Counselling for child behaviour
Therapy to Improve Children’s Mental Health
Mental, emotional, and behavioral disorders in childhood can cause long-term problems that may affect the health and well-being of children, families, and communities. Treating a child’s mental health problems as soon as possible can help children reduce problems at home, in school, and in forming friendships. It can also help with healthy development into adulthood.
A public health approach to children’s mental health includes promoting mental health for all children, providing preventive intervention to children at risk, and providing treatment for children with identified disorders. Psychological therapy is a key component to improving mental health. Depending on the type and severity of the problems, psychological therapy for children may be used in combination with medication. 1
New, easy-to-use, interactive web tools for children and teens to deal with thoughts and feelings in a healthy way.
A brief overview of therapy
Psychological therapy is meant to treat a mental health condition or help a child manage their symptoms so that they can function well at home, in school, and in their community.
When children are young, it is common for therapy to include the parent. Sometimes therapists work with the parents alone. Older children may meet with a therapist alone as well. Some types of therapy include working with the whole family or other important adults in the child’s life (for example, a teacher).
Parent-focused approaches typically mean that parents talk with the therapist about the child’s behavior and feelings. Psychological therapy with children can include talking, playing, or other activities to help the child express feelings and thoughts. Therapists may also observe parents and children together and then make suggestions for finding different ways to react.
Psychological therapy for children can be done one-on-one or in groups. Sometimes, a combination of therapies is the most effective for helping a child.
What types of therapy are most effective for mental disorders in children?
Behavior therapy teaches children and their families how to strengthen positive child behaviors and eliminate or reduce unwanted or problem behaviors.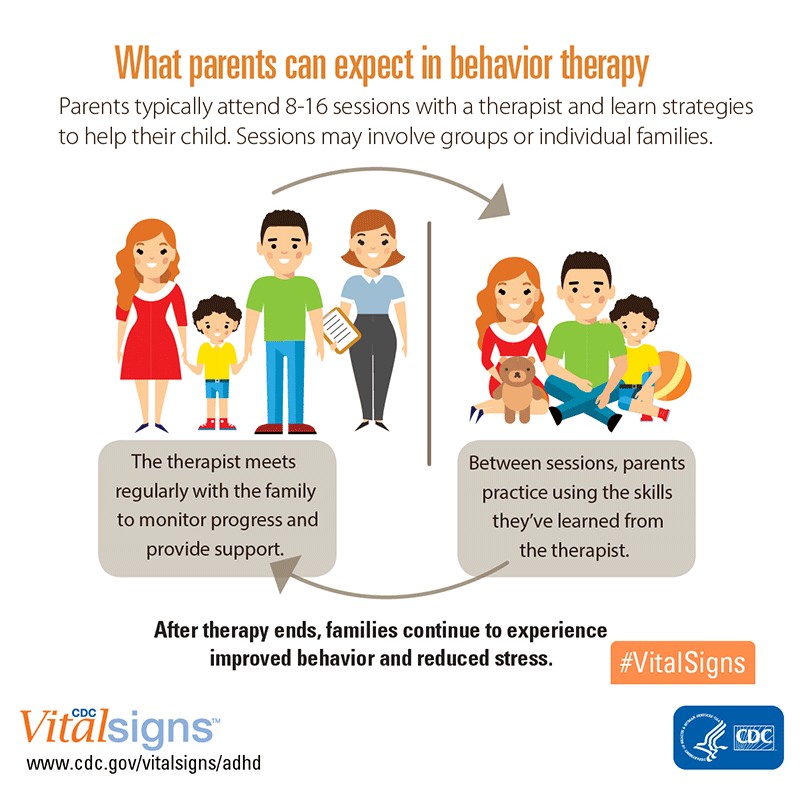
One type is parent training in behavior management. The therapist works with parents to learn or improve skills to manage their child’s behavior. Parents are encouraged to practice the skills with their child, either during the therapy session or at home. Teachers can also be trained in behavior management to help the child at their childcare center or school.
With older children or adolescents, the therapist usually works directly with the child to teach them how to choose positive behaviors. Parents can be involved to support and strengthen the skills their child is learning.
Cognitive-behavior therapy focuses on changing the thoughts and emotions that can affect a child’s behavior negatively.
The therapist helps the child become aware of their thoughts and feelings. The therapist also helps the child evaluate if feelings or thoughts may be distorted or illogical, and then helps the child through the process of changing the thoughts as well as the emotional reactions and behaviors that go along with them.
Cognitive-behavior therapy often works directly with the child, but can also include parents.
For the most common childhood conditions, like ADHD, behavior disorders, anxiety, or depression, approaches using behavior therapy and cognitive-behavior therapy are more likely to reduce symptoms, but there is limited information about which type of therapy is best for treating each specific childhood mental disorder.
Based on the scientific evidence available, different therapies seem to work well for different types of problems:
Parent training in behavior management works well for
- ADHD; and
- Disruptive behavior disorders.
Child behavior therapy works well for
- ADHD; and
- Disruptive behavior disorders.
Cognitive-behavior therapy works well for
- Disruptive behavior disorder;
- Depression;
- Anxiety; and
- PTSD.
Additional types of therapy can be effective for adolescents.
- Adolescents with disruptive behavior disorder may respond well to family therapy, an approach that includes multiple members of the family and focuses on learning better communication skills and ways to settle conflicts.
- Adolescents with depression may respond well to interpersonal psychotherapy, an approach in which the therapists help the adolescents learn ways to handle relationship problems.
Other therapy approaches may also be effective but have not been studied enough for researchers to understand if they work well. Information on what works best for which family is also still limited. Read more about which types of child therapy have been found to work.external icon
Finding the right therapy for your child
Therapy is most effective if it fits the needs of the specific child and family. You can talk to your child’s healthcare provider as a first step. Sometimes, health problems such as poor sleep, trouble breathing, poor vision, difficulty hearing, or learning problems can cause behavioral or emotional symptoms, or make them worse. Your child’s healthcare provider may want to find out if your child has any health problems before referring your child for therapy.
Your child’s healthcare provider may want to find out if your child has any health problems before referring your child for therapy.
Before starting therapy, a mental health provider typically conducts a comprehensive evaluationexternal icon of your child’s mental health to figure out what type of therapy might work best.
Here are some tools to help find a healthcare provider familiar with treatment options:
- American Psychological Association Psychologist Locatorexternal icon,
- American Association of Marriage and Family Therapy Locatorexternal icon
- American Board of Professional Psychology Locatorexternal icon
- Child and Adolescent Psychiatrist Finderexternal icon, a research tool by the American Academy of Child and Adolescent Psychiatry (AACAP).
- Find a Cognitive Behavioral Therapistexternal icon – A search tool by the Association for Behavioral and Cognitive Therapies
- Hospital and University Related ADHD Centersexternal icon
- MentalHealth.
 govexternal icon – Information on mental health services and resources
govexternal icon – Information on mental health services and resources - National Association of Social Workersexternal icon
- SAHMSA’s Behavioral Health Treatment Services Locatorexternal icon
Information about Medication
1 Read about medications used to treat children and adolescents
- FDA: Information on suicidality in children and adolescents treated with anti-depressant medication external icon
- FDA: Information on ADHD medicationsexternal icon.
References
- Evans, S., Owens, J., & Bunford, N. Evidence-based psychosocial treatments for children and adolescents with attention-deficit/hyperactivity disorder. Journal of Clinical Child & Adolescent Psychology, 43(4):527-51.
- Higa-McMillan, C.K., Francis, S. E., Rith-Najarian, L., & Chopita B. F. (2016). Evidence base update: 50 years of research on treatment for child and adolescent anxiety, Journal of Clinical Child & Adolescent Psychology, 45:2, 91-113.
- Kaminski, J. & Claussen, A. (2017). Evidence base update for psychosocial treatments for disruptive behaviors in children. Journal of Clinical Child & Adolescent Psychology. 1-23.
- McCart, M. R., & Sheidow, A. J. (2016). Evidence-based psychosocial treatments for adolescents with disruptive behavior. Journal of Clinical Child & Adolescent Psychology, 45, 529-563.
- Spence, S. H., O’Shea, G., & Donovan, C. L. (2016). Improvements in interpersonal functioning following interpersonal psychotherapy (IPT) with adolescents and their association with change in depression. Behavioural and Cognitive Psychotherapy, 44(3), 257-272.
- Weersing, V.R., Jeffreys, M. Do, M.T. Schwartz, K.T.G., & Bolano, C. (2016). Evidence base update of psychosocial treatments for child and adolescent depression. Journal of Clinical Child and Adolescent Psychology, 46(1):11-43.
Behavioral Therapy for Young Children
The American Academy of Pediatrics recommends that young children (ages 2 to 5) with ADHD receive behavior therapy for treatment first before trying medication. Behavior therapy for young children is most effective when their parents learn strategies from therapists and use those strategies to manage their children’s behavior. Parents learn to create structure, reinforce good behavior, discourage negative behaviors, provide consistent discipline, and strengthen the relationship with their child through positive communication. These techniques not only help children with ADHD but also children without a diagnosis to function successfully at home and at school.
Behavior therapy for young children is most effective when their parents learn strategies from therapists and use those strategies to manage their children’s behavior. Parents learn to create structure, reinforce good behavior, discourage negative behaviors, provide consistent discipline, and strengthen the relationship with their child through positive communication. These techniques not only help children with ADHD but also children without a diagnosis to function successfully at home and at school.
A recent study by researchers at the Centers for Disease Control and Prevention (CDC) reports that despite these guidelines, only one in two young children diagnosed with ADHD are receiving psychological services, which may include behavior therapy.
How does behavior therapy help me and my child?
The inattention and impulsivity associated with ADHD can contribute to negative interactions and behaviors in children. They may tend to misbehave and be punished more frequently than other children. This frequent punishment can have a negative effect on their self-image and cause problem behaviors to increase. Parents may find that their typical parenting strategies do not work very well. Parents can learn to manage the behavior of young children who have ADHD by receiving training in the use of behavioral techniques and work with caregivers (daycare providers, preschool teachers, and others) to help reduce these negative behaviors and interactions.
This frequent punishment can have a negative effect on their self-image and cause problem behaviors to increase. Parents may find that their typical parenting strategies do not work very well. Parents can learn to manage the behavior of young children who have ADHD by receiving training in the use of behavioral techniques and work with caregivers (daycare providers, preschool teachers, and others) to help reduce these negative behaviors and interactions.
What does behavior therapy look like?
Parenting children with ADHD presents unique challenges. Children develop differently, and ADHD may present differently in each child. A professional can help parents determine when and what types of responses are appropriate for their child. It can be very difficult for parents to learn these parenting strategies just from books and websites and to implement them on their own. Parents can learn specific skills and strategies that are most effective with their children who have ADHD. The training includes practice and therapist support in applying these techniques effectively and consistently. Help from a professional can be very helpful.
The training includes practice and therapist support in applying these techniques effectively and consistently. Help from a professional can be very helpful.
Therapy for ADHD generally includes teaching parents the following skills:
- Establishing house rules, structure, and consistent routines
- Learning to provide specific praise and attention for appropriate behaviors (praising good behavior often) and not providing attention for mild, annoying but not harmful behaviors (choosing your battles)
- Using developmentally appropriate directions and commands
- Planning ahead and working with children in public places
- Using consistent and effective disciplinary strategies
For parents of young children, the training will need to be particularly sensitive to the child’s developmental level. Preschool-age children change more rapidly than older children. They are more likely to engage in tantrums and other oppositional behavior that can be normal for this developmental period. However, children with ADHD are likely to perform these behaviors with greater frequency and intensity. Again, a professional will help parents to determine at what point a behavior requires intervention and which strategies work best with each child.
However, children with ADHD are likely to perform these behaviors with greater frequency and intensity. Again, a professional will help parents to determine at what point a behavior requires intervention and which strategies work best with each child.
Unlike older children who generally have had various social experiences and have acquired many social behaviors, learning how to get along with other children in pairs and groups is just emerging for young children. Because group situations can be challenging for young children with ADHD, behavioral parent training will help parents learn how to foster these skills. Behavioral parent training typically runs for 8–12 sessions. However, some families may require more sessions.
The therapist will train parents to consistently use effective communication and other strategies to manage their children’s behavior and strengthen their relationship with their child. Between sessions, parents use and practice what they have learned and return to the next session to discuss progress, adjust strategies as needed, and learn new skills.
Applying these skills with children with ADHD takes work on the part of parents. However, the hard work pays off. Parents who master and consistently apply these skills will see fewer behavior problems and better family functioning. Their child will have improved self-esteem and better relationships with parents, siblings, teachers, and others.
What parent management training programs are out there for parents of preschoolers?
The following parent behavioral training programs for parents of preschool-aged children that currently have enough research evidence to be described as effective:
- Helping the Noncompliant Child
- Incredible Years Parenting Program
- New Forest Parenting Programme
- Parent-Child Interaction Therapy
- Triple P (Positive Parenting Program)
According to a 2011 review by the Agency for Healthcare Research and Quality (AHRQ), behavioral parent training programs taught by trained therapists can “help parents manage their child’s problem behavior with more effective discipline strategies using rewards and nonpunitive consequences. An important aspect of each is to promote a positive and caring relationship between parents and their child.” The AHRQ review found the following common therapeutic components across the effective programs:
An important aspect of each is to promote a positive and caring relationship between parents and their child.” The AHRQ review found the following common therapeutic components across the effective programs:
- help parents develop a positive relationship with their child
- help them manage negative behavior and increase positive behavior with positive discipline
For parents who do not have access to the specific programs mentioned above, seeing a therapist who focuses on the same elements may be helpful.
Parents and caregivers who wish to learn more about ADHD and ways to help their child may wish to enroll in Parent to Parent: Family Training on ADHD offered through CHADD.
References
Centers for Disease Control and Prevention, http://www.cdc.gov/ncbddd/adhd/treatment.html, accessed 03/16/2016.
Centers for Disease Control and Prevention, Vital Signs: ADHD in Young Children, http://www.cdc.gov/vitalsigns/adhd/, accessed 05/04/2016.
Charach A, Dashti B, Carson P, et al. Attention Deficit Hyperactivity Disorder: Effectiveness of Treatment in At-Risk Preschoolers; Long-Term Effectiveness in All Ages; and Variability in Prevalence, Diagnosis, and Treatment . Comparative Effectiveness Review No. 44. AHRQ Publication No. 12-EHC003-EF. Rockville, MD. Agency for Healthcare Research and Quality. October 2011.
Zwi, M, Jones, H, Thorgaard, C, York, A, Dennis, J. (2011). Parent Training Interventions for Attention Deficit Hyperactivity Disorder (ADHD) in Children Aged 5 to 18 Years. Campbell Systematic Reviews.
Algorithms for counseling families and children with special needs
The life situation of a child with special needs family is obviously much more traumatic than the situation of the life of an "ordinary" child and his family - primarily due to "enrichment" of the spectrum of social, medical and psychological problems associated with social rejection, inattention, fear and rejection. Therefore, the child's disability is one of the reasons for his maladaptation. and deviance, as well as the cause of many problems psychological and social plan of his parents. Among disabled children there are many who, running away from widespread disability (“racism” in society) for disabled people and their relatives) and disability strategies (reinforcing the feeling of a person with OH himself "as inferior"), hits extremes of diverse psychological and social deviations. Many run away social control and society as such - many different ways. Consultative work with such people – a chance to bring them back into public life. When the child lives in a family or constantly communicates with parents, establishing the fact of the disease child, is a situation of psychological shock for parents. Implementation own plans becomes problematic, the prospects for the fate of the child. Parents themselves, as a rule, are not ready for such test. As a rule, these are disadvantaged families that are most in need of the help of specialists.
Therefore, the child's disability is one of the reasons for his maladaptation. and deviance, as well as the cause of many problems psychological and social plan of his parents. Among disabled children there are many who, running away from widespread disability (“racism” in society) for disabled people and their relatives) and disability strategies (reinforcing the feeling of a person with OH himself "as inferior"), hits extremes of diverse psychological and social deviations. Many run away social control and society as such - many different ways. Consultative work with such people – a chance to bring them back into public life. When the child lives in a family or constantly communicates with parents, establishing the fact of the disease child, is a situation of psychological shock for parents. Implementation own plans becomes problematic, the prospects for the fate of the child. Parents themselves, as a rule, are not ready for such test. As a rule, these are disadvantaged families that are most in need of the help of specialists. To organize the highest quality work process with such families need close interaction of specialists working with disabled children and families. Parents should be aware of the rehabilitation potential of the child, expected results and all types of rehabilitation measures necessary for the child. It contributes involvement of parents in the rehabilitation of their child. family, from the first meeting with her, one should prepare for cooperation with a doctor, psychologist, teacher, social worker, to the conscientious fulfillment of all assigned these task specialists. It is important to convince parents that all prescribed rehabilitation measures throughout the cycle rehabilitation. Many parents, no less than a child, need help and support. specialists.
To organize the highest quality work process with such families need close interaction of specialists working with disabled children and families. Parents should be aware of the rehabilitation potential of the child, expected results and all types of rehabilitation measures necessary for the child. It contributes involvement of parents in the rehabilitation of their child. family, from the first meeting with her, one should prepare for cooperation with a doctor, psychologist, teacher, social worker, to the conscientious fulfillment of all assigned these task specialists. It is important to convince parents that all prescribed rehabilitation measures throughout the cycle rehabilitation. Many parents, no less than a child, need help and support. specialists.
Impairment of physical or mental development, like any other functional change of the body, aging or disease, not limited within the framework of a purely medical phenomenon. Its impact on family, environment or the individual himself is determined by the meaning given to him by society and culture. Disability is a process in which violations physique, bodily functions or environmental conditions make human activity or the functioning of its organs is difficult or impossible. The reason for the limited capacity may be unsuitability of the environment for the socialization of certain groups people, for example, the lack or imperfection of educational programs, medical and social services needed by children with an atypical condition health.
Disability is a process in which violations physique, bodily functions or environmental conditions make human activity or the functioning of its organs is difficult or impossible. The reason for the limited capacity may be unsuitability of the environment for the socialization of certain groups people, for example, the lack or imperfection of educational programs, medical and social services needed by children with an atypical condition health.
Counseling parents with a child with OD and themselves child with ON is based on the following principles: 1) the need, including critical periods and as part of support, 2) compulsion - social order, 3) complexity, 4) permanent nature, including periodic consultations, etc., 5) the interaction of subsystems of the work of a psychologist with a child, with parents and other specialists of the CSO, boarding school.
There are important differences in counseling a family with child with special needs from current systems counseling. First, within the framework of family or age-psychological counseling is assumed to be completely voluntary access to a specialist. This means sufficient motivation, emotional readiness for a meeting, the desire to state everything that seems important. When counseling a child with suspicion of deviant development, the family is “forced” to counseling by any specialist (or society) who suspected a developmental disorder in child - that is, in the direction (or, which is milder, - "advice").
First, within the framework of family or age-psychological counseling is assumed to be completely voluntary access to a specialist. This means sufficient motivation, emotional readiness for a meeting, the desire to state everything that seems important. When counseling a child with suspicion of deviant development, the family is “forced” to counseling by any specialist (or society) who suspected a developmental disorder in child - that is, in the direction (or, which is milder, - "advice").
Secondly, standard counseling involves the opportunity for the family to stop communicating with the specialist at any time. The practice of counseling children with special needs shows that in In some cases, the family does not follow through with counseling or, dissatisfied with the results of the examination, begins to look for another, “more convenient” specialist who, after a second examination, would give more favorable information that meets the present needs and condition parents. This behavior of the family is called "walking in a circle doctors." Based on the principle of respecting the interests of the child, it is necessary to “keep” parents from premature termination of counseling, give the possibility of carrying out psycho-correctional work in full, to minimize the number of visits to other institutions and specialists in order to "remove" or mitigate the diagnosis, to achieve an adequate awareness of the problem by parents and making the right decisions on the upbringing and teaching a child with OH.
This behavior of the family is called "walking in a circle doctors." Based on the principle of respecting the interests of the child, it is necessary to “keep” parents from premature termination of counseling, give the possibility of carrying out psycho-correctional work in full, to minimize the number of visits to other institutions and specialists in order to "remove" or mitigate the diagnosis, to achieve an adequate awareness of the problem by parents and making the right decisions on the upbringing and teaching a child with OH.
Typical problems and referrals of parents of children with OD corrections:
-
passive attitude towards life and illness of a child - it suggests the need for activation - through understanding the successes families and broadcasting the successes of parents from other families occupying an active position, detection and study of the “losses” of the child and parents from their passivity.
-
negative attitude to life, including depressive attitudes and states - reformulation (positive rethinking),
-
positive - "rental" attitude to the life and illness of the child - assistance is required to the family in the direction of finding "dummy targets", their overthrow and replacement by "real" goals,
-
protective behavior, including - ignoring the disease - requires the consultant to help the family in the direction of dispelling illusions "normality" and "health" of the child, as opposed to the need for constant concerns about its development, state as active and complex.
 permanent actions and efforts,
permanent actions and efforts, -
"ashamed" behavior - suggests in working with clients discovery of the "universality" of restrictions in people's lives, analysis of the process stigmatization, "environmental correction" is possible - for example, temporary stay in village, visiting a boarding school for disabled children, etc., analysis of disability as "racism" against children and their families,
-
overprotective parents - assistance to them includes joint search for the causes of overprotection - the fear of parents for the life of the child and the fear of being unloving and not accepting, hidden tendencies to suppress and "destroy" ("detocid") of the child, debunking insincerity and building more sincere patterns of behavior,
-
chronic fatigue syndrome - involves assistance in developing a positive self-attitude and accepting the situation as a “life challenge”, an existential task, it is necessary to support a sense of pride for your "home" or "disabled" work, the development of relationships a married couple in order to strengthen their internal resources, improve bodily forms of mutual support of spouses and children,
-
understanding of the child's illness as a "punishment", a sense of guilt - it is necessary to develop parents' ideas about their guilt in the direction search for irrational prejudices, psychogenetic analysis is possible, "goal-oriented" transformation of problem situations, their value comprehension,
-
hypochondriacal reactions - narcissistic, hysterical or mixed types - require assistance in correcting the "image I" and "image of the child" in parents are productive complex - including – body-oriented methods of assistance, identification of “incompatible symptoms” and “behaviors”, etc.

-
problems of partial acceptance of the child and feelings of guilt - productive analysis of the impossibility of full acceptance and usefulness, the role rejection in the positive development of the child, analysis of possible schemes of manipulation child by parents who support and exploit their sense of guilt, discovery and development of more productive patterns of interpersonal interaction in family.
-
parental support for formation and development secondary defects in the development of the child - counseling is necessary the possibilities of correction and "compensation" of one or another primary defect, teaching exercises to help overcome problems associated with isolation child, etc.
-
problems of parents of autistic children who are closed in their experiences on oneself - parents need help in revealing their feelings and experiences,
-
child-centrism - overcoming it is connected with solving the problem reorientation of parents to their own lives, disclosure of unused opportunities and their importance.

-
Parent(s) "offline" problems, e.g. couples that existed before the child, his disability - common approaches are productive plus an analysis of the "developing possibilities" of children's presence, perhaps - identification of the "unconscious" relationship between parents and the child the intensity of the problems of the spouses and the illness of the child.
Typical positions of clients in counseling and their conversion:
-
passive - requires activation, translation responsibility and demonstration of the success of active families and children with ON,
-
"squeezed" - fear of counseling and fear changes in general - it is necessary to show the family the role of changes, discuss the phenomenon of "snowball", "double effect of self-disclosure", etc.
-
dependent - requires activity translation, existence alternative approaches, the importance of finding them,
-
productive - active - need help finding information and identification of attitudes, behaviors and etc.
 ,
, -
rental - it is important to ask the parent the question of whether what gives him today's behavior, whether it is necessary to preserve, strengthen, that he will lose if they stop pitying him, etc., which will bring him more productive ways to solve your problems and the child,
-
negative ("testing") - the consultant demonstrates unwillingness of the client to work, this is a test of professionalism counselor: frontal questions about whether the client wants to continue counseling and whether it should be stopped because the client does not show due interest and disclosure.
Problems of parents in an accompaniment situation form several typical groups, for example:
-
problems of a married couple, including their existence, differences in the perception of the child and his illness - for this couple it is necessary help in finding a common - more constructive - loving - strategy for the organization relationships with the world and with each other,
-
problems of interaction between a child and parents - whims and rejection, inadequate forms of compensation for illness, etc.
 – necessary assistance to clients in changing interaction systems, love and "training" in relationships with people,
– necessary assistance to clients in changing interaction systems, love and "training" in relationships with people, -
child's interaction with the world of other children and adults - "targeted" work is often needed in the direction prevention of dysmorphophobia, hypochondria, disability, etc.
Conflict situations in different situations counseling:
-
do not occur if observed: compliance with ethical principles, principles of primary and secondary contract, open discussion interactions between the client and the consultant, their compliance with the contract, professional and personal maturity of the consultant, readiness of the client to counseling,
-
occur if: "combustion consultant", the imposition of the problems of the client and the consultant, interaction of personal "immaturities", etc.
-
conflict correction acts as: situation for disclosure, the situation of debunking the illusion of understanding - for mutual understanding, turning point, study of the situation, extinguishing the "imaginary conflict" discovery and opposition of positions, change of consultant.

Guidelines for the client consultation process this group are based on well-known principles existential-humanistic psychotherapy: acceptance, empathy, congruence, specificity, unusualness, plasticity of behavior and upholding values. In addition, in working with these clients it is important to be able to "ground" these principles in the practice of direct communication: systemic deviations in the development of the personality and its relations in a situation "ON" requires the consultant to be able to "technologize" and “operationalize” your love and acceptance of clients as people by helping they will learn the same acceptance and love, not only at the level of "simple relationship", but also at the level of direct behavior, in everyday vital activity.
Psychological support is provided in the process of communication with the child with the family, her life. This before in total, counseling of preventive-informative and psychotherapeutic nature associated with the disclosure of general trends development of the abnormal child, his relations with the world and family relationships.
📖 Correction of the position of the parent in relation to the child, 4. CONSULTATION OF PARENTS ON DIFFICULTIES IN RELATIONSHIPS WITH ADULTS. Individual and family psychological counseling. Aleshina Yu. E. Page 7. Read online
One of the most common problems encountered in counseling work is parents' complaints about difficulties in relationships with their adult children. Usually mothers come with such complaints, but it happens that both parents or even one father. At the same time, they usually want to keep the fact of their request for help a secret from their children. This means that from the very beginning of the conversation, the psychologist should be focused on resolving the conflict “by the forces of those present”, without attracting additional information, without being able to look at this situation through the eyes of the “accused” - children. Since this manual deals only with the problems of adult counseling and does not intend to take into account any features of child psychology, here we will analyze the difficulties in the relationship of parents with children over 15-16 years old, i. e. already largely overcome the difficulties of adolescence.
e. already largely overcome the difficulties of adolescence.
Very conditionally parents' complaints about children can be divided into four groups (of course, they are not mutually exclusive, but most often accompany each other).
1. Lack of contact with children: lack of understanding of how they live, what they are interested in, the inability to talk heart to heart with them, the feeling of parental uselessness, alienation to the child, etc. Clients with such problems are characterized by statements like: “I don’t understand him (her) at all” or “I don’t know anything about her, where she goes, who her friends are” or “He doesn’t tell me anything about himself, doesn’t trust” and etc.
2. Disrespectful, harsh attitude of children towards their parents, constant quarrels and conflicts with them over trifles. Such complaints are characterized by statements like: “He is constantly rude to me”, or “He absolutely does not consider me”, “He (she) does not want to do anything around the house, does not help in anything. ”
”
3. Anxiety for children, caused by the fact that they do not live the way they should, from the point of view of their parents. Often at the same time, parents perceive their children as unhappy, unlucky, confused, lonely, etc., which is the reason for seeking advice. Complaints are usually formulated like this: “My daughter has a very bad relationship with her husband, I would really like to help her improve family relationships, but I don’t know how to do it” or “My son dropped out of college, where he studied for four years” or “My daughter is nineteen years, and she has already had two abortions.”
4. Problems associated with non-standard, deviant behavior of children: “My daughter uses drugs, how can I help her quit?”, “My son is a member of a gang engaged in profiteering and theft, what should I do?”
Naturally, whatever the client's complaint, the first task of the consultant is to understand the essence of the problem, to understand how the parent's claims and assessments correspond to reality, to make his own diagnosis of the problem. The most obvious way to do this is to collect concrete facts. Most often, the parent who comes to the appointment is a talkative client who readily, without leading questions, tells his story. And yet, in order to obtain information about specific situations, the consultant has to specifically ask questions about exactly how the interaction between the child and the parent unfolds, what they say to each other, why and how quarrels break out, what exactly serves as a basis for concern and suspicion. Important points in making an accurate psychological diagnosis, which allows to put forward and formulate further hypotheses, are:
The most obvious way to do this is to collect concrete facts. Most often, the parent who comes to the appointment is a talkative client who readily, without leading questions, tells his story. And yet, in order to obtain information about specific situations, the consultant has to specifically ask questions about exactly how the interaction between the child and the parent unfolds, what they say to each other, why and how quarrels break out, what exactly serves as a basis for concern and suspicion. Important points in making an accurate psychological diagnosis, which allows to put forward and formulate further hypotheses, are:
a) finding out how serious the cause of the parent's concern about the child is, in other words, whether the child is “normal”, i.e. whether his difficulties, oddities or peculiarities of behavior are manifestations of independence, independence, ideas about life that are different from those of his parents, or are there really some features in his behavior, statements and reactions that indicate any mental and social deviations;
b) understanding what the parent's position really is in relation to the child, what underlies the coming to the consultation - their own problems or concern for their son (daughter), the desire to help him (her) or the desire to get help and support for themselves and get rid of from their own fears, feelings of guilt, uselessness, etc.
Often there are situations when both are true, especially since trouble, self-doubt, inadequacy of the position of the parent himself are always grounds for a child to also have difficulties and problems in life. But since the real client who applied for advice is still a parent, the main attention of the consultant should always be directed to helping him understand his own fears and problems, to understand how appropriate and appropriate worries for the child are.
Correction of the position of the parent in relation to the child child, the desire to guide, advise, recommend without understanding the true needs of the child.In this case, the child's behavior that underlies complaints - inattention, harshness, secrecy, there are ways to fight for their own independence, attempts to avoid overprotectiveness.Such overprotective parents tend to either not notice dominance of one’s own behavior, or perceive it as something normal and natural: “I only want the best for him”, “I know better how to act in such situations.
 ”
” The inadequacy of the client, his uncritical attitude to his own behavior requires the psychologist to be especially careful during the conversation. Feedback, evaluation of human behavior can be given only after a sufficient number of facts have been accumulated to support such an interpretation. When working with an overprotective parent, it can be especially helpful to find out the requirements that he (she/they) make to the child in general (i.e. how he (she) would like his son (daughter) to be, as well as when and how these requirements are presented what and for what reason the parent most often says to the child).
Usually, in a situation of overprotection, a parent has demands that are made almost daily, and these, as a rule, underlie the conflicts and quarrels that flare up, one has only to sound these “magic” words. Such requirements can be associated both with some social tasks facing adult children (“When will you start preparing for college?”, “All your classmates have long defended their dissertations”), and with everyday household situations (“Stop pampering a child !”, “Don’t talk on the phone for a long time!”, “Why are you always late everywhere”, “Wash the dishes immediately!”).
Often, during a detailed conversation with parents about the demands that they place on their children, a feeling of bewilderment arises: to whom are they addressed, in other words, how old is the child? They often sound as if the conversation is about a 10-11-year-old child (although you should not abuse such formulations in relation to a child of this age). But here we are talking about children, most often long gone from this age! This, in itself, testifies to the inadequacy of the position of the parents. An even greater inconsistency with the reality of the parental position can manifest itself if the client is asked: “What is the purpose of what you are saying all this to him?” Most often in such cases, the counselor will hear in response: "I'm trying to teach or get him (her) to do what is necessary" or "I remind him, otherwise he will forget to do it."
Such answers hide: a) the idea of their role as a teacher, the only one who knows and understands what, when and how to do, and, accordingly, does not allow any other options or assessments; b) confidence in the necessity and reality of achieving the goals - to educate, force, explain, convince, etc. ; c) a low assessment of the capabilities and abilities of the child himself, distrust of him, since such behavior of the parent means his conviction that the child himself will never be able to do anything worthwhile. The task of the consultant in such a situation is to destroy or question the expediency of the overprotective position in relation to the son (daughter), and also, if possible, to replace it with a different attitude and vision of what is happening.
; c) a low assessment of the capabilities and abilities of the child himself, distrust of him, since such behavior of the parent means his conviction that the child himself will never be able to do anything worthwhile. The task of the consultant in such a situation is to destroy or question the expediency of the overprotective position in relation to the son (daughter), and also, if possible, to replace it with a different attitude and vision of what is happening.
But before that, one more very important step needs to be taken: to link the characteristics of the parent's behavior (overprotectiveness) and the behavior of the child (secrecy, coldness, harshness, disrespectful attitude).
Often during the course of the conversation, the counselor can clearly point out to the client the connection between the parent's statements and the child's response. This can be done in situations where it follows from the client's story that after the presentation of parental demands in one form or another, an aggressive or devaluing father (mother) reaction from the son (daughter) clearly follows. Another equally important source of information is the assessment of the parent by the child, given by the parent himself. In order to obtain such information, it is enough to ask the question: “How does your son (daughter) perceive your behavior, what do they say about you?” Don't settle for answers like "Nothing" or "I don't know." Having shown some perseverance (“Well, what does he (she) say to you when you quarrel?”), You can get very valuable information for further work like: “He (she) starts screaming at me: why are you pestering me all the time?”, “Tired”, “Bore!”, “You don’t understand anything!” That is, the child does not just not like what and when the parent says, but parental statements are directly rejected, evaluated and perceived very negatively.
Another equally important source of information is the assessment of the parent by the child, given by the parent himself. In order to obtain such information, it is enough to ask the question: “How does your son (daughter) perceive your behavior, what do they say about you?” Don't settle for answers like "Nothing" or "I don't know." Having shown some perseverance (“Well, what does he (she) say to you when you quarrel?”), You can get very valuable information for further work like: “He (she) starts screaming at me: why are you pestering me all the time?”, “Tired”, “Bore!”, “You don’t understand anything!” That is, the child does not just not like what and when the parent says, but parental statements are directly rejected, evaluated and perceived very negatively.
Another source of information, the use of which can greatly help to uncover the mechanisms underlying overprotection, is an analysis of why the parent sought psychological help right now, why relationship problems have become especially acute, what has changed in the relationship with the child, in a situation or in the parent itself recently this way. It happens that the aggravation of relations is simply the natural process of the child growing up and leaving him out of parental control, but most often this is facilitated by a sharp change in the situation either in the child’s life (the child returned from the army, got married, went to college, and as a result, the possibilities of control decreased ), or in the life of a parent (the client retired, divorced, and as a result, the need for overprotection, and sometimes the opportunities increased). It is also possible that the child himself has changed: he began to study worse than before, became interested in something that does not suit the parent, he had secrets and, thus, he began to slip out of parental care and control. Finding a moment of aggravation in a relationship and analyzing why and how it happens, from the client's point of view, can be excellent material for a parent to understand their overprotective position. As an illustrative example, we will give a specific situation of treatment.
It happens that the aggravation of relations is simply the natural process of the child growing up and leaving him out of parental control, but most often this is facilitated by a sharp change in the situation either in the child’s life (the child returned from the army, got married, went to college, and as a result, the possibilities of control decreased ), or in the life of a parent (the client retired, divorced, and as a result, the need for overprotection, and sometimes the opportunities increased). It is also possible that the child himself has changed: he began to study worse than before, became interested in something that does not suit the parent, he had secrets and, thus, he began to slip out of parental care and control. Finding a moment of aggravation in a relationship and analyzing why and how it happens, from the client's point of view, can be excellent material for a parent to understand their overprotective position. As an illustrative example, we will give a specific situation of treatment.
A mother came to counseling with a complaint that her daughter avoids talking to her, is rude, returns late, and refuses to do what she is asked to do. From the point of view of the mother, before the daughter has always been a very obedient and successful girl, but recently something has happened to her. The client also says that this summer her daughter did not go to college, although she studied well at school. Her parents arranged for her to work as a laboratory assistant at a research institute with friends, and although they do not complain about her at work, her relationship with her family has deteriorated sharply.
As a result of a more detailed questioning of the client, it turns out that the daughter for the first time in her life showed independence, deciding to enter not the institute that her parents chose for her and where they had connections and acquaintances, but where she herself wanted. Her mother cannot forgive her for this and, remembering her failure in the exam every day, explains to her that “you must obey your mother. ” She was placed to work at the specialized institute of the educational institution to which her parents forced her to enter, and besides, every day they try to force her to study and prepare for the institute they chose, accusing her daughter of the fact that with her failure in the exams she “disgraced herself and the whole family, But she still can't get anywhere."
” She was placed to work at the specialized institute of the educational institution to which her parents forced her to enter, and besides, every day they try to force her to study and prepare for the institute they chose, accusing her daughter of the fact that with her failure in the exams she “disgraced herself and the whole family, But she still can't get anywhere."
Sometimes the child’s harsh statements directly indicate that it is precisely in the position and behavior of the parent that serves as the basis for quarrels and conflicts: “I won’t tell you another word about my problems, you distort all the facts and use everything against me!” or even something like this, said in the heat of a quarrel: “If you tell me that again, I'll hang myself! I'm tired of hearing the same things from you." Based on these statements that characterize the behavior of the client, you can ask him: “Do you really say this to her every day?” or “What does he mean when he says you are using this against him?”. More often than not, such a remark is enough to make the parent realize that his own behavior is worthy of criticism. Of course, various excuses may arise in this case: “What else remains for me to do?”, But the fact remains.
More often than not, such a remark is enough to make the parent realize that his own behavior is worthy of criticism. Of course, various excuses may arise in this case: “What else remains for me to do?”, But the fact remains.
Evaluation of one's own position as a manifestation of overprotectiveness is one of the turning points in counseling such cases. But in order for something to change and the problem to be solved, this is not enough - it is necessary to review together with the client at least three points already mentioned above: his position in relation to the child, the tactics of everyday behavior, as well as his idea of \u200b\u200bhis own child, the image what he is.
First of all, one should question the legitimacy and expediency of the position of the omniscient teacher, which is taken by the parent, and also the fact that, by explaining something daily to a twenty-, thirty-, or even forty-year-old “child,” one can achieve any positive result. Sometimes it is enough to ask the client a question: “Are you sure that this is exactly what your child needs?” or “If everything you say is absolutely correct, why do you think he doesn’t listen to you?” Such problems are often associated with the difference in ideas about life, its norms and values among parents and the child, with confidence in one's rightness and inability or unwillingness to part with this “rightness”. Often, when working with an overprotective, overdominant parent, discussion of the peculiarities of his views is not necessary, and even impossible - these clients are too far from understanding the relativity of their own life principles. Therefore, it is more effective, having expressed doubts about the legitimacy of their instructive aspirations, to proceed to an analysis of their behavior - perseverance, control, critical comments, that is, to what directly underlies their disagreements and difficulties in relations with children.
Often, when working with an overprotective, overdominant parent, discussion of the peculiarities of his views is not necessary, and even impossible - these clients are too far from understanding the relativity of their own life principles. Therefore, it is more effective, having expressed doubts about the legitimacy of their instructive aspirations, to proceed to an analysis of their behavior - perseverance, control, critical comments, that is, to what directly underlies their disagreements and difficulties in relations with children.
The discussion of daily behavioral tactics between parent and child can go in different directions. In particular, it is reasonable to say that: 1) direct influence is ineffective, especially when it is based on negative examples and statements; 2) the behavior of parents, perceived and felt as pressure, most often causes not submission, but resistance, negativism, that is, the result is the opposite of what is desired; 3) pressure and control lead to only one thing - relations with the child deteriorate, acquire an undesirable character, which, in fact, is the reason for going to counseling. The probability that in a situation of bad relations it will be possible to explain something, force them to do something, educate them, is practically equal to zero.
The probability that in a situation of bad relations it will be possible to explain something, force them to do something, educate them, is practically equal to zero.
Speaking about the inefficiency of such forms of parental control, one should by no means forget the problem of a parent's attitude towards his child, how the client perceives and evaluates him. Without this, the main request of the client will not be satisfied - the relationship will not be established.
Correction of the parent's attitude to the child
It is usually not difficult to approach the discussion of this issue, because during the conversation quite a lot of statements such as “Without me, he will not do anything” or “She does not understand this” are typed. These and similar remarks are clear evidence of the parent's distrust of the child, the low assessment of his ability to show independence and independence, to be an adult. Of course, there will always be clients who readily assert that for a parent, a child of any age is still a child. But here the main thing is to understand what it really means to be a child: to be loved, loved, significant or helpless, inept, weak? It is one thing to worry about the fate of your neighbor, and quite another to show this anxiety at every step, controlling and actually preventing him from living on his own. One of the options for discussing this difficult and complex topic is a conversation from the point of view of the ideas formulated in humanistic psychology, in particular, by K. Rogers (Rogers S., 1959). A person can truly become an adult and independent person only when he is trusted, and only in this case is he able to believe in his own strength. The doubt of others in the capabilities of a person, manifested, in particular, in hyper-custody (after all, the weak need care!), undermines his faith in his own strength, makes him passive and helpless.
But here the main thing is to understand what it really means to be a child: to be loved, loved, significant or helpless, inept, weak? It is one thing to worry about the fate of your neighbor, and quite another to show this anxiety at every step, controlling and actually preventing him from living on his own. One of the options for discussing this difficult and complex topic is a conversation from the point of view of the ideas formulated in humanistic psychology, in particular, by K. Rogers (Rogers S., 1959). A person can truly become an adult and independent person only when he is trusted, and only in this case is he able to believe in his own strength. The doubt of others in the capabilities of a person, manifested, in particular, in hyper-custody (after all, the weak need care!), undermines his faith in his own strength, makes him passive and helpless.
Sadly, most parents in our culture don't think about things like trusting their children, and often talking about it sounds like a real revelation to them. Moreover, in relation to one's own child, there is often a share of a certain skepticism - “he is too vulnerable”, “I have a lack of independence”. Of course, a person with overprotective tendencies is comfortable when others need him, and therefore it can be difficult for such clients to admit that they really “badly” evaluate their child in the sense that they underestimate him, and if they are right in their assessment, then it's not so much the child's fault as the parent who raised him that way. All this means that the client also has a certain responsibility, which obliges him to re-educate himself.
Moreover, in relation to one's own child, there is often a share of a certain skepticism - “he is too vulnerable”, “I have a lack of independence”. Of course, a person with overprotective tendencies is comfortable when others need him, and therefore it can be difficult for such clients to admit that they really “badly” evaluate their child in the sense that they underestimate him, and if they are right in their assessment, then it's not so much the child's fault as the parent who raised him that way. All this means that the client also has a certain responsibility, which obliges him to re-educate himself.
It can be very important for an overprotective, anxious parent to understand how overprotectiveness manifests itself in his relationship with the child, why certain very “good” intentions turn out to be overwhelming rather than helping, what the absence of control, constant reminders, instructions, prohibitions on independent actions. At this stage of the conversation, the consultant has to not only work with the initial request of the client, but also solve new problems related to the need to replace old ways of behavior with others that are more flexible and adequate to the relationship of a parent with an adult person - their own child. All this is not so easy to do, because the controlling, custodial parent usually firmly believes that if it were not for his reminders and remarks, the child would be “overgrown with dirt”, “everywhere was late”, “could not be able to study”, etc. Therefore, the goals and requirements of the parent, often quite reasonable and relevant in their own right, should also be discussed. When working with a parent, a consultant should understand that although parental control most often does not have a very strong effect on a child’s life outside the parental family, it still happens that over the years of living together, control becomes a necessary element for him in life. It is necessary to prepare the parent for the fact that a change in his behavior is unlikely to lead to an immediate and rapid increase in the independence and consciousness of the child. Rather, on the contrary, a person who has been weaned for many years to be independent may not feel relieved due to the lack of control and reminders, but deep confusion, become more dependent, passive.
All this is not so easy to do, because the controlling, custodial parent usually firmly believes that if it were not for his reminders and remarks, the child would be “overgrown with dirt”, “everywhere was late”, “could not be able to study”, etc. Therefore, the goals and requirements of the parent, often quite reasonable and relevant in their own right, should also be discussed. When working with a parent, a consultant should understand that although parental control most often does not have a very strong effect on a child’s life outside the parental family, it still happens that over the years of living together, control becomes a necessary element for him in life. It is necessary to prepare the parent for the fact that a change in his behavior is unlikely to lead to an immediate and rapid increase in the independence and consciousness of the child. Rather, on the contrary, a person who has been weaned for many years to be independent may not feel relieved due to the lack of control and reminders, but deep confusion, become more dependent, passive. But this stage must be experienced if the parent wants his child to become a truly adult. The help of a parent in acquiring independence by a child may not consist in instructions and advice, but in expressing support and approval on this difficult path.
But this stage must be experienced if the parent wants his child to become a truly adult. The help of a parent in acquiring independence by a child may not consist in instructions and advice, but in expressing support and approval on this difficult path.
Even if the consultation is very successful, the outward change in the parent's behavior is unlikely to happen overnight. But even if the change had happened, it most likely would not have been noticed and appreciated by the child - habits and stereotypes play too great a role in the relations of close people, which do not allow sensitive enough to capture what is happening in another. But the main request of the parent in the discussed version of the appeal is precisely to establish relations with the child! The prospect of postponing his decision to a distant future, when the son (daughter) will notice and appreciate the changes that have occurred with the client, can hardly serve as a sufficient incentive on this good path. Reinforcement, at least in the form of minimal positive changes, should happen quickly enough, and this can be tried to organize during the conversation. What can serve as the beginning of strategic changes in the relationship between the child and the parent, what might tactical steps look like here? Here are a few possible tactics.
Reinforcement, at least in the form of minimal positive changes, should happen quickly enough, and this can be tried to organize during the conversation. What can serve as the beginning of strategic changes in the relationship between the child and the parent, what might tactical steps look like here? Here are a few possible tactics.
Actions of trust
This event is especially appropriate when there is some disagreement (barrier) in the relationship between the child and the parent, which serves as a pretext for numerous quarrels and conflicts and, at the same time, is clearly and unambiguously outlined. For example, a mother requires her son not to drop out of college, or forbids her daughter to be friends with people she likes, but parents seem unreliable and suspicious. Then the action of trust on the part of the parents will consist in the “public” removal (surrender) of a long-standing demand or ban, for example: “I thought about it and decided that quitting or not quitting school is, after all, your own business, you are an adult well, you can decide for yourself. I won’t say a word about this to you again” or “After all, these are your friends, you know them better, meet them whenever you want.” If one of the problems was a ban on traveling somewhere, coming too late, etc., then its removal would also be such an action of trust. It is important that this does not look like a handout from the parent or a demonstration according to the “Do as you know!” principle, but as a manifestation of trust, as evidence of a different, more mature and respectful attitude towards the child's personality. Of course, an action of trust will be such only if, having declared something, the parent will never back down from his decision, but this should be clear to the client himself.
I won’t say a word about this to you again” or “After all, these are your friends, you know them better, meet them whenever you want.” If one of the problems was a ban on traveling somewhere, coming too late, etc., then its removal would also be such an action of trust. It is important that this does not look like a handout from the parent or a demonstration according to the “Do as you know!” principle, but as a manifestation of trust, as evidence of a different, more mature and respectful attitude towards the child's personality. Of course, an action of trust will be such only if, having declared something, the parent will never back down from his decision, but this should be clear to the client himself.
Talking about one's own feelings and experiences
This task is somewhat more difficult, if only because, before the parent begins to express his feelings to the child, he must try to understand them himself. To do this, the consultant should carry out special work aimed at identifying what is hidden behind parental overprotection. Here it makes no sense to go into the “psychoanalysis” of parental feelings, and therefore it is enough, asking the question “Why do you take care of him (her) so much, so guide him (her)?”, To be satisfied with the first answer, which for most clients is unambiguous: “I I'm afraid for him”, “I'm worried about her”. From the point of view of depth psychology, of course, this answer is not complete. Here one could talk about the need of a parent, like any person, to control and manage others, and about the realization of problems of one's own significance, and about the fear of loneliness, and about many other things, which in the case of a reflective client and enough time for discussion, it may well be affected, and which would obviously guarantee much greater success for the proposed changes.
Here it makes no sense to go into the “psychoanalysis” of parental feelings, and therefore it is enough, asking the question “Why do you take care of him (her) so much, so guide him (her)?”, To be satisfied with the first answer, which for most clients is unambiguous: “I I'm afraid for him”, “I'm worried about her”. From the point of view of depth psychology, of course, this answer is not complete. Here one could talk about the need of a parent, like any person, to control and manage others, and about the realization of problems of one's own significance, and about the fear of loneliness, and about many other things, which in the case of a reflective client and enough time for discussion, it may well be affected, and which would obviously guarantee much greater success for the proposed changes.
But more often than not, due to various limitations within the counseling framework, these issues cannot be worked through. Therefore, from our point of view, it is better to orient the parent on the path of behavioral changes associated with compensation for parental anxiety and the need for control than to start an in-depth analysis without the possibility of successfully completing it. Such an important behavioral change is the reorientation of the parent from constant control to the manifestation of their own feelings and experiences associated with the child, an inadequate expression of which, in a sense, is overprotection. Such a goal, at first glance, seems quite simple. This means that the client should instead of “Don’t you dare think about dropping out of college!” say “I'm so afraid that you will break your whole life if you stop studying. At one time, everyone advised me to finish my dissertation, but I just got married, there was absolutely no time, and in the end I was left with nothing, and I’m terribly afraid that you will succeed too.”
Such an important behavioral change is the reorientation of the parent from constant control to the manifestation of their own feelings and experiences associated with the child, an inadequate expression of which, in a sense, is overprotection. Such a goal, at first glance, seems quite simple. This means that the client should instead of “Don’t you dare think about dropping out of college!” say “I'm so afraid that you will break your whole life if you stop studying. At one time, everyone advised me to finish my dissertation, but I just got married, there was absolutely no time, and in the end I was left with nothing, and I’m terribly afraid that you will succeed too.”
It may seem like a small difference, but it's surprising how difficult it is for clients to simply complete the phrase "I feel like...". The expression of one's own feelings can be very effective in resolving the situation, because sometimes it is precisely because these people rarely speak out or analyze their own feelings in front of anyone that the feelings and experiences of others remain incomprehensible to them or are interpreted quite primitively: “He acts to spite me”, "She doesn't understand anything. " But as soon as the client is able to reveal his feelings to another - in this case, his own adult child, the child's experiences may also be revealed to him; and, having understood them, the parent may no longer feel the need to control or worry about anything (everything may turn out to be not so scary: the child is not too passive, friends are not so loose, etc.).
" But as soon as the client is able to reveal his feelings to another - in this case, his own adult child, the child's experiences may also be revealed to him; and, having understood them, the parent may no longer feel the need to control or worry about anything (everything may turn out to be not so scary: the child is not too passive, friends are not so loose, etc.).
During a conversation with a client, it is appropriate not only to discuss the problem of feelings, but also to talk about why it is so necessary to share them with others, to make them feel what it means to express them. So, the client can be offered to play the situation using the “empty chair” technique, on which he must imagine sitting his son or daughter, that is, those who need to be told what feelings and experiences he experiences about the difficulties and quarrels that arise in relationships every day . The use of Gestalt therapy techniques for this purpose must necessarily be combined with a discussion of what exactly was difficult to talk about and why, how these difficulties can be overcome, how to more accurately formulate what the client wants to say, etc.
Arranging a rapport
Attitude change is an extraordinarily complex process, so it is often appropriate to force this reorientation somewhat by arranging a parent-child rapport. The purpose of such a conversation is to show the client’s son or daughter that the attitude towards him (her) has changed, to try to reach a level of deeper contact and interaction than before, telling about yourself, about your feelings and experiences, which are based on parental anxiety. , anxiety and love for the child. Such a conversation, in which both - both the parent and the child - have the opportunity to repent of their “sins”, open their souls, get rid of accumulated grievances and claims, can be a real milestone in their relationship.
In this regard, I would like to draw attention to one of the most important rules of counseling. If it is necessary for some event in the life of the client to take place, it should be discussed as specifically as possible, and, if possible, even set a time for its implementation during the conversation. A specific discussion is the choice of a suitable place, time, enumeration of possible options for starting, etc. Such specification is necessary in order to identify possible obstacles in the way of completing the task, which may not be noticed during a superficial discussion, but are quickly revealed when specific planning begins. For example, a client decides to talk to her daughter, but it turns out that she returns home very late, when her parents are already sleeping, and on the weekend the parents go to the country. Thus, in order to have a long, calm conversation, you need to specifically find and plan a time convenient for both parties. The consultant, acting in this situation as a “generator of ideas”, can greatly contribute to the expedient solution of this problem. When a decision is made not “in principle”, but quite specifically (its time is set, the appropriate form is chosen), then, firstly, it is much more difficult not to fulfill it, and, secondly, the analysis of the reasons for non-fulfillment can become good basis for a deeper understanding of the causes of disagreement.
A specific discussion is the choice of a suitable place, time, enumeration of possible options for starting, etc. Such specification is necessary in order to identify possible obstacles in the way of completing the task, which may not be noticed during a superficial discussion, but are quickly revealed when specific planning begins. For example, a client decides to talk to her daughter, but it turns out that she returns home very late, when her parents are already sleeping, and on the weekend the parents go to the country. Thus, in order to have a long, calm conversation, you need to specifically find and plan a time convenient for both parties. The consultant, acting in this situation as a “generator of ideas”, can greatly contribute to the expedient solution of this problem. When a decision is made not “in principle”, but quite specifically (its time is set, the appropriate form is chosen), then, firstly, it is much more difficult not to fulfill it, and, secondly, the analysis of the reasons for non-fulfillment can become good basis for a deeper understanding of the causes of disagreement. So, for example, in our case, the client may have to go to bed later one day in order to wait for her daughter and talk to her. And even if by this time she will be so annoyed that she will not be able to talk normally with her daughter, this failed conversation can be excellent material for a deeper discussion of her relationship with her child, since the irritation that arose while waiting is very revealing and can become the basis for analysis of the relationship of the client to her daughter.
So, for example, in our case, the client may have to go to bed later one day in order to wait for her daughter and talk to her. And even if by this time she will be so annoyed that she will not be able to talk normally with her daughter, this failed conversation can be excellent material for a deeper discussion of her relationship with her child, since the irritation that arose while waiting is very revealing and can become the basis for analysis of the relationship of the client to her daughter.
Counseling parents about problems and difficulties in a child's life
An overprotective position of a parent is also dangerous because it often leads to an incorrect assessment of their own child: the parent begins to perceive his behavior as abnormal, causing serious concern, etc. Sometimes a client, when asking for help, puts forward arguments so inadequate that they begin to seem simply absurd. “It seems to me that my daughter is a drug addict: she sometimes comes back late, and her eyes are so sparkling!” or “I am very worried about the moral character of my girl. Several times I saw young people accompanying her, and she kissed two of them. But the consultant should treat any statements of the client carefully and with restraint, since, on the one hand, something more serious can be hidden behind them than the exaggerations of the mother, and on the other hand, it is possible to influence the opinion of a person, calm anxieties only when a good trust is established. contact, which is impossible without accepting everything that is said at the beginning of the conversation.
Several times I saw young people accompanying her, and she kissed two of them. But the consultant should treat any statements of the client carefully and with restraint, since, on the one hand, something more serious can be hidden behind them than the exaggerations of the mother, and on the other hand, it is possible to influence the opinion of a person, calm anxieties only when a good trust is established. contact, which is impossible without accepting everything that is said at the beginning of the conversation.
Further work with the client depends on how real the fears and concerns expressed by the client are. If there are no grounds for them, the reason for contacting a psychologist is most often associated with the problems of the parent himself, while complaints about children in such a situation act as a kind of socially acceptable reason for coming. This option of contacting a consultation about the problems of another is a classic, a lot has been written about it both in domestic and foreign literature (Varga A. Ya., 1985, Eidemiller E.G., 1980). But before trying to get to the problems of the parent himself, it is necessary to complete the topic of the child by analyzing situations where asking for help turns out to be associated with real problems and difficulties in the life of a son / daughter, which really require intervention and help from parents to one degree or another.
Ya., 1985, Eidemiller E.G., 1980). But before trying to get to the problems of the parent himself, it is necessary to complete the topic of the child by analyzing situations where asking for help turns out to be associated with real problems and difficulties in the life of a son / daughter, which really require intervention and help from parents to one degree or another.
Of course, before making such a “diagnosis”, the consultant must collect enough concrete facts to support the fears. Unfortunately, there are times when there is no doubt about the seriousness of the problems. For example, a client says: “My daughter is a drug addict, she admitted it herself. She tried to quit, but it didn't work. What do we do now?" Very often, problems associated with various social and mental deviations from the norm are intertwined with the fear of turning to any official (medical, legal, etc.) authorities. Such fears, unfortunately, are quite justified; one does not have to go far for negative examples. Of course, a psychologist should in no case replace medical or any other institutions, but with such treatment, there are a number of psychological tasks, the solution of which can significantly improve the client's life situation and which can be professionally solved only with the help of a consultant . Among them are: 1) listen to the client, let him talk and support him; 2) give a qualified recommendation where, why and how to apply; 3) help find ways to show the specialist even the most intractable person what the client’s child is in this situation; 4) help the client establish normal relationships with their own child.
Of course, a psychologist should in no case replace medical or any other institutions, but with such treatment, there are a number of psychological tasks, the solution of which can significantly improve the client's life situation and which can be professionally solved only with the help of a consultant . Among them are: 1) listen to the client, let him talk and support him; 2) give a qualified recommendation where, why and how to apply; 3) help find ways to show the specialist even the most intractable person what the client’s child is in this situation; 4) help the client establish normal relationships with their own child.
The first of these tasks can be solved quite simply: probably even a novice consultant can listen to a client in a qualified manner. Perhaps, in such a situation, there is only one particularly important point: a person in such a situation often thinks that something terrible is happening to him, that this has never happened anywhere, never to anyone and there is no solution to this problem. Such fears should be given special attention in order to reduce the feeling of uniqueness and reassure the possibility of changing the existing situation.
Such fears should be given special attention in order to reduce the feeling of uniqueness and reassure the possibility of changing the existing situation.
Quite often the client does not know where and how to apply, where drug addicts are treated, where and how they can provide psychiatric assistance without registering, etc. If the psychologist has the information necessary for the client, in this case he can act as an adviser - where and how to go, to whom and what to say, what to ask, etc. Often in the case of such a request, the consultant is called upon to perform another implicit, but often very important task. After all, the client checks on him the possible reaction of the social environment. Perhaps for the first time he told something that clearly compromises both himself as a parent and his child. And what happened? How did they react? What did they say? In this sense, the consultant should serve as a guarantee that others can and are ready to help the client in every possible way, and turning to other specialists will bring not only feelings of grief and shame from talking about the problem, but also the desired help.
Referring to a specialist a person who for some reason is afraid of an appropriate consultation is a rather difficult task. A parent who refers their child to a specialist in such a situation often cannot find the right tone and ways to motivate. In most cases, he threatens, promises that “everyone will explain to you who you really are”, that is, he emphasizes, first of all, the negative aspects associated with the upcoming visit, which, of course, does not motivate at all, but only undermines the child’s trust in the father or mother. After discussing with the parent what and how he says to his son or daughter in this situation, the consultant can try to remove the negative and bring positive points into the “motivation process” as much as possible. As such, here may be: a) assistance that must be provided in a timely manner, as a result of which the child will be spared unnecessary mental or physical suffering; b) adequate organization of assistance that a parent can provide - anonymity (if it is important), turning not just to someone, but to a qualified, well-known specialist; c) a story about the feelings and experiences experienced by the parent about the child (of course, they must be presented in the appropriate form, without blaming anyone), which can serve as another indication of the need for treatment (“You are so good to me. happened to you, it's an accident, let's fix it as soon as possible and return to normal life").
happened to you, it's an accident, let's fix it as soon as possible and return to normal life").
In most cases, except for endogenous diseases, the parent bears a certain amount of guilt and responsibility for what happened to the child. But the analysis of the situation, which in itself is quite complex and requires an immediate solution, is also often not possible from this point of view, although there is a category of clients who seek to understand “why and how this happened”. The main thing that the consultant needs to do, regardless of whether the reasons for what is happening or not will be analyzed during the conversation, is to reorient the client from the position of accusation and dissatisfaction, which he most often consciously or unconsciously takes, to the position of acceptance and support.
Unfortunately, many parents in a situation of severe mental or social difficulties experienced by their children tend to teach their children, criticize them, point out some of their former rightness. And children who already have a hard time can be extremely painful to perceive even such harmless, at first glance, remarks as “I warned you not to mess with them” or “Now it’s better for you to be silent, and not to argue” - and consider them evidence of rejection and unwillingness to help. In such cases, as in situations associated with the manifestation of overprotection, it is too late and pointless to teach something. Children need support. And it is not advice or even more punishment that can save them from further “falling”, but a feeling of acceptance and sympathy from the parent. The consultant often has to act as a kind of translator and interpreter of the meaning of what the child says and does, and explain to the client how hard it is for the child, to prove that irascibility and negativism in behavior do not indicate disrespect and arrogance, but the severity of experiences and the lack of opportunity for someone or talk about them. “Imagine yourself in his place. After all, you would like to be helped first of all, right?”
And children who already have a hard time can be extremely painful to perceive even such harmless, at first glance, remarks as “I warned you not to mess with them” or “Now it’s better for you to be silent, and not to argue” - and consider them evidence of rejection and unwillingness to help. In such cases, as in situations associated with the manifestation of overprotection, it is too late and pointless to teach something. Children need support. And it is not advice or even more punishment that can save them from further “falling”, but a feeling of acceptance and sympathy from the parent. The consultant often has to act as a kind of translator and interpreter of the meaning of what the child says and does, and explain to the client how hard it is for the child, to prove that irascibility and negativism in behavior do not indicate disrespect and arrogance, but the severity of experiences and the lack of opportunity for someone or talk about them. “Imagine yourself in his place. After all, you would like to be helped first of all, right?”
Only by having a good, trusting relationship with a child, a parent can have at least some influence on him and, thus, not with advice, but with empathy, keep him from taking a rash step, taking drugs, contacts with socially dangerous people, etc. If there are trusting relations with parents, on the one hand, the child tends to listen to them more, and on the other hand, the strongest deterrent works, the fear of hurting loved ones: feeling the experiences of the father / mother, it is more difficult to hurt him / her than when he / she looks cold and judgmental. Thus, the situation of trust provides more opportunities for control, but not for direct, but for indirect. If the relationship between a parent and a child is already quite severely disturbed by the time of arrival at the consultation, special measures can be discussed aimed at normalizing them - actions of trust, a frank conversation, etc., as already mentioned above.
If there are trusting relations with parents, on the one hand, the child tends to listen to them more, and on the other hand, the strongest deterrent works, the fear of hurting loved ones: feeling the experiences of the father / mother, it is more difficult to hurt him / her than when he / she looks cold and judgmental. Thus, the situation of trust provides more opportunities for control, but not for direct, but for indirect. If the relationship between a parent and a child is already quite severely disturbed by the time of arrival at the consultation, special measures can be discussed aimed at normalizing them - actions of trust, a frank conversation, etc., as already mentioned above.
Inexperienced counselors often face particular difficulties in dealing with the above cases when, after a successful conversation with a father or mother, they are ready to agree (in response to the client's persuasion) to work with a child whose condition most often requires a completely different intervention. Of course, a conversation with a psychologist can be useful for such a client, but in no case should it replace other forms of influence on him.
Of course, a conversation with a psychologist can be useful for such a client, but in no case should it replace other forms of influence on him.
Counseling parents about their own problems
We have already mentioned that parents often turn to a psychologist about their children, talking about them and their problems with them in such a way that the question arises: why and with what real problems did these clients come to the consultation. Many of them immediately report that they came secretly from their children, confident that they most likely will not approve of their act, and talking about their relationship with their son (daughter), they report that they are completely independent people, often living separately and, in general, little listening to the opinion of their parents.
After listening to the story of such a client, the psychologist can state at least three points that make it difficult to provide psychological assistance: 1) one cannot be sure that the problem also exists from the point of view of the child, and not only from the point of view of the parents; 2) the client does not enjoy such great authority that his advice or help really serves to change the situation; 3) the consultant does not have the opportunity to make contact with the person whose life he is asked to influence. The preoccupation, the involvement of the client in the affairs of another, even if this other is his own child, is suspicious: does the true reason for the arrival correspond to the explicit one reported by the client? The task of the consultant with this type of treatment is to take the conversation to a deeper level, to find other, often unconscious or unannounced reasons for the client to come. You can go to this deeper level based on: a) the facts of the client's story; b) certain methods of conducting a conversation; c) opinions about the client's children or other spouse.
The preoccupation, the involvement of the client in the affairs of another, even if this other is his own child, is suspicious: does the true reason for the arrival correspond to the explicit one reported by the client? The task of the consultant with this type of treatment is to take the conversation to a deeper level, to find other, often unconscious or unannounced reasons for the client to come. You can go to this deeper level based on: a) the facts of the client's story; b) certain methods of conducting a conversation; c) opinions about the client's children or other spouse.
Specifying the problem situations described by the client often leads to the fact that the client begins to feel that he is not included in the events described and is not informed. Interest in his personal experiences, which arise only about those problems that he sees in a child, quickly begins to prevail in his story over concern for the problems of his daughter or son. So, for example, the problem of a daughter can be expressed by the mother in the following words: “She shouldn’t quarrel with her husband like that, she will remain, like me, alone with two children in her arms. ” But often the theme of their own problems and failures, which sounds obvious to the consultant, is poorly understood by the parent himself. However, in order to identify the real reason for coming to the consultation and assistance to the client, it is necessary that he himself feels the substitutive nature of his initial complaints. To do this, the psychologist can take a more active position, using certain conversation techniques, for example, asking paradoxical questions like: “Why are you so worried about your child’s difficulties?” or “Have you ever felt such involvement in his affairs as excessive?”. When working with a client who is not prone to reflection, for whom the concern of parents about children, even excessive, is perceived simply as part of parental duty, another approach is possible:
” But often the theme of their own problems and failures, which sounds obvious to the consultant, is poorly understood by the parent himself. However, in order to identify the real reason for coming to the consultation and assistance to the client, it is necessary that he himself feels the substitutive nature of his initial complaints. To do this, the psychologist can take a more active position, using certain conversation techniques, for example, asking paradoxical questions like: “Why are you so worried about your child’s difficulties?” or “Have you ever felt such involvement in his affairs as excessive?”. When working with a client who is not prone to reflection, for whom the concern of parents about children, even excessive, is perceived simply as part of parental duty, another approach is possible:
Counselor: Have you ever been told by your child or anyone close to you that you worry too much about him?
Client: What else should I worry about if not about my child? (or: Maybe you will advise me something useful for him, and I will give him, and he will respect me more, obey me).
Counselor: Do you really have nothing else to worry about in your life? (or: Why do you need authority and respect in the eyes of your child?)
Within the framework of such a dialogue, one can try to formulate the true reason for the appeal. Ultimately, the basis of the conversion is always the problems of the one who applies. What personal problems and experiences can underlie the parents' treatment of their adult children?
1. Feeling of one's emptiness, uselessness, inability to manage one's own life, a feeling of resentment towards others and children (“Here, I have grown old, nobody needs me”).
2. The feeling of one's own unfulfillment in life™, failure and the projection of these fears onto children (“Let them not repeat my mistakes”).
3. Feeling of parental incompetence, guilt before the child for miscalculations in upbringing, for the lack of attention to him in childhood, an attempt to compensate for this.
4. Deeper personal problems, fears, etc.
Reframing the problems of clients in such a way that the locus of their concern is not their children, but themselves, is an important step in the process of work. At the same time, in no case should a person have the feeling that he was forced to confess why he came. Turning to a discussion of the client’s own problems, the psychologist can offer the client some kind of rationalization such as: “It’s hardly worth worrying about adult children like that, they won’t appreciate it anyway, it’s better to think about yourself” or: “You took care of them enough, it’s time for you to take care of yourself." Do not insist that the client colorfully paint his life as empty or unfulfilled. It is enough for him to be convinced that the main thing in which he needs help is himself, and that there is nothing unworthy or shameful in seeking such help or advice. This can then be followed by a more detailed discussion of the problems.
Let's dwell briefly on the work strategies depending on the reasons for the arrival of clients.
1. In a situation where the client feels empty, unfulfilled in his own life, the task of counseling work is to help fill his life, to find things that are interesting and enjoyable for him. To this end, he can be asked about what he likes or liked to do, what was interesting, is there something that he would like to do, but what has been put off for a long time, and now the client does not dare to take it on. With such a detailed questioning, a person will usually have many ideas about interesting things that could be worth doing. Social desirability provides a kind of help to the psychologist in this work, since from the point of view of generally accepted ideas, one who is not interested in anything (except for family and children) is an uninteresting and empty person. And naturally, no one wants to look like that in the eyes of a significant other - a consultant. But it is not enough for a psychologist to simply hear that a client has interests; it is necessary to make sure that he really takes a more active position in relation to his own life, begins to fill and organize his time himself, to go about his own business. The guarantee of such activity of the client is most often the presence of a partner, someone with whom one could do something together and, thus, not only interesting to live, but also to be necessary and interesting for someone. In principle, one can imagine three possible options for the appearance of such a partner - one of the family members, old friends and acquaintances, some new acquaintances.
The guarantee of such activity of the client is most often the presence of a partner, someone with whom one could do something together and, thus, not only interesting to live, but also to be necessary and interesting for someone. In principle, one can imagine three possible options for the appearance of such a partner - one of the family members, old friends and acquaintances, some new acquaintances.
Paradoxically, in such a situation, clients often underestimate their own family, their relatives, children and grandchildren. Trying to prove their usefulness by interfering in their affairs, they forget about what can be found in the family of those who themselves will need and be interested. So, as partners in cultural events and entertainment, the grandchildren of clients, whom they often look at as small, not understanding, not interested, and who can, with the help of a consultant, can act for them in a different role - as those who want to know new about the world, who really needs guardianship and guidance in understanding the world of art, life, and other people. Often there are other people in the family who need participation, care, help, and to whom the client for some reason does not pay attention or does not perceive his role in relation to this person as necessary and important. Talking about this with a psychologist can help you look differently at your position in the system of family relationships.
Often there are other people in the family who need participation, care, help, and to whom the client for some reason does not pay attention or does not perceive his role in relation to this person as necessary and important. Talking about this with a psychologist can help you look differently at your position in the system of family relationships.
Many of the problems of such clients suffering from their own uselessness and feelings of loneliness are associated with difficulties in communication. So, very often they have friends, but they rarely meet with these friends, they are afraid to be intrusive, they do not dare to offer their own options for spending free time. Thus, in order for the situation of their life to really change, the consultant should plan these changes as carefully as possible, discuss how and to whom of the acquaintances you can contact, what to offer, for whom a call or meeting with a client can really bring joy, who can keep company in spending free time. The support and attention of the consultant during the discussion for such a lonely person can already have a healing effect in themselves - help them think about themselves and their desires, start acting, feel active and needed. Unfortunately, it happens that a client has few or rather amorphous ideas of his own, and among his friends and relatives it is difficult to find a person who could act as a partner of interest. Therefore, for successful work, the psychologist must be able to offer for discussion some of his ideas, where and how the client can go, what to do, always taking into account what the client wants or dreams about - to become needed, to become informed, cultured, travel, etc. As a material for discussion, the consultant can offer information about various clubs, associations, evenings, while it is not important how the proposed option suits this client, it is more important to “rock” him, move him to search for new ideas and life options, focus on acquiring new acquaintances and friends.
The support and attention of the consultant during the discussion for such a lonely person can already have a healing effect in themselves - help them think about themselves and their desires, start acting, feel active and needed. Unfortunately, it happens that a client has few or rather amorphous ideas of his own, and among his friends and relatives it is difficult to find a person who could act as a partner of interest. Therefore, for successful work, the psychologist must be able to offer for discussion some of his ideas, where and how the client can go, what to do, always taking into account what the client wants or dreams about - to become needed, to become informed, cultured, travel, etc. As a material for discussion, the consultant can offer information about various clubs, associations, evenings, while it is not important how the proposed option suits this client, it is more important to “rock” him, move him to search for new ideas and life options, focus on acquiring new acquaintances and friends. Having felt the possibility of such a search, a person, without the help of a consultant, will be able to find something to his own taste, although it is often useful to specifically discuss with him how to make new acquaintances, expand and deepen the circle of communication (we will talk more about this in the next chapter) .
Having felt the possibility of such a search, a person, without the help of a consultant, will be able to find something to his own taste, although it is often useful to specifically discuss with him how to make new acquaintances, expand and deepen the circle of communication (we will talk more about this in the next chapter) .
2. The feeling of one’s own unfulfillment, of an unsuccessfully lived life, as well as the desire that in his life the child achieve and do everything that his parents failed to do in his time, and the fear that he will not succeed is a fairly common problem. Usually, such experiences of parents seriously complicate their relationship with their children, making them unwitting tyrants who restrict the freedom of their child. It is not an easy task to change the attitude towards one's own life in a fairly elderly person who has already lived most of it, especially since often such people's life really did not pass quite simply and successfully. Moreover, now another external aspect of this problem has appeared, connected with a sharp change in social circumstances, when thousands of people suddenly realized that what they had served for years, what they believed in, was, in essence, a lie, but it was time to live life the other is almost gone.
First of all, such clients need to be reassured, to increase their own value in their eyes. Dealing with such problems requires great skill from the psychologist. What exactly can be done? Firstly, to express confidence that he did everything he could in his life, that the difficulties that the client overcame were really serious and there is nothing surprising that so much effort was spent on them. Secondly, to emphasize the importance of the client's life achievements, and many things can act as real achievements: scientific results, spiritual values, helping people, grown children. And, thirdly, discuss with the client that what matters in life is not what a person has achieved, but how he achieved this, what life values he adhered to. In this sense, for example, honesty, kindness, sincerity of the client can act as the most important values that have been realized in life, no matter what. Special literature can be of great help in working with such problems to a psychologist (Frankl V. , 1989; Fromm E., 1989, 1990 and others).
, 1989; Fromm E., 1989, 1990 and others).
3. A parent's feeling of guilt towards a child is a fairly common phenomenon, but this guilt is especially inappropriate in the situations discussed, since it is associated with actions and events from the distant past. The simplest tactic of work in this case is to demonstrate the senselessness of the feeling experienced by the client. This can be done in different ways, for example, by showing the client the inexpediency, the inappropriateness of those actions, clarifications and explanations that are undertaken by him in order to make amends for this guilt. Such smoothing over, often in the form of intervention, only complicates the relationship with the child. It is also useful to discuss the past with the client and show him that his actions in those cases that are now the object of anxiety and experiences were the only real and possible ones, that their negative consequences could not be foreseen, that judging oneself of the past from the position of one’s present one is, in principle, a meaningless task that does not lead to a solution to the situation.
As an example of such self-criticism, let's cite the case of a client who, from her point of view, sent her daughter to kindergarten too early, because she needed money, she had to go to work, and there was no one to take care of the girl. In the garden, the girl fell ill with a sore throat, which gave a complication to her ears, as a result of which she practically cannot hear in one ear. This girl has long been an adult woman, and the client still punishes herself for what happened, she believes that her daughter's problems with her husband are the result of her deafness.
Psychology bookap
A parent's experience of guilt towards a child is most often aggravated by fears and feelings of own uselessness, which were mentioned above and which should also be discussed with the client. Moreover, the aggravation of feelings of guilt is usually associated with some real situations that intensify the client's problems of his own life and loneliness. In the example above, the client hoped that, in retirement, she would finally be able to devote all her time to her daughter in order to atone for her guilt, but she, of course, does not need this for a long time, such a prospect can only scare her.