Aversion therapy definition psychology
What It Is, Efficacy, Controversy, and More
Aversion therapy, sometimes called aversive therapy or aversive conditioning, is used to help a person give up a behavior or habit by having them associate it with something unpleasant.
Aversion therapy is most known for treating people with addictive behaviors, like those found in alcohol use disorder. Most research has been focused on its benefits relating to substance use.
This type of therapy is controversial and research is mixed. Aversion therapy isn’t often a first-line treatment and other therapies are preferred.
How long the therapy lasts for has also been criticized, as outside of the therapy, relapse may occur.
Aversion therapy is based off the theory of classical conditioning. Classical conditioning is when you unconsciously or automatically learn a behavior due to a specific stimuli. In other words, you learn to respond to something based on repeated interactions with it.
Aversion therapy uses conditioning but focuses on creating a negative response to an undesirable stimulus, such as drinking alcohol or using drugs.
Many times, in people with substance use disorders, the body is conditioned to get pleasure from the substance — for instance, it tastes good and makes you feel good. In aversion therapy, the idea is to change that.
The exact way aversion therapy is performed depends on the undesirable behavior or habit that’s being treated. One commonly used aversive therapy is chemical aversion for alcohol use disorder. The goal is to reduce a person’s craving for alcohol with chemically-induced nausea.
In chemical aversion, a doctor administers a drug that causes nausea or vomiting if the person being treated drinks alcohol. They then give them alcohol so that the person gets sick. This is repeated until the person begins to associate drinking alcohol with feeling ill and thus no longer craves alcohol.
Other methods that have been used for aversion therapy include:
- electrical shock
- another type of physical shock, like from a rubber band snapping
- an unpleasant smell or taste
- negative imagery (sometimes through visualization)
- shame
Can you do aversion therapy at home?Traditional aversion therapy is done under the supervision of a psychologist or other therapist.
You can, however, use aversion conditioning at-home for simple bad habits, such as biting your nails.
To do this, you can place a clear coat of nail polish on your nails, which will taste bad when you go to bite them.
Aversion therapy is believed to be helpful for people wanting to quit a behavior or habit, typically one that’s interfering with their life negatively.
While a lot of research has been done on aversion therapy and alcohol use disorder, other uses for this type of therapy have included:
- other substance use disorders
- smoking
- eating disorders
- oral habits, such as nail biting
- self-injurious and aggressive behaviors
- certain inappropriate sexual behaviors, such as voyeuristic disorder
Research on these applications is mixed. Some, like lifestyle behaviors, have been generally shown as ineffective. More promise has been found for addiction when using chemical aversion.
Some research has shown that aversion therapy is effective for treating alcohol use disorder.
Recent research found that participants who craved alcohol prior to the therapy reported avoiding alcohol 30 and 90 days after treatment.
Yet, research is still mixed on the effectiveness of aversion therapy. While many studies have shown promising short-term results, the long-term effectiveness is questionable.
While the previously mentioned study found that 69 percent of participants reported sobriety 1 year after treatment, a longer-term study would help to see if it lasted past that first year.
In some of the most comprehensive research on aversion therapy in the 1950s, researchers noted a decline in abstinence over time. After 1 year, 60 percent remained alcohol-free, but it was only 51 percent after 2 years, 38 percent after 5 years, and 23 percent after 10 years or more.
It’s believed that the lack of long-term benefit occurs because most aversion therapy happens in-office. When you’re away from the office, the aversion is harder to maintain.
While aversion therapy may be effective in the short-term for alcohol, there have been mixed results for other uses.
Most research has found aversion therapy to be unhelpful for smoking cessation, especially when the therapy involves rapid smoking. For example, a person would be asked to smoke an entire pack of cigarettes in a very short amount of time until they feel ill.
Aversion therapy has also been considered for treating obesity, but it was extremely hard to generalize to all foods and maintain outside of the therapy.
Aversion therapy has had backlash in the past for several reasons.
Some experts believe that using negative stimulus in aversion therapy is equal to using punishment as a form of therapy, which is unethical.
Before the American Psychiatric Association (APA) deemed it an ethical violation, some researchers used aversion therapy to “treat” homosexuality.
Prior to 1973, homosexuality was considered a mental illness in the Diagnostic and Statistical Manual of Mental Disorders (DSM). Some medical professionals believed that it was possible to “cure” it. A homosexual person could be imprisoned or potentially forced into a program of aversion therapy for revealing their orientation.
A homosexual person could be imprisoned or potentially forced into a program of aversion therapy for revealing their orientation.
Some people did voluntarily seek this or other types of psychiatric therapy for homosexuality. This was often due to shame and guilt, as well as societal stigma and discrimination. However, evidence showed that this “treatment” was both ineffective and harmful.
After the APA removed homosexuality as a disorder due no scientific evidence, most research on aversion therapy for homosexuality stopped. Yet, this harmful and unethical use of aversion therapy left it with a bad reputation.
Aversion therapy may be helpful for stopping specific types of unwanted behaviors or habits. Yet, experts believe that even if used, it shouldn’t be used alone.
Aversion therapy is a type of counterconditioning treatment. A second one is called exposure therapy, which works by exposing a person to something they fear. Sometimes these two types of therapies can be combined for a better outcome.
Therapists may also recommend other types of behavioral therapy, along with in or outpatient rehabilitation programs for substance use disorders. For many people who experience addiction, support networks can also help to keep them on track with recovery.
Medication may be prescribed in some cases, including for smoking cessation, mental health conditions, and obesity.
Aversion therapy aims to help people stop undesirable behaviors or habits. Research is mixed on its uses, and many doctors may not recommend it due to criticism and controversy.
You and your healthcare provider can discuss the right treatment plan for you, whether that includes aversion therapy or not. Often, a combination of treatments including talk therapy and medication can help you cope with your concern.
If you have a substance use disorder or believe you may be experiencing addiction, reach out to a healthcare provider. If you’re not sure where to start, you can call SAMHSA’s National Helpline at 800-662-4357.
5 Examples of Aversion Therapy
What is aversion therapy and what are some examples of this therapeutic approach? The subject of our post here truly is a unique concept in behavior modification approaches. For those interested, let’s take a closer look.
The Basics of Aversion Therapy
Aversion is the predisposition of one to not like or even be deterred by a specific object or concept. Consequently, therapy through aversion is defined as “therapy intended to suppress an undesirable habit or behavior by associating the habit or behavior with a noxious or punishing stimulus.”
In other words, aversion therapy is a way of fixing bad habits. Whether it’s smoking, drinking, gambling or overeating, aversion therapy can be utilized to re-direct your urges and stop unwanted behaviors.
Aversion therapy is used by many professionals in the field of psychology, including counselors, addiction therapists and even licensed hypnotists. It can be a specialization or just one of many forms of treatment offered at a clinic or rehab facility. You might also see it called “aversive therapy” or “aversive conditioning.”
You might also see it called “aversive therapy” or “aversive conditioning.”
Important note: Aversion therapy is sometimes referred to as a “habit reversal method,” but this label isn’t exclusive to aversion therapy and can include other methods unrelated to it.
The Pros and Cons of Aversion Therapy
As with any psychological treatment, there are both pros and cons to aversion therapy.
One of the biggest benefits is related to brain chemistry. The principle behind aversion therapy is that it changes the brain’s response to certain stimuli, so instead of associating an unwanted habit with good things like satisfaction or stress relief, you’ll associate it with bad things like shocks, noises and unpleasant images. In scientific terms, this is called “reducing positive cues.” It means that you aren’t just avoiding or exercising self-control over bad habits; you’re rewiring the way that your brain sees them on a fundamental level.
Another potential advantage to aversion therapy is its effectiveness. It’s seen good results in a number of clinical trials related to smoking, drinking and weight loss. While it hasn’t been studied as much as other techniques, there’s enough evidence to call it an established method for breaking bad habits.
It’s seen good results in a number of clinical trials related to smoking, drinking and weight loss. While it hasn’t been studied as much as other techniques, there’s enough evidence to call it an established method for breaking bad habits.
The cons of aversion therapy are usually related to ethics. There’s an ongoing debate over the morality of aversion therapy, especially in the context of doctors delivering painful treatments to their patients. This question becomes especially relevant when the patient is an addict who might be vulnerable and not in their right mind to truly consent.
Ultimately, however, aversion therapy is an accepted practice among today’s physicians. It’s a non-invasive behavior modification method that has shown good results in trials and through patient testimonials, and there are many ways to customize aversion therapy for people from all walks of life.
Having covered the basics of what this type of therapy actually is, let’s now move on to examples of it in use.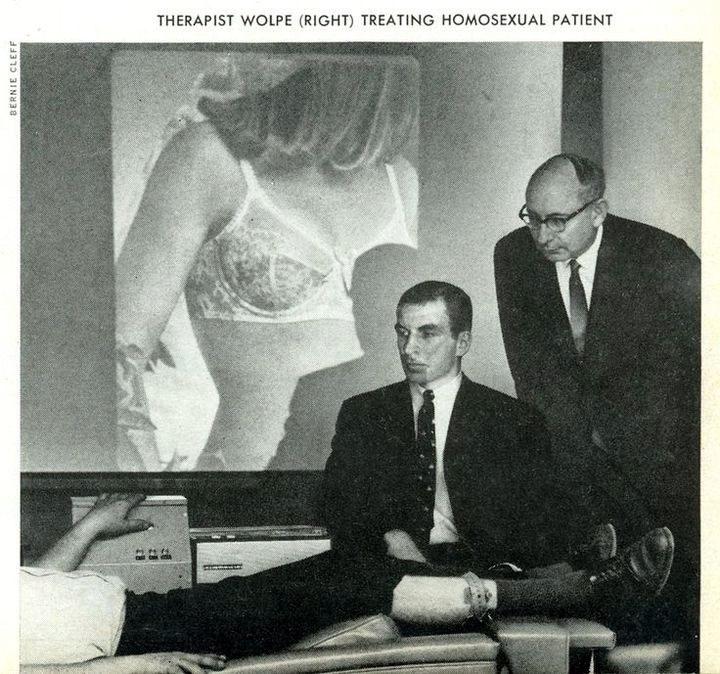
To Stop Nail Biting
Nail biting is a rather common, habitual behavior that affects many people of all ages. Some can stop the habit at the outset of the resolution to do so. On the other hand, many others can really struggle to stop the habit.
Aversion therapy here typically involves the introduction of some unpleasant element to the process. Some people apply a bitter or foul-tasting substance to the nail area so as to remind and deter the habitual offender. Others deliver a mildly painful punishment to themselves, such as a pinch or an ice cube, that serves as a negative counteraction to the nail biting.
There are even “behavior training devices” that can be worn on the body to deliver mild shocks whenever you find yourself gnawing on your nails. As with other aversion techniques, the idea is that the brain will come to associate nail biting with unpleasant stimuli and will try to avoid that stimuli in the future.
Another kind of aversion therapy for nail biting may involve placing tape over the nails or wrapping it around the fingertips. The inconvenience of unwrapping the nails for the purpose of biting then acts as the deterrent. Fittingly, this is called the “deterrent method,” which is sometimes distinguished as a special subset of aversion therapy.
The inconvenience of unwrapping the nails for the purpose of biting then acts as the deterrent. Fittingly, this is called the “deterrent method,” which is sometimes distinguished as a special subset of aversion therapy.
Studies with aversion therapy for nail biting have shown great promise. Whether it’s applying unpleasant substances to the nails or covering them up to make them inaccessible, many nail biters have seen success with the aversion method.
To Stop Smoking
People have employed countless measures in the fight to break free of the addiction of nicotine and tobacco products. When many of these more common approaches fail, sufferers often revert to other endeavors. Therapeutic aversion is one feasible route.
Medically administered, shock therapy is actually the primary method of expert-overseen aversion techniques in smoking cessation. In shock therapy, the patient meets with the doctor on a set schedule to undergo this rather unpleasant routine. Whenever the patient is struck with the urge to smoke or begins the process of lighting up, a shock is administered by the overseeing doctor. With repeated application, the idea is that the brain becomes quite convinced that the hunt for nicotine leads directly to too much discomfort to be worth it.
Whenever the patient is struck with the urge to smoke or begins the process of lighting up, a shock is administered by the overseeing doctor. With repeated application, the idea is that the brain becomes quite convinced that the hunt for nicotine leads directly to too much discomfort to be worth it.
There are also milder forms of aversion therapy for smokers. Some people might put a few dabs of an unpleasant substance over their cigarettes to make them taste bad, or they might only purchase types of cigarettes that they don’t like. Others might view off-putting images while they smoke, including images of charred lungs and other forms of smoke damage.
In a clinical setting, some people might have behavioral specialists blow warm, stale smoke into their faces whenever they take a puff. It’s also a common aversion technique to draw smoke into the mouth and hold it there for 30 seconds or more, often while the behaviorist is talking about and thereby reinforcing the negative health consequences of smoking.
Last but not least, some experts recommend a technique called “rapid smoking.” This is when a cigarette is smoked in quick puffs that don’t allow the smoker to enjoy it. In some cases, it might even cause nausea or respiratory distress. It can be especially useful for bored or social smokers who are used to lingering over their cigarettes.
In all cases of aversion therapy for smoking, the idea is that you need to take some kind of action that makes smoking more unpleasant than it is pleasurable. You have to counteract the “high” of the nicotine with a “down” of equal or greater strength. Whether that’s through shocks, foul tastes or rapidly smoked cigarettes is up to you.
To Curb Alcoholism
For as long as alcohol has been known to man, this same substance has been responsible for countless addictions and other health problems associated with its heavy use. Aversion techniques have thus been born from the need to treat these pitfalls of alcoholism.
One of the most interesting approaches for alcohol aversion therapy can be seen in the physician-overseen administration of specialty tryptophan metabolites. When taken regularly, these compounds prevent regular processing of alcohol within the body. As a result, drinking brings about a set of distinct digestive pains and troubles. Likewise, abstaining from drinking while on the medication promotes a great sense of well-being and euphoria.
When taken regularly, these compounds prevent regular processing of alcohol within the body. As a result, drinking brings about a set of distinct digestive pains and troubles. Likewise, abstaining from drinking while on the medication promotes a great sense of well-being and euphoria.
Other methods of aversion therapy for drinking include shocks, distractions, painful counteractions and sabotaging one’s drinks with unpleasant tastes and textures. Some of these techniques you’ve seen before with things like smoking and nail biting, but they’ve been shown to be effective across multiple bad habits. They can also be combined with more traditional methods of therapy such as cognitive behavioral therapy (CBT) for a broader range of behavior modification.
Because of the serious nature of alcohol abuse, many people seek aversion therapy through clinics and rehabs where they can be carefully monitored as they try to kick the habit. In the case of aversive medications, a prescription is required, and taking it under the supervision of a professional is often a requirement to both ensure the health of the patient and to prevent the addiction from shifting to another source.
It’s less common to see people self-administrating aversion therapy for drinking. It’s risky, and it can be less effective than therapy guided by an addiction specialist. It can also be difficult when the addiction is too severe for the patient to self-regulate their own recovery efforts.
To Resolve Weight or Diet Issues
The drive to eat can be the greatest of all human desires and drives. When we have a drive to eat all the wrong things, our bodies and our greater health thus suffer many bad consequences. Science has consequently developed all kinds of dietary and food aversion techniques and products.
There are many medications that can be taken to avert the consumption of unhealthy foods. Some are garden variety diet pills that suppress the appetite and stimulate the body into action with small doses of caffeine. Others are more specialized, and they might involve treating anxiety, depression or compulsive disorders in order to help you control your urges and avoid mental states where eating is a comfort. Depending on the type of medication that you’re considering, you might need a prescription from a doctor to obtain it.
Depending on the type of medication that you’re considering, you might need a prescription from a doctor to obtain it.
Outside of medication, any number of personal aversion techniques can be employed so as to avoid prior binging or overeating habits. You can shock yourself with a wristband. You can cover a desired food with an undesired topping, or you can only buy snacks that you don’t like that much. One of the most effective aversion techniques involves leaving junk food at the store so that when the urge comes, an inconvenient trip out is always required in order to satisfy the craving. This is an example of the deterrent method.
Other deterrents can be psychological rather than physical. For example, a common tactic employed by weight loss clinics is to show nauseating images while someone is eating unhealthy foods. Some clinics even bring in hypnotists to put patients in a trance and associate words like “sugar” and “carbs” with other, more unpleasant words.
Aversion therapy for weight loss is another area that should be tread carefully. It’s very easy to develop disordered eating habits even with the best of intentions, so if you’re considering this form of treatment for a diet or weight loss routine, make sure that you consult with trained professionals first.
It’s very easy to develop disordered eating habits even with the best of intentions, so if you’re considering this form of treatment for a diet or weight loss routine, make sure that you consult with trained professionals first.
To Stop Gambling Addiction
Gambling addiction occurs when someone becomes addicted to gambling in any of its various forms. While there are no medications that can be prescribed here, there are a number of techniques that can be applied in order to avert the desire.
One method involves paying a considerable fee to family or even a charity every time the individual seeks to gamble. This acts as both a psychological deterrent and a physical means of restricting the amount of money that one has available to gamble. A similar technique is punishing the act of gambling with some kind of self-imposed consequence such as writing a public apology letter.
Another, more serious approach is through familial shunning, or the family’s direct reaction to further gambling via refusal to associate as usual with the gambler. The time applied to this unpleasant, consequential action may vary from hours to days.
The time applied to this unpleasant, consequential action may vary from hours to days.
A recent anti-gambling technique that’s gaining attention is something called “imaginal desensitization.” With this method, the gambler is gradually desensitized to the rush of gambling through relaxation techniques and mindfulness exercises. It reconditions their brain not to light up at the sight of casinos and other associated gambling imagery. Aversion therapy is sometimes included with this technique as a counterbalance: Pleasant images will be played over non-gambling images while unpleasant ones will be played over casinos.
Additional forms of aversion therapy for gambling can involve shocks, noises, hypnosis and various strange and frightening stimuli. As with all forms of aversion therapy, the goal is to replace the highs of gambling with the lows of something far less nice. When the brain comes to associate the very notion of gambling with these distasteful things, the aversion therapy has succeeded, and the subject will avoid gambling on their own.
Sometimes it can be quite difficult to abstain form past behaviors and addictions. There are many professional techniques to help in this arena. However, for those that don’t get the desired results with more common methods, approaches in aversion therapy can often serve as just the right motivation to get the job done.
Related Resources:
- Top 6 Most Affordable Online PhD/PsyD Programs in Clinical Psychology
- How Effective Is Dialectical Behavior Therapy in Treating Mental Illness?
- What is Cognitive Behavioral Therapy?
- What is Dialectical Behavioral Therapy?
- What is Rational Emotive Behavioral Therapy?
Aversion therapy
Consider others methods of treatment of tobacco dependence. The most common and effective of which are aversion methods therapies aimed at negative conditioned reflex to smoking. Such methods are enough many, but the most popular use techniques using injections of apomorphine, "rapid smoking" and hypnosis.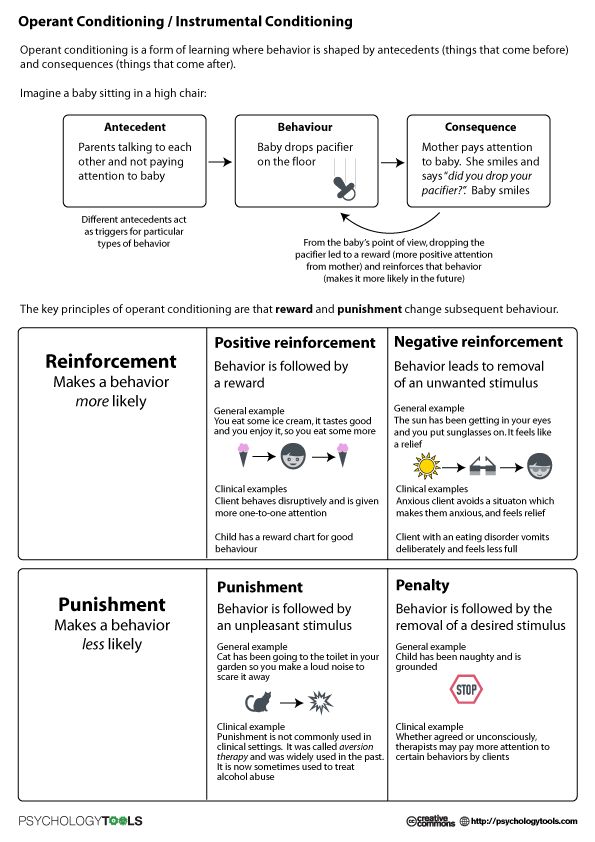
Method using apomorphine is that the patient is injected subcutaneously with 0.1-0.3 ml of 1% an aqueous solution of apomorphine, after which offer to smoke two or three cigarettes. Then, against the background of emerging under the action apomorphine discomfort, spend imperative suggestion of disgust smoking.
Almost any patient visiting a doctor of any recommendations knows that “to smoke harmful." Another thing is that it is far from every patient has an idea what harm smoking does his personal health. Therefore, on our view, the doctor's advice should be maximally customized
This method can used in complex therapy smoking, but its essential The disadvantage is that in this case character negative unconditioned stimulus (injection apomorphine) is not the same type behavior to which disgust (smoking). In the same time known that the maximum therapeutic types of aversion have an effect incentive-based therapies characteristic of that mode of behavior, which needs to be eliminated. This the rule is satisfied by the “fast smoking”, which is apparently the most common method of treatment tobacco addiction around the world.
This the rule is satisfied by the “fast smoking”, which is apparently the most common method of treatment tobacco addiction around the world.
At the heart of the method lies the principle that reinforcing aspect of any stimulus is reduced and eventually becomes aversive if this stimulus is presented at an unusually high frequency and intensity. In this way, in this case as a negative unconditioned stimulus (aversion stimulus) smoking itself is used.
sessions of "quick smoking” are carried out, as a rule, with a group of patients of two to five people, which promotes mutual suggestion and creating an atmosphere of cooperation. On the session as "viewers" can be invite future participants in therapy. Before it begins, the doctor emotionally declares that “smoking will be disgusting, disgusting, disgusting. Look and smell tobacco smoke will cause disgust, coughing, drooling, nausea and vomiting.” Then comes the command: “And now smoke!"
Subsequently every 6 seconds the doctor commands: “Take a drag!” and the patient smokes in at such an accelerated pace until vomiting. There are three to five sessions in total.
There are three to five sessions in total.
peculiar a modification of this method was developed G. P. Andrukh. The author suggests to patients smoking while standing as fast as possible two cigarettes at the same time. In the moment the patient should experience dizziness sit on the couch. Unlike the traditional procedures while the patient is smoking the doctor does not give the command to tighten, and conducts imperative suggestion approximately the following content: “Deep and tighten continuously, carefully listen to me. If your head spins sit on the couch. Smoke... Heart fast pounding, legs like cotton, breathing difficult, forehead covered with cold then, saliva stands out ... sick, vomits! Smoking becomes disgusting, vile. Here coughing, choking, nausea, vomit is coming! ..” etc. After that how the patient sits down and stops smoking, he is blown in for several minutes in the face of tobacco smoke from a special vial, at the same time suggesting that it is not only can't smoke, but can't stand it either the smell of tobacco smoke from others smokers.
The “quick smoking” is very effective, however poses a potential danger powerful toxic effect nicotine on cardiovascular and nervous system. Therefore, to carry out This type of treatment should only be no contraindications, which are, in particular, cardiovascular diseases and epilepsy. As alternative method in patients suffering from these diseases, use a similar procedure which the patient is not delayed, but only absorbs tobacco smoke into his mouth.
Hypnotherapy as method of treating tobacco smoking our country has a long tradition. Method relatively simple, has a minimum contraindications and can successfully used in hypnotic patients. Hypnotherapy is also best done with a group of patients. The course of treatment consists from 8 to 16 sessions.
During the session the patient is put into a hypnotic trance according to one of the traditional methods (with using gaze fixation metronome or only verbal suggestion). Then the suggestion is made roughly as follows: "To you nice and good. The heart beats evenly calmly. Breathing is deep and regular. With every breath, it penetrates the body pleasant feeling of freshness and health. But now a trickle is woven into the air poisonous impurity, it is tobacco smoke, the smell of burning, decay, death. You nauseated, nauseated, vomited. Smell and taste of tobacco the smoke is unbearable, disgusting! (in that moment in the face of the patient they blow tobacco smoke). Now the smell of tobacco smoke and even one kind of smoking people will cause you feel dizzy and nauseous. With every subsequent session of hypnosis disgust to tobacco will intensify and grow.”
Then the suggestion is made roughly as follows: "To you nice and good. The heart beats evenly calmly. Breathing is deep and regular. With every breath, it penetrates the body pleasant feeling of freshness and health. But now a trickle is woven into the air poisonous impurity, it is tobacco smoke, the smell of burning, decay, death. You nauseated, nauseated, vomited. Smell and taste of tobacco the smoke is unbearable, disgusting! (in that moment in the face of the patient they blow tobacco smoke). Now the smell of tobacco smoke and even one kind of smoking people will cause you feel dizzy and nauseous. With every subsequent session of hypnosis disgust to tobacco will intensify and grow.”
The session ends returning the patient to relaxation a state of cheerfulness posthypnotic period.
how does aversion therapy work? |
Review
Source: pxhere.com
Abominable therapy first appeared in 1932 and has been used and controversial ever since. This type of conditioning therapy is a treatment in which a person experiences an irritant and at the same time experiences some discomfort. The idea is that the mind will associate the discomfort with the behavior being treated, and that discomfort will eventually discourage the person from engaging in the unwanted behavior. Aversion therapy is performed by a therapist, psychologist, psychiatrist, or other certified psychiatrist. There are many reasons for choosing aversion therapy as a treatment for unwanted behaviors, but the most common reason for its recent use is addiction.
This type of conditioning therapy is a treatment in which a person experiences an irritant and at the same time experiences some discomfort. The idea is that the mind will associate the discomfort with the behavior being treated, and that discomfort will eventually discourage the person from engaging in the unwanted behavior. Aversion therapy is performed by a therapist, psychologist, psychiatrist, or other certified psychiatrist. There are many reasons for choosing aversion therapy as a treatment for unwanted behaviors, but the most common reason for its recent use is addiction.
This type of therapy is called behavioral therapy. Behavioral therapies are psychological therapies that are used to change unwanted behavior. Changing unwanted behavior is achieved through conditioning, and conditioning goes back to classical conditioning theories. The idea that the mind can be tuned through associations, repetitions, and influences to change unwanted behavior is at the heart of all types of behavioral therapy.
Counterconditioning, desensitizing conditioning, aversion therapy, and flooding are all types of behavioral therapy. Each therapy has its own strengths, and therapists use these different therapies to achieve specific results. Different people respond to therapy differently, so only a therapist, counselor, or psychologist can advise you on which type of therapy is right for you.
Aversion therapy was once popular for treating addiction, but has also been used with varying degrees of success to banish other unwanted behaviors. One of the most controversial uses of this therapy in the past has been electroshock therapy to "treat" homosexuality. For those who gamble, smoke, or engage in relationship-destroying behaviors, this type of therapy was once thought to be effective.
Addiction Aversion Therapy
Source: rawpixel.com
For many, addiction is detrimental to their lives and relationships. Marriages break down, friendships suffer, and close family ties break down when addiction is present. Aversion therapy is a behavioral therapeutic intervention that has been successful in dealing with addictive behaviors. Aversion therapy for addiction relies heavily on medications, but other types of aversion therapy are also used. The main problem that occurs when this therapy helps change behavior is relapse.
Aversion therapy is a behavioral therapeutic intervention that has been successful in dealing with addictive behaviors. Aversion therapy for addiction relies heavily on medications, but other types of aversion therapy are also used. The main problem that occurs when this therapy helps change behavior is relapse.
The type of drugs used in addiction therapy for aversion include naltrexone and disulfiram. Naltrexone blocks the action of opioids and thus reduces the desire to use addictive drugs. Naltrexone reduces alcohol cravings, improves abstinence, and reduces the chance of relapse.
Disulfiram causes an aversion to alcohol, causing a hangover-type reaction when taken orally. Some people benefit from disulfiram, but others may choose not to take the medication if they plan to drink. However, when taken regularly, this drug acts as a deterrent, as once taken, alcohol causes an immediate hangover reaction.
Other types of aversion therapy for addiction treatment include electricity aversion techniques and image aversion techniques. Electricity aversion works by applying an electric shock when the person exhibits unwanted behavior. Disgust imaging techniques use images to "shock" or induce "disgust" when a person engages in unwanted behavior. Both methods are based on the assumption that eventually the person will associate negative things with unwanted behavior and change that behavior.
Electricity aversion works by applying an electric shock when the person exhibits unwanted behavior. Disgust imaging techniques use images to "shock" or induce "disgust" when a person engages in unwanted behavior. Both methods are based on the assumption that eventually the person will associate negative things with unwanted behavior and change that behavior.
Criticism
Drug aversion therapy has been criticized because of the problems it can cause. Disulfiram and other drugs that cause hangovers or make you sick when you drink alcohol can make some people seriously ill. Another problem with drug aversion therapy is that naltrexone should not be taken until the person is completely sober or may experience negative side effects such as immediate and severe withdrawal symptoms.
Criticism of electrical and imaging techniques revolves around their overall effectiveness. While many believe that electroshock and imaging techniques work and disgust addiction; Clinical studies show that these aversion therapies are less effective than drug aversion therapy. The effectiveness of these two methods largely depends on the person and how they respond.
The effectiveness of these two methods largely depends on the person and how they respond.
Most psychologists/psychiatrists, counselors and therapists agree that the relapse rate is high after using aversion therapy. Aversion therapy can help those who are addicted while they are in the therapist's office, but the therapy becomes less effective after they leave the office. With such a high relapse rate, most, if not all, psychologists and therapists are using new cognitive-behavioral methods to treat addiction.
Aversion therapy and compulsive disorders
Source: rawpixel.com
Aversion therapy is a behavior modification therapy and this type of therapy works well for compulsive disorders. There are several types of aversion therapy used to control compulsive disorders such as nail biting, skin pulling, hair pulling, and others. Behavior modification through aversion therapy can be as simple as putting on a rubber band around your wrist or as intense as getting an electric shock.
The usual treatment for nail biting aversion is to apply a bitter tasting substance to the nail. After applying the substance, when a person bites a nail, they experience the bitter taste of the substance, and this may be enough to change the unwanted behavior. Studies show that electric shock aversion therapy is also good for nail biting, with up to 80% effectiveness.
There aren't many studies on electrical aversion therapy for hair pulling, but what little there is shows that electrical aversion therapy does help with hair pulling control. Other types of obsessive-compulsive and compulsive disorders have been treated with electrical shock aversion therapy in the past. Electric shock is applied whenever compulsive behavior occurs, and this discomfort is combined with unwanted behavior. Once the shock and the behavior are combined in the mind, the person no longer wants to engage in the unwanted obsessive-compulsive behavior, at least that's the theory.
Criticism
Many therapists and psychiatrists/psychologists disagree with the use of aversion therapy for obsessive-compulsive disorder (OCD).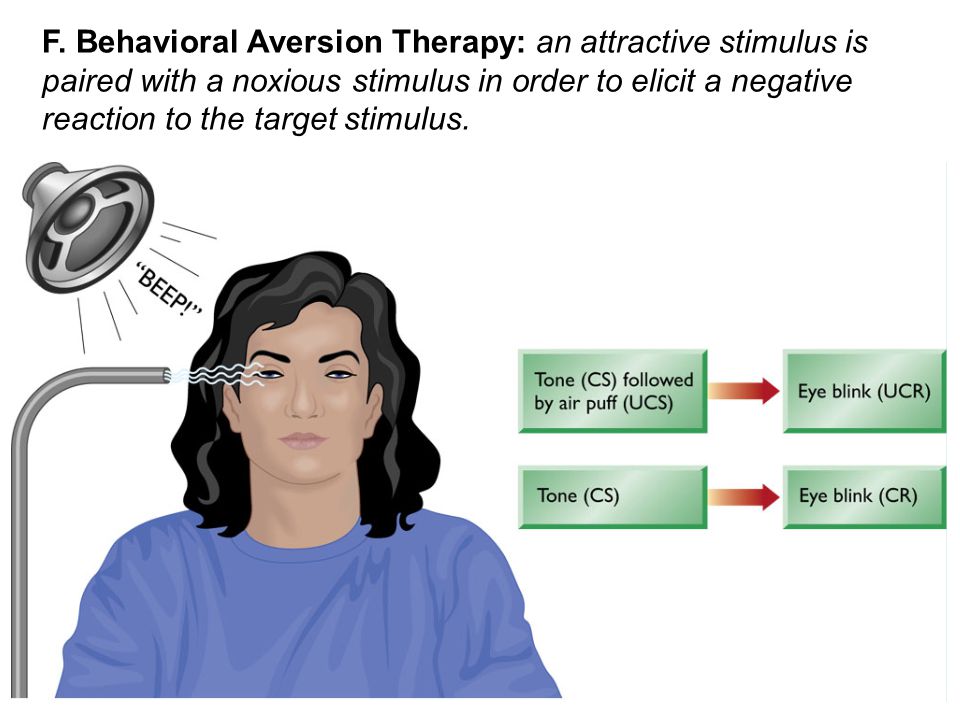 Most doctors and therapists agree that the most effective treatment for OCD is cognitive behavioral therapy. Using a painful stimulus to create aversion to OCD behavior is not usually the first type of therapy used to treat this problem.
Most doctors and therapists agree that the most effective treatment for OCD is cognitive behavioral therapy. Using a painful stimulus to create aversion to OCD behavior is not usually the first type of therapy used to treat this problem.
Some websites list aversion therapy as an effective treatment for OCD, but most mental health professionals disagree with this treatment and agree that exposure and response therapy (ERT) and cognitive behavioral therapy (CBT) work better Total. and are the first treatments for OCD.
Ethical considerations regarding the use of pain shocks have made disgust therapy obsolete. Psychology has made a lot of progress in understanding OCD, and modern therapies are having a much greater effect in combating this anxiety disorder. Simple aversion techniques, such as snapping a rubber band around your wrist every time an unwanted behavior occurs, can help a person refocus attention, but electric shocks are almost a thing of the past.
Alternatives to Modern Aversion Therapy
Source: pexels. com
com
Modern addiction treatments rarely include aversion methods. Drugs are still used to support people with addiction problems, but they are not disgusting drugs. Drugs are used to support the addict during withdrawal; then they gradually wean from the maintenance drug. Withdrawal symptoms can be life-threatening, and using drugs to support someone during withdrawal is common.
Once a person has completed detox, they can begin treatment for the underlying causes of addiction. Cognitive behavioral therapy is most commonly used to treat these underlying problems. Support groups and counseling are important for successful recovery and relapse prevention. Scientific research on addiction has shown that the physical and psychological causes of addiction require more than simple aversion therapies.
Exposure and Response Therapy (ERT) is a modern alternative to outdated methods of aversion therapy. Exposure and reaction works better than aversion therapy because it focuses on facing the real problem and then learning to deal effectively with the stress that comes when behavior doesn't respond to action.