Do i need to see a therapist for depression
SAMHSA’s National Helpline | SAMHSA
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Main page content
-
SAMHSA’s National Helpline is a free, confidential, 24/7, 365-day-a-year treatment referral and information service (in English and Spanish) for individuals and families facing mental and/or substance use disorders.
Also visit the online treatment locator.
SAMHSA’s National Helpline, 1-800-662-HELP (4357) (also known as the Treatment Referral Routing Service), or TTY: 1-800-487-4889 is a confidential, free, 24-hour-a-day, 365-day-a-year, information service, in English and Spanish, for individuals and family members facing mental and/or substance use disorders.
This service provides referrals to local treatment facilities, support groups, and community-based organizations.
Also visit the online treatment locator, or send your zip code via text message: 435748 (HELP4U) to find help near you. Read more about the HELP4U text messaging service.
The service is open 24/7, 365 days a year.
English and Spanish are available if you select the option to speak with a national representative. Currently, the 435748 (HELP4U) text messaging service is only available in English.
In 2020, the Helpline received 833,598 calls. This is a 27 percent increase from 2019, when the Helpline received a total of 656,953 calls for the year.
The referral service is free of charge. If you have no insurance or are underinsured, we will refer you to your state office, which is responsible for state-funded treatment programs. In addition, we can often refer you to facilities that charge on a sliding fee scale or accept Medicare or Medicaid. If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
The service is confidential. We will not ask you for any personal information. We may ask for your zip code or other pertinent geographic information in order to track calls being routed to other offices or to accurately identify the local resources appropriate to your needs.
No, we do not provide counseling. Trained information specialists answer calls, transfer callers to state services or other appropriate intake centers in their states, and connect them with local assistance and support.
-
Suggested Resources
What Is Substance Abuse Treatment? A Booklet for Families
Created for family members of people with alcohol abuse or drug abuse problems. Answers questions about substance abuse, its symptoms, different types of treatment, and recovery. Addresses concerns of children of parents with substance use/abuse problems.
Addresses concerns of children of parents with substance use/abuse problems.It's Not Your Fault (NACoA) (PDF | 12 KB)
Assures teens with parents who abuse alcohol or drugs that, "It's not your fault!" and that they are not alone. Encourages teens to seek emotional support from other adults, school counselors, and youth support groups such as Alateen, and provides a resource list.After an Attempt: A Guide for Taking Care of Your Family Member After Treatment in the Emergency Department
Aids family members in coping with the aftermath of a relative's suicide attempt. Describes the emergency department treatment process, lists questions to ask about follow-up treatment, and describes how to reduce risk and ensure safety at home.Family Therapy Can Help: For People in Recovery From Mental Illness or Addiction
Explores the role of family therapy in recovery from mental illness or substance abuse. Explains how family therapy sessions are run and who conducts them, describes a typical session, and provides information on its effectiveness in recovery.
For additional resources, please visit the SAMHSA Store.
Last Updated: 08/30/2022
SAMHSA Behavioral Health Treatment Services Locator
HomeWelcome to the Behavioral Health Treatment Services Locator, a confidential and anonymous source of information for persons seeking treatment facilities in the United States or U.S. Territories for substance use/addiction and/or mental health problems.
PLEASE NOTE: Your personal information and the search criteria you enter into the Locator is secure and anonymous. SAMHSA does not collect or maintain any information you provide.
Please enter a valid location.
please type your address
-
FindTreatment.
 gov
gov Millions of Americans have a substance use disorder. Find a treatment facility near you.
-
988 Suicide & Crisis Lifeline
Call or text 988
Free and confidential support for people in distress, 24/7.
-
National Helpline
1-800-662-HELP (4357)
Treatment referral and information, 24/7.
-
Disaster Distress Helpline
1-800-985-5990
Immediate crisis counseling related to disasters, 24/7.
- Overview
- Locator OverviewLocator Overview
- Locator OverviewLocator Overview
- Finding Treatment
- Find Facilities for VeteransFind Facilities for Veterans
- Find Facilities for VeteransFind Facilities for Veterans
- Facility Directors
- Register a New FacilityRegister a New Facility
- Register a New FacilityRegister a New Facility
- Other Locator Functionalities
- Download Search ResultsDownload Search Results
- Use Google MapsUse Google Maps
- Print Search ResultsPrint Search Results
- Use Google MapsUse Google Maps
- Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
 Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). - Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). Find programs providing methadone for the treatment of opioid addiction (heroin or pain relievers).
The Locator is authorized by the 21st Century Cures Act (Public Law 114-255, Section 9006; 42 U.S.C. 290bb-36d). SAMHSA endeavors to keep the Locator current. All information in the Locator is updated annually from facility responses to SAMHSA’s National Substance Use and Mental Health Services Survey (N-SUMHSS). New facilities that have completed an abbreviated survey and met all the qualifications are added monthly. Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Depression: when should I go to a psychiatrist?
~ The article describes well when and why in case of depression one should go to a psychiatrist or choose a psychologist very carefully, how to talk to a depressed person, what is dangerous to ignore the state ~
Who to go to: a psychologist, psychotherapist or psychiatrist?
You can find out if you have depression using the Beck or Hamilton Depression Scale. Often with depression, people start with a psychologist or psychotherapist, but you need to carefully choose a specialist.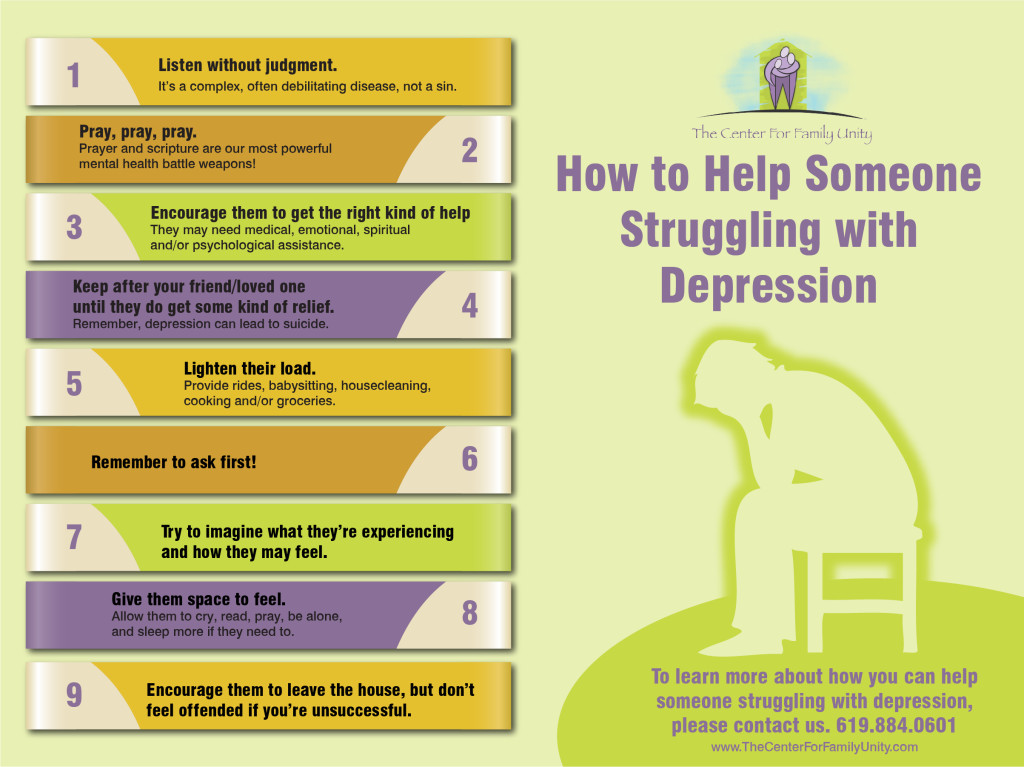 A psychotherapist is not a shaman, not a stage hypnotist, he is a doctor who treats without drugs, you can find him in a psychiatric clinic.
A psychotherapist is not a shaman, not a stage hypnotist, he is a doctor who treats without drugs, you can find him in a psychiatric clinic.
What a depressed person says:
- My hands drop.
- Everything has lost its meaning.
- Nothing pleases me.
- I feel bad.
- I don't want anything.
When choosing a psychologist, you need to be careful. There are psychologists who understand that their client has a clinical problem that requires the intervention of another specialist, and there are those who say to a mentally ill person: “You don’t need to see a doctor, you don’t need to take pills.” It is best to contact a psychologist after visiting a psychiatrist.
For example, if you have sleep disorders, it is better not to see a psychologist, but go straight to a psychiatrist. And not only with them. If you feel bad not only morally and emotionally, but also physically, if you have weight loss, a violation of pressure, interruptions in the work of the heart, pain in the chest and abdomen, then you better immediately see a psychiatrist.
If you feel bad not only morally and emotionally, but also physically, if you have weight loss, a violation of pressure, interruptions in the work of the heart, pain in the chest and abdomen, then you better immediately see a psychiatrist.
10 reasons to see a psychiatrist
People are afraid of psychiatrists, and even more afraid of pills. In vain they are. Maria Leibovich, 9 told Pravmir about this0010 factory Department of Rehabilitation NTSPZ (Scientific Center for Mental Health), psychiatrist, psychotherapist of the highest category, Ph.D.
1. A person may not notice how far things have gone
The first time I went to the doctor at the age of 34, when several events happened at the same time: the child got two in the quarter, I was called to school for dressing, my husband and I had a fight, I lost a job that didn't pay me for the last two months. And I cried all the time. I just couldn't stop crying.
I cried at home when I was brushing my teeth, I cried on the subway on my way to work, I cried on the escalator. I also cried at work. It made my life very difficult and I couldn't stop crying.
I asked my friends to find a doctor for me and went to surrender to a psychiatric dispensary. There she received her diagnosis and her first prescription. There I learned that my depression is endogenous, hereditary. I think the first depressive episodes were in childhood and adolescence, but I just didn’t understand why I was constantly feeling so bad and wanting to die. I have since learned to live with my depression and keep it under control.
Depression is often associated with weakness, so people endure it and don't go to the doctor. And the symptoms get worse.
It's like gaining weight: size 42 gradually increased to size 52. A person who has not seen you for a long time will say: “Wow, how you have changed.” So the symptoms of depression most often appear and intensify gradually, day after day.
Usually the first time a person comes to us in the most difficult condition. This is a 100% rule. On the second and subsequent visits, no one comes in such a serious condition as the first, because they already know what is happening. I have a patient who initially required medical treatment because he had an advanced condition. The second time, no medication was needed, there was enough psychotherapy to cope. He has learned to determine these states himself, he knows what to do.
Signs of depression must be sufficiently persistent to be diagnosed with depression. Everyone can spend the day in bed. We all get in a bad mood from time to time, we can spend the weekend without getting out of bed, but a walk, rest or a good event changes our mood. There may simply be no appetite for a couple of days, and when these symptoms last longer than two weeks, and changes in the external situation do not affect them, then this is depression.
2. Relatives cannot objectively assess the severity of a person's condition
Almost all depressed patients say that they are not understood at home: “ They tell me that I am lazy, I don’t want to control myself, I make up everything ”. You need to take seriously the feelings of a person who says that he is ill.
You need to take seriously the feelings of a person who says that he is ill.
I had a patient whose mother believes that the best remedy for depression is to clean the floor in the whole apartment.
Washing floors can help if a person is a little sad and anxious, not when depressed. But if a person does not get up for 2-3 days, does not wash, does not brush his teeth and does not go outside, then mopping the floor will not help him.
It will be good if relatives can create conditions for a depressed person to start talking about his experiences. And when a person says: “ I feel bad. It seems to me that my life does not make sense ”, and they answer him:“ Pull yourself together ”, the person closes, he will not tell anything. You need to say: “ I see that you feel bad. Do you want to talk to me? Do you want to go for a walk? Is there anything I can help you with? » If a person refuses, then there is no need to insist. Contact may not take place immediately, sometimes you need to wait, just be there.
My patients say: “Those who have not experienced such a state will not understand. Let them at least not advise what to do.
The offer “If you want, I will come and cook soup for you” is valuable for a depressed person. But teachings and advice - no.
3. Not every depression can go away on its own
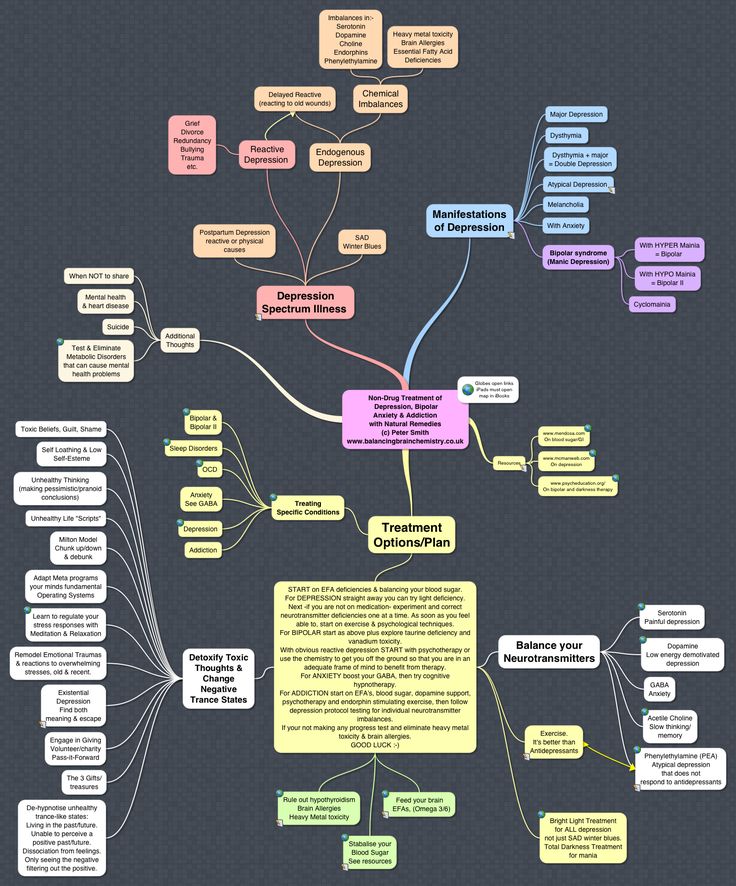
There are two types of depression. Depression, which is provoked by some external factors, is called reactive . Reactive depression, as a person has coped with the condition or the external situation has changed, can pass by itself. The duration of reactive depression is very dependent on the individual. It happens (usually this happens after the death of a parent), people come to us only after 3-4 years. That is, a person is in a subdepressive state, then his condition is worse, then better.
There is endogenous depression that comes from within. Endogenous depression rarely resolves on its own. It can escalate, subside, and escalate again. But usually it doesn't go away on its own. The causes of endogenous depression are the lack of neurotransmitters (serotonin, norepinephrine, dopamine).
It can escalate, subside, and escalate again. But usually it doesn't go away on its own. The causes of endogenous depression are the lack of neurotransmitters (serotonin, norepinephrine, dopamine).
Many are confused by the fact that in psychiatry the main method of research is conversation. How can a doctor just tell me what disease I have? They just talked to me.
Yes, there are many types of tests now, but they are used more for research purposes than for diagnosis. Separately, without a general clinical picture, such studies are not indicative.
4. Only a doctor can recognize some conditions
There was no loss of energy, so at first I did not think about depression, but I was tormented by a feeling of depression, which did not allow me to sleep, eat, or communicate. For eight months it got worse and worse, and at some point it became clear that it would not go away on its own. I turned to a specialist, he prescribed pills, it became easier.
Depression can be hidden, invisible to others. For us psychiatrists, one of the most difficult types of depression is “ironic depression”. When a person does not say: “I’ll go out the window now” or “I feel bad”, and when he has an ironic mask on his face. The person smiles, and to the question: “How are you?” he answers with restraint that everything is fine with him, ironically refers to his oppressed state. A person with ironic depression is dangerous in terms of committing sudden suicides.
But don't take the blame for unnoticed depression. In fact, it is impossible for a non-specialist to recognize some states. Relatives of our patients blame themselves for not noticing changes in a person. But they didn't notice because they never experienced these problems.
5. Sometimes a person needs help to get to the doctor
Someone comes to the doctor himself, someone is brought by relatives. Someone asks relatives to bring him. Our patients often say that they were going to see a specialist for six months, but still could not decide. A relative can offer help: “Do you want me to go to the doctor with you?” Sit in line, stand next to me, just for the sake of support. This is very valuable for a depressed person.
Our patients often say that they were going to see a specialist for six months, but still could not decide. A relative can offer help: “Do you want me to go to the doctor with you?” Sit in line, stand next to me, just for the sake of support. This is very valuable for a depressed person.
6. Postpartum depression: it is very serious and will not go away on its own.
A woman with postpartum depression is immediately visible. The mother of the newborn is very involved in it. The woman was expecting that she would give birth to a child, there was a joyful premonition, and after the birth she suddenly lay down and could not get up. Or suddenly anxiety sets in. Postpartum depression is difficult to confuse with something. The state changes suddenly: CLICK, and it became like this.
The worst thing is that there are those who really go out the window. If you suspect a woman has postpartum depression, you need to grab her in an armful and take her to the doctor.
There are women who endured the most difficult period, 2-3 months, and somehow managed on their own, but many still have some rudimentary symptoms - some have obsessive states, some have fears, some are afraid going out. Postpartum depression leaves a mark, someone will have fears and anxieties, and someone's husband may leave.
Another argument in favor of antidepressants. They allow to reduce social losses to a minimum. Maintain quality of life. After all, due to illness, a person can lose his job, family, friends.
7. Antidepressants really help
Psychiatric intervention improves the quality of life, antidepressants are a temporary measure, it allows you to survive the acute period without loss. In my practice, I often encounter those people who take medication and return to normal life. There is no dependence on antidepressants. It is a myth. There is no physical dependence on antidepressants. And psychological dependence can arise from anything, from shopping, from your favorite cups of coffee.
Now the level of development of psychopharmacology is such that it allows you to choose a medicine in most cases, the patient will not notice the side effects of this medicine. A “vegetable”, inhibited state that everyone is afraid of, severe sedation, etc. is either a necessary moment in the treatment of severe conditions, or a short period at the beginning of treatment. It is important to discuss everything with the doctor, tell him about your symptoms so that he can adjust the treatment.
There are three groups of antidepressants: sedatives - those that calm, stimulants - for those who cannot get out of bed, and drugs of a balanced type.
When a person in depression cannot sit still, his head is constantly spinning with different thoughts, then we, doctors, make a choice in favor of sedatives. If we see lethargy, apathy, drowsiness, fatigue in our patient, he does not have the strength and desire to live, we prescribe stimulating antidepressants. But most often we use antidepressants with a balanced effect, in which there is both, which even out the condition.
Usually we wait 7-10 days for the result, during which time the drug accumulates in the blood. As a rule, after this we see a reduction in symptoms: their decrease or disappearance. The patient comes to us a week later and says that he has become much calmer.
In general, in psychiatry, everything does not happen quickly. But when the condition improves, the person feels it. You can't confuse this with anything.
8. Due to depression, you will not be registered with the PND and will not be reported to work that's why it functions every other time and is always ready to hang, slow down. I couldn’t go anywhere except work, sometimes I see an interesting event in the evening, I have to go after work, and at the end of the working day I sit and I can’t get up from my chair, raise my hand. He began to fall on the streets, sometimes in dangerous places, once he fell on the tram tracks. There were also thoughts of suicide.
People are afraid that if they see a doctor with depression, they will be registered and sent to work. It is not true. Accounting is a form of dispensary work. And what everyone is afraid of and calls accounting is most likely “observation”.
It is not true. Accounting is a form of dispensary work. And what everyone is afraid of and calls accounting is most likely “observation”.
The IPA reports a person who is a danger to himself or to society when there is a risk that he will not take his pills when he is discharged from the clinic. He is reported to need to be monitored, he will come to the PND once a week, the doctors will monitor whether he is taking pills and see how he feels. But this is 2% of all patients.
Now the law is generally on the side of the patient. The patient, before starting to talk with a psychiatrist, signs a paper about who exactly he allows to report information about his illness. I repeat, before the conversation, not after. One person wrote that it is possible to provide health information to parents and sister. And another girl wrote: "No one." If her parents come and ask if it is possible to find out what their daughter is being treated for, then we will answer: “No.” This information can only be requested at the request of the court. We do not tell any employer. How do you imagine it? I call the patient at work and say: “You know, the psychiatrist is worried about you ...” No. We don't do that.
We do not tell any employer. How do you imagine it? I call the patient at work and say: “You know, the psychiatrist is worried about you ...” No. We don't do that.
What should not be said to a depressed person? You can't say: "Pull yourself together", "Don't worry", "Everything will be fine". You can't blame or blame. If accusations are made, people think they are bad and deserve it.
It is worth saying: “You have such a state when it seems that this will never pass. But this is not true. It's just a symptom of the disease. And it will pass”, “You deserve help”.
9. Depression is not laziness, and washing the floors will not help here
They say that a sign of depression is when a person stops keeping order and cleaning the house. Yesterday I had a patient who said that she washes the floors once a week and it worries her, she used to wash every day. How to distinguish depression from ordinary fatigue? A depressed person stops enjoying life. There are people who do not wash floors, but have fun with friends, enjoy reading. And if a person does not wash the floor, because everything is meaningless and nothing brings him pleasure, then he has depression.
There are people who do not wash floors, but have fun with friends, enjoy reading. And if a person does not wash the floor, because everything is meaningless and nothing brings him pleasure, then he has depression.
Adolescents are unusual patients. When depressed, they stop learning in the first place. They say, "I can't study." And parents often do not attach any importance to this: “Did you drop out of school? Yes, his company distracted. But this is a serious sign. It is imperative to talk with a teenager about this: “What does it mean that it’s hard for you to study? What, you don't remember? Can't concentrate? Did you read it and then forget it?
10. Talking about suicide is not dangerous, if a person talks about it - listen to him
There is a myth that talking about it with a person who has suicidal thoughts will make things worse. It is not true. You can't push suicide by talking about it.
We need to talk about it. In fact, many people have suicidal thoughts. Many of our patients fantasize about this as getting rid of their suffering and experiences, but a very small percentage of them commit some kind of suicidal act.
Many of our patients fantasize about this as getting rid of their suffering and experiences, but a very small percentage of them commit some kind of suicidal act.
Just talking to a person who has suicidal thoughts is not a push. It doesn't matter what words you use with the person. It is important that you do not judge or scold. You can say, "Wow - how bad you feel that you decided that you are not worth living."
But this is also a whole science – psychologists work in crisis conditions, as they dissuade. It is important not to criticize or devalue a person's experiences. Don't be afraid to talk about it.
How can I tell if I'm not depressed?
Flash mob #faceofdepression on Facebook caused a great response in Russia and encouraged many people to publish their stories, but it also scared everyone pretty much. It suddenly turned out that any photo of a happy person in social networks could be a selfie from a neurosis clinic.
Read about depression. I realized that the indisputable symptoms are when you can’t get out of bed and think about suicide. But this is a difficult stage, because something precedes this? No matter how much I read, it turns out that anything can be a sign of depression. Eat a lot - depression. Eat little - depression. Sleep a lot or sleep a little - the same thing. You work for days - from depression. If you can't work, it's definitely depression. Difficulty communicating with people is a sign of depression. Not a day without a party - depression. Help me! How do I know if I have depression or not?
Psychotherapist Anton Burno:
– Depression is not something you can skip. This is a distinct state. A person can usually tell exactly when he fell ill. It is worth paying attention to changes in the state, to the symptoms that have appeared. In most cases, a person has a feeling that something is wrong with him. In chronic depression, when episodes have occurred since childhood, it is sometimes difficult for a person to determine where is a healthy life and where is his depression, because depression is always present in some kind of veil.
- But there are people who, like the donkey Eeyore, have a reduced emotional background all their lives, how to understand - do they have depression or do they just live like that?
- Here we must ask the question - do they suffer from life or from their condition? If so, then it might be depression. This is the difference between depression, for example, from laziness. A person does not suffer from laziness, he just lives like that. And depression is always associated with dissatisfaction with one's condition. Depressive laziness is when you want to want. Such painful laziness is real suffering.
Source: http://www.pravmir.ru/da-vam-k-psihiatru-nado/
"Psychiatrists should treat depression": three signs of the disease and how to avoid it
April 7, 2017, 07:48
More than 300 million people in the world today are living with depression. Therefore, it is not surprising that the theme of World Health Day, which is celebrated on April 7, is depression.
According to the World Health Organization (WHO), depression is one of the leading causes of ill health and disability worldwide. In the 10 years from 2005 to 2015, the number of people with depression increased by more than 18%. "Due to a lack of support, many people with mental disorders do not seek the treatment they need to live healthy and productive lives," the organization said. The WHO is urging countries to increase investment in mental health, reminding that even in high-income countries, about 50% of people with depression do not receive treatment.
Meanwhile, most depressions are treated on an outpatient basis, if the patient turns to a psychiatrist for help in time. This was told to TASS by the chief freelance specialist of the Ministry of Health of the Russian Federation in psychiatry, director of the State Scientific Institute of Forensic and Social Psychiatry. V.P. Serbian Zurab Kekelidze. “Of course, there are chronic, resistant severe conditions when serious measures must be taken,” the expert added.
From 3.7% of the population to 6.5% in different countries - the percentage of people diagnosed with depression. Russia is in the middle of this list - we have about 5.5%
Kekelidze notes that, according to statistics, there are more women diagnosed with depression. However, this may be partly due not to a predisposition to depression, but to the fact that women are more attentive to their health. “They notice deviations faster, see a doctor more often and are more attentively treated,” he said.
Three signs of depression
See also0002 The chief specialist of the Ministry of Health of the Russian Federation in psychiatry notes that a bad mood is not only from real external causes, but also from a disease called "depression".
"Three main signs are standardly distinguished: a feeling of low mood, motor (motor) retardation, idiotic retardation (when a person feels that it has become harder for him to think, to choose words more slowly, a feeling that he is not thinking about anything)," Kekelidze explained .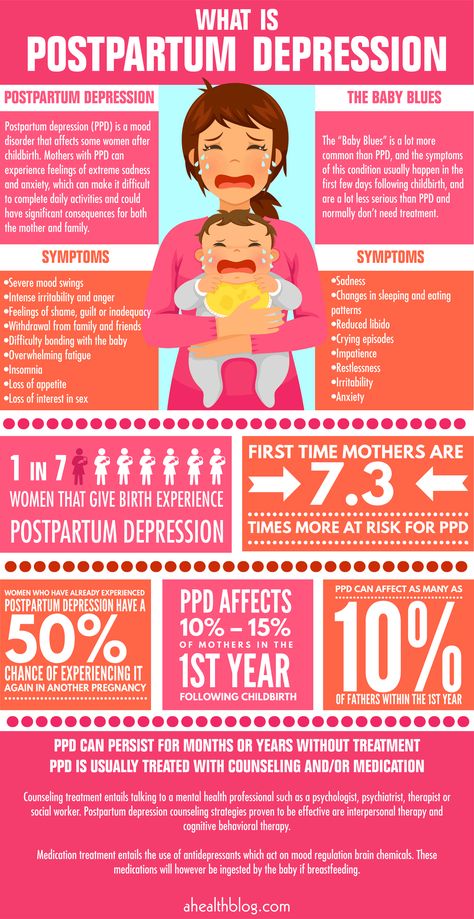
In addition to the main signs of depression, there are many varieties: masked (mild depression), seasonal, postpartum, depression that accompanies other somatic conditions - Alzheimer's disease, hypothyroidism and many others.
The psychiatrist advises parents to take a closer look at changes in the child's behavior: sleep disturbances, changes in appetite (stopped eating or eats a lot of sweets) can be early signs of depression.
What prevents Russians from treating depression
In Russia, according to Kekelidze, the problem that not all people with depression receive the necessary treatment is due to the lack of habit of taking care of their health preventively, as well as the fact that people in Russia still For the time being, they are afraid of neuropsychiatric dispensaries, where they try not to go unless absolutely necessary. Not the last role is played by the stigmatization of mental illness - hence the fear of turning to a psychiatrist for help.
However, according to the expert, one should not hope that depression will go away on its own. It is a disease, and like any disease, it must be dealt with by a medical specialist.
Depression should be treated by psychiatrists or psychotherapists. But most people do not go to doctors, they are afraid that they will register
The psychiatrist noted that not every patient needs to be registered with a dispensary, and there are a number of criteria for this. The basis is a danger to oneself and others.
According to the expert, depression is characterized by lack of will, so the worst thing you can advise a depressed person is to tell him "get it together", "pull yourself together." A professional psychiatrist or psychotherapist should say this to the patient, because otherwise the feeling of guilt for "not being able to pull himself together" will grow.
The Rule of Three Eights
Read also
Vital necessity: what you might not know about dreams
- to work, eight - to rest.