Does atenolol help with anxiety
Benefits, Side Effects, and Risks
What are beta-blockers?
Beta-blockers are a class of medication that helps control your body’s fight-or-flight response and reduce its effects on your heart. Many people take beta-blockers to treat heart-related conditions, such as:
- high blood pressure
- heart failure
- an irregular heartbeat
Doctors can also prescribe beta-blockers for off-label use like for help managing anxiety symptoms. Read on to learn more about how beta-blockers impact anxiety, and whether they could work for you.
Beta-blockers are also called beta-adrenergic blocking agents. They prevent adrenaline — a stress-related hormone — from making contact with your heart’s beta receptors. This prevents adrenaline from making your heart pump harder or faster.
In addition to relaxing your heart, some beta-blockers also relax your blood vessels, which can help to reduce blood pressure.
There are many beta-blockers available, but some of the more common ones include:
- acebutolol (Sectral)
- bisoprolol (Zebeta)
- carvedilol (Coreg)
- propranolol (Inderal)
- atenolol (Tenormin)
- metoprolol (Lopressor)
All beta-blockers used to treat anxiety are prescribed off-label. Propranolol and atenolol are two beta-blockers that are often prescribed to help with anxiety.
Off-label drug useUsing a drug off-label means that a drug has been approved by the FDA for one purpose, and it’s being used for a different purpose that hasn’t been approved. A doctor can still prescribe it for this purpose because the FDA regulates the testing and approval of drugs, not how doctors use them to treat their patients. Your doctor can prescribe a drug off-label if they think it’s best for your care.
Beta-blockers won’t treat the underlying psychological causes of anxiety, but they can help you manage some of your body’s physical reactions to anxiety, such as:
- a fast heart rate
- shaky voice and hands
- sweating
- dizziness
By decreasing your body’s physical reactions to stress, you may feel less anxious during stressful times.
Beta-blockers work best for managing short-term anxiety about specific events, rather than long-term anxiety. For example, you can take a beta-blocker before giving a public speech if that’s something that makes you feel anxious.
For example, you can take a beta-blocker before giving a public speech if that’s something that makes you feel anxious.
A 2016 review of existing research about using short-term propranolol for treating different anxiety disorders found that its effects were similar to those of benzodiazepines. These are another class of medication that’s often used to treat anxiety and panic disorders. However, benzodiazepines can cause a range of side effects, and some people have a higher risk of becoming dependent on them.
Still, the same review found that beta-blockers weren’t very effective for social phobias.
People respond differently to medications, especially when it comes to treating mental health issues like anxiety. What works for one person may not work at all for someone else. You may also need additional treatment options for your anxiety while taking beta-blockers, to get to the more psychological aspects.
Both atenolol and propranolol come in pill form. The amount you should take depends on both the type of beta-blocker and your medical history. Never take more than what your doctor prescribes.
Never take more than what your doctor prescribes.
You’ll likely notice results the first time you take beta-blockers for anxiety, but they can take an hour or two to reach their full effect. During this time, you’ll feel your heart rate decrease, which might make you feel more relaxed.
Depending on your symptoms, your doctor might suggest taking a beta-blocker regularly or just before stressful events. Usually, beta-blockers will be used in combination with other treatments such as therapy, lifestyle changes, and other medications.
Beta-blockers can cause some side effects, especially when you first start taking them.
Possible side effects include:
- fatigue
- cold hands and feet
- headache
- dizziness or lightheadedness
- depression
- shortness of breath
- vomiting, diarrhea, or constipation
Call your doctor if you experience any more serious side effects, including:
- very slow or irregular heartbeat
- low blood sugar
- an asthma attack
- swelling and fluid retention, along with weight gain
If you notice mild side effects, don’t stop taking the beta-blocker without talking to your doctor first. If you take beta-blockers regularly, you may have serious withdrawal symptoms if you suddenly stop.
If you take beta-blockers regularly, you may have serious withdrawal symptoms if you suddenly stop.
For some people, the side effects of beta-blockers may actually cause anxiety symptoms. You should follow up with your doctor as soon as possible if you feel like taking beta-blockers is increasing your anxiety.
While beta-blockers are generally safe, certain people shouldn’t take them.
Before taking beta-blockers, make sure to tell your doctor if you have:
- asthma
- low blood sugar
- final stage heart failure
- very low blood pressure
- very slow heart rate
If you have any of these conditions or symptoms, you may still be able to take beta-blockers, but you’ll need to work with your doctor to weigh the risks and benefits.
Beta-blockers can also interact with other medications used to treat many heart conditions and antidepressants, so make sure you keep your doctor up to date about any medications, supplements, or vitamins you take.
Beta-blockers can be helpful in managing symptoms for some people with anxiety. It’s been shown as a viable treatment option for short-term anxiety, especially before a stressful event. However, beta-blockers aren’t as useful for long-term treatment.
If you’re interested in trying beta-blockers for managing your anxiety, speak with your doctor. They can advise on the best treatment plan for you that will help manage your specific symptoms.
Benefits, Side Effects, and Risks
What are beta-blockers?
Beta-blockers are a class of medication that helps control your body’s fight-or-flight response and reduce its effects on your heart. Many people take beta-blockers to treat heart-related conditions, such as:
- high blood pressure
- heart failure
- an irregular heartbeat
Doctors can also prescribe beta-blockers for off-label use like for help managing anxiety symptoms. Read on to learn more about how beta-blockers impact anxiety, and whether they could work for you.
Beta-blockers are also called beta-adrenergic blocking agents. They prevent adrenaline — a stress-related hormone — from making contact with your heart’s beta receptors. This prevents adrenaline from making your heart pump harder or faster.
In addition to relaxing your heart, some beta-blockers also relax your blood vessels, which can help to reduce blood pressure.
There are many beta-blockers available, but some of the more common ones include:
- acebutolol (Sectral)
- bisoprolol (Zebeta)
- carvedilol (Coreg)
- propranolol (Inderal)
- atenolol (Tenormin)
- metoprolol (Lopressor)
All beta-blockers used to treat anxiety are prescribed off-label. Propranolol and atenolol are two beta-blockers that are often prescribed to help with anxiety.
Off-label drug useUsing a drug off-label means that a drug has been approved by the FDA for one purpose, and it’s being used for a different purpose that hasn’t been approved.
A doctor can still prescribe it for this purpose because the FDA regulates the testing and approval of drugs, not how doctors use them to treat their patients. Your doctor can prescribe a drug off-label if they think it’s best for your care.
Beta-blockers won’t treat the underlying psychological causes of anxiety, but they can help you manage some of your body’s physical reactions to anxiety, such as:
- a fast heart rate
- shaky voice and hands
- sweating
- dizziness
By decreasing your body’s physical reactions to stress, you may feel less anxious during stressful times.
Beta-blockers work best for managing short-term anxiety about specific events, rather than long-term anxiety. For example, you can take a beta-blocker before giving a public speech if that’s something that makes you feel anxious.
A 2016 review of existing research about using short-term propranolol for treating different anxiety disorders found that its effects were similar to those of benzodiazepines. These are another class of medication that’s often used to treat anxiety and panic disorders. However, benzodiazepines can cause a range of side effects, and some people have a higher risk of becoming dependent on them.
These are another class of medication that’s often used to treat anxiety and panic disorders. However, benzodiazepines can cause a range of side effects, and some people have a higher risk of becoming dependent on them.
Still, the same review found that beta-blockers weren’t very effective for social phobias.
People respond differently to medications, especially when it comes to treating mental health issues like anxiety. What works for one person may not work at all for someone else. You may also need additional treatment options for your anxiety while taking beta-blockers, to get to the more psychological aspects.
Both atenolol and propranolol come in pill form. The amount you should take depends on both the type of beta-blocker and your medical history. Never take more than what your doctor prescribes.
You’ll likely notice results the first time you take beta-blockers for anxiety, but they can take an hour or two to reach their full effect. During this time, you’ll feel your heart rate decrease, which might make you feel more relaxed.
Depending on your symptoms, your doctor might suggest taking a beta-blocker regularly or just before stressful events. Usually, beta-blockers will be used in combination with other treatments such as therapy, lifestyle changes, and other medications.
Beta-blockers can cause some side effects, especially when you first start taking them.
Possible side effects include:
- fatigue
- cold hands and feet
- headache
- dizziness or lightheadedness
- depression
- shortness of breath
- vomiting, diarrhea, or constipation
Call your doctor if you experience any more serious side effects, including:
- very slow or irregular heartbeat
- low blood sugar
- an asthma attack
- swelling and fluid retention, along with weight gain
If you notice mild side effects, don’t stop taking the beta-blocker without talking to your doctor first. If you take beta-blockers regularly, you may have serious withdrawal symptoms if you suddenly stop.
For some people, the side effects of beta-blockers may actually cause anxiety symptoms. You should follow up with your doctor as soon as possible if you feel like taking beta-blockers is increasing your anxiety.
While beta-blockers are generally safe, certain people shouldn’t take them.
Before taking beta-blockers, make sure to tell your doctor if you have:
- asthma
- low blood sugar
- final stage heart failure
- very low blood pressure
- very slow heart rate
If you have any of these conditions or symptoms, you may still be able to take beta-blockers, but you’ll need to work with your doctor to weigh the risks and benefits.
Beta-blockers can also interact with other medications used to treat many heart conditions and antidepressants, so make sure you keep your doctor up to date about any medications, supplements, or vitamins you take.
Beta-blockers can be helpful in managing symptoms for some people with anxiety. It’s been shown as a viable treatment option for short-term anxiety, especially before a stressful event. However, beta-blockers aren’t as useful for long-term treatment.
It’s been shown as a viable treatment option for short-term anxiety, especially before a stressful event. However, beta-blockers aren’t as useful for long-term treatment.
If you’re interested in trying beta-blockers for managing your anxiety, speak with your doctor. They can advise on the best treatment plan for you that will help manage your specific symptoms.
FGBNU NTsPZ. ‹‹Sociophobia››
Introduction
Severe impairment, inappropriate, harmful coping patterns, and comorbid conditions associated with social phobia can be prevented or reduced by early pharmacological and/or psychotherapeutic treatment. Therefore, once a diagnosis of social phobia has been made, it is essential that effective therapeutic measures be applied without delay.
Unfortunately, only about 25% of those suffering from social phobia are currently receiving any treatment, and even fewer patients receive therapy with proven effectiveness. nine0005
When to treat
In general, the decision to treat social phobia should be reserved for those cases in which the symptoms of the disease or avoidance behavior are associated with significant psychosocial impairment.
Treatment should be offered to any patient in whom avoidance behavior interferes with work or social life, who is greatly disturbed by fears, or whose ability to form social bonds is severely impaired. nine0005
To assess the degree of maladaptation in a particular patient, special scales have been developed (see Annexes I and II). These scales are a good illustration of what needs to be assessed to decide on the severity of symptoms.
How to present to the patient the need for treatment
Many patients with social phobia have never heard of such a disease. They may view their symptoms as extreme timidity or unfortunate personality traits, so they should be reassured that long-term treatment can help them. nine0005
Devoting sufficient time to explain the need for drug therapy can markedly improve patient compliance and patient satisfaction with treatment outcomes.
There are five complementary approaches to presenting the need for treatment to the patient:
emphasize that social phobia is a well-studied disease and that, according to many studies, it responds well to appropriate treatment; nine0005
Explain that phobic avoidance is caused by anxiety. Medications can directly reduce this anxiety;
Medications can directly reduce this anxiety;
in generalized social phobia explain that over-sensitivity to criticism or rejection can be specifically affected by certain medications;
explain that the drug treatment is not addictive, will not be habit-forming, and will not cause withdrawal symptoms when stopped; nine0005
Establish a treatment "contract" with the patient. Medical "contract"
A formal treatment contract can go a long way in helping the patient comply with medical advice. The contract must:
explain the patient's symptoms as a social phobia
emphasize that social phobia is a well-recognised disease that responds well to treatment
describe the treatment regimen
list problems and priorities nine0005
set a realistic time frame for improvement
discuss regular review of the treatment regimen.
How long to treat
It is important to specifically point out to the patient that social phobia is a chronic disease that is likely to require long-term treatment.
Even if treatment is continued for 6 months, the relapse rate after discontinuation of drugs is about 50%.
Therefore, drugs should be discontinued gradually, with occasional attempts to reduce the dose. nine0003 Management of non-responders
Pharmacotherapy should begin with the most effective and safest drug available. After the initial period of treatment (1 2 months), it is necessary to evaluate the clinical effectiveness (see table). If the patient's symptoms persist to a significant extent, the doctor may increase the dose to the maximum effective one or prescribe a drug from a different group. You should also be aware of the possible use of psychotherapy in addition to taking medications. nine0005
Clinical response evaluation
The outcome of a pharmacotherapeutic intervention can be assessed by the presence of a significant improvement in the following areas:
anxiety that the patient feels during social communication or the need for any activity, and also, possibly, the quality of the performance of this activity and social interactions
- anxiety experienced in anticipation of a "frightening" situation (premonition anxiety)
- avoidance of social interaction or commitment, opportunities to form relationships or perform activities
- comorbidity associated with social phobia such as secondary depression, demoralization or alcoholism
general functional disorders caused by social phobia.
Adapted from Social Phobia Diagnosis, Assessment and Treatment. Ed.: Heimberg, Liebowitz, Hope and Schneier. The Guildford Press. London. In press. nine0088
Drug choice
Drugs commonly effective in social phobia include inhibitors of the enzyme monoamine oxidase in the central nervous system, reversible monoamine oxidase inhibitors (RIMAs) and monoamine oxidase inhibitors (MAOIs). Other drugs used in the treatment of social phobia include benzodiazepines, beta-blockers, and selective serotonin reuptake inhibitors (SSRIs).
OIMA
RIMAs are a new class of drugs that selectively act on the monoamine oxidase A isoenzyme. RIMAs bind reversibly to the isoenzymes so that MAO activity is restored after a decrease in the serum concentration of the drug.
RMAs are safer and better tolerated than MAOIs.
The AMI drug moclobemide was studied in four placebo-controlled studies, one of which was on long-term therapy. Studies included more than 1000 patients with social phobia and showed significant benefits and a pronounced dependence of the effectiveness of the drug on the dose. nine0005
Studies included more than 1000 patients with social phobia and showed significant benefits and a pronounced dependence of the effectiveness of the drug on the dose. nine0005
In a comparative study, a good effect was observed in 80-90% of patients treated with moclobemide or phenelzine, in whom the symptoms of social phobia almost disappeared after 16 weeks.
RIMA was much better tolerated than the older drug, with adverse reactions occurring in approximately 11.8% of patients treated with moclobemide compared with 95.2% of patients treated with phenelzine. In the phenelzine group, adverse reactions also persisted longer, were more pronounced, occurred in greater numbers per patient, and required more measures to control and eliminate them. nine0005
Moclobemide is the only drug that has been studied in long-term studies for the treatment of social phobia. However, it is still too early to estimate the frequency of relapses after its withdrawal. It is possible that in order to maintain the effect achieved with the help of pharmacotherapy, a method of selective "immersion" in frightening situations and behavioral correction is necessary.
Reversible monoamine oxidase inhibitors for social phobia
| Treatment | p | Dose (mg/day) | Duration (weeks) | Results |
| International Multicenter Study Group, presented at the European Congress of Minor Psychiatry, 1994 | 578 | 300-600 | 10-12 | nine0118 |
| US multicenter study group presented at ECMP 1994 | 506 | 75-900 | 12 | Pronounced dose-response |
| Versiani et al. | 78 | up to 600 up to 90 | 16 | Significant benefits of both moclobemide and phenelzine over placebo. More adverse reactions to phenelzine. |
| Versiani et al. (Long study), data from the archives of F. Hoffmann-La Roche Ltd. | 101 | up to 750 mg | up to 44 months | Maximum effect between 4 and 6 months of treatment. Relapse after drug withdrawal |
| Bisserbe et al., Clin Neuropharmacol., 1994 | 35 | 300-600 | 12 | Significant benefits in 48% of patients |
| van Vliet et al. | 30 | 150 | 12 | Significant advantage over placebo |
 , Br J. Psychiatry, 1992
, Br J. Psychiatry, 1992  , Eur Neurophsychopharmacol., 1992
, Eur Neurophsychopharmacol., 1992 MAOIs
Phenelzine, a monoamine oxidase inhibitor, has been shown to provide rapid benefit in approximately 60-75% of patients; while a significant clinical improvement is observed after 8-12 weeks of treatment (see table). With long-term use, phenelzine remains effective: although a fairly high relapse rate is observed after discontinuation of treatment. nine0005
One of the problems associated with phenelzine therapy is how to convince patients to follow their doctor's orders.
A number of unpleasant side effects can cause a large number of patients to drop out of a treatment program before it is fully effective. These adverse reactions include hypertensive crisis in non-compliance with dietary restrictions (refusal of tyramine-containing products), insomnia, sexual dysfunction, orthostatic hypotension and weight gain.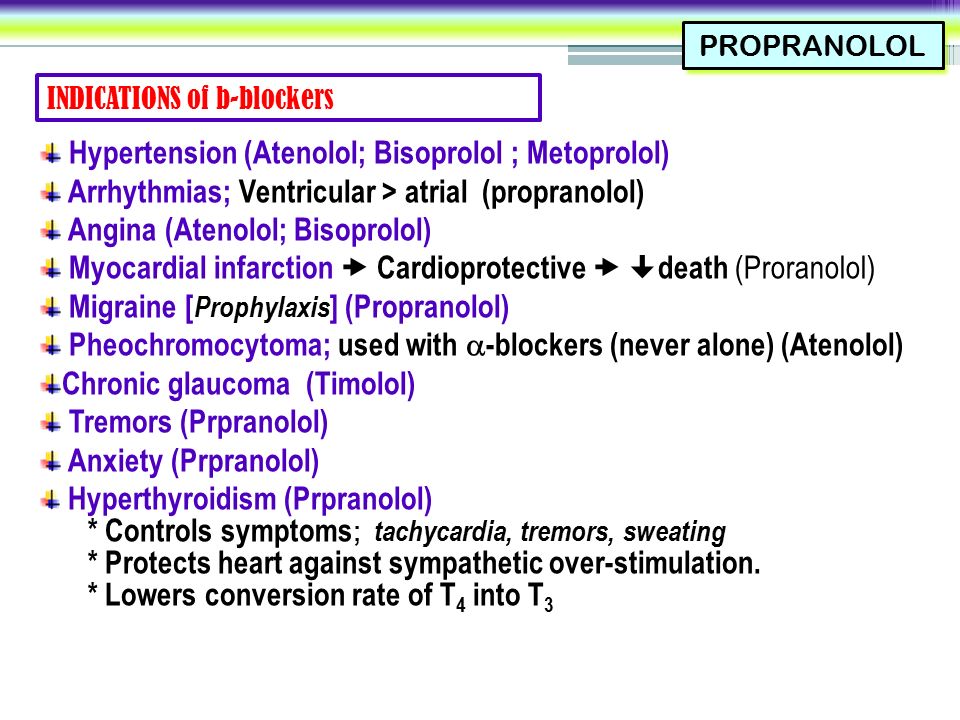 nine0005
nine0005
In addition to phenelzine, other irreversible monoamine oxidase inhibitors have been studied, although data from controlled studies are not available. The results of two open studies of tranylcypromine indicate the therapeutic efficacy of the drug. Phenelzine for social phobia
| Treatment | n | Dose (mg) | Results |
| Liebowitz et al., Arch Gen Psychiatry, 1992 | 74 | 60 100 | Significant improvement in 64% of patients on phenelzine, 30% on atenolol, and 23% on placebo |
| Versiani et al., Br. J Psychiatry, 1992 | 74 | up to 90 up to 600 | nine0118 |
| Gelernter et al., Arch Gen Psychiatry, 1991 | 65 | up to 90 up to 7.3 | According to subjective assessment scales significant improvement in all groups |
 Moclobemide is better tolerated
Moclobemide is better tolerated Benzodiazepines
Benzodiazepines have not gained a reputation as suitable drugs for the treatment of social phobia.
A possible exception is clonazepam, which also has serotonergic effects. In one placebo-controlled study of 75 patients treated with either clonazepam or placebo for 10 weeks, it was found that a positive response to treatment was observed in 78% of patients on benzodiazepine and only 20% on placebo. However, the treatment of social phobia with benzodiazepines has disadvantages, not the least of which is the danger of developing physical dependence in patients receiving this therapy for a long time. The link between social phobia and alcoholism also suggests that in many patients benzodiazepines should not be the drug of choice. nine0005
The link between social phobia and alcoholism also suggests that in many patients benzodiazepines should not be the drug of choice. nine0005
b-blockers
There is very little evidence that b-blockers have any beneficial effect on the underlying disease in social phobia. However, they can be taken intermittently to relieve the tremors, palpitations, and tachycardia that people with social phobia often experience in certain situations that force them to be active.
For this reason, many patients with social phobia take drugs such as propranolol when needed. nine0003 Other medicines
Open studies have suggested that a number of other drugs may be used for social phobia. The most promising of these are buspirone, a non-benzodiazepine anxiolytic, and fluoxetine and fluvoxamine, selective serotonin reuptake inhibitors.
Comorbidity
One of the main problems in the treatment of social phobia is the extremely high prevalence of comorbid conditions. nine0005
nine0005
As a general rule, it is preferable to treat with a single drug that is effective for each component of the pathology. If one of the diseases is clearly secondary, treatment can be focused on the primary pathology. Combination therapy with the use of compatible drugs may also be required, each of which has an effect on “its own” disease.
When social phobia is combined with depression, treatment should include antidepressants suitable for both disorders, such as ARMI, MAOIs, and SSRIs. nine0005
It should be noted that SSRIs, which are the drugs of choice for obsessive-compulsive disorders, may not be as effective when social phobia is present. It has recently been found that patients with social phobia who also have obsessive-compulsive disorders respond worse to SSRIs than to MAOIs.
When treating patients with social phobia with comorbid panic disorder or a history of any unexpected panic symptoms, SSRIs and tricyclic antidepressants should be started at very low doses to avoid exacerbation of panic symptoms. nine0005
nine0005
Because of the risk of dependence, benzodiazepine treatment should be undertaken with great caution.
Pharmacological approaches to social phobia and comorbid conditions
Social phobia and depression
- OIMA
- IMAO
- SSRIs
Social phobia and alcoholism
- OIMA
- SSRIs
Social phobia and obsessive-compulsive disorder nine0005
- SSRIs
- Clomipramine
- IMAO
- AIMA
Social phobia and panic disorder/agoraphobia
- 0IMA
- IMAO
- Clonazepam
- SSRIs
Social phobia psychotherapy
The purpose of psychological care is to help patients cope with negative attitudes, such as belief in the inevitability of failure or failure in social situations, attitudes that are believed to underlie social phobia. nine0005
A number of studies evaluating the use of cognitive therapy in the treatment of social phobia have yielded interesting results, although some adjustments need to be made to these findings. Most of the studies were very small in size and did not have sufficient statistical power to adequately assess treatment efficacy. In addition, a difficulty in the study of behavioral therapy lies in the selection of a truly neutral control group.
Most of the studies were very small in size and did not have sufficient statistical power to adequately assess treatment efficacy. In addition, a difficulty in the study of behavioral therapy lies in the selection of a truly neutral control group.
Since one of the main goals of cognitive therapy is to help patients cope with their anxiety, group forms of treatment are especially useful for social phobia. Psychotherapeutic techniques can be used as an adjunct or alternative to pharmacotherapy. nine0005
Summary
Social phobia lends itself well to baking.
Early initiation of therapy may prevent severe maladjustment, the development of inadequate adaptive mechanisms, and the occurrence of comorbid conditions such as severe depression and alcoholism.
Treatment should be initiated when symptoms or avoidance behaviors are accompanied by significant psychosocial impairment.
Patients will better follow doctor's advice if they are informed that they are likely to need medication for a period of time and the rationale for such treatment is explained. nine0005
nine0005
It has been established that the most effective pharmacological drugs for the treatment of social phobia are inhibitors of the enzyme monoamine oxidase in the central nervous system OMA and MAOI. Other drugs used to treat social phobia are benzodiazepines, b-blockers, and SSRIs.
Psychotherapy may also be useful and is used either as monotherapy or in combination with drugs.
Migraine prophylaxis - effective for migraine, migraine preventive treatment
- Home
- >Headache
- >Migraine
- >Migraine prevention
Migraine prevention really exists. The bottom line is that a person with this type of headache every day, for a certain time, takes a certain drug. His choice is made by a neurologist after examination. This medicine is effective for migraine, because it does not act on the symptoms, but on the very mechanisms of development of attacks. Due to this, the number and severity of migraine attacks are reduced, and the burden of consumed painkillers is reduced. nine0005
nine0005
But this prophylactic treatment for migraine is not given to all patients with migraine.
It is justified if:
- headache attacks increase up to eight times a month or twice a week;
- Even special anti-migraine painkillers – triptans – are of little help to a person: amigrenin, relpax, zomig;
- the patient cannot take analgesics and triptans due to contraindications - in the presence of uncontrolled hypertension, coronary heart and brain disease, after a heart attack; nine0423
- a person does not tolerate migraine medication well. So, for example, in some people, after taking such drugs, blood pressure rises or falls, and the pulse quickens. There are flushes of heat and a sensation of a lump in the throat. Abdominal pain and dry mouth appear. And although these side effects are temporary, not all patients can put up with them;
- a person has a rare hereditary form of headache - the so-called hemiplegic migraine. With its development, the risk of stroke increases.
 nine0423
nine0423
Choosing a Migraine Prevention Drug
Seven groups of drugs are currently used as treatment for migraine prevention, ranging from blood pressure medications to drugs to reduce female sex hormones. Almost all drugs used for the prevention of migraine were discovered by chance, in their practical use, and were not created specifically for this purpose. Therefore, at first glance, it may seem strange why a person with migraine is given a medicine for epilepsy or depression. And so that he does not have a desire to cancel it, the doctor explains what his benefits are. nine0005
Choosing such a preventive drug for migraine is an art. The doctor must take into account the mechanism of its action, effectiveness, range of adverse reactions. Looks at a person's comorbidities. First of all, on the existing mental disorders. When choosing a drug for the prevention of migraine, it is important that the prescribed drug does not exacerbate these problems, but helps to treat them. It also takes into account previous experience with the use of drugs and their compatibility. For example, concomitant use of vasodilators may negate all preventive treatment for migraine. nine0005
In addition, it must be taken into account that there may not be a quick effect of such treatment. We need to wait, be patient. Preparations for the prevention of migraine show their properties within three months. In this case, the treatment is considered effective if the number of attacks is halved. For example, if you used to have a migraine eight times a month, and now only four, that's good. In the future, there will be even fewer attacks. And those that do occur can be treated with smaller doses of analgesics and triptans. nine0005
Migraine prevention with Botox
In addition to drugs, Botox and its analogues are used to prevent migraine. Migraine prevention with Botox is now the "gold standard" of treatment. This is a scientifically proven, well-tested and proven technique.
The drug is injected into places of greatest tension and pain on the head. It relaxes stiff muscles. The nerve endings that transmit pain are blocked. And thus the frequency and strength of migraine attacks is reduced. nine0005
One injection usually lasts 4-6 months. Then the drug is completely excreted from the body. And its introduction can be repeated. And if you don’t like something, refuse or reduce the dose of the medicine. Moreover, if the injected Botox causes discomfort, there are approaches that allow you to neutralize its effect ahead of time.
Migraine prophylaxis needs to be repeated
However, no matter how successful migraine prophylaxis is, it will not be possible to get rid of migraine forever. After all, migraine is a chronic disease, most often embedded in the genes. This means that under the influence of various provocateurs (causes of migraine) and at different periods of life, migraine can return. Therefore, it is necessary to carry out the prevention of migraine from time to time. It is possible to change the drugs, their dosages, the mode of application. nine0005
It is possible to change the drugs, their dosages, the mode of application. nine0005
But a person's own attitude towards illness is also important. Every migraine patient should understand that the frequency of migraine is directly related to his lifestyle.
It is necessary to identify all your personal risks - those factors that provoke a migraine attack specifically for you. They can be stress or any strong emotions, lack of sleep, processing at the computer, eating certain foods or drinks, inhaling odors.
And as soon as the impact of one of these factors is expected, preventive treatment for migraine is applied the day before. Say, if you know that in two days you will take an exam, sleep little and strain your eyesight a lot, you need to take, for example, some kind of nootropic. So called drugs to improve blood flow in the brain. nine0005
Another purely female case of episodic migraine prophylaxis is menstrual migraine. It appears at the end of the cycle due to a drop in hormone levels. In this situation, 3-4 days before the onset of menstruation, a woman is recommended to take NSAIDs - non-steroidal anti-inflammatory drugs. This will help prevent the development of severe attacks and serve as a good prevention of migraine.
In this situation, 3-4 days before the onset of menstruation, a woman is recommended to take NSAIDs - non-steroidal anti-inflammatory drugs. This will help prevent the development of severe attacks and serve as a good prevention of migraine.
Migraine prophylaxis drugs
| Drug group | Drug examples | Comorbidities not prescribed | Comorbidities not prescribed | ||
|---|---|---|---|---|---|
| Hypertension drugs: 1. Beta-blockers | Propranolol, Metoprolol, Atenolol, Deprolol | hemiplegic migraine is a hereditary form of the disease with aura and an increased risk of stroke. Caution - low blood pressure | Hypertension, coronary heart disease, panic attacks | Increased blood clotting and tendency to form blood clots, severe varicose veins, previous or threatened stroke | Hormone-dependent types of migraine, primarily menstrual migraine |
| Non-steroidal anti-inflammatory drugs | Ibuprofen, Naproxen, 950,61 | Menstrual migraine, arthritis and other pain syndromes | |||
| Botulinum toxin type A | Botox, Xeomin, Lantox | Severe liver and kidney disease, high degree of myopia, allergies, tendency to bleed, hemophilia, cancer | Chronic migraine, failure of drug prophylaxis or drug intolerance |
For effective migraine prevention, contact a specialist: Valentinovna
Chief physician, doctor of medical sciences, professor, neurologist of the highest category
Filatova Elena Glebovna
neurologist, professor, doctor of medical sciences
Oknin Vladislav Yuryevich
Neurologist, Doctor of Medical Sciences
Ekusheva Yevgenia Viktorovna
Neurot, Professor
Latmysheva Nina Ninaovna Ninaovna.