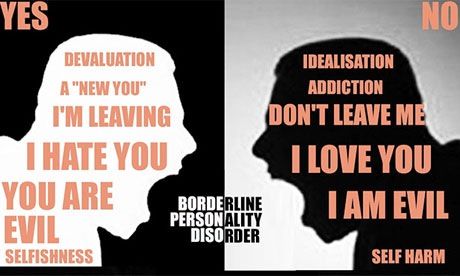
Evil personality disorder
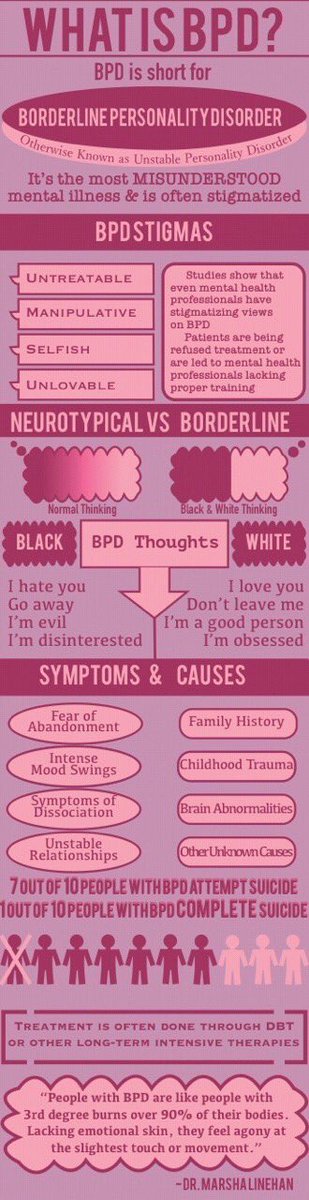
What is borderline personality disorder (EUPD)?
This section has information on borderline personality disorder (BPD), including symptoms, causes and treatments. This information is for people affected by BPD in England who are 18 or over. It’s also for their carers, friends and relatives and anyone interested in this subject.
Borderline personality disorder is also called emotionally unstable personality disorder (EUPD) and emotional intensity disorder (EID). In this factsheet, we call it BPD as this is still the most common term for the condition. But we appreciate that all 3 terms can be controversial.
If you would like more advice or information you can contact our Advice and Information Service by clicking here.
Download Borderline personality disorder (BPD) factsheet
- Overview
- About
- Symptoms
- Causes and treatment
- Problems and self-care
- Information for carers
- Further reading
- Useful contacts
Overview
- BPD means that you feel strong emotions that you struggle to cope with.
You may feel upset or angry a lot of the time.
- Around 1 in 100 people live with BPD.
- There are different reasons why people get BPD. A lot of people who live with a diagnosis of BPD have had traumatic experiences in their childhood.
- If you are someone living with a diagnosis of BPD, it is more likely that you will self-harm. And have challenges with relationships, alcohol or drugs. There is help available.
- There are different ways to treat BPD. The NHS should normally offer you therapy.
Need more advice?
If you need more advice or information you can contact our Advice and Information Service.
Contact us Contact us
About
What is borderline personality disorder (BPD)?
Everyone has different ways of thinking, feeling, and behaving. It is these thoughts, feelings, and behaviours that make up our ‘personality’. These are often called our traits. They shape the way we view the world and the way we relate to others. By the time we are adults these will make us part of who we are.
It is these thoughts, feelings, and behaviours that make up our ‘personality’. These are often called our traits. They shape the way we view the world and the way we relate to others. By the time we are adults these will make us part of who we are.
You can think of your traits as sitting along a scale. For example, everyone may feel emotional, get jealous, or want to be liked at times. But it is when these traits start to cause problems that you may be diagnosed as having a personality disorder.
BPD is a type of ‘personality disorder’.
BPD can affect how you cope with life, manage relationships, and feel emotionally. You may find that your beliefs and ways of dealing with day-to-day life are different from others. You can find it difficult to change them.
You may find your emotions confusing, tiring, and hard to control. This can be distressing for you and others. Because it is distressing, you may find that you develop other mental health problems like depression or anxiety. You may also do other things such as drink heavily, use drugs, or selfharm to cope.
You may also do other things such as drink heavily, use drugs, or selfharm to cope.
Research shows that around 1 in 100 people live with BPD. It seems to affect men and women equally, but women are more likely to have this diagnosis. This may be because men are less likely to ask for help. BPD is sometimes called emotionally unstable personality disorder (EUPD). Some people feel that this describes the illness better.
Some people who live with BPD think that the name is insulting or makes them feel labelled. Doctors don’t use this term to make you feel judged or suggest that the illness is your fault. It is meant to describe the way the illness develops. It’s important to remember this is a health condition. And not a judgement of your character or you as a person.
Symptoms
What are the symptoms of BPD?
Everyone will experience BPD differently. If you live with BPD, you may have difficulties with:
- being impulsive. This means that you like to do things on the spur of the moment,
- feeling bad about yourself,
- controlling your emotions,
- self-harming,
- suicidal thoughts and attempts to take your own life,
- feeling 'empty’,
- dissociation.
 This could be a feeling of being disconnected from your own body. Or feeling disconnected from the world around you.
This could be a feeling of being disconnected from your own body. Or feeling disconnected from the world around you. - identity confusion. You might not have a sense of who you are.
- feeling paranoid or depressed,
- hearing voices or noises when you are stressed, and
- intense but unstable relationships with others.
Not everyone will experience all these symptoms.
Sam's Story
Many people who live with BPD will also experience other mental health problems. Such as depression, anxiety, eating disorders, PTSD and alcohol or drug misuse. People who live with BPD can also be diagnosed with bipolar disorder. The symptoms of bipolar disorder can often be confused with those of BPD.
You can find more information about:
- Personality disorders by clicking here.
- Dissociation and dissociative disorders by clicking here.
- Self-harm by clicking here.
- Anxiety disorders by clicking here.
- Depression by clicking here.
- PTSD by clicking here.
- Drugs, alcohol and mental health by clicking here.
- Bipolar disorder by clicking here.
Causes & treatment
What causes BPD?
There’s no single reason why some people develop borderline personality disorder (BPD). Professionals can’t use things like blood tests or brain scans to help diagnose people.
It is thought that BPD may be caused by a combination of factors:
- Genetics – you may be more vulnerable to BPD if a close family member also lives with BPD. There is no evidence though of a particular gene being responsible for BPD.
- Brain chemicals – problems with levels of your brain chemicals, particularly serotonin.
- Brain development – many people who live with BPD have smaller, or more active, parts of their brain. These parts of the brain are affected by your early upbringing.
 And can affect the regulation of your emotions, behaviour and self-control. They can also affect you planning and decision making.
And can affect the regulation of your emotions, behaviour and self-control. They can also affect you planning and decision making. - Environmental factors – a number of environmental factors seem to be common with people who live with BPD. These can include:
- experiencing abuse,
- experiencing long-term fear or distress as a child,
- being neglected by 1, or both, of your care-givers as a child, and
- growing up with a family member who had a serious mental health condition. Such as bipolar disorder or a problem with alcohol or drugs.
How can I get help if I think I have BPD?
The first step to get help is to speak to your GP.
Your GP will look at different things when deciding how best to help you. So, it can help to keep a record of your symptoms. This can help you and your GP to understand what difficulties you are facing. It may help if you keep a record of:
- how distressed you feel,
- any risks to yourself or other people, and
- details of anything you have done to try and reduce your levels of anxiety and distress.
Your GP can’t diagnose BPD. Only a psychiatrist should make a formal diagnosis. A psychiatrist is part of the community mental health team (CMHT). If your GP feels that you need more support they will refer you to the CMHT.
What happens if my GP refers me to the community mental health team (CMHT)?
There may be a waiting list to see your CMHT. You can ask your GP, or contact the CMHT, about how long the waiting list is.
When you have your first appointment with the CMHT they will ask you questions to understand how your mental health is affecting you. They will talk to you about:
- how you manage your day to day life, relationships and work,
- coping strategies that you use,
- your strengths,
- areas in your life that you find difficult.
- any other mental health problems you may have,
- any other social problems that you may have,
- any social care and support needs you may have,
- any support you may need in staying in your job, or finding a job,
- any psychological treatment you may need.
 This is also known as ‘talking therapy’, and
This is also known as ‘talking therapy’, and - the needs of any dependent children that you have.
How will the CMHT decide if I have BPD?
Psychiatrists use the following guidelines to decide if you have a mental disorder.
- International Classification of Diseases (ICD-10), produced by the World Health Organisation (WHO).
- Diagnostic and Statistical Manual of Mental Disorders (DSM-5), produced by the American Psychiatric Association.
The guidelines tell your psychiatrist what to look for. They will diagnose you with BPD if you have at least five of the symptoms below.
- Extreme reactions to feeling abandoned.
- Unstable and intense relationships with others
- Confused feelings about your self-image or your sense of identity.
- Being impulsive in ways that could be damaging. For example, spending, sex, substance abuse, reckless driving, and binge eating
- Regular self-harming, suicidal threats or behaviour.
- Long lasting feelings of emptiness or being abandoned.
- Inappropriate or intense anger. And difficulty controlling your anger. For example, losing your temper or getting into fights.
- Intense, highly changeable moods.
- Paranoid thoughts, or severe dissociation, when you’re stressed. Dissociation is a feeling of being disconnected from your own body. Or feeling disconnected from the world around you
You can find more information about:
- NHS Mental Health Teams (MHTs) by clicking here.
- Dissociation and dissociative disorders by clicking here.
What treatment should the NHS offer me?
You can check what treatment and care is recommended for BPD on the National Institute for Health and Care Excellence (NICE) website. NICE produce guidelines for how health professionals should treat certain conditions. You can download these from their website at:
www.nice.org.uk.
The NHS does not have to follow these recommendations. But they should have a good reason for not following them.
But they should have a good reason for not following them.
People who live with BPD have sometimes been excluded from NHS services because of their diagnosis. But the NHS should not refuse to give you specialist help because of your diagnosis. They should have services to support people with BPD.
If your local NHS doesn’t offer you appropriate treatment then there are things that you can do. For information about your options please see further down this page.
Should I be offered medication?
There is no medication to treat BPD. But your doctor may offer you medication if you also have symptoms of another mental illness like anxiety or depression.
What psychological treatment should I be offered?
Psychological therapy is also known as ‘talking therapy’. There are lots of different types of talking therapies and your doctor should talk to you about what is available, how it may help you and what type of therapy you would like.
We have included details below of some of the therapies that your doctor may use. But these are not available everywhere. And your doctor may recommend other types of talking therapy.
But these are not available everywhere. And your doctor may recommend other types of talking therapy.
Your doctor will also think about:
- how much BPD is affecting you,
- how much you are willing to engage with therapy,
- if you want to change how react to your thoughts and feelings,
- if you will be able to work effectively with a counsellor, and
- the personal and professional support that is available.
The therapy you are offered should last at least 3 months. If your doctor decides that talking therapies are not suitable, they should explain why.
Dialectical behavioural therapy (DBT)
The guidance says that the NHS should offer DBT to women with BPD if they self-harm regularly.
DBT is a type pf therapy specifically designed to treat people with BPD. The goal of BPD is to help you accept that your emotions are real and acceptable. And to challenge how you respond to those emotions by being open to ideas and opinions which are different to your own.
DBT usually involves weekly individual and group sessions. And you should be given an out-of-hours contact number to call if your symptoms get worse.
DBT is based on teamwork. You'll be expected to work with your therapist and the other people in your group sessions. In turn, the therapists work together as a team.
Mentalisation-based therapy (MBT)
Mentalisation means the ability to think about thinking. This means looking at your own thoughts and beliefs. And working out if they are helpful and realistic.
This type of therapy also helps you to recognise that other people have their own thoughts, emotions and beliefs. And that you may not always understand these. The therapy also helps you to think about how your actions might affect what other people think or feel.
A course of MBT usually lasts around 18 months. You may first be offered MBT in a hospital as an inpatient. The treatment usually consists of daily individual sessions with a therapist and group sessions with other people with BPD.
Some hospitals and specialist centres like you to remain in hospital whilst you are having MBT. But others recommend that you leave the hospital after a certain period of time but remain being treated as an outpatient. This means that you will visit the hospital regularly.
Arts therapies
There are different types of arts of creative therapies. These include:
- art therapy,
- drama therapy,
- music therapy, and
- dance movement therapy.
These therapies can be offered individually but they are often done in groups. Sessions are usually weekly. These therapies can be helpful to people who find it hard to talk about their thoughts and feelings.
Therapeutic communities
Therapeutic communities are not a treatment themselves. They are places you can go to have treatment. Most therapeutic communities are residential. They help people with long-term emotional problems, and a history of self-harming, by teaching them skills to help them have better relationships.
These communities often set strict rules on behaviour. For example, no drinking alcohol, no violence and no attempts at self-harming.
You may stay for a few weeks or months, or you may visit for just a few hours a week. You may have group therapy and self-help sessions. You would be expected to take part in other activities to improve your self-confidence and social skills. These activities may include household chores, games and preparing meals.
Therapeutic communities vary a lot because they are often run by the people who use them. And they shape them based on what they want to achieve.
What happens if the CMHT can’t successfully treat me?
You may get support from a specialist service if your symptoms are getting worse. These specialist services are also called ‘Tier 3’ or ‘Tier 4’ services.
These services are not available in all NHS Trusts. And they can be difficult to access. You can speak to your CMHT and if they can refer you to a specialist service.
You can find more information about Tier 3 and Tier 4 services in our factsheet ‘Second Opinions’ by clicking here.
What treatment should I get if I am in crisis?
A mental health crisis is when you need urgent help. You may be feeling suicidal or wanting to self-harm. And you don’t think that you can use your normal coping strategies to stop yourself from acting on your feelings.
If you have a diagnosis of BPD but are not under the care of your local community mental health team (CMHT), then you should speak to your GP. Your GP should:
- assess the level of risk to yourself or others,
- talk to you about previous mental health crises. And what skills you have used to cope with these,
- help you to use these skills and focus on your current problems,
- help you to identify changes which you can put in place to manage your current problems, and
- offer you a follow-up appointment.
If you are already under the CMHT, or a specialist service, then you should have a care plan. The care plan should include a crisis plan that you can follow. Your crisis plan is written by you and your mental health team. It should include:
The care plan should include a crisis plan that you can follow. Your crisis plan is written by you and your mental health team. It should include:
- what triggers might lead to a mental health crisis,
- self-management skills which you have used before and find helpful,
- details of how to access help if the self-management skills aren’t helping. This should include a list of support numbers for out-of-hours teams and crisis teams.
Your doctor may think about offering you sedative medication. Sedatives can help you feel more relaxed. But your doctor should not give you sedatives for more than a week.
Some people find it helpful to contact emotional support lines during a mental health crisis. There is a list of contact numbers at the bottom of this page.
You can find more information about ‘Getting help in a crisis’ by clicking here.
Problems & self-care
What risks and complications can BPD cause?
Self-harm
It is common for people who live with BPD to self-harm. Some people find self-harming can help them to deal with painful feelings. But it can cause serious injury, scars, infections, or accidental death. A big focus of BPD treatment is to find other ways to deal with painful emotions.
Some people find self-harming can help them to deal with painful feelings. But it can cause serious injury, scars, infections, or accidental death. A big focus of BPD treatment is to find other ways to deal with painful emotions.
You can find more information about ‘Self-harm’ by clicking here.
Suicide
People who live with BPD are more at risk of suicide or of attempting suicide. Most people who live with BPD who feel suicidal will feel more positive within a few hours. So it is important to use techniques to try and distract from the strong suicidal feelings.
You can find more information about ‘Suicidal thoughts’ by clicking here.
Drugs and alcohol
People who live with BPD may:
- behave impulsively,
- drink too much alcohol,
- misuse prescription medication, or
- take illegal drugs.
You are more likely to die by suicide if you are also using alcohol. So If you are feeling suicidal you can help keep yourself safer by making sure that you don’t use alcohol.
You may be at an increased risk of becoming dependent on alcohol or drugs if you have BPD.
If you drink a lot of alcohol or use drugs, you may find it difficult to get treatment for BPD. But NICE guidelines state that you should be referred to a service that can help with your substance use. And you should be able to continue with BPD treatment where appropriate.
You can find more about ‘Drugs, alcohol and mental health’ by clicking here.
Impulsive behaviours
When people make decisions quickly without thinking about the consequences, doctors call this ‘impulsive’. This can include driving erratically or having multiple sexual partners. Or spending money on things you can't afford or don't need.
If impulsive behaviour leads you to have debt problems you can find more support and information at: www.mentalhealthandmoneyadvice.org.
What if I am not happy with my treatment?
If you are not happy with your treatment you can:
- talk to your doctor about your treatment options,
- ask for a second opinion,
- get an advocate to help you speak to your doctor,
- contact Patient Advice and Liaison Service (PALS) and see whether they can help, or
- make a complaint.
There is more information about these options below.
Treatment options
You should first speak to your doctor about your treatment. Explain why you are not happy with it. You could ask what other treatments you could try.
Tell your doctor if there is a type of treatment that you would like to try. Doctors should listen to your preference. If you are not given this treatment, ask your doctor to explain why it is not suitable for you.
Second opinion
A second opinion means that you would like a different doctor to give their opinion about what treatment you should have. You can also ask for a second opinion if you disagree with your diagnosis.
You don’t have a right to a second opinion. But your doctor should listen to your reason for wanting a second opinion.
Advocacy
An advocate is independent from the NHS. They are free to use. They can be useful if you find it difficult to get your views heard. There are different types of advocates available.
Community advocates can support you to get a health professional to listen to your concerns. And help you to get the treatment that you would like. This type of service doesn’t exist in all areas.
An NHS Complaints Advocate can help you if you want to complain about the NHS. This service exists in all areas.
To search for services, you can try the following.
- Use an internet search engine – use search terms like ‘advocacy Leicestershire’ or ‘mental health advocacy Devon’.
- Ask a support worker or key worker, if you have one.
- Ask your local council whether they have a list.
- Ask your local NHS Patient Advice and Liaison Service (PALS) whether they have a list of local advocacy services.
- Look at local service directories. You can sometimes find useful directories of mental health services online.
- Get in touch with organisations that offer advocacy such as Rethink Mental Illness, Mind, The Advocacy People, Voiceability and POhWER.
The Patient Advice and Liaison Service (PALS)
PALS is part of the NHS. They give information and support to patients.
You can find your local PALS’ details through this website link:
www.nhs.uk/Service-Search/Patient-advice-and-liaison-services-(PALS)/LocationSearch/363.
You can find out more about:
- Medication. Choice and managing problems by clicking here.
- Second opinions by clicking here.
- Advocacy by clicking here.
- Complaining about the NHS or social services by clicking here.
What can I do to manage my symptoms?
You can learn to manage your symptoms by looking after yourself. Selfcare is how you take care of your diet, sleep, exercise, daily routine, relationships and how you are feeling.
Lifestyle
Making small lifestyle changes can improve your wellbeing and can help your recovery.
Routine helps many people with their mental wellbeing. It will help to give a structure to your day and may give you a sense of purpose. This could be a simple routine such as eating at the same time each day, going to bed at the same time each day and buying food once per week.
This could be a simple routine such as eating at the same time each day, going to bed at the same time each day and buying food once per week.
Breathing exercises
Breathing exercises can help to calm you when you are feeling anxious. You will get the most benefit if you do them regularly, as part of your daily routine.
There is more information about breathing exercises in the further reading section at the bottom of this page.
Support groups
You could join a support group. A support group is where people come together to share information, experiences and give each other support.
You might be able to find a local group by searching online. Rethink Mental Illness have support groups in some areas. You can find out what is available in your area if you follow this link: www.rethink.org/about-us/our-support-groups. Or you can call the Rethink Mental Illness Advice Service on 0808 801 0525 for more information.
Recovery College
Recovery colleges are part of the NHS. They offer free courses about mental health to help you manage your symptoms. They can help you to take control of your life and become an expert in your own wellbeing and recovery. You can usually self-refer to a recovery college. But the college may inform your care team.
They offer free courses about mental health to help you manage your symptoms. They can help you to take control of your life and become an expert in your own wellbeing and recovery. You can usually self-refer to a recovery college. But the college may inform your care team.
Unfortunately, recovery colleges are not available in all areas. To see if there is a recovery college in your area you can use a search engine such as Google. Or contact Rethink Mental Illness Advice Service on 0808 801 0525.
You might also find some of the following things helpful.
- Make sure you speak to a doctor if you think that your relationships with others are being affected.
- Think about how you will benefit from making changes to your lifestyle.
- Don’t pay too much attention to the name of the condition. BPD is a common condition and it is not meant to label you or to suggest that your situation won’t change.
- If you’re offered group therapy or support, give it a chance.
 It may seem intimidating to start with, but a lot of people find it helpful in the long-run.
It may seem intimidating to start with, but a lot of people find it helpful in the long-run. - If something annoys or upsets you, try to wait a while before responding. Think carefully about what you’re going to say and how you’re going to say it.
- Try to find ways of relaxing. Meditation, breathing techniques, listening to music and exercising may be helpful.
- Look for patterns in the ways you respond to things that upset you. This may help you to work through problems in relationships.
- If you self-harm to deal with distress, think of other ways to deal with this. Try punching a pillow or writing about how you feel.
- Use an online mental health forum. Make sure that you check with a mental health professional how trustworthy the website is for helpful information on BPD.
You can find more information about:
- Recovery by clicking here.
- Self-harm by clicking here.
- Suicidal feelings – how to cope by clicking here.

Information for carers, friends and relatives
Information for carers, friends and relatives
As a carer, friend or family member of someone living with borderline personality disorder (BPD), you might find that you need support.
How can I get support?
You can do the following.
- Speak to your relative’s care team about a carer’s assessment.
- Ask for a carer’s assessment from your local social services.
- Join a carers service. They are free and available in most areas.
- Join a carers support group for emotional and practical support. Or set up your own.
- Speak to your GP about medication and talking therapies for yourself if your mental health is affecting your day-to-day life.
What is a carer’s assessment?
A carer’s assessment is an assessment of the support that you need so that you can continue in your caring role.
To get a carers assessment you need to contact your local authority.
How do I get support from my peers?
You can get peer support through carer support services or carers groups. You can search for local groups in your area by using a search engine such as Google. Or you can contact the Rethink Mental Illness Advice Service and we will search for you.
How can I support the person I care for?
You can do the following.
- Read information about BPD.
- Ask the person you support to tell you what their symptoms are and if they have any self-management techniques that you could help them with.
- Encourage them to see a GP if you are worried about their mental health.
- Ask to see a copy of their care plan, if they have one. They should have a care plan if they are supported by a care coordinator.
- Help them to manage their finances.
How can learning about BPD help?
Learning about BPD can help you to:
- support the person who has BPD,
- understand why they may act in certain ways, and perhaps take things less personally, and
- become more aware of what situations make them more distressed.

Craig's Story
What is a care plan?
The care plan is a written document that says what care your relative or friend will get and who is responsible for it.
A care plan should always include a crisis plan. A crisis plan will have information about who to contact if they become unwell. You can use this information to support and encourage them to stay well and get help if needed.
Can I be involved in care planning?
As a carer you can be involved in decisions about care planning. But you don’t have a legal right to this.
Your relative or friend needs to give permission for the NHS to share information about them and their care.
You can find out more about:
- Supporting someone with a mental illness by clicking here.
- Getting help in a crisis by clicking here.
- Suicidal thoughts. How to support someone by clicking here.
- Responding to unusual thoughts and behaviours by clicking here.

- Carers assessment by clicking here.
- Confidentiality and information sharing. For carers, friends and family by clicking here.
- Money matters: dealing with someone else’s money or benefits by clicking here.
- Worried about someone’s mental health by clicking here.
- Benefits for carers by clicking here.
- Stress by clicking here.
Further reading
North West Boroughs Healthcare NHS Foundation Trust
This NHS website has information dedicated to different breathing techniques. These techniques can help you when you feel anxious.
Website: www.nwbh.nhs.uk/healthandwellbeing/Pages/Breathing-Techniques-.aspx
Centre for Clinical Interventions
This website is provided by the department of Health in Western Australia. They have some useful information sheets and a workbook for people who are experiencing problems with coping with their feelings. And for people experiencing distress.
And for people experiencing distress.
Website: www.cci.health.wa.gov.au/Resources/For-Clinicians/Distress-Tolerance
You can find out more about:
- Getting help in a crisis by clicking here.
- Suicidal thoughts - How to cope by clicking here.
- Self-harm by clicking here.
- Drugs, alcohol and mental health by clicking here.
- Carers assessment - Under the Care Act 2014 by clicking here.
- Confidentiality and information sharing - For carers, friends and family by clicking here.
- Worried about someone’s mental health by clicking here.
- Stress - How to cope by clicking here.
Useful contacts
BPD World
Provides information and support to people affected by personality disorders. It has an online support forum.
Website: www.bpdworld.org
Samaritans
Can be contacted by telephone, letter, e-mail and mini-com. There's also a face-to-face service, available at their local branches. They are open 24 hours a day, every day of the year.
There's also a face-to-face service, available at their local branches. They are open 24 hours a day, every day of the year.
Telephone: 116 123
Email: [email protected]
Website: www.samaritans.org
ASSISTline
National helpline offering supportive listening service to anyone throughout the UK with thoughts of suicide or thoughts of self-harm. They are open 24/7.
Telephone: 0800 689 5652
Website: www.spbristol.org/
Sane Line
Work with anyone affected by mental illness, including families, friends and carers. They also provide a free text-based support service called Textcare and an online supportive forum community where anyone can share their experiences of mental health.
Telephone: 0300 304 7000
Textcare: www.sane.org.uk/what_we_do/support/textcare
Support Forum: www. sane.org.uk/what_we_do/support/supportforum
sane.org.uk/what_we_do/support/supportforum
Website: www.sane.org.uk
Support Line
They offer confidential emotional support to children, young adults and adults by telephone, email and post. They work with callers to develop healthy, positive coping strategies, an inner feeling of strength and increased self-esteem to encourage healing, recovery and moving forward with life. Their opening hours vary so you need to ring them for details.
Telephone: 01708 765200
E-mail: [email protected]
Website: www.supportline.org.uk
CALM (Campaign Against Living Miserably)
CALM is leading a movement against suicide. They offer accredited confidential, anonymous and free support, information and signposting to people anywhere in the UK through their helpline and webchat service.
Telephone: 0800 58 58 58
Webchat: through the website
Website: www. thecalmzone.net
thecalmzone.net
My Black Dog
Provides peer support webchat with volunteers who have experienced mental illness. Available evenings and weekends. Check the website for opening times.
Website: www.myblackdog.co
Papyrus UK
Work with people under 35 who are having suicidal feelings. And with people who are worried about someone under 35.
Telephone: 0800 068 41 41
Email: [email protected]
Text: 07786 209697
Website: www.papyrus-uk.org
Shout
If you’re experiencing a personal crisis, are unable to cope and need support, text Shout to 85258. Shout can help with urgent issues such as suicidal thoughts, abuse or assault, self-harm, bullying and relationship challenges.
Text: Text Shout to 85258
Website: www.giveusashout.org/
Need more advice?
If you need more advice or information you can contact our Advice and Information Service.
Contact us Contact us
More resources
10 Signs of Pure "Evil"
A discussion of delusions, hallucinations, and psychotic disorders can be complicated.
For most people, psychosis is difficult to understand and live with, especially when a person threatens your livelihood and/or your life.
This article will discuss some of the behaviors and characteristics that can be very threatening to others.
It can be extremely difficult to identify the differences between mental illness and a personality disorder.
Skilled mental health professionals also struggle with identification and treatment of individuals with co-occurring disorders such as mental illness (i.e., bipolar disorder, depression, anxiety, etc) and a personality disorder (i.e., borderline personality disorder, narcissism, or sociopathy). What do you treat first? The personality disorder or the mental illness? Can we treat both? Sometimes we can and sometimes we cannot.
These women struggled for many years trying to determine the best course of action. I remember asking why it was so difficult for them to identify what was needed to save not only themselves but their children.
Paranoid or delusional behavior may be a sign of a mental illness and a personality disorder
Over the course of the 9 years I have been doing psychotherapy, I have worked with at least 8 women who were trying to cope with their husbands who displayed delusional thinking patterns and paranoia. These women had more than one thing in common. All 8 of these women struggled with fear, uncertainty, confusion, blame, doubt, anger and resentment, anxiety, depression, and conflicted emotions and thoughts about divorcing or leaving their spouse.
Sadly, delusional thinking and paranoia can also be a personality disorder ( a chronic pattern of behaviors that cannot be easily changed with therapy or affected by medication) and not a psychotic disorder (a mental illness that can be altered by medication and therapy). As a result, the delusional thought patterns and paranoia may not go away so easily.
As a result, the delusional thought patterns and paranoia may not go away so easily.
Behaviors of a psychologically or emotionally disturbed individual can tear families apart
I have listed 10 things I believe makes it difficult to trust, care for, live with, and help someone with delusional and paranoid thinking patterns:
- They threaten violence and feel empowered: Threatening violence not only causes fear and anger but also confusion. Although the majority of individuals with psychotic disorders do not threaten violence (according to research), when they do, it causes confusion. It also causes anger because no one wants to be threatened.
- They are pathological liars and simply don’t care: It is certainly difficult to cope or live with someone who is displaying delusional thought patterns and paranoia. But it can be equally (if not more) difficult to live with someone who is also lying and engaging in lying on a frequent basis.
 Pathological lying may occur for no reason at all. Here is an article I wrote on the topic a few years ago. Pathological lying not only complicates the world of the individual with delusional patterns of thinking but also complicates the world of those around them.
Pathological lying may occur for no reason at all. Here is an article I wrote on the topic a few years ago. Pathological lying not only complicates the world of the individual with delusional patterns of thinking but also complicates the world of those around them. - They are manipulative and cunning: If delusional thought patterns are coupled with manipulative and cunning behaviors that put others in jeopardy or harm them, it can be extremely difficult to show compassion or understanding toward this person. Can you blame them? Cunning, manipulative, or spiteful behaviors are premeditated and thought out. They are not a symptom of the illness. They are more so a characteristic of the person’s personality.
- They are sociopathic: Sociopathic traits often include pathological lying, social charm and glib, manipulation, lack of empathy or concern for the rights of others, behavioral problems, insensitivity, arrogance, etc. In some cases, delusional and paranoid thought patterns coupled with sociopathic traits can be very difficult for others to live with.
 In many cases, these individuals end up isolated from society.
In many cases, these individuals end up isolated from society. - They refuse treatment to prove a point: It can be very difficult to live a life with someone, who is experiencing delusions or paranoia, who refuses psychiatric treatment. Refusing treatment means that the person does not think they need help when everyone around them does. How can you live with someone refusing treatment? You can’t.
- They have a history of violence and severe aggression: Research suggests that a history of violence means that future violence is more likely. Someone who has difficulty with reality testing and seeing things as they truly are can really become a threat to others around them. For example, a previous client of mine struggled with getting her husband to agree to medication management and therapy. Despite him having a tendency toward challenging police and attempting to harm a neighbor with violence, he refused treatment. This led to a very complicated and overwhelming divorce.
 She could not live with him and did not feel safe letting her children stay with him.
She could not live with him and did not feel safe letting her children stay with him. - They disrespect authority of any kind: Some individuals challenge authority, even authority figures who are on their side. As I stated above, some individuals with a history of violence refuse treatment because they don’t believe they need it. Others refuse treatment because they are being difficult and oppositional. Still others may refuse medication because of side effects, horror stories they have heard, or fear. Either way, individuals who disrespect or undermine authority are difficult to have a life with. They are not willing to (or cannot) make proper decisions which can put everyone, including them, in harms way.
- They are substance abusers with a propensity toward criminal mischief: Could you live with someone who displayed delusional and paranoid thought patterns, refuses medication or treatment, and then abuses alcohol or drugs? Most people could not.
 Sadly, self-medication is not a shocker in the lives of those struggling with delusions or paranoia. In cases such as these, safety is a major challenge because not only does the individual think they are thinking appropriately and do not need treatment, but they also believe that the alcohol or drug(s) calms them or helps them cope. In some cases, it may. But in many other cases it does not.
Sadly, self-medication is not a shocker in the lives of those struggling with delusions or paranoia. In cases such as these, safety is a major challenge because not only does the individual think they are thinking appropriately and do not need treatment, but they also believe that the alcohol or drug(s) calms them or helps them cope. In some cases, it may. But in many other cases it does not. - They have strong delusions that results in family discord: “Strong delusions” (as I call them) are delusions that can result in the individual threatening violence or trying to harm someone else. For example, a husband may have a strong delusion that his wife has teamed up with the FBI to kill him. This delusion can result in an act of violence or rage toward the wife. I once counseled a woman whose husband threatened to kill her if he ever found her talking to the FBI. One she had been talking to a long distance friend and he walked in the room accusing her of talking to the police and FBI about some secrete “data” he had on his computer.
 The situation was extremely difficult to navigate because his delusions were not bizarre (i.e., they were not abnormal because he did have “secret data” on his computer for his job) and he seemed very cognizant outside of this strong delusion.
The situation was extremely difficult to navigate because his delusions were not bizarre (i.e., they were not abnormal because he did have “secret data” on his computer for his job) and he seemed very cognizant outside of this strong delusion. - They display complex Borderline Personality Disorder traits and enjoy the chaos they create: Borderline traits can make delusional thought patterns 10x worse. Because individuals with a diagnosis of BPD already struggle with regulating and controlling emotions, navigating relationships, and coping with negative thought patterns, delusional thought patterns and paranoia can make things worse. For more information on the symptoms of BPD, visit the National Alliance for Borderline Personality Disorder thanks to a visitor from last week’s article.
What has been your experience with this topic? Would you be able to identify someone who could be dangerous to you? What would you do if you needed to protect yourself from them? Although the percentage of violence in people with severe mental illness, it does exist and we cannot ignore it or sweep it under the carpet. It exists. Sometimes it exists right around the corner. We must be aware of this and willing and ready to act.
It exists. Sometimes it exists right around the corner. We must be aware of this and willing and ready to act.
As always, looking forward to connecting with you.
All the best
Like this:
Like Loading...
Types of personality disorders and features of their treatment. Paranoid, schizoid, dissocial, hysterical disorder, obsessive-compulsive, obsessive-compulsive, anxious, narcissistic
The main feature of personality disorders are pronounced maladaptive features of the psyche - such patients do not know how and cannot get along with others, adapt to new conditions. Previously, personality disorders were called psychopathy, but over time, experts adopted a Western point of view - psychopathy is still a separate mental disorder. There are several types of personality disorders, sometimes there are mixed types of the disease. Treatment should only be carried out by experienced professionals, but the main problem with this disorder is that patients for the most part do not recognize their mental problems.
Submit an application for diagnosis and treatment
I confirm that I accept the terms of consent to the processing of personal data.
Types of personality disorders and features of their treatment
Every fifteenth inhabitant of our planet suffers from a personality disorder. Moreover, he himself hardly perceives his condition as a disease that requires an appeal to specialists. He will justify all his actions and consider his behavior normal. Treatment denies, and the consequences are unpredictable.
Personality disorder: adjustment difficulties
Personality disorder is a maladaptive pattern of behavior caused by a persistent mental disorder that is not associated with a physical or neurological disease. This pathology is difficult to correct, because the patient does not believe that he needs treatment. There is no motivation, which is a catalyst for positive changes. The individual himself does not seek to get rid of the violation and does not make good contact with psychotherapists. Late appeal to specialists leads to the fact that the patient gets an appointment with a psychiatrist already in the stage of deep neglect of the disease. It can be difficult to relieve symptoms and cure. The first signs of the disease are actively manifested in adolescence. Before this period, individual episodes are possible, but only after the period of puberty can we talk about the problem. Individuals with cognitive personality disorder do not understand why others talk about any of their problems. After all, they believe that behavior and actions are normal. People with personality disorders are poorly perceived in society. They often have difficulties in personal communication. But at the same time, patients do not feel pangs of remorse and have no sympathy for others. After a certain time, their relationship with the world is built not according to the principle of personal adaptation to society, but according to the scheme, when the society is forced to accept or not accept a problematic person.
The individual himself does not seek to get rid of the violation and does not make good contact with psychotherapists. Late appeal to specialists leads to the fact that the patient gets an appointment with a psychiatrist already in the stage of deep neglect of the disease. It can be difficult to relieve symptoms and cure. The first signs of the disease are actively manifested in adolescence. Before this period, individual episodes are possible, but only after the period of puberty can we talk about the problem. Individuals with cognitive personality disorder do not understand why others talk about any of their problems. After all, they believe that behavior and actions are normal. People with personality disorders are poorly perceived in society. They often have difficulties in personal communication. But at the same time, patients do not feel pangs of remorse and have no sympathy for others. After a certain time, their relationship with the world is built not according to the principle of personal adaptation to society, but according to the scheme, when the society is forced to accept or not accept a problematic person. The lack of motivation and desire to be treated exacerbates the problem, since not every doctor can find an approach to such a patient, relieve the symptoms of exacerbation and help get rid of the problem.
The lack of motivation and desire to be treated exacerbates the problem, since not every doctor can find an approach to such a patient, relieve the symptoms of exacerbation and help get rid of the problem.
Specific personality disorders
In Soviet times, overly emotional individuals were often called psychopaths. Such a characterization and classification was not inherent in Western psychiatry. Psychopathy is a serious violation of a behavioral nature, in which, against the background of underdevelopment of a number of personality traits, one clearly dominates. This includes a number of deviations. Types of personality disorders:
- § Paranoid - the patient is dominated by overvalued ideas. He attaches special importance to his personality. But he treats others with hostility, suspecting them of malicious intent. A person with a pathology does not recognize its presence. When relatives or friends pay attention to a cognitive deviation and try to take him to a specialist, he will assure that everything is in order with him and deny the existence of a problem.
 Very sensitive to criticism.
Very sensitive to criticism. - § Schizoid - this diagnosis is characterized by introversion, isolation, decreased interest in life's things. The patient does not perceive the accepted norms of social behavior, often behaves eccentrically. Schizoid personality disorders are associated with a great passion for some kind of activity in which the individual succeeds. For example, he may be pathologically addicted to various health systems, to the point of attracting other people to his interests. Experts believe that in this way a certain asociality is replaced. Also, such patients may have problems with alcohol, drugs or other types of addiction.
- § Dissocial - a characteristic feature of this personality disorder is the patient's cognitive defiant behavior in order to get what he wants. With all this, such patients are able to win over people, including doctors. This type is especially pronounced in late adolescence.
- § Hysterical - the main goal of such patients is to draw attention to their person in any way, including defiant behavior.
 The diagnosis is more typical for women. Atypical capriciousness, inconstancy of desires, extravagance, deceit are observed. In order to attract attention, the patient invents non-existent diseases for himself, the symptoms of which can be given out by the autonomic system and which is difficult to remove.
The diagnosis is more typical for women. Atypical capriciousness, inconstancy of desires, extravagance, deceit are observed. In order to attract attention, the patient invents non-existent diseases for himself, the symptoms of which can be given out by the autonomic system and which is difficult to remove. - § Obsessive-compulsive - patients with this type of personality disorder pathologically strive for order and perfection. They have no sense of humor, they try to be perfect in everything. When the set ideal goals are not achieved, they can fall into depressive states.
- § Anxiety - such a personality disorder is characterized by the cultivation of a personal inferiority complex. Patients are in a state of perpetual anxiety and uncertainty. From childhood, such patients are shy and timid. Often suspect others of hostility. They are prone to depression.
- § Narcissistic - a deviation in which a person manifests narcissism from childhood, a desire to be constantly admired.
 Such a patient does not accept criticism: he reacts to it either with resentment or with aggression. Indifferent to the feelings of other people, prone to exploiting them to achieve their own goals.
Such a patient does not accept criticism: he reacts to it either with resentment or with aggression. Indifferent to the feelings of other people, prone to exploiting them to achieve their own goals.
Different forms of psychopathy require an individual approach to treatment. Personality disorders should not be confused with character accentuation. In the latter case, a person also has behavioral features, but they lie within the upper limit of the norm. In addition, it is adapted to social conditions. The classification of classical psychopathy is inappropriate here. Diagnosis and types are different.
Causes that cause personality and behavioral disorders
All specific personality disorders are usually divided into three clusters. Their classification:
- § types of cluster A psychopathy: paranoid and schizoid;
- § Cluster B psychopathy: hysterical, asocial, narcissistic;
- § Types of cluster B psychopathy: obsessive-compulsive, depressive.
The causes of cluster A psychopathy are considered to be genetic and hereditary. The fact is that among the relatives of patients who have a personality disorder, as a rule, there is at least one with schizophrenia. A hereditary predisposition to pathologies can also be traced in cluster B and C psychopathy. The first option can also be aggravated by problems with alcohol: in families of people who drink, children often develop with disorders. There is a version that cognitive specific personality disorders may be associated with hormonal disorders in the body. If a person has elevated levels of testosterone, estrone and estradiol, the consequences of this are manifested in the form of aggression. In addition, he does not produce enough endorphins, which, in turn, leads to depressive disorders. The social factor also plays an important role in the formation of the psychotype. For active children, space is important. If they are forced to be brought up in a closed space, small areas, this leads to the appearance of hyperactivity. Anxious babies from birth can become balanced if they are raised by emotionally stable parents. A calm mother can help a child become confident, and an anxious one can not remove, but increase his personal anxiety state. Character traits become noticeable already in early childhood. In adolescence, they can already develop as a personality disorder. Cognitive impairment is manifested in a decrease in memory, increased fatigue. Pathologies of the nervous system are observed more often in people with an asocial temperament.
Anxious babies from birth can become balanced if they are raised by emotionally stable parents. A calm mother can help a child become confident, and an anxious one can not remove, but increase his personal anxiety state. Character traits become noticeable already in early childhood. In adolescence, they can already develop as a personality disorder. Cognitive impairment is manifested in a decrease in memory, increased fatigue. Pathologies of the nervous system are observed more often in people with an asocial temperament.
Mixed personality disorder
This type of psychopathy has been less studied than others. The classification has no special criteria. The patient manifests forms of one or the other type of disorders that are not persistent. Therefore, this type of disorder is also called mosaic psychopathy. But it is also difficult for a person with a mixed type of disorder to get along in society because of the peculiarities of their behavior. Instability of character is often the basis that contributes to the development of various types of addiction. Mixed personality disorder may be accompanied by alcoholism, drug addiction, gambling addiction. Mosaic psychopathy can combine symptoms of the schizoid and paranoid types. Such people do not know how to build social contacts in society, they are obsessed with overvalued ideas. With the predominance of paranoid symptoms, patients suffer from increased suspicion. They are prone to scandals, threats, like to write angry complaints about everyone and everything. Specialists are alarmed if signs (classification) of several disorders coexist in one patient: schizoid, hysterical, asthenic, excitable. In this case, there is a high risk of developing schizophrenia. Brain injuries or complications after a number of diseases can lead to mosaic types of pathology. This mixed personality disorder is considered acquired. If we consider the situation in detail, it will look like this: a person already has an innate tendency to mosaic psychopathy, which, due to certain circumstances, is superimposed by organic pathology.
Instability of character is often the basis that contributes to the development of various types of addiction. Mixed personality disorder may be accompanied by alcoholism, drug addiction, gambling addiction. Mosaic psychopathy can combine symptoms of the schizoid and paranoid types. Such people do not know how to build social contacts in society, they are obsessed with overvalued ideas. With the predominance of paranoid symptoms, patients suffer from increased suspicion. They are prone to scandals, threats, like to write angry complaints about everyone and everything. Specialists are alarmed if signs (classification) of several disorders coexist in one patient: schizoid, hysterical, asthenic, excitable. In this case, there is a high risk of developing schizophrenia. Brain injuries or complications after a number of diseases can lead to mosaic types of pathology. This mixed personality disorder is considered acquired. If we consider the situation in detail, it will look like this: a person already has an innate tendency to mosaic psychopathy, which, due to certain circumstances, is superimposed by organic pathology. Mosaic disorder requires specific treatment only when symptoms worsen, or if there is organic build-up. Then neuroleptics, tranquilizers, vitamins can be prescribed by a specialist.
Mosaic disorder requires specific treatment only when symptoms worsen, or if there is organic build-up. Then neuroleptics, tranquilizers, vitamins can be prescribed by a specialist.
Infantile personality disorder
With this type of psychopathy, signs of social immaturity are pronounced. A person is not able to withstand stressful situations and relieve tension. In difficult circumstances, he does not control his emotions in the same way as children do. Infantile personality disorders for the first time clearly declare themselves in adolescence. Hormonal storms that occur at this time with a person cause changes in the psycho-emotional sphere. As you get older, the diagnosis can only progress. It is possible to finally talk about the presence of the disease only after reaching 16-17 years. In stressful circumstances, the patient manifests himself immature, poorly controls aggression, anxiety, fear. Such a person is not hired for military service, they are denied employment in law enforcement agencies. Permits to carry weapons or obtain a driver's license are decided on a limited and strictly case-by-case basis, according to an assessment of signs and condition.
Permits to carry weapons or obtain a driver's license are decided on a limited and strictly case-by-case basis, according to an assessment of signs and condition.
Transient personality disorder
This diagnosis refers to borderline conditions, when the symptoms of deviation are difficult to attribute to any type of personality disorder. The main causes of psychopathy are long-term stressful situations. In the modern world, a person is surrounded by many unfavorable factors: troubles at work, military operations, difficult family circumstances, financial failures, moving... All this disrupts the usual way of life and unbalances. If such circumstances last too long, the human psyche does not always have a reserve to survive and overcome them. Transient personality disorder has its own characteristics:
- § disorientation;
- § hallucinations;
- § nonsense;
- § inhibition of verbal and motor functions.
Even one of the symptoms can already signal a disorder. This diagnosis is special in that the disease does not last too long: sometimes only a day, and sometimes a month. It suddenly arises and just as it passes. Sometimes a person can go to sleep with a disturbance, and get up in a normal emotional state with residual effects in the form of increased anxiety or sleep disturbances. With each new stress, a spontaneous return of pathology is possible. Such a diagnosis does not pass without a trace. In the event that there are signs of delirium or hallucinations, such a person requires special treatment, because his condition can also threaten those around him. In the period between exacerbations, the patient experiences emotional burnout, in which nerve cells are also destroyed. Therefore, even for preventive purposes, it is recommended to take vitamins and herbal remedies. As historical examples show, partial transient personality disorder is not a benign condition. Many of the famous serial killers and maniacs had this diagnosis. They led a normal life, had families, work, but during the period of exacerbations they committed crimes.
This diagnosis is special in that the disease does not last too long: sometimes only a day, and sometimes a month. It suddenly arises and just as it passes. Sometimes a person can go to sleep with a disturbance, and get up in a normal emotional state with residual effects in the form of increased anxiety or sleep disturbances. With each new stress, a spontaneous return of pathology is possible. Such a diagnosis does not pass without a trace. In the event that there are signs of delirium or hallucinations, such a person requires special treatment, because his condition can also threaten those around him. In the period between exacerbations, the patient experiences emotional burnout, in which nerve cells are also destroyed. Therefore, even for preventive purposes, it is recommended to take vitamins and herbal remedies. As historical examples show, partial transient personality disorder is not a benign condition. Many of the famous serial killers and maniacs had this diagnosis. They led a normal life, had families, work, but during the period of exacerbations they committed crimes. When Western experts studied the brains of executed criminals, they did not find significant changes in it. All its parts corresponded to the norm of a healthy person. And only stressful conditions could lead to the appearance of signs of a personality disorder, which entailed antisocial acts. Perhaps, if during the period when the first signs of the disease appeared, there would have been a person nearby who noticed this and helped to contact a specialist, such consequences could have been avoided. Being face-to-face with continuous stressful situations, the psyche simply could not stand it. The mechanism of the development of the disease was launched.
When Western experts studied the brains of executed criminals, they did not find significant changes in it. All its parts corresponded to the norm of a healthy person. And only stressful conditions could lead to the appearance of signs of a personality disorder, which entailed antisocial acts. Perhaps, if during the period when the first signs of the disease appeared, there would have been a person nearby who noticed this and helped to contact a specialist, such consequences could have been avoided. Being face-to-face with continuous stressful situations, the psyche simply could not stand it. The mechanism of the development of the disease was launched.
Treatment for personality disorders
When a person is diagnosed with psychopathy, they rarely agree with it. The peculiarity of this disease is that the patient does not see problems in himself, but looks for them in others. Treatment in this case is always difficult. According to statistics, only one in five of them agree to accept help. Treatment of psychopathy is carried out individually. It includes sessions of psychotherapy and, if necessary, the use of drugs. In difficult cases, when the antisocial behavior of the patient poses a threat to others, treatment can be carried out in a hospital. Disputes among specialists are caused by the treatment of borderline conditions. Some believe that the patient needs help only during exacerbations, while others insist on constant support. In any case, the treatment of psychopathy has been going on for many years. With the patient's tendency to impulsive acts that can threaten life and health, psychotropic drugs are connected.
Treatment of psychopathy is carried out individually. It includes sessions of psychotherapy and, if necessary, the use of drugs. In difficult cases, when the antisocial behavior of the patient poses a threat to others, treatment can be carried out in a hospital. Disputes among specialists are caused by the treatment of borderline conditions. Some believe that the patient needs help only during exacerbations, while others insist on constant support. In any case, the treatment of psychopathy has been going on for many years. With the patient's tendency to impulsive acts that can threaten life and health, psychotropic drugs are connected.
How to recognize schizotypal personality disorder and what to do next
July 3, 2021LikbezZdorovye
This disorder is not yet schizophrenia. But dangerously close to her. What is Schizotypal Personality Disorder? For example, regularly behaves too provocatively or tactlessly. Or it can be too eccentric - to such an extent that it scares and even repels others.
The person with schizotypal personality disorder feels that something is wrong in his relationship with others. However, he is unable to understand the reason. In order to somehow explain the problems in relationships, he creates for himself a kind of alternative reality in which the people around him envy him and his talents, wish bad things. Why are there people - in the ideas of such a person, the whole world is full of evil forces that want to poison the life of him, the representative of the good side.
How to recognize schizotypal personality disorder
Eccentricity or distrust of others does not mean that a person has schizotypal disorder. A diagnosis can only be assumed if it exhibits at least five of the ten most characteristic symptoms of the disorder. Here they are:
- Tendency to loneliness, lack of trusting relationships with anyone outside the family .
- Inappropriate, inappropriate emotional reactions .
 For example, a person may laugh out loud at a funeral after accidentally remembering a funny scene involving the deceased. Or remain gloomy and dissatisfied when everyone around is happy.
For example, a person may laugh out loud at a funeral after accidentally remembering a funny scene involving the deceased. Or remain gloomy and dissatisfied when everyone around is happy. - Excessive and persistent social anxiety . Offended position "no one can understand and appreciate me."
- Inadequate interpretation of events around . They are given too much personal importance. For example, a person is sure that if the neighbors started repairs, it is only to annoy him with noise and dust. And if one of the acquaintances did not accidentally say hello on the street, then it was definitely because he wanted to express his hatred.
- Eccentric beliefs and mannerisms . Let's say a person with a disorder can be sure that special services are following him. Or that acquaintances always need to tell the truth in the eye - and do it straightforwardly, even to the point of tactlessness.
- Suspicion of others .
 Even if one of the acquaintances sincerely tries to please or help, a person with schizotypal disorder will look for malicious intent in his motives.
Even if one of the acquaintances sincerely tries to please or help, a person with schizotypal disorder will look for malicious intent in his motives. - Belief in personal supernatural powers . “I see through everyone”, “I have prophetic dreams”, “I have magical abilities, damn it, it won’t seem enough” - this is a conviction from a schizotypal arsenal.
- Unusual sensations experienced . A person may claim to feel the presence of someone who is actually very far away. Or tell them that they physically feel the approach of danger.
- Unique appearance . For example, tousled hair of a bright color. Unusually fitting or deliberately unkempt clothing. Confidence that you can not wash for months and be proud of the natural smell of the body.
- Unusual way of speaking . Suppose a person can mumble something incoherently to the side. Or speak by singing the words.
How schizotypal personality disorder differs from schizophrenia
Some manifestations of schizotypal personality disorder do resemble the symptoms of schizophrenia. For example, the same sincere belief that caring relatives really only think about how to add poison.
For example, the same sincere belief that caring relatives really only think about how to add poison.
For this reason, schizotypy is sometimes considered a milder form of schizophrenia than the classical form.
However, there is a subtle difference. If a schizophrenic lives in a world full of delusions and hallucinations, then a person with schizotypal disorder is more rational. He may believe he has some supernatural powers. But it is unlikely that he will be told that at night the aliens reprogram his brain, and the iron, in his absence, deliberately turns on tiny green devils.
In addition, schizotypal disorder does not interfere with social adaptation too much. Such a person can even become popular - an artist, musician, artist, writer, teacher, and his oddities will be perceived as signs of genius.
Where does schizotypal personality disorder come from
As in the case of other mental disorders, scientists admit that they do not yet know.
Schizotypal disorder usually presents in early adulthood and is most likely caused by several factors.
1. Heredity
The tendency to schizotypal disorders and schizophrenia is often inherited. Which gene is responsible for this is not yet clear.
2. Experienced stresses
Emotional trauma in childhood or chronic stress increases the risk of developing schizotypy.
3. Some features of a person's personality
Someone experiences stress relatively easily, but for someone, a catastrophe is seen in every trouble. The latter have a significantly higher risk of schizotypal disorder than the former.
Why schizotypal personality disorder is dangerous
Not only possible social isolation and lack of close friends. Experts from the American medical organization Mayo Clinic argue that schizotypal personality disorder, if not corrected, can lead to serious trouble. For example:
- depression;
- high-grade schizophrenia;
- development of other personality disorders;
- nervous breakdowns in response to elemental stress;
- alcohol and drug problems;
- suicide attempts.
What to do if you suspect schizotypal disorder
People with schizotypal disorder usually do not see the need to see a psychotherapist. After all, they are sure that everything is in order with them - it is those around them that are unpleasant and bad.
In this case, relatives and friends, if any, play an important role. Their task is still to convince a loved one to consult a specialist.
The easiest way to do this is to wait for the moment when a black streak begins in the life of a person with a disorder. For example, he realizes that he is not able to enjoy his own success, or he will face another fictitious betrayal of someone whom he seems to have just begun to trust. As soon as this happens, you need to take a loved one by the hand and lead them to talk to a “good person” - a psychotherapist.
One conversation is enough for a specialist to make a preliminary diagnosis. Then he will be able to recommend several ways to improve life.