Effexor with wellbutrin
Venlafaxine and bupropion combination therapy in a case of treatment-resistant depression
Save citation to file
Format: Summary (text)PubMedPMIDAbstract (text)CSV
Add to Collections
- Create a new collection
- Add to an existing collection
Name your collection:
Name must be less than 100 characters
Choose a collection:
Unable to load your collection due to an error
Please try again
Add to My Bibliography
- My Bibliography
Unable to load your delegates due to an error
Please try again
Your saved search
Name of saved search:
Search terms:
Test search terms
Email: (change)
Which day? The first SundayThe first MondayThe first TuesdayThe first WednesdayThe first ThursdayThe first FridayThe first SaturdayThe first dayThe first weekday
Which day? SundayMondayTuesdayWednesdayThursdayFridaySaturday
Report format: SummarySummary (text)AbstractAbstract (text)PubMed
Send at most: 1 item5 items10 items20 items50 items100 items200 items
Send even when there aren't any new results
Optional text in email:
Create a file for external citation management software
Full text links
Atypon
Full text links
Case Reports
. 1999 Jun;33(6):701-3.
doi: 10.1345/aph.18249.
S H Fatemi 1 , E S Emamian, D A Kist
Affiliations
Affiliation
- 1 Department of Psychiatry, School of Medicine, University of Minnesota, Minneapolis 55455, USA.
- PMID: 10410184
- DOI: 10.1345/aph.18249
Case Reports
S H Fatemi et al. Ann Pharmacother. 1999 Jun.
. 1999 Jun;33(6):701-3.
doi: 10. 1345/aph.18249.
1345/aph.18249.
Authors
S H Fatemi 1 , E S Emamian, D A Kist
Affiliation
- 1 Department of Psychiatry, School of Medicine, University of Minnesota, Minneapolis 55455, USA.
- PMID: 10410184
- DOI: 10.1345/aph.18249
Abstract
Objective: To report the therapeutic efficacy of venlafaxine and bupropion in a patient with treatment-refractory major depression.
Case summary: A 21-year-old white woman with chronic and recurrent major depression presented with lack of response to several antidepressants. On examination, the patient exhibited neurovegetative signs of depression, guilt feelings, and suicidal ideation. The patient was administered venlafaxine 75 mg three times daily. The dose was titrated to 150 mg three times daily over the next month. Later bupropion was instituted up to 100 mg three times daily over a four-month period. The patient responded favorably to combination therapy and has remained free of depression for approximately 23 months.
On examination, the patient exhibited neurovegetative signs of depression, guilt feelings, and suicidal ideation. The patient was administered venlafaxine 75 mg three times daily. The dose was titrated to 150 mg three times daily over the next month. Later bupropion was instituted up to 100 mg three times daily over a four-month period. The patient responded favorably to combination therapy and has remained free of depression for approximately 23 months.
Discussion: Venlafaxine and bupropion are antidepressant agents with unique pharmacologic profiles, each effective in the treatment of depression. Recent data indicate that combinations of selective serotonin-reuptake inhibitors and bupropion can convert partial response to full response in patients with treatment-resistant depression. We considered whether a combination of venlafaxine and bupropion would reduce the depressive symptoms of a patient who was unresponsive to various classes of psychotropic agents. Gradual administration of venlafaxine and bupropion acted synergistically to significantly reduce depressive symptoms (p < 0.002) and significantly increase social function (p < 0.002) over a period of eight months.
Gradual administration of venlafaxine and bupropion acted synergistically to significantly reduce depressive symptoms (p < 0.002) and significantly increase social function (p < 0.002) over a period of eight months.
Conclusions: To our knowledge this is the first report of successful combination therapy with venlafaxine and bupropion in treatment of chronic recurrent and refractory major depression.
Similar articles
-
Bupropion and venlafaxine responders differ in pretreatment regional cerebral metabolism in unipolar depression.
Little JT, Ketter TA, Kimbrell TA, Dunn RT, Benson BE, Willis MW, Luckenbaugh DA, Post RM. Little JT, et al. Biol Psychiatry. 2005 Feb 1;57(3):220-8. doi: 10.1016/j.biopsych.2004.10.033. Biol Psychiatry. 2005. PMID: 15691522 Clinical Trial.

-
Mechanisms of action and clinical characteristics of three atypical antidepressants: venlafaxine, nefazodone, bupropion.
Horst WD, Preskorn SH. Horst WD, et al. J Affect Disord. 1998 Dec;51(3):237-54. doi: 10.1016/s0165-0327(98)00222-5. J Affect Disord. 1998. PMID: 10333980 Review.
-
A double-blind comparison between bupropion XL and venlafaxine XR: sexual functioning, antidepressant efficacy, and tolerability.
Thase ME, Clayton AH, Haight BR, Thompson AH, Modell JG, Johnston JA. Thase ME, et al. J Clin Psychopharmacol. 2006 Oct;26(5):482-8. doi: 10.1097/01.jcp.0000239790.83707.ab. J Clin Psychopharmacol. 2006. PMID: 16974189 Clinical Trial.
-
Geriatric depression treatment in nonresponders to selective serotonin reuptake inhibitors.
Whyte EM, Basinski J, Farhi P, Dew MA, Begley A, Mulsant BH, Reynolds CF. Whyte EM, et al. J Clin Psychiatry. 2004 Dec;65(12):1634-41. doi: 10.4088/jcp.v65n1208. J Clin Psychiatry. 2004. PMID: 15641868 Clinical Trial.
-
Efficacy, tolerability, and acceptability of bupropion for major depressive disorder: a meta-analysis of randomized-controlled trials comparison with venlafaxine.
Maneeton N, Maneeton B, Eurviriyanukul K, Srisurapanont M. Maneeton N, et al. Drug Des Devel Ther. 2013 Sep 27;7:1053-62. doi: 10.2147/DDDT.S46849. eCollection 2013. Drug Des Devel Ther. 2013. PMID: 24101861 Free PMC article. Review.
See all similar articles
Cited by
-
Pharmacological Augmentation in Unipolar Depression: A Guide to the Guidelines.

Taylor RW, Marwood L, Oprea E, DeAngel V, Mather S, Valentini B, Zahn R, Young AH, Cleare AJ. Taylor RW, et al. Int J Neuropsychopharmacol. 2020 Dec 3;23(9):587-625. doi: 10.1093/ijnp/pyaa033. Int J Neuropsychopharmacol. 2020. PMID: 32402075 Free PMC article.
-
A Review of Psychostimulants for Adults With Depression.
Pary R, Scarff JR, Jijakli A, Tobias C, Lippmann S. Pary R, et al. Fed Pract. 2015 Apr;32(Suppl 3):30S-37S. Fed Pract. 2015. PMID: 30766117 Free PMC article.
-
Multimodal antidepressant vortioxetine increases frontal cortical oscillations unlike escitalopram and duloxetine--a quantitative EEG study in rats.
Leiser SC, Pehrson AL, Robichaud PJ, Sanchez C. Leiser SC, et al.
 Br J Pharmacol. 2014 Sep;171(18):4255-72. doi: 10.1111/bph.12782. Br J Pharmacol. 2014. PMID: 24846338 Free PMC article.
Br J Pharmacol. 2014 Sep;171(18):4255-72. doi: 10.1111/bph.12782. Br J Pharmacol. 2014. PMID: 24846338 Free PMC article. -
Therapeutic options for treatment-resistant depression.
Shelton RC, Osuntokun O, Heinloth AN, Corya SA. Shelton RC, et al. CNS Drugs. 2010 Feb;24(2):131-61. doi: 10.2165/11530280-000000000-00000. CNS Drugs. 2010. PMID: 20088620 Review.
Publication types
MeSH terms
Substances
Full text links
Atypon
Cite
Format: AMA APA MLA NLM
Add to Collections
- Create a new collection
- Add to an existing collection
Name your collection:
Name must be less than 100 characters
Choose a collection:
Unable to load your collection due to an error
Please try again
Send To
Differences, similarities, and which is better for you
Drug overview & main differences | Conditions treated | Efficacy | Insurance coverage and cost comparison | Side effects | Drug interactions | Warnings | FAQ
Effexor (venlafaxine) and Wellbutrin (bupropion) are two different antidepressant medications that can be used to treat depression.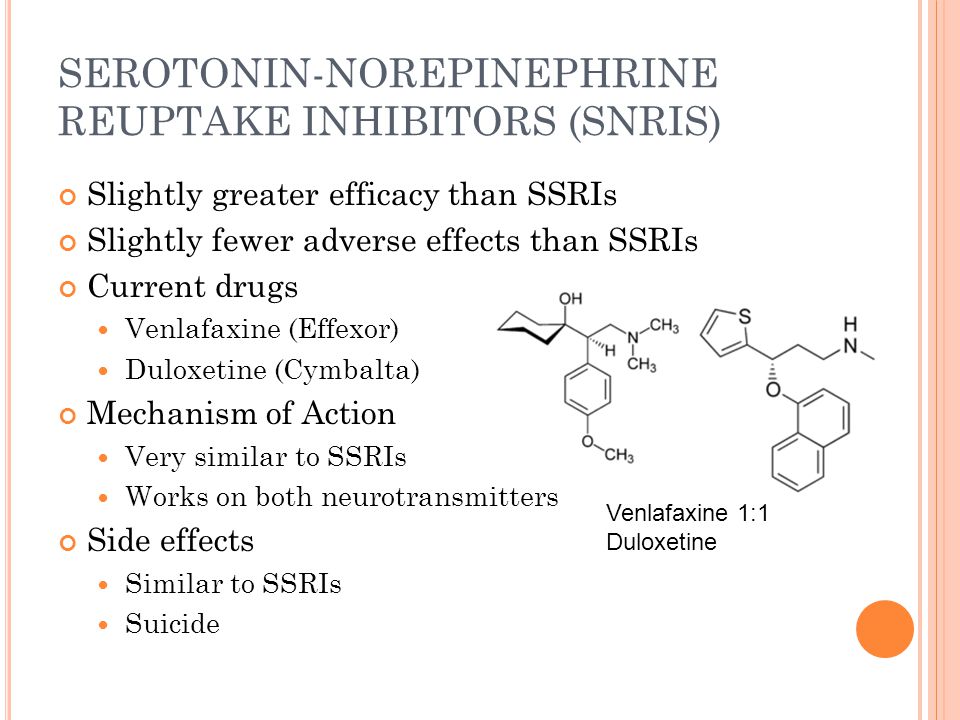 Both Effexor and Wellbutrin work by boosting specific neurotransmitters, such as norepinephrine and dopamine, in the brain. Balancing these neurotransmitters can help improve mood, promote better sleep, and boost your appetite and focus. Antidepressants are also useful for treating other mental health problems in addition to major depression.
Both Effexor and Wellbutrin work by boosting specific neurotransmitters, such as norepinephrine and dopamine, in the brain. Balancing these neurotransmitters can help improve mood, promote better sleep, and boost your appetite and focus. Antidepressants are also useful for treating other mental health problems in addition to major depression.
Despite their similarities, Effexor and Wellbutrin work differently and are FDA approved to treat different conditions.
What are the main differences between Effexor and Wellbutrin?
Effexor is the brand name for venlafaxine. It is chemically identical to Pristiq (desvenlafaxine) and belongs to a drug class called serotonin-norepinephrine reuptake inhibitors (SNRIs). Effexor works by blocking the reabsorption of serotonin, norepinephrine, and dopamine in the brain. Blocking their reabsorption, or reuptake, increases their availability and overall effects.
Brand-name Effexor in immediate-release tablets has been discontinued. Instead, an extended-release form called Effexor XR is prescribed. Effexor XR comes in strengths of 37.5 mg, 75 mg, and 150 mg.
Instead, an extended-release form called Effexor XR is prescribed. Effexor XR comes in strengths of 37.5 mg, 75 mg, and 150 mg.
Wellbutrin is the brand name for bupropion. It is a unique antidepressant classified as an aminoketone. Wellbutrin is believed to work by blocking the reuptake of norepinephrine and dopamine neurotransmitters to boost their effects. Unlike Effexor, Wellbutrin does not alter serotonin levels as much.
Wellbutrin comes in immediate-release oral tablets with strengths of 75 mg or 100 mg. However, it is usually prescribed as a sustained-release tablet (Wellbutrin SR) or an extended-release tablet (Wellbutrin XL). Wellbutrin SR and Wellbutrin XL are released gradually in the body and can be taken once per day.
Conditions treated by Effexor and Wellbutrin
Effexor is labeled to treat major depression or major depressive disorder. It can also treat anxiety disorders, among other mental health conditions. Immediate-release venlafaxine can help treat panic attacks while the extended-release form is approved to treat generalized anxiety disorder. Off-label uses of Effexor include treatment of obsessive-compulsive disorder (OCD) and premenstrual dysphoric disorder (PMDD).
Off-label uses of Effexor include treatment of obsessive-compulsive disorder (OCD) and premenstrual dysphoric disorder (PMDD).
Wellbutrin is FDA approved to treat major depressive disorder and seasonal affective disorder. It is also sometimes used as an off-label drug to treat bipolar disorder, attention deficit hyperactivity disorder (ADHD), and sexual dysfunction caused by SSRI antidepressants.
Is Effexor or Wellbutrin more effective?
Effexor and Wellbutrin are effective medications for treating depression symptoms. However, the more effective antidepressant is the one that works best for you.
According to a meta-analysis, Effexor and Wellbutrin are similarly effective for treating adults with major depressive disorder. Although they both work similarly, Wellbutrin has been shown to produce less sexual dysfunction as a side effect. Sexual dysfunction is a common side effect of antidepressants, especially selective serotonin reuptake inhibitors (SSRIs).
Wellbutrin and Effexor have also been compared to SSRI antidepressants like sertraline, escitalopram, fluoxetine, paroxetine, and duloxetine. Clinical trials have shown that Wellbutrin is similar in effectiveness to SSRIs. Conversely, Effexor has been found to be more effective than SSRIs, although more people may stop taking Effexor because of side effects.
Clinical trials have shown that Wellbutrin is similar in effectiveness to SSRIs. Conversely, Effexor has been found to be more effective than SSRIs, although more people may stop taking Effexor because of side effects.
Consult your healthcare provider for the best treatment for you. After a complete evaluation of your overall symptoms, your doctor will work with you to find an appropriate medication.
Coverage and cost comparison of Effexor vs. Wellbutrin
Effexor XR requires a prescription. It is usually covered by most Medicare and insurance plans. For a 30-day supply of 75 mg tablets, the average retail cost is around $146. Using an Effexor XR SingleCare card can lower this price to $15 depending on the pharmacy you use.
Your doctor will likely prescribe Wellbutrin SR or Wellbutrin XL. These versions of Wellbutrin release the drug gradually in the body. Most Medicare and insurance plans will cover Wellbutrin XL or Wellbutrin SR. If you don’t have insurance, the average cash price of Wellbutrin can be more than $100. Even if you have insurance, you can use a Wellbutrin XL SingleCare card or a Wellbutrin SR SingleCare card to save money on your prescription.
Even if you have insurance, you can use a Wellbutrin XL SingleCare card or a Wellbutrin SR SingleCare card to save money on your prescription.
Common side effects of Effexor vs. Wellbutrin
The most common side effects of Effexor are drowsiness, insomnia, dizziness, nervousness, nausea, and headache. Other common side effects include dry mouth, muscle weakness, sweating, and an increased heart rate (palpitations). Sexual side effects, including sexual dysfunction and abnormal ejaculation, are also common while using Effexor.
The most common side effects of Wellbutrin are insomnia, dizziness, dry mouth, nausea, headache, and sweating. Wellbutrin may also cause nervousness, muscle weakness, and palpitations, among other side effects.
Effexor and Wellbutrin can also cause changes in weight. Both antidepressants may cause either weight gain or weight loss depending on your response to the drug.
Serious side effects of Effexor and Wellbutrin include new or worsened mental health problems, suicidal thoughts, agitation, and hostility. Monitor any changes in mood while taking these medications. Consult your healthcare provider if you experience any severe side effects.
Monitor any changes in mood while taking these medications. Consult your healthcare provider if you experience any severe side effects.
*not reported
Frequency is not based on data from a head-to-head trial. This may not be a complete list of adverse effects that can occur. Please refer to your doctor or healthcare provider to learn more.
Source: FDA Label (Effexor), FDA Label (Wellbutrin)
Drug interactions of Effexor vs. Wellbutrin
Effexor and Wellbutrin can interact with monoamine oxidase inhibitors (MAOIs). Taking an MAOI, like isocarboxazid or phenelzine, with Effexor or Wellbutrin can increase the risk of serotonin syndrome. Effexor and Wellbutrin should not be taken with an MAOI or within 14 days of stopping an MAOI.
Effexor and Wellbutrin can interact with serotonergic drugs. For example, taking a serotonergic drug like nortriptyline, a tricyclic antidepressant, can increase the risk of serotonin syndrome when combined with another antidepressant.-Tab-150mg-UK-1.jpg) Effexor and Wellbutrin should also be avoided with St. John’s wort, an herbal drug frequently used for its antidepressant effects. Tell your doctor if you’re taking other antidepressants before starting Effexor or Wellbutrin.
Effexor and Wellbutrin should also be avoided with St. John’s wort, an herbal drug frequently used for its antidepressant effects. Tell your doctor if you’re taking other antidepressants before starting Effexor or Wellbutrin.
Effexor and Wellbutrin can affect the functions of platelets and blood clotting. The use of Effexor or Wellbutrin could decrease the effectiveness of warfarin or other anticoagulants.
Consult a healthcare professional for other possible drug interactions.
Warnings of Effexor and Wellbutrin
The use of Effexor or Wellbutrin can lead to an increased risk of suicidal thoughts, especially in adolescents and young adults. Behavioral and mood changes should be monitored when starting a medication like Effexor or Wellbutrin. If you experience severe behavioral changes, antidepressants may be discontinued or adjusted by your healthcare provider.
Effexor and Wellbutrin can increase blood pressure. Therefore, it’s important to monitor blood pressure while taking these medications. Consult your doctor if you have a history of high blood pressure before taking these medications.
Consult your doctor if you have a history of high blood pressure before taking these medications.
Certain antidepressants like SSRIs and SNRIs can increase the risk of bleeding. Effexor should be avoided with anticoagulants and other drugs that affect blood clotting. Wellbutrin, which is not an SSRI or SNRI, is less likely to affect platelet functions.
When used with serotonergic drugs, Effexor and Wellbutrin can increase the risk of serotonin syndrome. Symptoms of serotonin syndrome include an increased heart rate, increased blood pressure, and fever. Consult your doctor if you experience any of these symptoms. Serotonin syndrome may require emergency medical attention.
Frequently asked questions about Effexor vs. Wellbutrin
What is Effexor?
Effexor is a brand-name medication used to treat major depressive disorder. The generic name of Effexor is venlafaxine. Effexor XR is the extended-release version of Effexor and can be taken once daily. Effexor can also treat anxiety and panic disorders.
What is Wellbutrin?
Wellbutrin is known by its generic name bupropion. It is primarily used to treat major depressive disorder. Wellbutrin is usually prescribed as Wellbutrin SR or Wellbutrin XL to treat depression and other mental health conditions. The extended-release form of Wellbutrin can be taken once daily.
Are Effexor and Wellbutrin the same?
Both Effexor and Wellbutrin can treat symptoms of depression. However, Effexor is a serotonin-norepinephrine reuptake inhibitor (SNRI) and Wellbutrin is an aminoketone. Therefore, these drugs work in different ways. They also have different FDA-approved uses.
Is Effexor or Wellbutrin better?
Effexor and Wellbutrin are both effective drugs that treat depression. Effexor is better than Wellbutrin for treating anxiety disorders that are experienced alongside depression. However, compared to Wellbutrin, Effexor may cause more sexual side effects, such as abnormal ejaculation and impotence.
Can I use Effexor or Wellbutrin while pregnant?
Effexor and Wellbutrin are in pregnancy class C and may increase the risk of birth defects. Both drugs are also secreted in breast milk. The use of Effexor and Wellbutrin should be cautioned or avoided during pregnancy.
Both drugs are also secreted in breast milk. The use of Effexor and Wellbutrin should be cautioned or avoided during pregnancy.
Can I use Effexor or Wellbutrin with alcohol?
It is not recommended to drink alcohol while taking Effexor or Wellbutrin. Alcohol use with Effexor or Wellbutrin can lead to increased drowsiness, dizziness, and other side effects. Alcohol use can also increase the risk of seizures in people who take Wellbutrin.
Effexor vs Wellbutrin: Differences, Similarities & What's Best for You - Drug Vs. Friend
Home >> Drug Vs. Friend >> Effexor vs Wellbutrin: Differences, Similarities & Which is Best for You
Drug Vs. Friend
Drug Overview and Key Differences | Conditions of treatment | Efficiency | Insurance coverage and cost comparison | Side effects | Drug Interactions | Warnings | FAQ
Effexor (venlafaxine) and Wellbutrin (bupropion) are two different antidepressants that can be used to treat depression. Both Effexor and Wellbutrin work by boosting certain neurotransmitters like norepinephrine and dopamine in the brain. Balancing these neurotransmitters can help improve mood, improve sleep, increase appetite, and increase focus. Antidepressants are also useful for treating other mental health problems in addition to major depression.
Both Effexor and Wellbutrin work by boosting certain neurotransmitters like norepinephrine and dopamine in the brain. Balancing these neurotransmitters can help improve mood, improve sleep, increase appetite, and increase focus. Antidepressants are also useful for treating other mental health problems in addition to major depression.
Despite their similarities, Effexor and Wellbutrin work differently and are FDA approved for different conditions.
What are the main differences between Effexor and Wellbutrin?
Effexor is the brand name for venlafaxine. It is chemically identical to Pristiq (desvenlafaxine) and belongs to a class of drugs called serotonin-norepinephrine reuptake inhibitors (SNRIs). Effexor works by blocking the reabsorption of serotonin, norepinephrine, and dopamine in the brain. Blocking their reabsorption or reuptake increases their availability and overall effect.
Blocking their reabsorption or reuptake increases their availability and overall effect.
The Effexor brand name in immediate release tablets is no longer available. Instead, an extended release form called Effexor XR is prescribed. Effexor XR is available in doses of 37.5 mg, 75 mg and 150 mg.
Wellbutrin is the brand name for bupropion. This is a unique antidepressant belonging to the group of amino ketones. Wellbutrin is thought to work by blocking the reuptake of the neurotransmitters norepinephrine and dopamine to enhance their effects. Unlike Effexor, Wellbutrin does not alter serotonin levels as much.
Wellbutrin is available as immediate-release oral tablets in 75 mg or 100 mg strength. However, it is usually prescribed as sustained release tablets (Wellbutrin SR) or extended release tablets (Wellbutrin XL). Wellbutrin SR and Wellbutrin XL are released gradually in the body and can be taken once a day.
| Main differences between Effexor and Wellbutrin | ||
|---|---|---|
| Bupropion | ||
| What form(s) does the drug come in? | Oral tablet | Oral tablet |
| What is the standard dosage? | Initially 75 mg daily. The dosage can be increased by 75 mg per day every 4 days. Dosage should not exceed 225 mg per day in divided doses. The dosage can be increased by 75 mg per day every 4 days. Dosage should not exceed 225 mg per day in divided doses. | Initially 100 mg twice daily. After 3 days, the dosage can be increased to 100 mg 3 times a day. The dosage should not exceed 150 mg at a time. |
| How long does a typical treatment take? | Long-term treatment | Long-term treatment |
| Who usually takes this medicine? | Adults 18 years of age and older | Adults 18 years of age and older |
Conditions treated with Effexor and Wellbutrin
Effexor is indicated for the treatment of major depression or major depressive disorder. It can also help treat anxiety disorders among other mental health conditions. Venlafaxine immediate release may help treat panic attacks, while the extended release form is approved for the treatment of generalized anxiety disorder. Off-label use of Effexor includes the treatment of obsessive compulsive disorder (OCD) and premenstrual dysphoric disorder (PMDD).
Wellbutrin is FDA approved for the treatment of major depressive disorder and seasonal affective disorder. It is also sometimes used as an off-label drug for the treatment of bipolar disorder, attention deficit hyperactivity disorder (ADHD), and sexual dysfunction caused by SSRI antidepressants.
| Condition | Effexor | Wellbutrin | No |
| Bipolar disorder | not for the purpose of | not for the purpose of | |
| attention deficit syndrome (ADHG) | not for the appointment of | yes |
Is Effexor or Wellbutrin more effective?
Effexor and Wellbutrin are effective drugs for the treatment of symptoms of depression. However, the more effective antidepressant is the one that works best for you.
According to a meta-analysis, Effexor and Wellbutrin are equally effective in the treatment of adults with major depressive disorder. Although they both work in the same way, Wellbutrin has been shown to cause less sexual dysfunction as a side effect. Sexual dysfunction is a common side effect of antidepressants, especially selective serotonin reuptake inhibitors (SSRIs).
Although they both work in the same way, Wellbutrin has been shown to cause less sexual dysfunction as a side effect. Sexual dysfunction is a common side effect of antidepressants, especially selective serotonin reuptake inhibitors (SSRIs).
Wellbutrin and effexor have also been compared with SSRI antidepressants such as sertraline, escitalopram, fluoxetine, paroxetine and duloxetine. Clinical trials have shown that Wellbutrin is similar in effectiveness to SSRIs. Conversely, Effexor has been shown to be more effective than SSRIs, although more people may stop taking Effexor due to side effects.
Talk to your doctor about the most appropriate treatment for you. After a complete assessment of your general symptoms, your doctor will work with you to select the appropriate medication.
Coverage and Cost Comparison of Effexor and Wellbutrin
A prescription is required to use Effexor XR. This is usually covered by most Medicare and insurance programs. The average retail price for a 30-day supply of 75mg tablets is about $146. Using an Effexor XR SingleCare card can bring this price down to $15 depending on the pharmacy you use.
The average retail price for a 30-day supply of 75mg tablets is about $146. Using an Effexor XR SingleCare card can bring this price down to $15 depending on the pharmacy you use.
Your doctor will likely prescribe Wellbutrin SR or Wellbutrin XL. These versions of Wellbutrin release the drug gradually in the body. Most Medicare programs and insurance plans cover Wellbutrin XL or Wellbutrin SR. If you don't have insurance, the average cash price of Wellbutrin can be over $100. Even if you have insurance, you can use the Wellbutrin XL SingleCare Card or the Wellbutrin SR SingleCare Card to save on your prescription.
| Effexor | Wellbutrin | |
| yes | yes | |
| Usually covered by Medicare Part D? | yes | yes |
| Standard dosage | Effexor XR: 75 mg tablets once daily (30 pcs. ) ) | Vellbutrin SR / XL: 150 mg once a day (30 pcs.) |
| Typical surcharge Medicare | 0–1 dollar USA | 0–22 dollar | cost Singlecare Cost Singlecare | 15+ US$ | $11 + | |
Common side effects of Effexor compared to Wellbutrin
The most common side effects of Effexor are drowsiness, insomnia, dizziness, nervousness, nausea and headache. Other common side effects include dry mouth, muscle weakness, sweating, and increased heart rate (palpitations). Sexual side effects, including sexual dysfunction and abnormal ejaculation, are also common with Effexor.
The most common side effects of Wellbutrin are insomnia, dizziness, dry mouth, nausea, headache and sweating. Wellbutrin may also cause nervousness, muscle weakness, and palpitations among other side effects.
Effexor and Wellbutrin may also cause weight changes. Both antidepressants can cause either weight gain or weight loss depending on your response to the drug.
Serious side effects of Effexor and Wellbutrin include new or worse mental health problems, suicidal ideation, agitation and hostility. Watch for mood changes while taking these medications. Check with your doctor if you experience serious side effects.
| Effector | Vellbutrin | |||||||||
| Side effect | applicable? | Frequency | Applicable? | Frequency | ||||||
| Drowsiness | yes | 3% | No | - | ||||||
| Headache | Yes | 3% | Yes | 26% | ||||||
| Muscle weakness | Two% | * | * | * | * | Yes | * | Yes | 4% | |
| Sweating | Yes | Two% | 22% | |||||||
| Non -Organized ejaculation | yes | 3% | no | - |
*not reported
Frequency not based on face-to-face trial data. This may not be a complete list of side effects that may occur. Please contact your doctor or health care provider for more information.
This may not be a complete list of side effects that may occur. Please contact your doctor or health care provider for more information.
Source: FDA Label (Effexor), FDA Label (Wellbutrin)
Effexor and Wellbutrin Drug Interactions
Effexor and Wellbutrin may interact with monoamine oxidase inhibitors (MAOIs). Taking MAOIs such as isocarboxazid or phenelzine with effexor or wellbutrin may increase the risk of serotonin syndrome. Effexor and Wellbutrin should not be taken with an MAOI or within 14 days of stopping an MAOI.
Effexor and Wellbutrin may interact with serotonergic drugs. For example, taking a serotonergic drug such as nortriptyline, a tricyclic antidepressant, may increase the risk of serotonin syndrome when combined with another antidepressant. Effexor and Wellbutrin should also be avoided with St. John's wort, an herbal remedy often used for its antidepressant effects. Tell your doctor if you are taking other antidepressants before starting treatment with effexor or wellbutrin.
Effexor and Wellbutrin may increase blood pressure. Therefore, it is important to control blood pressure while taking these medications. Talk to your doctor before taking these medicines if you have a history of high blood pressure.
Some antidepressants, such as SSRIs and SNRIs, may increase the risk of bleeding. The use of Effexor with anticoagulants and other drugs that affect blood clotting should be avoided. Wellbutrin, which is not an SSRI or SNRI, is less likely to affect platelet function.
When used with serotonergic drugs, Effexor and Wellbutrin may increase the risk of serotonin syndrome. Symptoms of serotonin syndrome include palpitations, high blood pressure, and fever. Check with your doctor if you experience any of these symptoms. Serotonin syndrome may be a medical emergency.
Frequently Asked Questions about Effexor and Wellbutrin
What is Effexor?
Effexor is a brand name medication used to treat major depressive disorder. Effexor's generic name is venlafaxine. Effexor XR is an extended version of Effexor that can be taken once a day. Effexor can also treat anxiety and panic disorders.
Effexor's generic name is venlafaxine. Effexor XR is an extended version of Effexor that can be taken once a day. Effexor can also treat anxiety and panic disorders.
What is Wellbutrin?
Wellbutrin is known by the generic name bupropion. It is mainly used to treat major depressive disorder. Wellbutrin is commonly prescribed as Wellbutrin SR or Wellbutrin XL to treat depression and other mental health conditions. The extended release form of Wellbutrin can be taken once a day.
Are Effexor and Wellbutrin the same thing?
Both Effexor and Wellbutrin can treat symptoms of depression. However, Effexor is a serotonin-norepinephrine reuptake inhibitor (SNRI) and Wellbutrin is an aminoketone. Therefore, these drugs work differently. They also have various FDA approved uses.
Is Effexor or Wellbutrin better?
Effexor and Wellbutrin are effective drugs for the treatment of depression. Effexor is better than Wellbutrin for treating anxiety disorders that occur along with depression. However, compared to Wellbutrin, Effexor may cause more sexual side effects such as impaired ejaculation and impotence.
However, compared to Wellbutrin, Effexor may cause more sexual side effects such as impaired ejaculation and impotence.
Can I use Effexor or Wellbutrin while pregnant?
Effexor and Wellbutrin are pregnancy class C and may increase the risk of birth defects. Both drugs are also excreted in breast milk. Effexor and Wellbutrin should be used with caution or avoided during pregnancy.
Can I use Effexor or Wellbutrin with alcohol?
It is not recommended to drink alcohol while taking Effexor or Wellbutrin. Drinking alcohol with Effexor or Wellbutrin may result in increased drowsiness, dizziness, and other side effects. Drinking alcohol may also increase the risk of seizures in people taking Wellbutrin.
why it's not an absolute evil
Cognitive behavioral therapy (CBT) is one of the most popular treatments for depression. It really helps a lot. But it has a side effect: getting rid of negative illusions, the patient is affirmed in positive ones. What it is fraught with, our friends from the Reminder project tell.
What it is fraught with, our friends from the Reminder project tell.
Ben Blennerhassett
In The Noonday Demon, American journalist Andrew Solomon talks about his personal experience of dealing with depression. He managed to alleviate the condition only by creating a fortress around him from Zoloft, Paxil, Navan, Effexor, Wellbutrin, Serzon, Buspara, Zyprexa, Dexedrine, Xanax, Ambien and Viagra. As a result, the fortress walls turned out to be so high that reality was no longer visible because of them. But what if, by escaping depression, we are simultaneously shielding ourselves from reality? This question is asked by the philosopher and psychoanalyst Jules Resche in his Aeon article about the experience of depression. The cause of depression was the breakup of personal relationships. She herself calls her case quite normal. Only the conclusions she came to are unusual.
Today, doctors offer very few options for dealing with depression: either drugs (mainly antidepressants), or psychotherapy, or both in various combinations. Julie Resche, on the advice of friends, chose the "gold standard" in the treatment of depression - cognitive behavioral therapy.
Julie Resche, on the advice of friends, chose the "gold standard" in the treatment of depression - cognitive behavioral therapy.
CBT is based on the theory of cognitive distortions developed in the 1960s by the American psychiatrist Aaron Beck. The idea is that we perceive the world around us through the prism of "cognitive models". They can be compared to Instagram photo filters. In theory, they should convey reality more or less adequately, making the image sharper or brighter. But in practice, failures periodically occur: the details of reality are distorted or erased. Depression is a bug that distorts your world and makes you suffer. But, according to the principles of CBT, only your suffering is real here, because the depressive picture of the world is just an illusion. In fact, the problem is not that your life is meaningless or no one appreciates you, but that, due to a software error, everything is reflected in the negative on the screen of your psyche. The task of a cognitive therapist is to catch and fix such bugs. Then the picture of the world will again become positive. And you will return to reality? Jules Reshe doubts this.
Then the picture of the world will again become positive. And you will return to reality? Jules Reshe doubts this.
Reality is generally a subjective concept. Reche cites the study of the degree of objectivity of self-assessment as an example. It shows that 70-80% of people consider themselves "above average" in almost every dimension: learning ability, productivity, immunity to prejudice, personal well-being, intelligence level. But this cannot be true. Because then "above average" would be the most that neither is the average indicator.
We know from research that our thinking is woven from such illusions. Why is it that a depressed patient, in order to return to reality, is offered to get rid of not all distortions, but only those that interfere with a positive view of the world? At least, this is how Julie Reshe perceived her therapy: “It’s as if I’m a child who needs to be reassured by a good bedtime story so that he forgets about the terrible reality around.” They want to return you not to reality, she writes, but to a positive attitude. The question is how much more real it is than the negative. And if it reflects reality, why is it so difficult to keep it without psychological support, therapy and pills? Resche concludes: “In analyzing my experiences, I began to think that one cannot equate a positive attitude and a healthy perception, as well as between a negative attitude and a distorted perception of reality. What if, in fact, thanks to depression, I finally saw the world for what it is?
The question is how much more real it is than the negative. And if it reflects reality, why is it so difficult to keep it without psychological support, therapy and pills? Resche concludes: “In analyzing my experiences, I began to think that one cannot equate a positive attitude and a healthy perception, as well as between a negative attitude and a distorted perception of reality. What if, in fact, thanks to depression, I finally saw the world for what it is?
Who is closer to reality - an optimist or a pessimist? Take, for example, one important parameter - the illusion of control over the situation. To measure it, scientists recruited students and divided them into two groups according to the results of psychological tests: positive and depressive. Each subject was asked to press the button many times in succession to turn on the green light. The catch was that it periodically flashed without pressing. The students were then asked one question: how many times did they think the light bulb went on at their command. Suddenly, the real realists were students from the depressed group. They gave a more accurate answer. In contrast, participants in the positive group greatly overestimated their degree of control. This conclusion was confirmed by subsequent studies. Australian social psychologist Joseph Forgas has shown that optimists are more prone to stereotypical thinking and simplifications, since they are prone to the fact that in psychology since 19The 80s are called positive illusions.
Suddenly, the real realists were students from the depressed group. They gave a more accurate answer. In contrast, participants in the positive group greatly overestimated their degree of control. This conclusion was confirmed by subsequent studies. Australian social psychologist Joseph Forgas has shown that optimists are more prone to stereotypical thinking and simplifications, since they are prone to the fact that in psychology since 19The 80s are called positive illusions.
Positive illusions are the same perception filters. And although life through them is seen not in black and white, but in pink, they distort reality no less than negative ones. Or maybe more. After all, embellishment means either not noticing flaws, or censoring your impressions. Negative attitude is more honest. According to Resche, it promotes a more skeptical, detailed and focused perception: it enhances critical thinking, eliminates blind faith and sharpens attention. Some psychologists even counter positive illusions with “depressive realism. ” This, of course, is also far from an objective reality. But: "In the mind of a depressed person, the world is reflected more accurately."
” This, of course, is also far from an objective reality. But: "In the mind of a depressed person, the world is reflected more accurately."
Depression, commonly thought of as a dysfunction or disorder, may actually be an evolutionary coping mechanism, suggest psychologists Paul Andrews and Anderson Thomson. Yes, it is a painful experience. But fever during infection is not the most pleasant feeling. When pessimism hits you, Reche writes, don't rush to seek solace in alcohol, religion, or antidepressants. Don't drop the temperature right away. Take this as a chance to become aware of your true feelings and the new reality that is opening before you.
But why do we need awareness if we have to pay such a price for it? “Happiness is in ignorance,” Cypher says in The Matrix when he chooses a virtual heaven over a real hell. We don't really have a choice. You don't have to be a philosopher to understand that suffering is inevitable. Life is not a stream of happiness, the smooth flow of which is sometimes interrupted by minor annoyances. Even if you do not agree with the ideas of Arthur Schopenhauer, the classic of pessimism, who believed that tomorrow will definitely be worse than today, you know that positive illusions periodically collapse, and we have to reassemble our familiar world from their fragments again and again. With age, there are fewer and fewer illusions, and it becomes more and more difficult to rebuild a wall of them to protect against reality. Maybe let it collapse and see what happens when the dust settles. Sounds like surrender?
Even if you do not agree with the ideas of Arthur Schopenhauer, the classic of pessimism, who believed that tomorrow will definitely be worse than today, you know that positive illusions periodically collapse, and we have to reassemble our familiar world from their fragments again and again. With age, there are fewer and fewer illusions, and it becomes more and more difficult to rebuild a wall of them to protect against reality. Maybe let it collapse and see what happens when the dust settles. Sounds like surrender?
No, Jules Reche sees the disillusionment as a path to liberation. The pursuit of happiness, recognized as an “inalienable” human right since the Declaration of Independence, has now become almost a duty, sometimes an addiction, always an escape from the world. It is the pursuit of this elusive illusion that prevents us from feeling truly alive here and now. “We keep on chasing happiness, but it’s depression and existential fear that give us real clarity. Just accept that life is pain and be free.