Manic episodes without bipolar
Mania vs. Hypomania: What’s the Difference?
Mania and hypomania are symptoms that can occur with bipolar disorder. They can also occur in people who don’t have bipolar disorder.
What is mania?
Mania is more than just having extra energy. It’s a mood disturbance that makes you atypically energized, both physically and mentally, for a week or more. Mania can be severe enough to require you to be hospitalized.
Mania can occur in people with bipolar I disorder. In many cases of bipolar I, manic episodes can alternate with periods of depression.
However, people with bipolar I disorder don’t always have depressive episodes, and it’s very common for an individual to have more typical moods in between episodes.
What is hypomania?
Hypomania is a milder form of mania. If you’re experiencing hypomania, your energy level is higher than usual, but it’s not as extreme as in mania, and it may only last for a few days.
Other people may notice if you have hypomania, but in many cases, you won’t need to be hospitalized for it.
People with bipolar II disorder may experience hypomania that alternates with depression, or they may have more typical emotional states in between each.
The main differences between mania and hypomania are the intensity of the symptoms and how long those symptoms last. Symptoms of mania are much more intense than those of hypomania and can last for a week or more.
Symptoms of mania and hypomania
While they vary in intensity, most of the symptoms of mania and hypomania are the same. The key symptoms include:
- having higher-than-typical energy levels
- being restless or unable to sit still
- having a decreased need for sleep
- having increased self-esteem or confidence, or grandiosity
- being more talkative
- having a racing mind, or having lots of new ideas and plans
- having decreased inhibitions
- having increased sexual desire
- engaging in potentially risky behavior that may be atypical for you, such as having impulsive sex, gambling with life savings, or going on big spending sprees
The slight differences between mania and hypomania include:
| Mania | Hypomania |
|---|---|
Your behavior is so extreme that regular activities cannot be maintained.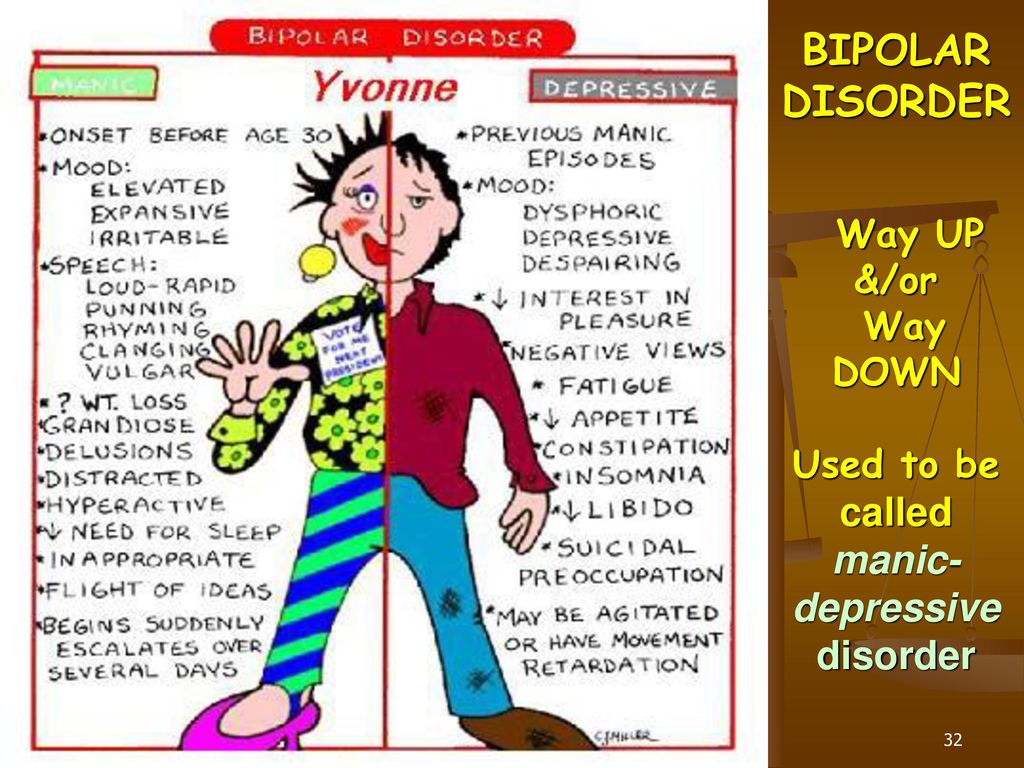 | People might notice changes, but your regular activities may still be maintained. |
| Delusions or hallucinations may occur. | Typically, delusions and hallucinations do not occur. |
| Feelings of invincibility are common. | Risk-taking is common. |
| You may feel “detached” from reality. | You may feel easily distracted. |
During a manic or hypomanic phase, you may not be able to recognize these changes in yourself.
The more severe symptoms of mania
Unlike hypomanic episodes, manic episodes can lead to serious consequences. When the mania subsides, you may experience remorse or depression for things you’ve done during the episode.
With mania, you may also have a break with reality. Psychotic symptoms can include:
- visual or auditory hallucinations
- delusional thoughts
- paranoid thoughts
Mania and hypomania are common symptoms of bipolar disorder. However, they can also be brought on by:
However, they can also be brought on by:
- sleep deprivation
- medication
- alcohol use
- drug use
The exact cause of bipolar disorder is unclear. Family history may play a role. You may be more likely to develop bipolar disorder if you have a family history of the illness.
Brain structure may also play a role, but there isn’t enough research to draw conclusions about this.
You’re at an increased risk of mania or hypomania if you’ve already had an episode. Your risk may also increase if you have bipolar disorder and are unable to take your medications as your doctor prescribes.
Mania and hypomania, as well as bipolar disorder itself, can’t be prevented. However, you can take steps to lessen the effects of an episode.
Maintaining your support systems and working with a mental health professional are two methods to lessen the possibility of an episode, as well as manage one if it occurs.
Above all, if you have a treatment plan, it’s important to stick with it. Take your medications as prescribed and keep an open line of communication with your doctor. Working together, you and your doctor can manage your symptoms and improve your quality of life.
Take your medications as prescribed and keep an open line of communication with your doctor. Working together, you and your doctor can manage your symptoms and improve your quality of life.
“Bipolar mania can be a scary thing to experience. But the good news is that bipolar disorder is treatable. Since receiving my diagnosis, I’ve found the right medication and the right dosage so that day-to-day life is totally normal.”
— Mara Robinson
If you believe you may be dealing with symptoms of mania, hypomania, or bipolar disorder itself, it’s a good idea to talk with your regular doctor first. During your appointment, your doctor will likely take your medical history and do a physical exam.
It’s important that you tell your doctor about all the prescription and over-the-counter medications and supplements you take, as well as any illegal drugs you may have taken.
If your doctor suspects you are indeed dealing with mania or hypomania, they will likely refer you to a mental health professional for an actual diagnosis.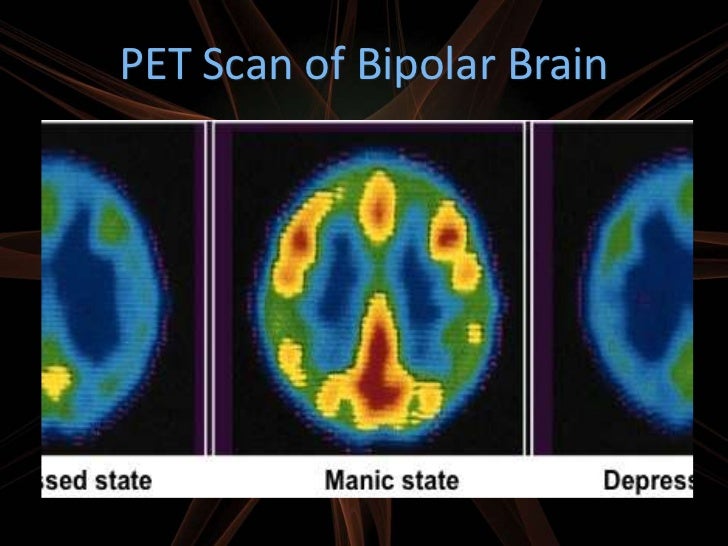
Diagnosing mania and hypomania can be complicated. For instance, you may not be aware of some symptoms or how long you’ve been having them.
Also, if you have depression but your doctor is unaware of your manic or hypomanic behavior, they may diagnose you with depression instead of bipolar disorder.
In addition, other health conditions can cause mania and hypomania.
Diagnosing mania
In most cases, symptoms must last at least a week for your doctor to diagnose them as mania. However, if your symptoms are so severe that you’re hospitalized, a diagnosis can be made even if the symptoms last for a shorter time.
Diagnosing hypomania
Your symptoms must persist for at least 4 days for your doctor to diagnose hypomania.
To treat mania and hypomania, your doctor may prescribe psychotherapy as well as medication. The medication can include mood stabilizers and antipsychotics.
You may need to try several different medications before your doctor discovers the right combination to treat your symptoms effectively.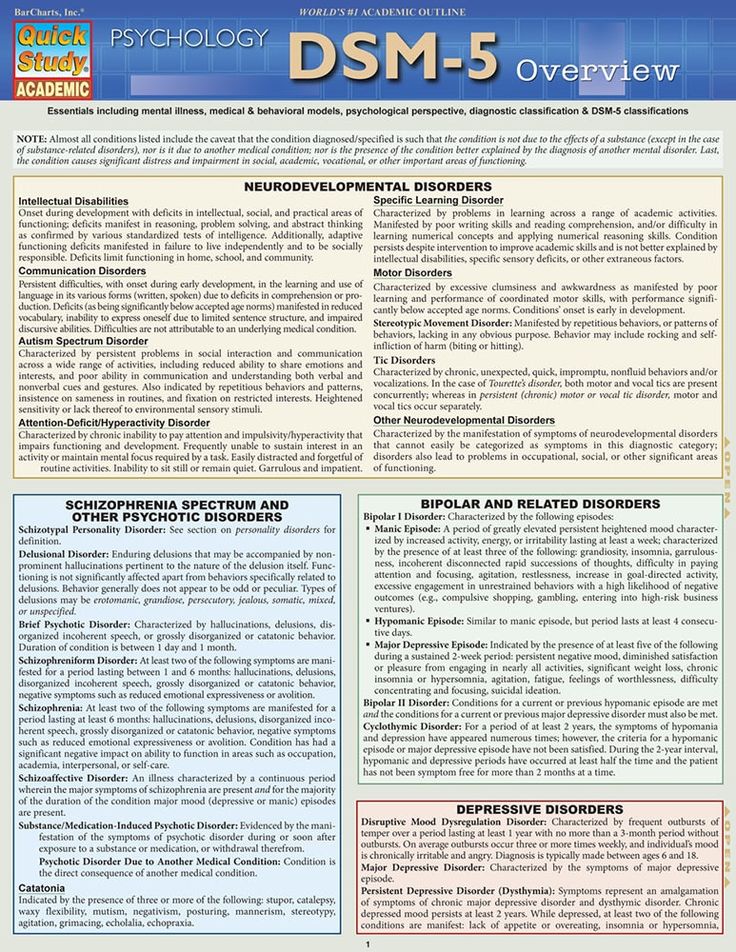
It’s important that you take your medication as your doctor prescribes. Even if you have side effects from the drugs, it can be dangerous to stop taking your medication without your doctor’s supervision.
If you have problems with side effects, talk with your doctor. They may be able to switch you to a different kind of treatment that isn’t so difficult on your body.
For hypomania, it’s often possible to cope without medication. Healthy lifestyle habits can help, such as:
- maintaining a balanced, nutritious diet
- getting physical activity every day
- keeping a regular sleep schedule and prioritizing rest
- keeping a journal that notes any mood changes or changes pointed out by loved ones
These tips can help you cope with mania and hypomania:
- Learning all you can about your condition. Mania and hypomania can be managed. Learn to recognize personal triggers so you can do your best to avoid them if possible.
- Keeping a mood diary. By charting your moods, you might be able to spot early warning signs. With your doctor’s help, you may also be able to prevent an episode from worsening. For instance, if you learn to spot the early warning signs of a manic episode, you can work with your doctor to manage it.
- Staying in treatment. If you have bipolar disorder, treatment is key. It might even be a good idea to get your family involved in therapy.
- Watching for suicidal thoughts. If you have thoughts of self-harm, speak with a trusted friend or family member immediately or contact a suicide prevention hotline.
- Reaching out to others for help. Asking for help is a strength, not a weakness. Talk with loved ones about your situation and how they can best help you succeed. Look up support groups for individuals living with bipolar disorder. The more support you have, the less alone you may feel.
Suicide prevention
If you have thoughts of harming yourself, tell your family or doctor right away.
You can also call the National Suicide Prevention Lifeline at 800-273-TALK (800-273-8255). Trained counselors are available 24/7.
Mania and hypomania are two common symptoms of bipolar disorder, but they can occur outside of that disorder as well. Both mania and hypomania can cause a marked increase in energy, uplifted emotions, risk-taking behaviors, and irritability.
While the episode may feel good while it’s occurring, both conditions can cause an individual to do things they might regret later.
Mania can be especially harmful if not properly managed.
Although these two mental health conditions share similar characteristics, the big differences between mania and hypomania are the severity and the length of time an episode lasts.
If you believe you or someone you love is experiencing a manic or hypomanic episode, talk with a mental health professional as soon as you can.
Manic episodes can be treated with medication, therapy, and support. Hypomanic episodes can sometimes be managed with lifestyle changes instead of medication.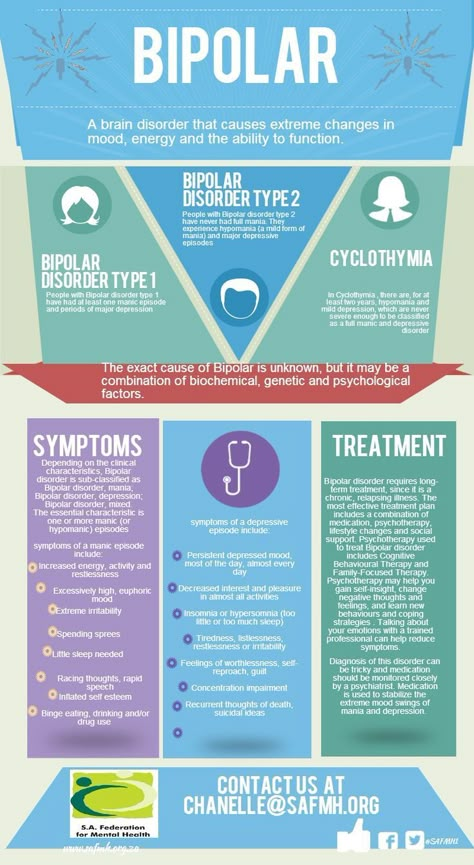
Mania vs. Hypomania: What’s the Difference?
Mania and hypomania are symptoms that can occur with bipolar disorder. They can also occur in people who don’t have bipolar disorder.
What is mania?
Mania is more than just having extra energy. It’s a mood disturbance that makes you atypically energized, both physically and mentally, for a week or more. Mania can be severe enough to require you to be hospitalized.
Mania can occur in people with bipolar I disorder. In many cases of bipolar I, manic episodes can alternate with periods of depression.
However, people with bipolar I disorder don’t always have depressive episodes, and it’s very common for an individual to have more typical moods in between episodes.
What is hypomania?
Hypomania is a milder form of mania. If you’re experiencing hypomania, your energy level is higher than usual, but it’s not as extreme as in mania, and it may only last for a few days.
Other people may notice if you have hypomania, but in many cases, you won’t need to be hospitalized for it.
People with bipolar II disorder may experience hypomania that alternates with depression, or they may have more typical emotional states in between each.
The main differences between mania and hypomania are the intensity of the symptoms and how long those symptoms last. Symptoms of mania are much more intense than those of hypomania and can last for a week or more.
Symptoms of mania and hypomania
While they vary in intensity, most of the symptoms of mania and hypomania are the same. The key symptoms include:
- having higher-than-typical energy levels
- being restless or unable to sit still
- having a decreased need for sleep
- having increased self-esteem or confidence, or grandiosity
- being more talkative
- having a racing mind, or having lots of new ideas and plans
- having decreased inhibitions
- having increased sexual desire
- engaging in potentially risky behavior that may be atypical for you, such as having impulsive sex, gambling with life savings, or going on big spending sprees
The slight differences between mania and hypomania include:
| Mania | Hypomania |
|---|---|
Your behavior is so extreme that regular activities cannot be maintained. | People might notice changes, but your regular activities may still be maintained. |
| Delusions or hallucinations may occur. | Typically, delusions and hallucinations do not occur. |
| Feelings of invincibility are common. | Risk-taking is common. |
| You may feel “detached” from reality. | You may feel easily distracted. |
During a manic or hypomanic phase, you may not be able to recognize these changes in yourself.
The more severe symptoms of mania
Unlike hypomanic episodes, manic episodes can lead to serious consequences. When the mania subsides, you may experience remorse or depression for things you’ve done during the episode.
With mania, you may also have a break with reality. Psychotic symptoms can include:
- visual or auditory hallucinations
- delusional thoughts
- paranoid thoughts
Mania and hypomania are common symptoms of bipolar disorder. However, they can also be brought on by:
However, they can also be brought on by:
- sleep deprivation
- medication
- alcohol use
- drug use
The exact cause of bipolar disorder is unclear. Family history may play a role. You may be more likely to develop bipolar disorder if you have a family history of the illness.
Brain structure may also play a role, but there isn’t enough research to draw conclusions about this.
You’re at an increased risk of mania or hypomania if you’ve already had an episode. Your risk may also increase if you have bipolar disorder and are unable to take your medications as your doctor prescribes.
Mania and hypomania, as well as bipolar disorder itself, can’t be prevented. However, you can take steps to lessen the effects of an episode.
Maintaining your support systems and working with a mental health professional are two methods to lessen the possibility of an episode, as well as manage one if it occurs.
Above all, if you have a treatment plan, it’s important to stick with it. Take your medications as prescribed and keep an open line of communication with your doctor. Working together, you and your doctor can manage your symptoms and improve your quality of life.
Take your medications as prescribed and keep an open line of communication with your doctor. Working together, you and your doctor can manage your symptoms and improve your quality of life.
“Bipolar mania can be a scary thing to experience. But the good news is that bipolar disorder is treatable. Since receiving my diagnosis, I’ve found the right medication and the right dosage so that day-to-day life is totally normal.”
— Mara Robinson
If you believe you may be dealing with symptoms of mania, hypomania, or bipolar disorder itself, it’s a good idea to talk with your regular doctor first. During your appointment, your doctor will likely take your medical history and do a physical exam.
It’s important that you tell your doctor about all the prescription and over-the-counter medications and supplements you take, as well as any illegal drugs you may have taken.
If your doctor suspects you are indeed dealing with mania or hypomania, they will likely refer you to a mental health professional for an actual diagnosis.
Diagnosing mania and hypomania can be complicated. For instance, you may not be aware of some symptoms or how long you’ve been having them.
Also, if you have depression but your doctor is unaware of your manic or hypomanic behavior, they may diagnose you with depression instead of bipolar disorder.
In addition, other health conditions can cause mania and hypomania.
Diagnosing mania
In most cases, symptoms must last at least a week for your doctor to diagnose them as mania. However, if your symptoms are so severe that you’re hospitalized, a diagnosis can be made even if the symptoms last for a shorter time.
Diagnosing hypomania
Your symptoms must persist for at least 4 days for your doctor to diagnose hypomania.
To treat mania and hypomania, your doctor may prescribe psychotherapy as well as medication. The medication can include mood stabilizers and antipsychotics.
You may need to try several different medications before your doctor discovers the right combination to treat your symptoms effectively.
It’s important that you take your medication as your doctor prescribes. Even if you have side effects from the drugs, it can be dangerous to stop taking your medication without your doctor’s supervision.
If you have problems with side effects, talk with your doctor. They may be able to switch you to a different kind of treatment that isn’t so difficult on your body.
For hypomania, it’s often possible to cope without medication. Healthy lifestyle habits can help, such as:
- maintaining a balanced, nutritious diet
- getting physical activity every day
- keeping a regular sleep schedule and prioritizing rest
- keeping a journal that notes any mood changes or changes pointed out by loved ones
These tips can help you cope with mania and hypomania:
- Learning all you can about your condition. Mania and hypomania can be managed. Learn to recognize personal triggers so you can do your best to avoid them if possible.
- Keeping a mood diary. By charting your moods, you might be able to spot early warning signs. With your doctor’s help, you may also be able to prevent an episode from worsening. For instance, if you learn to spot the early warning signs of a manic episode, you can work with your doctor to manage it.
- Staying in treatment. If you have bipolar disorder, treatment is key. It might even be a good idea to get your family involved in therapy.
- Watching for suicidal thoughts. If you have thoughts of self-harm, speak with a trusted friend or family member immediately or contact a suicide prevention hotline.
- Reaching out to others for help. Asking for help is a strength, not a weakness. Talk with loved ones about your situation and how they can best help you succeed. Look up support groups for individuals living with bipolar disorder. The more support you have, the less alone you may feel.
Suicide prevention
If you have thoughts of harming yourself, tell your family or doctor right away.
You can also call the National Suicide Prevention Lifeline at 800-273-TALK (800-273-8255). Trained counselors are available 24/7.
Mania and hypomania are two common symptoms of bipolar disorder, but they can occur outside of that disorder as well. Both mania and hypomania can cause a marked increase in energy, uplifted emotions, risk-taking behaviors, and irritability.
While the episode may feel good while it’s occurring, both conditions can cause an individual to do things they might regret later.
Mania can be especially harmful if not properly managed.
Although these two mental health conditions share similar characteristics, the big differences between mania and hypomania are the severity and the length of time an episode lasts.
If you believe you or someone you love is experiencing a manic or hypomanic episode, talk with a mental health professional as soon as you can.
Manic episodes can be treated with medication, therapy, and support. Hypomanic episodes can sometimes be managed with lifestyle changes instead of medication.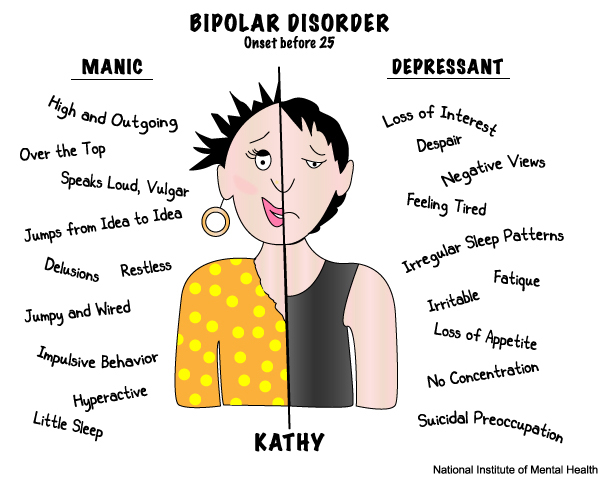
Bipolar Disorder | Symptoms, complications, diagnosis and treatment
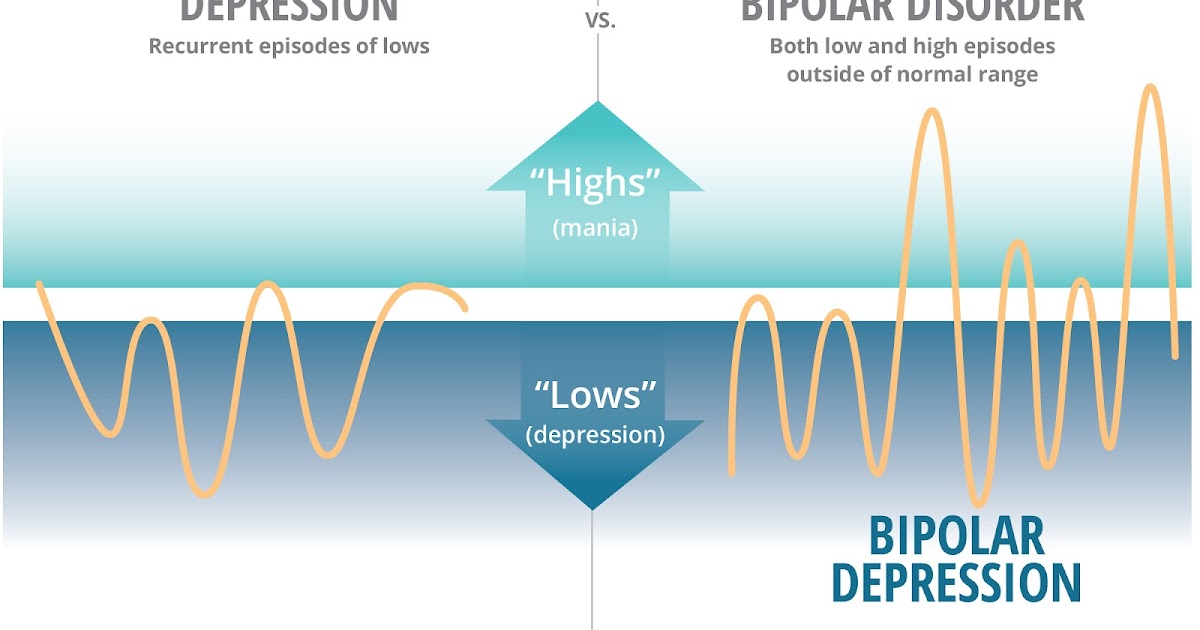
Bipolar disorder, formerly called manic depression, is a mental health condition that causes extreme mood swings that include emotional highs (mania or hypomania) and lows (depression). Episodes of mood swings may occur infrequently or several times a year.
When you become depressed, you may feel sad or hopeless and lose interest or pleasure in most activities. When the mood shifts to mania or hypomania (less extreme than mania), you may feel euphoric, full of energy or unusually irritable. These mood swings can affect sleep, energy, alertness, judgment, behavior, and the ability to think clearly.
Although bipolar disorder is a lifelong condition, you can manage your mood swings and other symptoms by following a treatment plan. In most cases, bipolar disorder is treated with medication and psychological counseling (psychotherapy).
Symptoms
There are several types of bipolar and related disorders. They may include mania, hypomania, and depression. The symptoms can lead to unpredictable changes in mood and behavior, leading to significant stress and difficulty in life.
They may include mania, hypomania, and depression. The symptoms can lead to unpredictable changes in mood and behavior, leading to significant stress and difficulty in life.
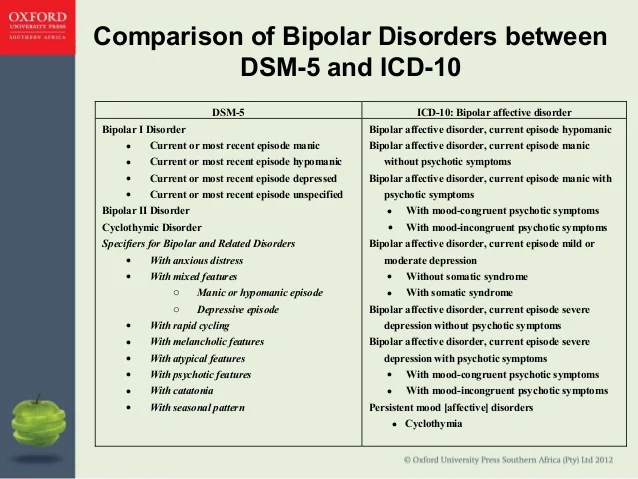
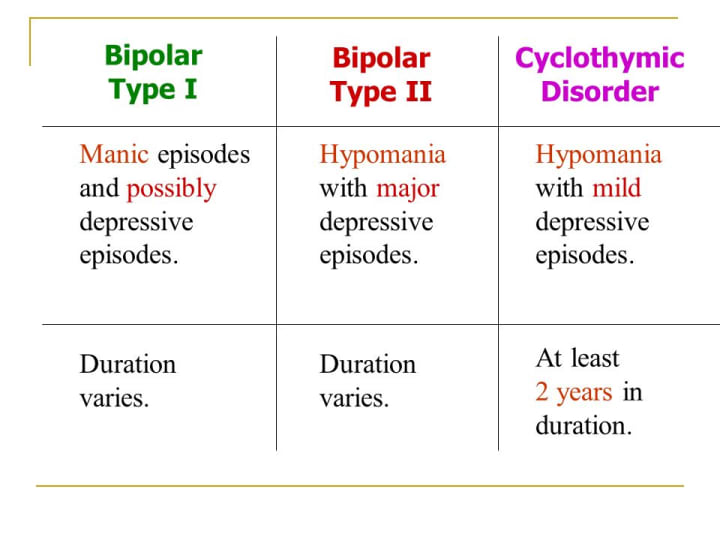
- Bipolar disorder I. You have had at least one manic episode, which may be preceded or accompanied by hypomanic or major depressive episodes. In some cases, mania can cause a break with reality (psychosis).
- Bipolar disorder II. You have had at least one major depressive episode and at least one hypomanic episode, but never had a manic episode.
- Cyclothymic disorder. You have had at least two years - or one year in children and adolescents - many periods of hypomanic symptoms and periods of depressive symptoms (though less severe than major depression).
- Other types. These include, for example, bipolar and related disorders caused by certain drugs or alcohol, or due to health conditions such as Cushing's disease, multiple sclerosis, or stroke.
Bipolar II is not a milder form of Bipolar I but is a separate diagnosis. Although bipolar I manic episodes can be severe and dangerous, people with bipolar II can be depressed for longer periods of time, which can cause significant impairment.
Although bipolar disorder can occur at any age, it is usually diagnosed in adolescence or early twenties. Symptoms can vary from person to person, and symptoms can change over time.
Mania and hypomania
Mania and hypomania are two different types of episodes, but they share the same symptoms. Mania is more pronounced than hypomania and causes more noticeable problems at work, school, and social activities, as well as relationship difficulties. Mania can also cause a break with reality (psychosis) and require hospitalization.
Both a manic episode and a hypomanic episode include three or more of these symptoms:
- Abnormally optimistic or nervous
- Increased activity, energy or excitement
- Exaggerated sense of well-being and self-confidence (euphoria)
- Reduced need for sleep
- Unusual talkativeness
- Distractibility
- Poor decision-making - for example, in speculation, in sexual encounters or in irrational investments
Major depressive episode
Major depressive episode includes symptoms that are severe enough to cause noticeable difficulty in daily activities such as work, school, social activities, or relationships.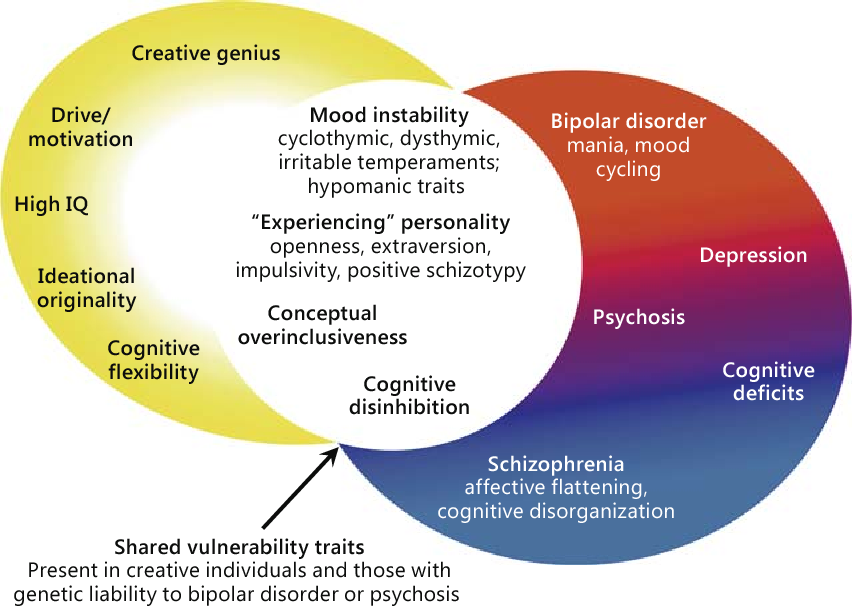 Episode includes five or more of these symptoms:
Episode includes five or more of these symptoms:
- Depressed mood, such as feeling sad, empty, hopeless, or tearful (in children and adolescents, depressed mood may manifest as irritability)
- Marked loss of interest or feeling of displeasure in all (or nearly all) activities
- Significant weight loss with no diet, weight gain, or decreased or increased appetite (in children, failure to gain weight as expected may be a sign of depression)
- Either insomnia or sleeping too much
- Either anxiety or slow behavior
- Fatigue or loss of energy
- Feelings of worthlessness or excessive or inappropriate guilt
- Decreased ability to think or concentrate, or indecisiveness
- Thinking, planning or attempting suicide
Other features of bipolar disorder
Signs and symptoms of bipolar I and bipolar II disorder may include other signs such as anxiety disorder, melancholia, psychosis, or others.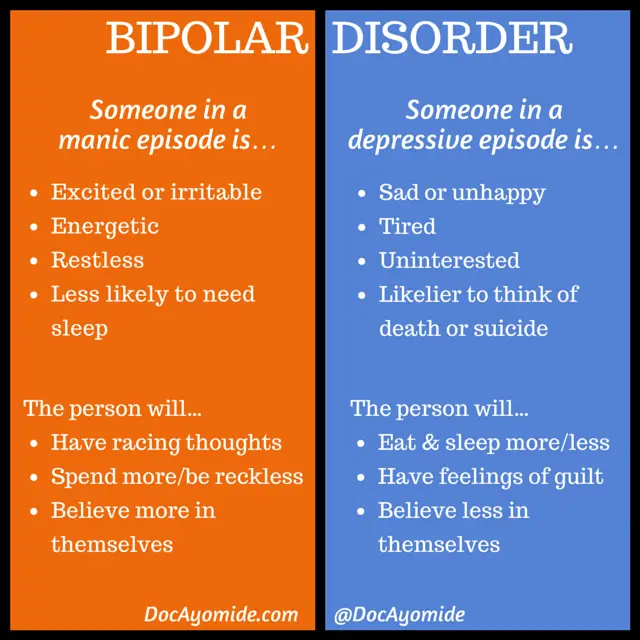 The timing of symptoms may include diagnostic markers such as mixed or fast cycling. In addition, bipolar symptoms may occur during pregnancy or with the change of seasons.
The timing of symptoms may include diagnostic markers such as mixed or fast cycling. In addition, bipolar symptoms may occur during pregnancy or with the change of seasons.
When to see a doctor
Despite extreme moods, people with bipolar disorder often do not realize how much their emotional instability disrupts their lives and the lives of their loved ones and do not receive the necessary treatment.
And if you are like people with bipolar disorder, you can enjoy feelings of euphoria and be more productive. However, this euphoria is always accompanied by an emotional disaster that can leave you depressed and possibly in financial, legal, or other bad relationships.
If you have symptoms of depression or mania, see your doctor or mental health professional. Bipolar disorder does not improve on its own. Getting mental health treatment with a history of bipolar disorder can help control your symptoms.
Bipolar affective disorder and everything you need to know about it
More than 60 million people in the world suffer from bipolar affective disorder (BAD). The essence of the disease is that a person has alternating periods of altered mood throughout his life: from a state with a minus sign to a state with a plus sign. How and why is this happening?
The essence of the disease is that a person has alternating periods of altered mood throughout his life: from a state with a minus sign to a state with a plus sign. How and why is this happening?
Marina KINKULKINA, psychiatrist of the highest category, head of the department of psychiatry and narcology, director of the Institute of Electronic Medical Education, First Moscow State Medical University. I. M. Sechenova, Corresponding Member of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences
Moreover, it is often not just about sadness or fun, as is often the case with emotional people, but about extreme degrees of either despair or euphoria. The change in these moods can take place both gradually and suddenly, and often for no apparent reason. This disease is attributed to Byron and Hemingway, Virginia Woolf and Edgar Poe, Van Gogh, Schumann, Vivien Leigh and many others. There is an assumption that even “our everything” suffered from a mild degree of BAD (contemporaries often mentioned mood swings) A. S. Pushkin. Modern stars - Catherine Zeta-Jones and Mel Gibson - openly admit to having this mental disorder. And rapper Kanye West even put the inscription on the cover of his album: "I hate being bipolar, it's amazing." A very accurate description of the essence of this disease.
S. Pushkin. Modern stars - Catherine Zeta-Jones and Mel Gibson - openly admit to having this mental disorder. And rapper Kanye West even put the inscription on the cover of his album: "I hate being bipolar, it's amazing." A very accurate description of the essence of this disease.
Genetics does not solve everything
BAD affects both men and women, but the weaker sex - more often. As for the age of onset of the disease, this disorder can also appear in a teenager (especially if there is an appropriate heredity), and in an adult, and even in an elderly person. Everything is individual. The main risk factor is genetics, but a specific gene that would be responsible for the development of bipolar disorder has not been identified. This is a polygenic disorder, and it makes no sense to take genetic tests to find out how great the risk of getting sick is, because scientists still do not have a consensus on what specific combination of genes can lead to a violation. But even if there is a genetic predisposition, it is not certain that the disease will develop. This was proven by studies on identical twins, one of which developed bipolar disorder over the years, while the other did not. Accordingly, there must be some other predisposing moments. Science knows about some of them: life at the limit of possibilities with constant hands-on work, stress and chronic lack of sleep, as well as night shift work, frequent flights with a significant change in hourly flights and, of course, the use of psychoactive substances contribute to the development of the disease. Therefore, they should be avoided. Scientists have yet to learn about other factors.
This was proven by studies on identical twins, one of which developed bipolar disorder over the years, while the other did not. Accordingly, there must be some other predisposing moments. Science knows about some of them: life at the limit of possibilities with constant hands-on work, stress and chronic lack of sleep, as well as night shift work, frequent flights with a significant change in hourly flights and, of course, the use of psychoactive substances contribute to the development of the disease. Therefore, they should be avoided. Scientists have yet to learn about other factors.
But not boring?
The number of people suffering from bipolar disorder among the population, according to various estimates, varies from fractions of one percent to several percent. Recently, psychiatrists note, the proportion of affective disorders has increased significantly, which can be explained by improved diagnostics. At first glance, the BAR does not look like something scary and dangerous. To ignorant people, this disorder even seems attractive - sometimes sad, sometimes fun, in general, you won’t get bored. In addition, being different from everyone else is now fashionable. And then, there is an opinion that people with BAD have higher intelligence and creative abilities than the “gray masses”. But even if this is so, then none of those who suffer from it will definitely call BAD a pleasant thing. It is especially difficult for those patients who do not seek medical help on time. Without treatment, both phases of bipolar disorder can last for months (although sometimes the disorder occurs with frequently alternating phases). Moreover, it is impossible to say which of the periods of the disease is more difficult, manic or depressive.
To ignorant people, this disorder even seems attractive - sometimes sad, sometimes fun, in general, you won’t get bored. In addition, being different from everyone else is now fashionable. And then, there is an opinion that people with BAD have higher intelligence and creative abilities than the “gray masses”. But even if this is so, then none of those who suffer from it will definitely call BAD a pleasant thing. It is especially difficult for those patients who do not seek medical help on time. Without treatment, both phases of bipolar disorder can last for months (although sometimes the disorder occurs with frequently alternating phases). Moreover, it is impossible to say which of the periods of the disease is more difficult, manic or depressive.
Bad when very bad
Those who have experienced real depression say that this is the worst thing that can happen in life. In this state, the whole world is seen in black, the mood is depressed, self-esteem drops, life loses its meaning. A person suffering from BAD in the depressive phase perceives his very existence as a chain of tragic mistakes, constantly blaming himself for all the troubles and sins, even those that do not even exist. In addition to mental suffering, physical ones also arise: a person even moves with difficulty, as if swimming against the current, it is difficult for him to perform the most familiar actions. In addition, he can feel tension throughout the body, experience various pain sensations. With an average degree of depression, people often complain of debilitating pain in the abdomen and other parts of the body. On this occasion, they turn to doctors, but the diagnosis cannot be made. And the daily pain continues to harass. Psychiatrists call this somatoform symptomatology. With severe depression, many have the so-called atrial depression. Patients complain of pain and heaviness in the chest, they say that "a stone lies on the heart." But even an in-depth examination does not reveal cardiac causes.
A person suffering from BAD in the depressive phase perceives his very existence as a chain of tragic mistakes, constantly blaming himself for all the troubles and sins, even those that do not even exist. In addition to mental suffering, physical ones also arise: a person even moves with difficulty, as if swimming against the current, it is difficult for him to perform the most familiar actions. In addition, he can feel tension throughout the body, experience various pain sensations. With an average degree of depression, people often complain of debilitating pain in the abdomen and other parts of the body. On this occasion, they turn to doctors, but the diagnosis cannot be made. And the daily pain continues to harass. Psychiatrists call this somatoform symptomatology. With severe depression, many have the so-called atrial depression. Patients complain of pain and heaviness in the chest, they say that "a stone lies on the heart." But even an in-depth examination does not reveal cardiac causes.
Often, with depression, patients (especially the elderly) complain of difficulty in thinking, memory impairment, they say that they have become stupid, they believe that they are developing dementia, they are afraid of “losing their mind”. In fact, affective disorders do not destroy the intellect. When treated with antidepressants, when the mood stabilizes, abilities are restored.
But the worst consequence of depression is suicide. Most suicide attempts are made in this state. Sometimes people in a very pronounced depression, believing that they have done something irreparable, and believing that the consequences of their actions can harm loved ones, decide on extended suicides, in which they settle scores not only with their lives, but also take their loved ones with them ( more often children).
Too bad when too good
The manic stage of BAD is subjectively more pleasant. Patients are not just in a very good, but in a great mood: they love the whole world and themselves in it.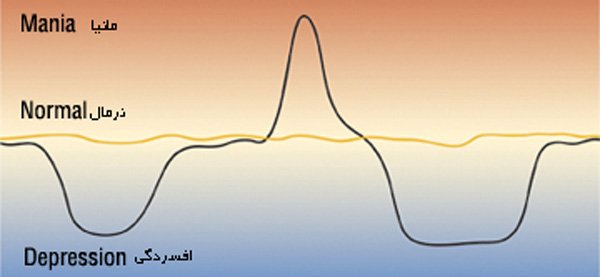 The reflection in the mirror pleases, there is not the slightest doubt about one’s own talents and mind, there is more than enough strength and energy, a bonus is accelerated mental activity. Many in this stage sleep for an hour a day, but do not experience fatigue. Sometimes they don’t sleep for whole days - and at least they are cheerful, like an “energizer”. It seems to be great. But no. With mania, desires and new ideas arise too quickly, so a person grabs at each new business, but, as a rule, does not bring any to the end. So productivity at this stage is no more than during depression. But it would be nice if that was the only thing.
The reflection in the mirror pleases, there is not the slightest doubt about one’s own talents and mind, there is more than enough strength and energy, a bonus is accelerated mental activity. Many in this stage sleep for an hour a day, but do not experience fatigue. Sometimes they don’t sleep for whole days - and at least they are cheerful, like an “energizer”. It seems to be great. But no. With mania, desires and new ideas arise too quickly, so a person grabs at each new business, but, as a rule, does not bring any to the end. So productivity at this stage is no more than during depression. But it would be nice if that was the only thing.
The main danger of mania is that a person has no criticism at this moment, and he can do things that he will later regret very much. For example, he can give away all his property to others (sometimes to unfamiliar people or scammers who specifically use this state of his). Or, say, take out loans to go on a trip to the other side of the world, and take a bunch of friends with him.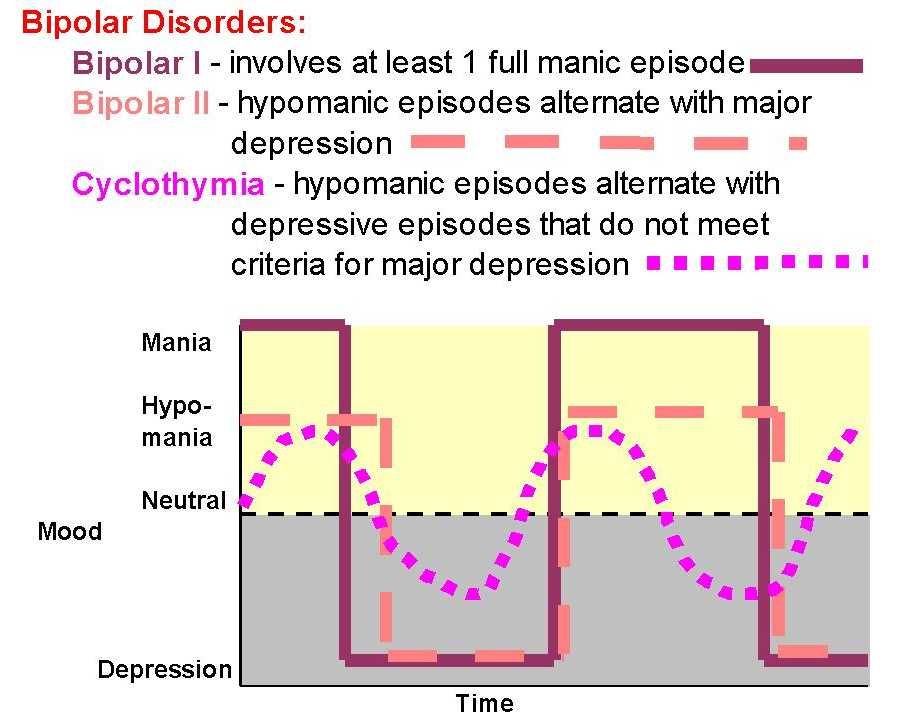 Maybe even steal something - for example, to make an expensive gift. Many patients at these moments enter into hasty intimate relationships, mistaking a chance meeting for the love of their life (and completely “forgetting” that family and children are waiting at home). Finally, often with mania, people, experiencing euphoria, ignore their severe somatic symptoms, as a result, they do not go to the doctor for a long time, and thus trigger a serious illness (pneumonia, for example). In addition, not all patients in the manic phase are "darlings." Often they show unreasonable aggression if, for example, others do not agree with their "brilliant" advice. As a result of such “angry mania”, conflicts and even situations arise that require the intervention of law enforcement agencies and the hospitalization of the patient without his consent in a psychiatric hospital.
Maybe even steal something - for example, to make an expensive gift. Many patients at these moments enter into hasty intimate relationships, mistaking a chance meeting for the love of their life (and completely “forgetting” that family and children are waiting at home). Finally, often with mania, people, experiencing euphoria, ignore their severe somatic symptoms, as a result, they do not go to the doctor for a long time, and thus trigger a serious illness (pneumonia, for example). In addition, not all patients in the manic phase are "darlings." Often they show unreasonable aggression if, for example, others do not agree with their "brilliant" advice. As a result of such “angry mania”, conflicts and even situations arise that require the intervention of law enforcement agencies and the hospitalization of the patient without his consent in a psychiatric hospital.
Good intentions…
The worst thing that relatives and friends of a person with bipolar disorder can do is ignore his problem, devalue suffering, while blaming the patient himself and appealing to his conscience. For example, they can call on a depressed person to “pull himself together, not become limp”, say that he is “mad with fat”, etc. A patient at the stage of mania is most often accused of immorality, irresponsibility, frivolity, promiscuity in relationships, etc. However, doing so is like blaming a person with diabetes for not being able to eat sweet cake, or a patient with heart failure for not running a marathon. BAD is a disease like many others. And she needs to be treated. The sooner you start the right therapy, the sooner you can stabilize the patient's condition and the better the further prognosis will be.
For example, they can call on a depressed person to “pull himself together, not become limp”, say that he is “mad with fat”, etc. A patient at the stage of mania is most often accused of immorality, irresponsibility, frivolity, promiscuity in relationships, etc. However, doing so is like blaming a person with diabetes for not being able to eat sweet cake, or a patient with heart failure for not running a marathon. BAD is a disease like many others. And she needs to be treated. The sooner you start the right therapy, the sooner you can stabilize the patient's condition and the better the further prognosis will be.
Psychiatrists don't bite
Despite the fact that recently people (especially young people) have ceased to be afraid to turn to psychiatrists, not everyone still decides to go to the doctor. Indeed, on the Internet in the public domain, you can find hundreds of questionnaires to test yourself for any mental disorder. And then, after reading various tips, you can also “cure”. Doctors strongly advise against doing this. The smallest harm of self-treatment is that it will not help or lead to incomplete improvement, but it can also worsen the condition. For example, inadequate intake of antidepressants in bipolar disorder can lead from a depressive phase into a severe manic state, from which it will then be difficult to get out. Only a psychiatrist (and not a psychologist, neurologist or doctor of any other somatic profile) can identify bipolar disorder and choose the right treatment. Treatment should be strictly individual, that is, the doctor selects it based on the characteristics of a particular patient and taking into account a specific moment in the course of the disease. The goal of therapy is not only to equalize the patient's mood, but also to prevent recurrence. In the treatment of bipolar disorder, the main role is played by drugs for stabilizing mood - mood stabilizers (lithium salts, some anticonvulsants (anticonvulsants) and antipsychotics of new generations).
Doctors strongly advise against doing this. The smallest harm of self-treatment is that it will not help or lead to incomplete improvement, but it can also worsen the condition. For example, inadequate intake of antidepressants in bipolar disorder can lead from a depressive phase into a severe manic state, from which it will then be difficult to get out. Only a psychiatrist (and not a psychologist, neurologist or doctor of any other somatic profile) can identify bipolar disorder and choose the right treatment. Treatment should be strictly individual, that is, the doctor selects it based on the characteristics of a particular patient and taking into account a specific moment in the course of the disease. The goal of therapy is not only to equalize the patient's mood, but also to prevent recurrence. In the treatment of bipolar disorder, the main role is played by drugs for stabilizing mood - mood stabilizers (lithium salts, some anticonvulsants (anticonvulsants) and antipsychotics of new generations). Modern drugs are much better tolerated than their predecessors, have fewer side effects, as they are designed for long-term use over many years. Against the background of their intake, women can even become pregnant and give birth. In depression, antidepressants are prescribed in exceptional cases, given the danger of changing the depressive stage to manic.
Modern drugs are much better tolerated than their predecessors, have fewer side effects, as they are designed for long-term use over many years. Against the background of their intake, women can even become pregnant and give birth. In depression, antidepressants are prescribed in exceptional cases, given the danger of changing the depressive stage to manic.
You won't be able to forget
The insidiousness of BAD is that this disease cannot be cured once and for all. But, alas, often, when the patient's mood can be balanced by medication and he begins to feel good (such a state - intermission - is completely indistinguishable from a state of complete health), he can stop taking the drugs. This is a big mistake that does not allow to achieve a stable result of treatment. Sometimes it is required to use medicines (necessarily under the supervision of a doctor) for several months, but more often for years (with periodic visits to the doctor). It is the long-term use of maintenance therapy individually selected by the doctor that allows patients to achieve a stable good condition and feel the joy of life for many years.
Link to publication: www.kiz.ru
Site embed code
More than 60 million people in the world suffer from bipolar affective disorder (BAD). The essence of the disease is that a person has alternating periods of altered mood throughout his life: from a state with a minus sign to a state with a plus sign. How and why is this happening?
Marina KINKULKINA, psychiatrist of the highest category, head of the department of psychiatry and narcology, director of the Institute of Electronic Medical Education, First Moscow State Medical University. I. M. Sechenova, Corresponding Member of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences
Moreover, it is often not just about sadness or fun, as is often the case with emotional people, but about extreme degrees of either despair or euphoria. The change in these moods can take place both gradually and suddenly, and often for no apparent reason. This disease is attributed to Byron and Hemingway, Virginia Woolf and Edgar Poe, Van Gogh, Schumann, Vivien Leigh and many others. There is an assumption that even “our everything” suffered from a mild degree of BAD (contemporaries often mentioned mood swings) A. S. Pushkin. Modern stars - Catherine Zeta-Jones and Mel Gibson - openly admit to having this mental disorder. And rapper Kanye West even put the inscription on the cover of his album: "I hate being bipolar, it's amazing." A very accurate description of the essence of this disease.
This disease is attributed to Byron and Hemingway, Virginia Woolf and Edgar Poe, Van Gogh, Schumann, Vivien Leigh and many others. There is an assumption that even “our everything” suffered from a mild degree of BAD (contemporaries often mentioned mood swings) A. S. Pushkin. Modern stars - Catherine Zeta-Jones and Mel Gibson - openly admit to having this mental disorder. And rapper Kanye West even put the inscription on the cover of his album: "I hate being bipolar, it's amazing." A very accurate description of the essence of this disease.
Genetics does not solve everything
BAD affects both men and women, but the weaker sex - more often. As for the age of onset of the disease, this disorder can also appear in a teenager (especially if there is an appropriate heredity), and in an adult, and even in an elderly person. Everything is individual. The main risk factor is genetics, but a specific gene that would be responsible for the development of bipolar disorder has not been identified. This is a polygenic disorder, and it makes no sense to take genetic tests to find out how great the risk of getting sick is, because scientists still do not have a consensus on what specific combination of genes can lead to a violation. But even if there is a genetic predisposition, it is not certain that the disease will develop. This was proven by studies on identical twins, one of which developed bipolar disorder over the years, while the other did not. Accordingly, there must be some other predisposing moments. Science knows about some of them: life at the limit of possibilities with constant hands-on work, stress and chronic lack of sleep, as well as night shift work, frequent flights with a significant change in hourly flights and, of course, the use of psychoactive substances contribute to the development of the disease. Therefore, they should be avoided. Scientists have yet to learn about other factors.
This is a polygenic disorder, and it makes no sense to take genetic tests to find out how great the risk of getting sick is, because scientists still do not have a consensus on what specific combination of genes can lead to a violation. But even if there is a genetic predisposition, it is not certain that the disease will develop. This was proven by studies on identical twins, one of which developed bipolar disorder over the years, while the other did not. Accordingly, there must be some other predisposing moments. Science knows about some of them: life at the limit of possibilities with constant hands-on work, stress and chronic lack of sleep, as well as night shift work, frequent flights with a significant change in hourly flights and, of course, the use of psychoactive substances contribute to the development of the disease. Therefore, they should be avoided. Scientists have yet to learn about other factors.
But not boring?
The number of people suffering from bipolar disorder among the population, according to various estimates, varies from fractions of one percent to several percent.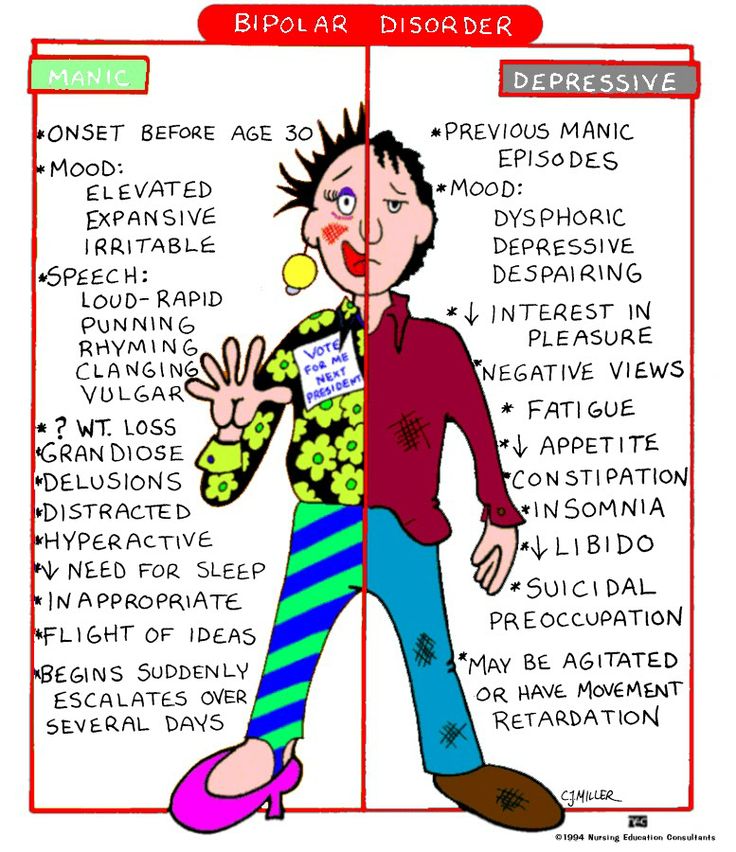 Recently, psychiatrists note, the proportion of affective disorders has increased significantly, which can be explained by improved diagnostics. At first glance, the BAR does not look like something scary and dangerous. To ignorant people, this disorder even seems attractive - sometimes sad, sometimes fun, in general, you won’t get bored. In addition, being different from everyone else is now fashionable. And then, there is an opinion that people with BAD have higher intelligence and creative abilities than the “gray masses”. But even if this is so, then none of those who suffer from it will definitely call BAD a pleasant thing. It is especially difficult for those patients who do not seek medical help on time. Without treatment, both phases of bipolar disorder can last for months (although sometimes the disorder occurs with frequently alternating phases). Moreover, it is impossible to say which of the periods of the disease is more difficult, manic or depressive.
Recently, psychiatrists note, the proportion of affective disorders has increased significantly, which can be explained by improved diagnostics. At first glance, the BAR does not look like something scary and dangerous. To ignorant people, this disorder even seems attractive - sometimes sad, sometimes fun, in general, you won’t get bored. In addition, being different from everyone else is now fashionable. And then, there is an opinion that people with BAD have higher intelligence and creative abilities than the “gray masses”. But even if this is so, then none of those who suffer from it will definitely call BAD a pleasant thing. It is especially difficult for those patients who do not seek medical help on time. Without treatment, both phases of bipolar disorder can last for months (although sometimes the disorder occurs with frequently alternating phases). Moreover, it is impossible to say which of the periods of the disease is more difficult, manic or depressive.
Bad when very bad
Those who have experienced real depression say that this is the worst thing that can happen in life.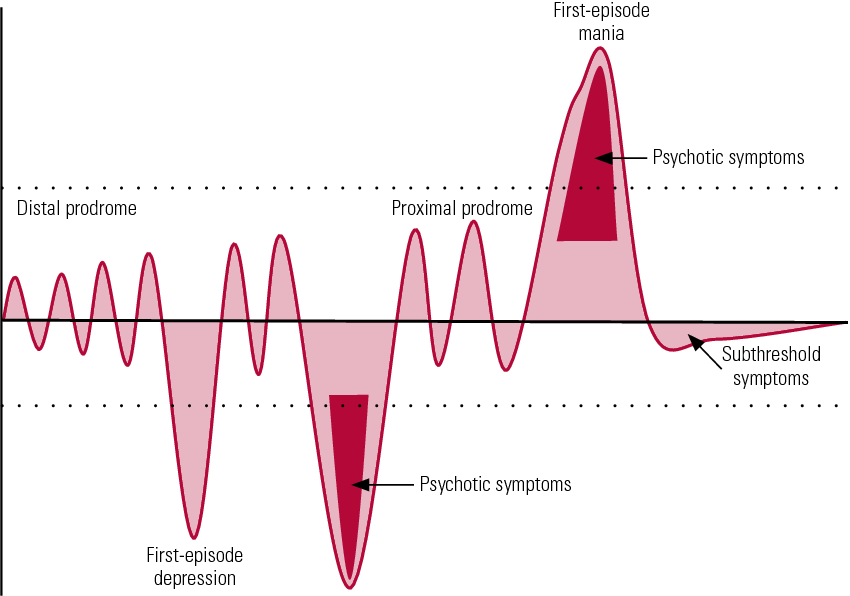 In this state, the whole world is seen in black, the mood is depressed, self-esteem drops, life loses its meaning. A person suffering from BAD in the depressive phase perceives his very existence as a chain of tragic mistakes, constantly blaming himself for all the troubles and sins, even those that do not even exist. In addition to mental suffering, physical ones also arise: a person even moves with difficulty, as if swimming against the current, it is difficult for him to perform the most familiar actions. In addition, he can feel tension throughout the body, experience various pain sensations. With an average degree of depression, people often complain of debilitating pain in the abdomen and other parts of the body. On this occasion, they turn to doctors, but the diagnosis cannot be made. And the daily pain continues to harass. Psychiatrists call this somatoform symptomatology. With severe depression, many have the so-called atrial depression. Patients complain of pain and heaviness in the chest, they say that "a stone lies on the heart.
In this state, the whole world is seen in black, the mood is depressed, self-esteem drops, life loses its meaning. A person suffering from BAD in the depressive phase perceives his very existence as a chain of tragic mistakes, constantly blaming himself for all the troubles and sins, even those that do not even exist. In addition to mental suffering, physical ones also arise: a person even moves with difficulty, as if swimming against the current, it is difficult for him to perform the most familiar actions. In addition, he can feel tension throughout the body, experience various pain sensations. With an average degree of depression, people often complain of debilitating pain in the abdomen and other parts of the body. On this occasion, they turn to doctors, but the diagnosis cannot be made. And the daily pain continues to harass. Psychiatrists call this somatoform symptomatology. With severe depression, many have the so-called atrial depression. Patients complain of pain and heaviness in the chest, they say that "a stone lies on the heart. " But even an in-depth examination does not reveal cardiac causes.
" But even an in-depth examination does not reveal cardiac causes.
Often, with depression, patients (especially the elderly) complain of difficulty in thinking, memory impairment, they say that they have become stupid, they believe that they are developing dementia, they are afraid of “losing their mind”. In fact, affective disorders do not destroy the intellect. When treated with antidepressants, when the mood stabilizes, abilities are restored.
But the worst consequence of depression is suicide. Most suicide attempts are made in this state. Sometimes people in a very pronounced depression, believing that they have done something irreparable, and believing that the consequences of their actions can harm loved ones, decide on extended suicides, in which they settle scores not only with their lives, but also take their loved ones with them ( more often children).
Too bad when too good
The manic stage of BAD is subjectively more pleasant. Patients are not just in a very good, but in a great mood: they love the whole world and themselves in it. The reflection in the mirror pleases, there is not the slightest doubt about one’s own talents and mind, there is more than enough strength and energy, a bonus is accelerated mental activity. Many in this stage sleep for an hour a day, but do not experience fatigue. Sometimes they don’t sleep for whole days - and at least they are cheerful, like an “energizer”. It seems to be great. But no. With mania, desires and new ideas arise too quickly, so a person grabs at each new business, but, as a rule, does not bring any to the end. So productivity at this stage is no more than during depression. But it would be nice if that was the only thing.
The reflection in the mirror pleases, there is not the slightest doubt about one’s own talents and mind, there is more than enough strength and energy, a bonus is accelerated mental activity. Many in this stage sleep for an hour a day, but do not experience fatigue. Sometimes they don’t sleep for whole days - and at least they are cheerful, like an “energizer”. It seems to be great. But no. With mania, desires and new ideas arise too quickly, so a person grabs at each new business, but, as a rule, does not bring any to the end. So productivity at this stage is no more than during depression. But it would be nice if that was the only thing.
The main danger of mania is that a person has no criticism at this moment, and he can do things that he will later regret very much. For example, he can give away all his property to others (sometimes to unfamiliar people or scammers who specifically use this state of his). Or, say, take out loans to go on a trip to the other side of the world, and take a bunch of friends with him.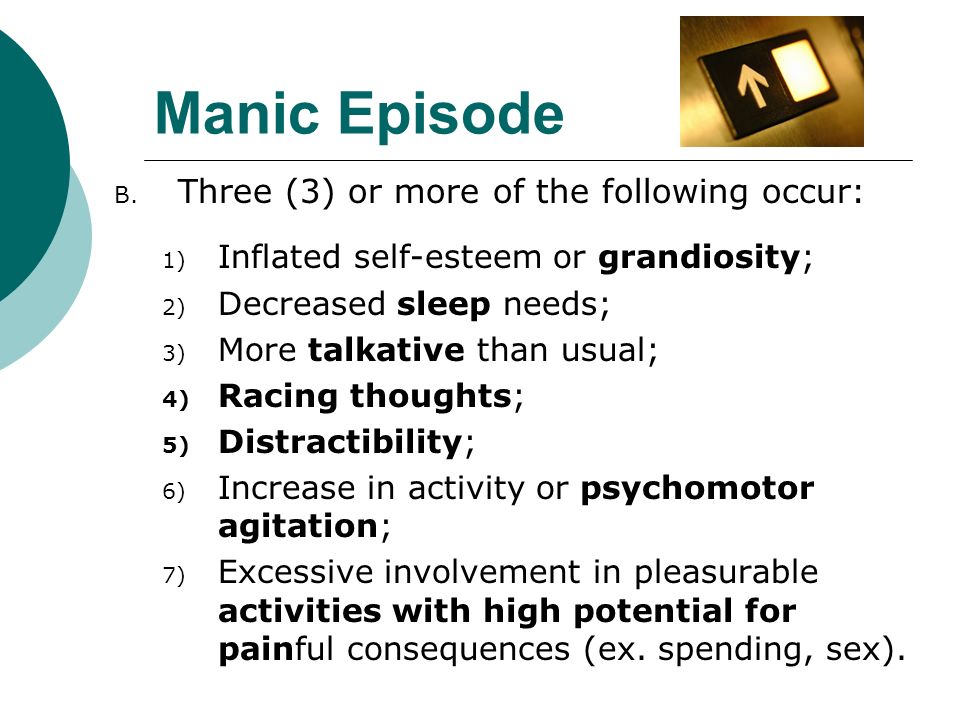 Maybe even steal something - for example, to make an expensive gift. Many patients at these moments enter into hasty intimate relationships, mistaking a chance meeting for the love of their life (and completely “forgetting” that family and children are waiting at home). Finally, often with mania, people, experiencing euphoria, ignore their severe somatic symptoms, as a result, they do not go to the doctor for a long time, and thus trigger a serious illness (pneumonia, for example). In addition, not all patients in the manic phase are "darlings." Often they show unreasonable aggression if, for example, others do not agree with their "brilliant" advice. As a result of such “angry mania”, conflicts and even situations arise that require the intervention of law enforcement agencies and the hospitalization of the patient without his consent in a psychiatric hospital.
Maybe even steal something - for example, to make an expensive gift. Many patients at these moments enter into hasty intimate relationships, mistaking a chance meeting for the love of their life (and completely “forgetting” that family and children are waiting at home). Finally, often with mania, people, experiencing euphoria, ignore their severe somatic symptoms, as a result, they do not go to the doctor for a long time, and thus trigger a serious illness (pneumonia, for example). In addition, not all patients in the manic phase are "darlings." Often they show unreasonable aggression if, for example, others do not agree with their "brilliant" advice. As a result of such “angry mania”, conflicts and even situations arise that require the intervention of law enforcement agencies and the hospitalization of the patient without his consent in a psychiatric hospital.
Good intentions…
The worst thing that relatives and friends of a person with bipolar disorder can do is ignore his problem, devalue suffering, while blaming the patient himself and appealing to his conscience. For example, they can call on a depressed person to “pull himself together, not become limp”, say that he is “mad with fat”, etc. A patient at the stage of mania is most often accused of immorality, irresponsibility, frivolity, promiscuity in relationships, etc. However, doing so is like blaming a person with diabetes for not being able to eat sweet cake, or a patient with heart failure for not running a marathon. BAD is a disease like many others. And she needs to be treated. The sooner you start the right therapy, the sooner you can stabilize the patient's condition and the better the further prognosis will be.
For example, they can call on a depressed person to “pull himself together, not become limp”, say that he is “mad with fat”, etc. A patient at the stage of mania is most often accused of immorality, irresponsibility, frivolity, promiscuity in relationships, etc. However, doing so is like blaming a person with diabetes for not being able to eat sweet cake, or a patient with heart failure for not running a marathon. BAD is a disease like many others. And she needs to be treated. The sooner you start the right therapy, the sooner you can stabilize the patient's condition and the better the further prognosis will be.
Psychiatrists don't bite
Despite the fact that recently people (especially young people) have ceased to be afraid to turn to psychiatrists, not everyone still decides to go to the doctor. Indeed, on the Internet in the public domain, you can find hundreds of questionnaires to test yourself for any mental disorder. And then, after reading various tips, you can also “cure”. Doctors strongly advise against doing this. The smallest harm of self-treatment is that it will not help or lead to incomplete improvement, but it can also worsen the condition. For example, inadequate intake of antidepressants in bipolar disorder can lead from a depressive phase into a severe manic state, from which it will then be difficult to get out. Only a psychiatrist (and not a psychologist, neurologist or doctor of any other somatic profile) can identify bipolar disorder and choose the right treatment. Treatment should be strictly individual, that is, the doctor selects it based on the characteristics of a particular patient and taking into account a specific moment in the course of the disease. The goal of therapy is not only to equalize the patient's mood, but also to prevent recurrence. In the treatment of bipolar disorder, the main role is played by drugs for stabilizing mood - mood stabilizers (lithium salts, some anticonvulsants (anticonvulsants) and antipsychotics of new generations).
Doctors strongly advise against doing this. The smallest harm of self-treatment is that it will not help or lead to incomplete improvement, but it can also worsen the condition. For example, inadequate intake of antidepressants in bipolar disorder can lead from a depressive phase into a severe manic state, from which it will then be difficult to get out. Only a psychiatrist (and not a psychologist, neurologist or doctor of any other somatic profile) can identify bipolar disorder and choose the right treatment. Treatment should be strictly individual, that is, the doctor selects it based on the characteristics of a particular patient and taking into account a specific moment in the course of the disease. The goal of therapy is not only to equalize the patient's mood, but also to prevent recurrence. In the treatment of bipolar disorder, the main role is played by drugs for stabilizing mood - mood stabilizers (lithium salts, some anticonvulsants (anticonvulsants) and antipsychotics of new generations). Modern drugs are much better tolerated than their predecessors, have fewer side effects, as they are designed for long-term use over many years. Against the background of their intake, women can even become pregnant and give birth. In depression, antidepressants are prescribed in exceptional cases, given the danger of changing the depressive stage to manic.
Modern drugs are much better tolerated than their predecessors, have fewer side effects, as they are designed for long-term use over many years. Against the background of their intake, women can even become pregnant and give birth. In depression, antidepressants are prescribed in exceptional cases, given the danger of changing the depressive stage to manic.
You won't be able to forget
The insidiousness of BAD is that this disease cannot be cured once and for all. But, alas, often, when the patient's mood can be balanced by medication and he begins to feel good (such a state - intermission - is completely indistinguishable from a state of complete health), he can stop taking the drugs. This is a big mistake that does not allow to achieve a stable result of treatment. Sometimes it is required to use medicines (necessarily under the supervision of a doctor) for several months, but more often for years (with periodic visits to the doctor). It is the long-term use of maintenance therapy individually selected by the doctor that allows patients to achieve a stable good condition and feel the joy of life for many years.