Fever stress induced
Psychogenic fever: how psychological stress affects body temperature in the clinical population
1. Bakwin H. Emotional deprivation in infants. J Pediatr 1949; 35:512-21; PMID:18143946; http://dx.doi.org/ 10.1016/S0022-3476(49)80071-0 [PubMed] [CrossRef] [Google Scholar]
2. White KL, Long WN Jr. The incidence of psychogenic fever in a university hospital. J Chronic Dis 1958; 8:567-86; PMID:13587612; http://dx.doi.org/ 10.1016/0021-9681(58)90050-X [PubMed] [CrossRef] [Google Scholar]
3. Meyer R, Beck D. Psychodynamics of psychogenic fever. Zeitschrift fur Psychosomatische Medizin und Psychoanalyse 1976; 22:169-70; PMID:941539 [PubMed] [Google Scholar]
4. Malleson N. Panic and phobia; a possible method of treatment. Lancet 1959; 1:225-7; PMID:13631975; http://dx.doi.org/ 10.1016/S0140-6736(59)90052-2 [PubMed] [CrossRef] [Google Scholar]
5. O'Toole JK, Dyck G. Report of psychogenic fever in catatonia responding to electroconvulsive therapy. Dis Nerv Syst 1977; 38:852-3; PMID:908250 [PubMed] [Google Scholar]
6. McNeil GN, Leighton LH, Elkins AM. Possible psychogenic fever of 103.5 degrees F in a patient with borderline personality disorder. Am J Psychiatry 1984; 141:896-7; PMID:6731643; http://dx.doi.org/ 10.1176/ajp.141.7.896 [PubMed] [CrossRef] [Google Scholar]
7. Weinstein L. Clinically benign fever of unknown origin: a personal retrospective. Rev Infect Dis 1985; 7:692-9; PMID:4059757; http://dx.doi.org/ 10.1093/clinids/7.5.692 [PubMed] [CrossRef] [Google Scholar]
8. Timmerman RJ, Thompson J, Noordzij HM, van der Meer JW. Psychogenic periodic fever. Neth J Med 1992; 41:158-60; PMID:1470287 [PubMed] [Google Scholar]
9. Miric D, Venet R, Aproh E, Nguyen-Duc H. Psychogenic fever or psychogenic hyperthermia? J Am Geriatr Soc 1997; 45:1287-8; PMID:9329503; http://dx.doi.org/ 10.1111/j.1532-5415.1997.tb03796.x [PubMed] [CrossRef] [Google Scholar]
10. Araki T, Oka T, Oyama N, Akamine M, Kubo C. A case of psychogenic fever treated successfully with art therapy. Jpn J Psychosom Med 2004; 44:289-94 [Google Scholar]
11. Nozu T, Uehara A. The diagnoses and outcomes of patients complaining of fever without any abnormal findings on diagnostic tests. Intern Med 2005; 44:901-2; PMID:16157998; http://dx.doi.org/ 10.2169/internalmedicine.44.901 [PubMed] [CrossRef] [Google Scholar]
Nozu T, Uehara A. The diagnoses and outcomes of patients complaining of fever without any abnormal findings on diagnostic tests. Intern Med 2005; 44:901-2; PMID:16157998; http://dx.doi.org/ 10.2169/internalmedicine.44.901 [PubMed] [CrossRef] [Google Scholar]
12. Kura N, Oka T, Ando T, Ishikawa T, Kubo C, Ago Y. A case of psychogenic fever treated successfully with tandospirone in combination with psychotherapy and autogenic training. Jpn J Psychosom Med 2004; 44:297-303 [Google Scholar]
13. Hiramoto T, Oka T, Yoshihara K, Kubo C. Pyrogenic cytokines did not mediate a stress interview-induced hyperthermic response in a patient with psychogenic fever: a case report. Psychosom Med 2009; 71:932-6; PMID:19875636; http://dx.doi.org/ 10.1097/PSY.0b013e3181bfb02b [PubMed] [CrossRef] [Google Scholar]
14. Oka T, Kanemitsu Y, Sudo N, Hayashi H, Oka K. Psychological stress contributed to the development of low-grade fever in a patient with chronic fatigue syndrome: a case report. Biopsychosoc Med 2013; 7:7; PMID:23497734; http://dx.doi.org/ 10.1186/1751-0759-7-7 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
Biopsychosoc Med 2013; 7:7; PMID:23497734; http://dx.doi.org/ 10.1186/1751-0759-7-7 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
15. Oka T, Oka K. Age and gender differences of psychogenic fever: a review of the Japanese literature. Biopsychosoc Med 2007; 1:11; PMID:17511878; http://dx.doi.org/ 10.1186/1751-0759-1-11 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
16. Kaneda Y, Tsuji S, Oka T. Age distribution and gender differences in psychogenic fever patients. Biopsychosoc Med 2009; 3:6; PMID:19379524; http://dx.doi.org/ 10.1186/1751-0759-3-6 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
17. Friedmann M, Kohnstmann O. Zur Pathogenese und Psychotherapie bei Basodowsher Krankheit. Ztschr f d ges Neurol u Psychiat 1914; 23:357; http://dx.doi.org/ 10.1007/BF02867687 [CrossRef] [Google Scholar]
18. Falcon-Lesses M, Proger SH. Psychogenic fever. N Engl J Med 1930; 203:1034-6; http://dx.doi.org/ 10.1056/NEJM193011202032113 [CrossRef] [Google Scholar]
19. Bakwin H. Psychogenic fever in infants. Am J Dis Child 1944; 67:176-81 [Google Scholar]
Bakwin H. Psychogenic fever in infants. Am J Dis Child 1944; 67:176-81 [Google Scholar]
20. Kintner AR, Rowntree LG. Long continued, low grade, idiopathic fever. JAMA 1934;102:889-92; http://dx.doi.org/ 10.1001/jama.1934.02750120001001 [CrossRef] [Google Scholar]
21. Wolf S, Wolf HD. Intermittent fever of unknown origin. Arch Internal Med 1942;70:293-302; http://dx.doi.org/ 10.1001/archinte.1942.00200200113007 [CrossRef] [Google Scholar]
22. Singer R, Harker CT, Vander AJ, Kluger MJ. Hyperthermia induced by open-field stress is blocked by salicylate. Physiol Behav 1986; 36:1179-82; PMID:3725924; http://dx.doi.org/ 10.1016/0031-9384(86)90497-X [PubMed] [CrossRef] [Google Scholar]
23. Soszynski D, Kozak W, Kluger MJ. Endotoxin tolerance does not alter open field-induced fever in rats. Physiol Behav 1998; 63:689-92; PMID:9523916; http://dx.doi.org/ 10.1016/S0031-9384(97)00515-5 [PubMed] [CrossRef] [Google Scholar]
24. Butterweck V, Prinz S, Schwaninger M. The role of interleukin-6 in stress-induced hyperthermia and emotional behaviour in mice. Behav Brain Res 2003; 144:49-56; PMID:12946594; http://dx.doi.org/ 10.1016/S0166-4328(03)00059-7 [PubMed] [CrossRef] [Google Scholar]
Behav Brain Res 2003; 144:49-56; PMID:12946594; http://dx.doi.org/ 10.1016/S0166-4328(03)00059-7 [PubMed] [CrossRef] [Google Scholar]
25. Long NC, Vander AJ, Kunkel SL, Kluger MJ. Antiserum against tumor necrosis factor increases stress hyperthermia in rats. Am J Physiol 1990; 258:R591-5; PMID:2316707 [PubMed] [Google Scholar]
26. Morimoto A, Nakamori T, Morimoto K, Tan N, Murakami N. The central role of corticotrophin-releasing factor (CRF-41) in psychological stress in rats. J Physiol 1993; 460:221-9; PMID:8487193; http://dx.doi.org/ 10.1113/jphysiol.1993.sp019468 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
27. Oka T, Oka K, Kobayashi T, Sugimoto Y, Ichikawa A, Ushikubi F, Narumiya S, Saper CB. Characteristics of thermoregulatory and febrile responses in mice deficient in prostaglandin EP1 and EP3 receptors. J Physiol 2003; 551:945-54; PMID:12837930; http://dx.doi.org/ 10.1113/jphysiol.2003.048140 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
28. Shibata H, Nagasaka T. Contribution of nonshivering thermogenesis to stress-induced hyperthermia in rats. Jpn J Physiol 1982; 32:991-5; PMID:7169705; http://dx.doi.org/ 10.2170/jjphysiol.32.991 [PubMed] [CrossRef] [Google Scholar]
Shibata H, Nagasaka T. Contribution of nonshivering thermogenesis to stress-induced hyperthermia in rats. Jpn J Physiol 1982; 32:991-5; PMID:7169705; http://dx.doi.org/ 10.2170/jjphysiol.32.991 [PubMed] [CrossRef] [Google Scholar]
29. Shibata H, Nagasaka T. Role of sympathetic nervous system in immobilization- and cold-induced brown adipose tissue thermogenesis in rats. Jpn J Physiol 1984; 34:103-11; PMID:6727066; http://dx.doi.org/ 10.2170/jjphysiol.34.103 [PubMed] [CrossRef] [Google Scholar]
30. Gao B, Kikuchi-Utsumi K, Ohinata H, Hashimoto M, Kuroshima A. Repeated immobilization stress increases uncoupling protein 1 expression and activity in Wistar rats. Jpn J Physiol 2003; 53:205-13; PMID:14529581; http://dx.doi.org/ 10.2170/jjphysiol.53.205 [PubMed] [CrossRef] [Google Scholar]
31. Ootsuka Y, Blessing WW, Nalivaiko E. Selective blockade of 5-HT2A receptors attenuates the increased temperature response in brown adipose tissue to restraint stress in rats. Stress 2008; 11:125-33; PMID:18311601; http://dx. doi.org/ 10.1080/10253890701638303 [PubMed] [CrossRef] [Google Scholar]
doi.org/ 10.1080/10253890701638303 [PubMed] [CrossRef] [Google Scholar]
32. Borsini F, Lecci A, Volterra G, Meli A. A model to measure anticipatory anxiety in mice? Psychopharmacology (Berl) 1989; 98:207-11; PMID:2502791; http://dx.doi.org/ 10.1007/BF00444693 [PubMed] [CrossRef] [Google Scholar]
33. Zethof TJ, Van der Heyden JA, Tolboom JT, Olivier B. Stress-induced hyperthermia as a putative anxiety model. Eur J Pharmacol 1995; 294:125-35; PMID:8788424; http://dx.doi.org/ 10.1016/0014-2999(95)00520-X [PubMed] [CrossRef] [Google Scholar]
34. Vinkers CH, van Bogaert MJ, Klanker M, Korte SM, Oosting R, Hanania T, Hopkins SC, Olivier B, Groenink L. Translational aspects of pharmacological research into anxiety disorders: the stress-induced hyperthermia (SIH) paradigm. Eur J Pharmacol 2008; 585:407-25; PMID:18420191; http://dx.doi.org/ 10.1016/j.ejphar.2008.02.097 [PubMed] [CrossRef] [Google Scholar]
35. Beig MI, Baumert M, Walker FR, Day TA, Nalivaiko E. Blockade of 5-HT2A receptors suppresses hyperthermic but not cardiovascular responses to psychosocial stress in rats. Neuroscience 2009;159: 1185-91; PMID:19356699; http://dx.doi.org/ 10.1016/j.neuroscience.2009.01.038 [PubMed] [CrossRef] [Google Scholar]
Neuroscience 2009;159: 1185-91; PMID:19356699; http://dx.doi.org/ 10.1016/j.neuroscience.2009.01.038 [PubMed] [CrossRef] [Google Scholar]
36. Hayashida S, Oka T, Mera T, Tsuji S. Repeated social defeat stress induces chronic hyperthermia in rats. Physiol Behav 2010; 101:124-31; PMID:20438740; http://dx.doi.org/ 10.1016/j.physbeh.2010.04.027 [PubMed] [CrossRef] [Google Scholar]
37. Lkhagvasuren B, Nakamura Y, Oka T, Sudo N, Nakamura K. Social defeat stress induces hyperthermia through activation of thermoregulatory sympathetic premotor neurons in the medullary raphe region. Eur J Neurosci 2011; 34:1442-52; PMID:21978215; http://dx.doi.org/ 10.1111/j.1460-9568.2011.07863.x [PubMed] [CrossRef] [Google Scholar]
38. Lkhagvasuren B, Oka T, Nakamura Y, Hayashi H, Sudo N, Nakamura K. Distribution of Fos-immunoreactive cells in rat forebrain and midbrain following social defeat stress and diazepam treatment. Neuroscience 2014; 272:34-57; PMID:24797330; http://dx.doi.org/ 10.1016/j. neuroscience.2014.04.047 [PubMed] [CrossRef] [Google Scholar]
neuroscience.2014.04.047 [PubMed] [CrossRef] [Google Scholar]
39. Mohammed M, Ootsuka Y, Blessing W. Brown adipose tissue thermogenesis contributes to emotional hyperthermia in a resident rat suddenly confronted with an intruder rat. Am J Physiol Regul Integr Comp Physiol 2014; 306:R394-400; PMID:24452545; http://dx.doi.org/ 10.1152/ajpregu.00475.2013 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
40. Yokoi Y. Effect of ambient temperature upon emotional hyperthermia and hypothermia in rabbits. J Appl Physiol 1966; 21:1795-8; PMID:5929304 [PubMed] [Google Scholar]
41. Snow AE, Horita A. Interaction of apomorphine and stressors in the production of hyperthermia in the rabbit. J Pharmacol Exp Ther 1982; 220:335-9; PMID:7199085 [PubMed] [Google Scholar]
42. Kohlhause S, Hoffmann K, Schlumbohm C, Fuchs E, Flugge G. Nocturnal hyperthermia induced by social stress in male tree shrews: relation to low testosterone and effects of age. Physiol Behav 2011; 104:786-95; PMID:21827778; http://dx. doi.org/ 10.1016/j.physbeh.2011.07.023 [PubMed] [CrossRef] [Google Scholar]
doi.org/ 10.1016/j.physbeh.2011.07.023 [PubMed] [CrossRef] [Google Scholar]
43. Schmelting B, Corbach-Sohle S, Kohlhause S, Schlumbohm C, Flugge G, Fuchs E. Agomelatine in the tree shrew model of depression: effects on stress-induced nocturnal hyperthermia and hormonal status. Eur Neuropsychopharmacol 2014; 24:437-47; PMID:23978391; http://dx.doi.org/ 10.1016/j.euroneuro.2013.07.010 [PubMed] [CrossRef] [Google Scholar]
44. Pedernera-Romano C, Ruiz de la Torre JL, Badiella L, Manteca X. Effect of perphenazine enanthate on open-field test behaviour and stress-induced hyperthermia in domestic sheep. Pharmacol Biochem Behav 2010; 94:329-32; PMID:19799930; http://dx.doi.org/ 10.1016/j.pbb.2009.09.013 [PubMed] [CrossRef] [Google Scholar]
45. Muchlinski AE, Baldwin BC, Padick DA, Lee BY, Salguero HS, Gramajo R. California ground squirrel body temperature regulation patterns measured in the laboratory and in the natural environment. Comp Biochem Physiol A Mol Integr Physiol 1998; 120:365-72; PMID:9773514; http://dx. doi.org/ 10.1016/S1095-6433(98)10037-5 [PubMed] [CrossRef] [Google Scholar]
doi.org/ 10.1016/S1095-6433(98)10037-5 [PubMed] [CrossRef] [Google Scholar]
46. Lee BY, Padick DA, Muchlinski AE. Stress fever magnitude in laboratory-maintained California ground squirrels varies with season. Comp Biochem Physiol A Mol Integr Physiol 2000; 125:325-30; PMID:10794961; http://dx.doi.org/ 10.1016/S1095-6433(00)00157-4 [PubMed] [CrossRef] [Google Scholar]
47. Parr LA, Hopkins WD. Brain temperature asymmetries and emotional perception in chimpanzees, Pan troglodytes. Physiol Behav 2000; 71:363-71; PMID:11150569; http://dx.doi.org/ 10.1016/S0031-9384(00)00349-8 [PubMed] [CrossRef] [Google Scholar]
48. Meyer LC, Fick L, Matthee A, Mitchell D, Fuller A. Hyperthermia in captured impala (Aepyceros melampus): a fright not flight response. J Wildl Dis 2008; 44:404-16; PMID:18436672; http://dx.doi.org/ 10.7589/0090-3558-44.2.404 [PubMed] [CrossRef] [Google Scholar]
49. Gray DA, Maloney SK, Kamerman PR. Restraint increases afebrile body temperature but attenuates fever in Pekin ducks (Anas platyrhynchos). Am J Physiol Regul Integr Comp Physiol 2008; 294:R1666-71; PMID:18337310; http://dx.doi.org/ 10.1152/ajpregu.00865.2007 [PubMed] [CrossRef] [Google Scholar]
Am J Physiol Regul Integr Comp Physiol 2008; 294:R1666-71; PMID:18337310; http://dx.doi.org/ 10.1152/ajpregu.00865.2007 [PubMed] [CrossRef] [Google Scholar]
50. Bittencourt Mde A, Melleu FF, Marino-Neto J. Stress-induced core temperature changes in pigeons (Columba livia). Physiol Behav 2015; 139:449-58; PMID:25479572; http://dx.doi.org/ 10.1016/j.physbeh.2014.11.067 [PubMed] [CrossRef] [Google Scholar]
51. Oka T, Oka K, Hori T. Mechanisms and mediators of psychological stress-induced rise in core temperature. Psychosom Med 2001; 63:476-86; PMID:11382276; http://dx.doi.org/ 10.1097/00006842-200105000-00018 [PubMed] [CrossRef] [Google Scholar]
52. Vinkers CH, Groenink L, van Bogaert MJ, Westphal KG, Kalkman CJ, van Oorschot R, Oosting RS, Olivier B, Korte SM. Stress-induced hyperthermia and infection-induced fever: two of a kind? Physiol Behav 2009; 98:37-43; PMID:19375439; http://dx.doi.org/ 10.1016/j.physbeh.2009.04.004 [PubMed] [CrossRef] [Google Scholar]
53. Ivanov AI, Pero RS, Scheck AC, Romanovsky AA. Prostaglandin E(2)-synthesizing enzymes in fever: differential transcriptional regulation. Am J Physiol Regul Integr Comp Physiol 2002; 283:R1104-17; PMID:12376404; http://dx.doi.org/ 10.1152/ajpregu.00347.2002 [PubMed] [CrossRef] [Google Scholar]
Prostaglandin E(2)-synthesizing enzymes in fever: differential transcriptional regulation. Am J Physiol Regul Integr Comp Physiol 2002; 283:R1104-17; PMID:12376404; http://dx.doi.org/ 10.1152/ajpregu.00347.2002 [PubMed] [CrossRef] [Google Scholar]
54. Ivanov AI, Romanovsky AA. Prostaglandin E2 as a mediator of fever: synthesis and catabolism. Front Biosci 2004; 9:1977-93; PMID:14977603; http://dx.doi.org/ 10.2741/1383 [PubMed] [CrossRef] [Google Scholar]
55. Steiner AA, Ivanov AI, Serrats J, Hosokawa H, Phayre AN, Robbins JR, Roberts JL, Kobayashi S, Matsumura K, Sawchenko PE, et al.. Cellular and molecular bases of the initiation of fever. PLoS Biol 2006; 4:e284; PMID:16933973; http://dx.doi.org/ 10.1371/journal.pbio.0040284 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
56. Romanovsky AA, Steiner AA, Matsumura K. Cells that trigger fever. Cell Cycle 2006; 5:2195-7; PMID:16969135; http://dx.doi.org/ 10.4161/cc.5.19.3321 [PubMed] [CrossRef] [Google Scholar]
57. Yamagata K, Matsumura K, Inoue W, Shiraki T, Suzuki K, Yasuda S, Sugiura H, Cao C, Watanabe Y, Kobayashi S. Coexpression of microsomal-type prostaglandin E synthase with cyclooxygenase-2 in brain endothelial cells of rats during endotoxin-induced fever. J Neurosci 2001; 21:2669-77; PMID:11306620 [PMC free article] [PubMed] [Google Scholar]
Yamagata K, Matsumura K, Inoue W, Shiraki T, Suzuki K, Yasuda S, Sugiura H, Cao C, Watanabe Y, Kobayashi S. Coexpression of microsomal-type prostaglandin E synthase with cyclooxygenase-2 in brain endothelial cells of rats during endotoxin-induced fever. J Neurosci 2001; 21:2669-77; PMID:11306620 [PMC free article] [PubMed] [Google Scholar]
58. Engblom D, Saha S, Engstrom L, Westman M, Audoly LP, Jakobsson PJ, Blomqvist A. Microsomal prostaglandin E synthase-1 is the central switch during immune-induced pyresis. Nat Neurosci 2003; 6:1137-8; PMID:14566340; http://dx.doi.org/ 10.1038/nn1137 [PubMed] [CrossRef] [Google Scholar]
59. Schiltz JC, Sawchenko PE. Signaling the brain in systemic inflammation: the role of perivascular cells. Front Biosci 2003; 8:s1321-9; PMID:12957837; http://dx.doi.org/ 10.2741/1211 [PubMed] [CrossRef] [Google Scholar]
60. Kluger MJ. Fever: role of pyrogens and cryogens. Physiol Rev 1991; 71:93-127; PMID:1986393 [PMC free article] [PubMed] [Google Scholar]
61. Leon LR. Invited review: cytokine regulation of fever: studies using gene knockout mice. J Appl Physiol 2002; 92:2648-55; PMID:12015385; http://dx.doi.org/ 10.1152/japplphysiol.01005.2001 [PubMed] [CrossRef] [Google Scholar]
Leon LR. Invited review: cytokine regulation of fever: studies using gene knockout mice. J Appl Physiol 2002; 92:2648-55; PMID:12015385; http://dx.doi.org/ 10.1152/japplphysiol.01005.2001 [PubMed] [CrossRef] [Google Scholar]
62. Nakamura K, Matsumura K, Hubschle T, Nakamura Y, Hioki H, Fujiyama F, Boldogkoi Z, Konig M, Thiel HJ, Gerstberger R, et al.. Identification of sympathetic premotor neurons in medullary raphe regions mediating fever and other thermoregulatory functions. J Neurosci 2004; 24:5370-80; PMID:15190110; http://dx.doi.org/ 10.1523/JNEUROSCI.1219-04.2004 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
63. Rathner JA, Madden CJ, Morrison SF. Central pathway for spontaneous and prostaglandin E2-evoked cutaneous vasoconstriction. Am J Physiol Regul Integr Comp Physiol 2008; 295:R343-54; PMID:18463193; http://dx.doi.org/ 10.1152/ajpregu.00115.2008 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
64. Kerman IA, Enquist LW, Watson SJ, Yates BJ. Brainstem substrates of sympatho-motor circuitry identified using trans-synaptic tracing with pseudorabies virus recombinants. J Neurosci 2003; 23:4657-66; PMID:12805305 [PMC free article] [PubMed] [Google Scholar]
Brainstem substrates of sympatho-motor circuitry identified using trans-synaptic tracing with pseudorabies virus recombinants. J Neurosci 2003; 23:4657-66; PMID:12805305 [PMC free article] [PubMed] [Google Scholar]
65. Tanaka M, Owens NC, Nagashima K, Kanosue K, McAllen RM. Reflex activation of rat fusimotor neurons by body surface cooling, and its dependence on the medullary raphe. J Physiol 2006; 572:569-83; PMID:16484305; http://dx.doi.org/ 10.1113/jphysiol.2005.102400 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
66. Nakamura K, Morrison SF. Central efferent pathways for cold-defensive and febrile shivering. J Physiol 2011; 589:3641-58; PMID:21610139; http://dx.doi.org/ 10.1113/jphysiol.2011.210047 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
67. Nakamura K, Matsumura K, Kaneko T, Kobayashi S, Katoh H, Negishi M. The rostral raphe pallidus nucleus mediates pyrogenic transmission from the preoptic area. J Neurosci 2002; 22:4600-10; PMID:12040067 [PMC free article] [PubMed] [Google Scholar]
68. Lazarus M, Yoshida K, Coppari R, Bass CE, Mochizuki T, Lowell BB, Saper CB. EP3 prostaglandin receptors in the median preoptic nucleus are critical for fever responses. Nat Neurosci 2007; 10:1131-3; PMID:17676060; http://dx.doi.org/ 10.1038/nn1949 [PubMed] [CrossRef] [Google Scholar]
Lazarus M, Yoshida K, Coppari R, Bass CE, Mochizuki T, Lowell BB, Saper CB. EP3 prostaglandin receptors in the median preoptic nucleus are critical for fever responses. Nat Neurosci 2007; 10:1131-3; PMID:17676060; http://dx.doi.org/ 10.1038/nn1949 [PubMed] [CrossRef] [Google Scholar]
69. Morrison SF, Nakamura K. Central neural pathways for thermoregulation. Front Biosci 2011; 16:74-104; PMID:21196160; http://dx.doi.org/ 10.2741/3677 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
70. DiMicco JA, Sarkar S, Zaretskaia MV, Zaretsky DV. Stress-induced cardiac stimulation and fever: common hypothalamic origins and brainstem mechanisms. Auton Neurosci 2006; 126–127:106-19; PMID:16580890; http://dx.doi.org/ 10.1016/j.autneu.2006.02.010 [PubMed] [CrossRef] [Google Scholar]
71. Dimicco JA, Zaretsky DV. The dorsomedial hypothalamus: a new player in thermoregulation. Am J Physiol Regul Integr Comp Physiol 2007; 292:R47-63; PMID:16959861; http://dx.doi.org/ 10.1152/ajpregu. 00498.2006 [PubMed] [CrossRef] [Google Scholar]
00498.2006 [PubMed] [CrossRef] [Google Scholar]
72. Kataoka N, Hioki H, Kaneko T, Nakamura K. Psychological stress activates a dorsomedial hypothalamus-medullary raphe circuit driving brown adipose tissue thermogenesis and hyperthermia. Cell Metab 2014; 20:346-58; PMID:2498183715677520 [PubMed] [Google Scholar]
73. Saha S, Engstrom L, Mackerlova L, Jakobsson PJ, Blomqvist A. Impaired febrile responses to immune challenge in mice deficient in microsomal prostaglandin E synthase-1. Am J Physiol Regul Integr Comp Physiol 2005; 288:R1100-7; PMID:15677520; http://dx.doi.org/ 10.1152/ajpregu.00872.2004 [PubMed] [CrossRef] [Google Scholar]
74. Lecci A, Borsini F, Volterra G, Meli A. Pharmacological validation of a novel animal model of anticipatory anxiety in mice. Psychopharmacology (Berl) 1990; 101:255-61; PMID:1971957; http://dx.doi.org/ 10.1007/BF02244136 [PubMed] [CrossRef] [Google Scholar]
75. Bouwknecht JA, Hijzen TH, van der Gugten J, Maes RA, Olivier B. Stress-induced hyperthermia in mice: effects of flesinoxan on heart rate and body temperature. Eur J Pharmacol 2000; 400:59-66; PMID:10913585; http://dx.doi.org/ 10.1016/S0014-2999(00)00387-3 [PubMed] [CrossRef] [Google Scholar]
Eur J Pharmacol 2000; 400:59-66; PMID:10913585; http://dx.doi.org/ 10.1016/S0014-2999(00)00387-3 [PubMed] [CrossRef] [Google Scholar]
76. Olivier B, Bouwknecht JA, Pattij T, Leahy C, van Oorschot R, Zethof TJ. GABAA-benzodiazepine receptor complex ligands and stress-induced hyperthermia in singly housed mice. Pharmacol Biochem Behav 2002; 72:179-88; PMID:11900786; http://dx.doi.org/ 10.1016/S0091-3057(01)00759-6 [PubMed] [CrossRef] [Google Scholar]
77. Pecoraro N, de Jong H, Ginsberg AB, Dallman MF. Lesions of the medial prefrontal cortex enhance the early phase of psychogenic fever to unexpected sucrose concentration reductions, promote recovery from negative contrast and enhance spontaneous recovery of sucrose-entrained anticipatory activity. Neuroscience 2008; 153:901-17; PMID:18455879; http://dx.doi.org/ 10.1016/j.neuroscience.2008.03.043 [PubMed] [CrossRef] [Google Scholar]
78. Pae YS, Lai H, Horita A. Hyperthermia in the rat from handling stress blocked by naltrexone injected into the preoptic-anterior hypothalamus. Pharmacol Biochem Behav 1985; 22:337-9; PMID:4039067; http://dx.doi.org/ 10.1016/0091-3057(85)90400-9 [PubMed] [CrossRef] [Google Scholar]
Pharmacol Biochem Behav 1985; 22:337-9; PMID:4039067; http://dx.doi.org/ 10.1016/0091-3057(85)90400-9 [PubMed] [CrossRef] [Google Scholar]
79. Egawa M, Yoshimatsu H, Bray GA. Preoptic area injection of corticotropin-releasing hormone stimulates sympathetic activity. Am J Physiol 1990; 259:R799-806; PMID:2221147 [PubMed] [Google Scholar]
80. Vinkers CH, Bijlsma EY, Houtepen LC, Westphal KG, Veening JG, Groenink L, Olivier B. Medial amygdala lesions differentially influence stress responsivity and sensorimotor gating in rats. Physiol Behav 2010; 99:395-401; PMID:20006965; http://dx.doi.org/ 10.1016/j.physbeh.2009.12.006 [PubMed] [CrossRef] [Google Scholar]
81. Ootsuka Y, Mohammed M. Activation of the habenula complex evokes autonomic physiological responses similar to those associated with emotional stress. Physiol Rep 2015; 3:e12297; PMID:25677551; http://dx.doi.org/ 10.14814/phy2.12297 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
82. Zhang W, Sunanaga J, Takahashi Y, Mori T, Sakurai T, Kanmura Y, Kuwaki T.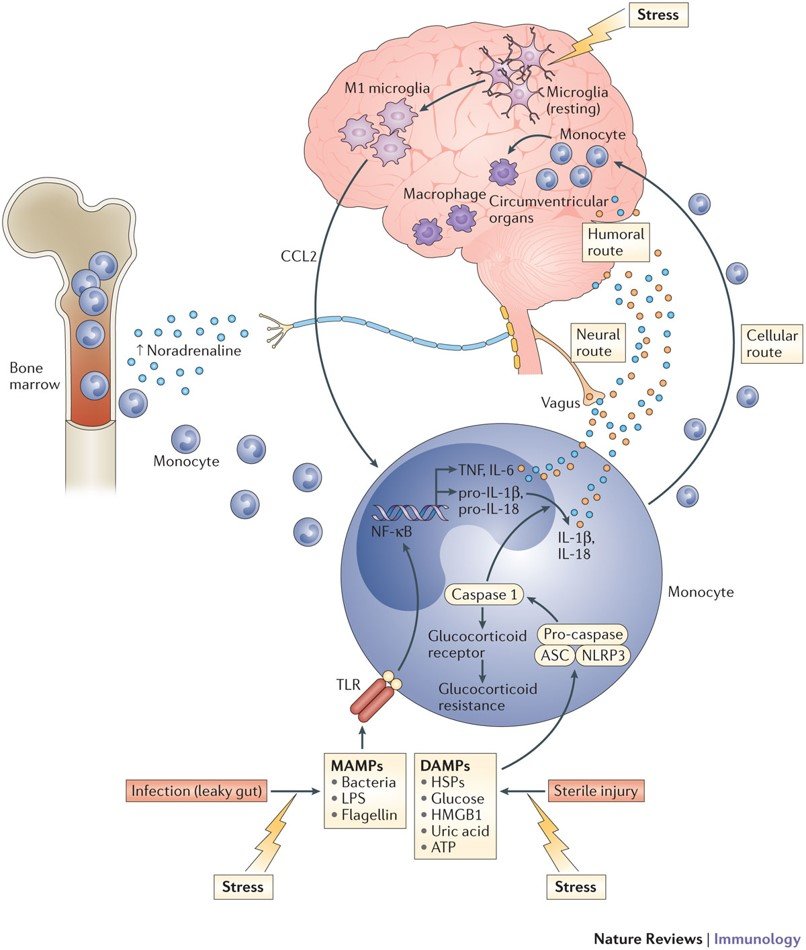 Orexin neurons are indispensable for stress-induced thermogenesis in mice. J Physiol 2010; 588:4117-29; PMID:20807795; http://dx.doi.org/ 10.1113/jphysiol.2010.195099 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
Orexin neurons are indispensable for stress-induced thermogenesis in mice. J Physiol 2010; 588:4117-29; PMID:20807795; http://dx.doi.org/ 10.1113/jphysiol.2010.195099 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
83. Eikelboom R. Learned anticipatory rise in body temperature due to handling. Physiol Behav 1986; 37:649-53; PMID:3749329; http://dx.doi.org/ 10.1016/0031-9384(86)90299-4 [PubMed] [CrossRef] [Google Scholar]
84. Pardon MC, Kendall DA, Perez-Diaz F, Duxon MS, Marsden CA. Repeated sensory contact with aggressive mice rapidly leads to an anticipatory increase in core body temperature and physical activity that precedes the onset of aversive responding. Eur J Neurosci 2004; 20:1033-50; PMID:15305872; http://dx.doi.org/ 10.1111/j.1460-9568.2004.03549.x [PubMed] [CrossRef] [Google Scholar]
85. Kant GJ, Bauman RA, Pastel RH, Myatt CA, Closser-Gomez E, D'Angelo CP. Effects of controllable vs. uncontrollable stress on circadian temperature rhythms. Physiol Behav 1991; 49:625-30; PMID:2062941; http://dx. doi.org/ 10.1016/0031-9384(91)90289-Z [PubMed] [CrossRef] [Google Scholar]
doi.org/ 10.1016/0031-9384(91)90289-Z [PubMed] [CrossRef] [Google Scholar]
86. Endo Y, Shiraki K. Behavior and body temperature in rats following chronic foot shock or psychological stress exposure. Physiol Behav 2000; 71:263-8; PMID:11150557; http://dx.doi.org/ 10.1016/S0031-9384(00)00339-5 [PubMed] [CrossRef] [Google Scholar]
87. Bhatnagar S, Vining C, Iyer V, Kinni V. Changes in hypothalamic-pituitary-adrenal function, body temperature, body weight and food intake with repeated social stress exposure in rats. J Neuroendocrinol 2006; 18:13-24; PMID:16451216; http://dx.doi.org/ 10.1111/j.1365-2826.2005.01375.x [PubMed] [CrossRef] [Google Scholar]
88. Nozu T, Okano S, Kikuchi K, Yahata T, Kuroshima A. Effect of immobilization stress on in vitro and in vivo thermogenesis of brown adipose tissue. Jpn J Physiol 1992; 42:299-308; PMID:1434095; http://dx.doi.org/ 10.2170/jjphysiol.42.299 [PubMed] [CrossRef] [Google Scholar]
89. Rygula R, Abumaria N, Havemann-Reinecke U, Ruther E, Hiemke C, Zernig G, Fuchs E, Flugge G. Pharmacological validation of a chronic social stress model of depression in rats: effects of reboxetine, haloperidol and diazepam. Behav Pharmacol 2008; 19:183-96; PMID:18469536; http://dx.doi.org/ 10.1097/FBP.0b013e3282fe8871 [PubMed] [CrossRef] [Google Scholar]
Pharmacological validation of a chronic social stress model of depression in rats: effects of reboxetine, haloperidol and diazepam. Behav Pharmacol 2008; 19:183-96; PMID:18469536; http://dx.doi.org/ 10.1097/FBP.0b013e3282fe8871 [PubMed] [CrossRef] [Google Scholar]
90. Marks A, Vianna DM, Carrive P. Nonshivering thermogenesis without interscapular brown adipose tissue involvement during conditioned fear in the rat. Am J Physiol Regul Integr Comp Physiol 2009; 296:R1239-47; PMID:19211724; http://dx.doi.org/ 10.1152/ajpregu.90723.2008 [PubMed] [CrossRef] [Google Scholar]
91. Carrive P, Gorissen M. Premotor sympathetic neurons of conditioned fear in the rat. Eur J Neurosci 2008; 28:428-46; PMID:18702716; http://dx.doi.org/ 10.1111/j.1460-9568.2008.06351.x [PubMed] [CrossRef] [Google Scholar]
92. Kuroshima A, Habara Y, Uehara A, Murazumi K, Yahata T, Ohno T. Cross adaption between stress and cold in rats. Pflugers Arch 1984; 402:402-8; PMID:6522247; http://dx.doi.org/ 10.1007/BF00583941 [PubMed] [CrossRef] [Google Scholar]
93. Kuroshima A, Yahata T. Changes in the colonic temperature and metabolism during immobilization stress in repetitively immobilized or cold-acclimated rats. Jpn J Physiol 1985; 35:591-7; PMID:4068366; http://dx.doi.org/ 10.2170/jjphysiol.35.591 [PubMed] [CrossRef] [Google Scholar]
Kuroshima A, Yahata T. Changes in the colonic temperature and metabolism during immobilization stress in repetitively immobilized or cold-acclimated rats. Jpn J Physiol 1985; 35:591-7; PMID:4068366; http://dx.doi.org/ 10.2170/jjphysiol.35.591 [PubMed] [CrossRef] [Google Scholar]
94. Sugama S, Fujita M, Hashimoto M, Conti B. Stress induced morphological microglial activation in the rodent brain: involvement of interleukin-18. Neuroscience 2007; 146:1388-99; PMID:17433555; http://dx.doi.org/ 10.1016/j.neuroscience.2007.02.043 [PubMed] [CrossRef] [Google Scholar]
95. Hinwood M, Morandini J, Day TA, Walker FR. Evidence that microglia mediate the neurobiological effects of chronic psychological stress on the medial prefrontal cortex. Cereb Cortex 2012; 22:1442-54; PMID:21878486; http://dx.doi.org/ 10.1093/cercor/bhr229 [PubMed] [CrossRef] [Google Scholar]
96. Hinwood M, Tynan RJ, Charnley JL, Beynon SB, Day TA, Walker FR. Chronic stress induced remodeling of the prefrontal cortex: structural re-organization of microglia and the inhibitory effect of minocycline. Cereb Cortex 2013; 23:1784-97; PMID:22710611; http://dx.doi.org/ 10.1093/cercor/bhs151 [PubMed] [CrossRef] [Google Scholar]
Cereb Cortex 2013; 23:1784-97; PMID:22710611; http://dx.doi.org/ 10.1093/cercor/bhs151 [PubMed] [CrossRef] [Google Scholar]
97. Johnson JD, Zimomra ZR, Stewart LT. Beta-adrenergic receptor activation primes microglia cytokine production. J Neuroimmunol 2013; 254:161-4; PMID:22944319; http://dx.doi.org/ 10.1016/j.jneuroim.2012.08.007 [PubMed] [CrossRef] [Google Scholar]
98. Oka T, Aou S, Hori T. Intracerebroventricular injection of interleukin-1 β induces hyperalgesia in rats. Brain Res 1993; 624:61-8; PMID:8252417; http://dx.doi.org/ 10.1016/0006-8993(93)90060-Z [PubMed] [CrossRef] [Google Scholar]
99. Oka T, Oka K, Hosoi M, Hori T. Intracerebroventricular injection of interleukin-6 induces thermal hyperalgesia in rats. Brain Res 1995; 692:123-8; PMID:8548295; http://dx.doi.org/ 10.1016/0006-8993(95)00691-I [PubMed] [CrossRef] [Google Scholar]
100. Raison CL, Capuron L, Miller AH. Cytokines sing the blues: inflammation and the pathogenesis of depression. Trends Immunol 2006; 27:24-31; PMID:16316783; http://dx.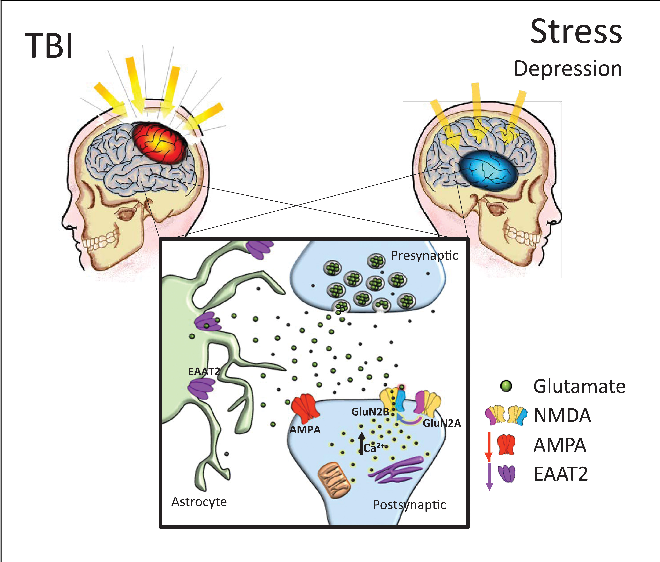 doi.org/ 10.1016/j.it.2005.11.006 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
doi.org/ 10.1016/j.it.2005.11.006 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
101. Song C, Wang H. Cytokines mediated inflammation and decreased neurogenesis in animal models of depression. Prog Neuropsychopharmacol Biol Psychiatry 2011; 35:760-8; PMID:20600462; http://dx.doi.org/ 10.1016/j.pnpbp.2010.06.020 [PubMed] [CrossRef] [Google Scholar]
102. Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry 2009; 65:732-41; PMID:19150053; http://dx.doi.org/ 10.1016/j.biopsych.2008.11.029 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
103. Wynn FR. The psychic factor as an element in temperature disturbance. JAMA 1919; 73:31-4; http://dx.doi.org/ 10.1001/jama.1919.02610270035010 [CrossRef] [Google Scholar]
104. Kleitman N. The effect of motion pictures on body temperature. Science 1945; 102:430-1; PMID:17730629; http://dx.doi.org/ 10.1126/science.102.2652. 430 [PubMed] [CrossRef] [Google Scholar]
430 [PubMed] [CrossRef] [Google Scholar]
105. Gotsev T, Ivanov A. Psychogenic elevation of body temperature in healthy persons. Acta Physiol Hung 1950; 1:53-62; PMID:14782995 [PubMed] [Google Scholar]
106. Aschoff J, Fatranska M, Gerecke U, Giedke H. Twenty-four-hour rhythms of rectal temperature in humans: effects of sleep-interruptions and of test-sessions. Pflugers Arch 1974; 346:215-22; PMID:4856415; http://dx.doi.org/ 10.1007/BF00595708 [PubMed] [CrossRef] [Google Scholar]
107. Renbourn ET. Body temperature and pulse rate in boys and young men prior to sporting contests. A study of emotional hyperthermia: with a review of the literature. J Psychosom Res 1960; 4:149-75; PMID:14437326; http://dx.doi.org/ 10.1016/0022-3999(60)90008-8 [PubMed] [CrossRef] [Google Scholar]
108. Marazziti D, Di Muro A, Castrogiovanni P. Psychological stress and body temperature changes in humans. Physiol Behav 1992; 52:393-5; PMID:1326118; http://dx.doi.org/ 10.1016/0031-9384(92)90290-I [PubMed] [CrossRef] [Google Scholar]
109. Briese E. Emotional hyperthermia and performance in humans. Physiol Behav 1995; 58:615-8; PMID:8587973; http://dx.doi.org/ 10.1016/0031-9384(95)00091-V [PubMed] [CrossRef] [Google Scholar]
Briese E. Emotional hyperthermia and performance in humans. Physiol Behav 1995; 58:615-8; PMID:8587973; http://dx.doi.org/ 10.1016/0031-9384(95)00091-V [PubMed] [CrossRef] [Google Scholar]
110. Shah SJ, PAtel HM. Effect of examination stress on parameters of autonomic functions in medical students. Int J Sci Res 2014; 3:273-6 [Google Scholar]
111. Vinkers CH, Penning R, Hellhammer J, Verster JC, Klaessens JH, Olivier B, Kalkman CJ. The effect of stress on core and peripheral body temperature in humans. Stress 2013; 16:520-30; PMID:23790072; http://dx.doi.org/ 10.3109/10253890.2013.807243 [PubMed] [CrossRef] [Google Scholar]
112. Oka T, Kaneda Y, Takenaga M, Hayashida S, Tamagawa Y, Kodama N, Tsuji S. Efficacy of paroxetine for treating chronic stress-induced low-grade fever. Jpn J Psychosom Intern Med 2006; 10:5-8 [Google Scholar]
113. Reimann HA. The problem of long, continued, low grade fever. JAMA 1936;107:1089-94; http://dx.doi.org/ 10.1001/jama.1936.02770400001001 [CrossRef] [Google Scholar]
114. Ziegler LH, Cash PT. A study of the influence of emotions and affects on the surface temperature of the human body. Am J Psychiatr 1938;95:677-96; http://dx.doi.org/ 10.1176/ajp.95.3.677 [CrossRef] [Google Scholar]
Ziegler LH, Cash PT. A study of the influence of emotions and affects on the surface temperature of the human body. Am J Psychiatr 1938;95:677-96; http://dx.doi.org/ 10.1176/ajp.95.3.677 [CrossRef] [Google Scholar]
115. Duras FP. Hyperpyrexia due to hysteria. Lancet 1942; 11:39; http://dx.doi.org/ 10.1016/S0140-6736(00)62135-9 [CrossRef] [Google Scholar]
116. Oka T, Oka K. Mechanisms of psychogenic fever. Adv Neuroimmune Biol 2012; 3:3-17 [Google Scholar]
117. Bohorfoush JG, Craig JB, Patterson HS. Catatonia as a cause of fever of undetermined origin. J Med Assoc Ga 1965; 54:324-5; PMID:5887902 [PubMed] [Google Scholar]
118. Buchwald D, Goldenberg DL, Sullivan JL, Komaroff AL. The “chronic, active Epstein-Barr virus infection” syndrome and primary fibromyalgia. Arthritis Rheum 1987; 30:1132-6; PMID:2823835; http://dx.doi.org/ 10.1002/art.1780301007 [PubMed] [CrossRef] [Google Scholar]
119. Enerback S. Human brown adipose tissue. Cell Metab 2010; 11:248-52; PMID:20374955; http://dx. doi.org/ 10.1016/j.cmet.2010.03.008 [PubMed] [CrossRef] [Google Scholar]
doi.org/ 10.1016/j.cmet.2010.03.008 [PubMed] [CrossRef] [Google Scholar]
120. van Marken Lichtenbelt WD, Vanhommerig JW, Smulders NM, Drossaerts JM, Kemerink GJ, Bouvy ND, Schrauwen P, Teule GJ. Cold-activated brown adipose tissue in healthy men. N Engl J Med 2009; 360:1500-8; PMID:19357405; http://dx.doi.org/ 10.1056/NEJMoa0808718 [PubMed] [CrossRef] [Google Scholar]
121. Cypess AM, Lehman S, Williams G, Tal I, Rodman D, Goldfine AB, Kuo FC, Palmer EL, Tseng YH, Doria A, et al.. Identification and importance of brown adipose tissue in adult humans. N Engl J Med 2009; 360:1509-17; PMID:19357406; http://dx.doi.org/ 10.1056/NEJMoa0810780 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
122. Virtanen KA, Lidell ME, Orava J, Heglind M, Westergren R, Niemi T, Taittonen M, Laine J, Savisto NJ, Enerback S, et al.. Functional brown adipose tissue in healthy adults. N Engl J Med 2009; 360:1518-25; PMID:19357407; http://dx.doi.org/ 10.1056/NEJMoa0808949 [PubMed] [CrossRef] [Google Scholar]
123. Saito M, Okamatsu-Ogura Y, Matsushita M, Watanabe K, Yoneshiro T, Nio-Kobayashi J, Iwanaga T, Miyagawa M, Kameya T, Nakada K, et al.. High incidence of metabolically active brown adipose tissue in healthy adult humans: effects of cold exposure and adiposity. Diabetes 2009; 58:1526-31; PMID:19401428; http://dx.doi.org/ 10.2337/db09-0530 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
Saito M, Okamatsu-Ogura Y, Matsushita M, Watanabe K, Yoneshiro T, Nio-Kobayashi J, Iwanaga T, Miyagawa M, Kameya T, Nakada K, et al.. High incidence of metabolically active brown adipose tissue in healthy adult humans: effects of cold exposure and adiposity. Diabetes 2009; 58:1526-31; PMID:19401428; http://dx.doi.org/ 10.2337/db09-0530 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
124. Lkhagvasuren B, Masuno T, Kanemitsu Y, Sudo N, Kubo C, Oka T. Increased prevalence of postural orthostatic tachycardia syndrome in psychogenic fever patients. Psychother Psychosom 2013; 82:269-70; PMID:23735890; http://dx.doi.org/ 10.1159/000345171 [PubMed] [CrossRef] [Google Scholar]
125. Lkhagvasuren B, Tanaka H, Sudo N, Kubo C, Oka T. Characteristics of the orthostatic cardiovascular response in adolescent patients with psychogenic fever. Psychother Psychosom 2014; 83:318-9; PMID:25116930; http://dx.doi.org/ 10.1159/000360999 [PubMed] [CrossRef] [Google Scholar]
126. Oka T. Mechanism and treatment of psychogenic fever. Jpn J Psychosom Intern Med 2005; 9:117-21. [Google Scholar]
Mechanism and treatment of psychogenic fever. Jpn J Psychosom Intern Med 2005; 9:117-21. [Google Scholar]
127. Oka T, Hayashida S, Kaneda Y, Kodama N, Hashimoto T, Tsuji S. Why do chronic stress-induced hyperthermia patients worry about slightly elevated body temperature? Jpn J Psychosom Intern Med 2006; 10:243-6 [Google Scholar]
128. Oka T. Influence of psychological stress on chronic fatigue syndrome. Adv Neuroimmune Biol 2013; 4:301-9 [Google Scholar]
129. Almeida MC, Steiner AA, Branco LG, Romanovsky AA: Neural substrate of cold-seeking behavior in endotoxin shock. PLoS One 2006; 1:e1; PMID:17183631; http://dx.doi.org/ 10.1371/journal.pone.0000001 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
Psychogenic fever: how psychological stress affects body temperature in the clinical population
Review
. 2015 Jun 3;2(3):368-78.
doi: 10.1080/23328940. 2015.1056907. eCollection 2015 Jul-Sep.
2015.1056907. eCollection 2015 Jul-Sep.
Takakazu Oka 1
Affiliations
Affiliation
- 1 Department of Psychosomatic Medicine; Graduate School of Medical Sciences; Kyushu University ; Fukuoka, Japan.
- PMID: 27227051
- PMCID: PMC4843908
- DOI: 10.1080/23328940.2015.1056907
Free PMC article
Review
Takakazu Oka. Temperature (Austin). .
Free PMC article
. 2015 Jun 3;2(3):368-78.
doi: 10.1080/23328940.2015.1056907. eCollection 2015 Jul-Sep.
Author
Takakazu Oka 1
Affiliation
- 1 Department of Psychosomatic Medicine; Graduate School of Medical Sciences; Kyushu University ; Fukuoka, Japan.
- PMID: 27227051
- PMCID: PMC4843908
- DOI: 10.1080/23328940.
 2015.1056907
2015.1056907
Abstract
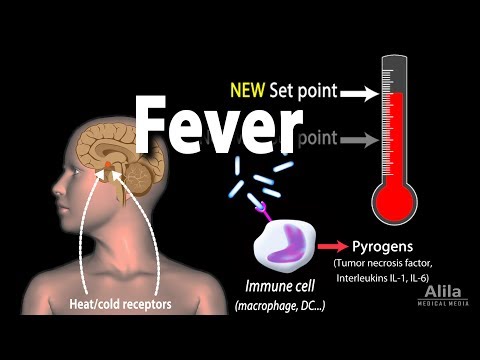
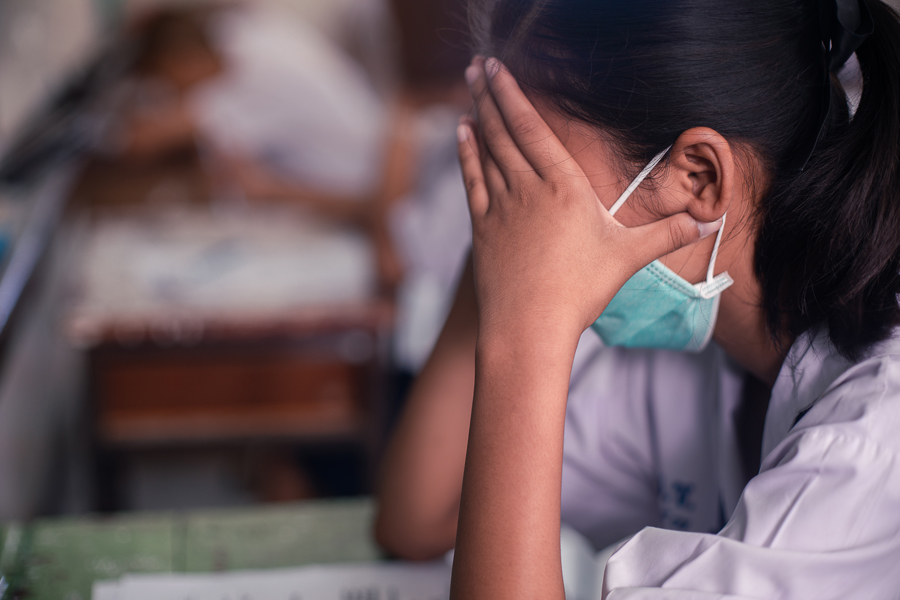
Psychogenic fever is a stress-related, psychosomatic disease especially seen in young women. Some patients develop extremely high core body temperature (Tc) (up to 41°C) when they are exposed to emotional events, whereas others show persistent low-grade high Tc (37-38°C) during situations of chronic stress. The mechanism for psychogenic fever is not yet fully understood. However, clinical case reports demonstrate that psychogenic fever is not attenuated by antipyretic drugs, but by psychotropic drugs that display anxiolytic and sedative properties, or by resolving patients' difficulties via natural means or psychotherapy. Animal studies have demonstrated that psychological stress increases Tc via mechanisms distinct from infectious fever (which requires proinflammatory mediators) and that the sympathetic nervous system, particularly β3-adrenoceptor-mediated non-shivering thermogenesis in brown adipose tissue, plays an important role in the development of psychological stress-induced hyperthermia. Acute psychological stress induces a transient, monophasic increase in Tc. In contrast, repeated stress induces anticipatory hyperthermia, reduces diurnal changes in Tc, or slightly increases Tc throughout the day. Chronically stressed animals also display an enhanced hyperthermic response to a novel stress, while past fearful experiences induce conditioned hyperthermia to the fear context. The high Tc that psychogenic fever patients develop may be a complex of these diverse kinds of hyperthermic responses.
Acute psychological stress induces a transient, monophasic increase in Tc. In contrast, repeated stress induces anticipatory hyperthermia, reduces diurnal changes in Tc, or slightly increases Tc throughout the day. Chronically stressed animals also display an enhanced hyperthermic response to a novel stress, while past fearful experiences induce conditioned hyperthermia to the fear context. The high Tc that psychogenic fever patients develop may be a complex of these diverse kinds of hyperthermic responses.
Keywords: emotional fever; fever of unknown origin; human; psychogenic fever; stress; stress-induced hyperthermia.
Figures
Figure 1.
Prominent psychogenic fever observed in…
Figure 1.
Prominent psychogenic fever observed in a 15-year-old schoolgirl. She was referred from a…
Figure 1.Prominent psychogenic fever observed in a 15-year-old schoolgirl. She was referred from a pediatrician to my outpatient clinic because she repeatedly developed antipyretic drug-resistant fever of unknown causes. I asked the patient to record her axillary temperature (Ta) using an electrothermometer 4 times a day (8 a.m., 12 a.m., 4 p.m., and 8 p.m.) and the events of the day in a “fever diary” to better understand mind (stressor)-body (temperature) relationships. I also asked her mother and school nurse to make sure the temperature she recorded was accurate. The fever diary demonstrated that she developed a high Ta up to 39°C only on the days when she went to school (underlined black bar). (Unpublished observation.)
Figure 2.
Chronic psychological stress-associated, persistent low-grade…
Figure 2.
Chronic psychological stress-associated, persistent low-grade high axillary temperature (Ta) observed in a 56-year-old…
Figure 2.Chronic psychological stress-associated, persistent low-grade high axillary temperature (Ta) observed in a 56-year-old head nurse. She had antipyretic drug-resistant, low-grade (37–38°C) high Ta for more than 3 months. © Japanese Society of Psychosomatic Internal Medicine. Reproduced by permission of Japanese Society of Psychosomatic Internal Medicine. Permission to reuse must be obtained from the rightsholder.
Figure 3.
Effects of indomethacin ( A…
Figure 3.
Effects of indomethacin ( A ), diazepam ( B ), and SR59230A (…
Figure 3.Effects of indomethacin (A), diazepam (B), and SR59230A (C), on social defeat stress-induced hyperthermia in rats. Rats received an intraperitoneal injection of indomethacin, a cyclooxygenase inhibitor (5 mg/kg), diazepam, an anxiolytic drug (4 mg/kg), SR59230A, a β3-adrenoceptor antagonist (5 mg/kg), or their respective vehicles at the time point indicated by arrows and were subsequently exposed to social defeat stress (Stress) or left undisturbed (Control) during the period indicated by the horizontal bars. © John Wiley and Sons. Reproduced by permission of John Wiley and Sons. Permission to reuse must be obtained from the rightsholder.
Figure 4.
Possible mechanisms of psychological stress-induced…
Figure 4.
Possible mechanisms of psychological stress-induced hyperthermia in comparison with infectious fever. Infectious fever…
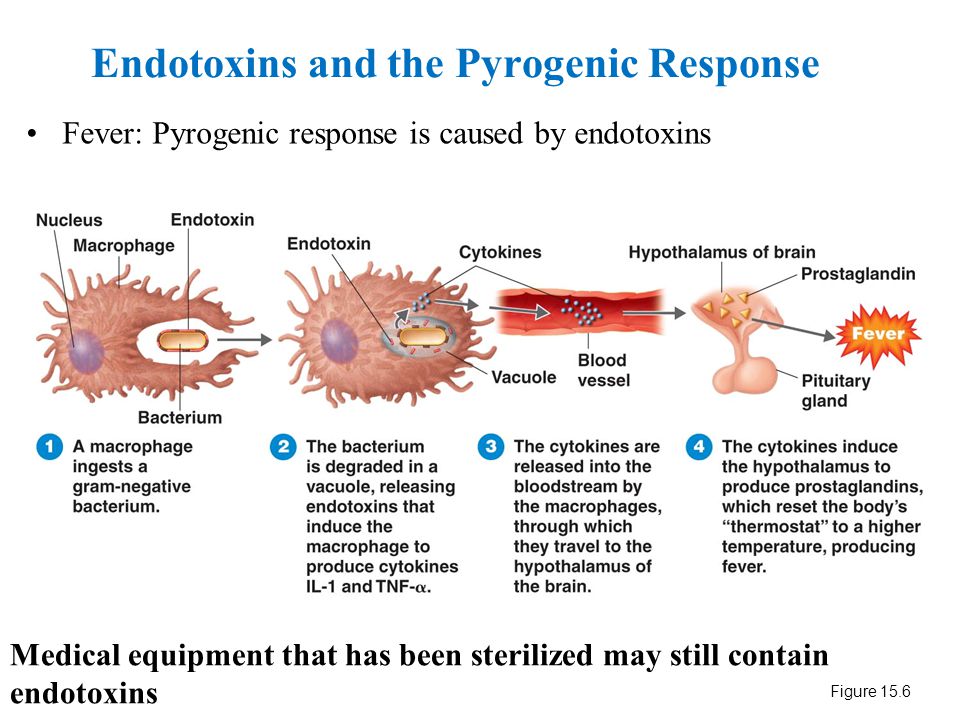
Figure 4.Possible mechanisms of psychological stress-induced hyperthermia in comparison with infectious fever. Infectious fever is induced by warmth-seeking behavior and shivering thermogenesis of the skeletal muscles, as well as sympathetic nerve-mediated non-shivering thermogenesis in brown adipose tissue and peripheral vasoconstriction. The HMS axis is known to mediate both sympathetic activation and shivering. In contrast, the brain region responsible for warmth-seeking behavior is currently unknown. Evidence suggests that neither the POA nor the DMH mediate warmth-seeking behavior. Infectious/inflammatory fever is accompanied with elevated acute-phase proteins such as CRP and sickness behavior. By contrast, psychological stress increased Tc without accompanying sickness-related symptoms because it increases Tc via cytokines and PGE2-independant manner. So far, it is not known how psychological stress activates the DMH neurons to increase Tc or how the POA and other brain regions are involved in the psychological stress-induced hyperthermia. BAT, brown adipose tissue; CRP, C-reactive protein; DMH, dorsomedial hypothalamic nucleus; HMS, hypothalamic-medullary-sympathetic; IML, intermediolateral cell column; IL, interleukin; Mϕ, macrophage; PG, prostaglandin; POA, preoptic area; rRPa, rostral raphe pallidus nucleus; Tc, core body temperature. Reprinted from Advances in Neuroimmune Biology, Vol 3, Oka T, Oka K, Mechanisms of psychogenic fever, Pages 3-17. © IOS Press. Reproduced by permission of IOS Press. Permission to reuse must be obtained from the rightsholder.
So far, it is not known how psychological stress activates the DMH neurons to increase Tc or how the POA and other brain regions are involved in the psychological stress-induced hyperthermia. BAT, brown adipose tissue; CRP, C-reactive protein; DMH, dorsomedial hypothalamic nucleus; HMS, hypothalamic-medullary-sympathetic; IML, intermediolateral cell column; IL, interleukin; Mϕ, macrophage; PG, prostaglandin; POA, preoptic area; rRPa, rostral raphe pallidus nucleus; Tc, core body temperature. Reprinted from Advances in Neuroimmune Biology, Vol 3, Oka T, Oka K, Mechanisms of psychogenic fever, Pages 3-17. © IOS Press. Reproduced by permission of IOS Press. Permission to reuse must be obtained from the rightsholder.
Figure 5.
Possible mechanisms for enhanced psychological…
Figure 5.
Possible mechanisms for enhanced psychological stress-induced hyperthermic response in chronically stressed rats. BAT,…
BAT,…
Possible mechanisms for enhanced psychological stress-induced hyperthermic response in chronically stressed rats. BAT, brown adipose tissue; SNS, sympathetic nervous system; Tc, core body temperature, UCP1, Uncoupling protein 1.
Figure 6.
Effects of stress interview on…
Figure 6.
Effects of stress interview on core and peripheral temperatures in a 26-year-old CFS…
Figure 6.Effects of stress interview on core and peripheral temperatures in a 26-year-old CFS patient. Changes in axillary (armpit) and tympanic membrane (tym.) temperatures (A) and fingertip temperature (B) during and after a 60-minute stress interview. Stress interview was conducted for one hour (0 min – 60 min). © BioMed Central. Reproduced by permission of BioMed Central. Permission to reuse must be obtained from the rightsholder.
Stress interview was conducted for one hour (0 min – 60 min). © BioMed Central. Reproduced by permission of BioMed Central. Permission to reuse must be obtained from the rightsholder.
Figure 7.
Inhibitory effects of tandospirone, a…
Figure 7.
Inhibitory effects of tandospirone, a 5-HT1A receptor agonist, on the axillary temperature (Ta)…
Figure 7.Inhibitory effects of tandospirone, a 5-HT1A receptor agonist, on the axillary temperature (Ta) and severity of fatigue in a 30-year-old woman with psychogenic fever. Vertical lines show axillary temperature (black line) and fatigue level (dotted line, with numerical rating scale in which 10 represents the most severe fatigue imaginable and 0 represents none). (A) Before the treatment (August 5th), (B) After tandospirone treatment Sep. 9th, and (C) After tandospirone treatment Sep. 18th. The patient started to take tandospirone, a 5-HT1A agonist, 30 mg from Sep. 2nd and 60 mg from Sep. 9th. © Japanese Society of Psychosomatic Internal Medicine. Permission to reuse must be obtained from the rightsholder. Before the treatment, as her Ta induced 0.5°C increased from 36.8°C to 37.3°C, her fatigue level increased remarkably from 4 to 9. She asked for the treatment of her low-grade fever hypochondriacally (A). However, after the treatment with tandospirone, she became less concerned about her low-grade fever, when although her Ta increased from 36.8°C to 37.3°C, her fatigue level increased from just 1 to 2 (B). Her Ta did not exceed 37°C (C).
(A) Before the treatment (August 5th), (B) After tandospirone treatment Sep. 9th, and (C) After tandospirone treatment Sep. 18th. The patient started to take tandospirone, a 5-HT1A agonist, 30 mg from Sep. 2nd and 60 mg from Sep. 9th. © Japanese Society of Psychosomatic Internal Medicine. Permission to reuse must be obtained from the rightsholder. Before the treatment, as her Ta induced 0.5°C increased from 36.8°C to 37.3°C, her fatigue level increased remarkably from 4 to 9. She asked for the treatment of her low-grade fever hypochondriacally (A). However, after the treatment with tandospirone, she became less concerned about her low-grade fever, when although her Ta increased from 36.8°C to 37.3°C, her fatigue level increased from just 1 to 2 (B). Her Ta did not exceed 37°C (C).
Figure 8.
Fever and fatigue chart recorded…
Figure 8.
Fever and fatigue chart recorded by a 24-year-old patient with chronic fatigue syndrome…
Figure 8.Fever and fatigue chart recorded by a 24-year-old patient with chronic fatigue syndrome and fibromyalgia syndrome. She worked as a telephone operator, a sedentary job. This chart tells that her axillary temperature is higher on the workday than on a day-off, showing that “workday hyperthermia” and the increase in axillary temperature is associated with increased fatigue. Reprinted from Advances in Neuroimmune Biology, Vol 4, Oka T, Influence of psychological stress on chronic fatigue syndrome, Pages 301-9. © IOS Press. Reproduced by permission of IOS Press. Permission to reuse must be obtained from the rightsholder.
See this image and copyright information in PMC
Similar articles
-
Stress-induced hyperthermia and hypothermia.
Oka T. Oka T. Handb Clin Neurol. 2018;157:599-621. doi: 10.1016/B978-0-444-64074-1.00035-5. Handb Clin Neurol. 2018. PMID: 30459027 Review.
-
Pyrogenic cytokines did not mediate a stress interview-induced hyperthermic response in a patient with psychogenic fever: a case report.
Hiramoto T, Oka T, Yoshihara K, Kubo C. Hiramoto T, et al. Psychosom Med. 2009 Nov;71(9):932-6. doi: 10.1097/PSY.0b013e3181bfb02b. Epub 2009 Oct 29. Psychosom Med. 2009. PMID: 19875636
-
Psychogenic fever, functional fever, or psychogenic hyperthermia?
Olivier B. Olivier B. Temperature (Austin). 2015 Aug 3;2(3):324-5. doi: 10.1080/23328940.2015.1071701. eCollection 2015 Jul-Sep. Temperature (Austin).
 2015. PMID: 27227037 Free PMC article.
2015. PMID: 27227037 Free PMC article. -
Transient visual impairment in a patient with psychogenic fever: A case report.
Wang A, Wang X, Wu P, Huang B. Wang A, et al. Am J Emerg Med. 2019 Aug;37(8):1601.e1-1601.e2. doi: 10.1016/j.ajem.2019.05.011. Epub 2019 May 6. Am J Emerg Med. 2019. PMID: 31088751
-
Neural circuit for psychological stress-induced hyperthermia.
Nakamura K. Nakamura K. Temperature (Austin). 2015 Oct 12;2(3):352-61. doi: 10.1080/23328940.2015.1070944. eCollection 2015 Jul-Sep. Temperature (Austin). 2015. PMID: 27227049 Free PMC article. Review.
See all similar articles
Cited by
-
Short Communication: Use of Infrared Thermometers for Cutaneous Temperature Recording: Agreement with the Rectal Temperature in Felis catus.

Giannetto C, Acri G, Pennisi M, Piccione G, Arfuso F, Falcone A, Giudice E, Di Pietro S. Giannetto C, et al. Animals (Basel). 2022 May 16;12(10):1275. doi: 10.3390/ani12101275. Animals (Basel). 2022. PMID: 35625121 Free PMC article.
-
Meta-Analysis of Children's Acute Psychological Stress and Action Stress on Immune Function under Microscope Images.
He H, Tan Y, Li L. He H, et al. J Healthc Eng. 2022 Mar 23;2022:6549805. doi: 10.1155/2022/6549805. eCollection 2022. J Healthc Eng. 2022. PMID: 35368932 Free PMC article.
-
Psychogenic fever and postural tachycardia syndrome among school-aged children and adolescents with fever of unknown origin.
Ishizaki Y, Yanagimoto Y, Fujii Y, Yamamoto M, Kaneko K.
 Ishizaki Y, et al. Biopsychosoc Med. 2022 Mar 29;16(1):9. doi: 10.1186/s13030-022-00238-1. Biopsychosoc Med. 2022. PMID: 35351159 Free PMC article.
Ishizaki Y, et al. Biopsychosoc Med. 2022 Mar 29;16(1):9. doi: 10.1186/s13030-022-00238-1. Biopsychosoc Med. 2022. PMID: 35351159 Free PMC article. -
Postoperative hyperthermia-induced multiple organ failure in a child with Down syndrome: a case report.
Koizumi K, Numano F, Tandou T, Takada K, Hoshiai M, Oyachi N. Koizumi K, et al. J Med Case Rep. 2022 Feb 27;16(1):84. doi: 10.1186/s13256-022-03305-x. J Med Case Rep. 2022. PMID: 35219343 Free PMC article.
-
A broader perspective: Functional symptoms beyond Neurology.
Benbadis S, Ledford R, Sawchuk T, Dworetzky B. Benbadis S, et al. Epilepsy Behav Rep. 2021 Nov 25;18:100506. doi: 10.1016/j.ebr.2021.100506. eCollection 2022. Epilepsy Behav Rep.
 2021. PMID: 35198949 Free PMC article. Review.
2021. PMID: 35198949 Free PMC article. Review.
See all "Cited by" articles
References
-
- Bakwin H. Emotional deprivation in infants. J Pediatr 1949; 35:512-21; PMID:18143946; http://dx.doi.org/10.1016/S0022-3476(49)80071-0 - DOI - PubMed
-
- White KL, Long WN Jr. The incidence of psychogenic fever in a university hospital. J Chronic Dis 1958; 8:567-86; PMID:13587612; http://dx.doi.org/10.1016/0021-9681(58)90050-X - DOI - PubMed
-
- Meyer R, Beck D.
 Psychodynamics of psychogenic fever. Zeitschrift fur Psychosomatische Medizin und Psychoanalyse 1976; 22:169-70; PMID:941539 - PubMed
Psychodynamics of psychogenic fever. Zeitschrift fur Psychosomatische Medizin und Psychoanalyse 1976; 22:169-70; PMID:941539 - PubMed
- Meyer R, Beck D.
-
- Malleson N. Panic and phobia; a possible method of treatment. Lancet 1959; 1:225-7; PMID:13631975; http://dx.doi.org/10.1016/S0140-6736(59)90052-2 - DOI - PubMed
-
- O'Toole JK, Dyck G.
 Report of psychogenic fever in catatonia responding to electroconvulsive therapy. Dis Nerv Syst 1977; 38:852-3; PMID:908250 - PubMed
Report of psychogenic fever in catatonia responding to electroconvulsive therapy. Dis Nerv Syst 1977; 38:852-3; PMID:908250 - PubMed
- O'Toole JK, Dyck G.
Publication types
A neurologist reported an influx of patients with "psychogenic fever" amid the pandemic stress.
Author:
medical editor Ekaterina Evchenko
one minute
According to Turgunkhuzhaev, doctors of medical centers are noticing an influx of patients who complain of fever up to 37.4 in the evening. Mostly they are middle-aged people who did not get sick or had COVID-19with a "clean" CT scan of the lungs and tests that did not reveal systemic inflammation. According to the doctor, this condition may be caused by the phenomenon of psychogenic fever, which was described in detail by Takakazu Oka, a Japanese specialist in psychosomatic conditions.
According to the doctor, this condition may be caused by the phenomenon of psychogenic fever, which was described in detail by Takakazu Oka, a Japanese specialist in psychosomatic conditions.
This is a hyperthermic reaction of the body to mental stress, which is most often not accompanied by mental disorders and does not depend on the patient's consciousness. In rare cases, the temperature can reach 41 degrees, but mostly psychogenic hyperthermia is characterized by a temperature of 37-38 for weeks, months, in rare cases - several years, after an acute traumatic situation, without a significant reaction to antipyretic drugs.
In his work, Takazu Oka distinguishes two principal mechanisms for the formation of elevated temperature: caused by infection and not caused by infection, writes Turgunkhuzhaev.
“Everything is clear with the first one. There is an infection, or its systemic display in blood counts, look for, treat. With the second, everything is not very clear, especially if the patient has neither clinical nor hormonal reasons for hyperthermia. And if we omit all the diagnostic search that can be applied to the patient, then it is worth remembering about one more condition that can cause a rise in temperature. Psychogenic, stress-induced, functional hyperthermia is a common cause of fever of unknown cause in a situation where there is no evidence for a systemic inflammatory response,” writes Oybek Turgunkhuzhaev.
And if we omit all the diagnostic search that can be applied to the patient, then it is worth remembering about one more condition that can cause a rise in temperature. Psychogenic, stress-induced, functional hyperthermia is a common cause of fever of unknown cause in a situation where there is no evidence for a systemic inflammatory response,” writes Oybek Turgunkhuzhaev.
Treatment of this condition consists in prescribing the correct anti-anxiety or antidepressant therapy, or identifying psychological triggers that should be excluded from avoidance.
Turgunkhuzhaev stressed that the psychogenic fever was described by scientists as scientists, and also against the backdrop of a pandemic.
“Many of us have already experienced such a state. For example, during a session, or while talking about a very uncomfortable and stressful event in your life, being at an unloved job, the doctor said.
He advised his colleagues to openly discuss with patients the likelihood of their developing functional hyperthermia due to stress, show them scientific articles and, if necessary, refer them to a psychotherapist or psychiatrist.
Comments Cackl e
ABC Medicine
Tachycardia is one of the most common heart rhythm disorders. The main mechanism for the development of pathology is to increase the automatism of the sinus node. In this case, the heart rate increases to more than 90 beats per minute. Tachycardia may not have subjective manifestations. Most often it is felt as an increased heartbeat. In the presence of pathologies of the cardiovascular system, this type of arrhythmia can worsen the general condition and provoke the development of complications. Therefore, the treatment of tachycardia should be prescribed and strictly monitored by a specialist.
Causes of tachycardia
Increased or increased heart rate does not always mean that there are problems with the cardiovascular system. For example, in preschool age, it is considered the norm and does not require special assistance. Symptoms of tachycardia of the heart can also appear in practically healthy people as a result of the activation of physiological compensatory mechanisms, that is, as a response of the body to the influence of one or another external factor. The reaction of the nervous and cardiovascular systems, accompanied by the release of adrenaline into the blood, causes an increase in heart rate. The occurrence of tachycardia can be provoked by the following factors:
The reaction of the nervous and cardiovascular systems, accompanied by the release of adrenaline into the blood, causes an increase in heart rate. The occurrence of tachycardia can be provoked by the following factors:
- stress, exercise and emotional arousal;
- increase in ambient air temperature;
- use of caffeinated drinks, alcohol, certain drugs;
- abrupt change in body position, etc.
When the provoking factor stops, the heart rhythm gradually returns to normal.
However, tachycardia often accompanies the presence of certain pathological conditions. It can be a manifestation of various cardiovascular diseases - arterial hypertension, myocardial infarction, heart disease (rheumatic or congenital), cardiosclerosis, etc. In addition, tachycardia can be neurogenic in nature, that is, it can be associated with disorders of the autonomic nervous system and brain. Other causes include fever, which develops against the background of an infectious and inflammatory process (pneumonia, tonsillitis, etc. ).
).
Symptoms of the disease
For tachycardia, which is a sign of a disease, the following symptoms are characteristic.
- Feeling interruptions and / or "failures" in the work of the heart - the most common manifestations.
- Shortness of breath (shortness of breath) that occurs with little exertion or even at rest.
- Pain in the region of the heart (accompanying an attack of tachycardia in vegetative-vascular dystonia and some other diseases).
- Dizziness and darkening of the eyes, pre-syncope and even fainting (this is due to a violation of the blood supply to the brain).
In general, the manifestation of clinical symptoms of tachycardia depends on the nature of the underlying disease, as well as on the severity and duration of the arrhythmia itself.
Consequences of tachycardia
Physiological tachycardia, which occurs in healthy people even in the presence of severe subjective manifestations, does not pose a threat to life and has a good prognosis. In patients with heart disease, the consequences can be quite serious. The main and severe complications are the development of heart failure, loss of consciousness and even sudden death. In addition, the presence of tachycardia increases the risk of blood clots, which in turn leads to frequent heart attacks and stroke. Therefore, timely assistance with tachycardia is so important.
In patients with heart disease, the consequences can be quite serious. The main and severe complications are the development of heart failure, loss of consciousness and even sudden death. In addition, the presence of tachycardia increases the risk of blood clots, which in turn leads to frequent heart attacks and stroke. Therefore, timely assistance with tachycardia is so important.
Diagnosis of tachycardia
Electrocardiography
ECG plays a leading role in the differential diagnosis of tachycardia and helps to identify its causes. This method allows you to determine the type of pathology, as well as rhythm and heart rate. With an increase in the severity of symptoms of cardiac tachycardia, it is advisable to conduct daily Holter ECG monitoring. This method is highly informative. It allows you to identify and analyze any heart rhythm disturbances within 24 hours. Holter monitoring helps to detect ischemic changes during normal physical activity.
Echocardiography
It is a standard examination method that allows to exclude heart pathology in case of any rhythm disturbances. Thanks to echocardiography, the doctor receives data on the size of the chambers of the heart, the thickness of the walls of the myocardium, and changes in the valvular apparatus. This examination allows you to identify violations of local contractility.
Electrophysiological examination
This is an invasive method for examining patients with cardiac pathology. An electrophysiological study is used with appropriate indications before surgery for the treatment of arrhythmias. Used to diagnose different types of tachycardia in a limited number of patients. This method is reduced to determining the nature of the propagation of an electrical impulse through the myocardium, allowing you to determine the mechanisms of tachycardia or conduction disorders of the heart.
Additional examinations
Additional research methods are used to identify the causes of cardiac pathology. The specialist may prescribe a blood test (general and thyroid hormones), electroencephalography. Rarely, an MRI of the heart is done, usually to look for congenital abnormalities.
The specialist may prescribe a blood test (general and thyroid hormones), electroencephalography. Rarely, an MRI of the heart is done, usually to look for congenital abnormalities.
Treatment of tachycardia
Medicinal
Drugs belonging to the following groups are used to treat tachycardia.
- Antiarrhythmic. These are medicines with different mechanisms of action. Only the attending physician can prescribe them, based on clinical data. Self-medication is dangerous, because the same medications can be effective for one type of tachycardia and contraindicated for another.
- Sedatives. These are most often synthetic or herbal products. They are prescribed for the treatment of tachycardia associated with vegetative-vascular dystonia. Such funds help to normalize the functioning of the nervous system and, as a result, reduce the frequency of arrhythmia attacks.
If tachycardia is accompanied by a drop in blood pressure, pressor amines are usually prescribed to raise it to a level of 100-110 mm Hg. Art.
Art.
Surgical
Minimally invasive surgery is a common definitive treatment for tachycardia. It is performed under local anesthesia. This can be radiofrequency catheter ablation, the installation of an artificial pacemaker, etc. Among the main reasons that require serious surgical care are the following.
- Hormonal disorders. Common causes of tachycardia are thyrotoxicosis (too much thyroid hormone) and pheochromocytoma (a hormonally active tumor in the kidney or adrenal glands). In such cases, surgical removal of the neoplasm or the area of the gland that produces excess hormones is usually recommended.
- Structural and functional changes. Cardiac surgery is performed in the presence of gross congenital heart defects, severe circulatory disorders (IBC), to eliminate the consequences of rheumatism, etc.
In some cases, arrhythmia does not require special treatment if it is a symptom of anemia, due to the presence of a malignant blood disease (for example, leukemia), occurs against a background of fever, etc.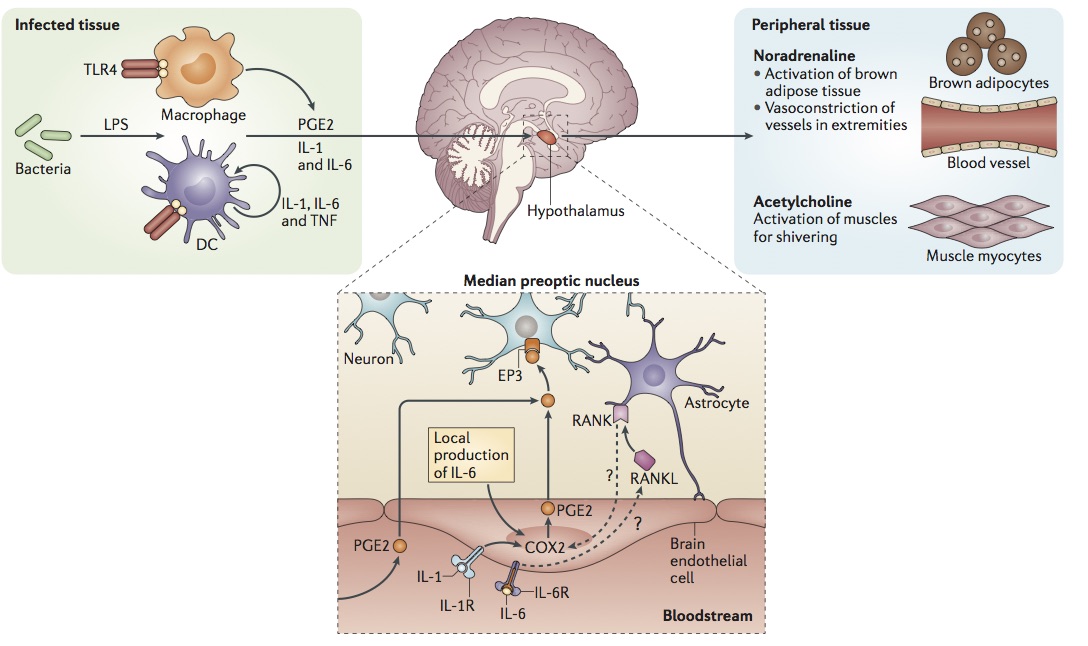 For tachycardia caused by such causes, the treatment is to eliminate the underlying disease.
For tachycardia caused by such causes, the treatment is to eliminate the underlying disease.
Prevention of tachycardia
Timely assistance in detecting tachycardia helps to avoid the occurrence of its attacks in the future. Therefore, it is important, first of all, to consult a doctor who will prescribe the correct treatment. Prevention of this disease consists in its early diagnosis, treatment of cardiac pathology, as well as elimination of the influence of non-cardiac factors that provoke the development of heart rate disorders.
Normalization of nutrition
It is important to limit or completely eliminate the consumption of products containing caffeine, alcohol. Instead of strong coffee or tea, you can drink herbal infusions that have a sedative effect. You should limit the consumption of sweet and fatty foods, follow the principles of a healthy diet. The most correct and useful choice for people suffering from heart disease will be a plant-milk diet. The presence of fruit and vegetable juices in the diet is also important.
The presence of fruit and vegetable juices in the diet is also important.
Taking vitamins and microelements
To prevent heart palpitations, it is recommended to take magnesium, which regulates the effects of calcium in heart cells. This microelement contributes to the establishment of rhythmic contractions and relaxations of the heart muscle. Potassium is also important for the proper functioning of the body. Please note that all drugs should be prescribed by a doctor based on the causes of the disease and provoking factors.
Active lifestyle
Sports and reasonable physical activity stimulate the heart and at the same time increase the body's resistance to the release of excess adrenaline. As a result, the general emotional background is normalized, irritability decreases. It is important to strictly dose the load, avoiding overvoltage. Regular and prolonged exposure to fresh air helps to reduce the frequency of occurrence of tachycardia attacks.