruminating over the subject of sexual orientation all day every day, avoiding anything that might make you happy, because happy things trigger the unwanted thoughts. You isolate yourself from the people who care about you. You avoid sex and all sexual expression in an attempt to cleanse yourself of any possibility of an unwanted sexual thought or feeling. And then at the end of your life, you decide this was all a sham. You’re who you always assumed you were and you just have OCD. But you threw your life away for no reason other than the avoidance of fear. And now it’s too late to start over. Which scenario is ultimately more disappointing?
And then at the end of your life, you decide this was all a sham. You’re who you always assumed you were and you just have OCD. But you threw your life away for no reason other than the avoidance of fear. And now it’s too late to start over. Which scenario is ultimately more disappointing?
Navigating Unwanted Sexual Sensations in HOCD
Few subjects get more attention and cause more distress for the HOCD sufferer than the subject of the so-called “groinal response.” This is, of course, not a clinical term, so let’s start with a definition. A groinal response in the context of the OCD experience is:
- Any physical reaction in the genital area (movement, tingling, swelling, etc.) after exposure to an OCD trigger, whether real or imagined, pleasurable or discomforting
The disorder has a way of distorting how we interpret our experiences, making it sometimes difficult to tell, “Was that a groinal response from my OCD or was that a genuine sensation of arousal because I’m gay?” Mental checking and mental review are compulsions aimed at getting certainty about this distinction. Through repeatedly analyzing the experience, the focus of the HOCD evolves from “how do I know if I’m gay?” to the even more abstract “what kind of sensation was that and what does it mean?” This leads to even further confusion. A sensation is a sensation and whether we define it as wanted or unwanted is all about the narrative we have about this experience. Efforts to be certain whether it was “just a sensation” or “evidence of attraction” always fall flat because it contributes to a story about sensation instead of the experience itself. The same is true of thoughts. Though we notably identify obsessions as unwanted thoughts and distinguish them from other kinds of thoughts, the truth is that thoughts themselves are simply words or images appearing in the mind. It is the judgment and analysis that gets us into trouble with OCD.
Through repeatedly analyzing the experience, the focus of the HOCD evolves from “how do I know if I’m gay?” to the even more abstract “what kind of sensation was that and what does it mean?” This leads to even further confusion. A sensation is a sensation and whether we define it as wanted or unwanted is all about the narrative we have about this experience. Efforts to be certain whether it was “just a sensation” or “evidence of attraction” always fall flat because it contributes to a story about sensation instead of the experience itself. The same is true of thoughts. Though we notably identify obsessions as unwanted thoughts and distinguish them from other kinds of thoughts, the truth is that thoughts themselves are simply words or images appearing in the mind. It is the judgment and analysis that gets us into trouble with OCD.
Why do groinal responses happen?
Any sensation anywhere in the body is going to have a variety of potential sources, the most common of which are:
- No apparent reason, stuff happens.

- Chemical changes naturally occurring in the body, sometimes affected by stress or diet, in which blood flow is increased or decreased in different areas.
- Fear itself. Fear is expressed in the body by a number of symptoms, including increased heart rate, sweating, shortness of breath, and for many, changes in blood flow to the groin.
- Happiness. Like it or not, when we feel happy, our bodies become activated, which sometimes results in sensations in the groin. This can be particularly triggering for an HOCD sufferer feeling the love of a meaningful friendship or someone with pedophile obsessions (a.k.a. POCD) experiencing the joy of parenthood.
- The presence of all sexual thoughts, whether preferred or not, trigger groinal responses by their very nature of being sexual thoughts.
- Focused attention on specific body parts resulting in increased perceptual sensitivity and either an actual physical response or the perception of a physical response.

The phenomenon of groinal response in HOCD is easily re-created in other parts of the body. If I ask you to divert your attention to the pinky finger on your right hand, you will immediately trigger the firing of nerve endings in that area. Now, focus only on the knuckle of that finger… now on one crease in that knuckle. Whenever your attention shifts away naturally, try to bring it back to the crease in the knuckle of your right pinky finger. Now tell yourself it feels weird. Does it feel weird? Tingling? Itching? Something is setting it apart from the rest of your body. The attention causes the magnification of thoughts about sensations. This leads to the perception of sensation and sensations themselves. Furthermore, thoughts and feelings about these perceived and real sensations intensify the experience, creating a vicious cycle of thinking, sensing, fearing, thinking, and sensing some more.
The HOCD sufferer is very likely to have groinal responses around the same sex for the precise reason that they are checking and telling themselves not to. Just as trying NOT to think of a purple unicorn just made you think of a purple unicorn, trying NOT to experience sensation often generates sensation in this very sensitive part of the body. Conversely, trying to generate groinal responses to the preferred attraction will often fail to produce results. By trying to create the experience, you are generating a somewhat synthetic version of what you were hoping for. Instead of the spontaneous arousal you assume you should be having, you get your brain’s attempt at arousal. It’s much like trying to tickle yourself. Because you are aware that you are doing it, it only sort of feels like tickling and doesn’t make you laugh. In the end, obsessions are more than intrusive thoughts. They are intrusive experiences.
Just as trying NOT to think of a purple unicorn just made you think of a purple unicorn, trying NOT to experience sensation often generates sensation in this very sensitive part of the body. Conversely, trying to generate groinal responses to the preferred attraction will often fail to produce results. By trying to create the experience, you are generating a somewhat synthetic version of what you were hoping for. Instead of the spontaneous arousal you assume you should be having, you get your brain’s attempt at arousal. It’s much like trying to tickle yourself. Because you are aware that you are doing it, it only sort of feels like tickling and doesn’t make you laugh. In the end, obsessions are more than intrusive thoughts. They are intrusive experiences.
HOCD and Testing Compulsions
Testing is a form of reassurance seeking that involves initially exposing oneself to triggers and then analyzing the reaction to those triggers with the intention of getting certainty about the meaning of those reactions. This often comes disguised as exposure with response prevention (ERP) but is actually an OCD trap. Truly, it is exposure without response prevention and not OCD treatment. Many people have written to me describing having watched same-sex pornography to see if they had the “right” reaction to it. Many also describe compulsively looking at their historically preferred erotic pictures or videos and then analyzing whether they liked it enough or as much as the triggering material. This often involves checking the body for signs of sexual arousal and then analyzing the significance of the findings. Because the experiment is fundamentally flawed, the “evidence” of your reactions to the experiment is completely useless. Nonetheless, OCD takes the experiences from compulsive testing and uses them to strengthen your obsession. But “evidence” collected during the course of a compulsion is no more evidence than a confession derived by torture is a reliable source of the truth.
This often comes disguised as exposure with response prevention (ERP) but is actually an OCD trap. Truly, it is exposure without response prevention and not OCD treatment. Many people have written to me describing having watched same-sex pornography to see if they had the “right” reaction to it. Many also describe compulsively looking at their historically preferred erotic pictures or videos and then analyzing whether they liked it enough or as much as the triggering material. This often involves checking the body for signs of sexual arousal and then analyzing the significance of the findings. Because the experiment is fundamentally flawed, the “evidence” of your reactions to the experiment is completely useless. Nonetheless, OCD takes the experiences from compulsive testing and uses them to strengthen your obsession. But “evidence” collected during the course of a compulsion is no more evidence than a confession derived by torture is a reliable source of the truth.
HOCD and the Fear of Being in Denial
The word “denial” is at the root of all forms of OCD. It is popularized culturally to relate to issues of sexual orientation, but every person with any form of obsessive-compulsive disorder experiences the fear of “denial” whenever they choose to do exposure instead of rituals. The compulsive hand washer who chooses to allow themselves to touch a dollar bill and then eat a French fry is sitting with the terror that they may be in denial of the cold hard fact that a molecule of someone’s feces may have made its way from the dollar, to the fry, to their mouth. The Harm OCD sufferer, who lives in a war-torn mind of horrific images of violence against loved ones, holds a baby in their arms and tries to breathe evenly while covertly contemplating whether or not they are simply in denial of their closeted sociopathic “true” nature. Still, nowhere does this word “denial” get tossed around more than in the context of HOCD, the obsessive-compulsive fear of being or becoming a sexual orientation not your own. So, what is denial?
So, what is denial?
Denial is actively choosing to behave in a way that directly opposes your values or beliefs without acknowledging it.
Denial is not:
- Choosing to disregard thoughts, feelings, and sensations associated with another sexual orientation
- Pursuing relationships of meaning and value despite thoughts and feelings whose content seems incompatible with this pursuit
- Committing to relationships you are invested in despite the presence of doubtful thoughts about sexual orientation
- Accepting the presence (without guilt, disgust, or fear) of sexual fantasies outside of your historically preferred orientation
- Letting go of seeking reassurance about your orientation
- Accepting uncertainty regarding your sexual orientation and the label that goes with it
HOCD Meets ROCD
One common concern among HOCD sufferers is that if they choose to accept uncertainty and stop doing rituals, they may discover that they are gay and that discovery will result in a revelation to their partner that they have been lying about their orientation. The obsession is therefore not only about sexual orientation, but about the authenticity and safety of the sufferer’s relationship with another person (as in Relationship OCD/ROCD). The fear thrives on an image of a tearful husband or wife feeling deceived, tricked, led on a long and ultimately meaningless journey to middle age alone, the victim of a fraud perpetrated by the a fool who couldn’t come to terms with their orientation. In other words, “I can’t just be with this person I love if there is any doubt as to the meaning of these gay thoughts, so I must get certainty to protect my loved one from a future betrayal.” To the contrary, cognitive behavioral treatment for HOCD when there is a significant other involved must include exposure to the idea of denial and the way in which it could destroy the other person. So, in addition to imaginal scripting exposures in which the sufferer could write out the feared consequences of persisting in gay denial in a relationship, the sufferer might also do exposures to strengthening their relationship.
The obsession is therefore not only about sexual orientation, but about the authenticity and safety of the sufferer’s relationship with another person (as in Relationship OCD/ROCD). The fear thrives on an image of a tearful husband or wife feeling deceived, tricked, led on a long and ultimately meaningless journey to middle age alone, the victim of a fraud perpetrated by the a fool who couldn’t come to terms with their orientation. In other words, “I can’t just be with this person I love if there is any doubt as to the meaning of these gay thoughts, so I must get certainty to protect my loved one from a future betrayal.” To the contrary, cognitive behavioral treatment for HOCD when there is a significant other involved must include exposure to the idea of denial and the way in which it could destroy the other person. So, in addition to imaginal scripting exposures in which the sufferer could write out the feared consequences of persisting in gay denial in a relationship, the sufferer might also do exposures to strengthening their relationship. By investing more fully and more completely in their love for their significant other, they are getting both exposure to the fear of destroying a loved one and, as an interesting side effect, a better, more meaningful relationship. In short, invest in your relationships in such a way that if they fail, it will be the most devastating. That is romance.
By investing more fully and more completely in their love for their significant other, they are getting both exposure to the fear of destroying a loved one and, as an interesting side effect, a better, more meaningful relationship. In short, invest in your relationships in such a way that if they fail, it will be the most devastating. That is romance.
Typical exposures for HOCD fears may involve looking at triggering materials, listening to triggering music, and being around triggering people (all without doing compulsions of course!). But for the specific fear of being denial, life itself is the trigger and exposure means committing to that life. This may mean following through on your plan to propose to your partner, letting yourself really be moved by a love story of a different orientation than your own, or allowing a thought to be enjoyable if it’s enjoyable even if it doesn’t fit your identity in that moment. Consider this – we may define denial as running from the truth. If this is the case, then it is far worse to be in denial of your OCD (and not committing seriously to treating it with CBT) than it is to be in denial of whatever your OCD is talking about. While the consequences of your fears coming true are quite unknowable, to deny yourself OCD treatment has clear and predictable consequences.
While the consequences of your fears coming true are quite unknowable, to deny yourself OCD treatment has clear and predictable consequences.
Impact therapy for HOCD? (2012)
Intrusive worries about someone coming out as gay even though he (he) has been straight for years without any doubt - got the HOCD label, homosexual obsessive-compulsive disorder , More properly such worries will be called obsessive-compulsive disorder of sexual orientation because they also affect gay people who suddenly wonder if they are straight.
Therapists who treat HOCD, such as Steve Seay PhD, often recommend the standard treatment for OCD: Exposure Prevention and Response. "Exposure" refers to voluntarily entering situations that may cause compulsions, and "response prevention" refers to the purposeful suppression of coping rituals. For example: resisting the urge to wash hands compulsively in certain situations.
However, the scientific reason that exposure therapy often helps some forms of OCD is the reason that this can backfire in the case of pornography associated with HOCD.
Some experts conceive of OCD as an exchange of important elements of behavioral addiction due to the role that reward plays, the OCD sufferer continues to perform their special rituals because they evoke reward-related neurochemical responses. The relief feels good.
When an OCD sufferer consistently withholds neurochemical rewards (“response avoidance”), their triggers gradually lose their power. Why? They no longer feel good. Do not wash your hands. No relief. No reward. Eventually the brain says, "Mm... there's no point in being activated by that fetal doorknob because I won't get the neurochemical reward."
The same principle applies to getting rid of addiction. Refrain from "rewarding" behavior long enough and (after a period of intense withdrawal discomfort) the brain will eventually stop activating the appropriate brain circuits with the same vindictiveness. It becomes easier as the whole set of addiction-related brain changes reverses.
Two types of HOCD
In short, the difference between HOCD and porn-related HOCD is:
- OCD + homosexual fears (or event) = HOCD
- Years of porn use + distress about escalating to gay/transsexual porn = porn-related HOCD
Random life events, such as unthinkable peer comments at vulnerable moments, can cause some people to start questioning their sexual orientation compulsively (HOCD).
However, the new stimulus for HOCD today is chronic overstimulation, which makes the brain less receptive to everyday pleasures and thus desperate for sensation. Passionate pornography makes chronic overspending easy. Compared to the erotica of the past, it is so stimulating that in some users it produces addiction-related brain changes. Not surprising. Quite apart from the non-stop sexual tickling, internet porn today activates the brain's reward system for all evolutionarily important stimuli, increasing memory formation (wiring):
- Strong emotions such as surprise, fear, disgust, anxiety,
- New,
- Search and search
- Anything that violates expectations, Including danger.
Moreover, it is possible that those who develop HOCD may, for some reason, have particularly plastic brains. According to a Chinese study, those with OCD tendencies prior to exposure to the Internet face an increased risk of addiction.
Either way, the brain of a porn addict can grow numb to normal pleasure even as it becomes hyper-reactive to select cues. Here's a guy describing the overall progress often reported by those who slip into porn-related HOCD:
Here's a guy describing the overall progress often reported by those who slip into porn-related HOCD:
29 y / o with 17 years of MO (in imagination and erotica) and 12 years of masturbation, building up to extreme / fetish porn. I started to lose interest in real sex. The accumulation and release from porn has become stronger than from sex. Porn offers unlimited variety. I could choose what I want to see at the moment. My delayed ejaculation during sex got so bad that sometimes I couldn't reach orgasm at all. It killed my last desire to have sex.
Classical sexual training
Once this degree of sensitization has been established internally, the scene for porn related to HOCD. Inconsistent porn breaks expectations, releases more dopamine and norepinephrine than earlier porn genres, and delivers an extra kick that fires up the lethargic (addict) reward circuitry. The user might start asking why he might go into fetish shemale porn/gay action until he is attracted to real sex partners who have called him out in the past.
His brain, however, automatically begins to transmit its sexual response to this genre-stimulating novel - in a classic case of sexual conditioning. As explained in an early post, Sexuality can be sustained by most anything, even the smell of death, so it's not surprising that many of today's porn users report that their porn tastes are transforming everywhere as their pleasure resonates.
Our user can now find that he can only is the culmination of his latest (and therefore most stimulating) genre. If it's one he finds incompatible with his primary sexual orientation, the shock value will be greater... and release even more anxiety-inducing neurochemicals. His arousal is partly heightened by his own stress. Three guys describe their experience:
First guy: I seriously thought I was going gay. At the time, my HOCD was so strong that I was about to dive off the nearest high-rise building. I was so depressed. I knew I loved girls and couldn't love another guy, but why do I have ED? Why did I need shemales/gays to wake me up?
Second guy: The scary thing is that I thought women were insanely attractive and men or the idea of men was pretty unsexual.
It's pretty weird for a gay guy who's only had relationships with other men since high school. Even when I see "ugly" ladies walking down the street, I can't help but imagine what it's like to have crazy sex with them right there. Will it stop? Is it reversible?
Third guy: For the first two days I had severe anxiety, I almost wanted to kill myself because I had lost all attraction to any woman. These thoughts make me think I'm gay, make me think about what I do, what I say, causing nausea. I can't eat. I think about intrusive thoughts... making me feel like I'm gay when I know I'm not.
The frustration of users trying to figure out if their sexual orientation has suddenly changed can lead to constant compulsive "tests" and other calming rituals. As with other varieties of OCD (including the non-porn-related HOCD), testing and seeking reinsurance offer temporary relief. Each "test" increases unwanted arousal - either grateful relief or electrified stress if the test fails. In this way, they reinforce problem triggers. .
In this way, they reinforce problem triggers. .
What should a therapist do?
Be aware that behavioral addictions and reward. We know from addiction theory that addiction heals gradually as these rewards no longer come from withdrawal. Slowly the brain weakens the connected pathways.
The therapist is best able to help correctly estimate the reward for a particular client's HOCD . If his motivating reward is primarily the relief from "testing" or from repeatedly declaring that his orientation has changed (to gain temporary confidence relief), then exposing and avoiding a reaction (no more anxiety-motivated tests or claims) may help. .
In the case of porn-related HOCD, however, the benefits of addiction may contain the lion's share of the client's task. There may well be two addictive rewards in the mix: fear and sexual arousal.
Fear as a reward
Distress may not seem helpful fear activates the brain's reward circuitry in some people. Think commercials and horror films. In a brain desperate for sensation (due to chronic overstimulation/addiction-induced brain changes), fear-induced activation can register as especially compelling. It raises dopamine and norepinephrine (a form of adrenaline).
Think commercials and horror films. In a brain desperate for sensation (due to chronic overstimulation/addiction-induced brain changes), fear-induced activation can register as especially compelling. It raises dopamine and norepinephrine (a form of adrenaline).
But something more is going on at the biological level. The stress neurochemical cortisol can also enhance positive effects by triggering the release of dopamine. After all, brain changes can make someone more sensitive to stressful cues. Research confirms that extreme stress and drug abuse and both increase the strength of related (addiction) brain pathways. Researchers believe that cortisol plays a key role in patronage-related behavioral pathologies.
The situation is similar to BDSM, where physical pain increases a person's sexual arousal due to the effect on the brain. In people with HOCD, agitation and panic achieve a similar goal. Bottom line: Despite intense emotional or physical discomfort, increased arousal can make the behavior very difficult to stop (addictive).
The brain of a person suffering from HOCD has learned to get some of its reward from its own suffering. To make matters worse, when the sufferer tries to give up porn, his anxiety will naturally increase over a long period of time. Withdrawal causes anxiety at all recovering addicts stoking powerful cravings for more stimulation, completely unrelated to HOCD problems.
For people suffering from HOCD, this predictable increase in anxiety tends to cause intense spikes (orientation panic) and frantic "checks" that often return them to addiction. Indeed, some report that their concerns about HOCD were trite. until they quit porn . As the addicted brain targets the strongest "fix" it can think of: panic + check + sexual arousal for HOCD-related stimuli, direct feelings seem to evaporate.
Sexual arousal as a reward
Addiction to Internet porn is an addiction to orgasm-help. Sexual arousal is the most powerful natural reward the brain can produce. However, the arousal from the constant novelty of Porn (every scene offers another excitatory neurochemical hit) can produce surprisingly powerful rewards. Sex, or even orgasm, can fade in intensity as porn addiction progresses and response to everyday pleasures decline. Some users end up hooked on the neurochemical buzz from edging to new porn for hours, deliberately delaying, or avoiding, climax.
However, the arousal from the constant novelty of Porn (every scene offers another excitatory neurochemical hit) can produce surprisingly powerful rewards. Sex, or even orgasm, can fade in intensity as porn addiction progresses and response to everyday pleasures decline. Some users end up hooked on the neurochemical buzz from edging to new porn for hours, deliberately delaying, or avoiding, climax.
The brain has evolved to assume that the source of intense sexual arousal is the potential for fertilization. If someone awakens themselves with something that releases a maximum of dopamine and norepinephrine, the brain automatically plugs it in as "valuable." It doesn't matter if this is consistent with his innate sexuality, because the brain measures significance according to reward circuit activation levels and not orientation. (It just so happens that in a brain that responds normally to pleasure, stimuli that match orientations tend to produce the most satisfying feelings. )
)
Not surprisingly, the sensitized brain pathways for intense sexual cues differ from less stimulating cues (even sexual ones). We can release the latter with relative ease, but not the former. This has been demonstrated in studies, as shown in James G. Pfaus et al:
Lalumière and Quinsey (1998) reported significant conditioned genital arousal in heterosexual men to the picture of a moderately attractive, partially naked woman who was in combined with a video depicting a highly arousing sexual interaction, the control group that accessed the image alone (no video) showed addiction [instead]. (highlighted by me)
As explained above, for porn-related HOCD sufferers, sexual signals are particularly intense because they are amplified by the neurochemical effects of fear.
Backlash Exposure Therapy When Porn Addiction Is Present
For an internet porn addict using standard HOCD therapy, real gay exposure does not consider the source of his HOCD conditioning, which is not for human or sex with humans, but rather pixels. However, if he tries exposure therapy with gay porn, he engages in the exact behavior he is addicted to. You can't make an addict get used to it by giving the very signals he's hooked on!
However, if he tries exposure therapy with gay porn, he engages in the exact behavior he is addicted to. You can't make an addict get used to it by giving the very signals he's hooked on!
So exposure therapy could very well be all wrong for guys trying to unravel porn-related HOCD. It's like drinking more alcohol based on the theory that she'll get tired of drinking, or that the player bets more until they get used to it. For an addict, constant use only deepens the rut of addiction in the brain. Thus, exposure therapy may deliver an unproductive mixed message to the HOCD porn addict instead of promoting a beneficial condition (addiction).
So where do you start? Porn addicts need to eliminate the use of Internet porn first and foremost. As their brains return to balance, many also notice that confusing sexual cues lose their power.
If porn addicts with HOCD try to use associated cues for therapeutic purposes rather than abstinence from them they reinforce their behavioral addictive neural pathways. This is Catch 22. An addict (and perhaps his therapist) may mistakenly conclude that his persistent and powerful response to problem cues is not HOCD, but rather "proof" that his sexual orientation has mysteriously changed.
This is Catch 22. An addict (and perhaps his therapist) may mistakenly conclude that his persistent and powerful response to problem cues is not HOCD, but rather "proof" that his sexual orientation has mysteriously changed.
The point is that addiction is an obstacle to standard therapy to prevent and respond to OCD exposure. Even if the addict stops looking for a reward in help (Based on testing or analysis), exposure to porn still “rewards” him by activating his sensitized addiction.
What does
do to help ?We are not therapists. However, we have read self-reports from a number of former Internet porn users who describe themselves as suffering/recovering from HOCD (sample self-report). We will summarize their experience if it turns out to be useful.
Guys report that withholding internet porn rewards and temporarily withholding rewards for sexual activity (other than relaxed, affectionate sex with a partner) helps resolve their HOCD. As they stop amplifying their simple reward (porn use), their brains gradually look around, and wire, other sexual rewards. This may take months. In light of these guys' experiences, doctors may want to invite clients to disconnect from Internet porn for several months before introducing therapy exposure (if ever).
As they stop amplifying their simple reward (porn use), their brains gradually look around, and wire, other sexual rewards. This may take months. In light of these guys' experiences, doctors may want to invite clients to disconnect from Internet porn for several months before introducing therapy exposure (if ever).
At first, the guys may not respond normally to partners, although relaxed attachment is calming (perhaps because it releases oxytocin). Plus, until the worst of the addiction is overcome, they also often experience more excruciating HOCD spikes.
Those who are recovering report that if they can accept HOCD obsessive thoughts without stress, they will bypass the neurochemical amplification of fear. In addition, they find it useful to learn to live with their insecurities about their sexual orientation and to avoid any trials and attempts to "find out the truth." Thus, they also stop rewarding fleeting relief and "confidence".
In other words, the HOCD patient must work on stop stop three rewarding habits: Internet porn use, relief shelter and distress.
One person's self-esteem
This person's report is interesting in that he started easing off the porn rewards, only to find that he wasn't dealing with the fear and relief (check) rewards.
I am currently over 3 months without porn, but I went into a daze of constantly checking various HOCD message boards. I spent hours on these sites every day, sometimes checking them several times an hour: at work, driving, in bed at night, and so on. and so on. My brain was rewarded when I read something that calmed me, and it became nervous when I read something that increased my anxiety.
I also extended my check to other message boards, including gay and bisexual boards. It just perpetuated the spiral. I didn't get much sleep because of all my anxiety and I wasn't really in my life. I was either on those boards or worried about what I was reading on them. Constantly. My relationship suffered. Sometimes, alone at night, I spent 2-3 hours checking HOCD on message boards on the Internet, and then I felt terrible.

I decided to stop. My friend deserves someone to be present and not be completely distracted. Since then, I've only had one 15 minute answer check session. I had to struggle to resist the temptation, but as a result, I feel SO much better.
This is really wonderful. My HOCD has decreased significantly now that I am not constantly signaling to my brain, "THIS HOCD THOUGHTS ARE IMPORTANT" by climbing the boards and doing checks and reassurances. I haven't read either book for several months, but now I'm moving on to the second one because I've given up on boards. I spend my free time at night either with a girl or reading by the fire. I sleep much better.
Yes, I still get spikes when I see an attractive guy. And then from checking thoughts about him. But there should be much fewer of them, and this thought disappears much faster.
Now I think my HOCD may have been due to the fact that when I finally overdosed on PMO after years and years I lost much of my attraction to real women.
Without it, women and men began to look the same to me and BAM worries about gay outburst.
Schwarz's non-exposure therapeutic approach
There is an existing therapeutic system for OCD that does not support exposure. It was developed by psychiatrist Jeffrey Schwartz. (Read description taken from Doidge The Brain That Changes Itself.)
Schwartz teaches his patients how neuroplasticity works so they understand that their compulsion is due to an unwanted, overactive brain loop (not unlike addiction). He then explains that the wiring of the brain can be changed by conscious effort.
In a sense, this is the exact opposite of exposure therapy. Instead of trying to get used to it through exposure, a person tries to rewire the brain by shifting gears at the moment when the appropriate signal appears. Schwartz suggests switching to a pre-selected constructive activity.
The goal is not to avoid discomfort in search of relief, but rather to activate unrelated brain pathways instead of problematic ones so that the brain disconnects from its former "rewards" and perhaps even begins to associate anxiety with a productive task.
As an aside, HOCD expert Fred Penzel also discourages the impact of therapy for porn addicts, even though he recommends exposure and response prevention therapy in classic cases of HOCD.
Hopefully researchers will soon determine which protocols are best for those with COPD. Many of those affected are desperately trying to resolve their anxiety. Indeed, of all the recovering sex addicts who visit our site, the HOCD guys are suffering the worst and relapsing the lightest.
Nowadays, many are hesitant to seek help for fear that sane therapists will say they are gay (or straight) when they know they are not.
Porn-related HOCD sufferers usually have no idea how to rewire because standard therapy doesn't work and the most promising solutions feel so illogical (they have to go away from relief, from analysis and from sexual arousal on time). Most of them will not be able to figure it out without informed professional help. To make progress, they may need to find a therapist who is well versed in addiction issues and the role of abstinence in freeing the brain of unwanted rewards.
Empirical support for this article:
- Signs of addiction and escalation to more extreme material? Over 30 study results consistent with escalating porn use (tolerance), addiction to pornography, and even withdrawal symptoms reporting
- Porn / sex addiction? This page lists 39 neurology-based studies (MRI, fMRI, EEG, neuropsychological, hormonal). They provide strong support for the addiction model because their results reflect the neurological data found in addiction research.
- Real expert opinions on porn/sex addiction? This list contains 16 recent literature reviews and comments by some of the world's leading neuroscientists. All support the dependency model.
COMMENTS ABOUT ARTICLE
Clear addiction first, then seek therapy if necessary
I came to this site and YBOP was looking for answers about a year ago. PMO has been a daily ritual for many years, 13 years I would say. I, like May you on this forum, have become de-sensitized to normal porn genres.
Searching for new or shocking material became the norm if I didn't know it on a conscious level. I never had a great sex life with women in real life, suffered from moderate ED, went to urologists for answers, got little blue pills, etc. Confidence in the bedroom was a problem. I am always trying to conjure up an image in my head of a porn scene to come out having real sex. Then came the problem with HOCD.
The difference in my story is that I never dared in the gay and transgender world, but I will say that my sexual tastes have changed, I needed weirder and more shocking thoughts in order to have an orgasm. When I was on vacation, HOID came into it. While I was masturbating, normal thoughts didn't work, and then a strange, semi-gay thought came into my head and I had this weak orgasm. I'm not sure if the shock of it all was the culprit, but I can tell it scared me. I never thought about sexual satisfaction and at the time I was 33.
I spent my entire holiday analyzing all my reactions to people, men and women.
I am obsessed with what my senses felt, and tested and tested and tested. I'm obsessed with whether or not I've become a homosexual, and the fact that my experiences with women have been mixed fueled HOCD at best. This obsession continued for two years until I sought professional help.
To backtrack a bit, I found YBOP a few months after all my HOCD-related Google searches and "how to know if you're straight" sites. The YBOP material made sense to me and was very interesting. Many people on the forums have claimed that their HOCD was cured without PMO. I have, of course, tried. By the way, I have been and still am in a relationship, so during this time I would have had sex, but not PMO. I found out that my ED was gone. Sex was no longer a mental image formation in my mind, but a shared action with the person in front of me. However, HOCD has not disappeared for me. The interrogation was as bad as ever.
Here I want to talk about my treatment because it has to do with traditional HOCD versus porn related HOCD.
I will leave it to you to judge for yourself based on my personal reports. I found a therapist who is an expert on OCD, in fact some of his articles are featured on YBOP. He ventured into reaction prevention and exposure therapy with me. For those of you who don't know, this therapy involves gradually exposing the patient to what they are afraid of, from things that make you a little afraid to things that really scare you. The idea is that if you want to think less about something, think more about it. Resisting negative thoughts causes them to return to your consciousness. As you agree with and open up to thoughts, you become desensitized to them. It's the equivalent of watching a scary movie for the first time. At first you are shocked, but if you see it 10 more times, it will not be so scary. We started by making a list of things that might bother me and rating them on a scale of one to ten, with ten being the scariest. We started by reading stories that came out, reading stuff that might be considered gay, listening to tapes that said I might be gay.
As therapy went on, I had to come to terms with the idea that I might be gay. It was an extremely intimidating proposal. Eventually the material moved to my number 10, but by the time I reached that level, I was better prepared. BTW- my number 10 watched gay porn because he was afraid that I might feel something. However, I was never allowed to "test" my reactions. I had to just "be" with the shocking material, allow myself to worry until I realized it wasn't going to work. The more I did the lessons, the less I was influenced by the material. In the end, I could say: "Yes, I could be gay, but who cares." You see, in the end, it was the questions and the need to find a definite answer that drove me crazy. Am I really gay? I don't think so, but I don't dwell on it anymore. I don't check anymore. I still have intrusive thoughts from time to time, but I agree with them and it quickly changes my focus. It no longer affects me the way it used to, although questions may randomly pop into my head.
Over time, the questions really subside.
In general, I agree that quitting porn is key before starting any therapy of this kind. Porn got me into this mess, but therapy got me out of it. I don't know if this therapy will work if you are a user who has traveled the world of gay porn or transgender porn. I would say to go first and see where you stand with HOCD in a few months. What I also learned from my therapist is that there are a lot of gay men who watch straight porn and think they can be straight, so this problem can go both ways. I will say that my journey is individual, but this therapy has been life changing for me. If you find help, go to the OCD specialist who handled it, not the general consultant. Be prepared, if they know what they are doing, they won't tell you to judge your orientation, but will help you stop pushing your questions. I hope this can influence my story and help you come back to life. Thank you.
https://www.reuniting.info/content/one-year-later-porn-and-hocd
I have OCD and read the book Brain Block and I learned
Deep Inside brain lies a structure called the caudate nucleus.
Scientists around the world have studied this structure and believe that, in people with OCD, the caudal nucleus may not work properly . Think of the caudal nucleus as a processing center or filtering station for very complex messages generated by the front of the brain, which is likely , is the part used in thinking, planning and understanding. Together with its sister structure, the putamen located next to it, the caudate nucleus functions like an automatic transmission in a car. The caudate nucleus and the putamen, which are collectively called the striatum, receive messages from very complex parts of the brain - those that control body movement, physical senses, thinking and planning that are associated with these movements and feelings. They function in unison like an automatic transmission, providing a smooth transition from one behavior to another.
From the book: http://www.worldcat.org/isbn/9780060987114
I then thought about how the caudate nucleus affects porn, and I found
Structural volume of the brain
They found that more hours porn viewing was correlated with a decrease in gray matter in an area of the brain called the right caudate nucleus .
This association remained after the elimination of the second correlation with internet addiction and sex addiction. An association has also been found between high porn consumption over the years and less gray matter in this area of the brain. The researchers took this as a sign of the effects of long-term exposure to porn.
Source: http://www.ncbi.nlm.nih.gov/pubmedhealth/behindtheheadlines/news/2014-05-30-watching-porn-associated-with-male-brain-shrinkage/
So, refraining from porn may help people with OCD.
PS: Knowing the connection between them makes me feel like a scientist. 😛
http://www.reddit.com/r/NoFap/comments/2jritu/link_between_ocd_and_porn_…
I wanted to add some nuance to this discussion. Effective therapy has proven to be very effective in people with NSOD. These are people who meet the criterion for having obsessions, which are obsessive thoughts associated with a major disorder that the person is trying to neutralize.
This does not include a person who is actually gay and is simply uncomfortable with their sexual orientation. An example of a person with OCD is a person who has a fear that thinking about other naked men will cause them to become gay. This is similar to other typical OCD obsessions such as thinking about hurting someone will actually result in the person losing control and killing someone. In HOCD, viewing nude same-sex images may only be part of the treatment, with the main intervention usually developing comfort with mental imagery until habituation occurs.
Antipsychotic therapy with atypical antipsychotics | Yastrebov
Recommended design of the bibliographic reference:
Yastrebov D.V. Antipsychotic therapy using atypical antipsychotics // Russian Psychiatric Journal. 2013. No. 1. pp. 71-82.
annotation
A review article discusses aspects of antipsychotic therapy using the atypical antipsychotic drug risperidone and discusses its administration and patient management.
Literature
1. Avrutsky G.Ya., Neduva A.A. Treatment of the mentally ill. - M.: Medicine, 1988. - 528 p. 2. Mosolov S.N. Fundamentals of psychopharmacotherapy. - M.: Vostok, 1996. - 288 p. 3. Yastrebov D.V. Therapy of obsessive and anxiety disorders in patients with non-psychotic forms of schizophrenia // Psychiatry and psychopharmacology. - 2011. - V. 13, No. 4. - S. 38-47. 4. Yastrebov D.V. Monotherapy with risperidone (ridonex) for obsessive and anxiety disorders in patients with schizophrenia. ter. psycho. disorders. - 2012. - No. 1. - S. 22-30. 5. Alevizos B., Lykouras L., Zervas I.M. et al. Risperidone-induced obsessive-compulsive symptoms: a series of six cases // J. Clin. Psychopharmacol. - 2002. - Vol. 22. - P. 461-467. 6. Baker R.W., Ames D., Umbricht D.S. et al. Obsessive-compulsive symptoms in schizophrenia: a comparison of olanzapine and placebo // Psychopharmacol. Bull. - 1996. - Vol. 32. - P. 8 9 - 9 3 . 7. Cutler J., Siris S.G. "Panic-like" symptomatology in schizophrenic and schizoaffective patients with postpsychotic depression: observations and implications // Compr. Psychiatry. - 1991. - Vol. 32. - P. 465-473. 8. Cutler J. Panic attacks and schizophrenia: assessment and treatment // Psych. Ann. - 1994. - Vol. 24. - P. 473-476. 9. Essock S.M., Covell N.H., Davis S.M. et al. Effectiveness of switching antipsychotic medications // Am. J. Psychiatry. - 2006. - Vol. 163 (12). - P. 2090-2095. 10. Farde L., Nordstrom A.L., Wiesel F. A. et al. Positron emission tomographic analysis of central D1 and D2 dopamine receptor occupancy in patients treated with classical neuroleptics and clozapine: relation to extrapyramidal side effects // Arch. Gen. Psychiatry. - 1992. - Vol. 49. - P. 538-544. 11. Gaebel W., Riesbeck M., Wolwer W. et al. Relapse prevention in first-episode schizophrenia - maintenance vs intermittent drug treatment with prodrome-based early intervention: results of a randomized controlled trial within the German Research Network on Schizophrenia // J.
Clin. Psychiatry. - 2011. - Vol. 72(2). - P. 205-218. 12. Ganguli R. Rationale and strategies for switching antipsychotics // Am. J. Health Syst. Pharm. - 2002. - Vol. 59. - P. S22-S26. 13. Gautam D., Han S.J., Hamdan F.F. et al. A critical role for beta cell M3 muscarinic acetylcholine receptors in regulating insulin release and blood glucose homeostasis in vivo // Cell Metab. - 2006. - Vol. 3(6). - P. 449-461. 14. Ghaemi S.N., Zarate C.A., Popli A.P. et al. Is there a relationship between clozapine and obsessive compulsive disorder? A retrospective chart review // Compr. Psychiatry. - 1995. - Vol. 36. - P. 267-270. 15. de Greef R., Maloney A., Olsson-Gislekog P. et al. Dopamine D2 Occupancy as a Biomarker for Antipsychotics: Quantifying the Relationship with Efficacy and Extrapyramidal Symptoms // AAPS J. - 2011. - Vol. 13, No. 1. - P. 121-130. 16. de Haan L., Beuk N., Hoogenboom B. et al. Obsessivecompulsive symptoms during treatment with olanzapine and risperidone: a prospective study of 113 patients with recent-onset schizophrenia or related disorders // J.
Clin. Psychiatry. - 2002. - Vol. 63. - P. 104-107. 17. de Haan L., Linszen D. H., Gorsira R. Clozapine and obsessions in patients with recent-onset schizophrenia and other psychotic disorders // J. Clin. Psychiatry. - 1999. - Vol. 60.-P. 364. 18. Haase H.J., Janssen P.A.J. The Action of Neuroleptic Drugs. - Chicago, IL: Year Book Medical, 1965. 19. Hiemke C., Weigmann H., Hartter S. et al. Elevated levels of clozapine in serum after addition of fluvoxamine // J. Clin. Psychopharmacol. - 1994. - Vol. 14. - P. 279-281. 20. Hwang M.Y., Opler L.A. Schizophrenia with obsessive-compulsive features: assessment and treatment // Psych. Ann. - 1994. - Vol. 24. - P. 468-472. 21. Insel T.R., Akiskal H.S. OCD with psychotic features: a phenomenologic analysis // Am. J. Psychiatry. - 1986.-Vol. 143. - P. 15 2 7-15 3 3 . 22. Kane J., Honigfeld G., Singer J. et al. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine // Arch. Gen. Psychiatry. - 1988. - Vol.
45. - P. 789-796. 23. Kapur S., Zipursky R.B., Remington G. et al. 5-HT2 and D2 receptor occupancy of olanzapine in schizophrenia: a PET investigation // Am. J. Psychiatry. - 1998. - Vol. 155. - P. 921-928. 24. Khullar A., Chue P., Tibbo P. Quetiapine and obsessive-compulsive symptoms (OCS): case report and review of atypical antipsychotic-induced OCS // J. Psychiatry Neurosci. - 2001. - Vol. 26.-P. 55-59. 25. Kinon B.J., Basson B.R., Gilmore J.A. et al. Strategies for switching from conventional antipsychotic drugs or risperidone to olanzapine // J. Clin. Psychiatry. - 2000. - Vol. 61. - P. 8 3 3 - 8 4 0 . 26. Mahendran R. Obsessive-compulsive symptoms with risperidone // J. Clin. Psychiatry. - 1999. - Vol. 60. - P. 261-263. 27. Margetis B. Aggravation of schizophrenia by clomipramine in a patient with comorbid obsessive-compulsive disorder // Psychopharmacol. Bull. - 2008. - Vol. 41. - P. 9-11. 28. Masand P.S. A review of pharmacological strategies for switching to atypical antipsychotics.
Prim Care Companion // J. Clin. Psychiatry. - 2005. - Vol. 7.-P. 121-129. 29. McEvoy J.P., Lieberman J.A., Perkins D.O. et al. Efficacy and tolerability of olanzapine, quetiapine, and risperidone in the treatment of early psychosis: a randomized, double-blind 52week comparison // Am. J. Psychiatry. - 2007. - Vol. 164(7). - P. 10 5 0 -10 6 0 . 30. Oransky I. Paul Janssen // Lancet. - 2004. - Vol. 363. - P. 251. 31. Poyurovsky M., Weizman A. Intravenous clomipramine for a schizophrenic patient with obsessive-compulsive symptoms // Am. J. Psychiatry. - 1998. - Vol. 155. - P. 1993. 32. Poyurovsky M. Obsessive-compulsive symptoms in schizophrenia: clinical characterization and treatment // Clinical Obsessive-Compulsive Disorders in Adults and Children / Eds R. Hudak, D.D. Dougherty. - Cambridge Univ. Press, 2011. - P. 7 1-9 1. 33. Reznik I., Sirota P. Obsessive and compulsive symptoms in schizophrenia: a randomized controlled trial with fluvoxamine and neuroleptics // J. Clin. Psychopharmacol.