Mmpi 2 items
Minnesota Multiphasic Personality Inventory-2 (MMPI-2) | Occupational Medicine
Navbar Search Filter Occupational MedicineThis issueOccupational MedicineBooksJournalsOxford Academic Mobile Microsite Search Term
Close
Navbar Search Filter Occupational MedicineThis issueOccupational MedicineBooksJournalsOxford Academic Microsite Search Term
Advanced Search
Journal Article
Mike Drayton
Mike Drayton
Search for other works by this author on:
Oxford Academic
PubMed
Google Scholar
Occupational Medicine
, Volume 59, Issue 2, March 2009, Pages 135–136, https://doi. org/10.1093/occmed/kqn182
Published:
01 March 2009
- Split View
-
- Article contents
- Figures & tables
- Video
- Audio
- Supplementary Data
-
Cite
Cite
Mike Drayton, The Minnesota Multiphasic Personality Inventory-2 (MMPI-2), Occupational Medicine, Volume 59, Issue 2, March 2009, Pages 135–136, https://doi.
 org/10.1093/occmed/kqn182
org/10.1093/occmed/kqn182Select Format Select format.ris (Mendeley, Papers, Zotero).enw (EndNote).bibtex (BibTex).txt (Medlars, RefWorks)
Close
-
Permissions
-
- More
Navbar Search Filter Occupational MedicineThis issueOccupational MedicineBooksJournalsOxford Academic Mobile Microsite Search Term
Close
Navbar Search Filter Occupational MedicineThis issueOccupational MedicineBooksJournalsOxford Academic Microsite Search Term
Advanced Search
A brief history
The original Minnesota Multiphasic Personality Inventory (MMPI) was published in 1940 and the second revised version—the MMPI-2—was published in 1989. It is the most widely used psychometric test for measuring adult psychopathology in the world. The MMPI-2 is used in mental health, medical and employment settings.
It is the most widely used psychometric test for measuring adult psychopathology in the world. The MMPI-2 is used in mental health, medical and employment settings.
Description
The test developers Hathaway and McKinley used an empirical test construction technique to develop the MMPI. This involved basing the test scales (for example the hypochondriasis scale) on the actual test items that differentiate people with hypochondriasis from ‘normals’. Often, the questions that do this most reliably are not concerned with health issues as such. This has two advantages. First, it makes it very difficult for subjects to ‘fake’ responses, deny problems or give a particular impression. Second, the MMPI-2 is based on empirical research and not on a clinician's assumptions about what answers indicate particular personality traits.
The data from MMPI-2 assessments are particularly useful in occupational health settings in complex presentations where doubt as to what is really wrong with the patient exists.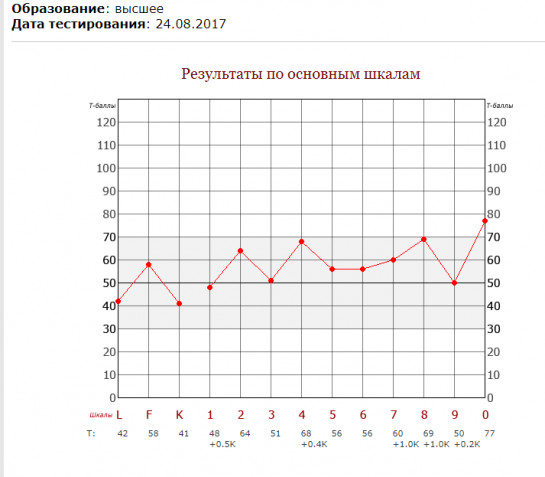 For example, the MMPI-2 should normally be able to detect unconsciously somatizing or consciously malingering in patients [1]. The MMPI-2 can also be used to assess psychological stability in workers in ‘high-risk’ professions such as airline pilots, police or workers in the nuclear power industry [2–4].
For example, the MMPI-2 should normally be able to detect unconsciously somatizing or consciously malingering in patients [1]. The MMPI-2 can also be used to assess psychological stability in workers in ‘high-risk’ professions such as airline pilots, police or workers in the nuclear power industry [2–4].
One of the disadvantages of the MMPI-2 for the occupational health physician is that the MMPI-2 is a strictly licensed test and can only be purchased, administered and interpreted by a suitably experienced clinical psychologist or psychiatrist. As such, it should be regarded as a complex diagnostic investigation for relatively infrequent use.
It takes most people between 1 h and 90 min to complete the MMPI-2.
Items
The MMPI-2 is a 567 item, true/false self-report measure of a person's psychological state. It has nine validity scales (or ‘lie’ scales), assessing for lying, defensiveness, faking good and faking bad and among others [5]. These scales make it very difficult to fake the MMPI-2 results. The measure has many clinical scales assessing mental health problems (i.e. depression, anxiety, post-traumatic stress disorder), personality characteristics (i.e. psychopathy) and general personality traits such as anger, somatization, hypochondriasis, ‘type A behaviour’ addiction potential, poor ego strength and many others.
These scales make it very difficult to fake the MMPI-2 results. The measure has many clinical scales assessing mental health problems (i.e. depression, anxiety, post-traumatic stress disorder), personality characteristics (i.e. psychopathy) and general personality traits such as anger, somatization, hypochondriasis, ‘type A behaviour’ addiction potential, poor ego strength and many others.
Validity
The MMPI-2 was validated using a normative sample of 2600 adults. There are ∼10 000 published papers using the MMPI-2 and this pool is added to by hundreds of papers every year. A symptom validity scale (FBS) has been added to the inventory in recent years to help exclude symptom exaggeration and has been reported as having very low false-positive rates.
Key research
Nordin et al. [6] applied the MMPI-2 to 307 female and 161 male patients with chronic pain. They found a strong relationship between reported pain disorder and conversion disorder (experiencing psychological and emotional problems as physical pain).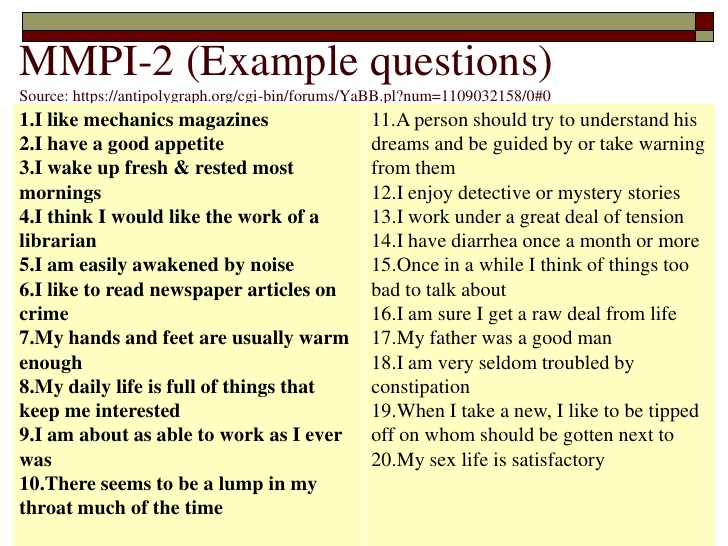 This is an extremely useful finding for occupational health physicians because it shows the utility of the MMPI-2 for determining whether a patient complaining of chronic pain would best benefit from medical treatment or psychological therapy.
This is an extremely useful finding for occupational health physicians because it shows the utility of the MMPI-2 for determining whether a patient complaining of chronic pain would best benefit from medical treatment or psychological therapy.
The MMPI-2 can be obtained from www.pearsonassessments.com/tests/mmpi_2.htm.
References
1.
Schretlen
DJ
.
The use of psychological tests to identify malingered symptoms of mental disorder
,
Clin Psychol Rev
,
1988
, vol.
8
(pg.
451
-
476
)
2.
Beutler
LE
.
Parameters in the prediction of police officer performance
,
Prof Psychol Res Pr
,
1985
, vol.
16
(pg.
324
-
335
)
3.
Butcher
JN
.
Psychological assessment of airline pilot applicants with the MMPI-2
,
J Pers Assess
,
1994
, vol.
62
(pg.
31
-
44
)
4.
Sellbom
M
,
Fischler
GL
,
Ben-Porath
YS
.
Identifying MMPI-2 predictors of police officer integrity and misconduct
,
Crim Justice Behav
,
2007
, vol.
34
(pg.
985
-
1004
)
5.
Butcher
JN
,
Dahlstrom
WG
,
Graham
JR
,
Tellegen
AM
,
Kreammer
B
. ,
The Minnesota Multiphasic Personality Inventory-2 (MMPI-2) Manual for Administration and Scoring
,
1989
Minneapolis, MN
University of Minneapolis Press
6.
Nordin
H
,
Eisemann
M
,
Richter
J
.
MMPI-2 subgroups in a sample of chronic pain patients
,
Scand J Psychol
,
2005
, vol.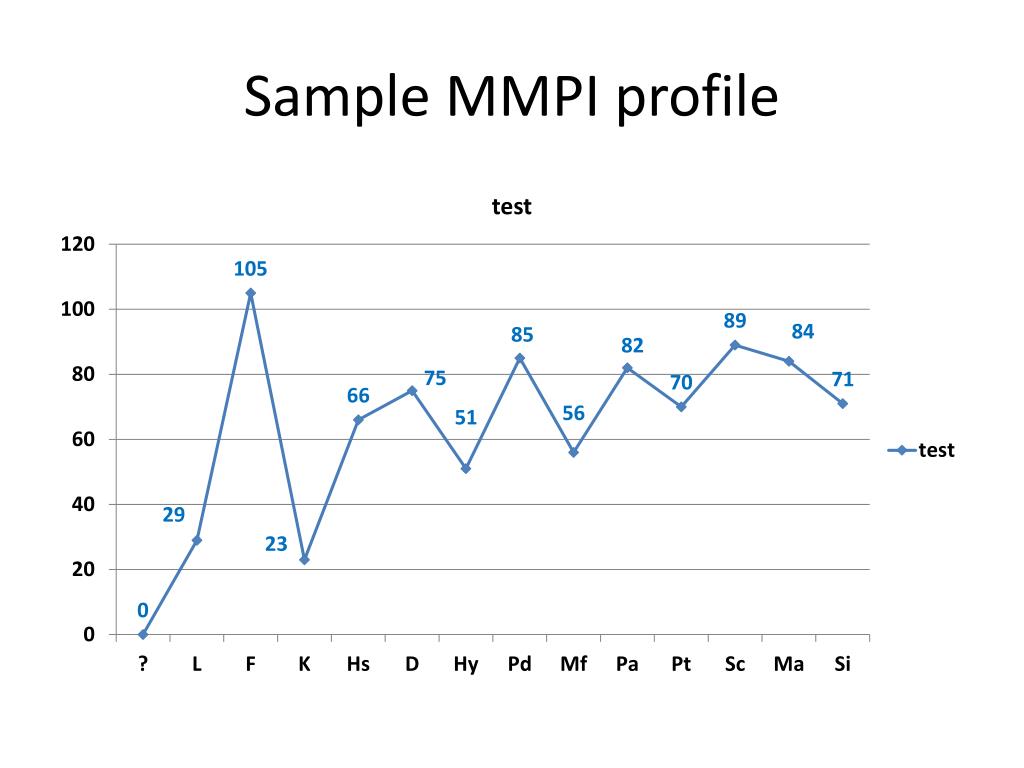
46
(pg.
209
-
216
)
© The Author 2009. Published by Oxford University Press on behalf of the Society of Occupational Medicine. All rights reserved. For Permissions, please email: [email protected]
© The Author 2009. Published by Oxford University Press on behalf of the Society of Occupational Medicine. All rights reserved. For Permissions, please email: [email protected]
Issue Section:
The Minnesota Multiphasic Personality Inventory-2 (MMPI-2)
Download all slides
Advertisement
Citations
Views
204,511
Altmetric
More metrics information
Email alerts
Article activity alert
Advance article alerts
New issue alert
Subject alert
Receive exclusive offers and updates from Oxford Academic
Citing articles via
-
Latest
-
Most Read
-
Most Cited
Cryoglobulins and cold agglutinins for hand arm vibration syndrome
Flour exposure, sensitization and respiratory health among Alberta trainee bakers
Climate change effects on mental health: are there workplace implications?
Acquired vibratory angioedema with a severe impact on work performance
Improved perception of work following a stress management intervention
Advertisement
MMPI-2 Scales — University of Minnesota Press
The 567-item MMPI-2 is composed of over 120 scales.
Validity Indicators
Superlative Self-Presentation Subscales
Clinical Scales
Restructured Clinical (RC) Scales
Content Scales
Content Component Scales
Supplementary Scales
Clinical Subscales (Harris-Lingoes and Social Introversion Subscales)
VALIDITY INDICATORS
?(CNS) - Cannot Say (reported as a raw score)
VRIN - Variable Response Inconsistency
TRIN - True Response Inconsistency
F - Infrequency
FB - Back F
FP - Infrequency – Psychopathology
FBS - Symptom Validity
L - Lie
K - Correction
S - Superlative Self-Presentation
SUPERLATIVE SELF-PRESENTATION SUBSCALES
S1 - Beliefs in Human goodness
S2 - Serenity
S3 - Contentment with Life
S4 - Patience / Denial of Irritability
S5 - Denial of Moral Flaws
CLINICAL SCALES
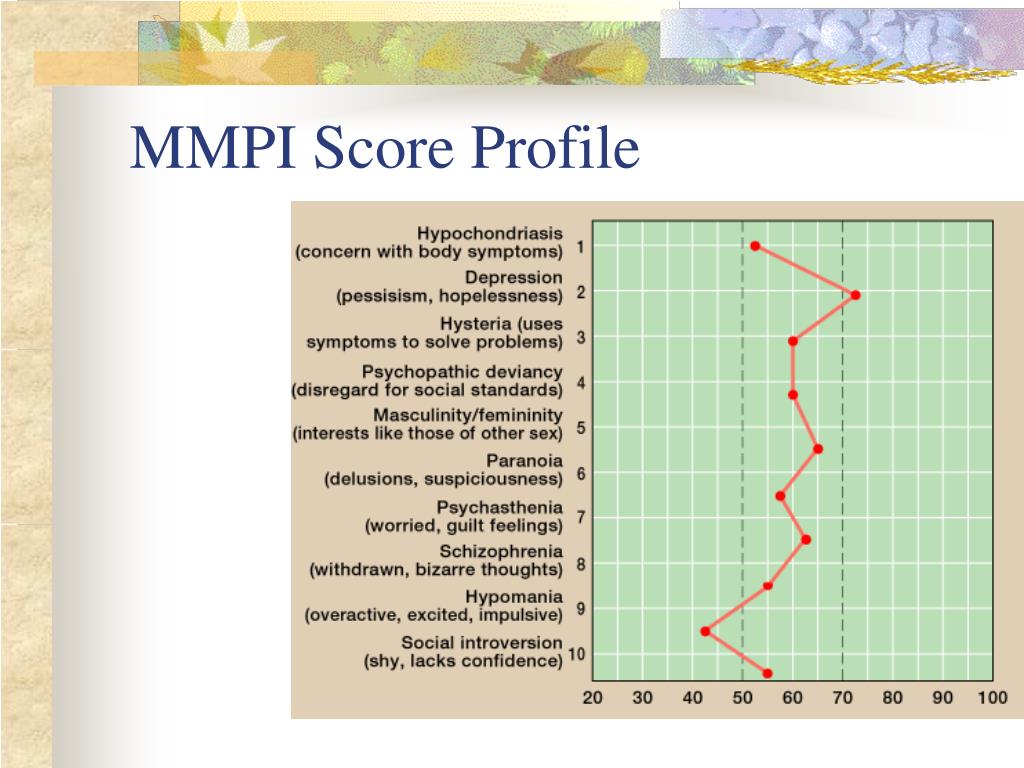
1 Hs - Hypochondriasis
2 D - Depression
3 Hy - Hysteria
4 Pd - Psychopathic Deviate
5 Mf - Masculinity/Femininity
6 Pa - Paranoia
7 Pt - Psychasthenia
8 Sc - Schizophrenia
9 Ma- Hypomania
0 Si - Social Introversion
RCd (dem) - Demoralization
RC1 (som) - Somatic Complaints
RC2 (lpe) - Low Positive Emotions
RC3 (cyn) - Cynicism
RC4 (asb) - Antisocial Behavior
RC6 (per) - Ideas of Persecution
RC7 (dne) - Dysfunctional Negative Emotions
RC8 (abx) - Aberrant Experiences
RC9 (hpm) - Hypomanic Activation
CLINICAL SUBSCALES
Harris-Lingoes Subscales
D1 - Subjective Depression
D2 - Psychomotor Retardation
D3 - Physical Malfunctioning
D4 - Mental Dullness
D5 - Brooding
Hy1 - Denial of Social Anxiety
Hy2 - Need for Affection
Hy3 - Lassitude-Malaise
Hy4 - Somatic Complaints
Hy5 - Inhibition of Aggression
Pd1 - Familial Discord
Pd2 - Authority Problems
Pd3 - Social Imperturbability
Pd4 - Social Alienation
Pd5 - Self-Alienation
Pa1 - Persecutory Ideas
Pa2 - Poignancy
Pa3 - Naïveté
Sc1 - Social Alienation
Sc2 - Emotional Alienation
Sc3 - Lack of Ego Mastery-Cognitive
Sc4 - Lack of Ego Mastery-Conative
Sc5 - Lack of Ego Mastery-Defective Inhibition
Sc6 - Bizarre Sensory Experiences
Ma1- Amorality
Ma2- Psychomotor Acceleration
Ma3- Imperturbability
Ma4- Ego Inflation
Social Introversion Subscales
Si1 - Shyness / Self-Consciousness
Si2 - Social Avoidance
Si3 - Alienation - Self and Others
CONTENT SCALES
ANX - Anxiety
FRS - Fears
OBS - Obsessiveness
DEP - Depression
HEA - Health Concerns
BIZ - Bizarre Mentation
ANG - Anger
CYN - Cynicism
ASP - Antisocial Practices
TPA - Type A
LSE - Low Self-Esteem
SOD - Social Discomfort
FAM - Family Problems
WRK - Work Interference
TRT - Negative Treatment Indicators
CONTENT COMPONENT SCALES
FRS1 - Generalized Fearfulness
FRS2 - Multiple Fears
DEP1 - Lack of Drive
DEP2 - Dysphoria
DEP3 - Self-Depreciation
DEP4 - Suicidal Ideation
HEA1 - Gastrointestinal Symptoms
HEA2 - Neurological Symptoms
HEA3 - General Health Concerns
BIZ1 - Psychotic Symptomatology
BIZ2 - Schizotypal Characteristics
ANG1 -Explosive Behavior
ANG2 -Irritability
CYN1 -Misanthropic Beliefs
CYN2 -Interpersonal Suspiciousness
ASP1 - Antisocial Attitudes
ASP2 - Antisocial Behavior
TPA1 - Impatience
TPA2 - Competitive Drive
LSE1 - Self-Doubt
LSE2 - Submissiveness
SOD1 -Introversion
SOD2 -Shyness
FAM1 - Family Discord
FAM2 - Familial Alienation
TRT1 - Low Motivation
TRT2 - Inability to Disclose
SUPPLEMENTARY SCALES
PSY-5 (Personality Psychopathology Five)
AGGR -Aggressiveness
PSYC -Psychoticism
DISC - Disconstraint
NEGE -Negative Emotionality / Neuroticism
INTR - Introversion / Low Positive Emotionality
Broad Personality Characteristics
A - Anxiety
R - Repression
Es - Ego Strength
Do -Dominance
Re -Social Responsibility
Generalized Emotional Distress
Mt - College Maladjustment
PK - Post-Traumatic Stress Disorder – Keane
MDS - Marital Distress
Behavioral Dyscontrol
Ho - Hostility
O-H - Overcontrolled Hostility
MAC-R - MacAndrew-Revised
AAS - Addiction Admission
APS - Addiction Potential
Gender Role
GM - Gender Role – Masculine
GF - Gender Role – Feminine
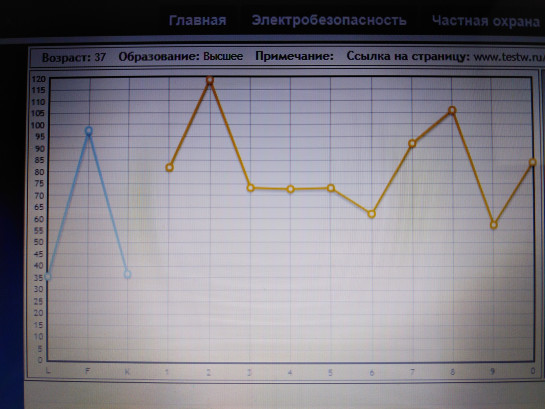
Standardized multifactorial method for the study of personality SMIL (modified MMPI test) Interpretation
 As a leading peak in the profile, which does not go beyond the norm, n reveals the predominance of a passive personal position. The leading motivational orientation is the avoidance of failure. For persons of this type, the following features are characteristic: a high level of awareness of existing problems through the prism of dissatisfaction and a pessimistic assessment of their prospects; propensity to think, inertia in decision-making, pronounced depth of feelings, analytical mindset, skepticism, self-criticism, some lack of self-confidence, one's abilities . Personalities whose profiles are accentuated on the 2nd scale are capable of refusing to realize momentary needs for the sake of distant plans. In order to avoid conflict with the social environment egocentric tendencies are inhibited.
As a leading peak in the profile, which does not go beyond the norm, n reveals the predominance of a passive personal position. The leading motivational orientation is the avoidance of failure. For persons of this type, the following features are characteristic: a high level of awareness of existing problems through the prism of dissatisfaction and a pessimistic assessment of their prospects; propensity to think, inertia in decision-making, pronounced depth of feelings, analytical mindset, skepticism, self-criticism, some lack of self-confidence, one's abilities . Personalities whose profiles are accentuated on the 2nd scale are capable of refusing to realize momentary needs for the sake of distant plans. In order to avoid conflict with the social environment egocentric tendencies are inhibited.  the need for understanding, love, self-benevolence is one of the leading, in fact, never satiated and at the same time primarily frustrated need, which largely determines the zone of psycho-traumatic impact.
the need for understanding, love, self-benevolence is one of the leading, in fact, never satiated and at the same time primarily frustrated need, which largely determines the zone of psycho-traumatic impact.  High scores on the 2nd scale may be associated with a situation of sharp disappointment after an experienced failure or in connection with a disease that disrupts the normal course of life and long-term plans of a person. Such a profile outlines a certain state, at least a depressive reaction within the framework of the adaptation syndrome. However, this is only a quantitative aspect, revealing the features of not only a psychogenically provoked state, but also providing for the predisposition of a given individual to such reactions in a stressful situation. Depressive state is the most common anthropotypical (i.e. inherent in man and humanity) reaction to distress. Nevertheless, with a pronounced sthenic (or hypersthenic) type of response, even in a situation of severe stress, such as, for example, a judicial-investigative situation with a very pessimistic perspective, we noted the absence of depression as such. On the contrary, the anxious expectation of the outcome of the situation and social deprivation evoked protest reactions in individuals of the hyperthymic type with exaltation, bravado, and active self-affirmation.
High scores on the 2nd scale may be associated with a situation of sharp disappointment after an experienced failure or in connection with a disease that disrupts the normal course of life and long-term plans of a person. Such a profile outlines a certain state, at least a depressive reaction within the framework of the adaptation syndrome. However, this is only a quantitative aspect, revealing the features of not only a psychogenically provoked state, but also providing for the predisposition of a given individual to such reactions in a stressful situation. Depressive state is the most common anthropotypical (i.e. inherent in man and humanity) reaction to distress. Nevertheless, with a pronounced sthenic (or hypersthenic) type of response, even in a situation of severe stress, such as, for example, a judicial-investigative situation with a very pessimistic perspective, we noted the absence of depression as such. On the contrary, the anxious expectation of the outcome of the situation and social deprivation evoked protest reactions in individuals of the hyperthymic type with exaltation, bravado, and active self-affirmation.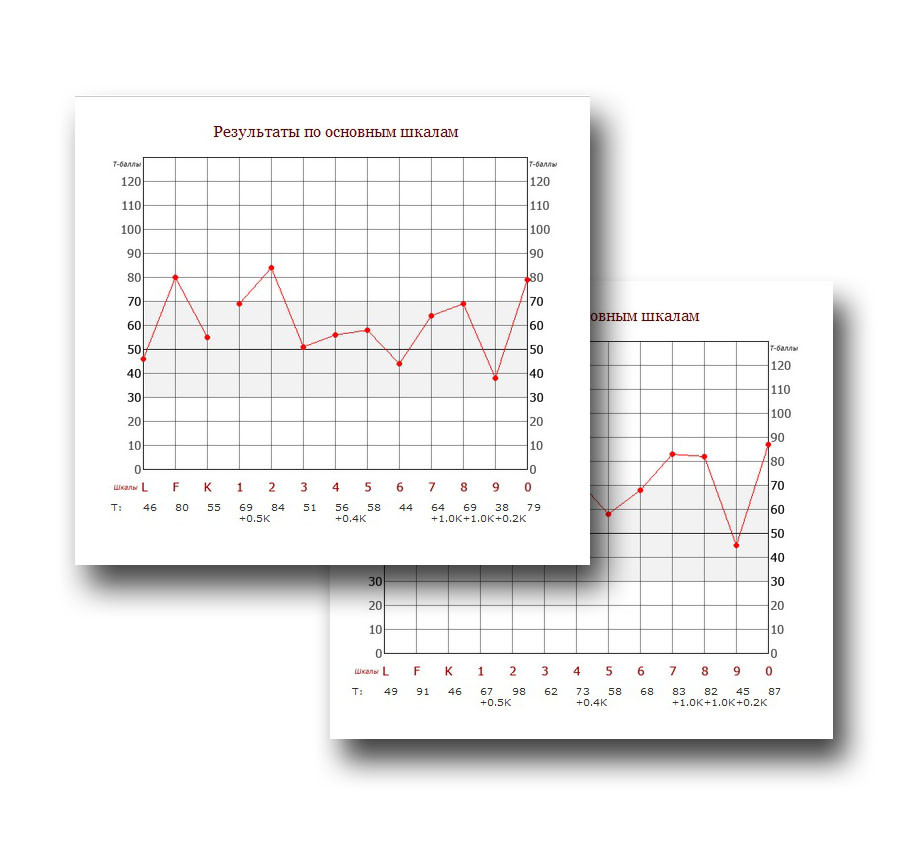
Experience shows that the depressive type of reaction is by no means a universal and strictly obligatory reaction to psychotrauma and develops only on the basis of a certain predisposition. Therefore, the rise of the profile on the 2nd scale above 70 T reveals in the subject not only a low mood due to negative experiences, but also personality traits - a tendency to acutely experience failures, to worries, to an increased sense of guilt with a self-critical attitude to their shortcomings, with self-doubt.
These features are exacerbated in the 270′-/9 type profile, characteristic of persons with inhibited type accentuation , with anxious and suspicious features. In the eternal conflict between egocentric and altruistic tendencies, representatives of this group of people prefer the latter. Refusal of self-realization eliminates the confrontation of these contradictory tendencies and reduces the risk of conflict with the environment. If an increase on the 1st scale means an unconscious, repressed refusal of self-actualization, then an increase on the 2nd one reveals conscious self-control, when unfulfilled intentions - due to external circumstances or internal reasons - are reflected in a lowered mood as a result of a deficit or loss. At the same time, people in this circle can be quite active, following the leader as the most conformal and socially compliant group. A moderate increase in the 2nd scale with the onset of adulthood is seen as natural “acquired skepticism”, a wiser attitude towards life problems, as opposed to the carelessness and optimism of youth, manifested by relatively lower scores on the 2nd and high scores on 9th (the “optimism” scale).
At the same time, people in this circle can be quite active, following the leader as the most conformal and socially compliant group. A moderate increase in the 2nd scale with the onset of adulthood is seen as natural “acquired skepticism”, a wiser attitude towards life problems, as opposed to the carelessness and optimism of youth, manifested by relatively lower scores on the 2nd and high scores on 9th (the “optimism” scale).
A simultaneous increase in the 2nd and 9th scales reflects a tendency to mood swings, cyclothymic personality variant or cyclothymia. Profile type 24′-/9 should be alarming in terms of increased suicidal risk (S-risk) , since in addition to the characteristics of the 2nd scale, a decrease in the level of vitality and optimism (determined by the 9th scale) and increased impulsivity (4th scale) are added scale).
Persons with a moderate rise on the 2nd scale as the dominant peak are fertile ground for both individual and group psychotherapy.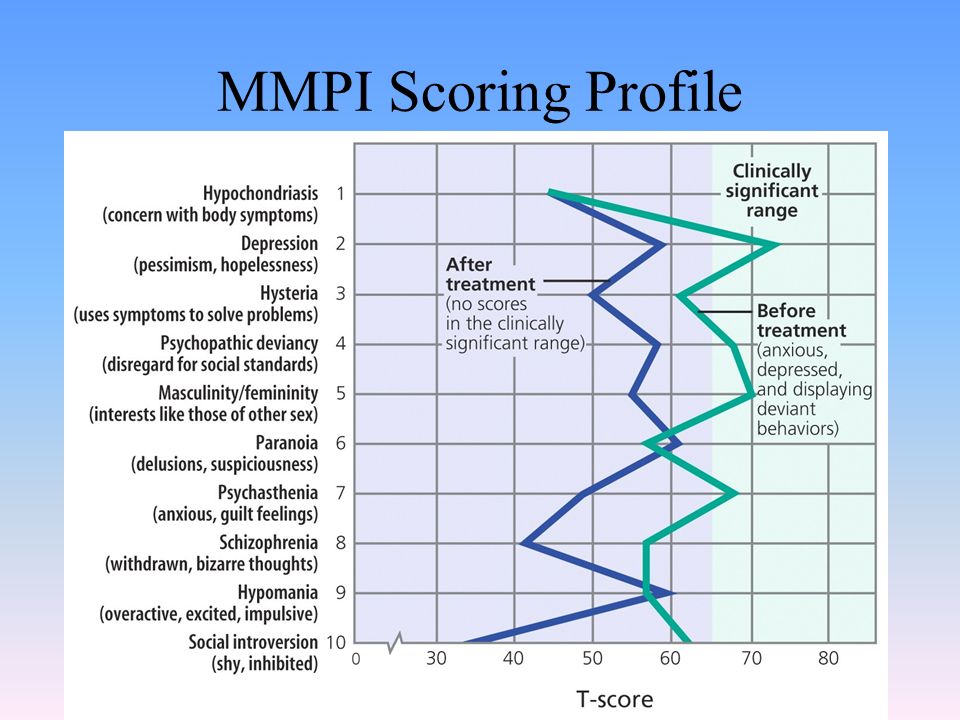
Of all the typological variants, persons with the 2nd scale predominant in the SM IL profile are distinguished by the greatest vulnerability in relation to life's adversities, the desire to comprehend and “slow down” their own immediate impulses, to avoid confrontation with the cruel laws of real life in connection with a pessimistic assessment their capabilities while countering the wall installations of others. The pattern (structure, drawing) of this personality is such that the fate-fulfilling tendency bears the imprint of a certain passivity, and circumstances may be overwhelming the character. Apparently, therefore, this type is characterized by fatalism, i.e. the tendency to rely on how everything “accompanies itself”, “where the curve will take you”, and “how lucky”, rather than trying to influence fate yourself. These are the passion-bearers: without realizing it, they revel in the role of the victim, meekly carrying his cross. (It is necessary to distinguish type “2” from senile passivity acquired over the years).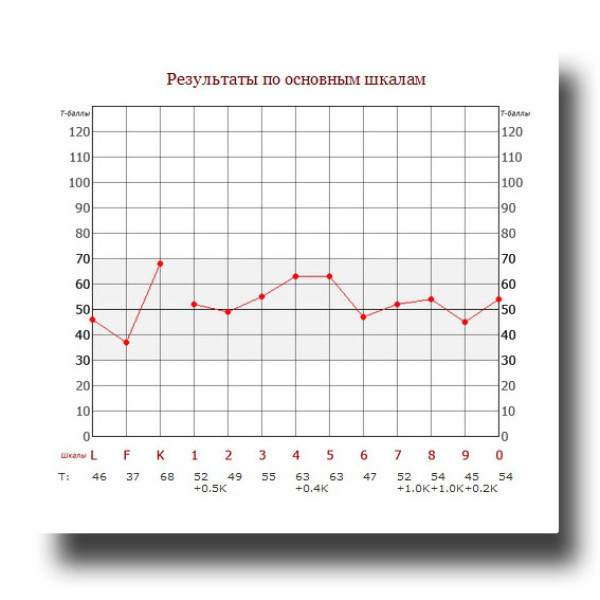 By refusing to realize momentary egoistic needs, type “2” individuals hope thereby to solve distant problems and form a base of spiritual values . Unrealized needs are sublimated and manifested by general humanistic tendencies. Personal aspects of life are determined by their desire to save the family; marry and get married, focusing on the similarity of characters or agreeing to a dependent position; show a pronounced responsibility for children, painfully react to separation from loved ones. Among personalities of this type, there are more monogamous people. In the presence of a social niche corresponding to personal inclinations, they successfully realize their abilities, while showing emphasized responsibility. Even in a criminal environment, they can only fulfill the most honest and leading roles (treasurer or “watchdog”). It is said of such people that they “have the fear of God in their souls”; they are more likely than others to be capable of altruistic manifestations.
By refusing to realize momentary egoistic needs, type “2” individuals hope thereby to solve distant problems and form a base of spiritual values . Unrealized needs are sublimated and manifested by general humanistic tendencies. Personal aspects of life are determined by their desire to save the family; marry and get married, focusing on the similarity of characters or agreeing to a dependent position; show a pronounced responsibility for children, painfully react to separation from loved ones. Among personalities of this type, there are more monogamous people. In the presence of a social niche corresponding to personal inclinations, they successfully realize their abilities, while showing emphasized responsibility. Even in a criminal environment, they can only fulfill the most honest and leading roles (treasurer or “watchdog”). It is said of such people that they “have the fear of God in their souls”; they are more likely than others to be capable of altruistic manifestations.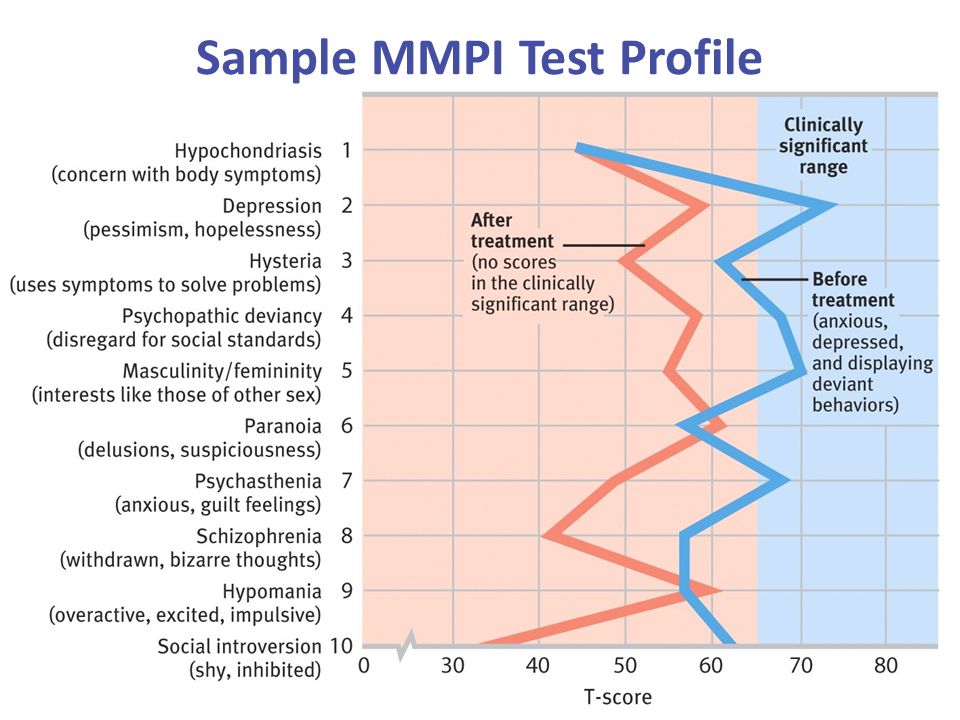 This does not mean that they do not have selfish aspirations, but the fear of inconsistency with their own idea of the ideal “I” and low stress resistance form a pronounced “Super-Ego”. However, this is only the shell of a snail hiding in its shell. If at the same time a low level of modest intellectual abilities is noted, then the personality is hardly noticeable. However, even such people have “their own genre in the soul”, it is only hidden from prying eyes. If these are people with high intelligence, then, not exchanging vainly for everyday trifles, they gravitate towards serious generalizations. The social role of such personalities is the formation of humane ideas and liberal tendencies in the quiet of offices, which is then used by wall pragmatists to achieve power. Among them are those philosophers who are either approached or punished by those in power, depending on whether these ideas are beneficial to them or dangerous. They do not enter into power of their own free will, but the halo of holiness flatters them.
This does not mean that they do not have selfish aspirations, but the fear of inconsistency with their own idea of the ideal “I” and low stress resistance form a pronounced “Super-Ego”. However, this is only the shell of a snail hiding in its shell. If at the same time a low level of modest intellectual abilities is noted, then the personality is hardly noticeable. However, even such people have “their own genre in the soul”, it is only hidden from prying eyes. If these are people with high intelligence, then, not exchanging vainly for everyday trifles, they gravitate towards serious generalizations. The social role of such personalities is the formation of humane ideas and liberal tendencies in the quiet of offices, which is then used by wall pragmatists to achieve power. Among them are those philosophers who are either approached or punished by those in power, depending on whether these ideas are beneficial to them or dangerous. They do not enter into power of their own free will, but the halo of holiness flatters them.
L. N. Sobchik
Correction scale K of the MMPI technique, SMIL, MMIL
Correction scale K MMPI was developed. (Meehl and Hathaway, 1946) to detect more subtle defensive responses than the L lie scale allows. The K scale reveals “false positive” aspects of responses to test statements, taking into account various aspects of psychological defense. When interpreting the MMPI, the k scale serves both as an indicator of the invalidity of the profile and as a means of correcting the results of responses on clinical scales, taking into account the defensive reaction.
In other words, the height of the K scale measures personality characteristics, not a pure profile validity construct. An increase in K-scores (especially with T-scores above 70) reflects a pronounced defensive position during testing. These may be subjects who seek to present a very favorable opinion of themselves, for example, those who are trying to prove that they do not need psychological help, or simply deny the problems that they have, which leads to an increase in K-scores. The level of the scale also correlates with other variables such as social class and education level. People from higher social classes may get higher K scores (between 55 and 60 T-points). Therefore, for groups of subjects with a high socioeconomic status, the conclusion about the presence of a protective reaction should not be made with indicators on the K scale that do not exceed 70 T-points. Other personality factors such as self-acceptance, independence, self-respect, and non-authoritarian values are also associated with modest increases in K scores.
The level of the scale also correlates with other variables such as social class and education level. People from higher social classes may get higher K scores (between 55 and 60 T-points). Therefore, for groups of subjects with a high socioeconomic status, the conclusion about the presence of a protective reaction should not be made with indicators on the K scale that do not exceed 70 T-points. Other personality factors such as self-acceptance, independence, self-respect, and non-authoritarian values are also associated with modest increases in K scores.
A pronounced defensive stance (K over 70 T-scores) in situations that require frankness and openness, such as in the context of treatment planning, may reflect the following characteristics: aloofness, rigidity, unwillingness to cooperate with the therapist, denial of problems, and the presence of unrealistic self-esteem.
Table 1 . Interpretation of K scores by socioeconomic status when planning an intervention
K T-score range: low social class
30-44 some problems, acceptance and expression of symptoms, problem-oriented response
45-55 expected normal level of K for a given socioeconomic class position
64-69 moderately pronounced defensive position, unwillingness to discuss feelings, denial as a psychological defense
70+ Pronounced defensive position, frank distortion of self-presentation, attempt to manipulate others, with extreme denial of existing symptoms.
K T-score range: middle to high social class
30-44 excessive complaining, exaggeration of symptoms, lack of defensive constructs, attempt to get attention through expression of symptoms
45-55 some recognition of symptoms, apparent willingness to discuss problems
56-63 expected normal score range for this socioeconomic class without any problems
64-69 somewhat reluctant to discuss personal problems
70+ defensive attitude, evasiveness, unwillingness to express one's feelings, symptoms, with some denial of symptoms.
High values over 65 T-scores (70 T-scores for MMPI, SMIL)
High K-scores are associated with defensiveness, emotional contraction, and reduction of symptoms. As a result, the therapist will have to evaluate what clients are saying, adjusting upwards for all symptoms and complaints (Caldwell, 2008). High scores on the K scale can occur for a number of reasons. Clients who are deliberately defensive in order to "pass" the test. However, in other cases, a high score on the K scale is a reflection of the higher socioeconomic status of the subjects. People from more affluent backgrounds tend to maintain a cultural value of excessive self-control, adherence to high social standards, and socially appropriate behavior. In some cultures, such as the British, public expression of emotions is frowned upon and viewed as inappropriate (Wagstaff & Rowledge, 1995). The ability to keep a face and a “hard upper lip” in stressful situations with the suppression of violent emotional reactions is considered appropriate and desirable. In such individuals, high K-scores reflect a cultural bias towards control and balance (Reynolds & Fletcher-Janzen, 2002). In some situations, high K scores may be better understood as reflecting personality variables rather than defensiveness. People who score high on the Correction scale are more likely to be balanced, have good emotional control, and are able to handle stressful situations well.
Clients who are deliberately defensive in order to "pass" the test. However, in other cases, a high score on the K scale is a reflection of the higher socioeconomic status of the subjects. People from more affluent backgrounds tend to maintain a cultural value of excessive self-control, adherence to high social standards, and socially appropriate behavior. In some cultures, such as the British, public expression of emotions is frowned upon and viewed as inappropriate (Wagstaff & Rowledge, 1995). The ability to keep a face and a “hard upper lip” in stressful situations with the suppression of violent emotional reactions is considered appropriate and desirable. In such individuals, high K-scores reflect a cultural bias towards control and balance (Reynolds & Fletcher-Janzen, 2002). In some situations, high K scores may be better understood as reflecting personality variables rather than defensiveness. People who score high on the Correction scale are more likely to be balanced, have good emotional control, and are able to handle stressful situations well.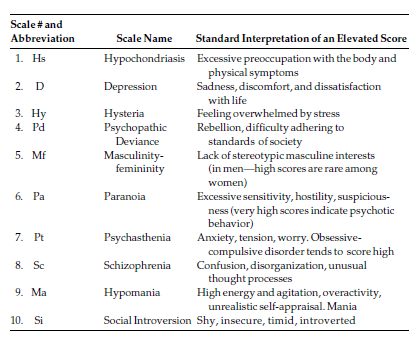 It is important for a psychologist to determine the true reason for the increase in the K scale.
It is important for a psychologist to determine the true reason for the increase in the K scale.
Descriptors as the K scale increases
Complaints Few or no complaints
Thoughts denial of problems, rational, logical
Emotions behavior Controlling, emotionally uncomfortable, conventional, conforming, socially acceptable, lacking self-awareness
Strengths Socially adequate, self-confident, positive self-concept, stable, strong ability to cope with emotional stress
Feedback for a client with elevated K scores (T>65)
You are a person for whom it is important to act in a socially acceptable way. You tend to approach life from a position of logic and rationality - you try to control your emotions so that they do not knock you off balance. You approached the test in a way that showed your best side and was careful not to appear socially inappropriate or emotionally unstable.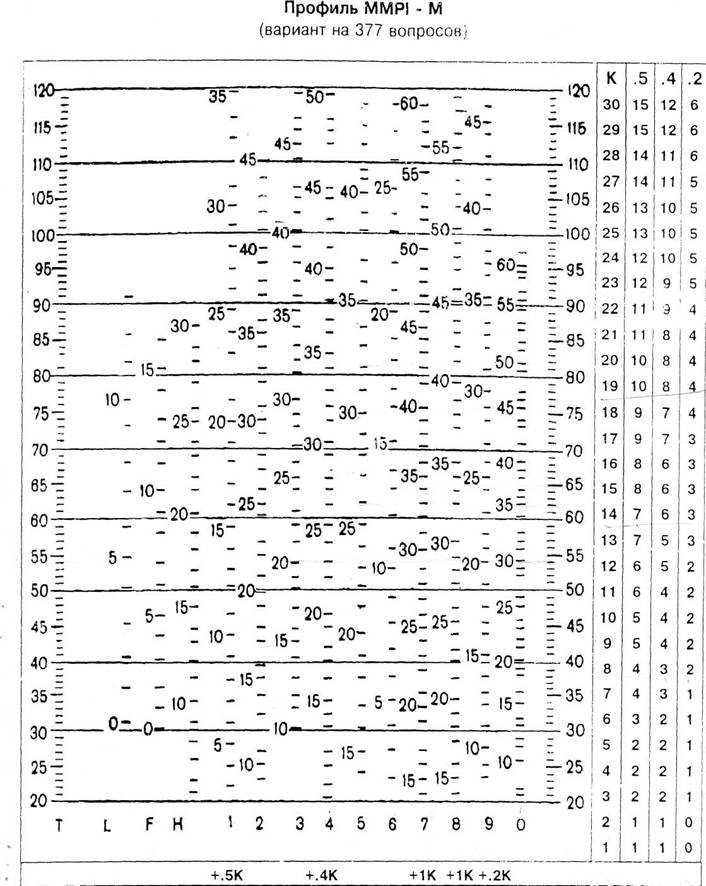 People may feel that you are defensive because you don't like expressing strong emotions. It's likely that you rarely feel like your emotions are overwhelming you and you can't handle them.
People may feel that you are defensive because you don't like expressing strong emotions. It's likely that you rarely feel like your emotions are overwhelming you and you can't handle them.
Perhaps people may see some emotional limitation in you, because you rarely express bright emotions. In order for people to empathize with you, they need to know that you are an extremely reserved person and your behavior may not reflect the full gamut of feelings you experience.
People with a profile like yours don't usually spend much time thinking about and analyzing their own feelings. They go through life working hard to avoid unpleasant emotions. They may not always be aware of how they feel and how their emotions drive certain aspects of their behavior. But in moments of crisis, when others become very emotional, you are unlikely to lose your head. You will appear cool, calm, and collected, making it hard for others to understand how you feel. You seem to handle emotionally charged situations well, rarely feeling off balance.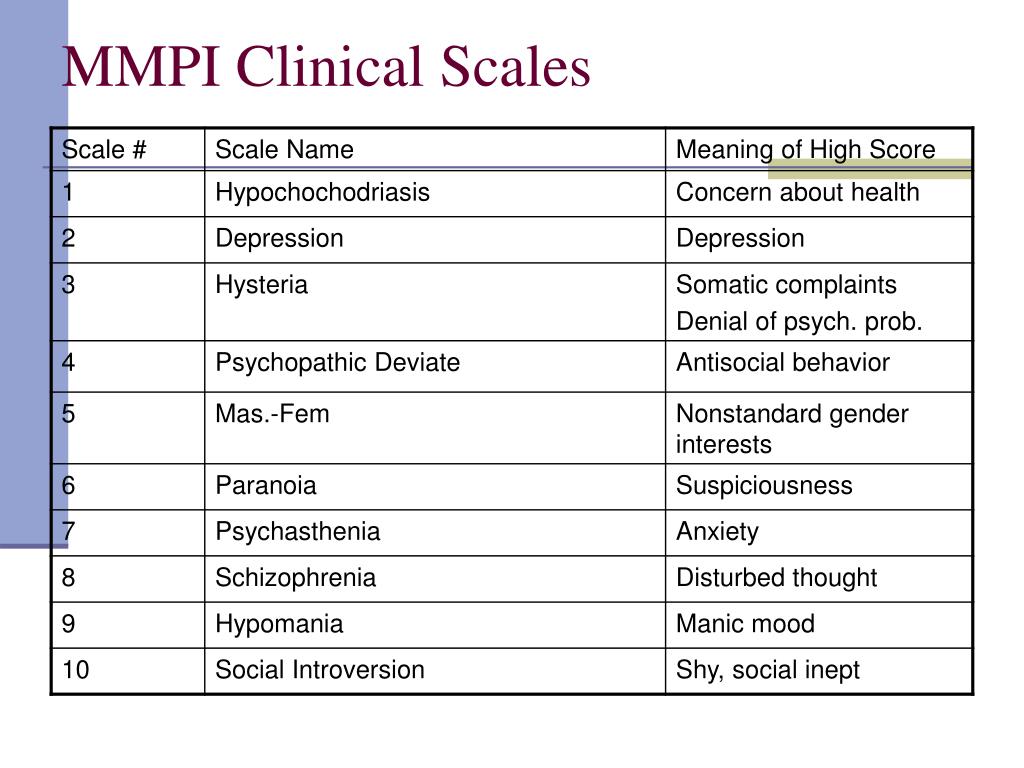
Psychological care and therapeutic pitfalls
The K scale, if properly interpreted, can be a useful indicator of a client's or patient's readiness for therapy or, in some cases, hesitancy about participating in treatment. In general, in its lower ranges—usually below T=40-45—the k scale reflects openness to emotional self-expression. In their upper ranges, usually above clinical scales and above 70 T-scores, these scores indicate aloofness towards expressing one's problems and discussing emotions.
As a rule, people with high K levels do not respond to cathartic and insight-oriented therapy. This is partly because they have emotional balance and control, but also because they may be wary of getting emotional. Therapy with such people can begin with a cognitive approach that helps to understand how people experience emotions. The therapist can help these clients understand how they have learned to control and suppress their emotions through cultural or learned inhibitions of emotional expressiveness.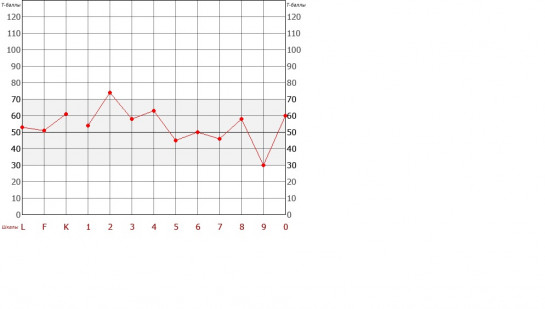 Once these clients are comfortable with discussing emotions, Gestalt techniques or role play can help release their emotions. Sometimes improvisation classes or acting lessons can help them become more emotionally expressive.
Once these clients are comfortable with discussing emotions, Gestalt techniques or role play can help release their emotions. Sometimes improvisation classes or acting lessons can help them become more emotionally expressive.
Recommendations for treatment and self-help
1. Start by learning to recognize your emotions. You and your therapist can work together to identify any feelings you may be experiencing during your therapy session. Think about the positive emotional experience and take some time to identify where in your body the feelings you are experiencing are reflected. Do the same for negative experiences. See if you are preventing the emotions from getting too intense.
2. Explore any childhood or later experiences in which you felt
the possibility of losing emotional control. Go back to that time and allow yourself to feel those moments so you can explore the full range of emotional expression.
3. Remember that when you express your emotions, you often do it in a subdued way so that others do not have to empathize with you. Sometimes ask others how they perceive your feelings so that you do not lose emotional contact with them.
Remember that when you express your emotions, you often do it in a subdued way so that others do not have to empathize with you. Sometimes ask others how they perceive your feelings so that you do not lose emotional contact with them.
4. As you begin to feel more comfortable with your ability to respond to emotions, maybe acting can help you become more spontaneous and maybe even more creative.
5. Increased adaptability: Get to know the concept of “emotional intelligence”, which is the ability to identify, evaluate and manage your
emotions in a healthy way. There are many good self-development books on developing emotional intelligence to improve your personal and work life.
Low K-scale values (less than 45 T-scores)
Extremely low Correction scale scores in cases where a normative score is expected from the subject in accordance with his social status, may indicate dissatisfaction, cynicism, “masochistic tendencies” and poor response to treatment.
Low scores on the K scale generally indicate directness, insensitivity, vulnerability, and lack of emotional control.
When the clinical scores are increased when the K-score is lowered, this indicates that the personality characteristics associated with the clinical scores will be pronounced and stable. In some cases, a low Correction scale score may indicate exaggeration of problems and a “cry for help,” especially with significantly elevated clinical scales (with a T-score of 80 or higher). Low scores on the K scale may reflect defective personality integration and poor adjustment. When clinical scales indicate a severe disorder, low scores on the K scale indicate coping difficulties, and the need for supportive therapeutic care, without focus on insight, until the client is stabilized.
In the absence of an increase in the clinical scale, low K scores do not reflect emotional disturbance, but rather emotional directness and lack of respect for sensitive social demands.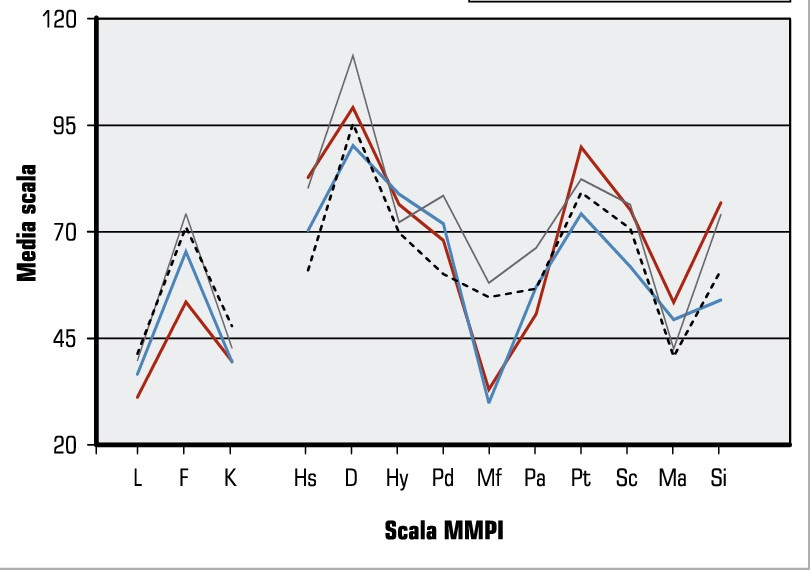 Individuals with low K scores tend to ignore or consider themselves superior to others' judgment of their emotional expressiveness.
Individuals with low K scores tend to ignore or consider themselves superior to others' judgment of their emotional expressiveness.
Descriptors
Complaints Depression, self-doubt, sometimes confusion, inefficiency, susceptibility to stress, low self-esteem
Thoughts Unsure of himself, self-critical, undeveloped, frightened, disorganized, jaded or cynical view of others
Emotions Fearful, ambivalent, depressed, uncontrollable, aloof from others.
Traits and behavior direct, defenseless, easily suppressed, cynical, complaining, impulsive, demanding
Strengths Open, honest, frank, spontaneous, emotionally authentic
Lifestyle and family background
Lower levels of the Correction scale are associated with lower educational levels and lower emotional intelligence. In people with low scores on the K scale, as a rule, excessive emotions and stress are likely to cause impairments in the efficiency and performance of executive functioning.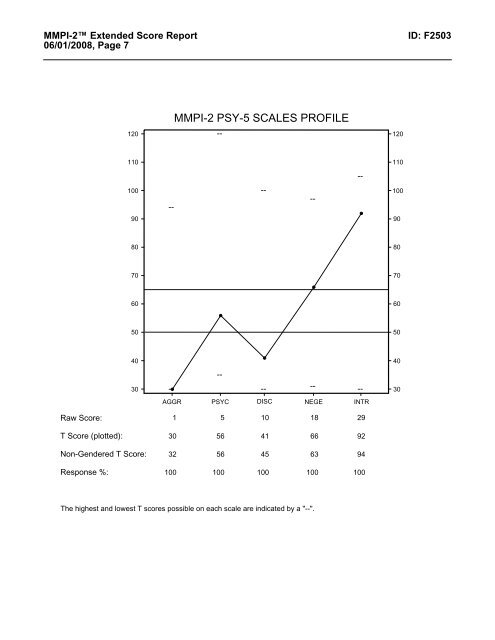 In the absence of any elevations on clinical scales, low scores on the K scale may demonstrate open, emotionally spontaneous, and uninhibited personalities. As a general rule, the lower the K, the more likely the person feels to be in the grip of emotional states.
In the absence of any elevations on clinical scales, low scores on the K scale may demonstrate open, emotionally spontaneous, and uninhibited personalities. As a general rule, the lower the K, the more likely the person feels to be in the grip of emotional states.
Modifying Scales
If the clinical and F scales are below 65 (70 for MMPI and SMIL) T-scores, a reduced Correction scale may reflect emotional immediacy bordering on cockiness.
Normal Range Feedback (45 to 65 (70) T-scores)
Your scores on this scale are within the normal range. This rating reflects that you answered the questions openly without trying to be too self-critical. Your approach was honest and precise to the best of your ability. You are likely to be quite independent and adventurous, as well as have good adaptability and coping skills. You have a wide range of interests and sufficient personal resources.
Feedback with reduced values of the scale Corrections
Important! Some of these feedback statements can be used to supplement feedback statements on clinical scales. These statements are not relevant if all clinical MMPI-2 scores are below the 60 T-point level (65 T-points for MMPI, SMIL).
These statements are not relevant if all clinical MMPI-2 scores are below the 60 T-point level (65 T-points for MMPI, SMIL).
Your profile suggests that your emotions and feelings are highly visible to others. If you feel upset or happy, others can easily see it. At the same time, if you feel angry, angry or sad, the intensity of your feelings may be perceived by others as excessive or inappropriate. Your feelings can overwhelm you and prevent you from functioning effectively. When stress arises, it can disorganize you so that you find it difficult to work effectively or do your usual things. The intensity of your emotions may even scare you.
Because you feel so out of balance, you may doubt yourself and therefore have difficulty making decisions. You may find it difficult to trust what you feel and what you think. You tend to be your own harshest critic and you always evaluate yourself from a very critical point of view.
Some of your thoughts may frighten you, and it will be difficult for you to get rid of them even if you try to do so.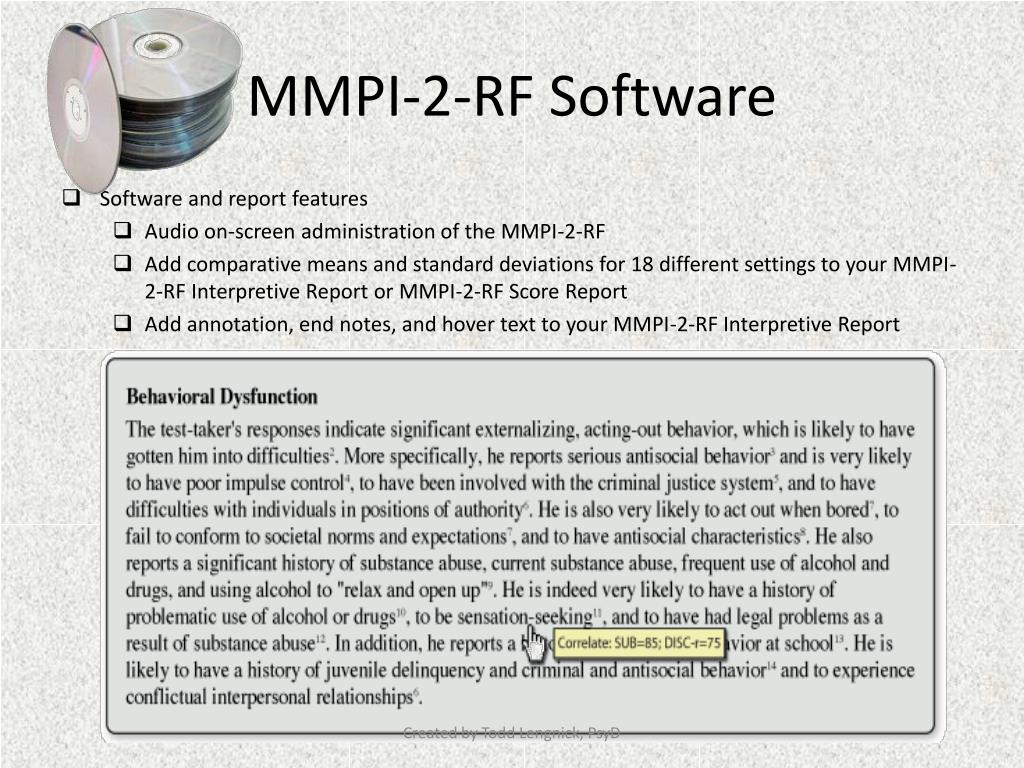 At present, you may be constantly on the edge, anxious and afraid that something bad will happen. People with your profile have a hard time controlling their thoughts and feelings, so they tend to be blunt and sometimes rude, which can sometimes backfire. The way you approached the test shows that you are very open and defenseless and willing to talk about how you feel.
At present, you may be constantly on the edge, anxious and afraid that something bad will happen. People with your profile have a hard time controlling their thoughts and feelings, so they tend to be blunt and sometimes rude, which can sometimes backfire. The way you approached the test shows that you are very open and defenseless and willing to talk about how you feel.
Psychological help and therapeutic pitfalls
In the presence of elevations on clinical scales, a low score on the Correction scale indicates the need for immediate, specific support and strengthening of the ego. It is recommended to use relaxation and thought-stopping techniques to cope with the emotional turmoil associated with clinical scale increases. In the presence of a serious disorder, low K values may indicate a collapse of the ego's defenses, so insight-oriented therapy is contraindicated. In such cases, it is necessary to take into account the possibility of a threat of suicide and the possibility of complete disorganization even with minor stress.