Can reiki cure depression
Reiki for Depression
Skip to contentPrevious Next
- View Larger Image
According to the World Health Organization (WHO), depression affects approximately 280 million people around the world. In early 2020 due to the global pandemic, depression rates in US adults rose from 8.5% to a shocking 27.8%. Even worse, Boston University School of Public Health published new research in October, 2021 in The Lancet showing that the depression rate has risen even further in 2021 to 32.8%. This is 1 in every 3 adults in the US. When depression isn’t properly treated, this condition reduces the quality of life for sufferers and can lead to a number of serious consequences. Many different treatments exist for depression.
Regardless of the main treatment methods chosen, patients dealing with the symptoms of depression may experience benefit from participating in Reiki sessions in conjunction with their professional treatment programs and methods.
The Dangers of Depression
Depression is a common condition that causes affected individuals to experience feelings of sadness, guilt, loss of interest in enjoyable activities, appetite disturbances, low self-esteem, and sleep issues. It can affect people regardless of age, gender, ethnicity, occupation, or any other characteristic. Although depression may occur after someone experiences a trauma, such as a death in the family, loss of a job, or a serious illness, it can also appear to occur without an apparent cause.
If left untreated, depression can affect the sufferer’s quality of life, as well as his or her personal relationships. Depression can also affect the individual’s professional life by impairing his or her ability to function while at work. In the worst cases, depression may even result in total disability or death by suicide.
Because it can be so serious, finding effective treatment for depression is essential. So, seeking a qualified professional skilled in therapy, treatment programs, and talking with your physician is the first course of action. Then, in conjunction with working with a professional team and or program, Reiki can help as an adjunct therapy.
Then, in conjunction with working with a professional team and or program, Reiki can help as an adjunct therapy.
Benefits of Reiki for Depressed Clients
Reiki can be beneficial to clients with depression in multiple ways. Some of the benefits of Reiki sessions for depressed clients include:
- Better sense of mental and physical balance. – Reiki may help restore a person’s overall sense of balance, both in the mind and the body. This may help to improve the person’s mood and help him or her to overcome feelings of guilt and/or sadness.
- Reiki is relaxing. – Depression is often accompanied by anxiety. However, Reiki can be relaxing, which may help to combat this anxiety. As the individual’s anxiety is relieved, his or her depression may improve as well.
- Reiki puts the client back in control. – Many people who are depressed feel like they are not in control of their own lives. When a client participates in a Reiki session, he or she is doing something proactive, thus restoring some of the feelings of control.
- Reiki allows the client to connect with another person. – One of the most common symptoms of depression involves withdrawing from friends and family or feeling disconnected from others. Reiki provides depressed clients with the opportunity to connect with a caring, compassionate practitioner, which may improve symptoms.
- Reiki relieves stress. – Stress can contribute to the development of depression, and ongoing stress can also worsen a depressed person’s symptoms. Reiki may help to relieve some of a client’s stress, which may, in turn, reduce the symptoms of depression.
Relevant Research
Several research studies support the use of Reiki for people with depression. Some of these studies are listed below.
- Reiki aids in relaxation. – Center for Reiki Research According to the Center for Reiki Research, Reiki has been shown to reduce sympathetic autonomic stimulation and produce a significant relaxation response among people who had been diagnosed with Burnout Syndrome, a disorder characterized by exhaustion and emotional issues.
 It is likely that the same relaxation response would be produced among clients with depression.
It is likely that the same relaxation response would be produced among clients with depression. - Reiki reduces the symptoms of depression. – Alternate Therapies in Health and Medicine In addition, according to a study published in Alternate Therapies in Health and Medicine, patients who received regular Reiki treatments demonstrated a significant reduction in the symptoms of psychological distress and depression. The symptom reduction experienced by these patients continued for one year after the treatment regimen was complete.
- Reiki may help reduce postoperative depression. – Anecdotal Evidence Furthermore, anecdotal reports by trained Reiki healer Julie Motz indicate that Reiki may effectively help reduce postoperative depression among heart transplant patients. These reports were generated as a result of Ms. Motz’s involvement in multiple heart transplant surgeries with television Dr.
 Mehmet Oz. Ms. Motz performed Reiki during the transplant procedures and the patients were evaluated for symptoms of postoperative depression during their recovery periods.
Mehmet Oz. Ms. Motz performed Reiki during the transplant procedures and the patients were evaluated for symptoms of postoperative depression during their recovery periods.
Reiki for Depression
Implications for Patients
Based on the research studies detailed above, as well as reports from patients who have experienced benefits from Reiki sessions, it seems that Reiki may be a valuable addition to treatment regimens for patients suffering from depression. However, although Reiki may help to alleviate some of the symptoms of depression, it will be more effective when used in conjunction with traditional therapies. Other treatments that may be beneficial to people who are suffering from depression include cognitive behavioral therapy, psychotherapy, and certain medications. Patients with depression may also experience a reduction in symptoms with regular physical activity.
For best results, people experiencing depression should participate in multiple Reiki treatments over an extended period of time. A single treatment may be helpful, but multiple treatments are more likely to result in long-term symptom improvement. If you are experiencing depression be sure to also see a qualified counselor, therapist, and/or medical professional to assist with your road to recovery. Reiki can also help on this road.
A single treatment may be helpful, but multiple treatments are more likely to result in long-term symptom improvement. If you are experiencing depression be sure to also see a qualified counselor, therapist, and/or medical professional to assist with your road to recovery. Reiki can also help on this road.
Finding a Practitioner
If you are suffering from depression, you may benefit from Reiki sessions in conjunction with your primary care. If you are interested in beginning Reiki treatments, you can search for a practitioner in your area right here on our website. For help and support please be sure to talk with family, friends, your physician, and/or reach out to depression resources. People care about you and can help!
Like This Article? JOIN IARP – Click to become a Professional Member today!
Sources: https://www.bu.edu/articles/2021/depression-rates-tripled-when-pandemic-first-hit/,https://www.thelancet.com/journals/lanam/article/PIIS2667-193X(21)00087-9/fulltext,https://www.
 who.int/news-room/fact-sheets/detail/depression
who.int/news-room/fact-sheets/detail/depressionIARP Memberships
JOIN IARP TODAY!
MEMBER BENEFITS
RENEW OR LOGIN
REIKI ARTICLES
Find exactly what you are looking for…
Search for:
Categories
Select CategoryAll Reiki Articles (128)International Reiki (15)Lifestyle (16)News and Information (22)Personal Experiences (16)Professional Development (30)Regional Reiki (19)Reiki and Chakras (6)Reiki and Medicine (45)Reiki and Religion (6)Reiki and the Family (21)Reiki Business (19)Reiki en Espanol (6)Reiki en Français (1)Reiki for Animals and Pets (10)Reiki Healing (12)Reiki in Hospitals (25)Reiki Near Me (15)Reiki Research (19)Self Care and Personal Development (28)What’s New? (126)
Translate this website
Watch: Grow Your Reiki Practice Video
Sign Up for our eNewsletter!
Download our free report:
“The 5 Cost-Free and Effective Ways to Expand Your Reiki Practice”and receive great Reiki articles, business tips and more!
Click HERE to receive The Reiki Report delivered to your inbox monthly, chock full of tips, articles and inspiring stories. (Link will open in a pop-up window. Make sure your browser is not blocking pop-ups.)
(Link will open in a pop-up window. Make sure your browser is not blocking pop-ups.)
Follow IARP!
IARP2021-11-22T15:03:59-07:00 Page load linkGo to Top
Reiki for depression and anxiety
Review
. 2015 Apr 3;(4):CD006833.
doi: 10.1002/14651858.CD006833.pub2.
Janine Joyce 1 , G Peter Herbison
Affiliations
Affiliation
- 1 Gardens, Dunedin, Otago, New Zealand, PO Box 8092.
- PMID: 25835541
- DOI: 10.
 1002/14651858.CD006833.pub2
1002/14651858.CD006833.pub2
Review
Janine Joyce et al. Cochrane Database Syst Rev. .
. 2015 Apr 3;(4):CD006833.
doi: 10.1002/14651858.CD006833.pub2.
Authors
Janine Joyce 1 , G Peter Herbison
Affiliation
- 1 Gardens, Dunedin, Otago, New Zealand, PO Box 8092.
- PMID: 25835541
- DOI: 10.1002/14651858.CD006833.pub2
Abstract
Background: Anxiety and depression affect many people. Treatments do not have complete success and often require people to take drugs for long periods of time. Many people look for other treatments that may help. One of those is Reiki, a 2500 year old treatment described as a vibrational or subtle energy therapy, and is most commonly facilitated by light touch on or above the body. There have been reports of Reiki alleviating anxiety and depression, but no specific systematic review.
Treatments do not have complete success and often require people to take drugs for long periods of time. Many people look for other treatments that may help. One of those is Reiki, a 2500 year old treatment described as a vibrational or subtle energy therapy, and is most commonly facilitated by light touch on or above the body. There have been reports of Reiki alleviating anxiety and depression, but no specific systematic review.
Objectives: To assess the effectiveness of Reiki for treating anxiety and depression in people aged 16 and over.
Search methods: Search of the Cochrane Register of Controlled Trials (CENTRAL - all years), the Cochrane Depression, Anxiety and Neurosis Review Group's Specialised Register (CCDANCTR - all years), EMBASE, (1974 to November 2014), MEDLINE (1950 to November 2014), PsycINFO (1967 to November 2014) and AMED (1985 to November 2014). Additional searches were carried out on the World Health Organization Trials Portal (ICTRP) together with ClinicalTrials.gov to identify any ongoing or unpublished studies. All searches were up to date as of 4 November 2014.
Additional searches were carried out on the World Health Organization Trials Portal (ICTRP) together with ClinicalTrials.gov to identify any ongoing or unpublished studies. All searches were up to date as of 4 November 2014.
Selection criteria: Randomised trials in adults with anxiety or depression or both, with at least one arm treated with Reiki delivered by a trained Reiki practitioner.
Data collection and analysis: The two authors independently decided on inclusion/exclusion of studies and extracted data. A prior analysis plan had been specified but was not needed as the data were too sparse.
Main results: We found three studies for inclusion in the review. One recruited males with a biopsy-proven diagnosis of non-metastatic prostate cancer who were not receiving chemotherapy and had elected to receive external-beam radiation therapy; the second study recruited community-living participants who were aged 55 years and older; the third study recruited university students. These studies included subgroups with anxiety and depression as defined by symptom scores and provided data separately for those subgroups. As this included only 25 people with anxiety and 17 with depression and 20 more with either anxiety or depression, but which was not specified, the results could only be reported narratively. They show no evidence that Reiki is either beneficial or harmful in this population. The risk of bias for the included studies was generally rated as unclear or high for most domains, which reduces the certainty of the evidence.
These studies included subgroups with anxiety and depression as defined by symptom scores and provided data separately for those subgroups. As this included only 25 people with anxiety and 17 with depression and 20 more with either anxiety or depression, but which was not specified, the results could only be reported narratively. They show no evidence that Reiki is either beneficial or harmful in this population. The risk of bias for the included studies was generally rated as unclear or high for most domains, which reduces the certainty of the evidence.
Authors' conclusions: There is insufficient evidence to say whether or not Reiki is useful for people over 16 years of age with anxiety or depression or both.
Similar articles
-
Pharmacotherapy for anxiety and comorbid alcohol use disorders.

Ipser JC, Wilson D, Akindipe TO, Sager C, Stein DJ. Ipser JC, et al. Cochrane Database Syst Rev. 2015 Jan 20;1(1):CD007505. doi: 10.1002/14651858.CD007505.pub2. Cochrane Database Syst Rev. 2015. PMID: 25601826 Free PMC article. Review.
-
Pharmacological interventions for somatoform disorders in adults.
Kleinstäuber M, Witthöft M, Steffanowski A, van Marwijk H, Hiller W, Lambert MJ. Kleinstäuber M, et al. Cochrane Database Syst Rev. 2014 Nov 7;(11):CD010628. doi: 10.1002/14651858.CD010628.pub2. Cochrane Database Syst Rev. 2014. PMID: 25379990 Review.
-
Morita therapy for anxiety disorders in adults.
Wu H, Yu D, He Y, Wang J, Xiao Z, Li C. Wu H, et al. Cochrane Database Syst Rev.
 2015 Feb 19;(2):CD008619. doi: 10.1002/14651858.CD008619.pub2. Cochrane Database Syst Rev. 2015. PMID: 25695214 Review.
2015 Feb 19;(2):CD008619. doi: 10.1002/14651858.CD008619.pub2. Cochrane Database Syst Rev. 2015. PMID: 25695214 Review. -
Psychological therapies for the treatment of post-traumatic stress disorder in children and adolescents (Review).
Gillies D, Taylor F, Gray C, O'Brien L, D'Abrew N. Gillies D, et al. Evid Based Child Health. 2013 May;8(3):1004-116. doi: 10.1002/ebch.1916. Evid Based Child Health. 2013. PMID: 23877914 Review.
-
Effect of Reiki therapy on pain and anxiety in adults: an in-depth literature review of randomized trials with effect size calculations.
Thrane S, Cohen SM. Thrane S, et al. Pain Manag Nurs. 2014 Dec;15(4):897-908. doi: 10.1016/j.pmn.2013.07.008. Epub 2014 Feb 28.
 Pain Manag Nurs. 2014. PMID: 24582620 Free PMC article. Review.
Pain Manag Nurs. 2014. PMID: 24582620 Free PMC article. Review.
See all similar articles
Cited by
-
Impact of spiritual healing on moderate depression in adults: a study protocol of a pilot randomised controlled trial (RCT).
Stub T, Irgens AC, Hansen AH, Knudsen-Baas O, Gåskjenn C, Kristoffersen AE. Stub T, et al. BMJ Open. 2022 Sep 15;12(9):e062683. doi: 10.1136/bmjopen-2022-062683. BMJ Open. 2022. PMID: 36109024 Free PMC article.
-
Stress and Anxiety Reduction Effects of a Reiki Program During the COVID-19 Pandemic Among Employees in Lima, Peru.
Gálvez Escudero D, Reyes-Bossio M. Gálvez Escudero D, et al. Holist Nurs Pract. 2022 Sep-Oct 01;36(5):E48-E56.
 doi: 10.1097/HNP.0000000000000545. Holist Nurs Pract. 2022. PMID: 35981119 Free PMC article.
doi: 10.1097/HNP.0000000000000545. Holist Nurs Pract. 2022. PMID: 35981119 Free PMC article. -
Does Reiki Benefit Mental Health Symptoms Above Placebo?
Zadro S, Stapleton P. Zadro S, et al. Front Psychol. 2022 Jul 12;13:897312. doi: 10.3389/fpsyg.2022.897312. eCollection 2022. Front Psychol. 2022. PMID: 35911042 Free PMC article.
-
Depressive and anxiety symptoms among Japanese cancer survivors: Japan cancer survivorship research project.
Endo M, Matsui K, Akaho R, Mitsui K, Yan Y, Imai Y, Ueda Y, Muto G, Deshpande GA, Terao Y, Takeda S, Saito M, Hayashi K, Nishimura K, Tanigawa T. Endo M, et al. BMC Cancer. 2022 Feb 2;22(1):134. doi: 10.1186/s12885-022-09215-x. BMC Cancer. 2022. PMID: 35109805 Free PMC article.
-
Reiki practitioners' perceptions of the impact of the COVID-19 pandemic on the experience, practice and future of Reiki.
Abdurahman F, Payne N. Abdurahman F, et al. Complement Ther Clin Pract. 2022 Feb;46:101530. doi: 10.1016/j.ctcp.2021.101530. Epub 2021 Dec 30. Complement Ther Clin Pract. 2022. PMID: 34990899 Free PMC article.
See all "Cited by" articles
Publication types
MeSH terms
Reiki Practice: Energy for Healing and Well-Being | Health
Reiki is part of a group of alternative healing therapies based on the use of energy to promote healing and well-being. Widely recognized even in the scientific community as an excellent tool for helping with various physical and emotional processes, it was once born in Japan.
History of Reiki
This therapy is considered by the World Health Organization as an adjunct to other treatments. Used to relieve pain, anxiety, fatigue, depression and improve sleep, Reiki is beneficial in many ways. nine0003
Reiki is a healing technique developed in Japan by Dr. Mikao Usui in the early 20th century. It is believed that it does not cure, but accelerates the healing process.
The roots of the word Reiki come from the combination of "Rei" which means "universal life" and "Ki" which means "energy". According to Reiki masters, those who practice it, the stagnation of energy in the body is associated with injuries, illnesses, stress and other mental illnesses. This means that energy blockade can lead to disease. nine0003
A Reiki session will help release energy for its natural and healthy flow. As a result, it reduces pain and stress and speeds up wound healing.
The value of Reiki therapy
Over the years, the creator of the now famous Reiki method added group values. According to him, the right way of thinking and acting in the world helps to maintain a normal and healthy flow of energy. These meanings are:
According to him, the right way of thinking and acting in the world helps to maintain a normal and healthy flow of energy. These meanings are:
- relationships are our foundation;
- devoted community; nine0024
- intellectual research;
- self-examination deepens understanding;
- service to express gratitude.
Reiki session
Usually a Reiki session takes place in a calm environment, but it is true that the technique can be applied anywhere. Some practitioners also put on soothing music to help the relaxation process.
READ ALSO: How Traditional Chinese Medicine Practices Heal the Human Body and Mind
The therapist uses their hands to apply this technique. Places hands at strategic points of the body for approximately 5 minutes each. The times vary, as the practitioner only changes location when the energy stops flowing. It is through their hands that the energy is transferred to the only person who receives Reiki. It is natural to feel this energy slightly, as the hands of the person undergoing Reiki become warm.
It is natural to feel this energy slightly, as the hands of the person undergoing Reiki become warm.
A session usually takes about one hour. Some therapists choose to start or end a message as a way to improve relaxation, but this is not necessarily part of the treatment. For effective treatment, one to three sessions are recommended. nine0003
Benefits of Reiki
Increases calmness and balance
Reiki has the ability to change energy, improving its flow and enhancing its positive vibrations. Therefore, a person immediately feels calmer, and the mind and body are more balanced.
Reduces depression and anxiety
By promoting balance, Reiki makes emotional moods more stable and promotes the development of positive energy. It has been scientifically proven to reduce depression, although more research is needed. nine0003
This makes it an extremely useful tool as an adjunct to other treatments for depression and anxiety. Many hospitals and medical professionals in the US and Europe are beginning to recommend Reiki, and some hospitals are even offering it to their patients.
Many hospitals and medical professionals in the US and Europe are beginning to recommend Reiki, and some hospitals are even offering it to their patients.
READ ALSO: What is Ayurveda, its elements, energies and doshas
Improves the quality of life of cancer patients. Cancer is one of the most difficult diseases to fight, along with some others. The stress of not knowing how to do it, family stress, and the side effects of treatment can lead to more anxiety, more pain, and more sadness. More and more physicians are advising their patients to take Reiki sessions along the way to help improve mood, hope, and reduce the painful effects of the treatment. The decision to attend Reiki sessions should be discussed with a physician and made with very good professionals who can also explain any effects, sensations and feelings that may come with this technique. nine0003
Improves sleep
By promoting internal balance, sleep is one of the first things that also regulates it. However, in more severe cases of sleep problems, it may be necessary to have Reiki sessions frequently.
However, in more severe cases of sleep problems, it may be necessary to have Reiki sessions frequently.
Helps with back pain
Many people report relief from back pain with Reiki treatment. Since the spine is connected to the flow of energy, and in many cases pain is also associated with anxiety and stress, the positive effects seem to be immediate. However, it should be used in addition to other therapies and exercise, and not on its own. nine0003
Effects of Reiki on Anxiety, Depression, Pain, and Physiological Indicators in the Elderly • Healing Hands
Richeson N., Spross J.A., Lutz K., Peng C. Effects of Reiki on Anxiety, Depression, Pain, and Physiological Factors in Community- Dwelling Older Adults. Research in Gerontological Nursing. 2010 Vol. 3, no. 3.
Summary of The purpose of this study was to evaluate the impact of Reiki as an alternative and complementary treatment approach for older adults who experience pain, depression and/or anxiety. Participants (N = 20) were randomized into an experimental group and a control group (waiting list). Pre- and post-test measures included the Hamilton Anxiety Scale, the Short Form Geriatric Depression Scale, the Pain Scale, and measurements of heart rate and blood pressure. The design of the study included an experimental part to explore the dynamics of quantitative indicators and a descriptive component (semi-structured interviews) to obtain information about the experience of people undergoing Reiki treatment. Significant differences were observed between the experimental and control groups in terms of pain, depression, and anxiety scales; no changes in heart rate and blood pressure were noted. Analysis of the content of the protocols of sessions and interviews revealed five broad categories of responses: relaxation; improved physical symptoms, improved mood and well-being; curiosity and desire to learn more; improving self-care; sensory and cognitive responses to Reiki. nine0003
Participants (N = 20) were randomized into an experimental group and a control group (waiting list). Pre- and post-test measures included the Hamilton Anxiety Scale, the Short Form Geriatric Depression Scale, the Pain Scale, and measurements of heart rate and blood pressure. The design of the study included an experimental part to explore the dynamics of quantitative indicators and a descriptive component (semi-structured interviews) to obtain information about the experience of people undergoing Reiki treatment. Significant differences were observed between the experimental and control groups in terms of pain, depression, and anxiety scales; no changes in heart rate and blood pressure were noted. Analysis of the content of the protocols of sessions and interviews revealed five broad categories of responses: relaxation; improved physical symptoms, improved mood and well-being; curiosity and desire to learn more; improving self-care; sensory and cognitive responses to Reiki. nine0003
Health problems in the elderly
One in five older adults is estimated to have a significant mental health disorder, with depression and anxiety being the most common (Centers for Disease Control and Prevention, & National Association of Chronic Disease Directors, 2008) and 10% to 15% of older adults seek treatment for anxiety (Kennedy-Malone et al.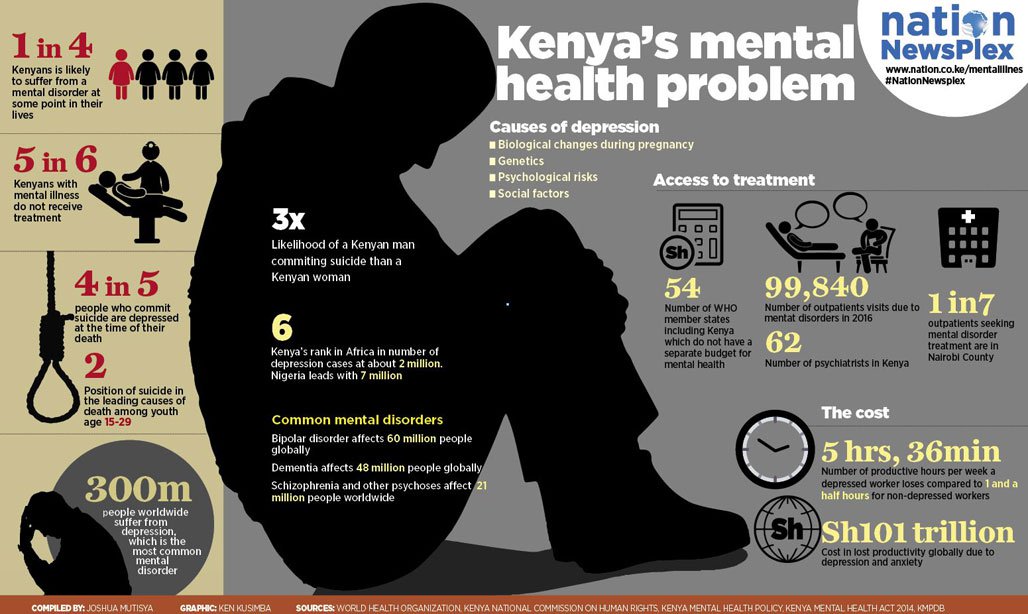 , 2004). In the US, more than one-third of the adult population aged 45 and over report bodily discomfort ranging from severe to severe pain, and more than 80% of the population over 75 suffer from arthritis pain (Kennedy-Malone et al., 2004). A high frequency of chronic diseases accompanied by pain is typical for older people. Kovacs et al report that inadequate pain management can contribute to depression, anxiety, weight loss, sleep disturbances, isolation, and limited mobility (Kovach, Noonan, Griffie, Muchka and Weissman, 2002). Loss of loved ones and reduced functional abilities are additional factors for depression and anxiety in older people (Thorson, 2000). Many older people have several chronic diseases that require constant use of a number of drugs. Evaluation and interpretation of new symptoms is complicated by the fact that people themselves and their physicians conclude that new signs are simply physiological changes in old age. In fact, these may be side effects of the medications taken or the result of their interaction with each other.
, 2004). In the US, more than one-third of the adult population aged 45 and over report bodily discomfort ranging from severe to severe pain, and more than 80% of the population over 75 suffer from arthritis pain (Kennedy-Malone et al., 2004). A high frequency of chronic diseases accompanied by pain is typical for older people. Kovacs et al report that inadequate pain management can contribute to depression, anxiety, weight loss, sleep disturbances, isolation, and limited mobility (Kovach, Noonan, Griffie, Muchka and Weissman, 2002). Loss of loved ones and reduced functional abilities are additional factors for depression and anxiety in older people (Thorson, 2000). Many older people have several chronic diseases that require constant use of a number of drugs. Evaluation and interpretation of new symptoms is complicated by the fact that people themselves and their physicians conclude that new signs are simply physiological changes in old age. In fact, these may be side effects of the medications taken or the result of their interaction with each other. The use of complementary and alternative medicine (CAM) may allow for lower dosages of drugs intended to reduce pain or regulate mood, which in turn will contribute to a reduced risk of adverse reactions. nine0003
The use of complementary and alternative medicine (CAM) may allow for lower dosages of drugs intended to reduce pain or regulate mood, which in turn will contribute to a reduced risk of adverse reactions. nine0003
According to NCCAM (2008), 38% of US adults have used alternative and complementary medicine (CAM) methods. CAM offers an alternative treatment that has a lower risk of unwanted side effects and a new perspective - healing patients, not just seeing them. Older people are interested in complementary and alternative approaches, so it is important that these methods are integrated into the health system. Quality of life should be considered when a person is offered pharmacological or invasive procedures, more medications and medical interventions are not always associated with improved quality of life. Reiki as a healing and preventive method encourages a holistic (mind, body and spirit) approach to health. nine0003
The primary purpose of this pilot study was to evaluate the effects of Reiki on pain, depression, anxiety and/or elevated heart rate (HR) and blood pressure (BP) in elderly people. An additional goal is to understand the benefits of Reiki from a patient's perspective and develop hypotheses for future research.
An additional goal is to understand the benefits of Reiki from a patient's perspective and develop hypotheses for future research.
Literature review
To date, few descriptive or experimental studies have evaluated the efficacy of Reiki for the treatment of pain, depression, anxiety, and physiological indicators such as heart rate and blood pressure in the elderly (Grzywacz et al, 2006). The NCCAM study found that 81.7% of older people who reported depression or anxiety actually used CAM. Interestingly, only 20% of them reported using complementary and alternative methods to restore their mental health. Mix et al (Meeks, Wetherell, Irwin, Redwine, Jeste, 2007) reviewed randomized clinical trials in which CAM approaches have been used to treat depression, anxiety, and sleep disorders in the elderly. Of the 885 identified studies, they selected 33 that had more than 30 subjects, treatment was greater than or equal to 2 weeks, and was published in English. Meeks then rated the scientific quality of these studies using the SASQI scale. They were further classified into positive and negative (showing statistically significant differences between the control and experimental groups at the level of p0.05 or not). It should be noted that the mean value of the quality of studies on the SASQI scale turned out to be higher for studies with a negative result than for studies with a positive result, that is, the former were conducted more strictly. The researchers concluded that CAMs should be further explored due to their wide popularity and the fact that many studies have reported positive results. The authors recommended that future research focus on methodology using robust experimental designs. The authors raised an interesting question about the complexity of CAM studies under Western standards of evaluation, where many subjective factors must be taken into account that affect the patient, treatment and its results. nine0003
Meeks then rated the scientific quality of these studies using the SASQI scale. They were further classified into positive and negative (showing statistically significant differences between the control and experimental groups at the level of p0.05 or not). It should be noted that the mean value of the quality of studies on the SASQI scale turned out to be higher for studies with a negative result than for studies with a positive result, that is, the former were conducted more strictly. The researchers concluded that CAMs should be further explored due to their wide popularity and the fact that many studies have reported positive results. The authors recommended that future research focus on methodology using robust experimental designs. The authors raised an interesting question about the complexity of CAM studies under Western standards of evaluation, where many subjective factors must be taken into account that affect the patient, treatment and its results. nine0003
Reiki and pain
Lee conducted a systematic review of randomized controlled trials to determine whether Reiki can reduce pain Lee (2008). Five randomized controlled trials met the inclusion criteria and were reviewed. Two of these studies reported a statistically significant reduction in pain when Reiki was used in addition to opioid agents, rest, or routine care for the majority (Olson, Hanson, & Michaud, 2003; Vitale, 2007). Assefi et al. (2008) found no significant differences between control and treatment groups in a study of fibromyalgia pain (pain was assessed using a visual analog scale). In Asefi's study, there were 100 subjects divided into 4 groups: Reiki, sham Reiki, remote Reiki, and sham remote Reiki. At the same time, Azefi sought to isolate the influence of Reiki from any other consequences: healers and actors used fictitious names, interacted with participants according to the script, and performed sessions in a room with white walls without incense and music (this is an atypical context for Reiki). In total, each subject received 16 sessions (8 weeks, 2 sessions per week). The authors acknowledged that they did not use the method recommended for Reiki to create an entourage and a comfortable environment.
Five randomized controlled trials met the inclusion criteria and were reviewed. Two of these studies reported a statistically significant reduction in pain when Reiki was used in addition to opioid agents, rest, or routine care for the majority (Olson, Hanson, & Michaud, 2003; Vitale, 2007). Assefi et al. (2008) found no significant differences between control and treatment groups in a study of fibromyalgia pain (pain was assessed using a visual analog scale). In Asefi's study, there were 100 subjects divided into 4 groups: Reiki, sham Reiki, remote Reiki, and sham remote Reiki. At the same time, Azefi sought to isolate the influence of Reiki from any other consequences: healers and actors used fictitious names, interacted with participants according to the script, and performed sessions in a room with white walls without incense and music (this is an atypical context for Reiki). In total, each subject received 16 sessions (8 weeks, 2 sessions per week). The authors acknowledged that they did not use the method recommended for Reiki to create an entourage and a comfortable environment. This study took clinical intervention out of the situation of emotional interpersonal relationships that are considered necessary for the therapeutic relationship in general and for pain management in particular (see, for example, Murinson, Agarwal & Haythornthwaite, 2008). nine0003
This study took clinical intervention out of the situation of emotional interpersonal relationships that are considered necessary for the therapeutic relationship in general and for pain management in particular (see, for example, Murinson, Agarwal & Haythornthwaite, 2008). nine0003
Olson et al. (2003) undertook a study to determine whether Reiki combined with standard opioid pain relievers was more effective in relieving pain in patients with cancer (Olson, Hanson, & Michaud, 2003). The study included twenty-five adults receiving palliative care with a pain rating greater than or equal to 3 on the VAS scale (10-point rating system) and requiring two to five doses of pain relief per day. After one hour of the first afternoon dose of analgesia, the subjects either received a session or simply rested. After a session or rest, the pain was replaced. In addition, daily doses of analgesics were recorded in the diary. A significant reduction in pain was recorded on the first and fourth days of the sessions (a decrease of 1. 2 on the VAS scale compared to 0.3 in the control group, difference p = 0.035). No significant differences were found in the use of pain medications. (Tradition holds that Reiki works on the cause, not on the symptoms, so pain relief is not a primary but a secondary effect in Reiki therapy, which may be delayed. Interestingly, in some cases Reiki did work to reduce pain, note translator). nine0003
2 on the VAS scale compared to 0.3 in the control group, difference p = 0.035). No significant differences were found in the use of pain medications. (Tradition holds that Reiki works on the cause, not on the symptoms, so pain relief is not a primary but a secondary effect in Reiki therapy, which may be delayed. Interestingly, in some cases Reiki did work to reduce pain, note translator). nine0003
Reiki and depression
Shore (2004) examined the long-term effect of energy healing methods on psychological depression and perceptions of stress using standardized scales (two for depression and one for stress). Forty-six participants were randomly assigned to receive Reiki, remote Reiki, or placebo. Participants received one session per week (1 to 1.5 hours) for 6 weeks. The data were analyzed using 3-dimensional analysis of variance. Prior to the start of the group, the three groups did not differ in the values of all 3 scales used. There was a statistically significant reduction (p 0.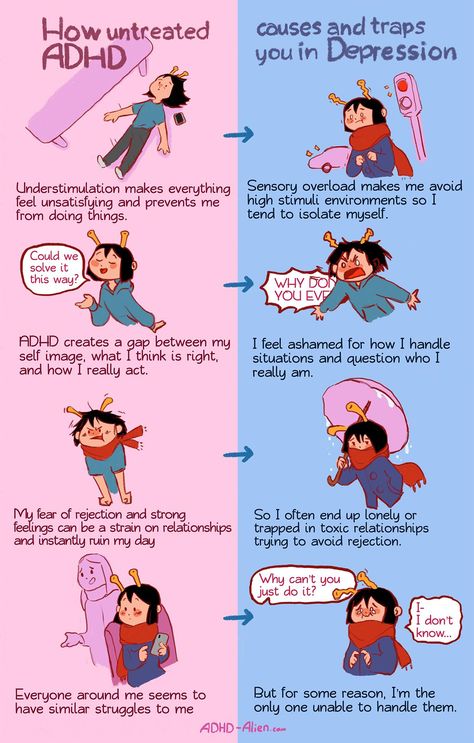 05) in symptoms of depression, perceived stress, hopelessness, and physiological stress in both treatment groups compared with the placebo group. nine0003
05) in symptoms of depression, perceived stress, hopelessness, and physiological stress in both treatment groups compared with the placebo group. nine0003
Reiki and anxiety, blood pressure and other biological correlates
A 2001 study by Wardell and Engebretson (2001) aimed to determine the effects of Reiki therapy on anxiety and physiological measures of stress. Physiological measures included blood pressure, GSR, muscle tension, skin temperature, IgA and cortisol biological parameters. From a biological point of view, it is believed that stress increases cortisol levels, which, in turn, reduces immunocompetence (immunocompetence), which is measured by IgA. There was no control group in this study, all participants received a 3 minute Reiki session. Data were collected before, during and after the session. Anxiety was measured using a standardized scale (STAI), blood pressure was measured with a Dinamap 845 automated cuff, cortisol was measured during salivary radioimmunoassay, and secretory IgA was also obtained from saliva. Anxiety modified by STAI decreased after the session (from 31.96 to 26.17, p = 0.02). Statistical differences were obtained in the level of IgA in saliva, but not in the level of cortisol. Systolic blood pressure decreased statistically significantly during the session (p = 0.003) and remained so until the end of the session. Diastolic pressure did not change significantly. The skin temperature did not change with the beginning of the session, but decreased significantly by the end of it (p = 0.02).
Anxiety modified by STAI decreased after the session (from 31.96 to 26.17, p = 0.02). Statistical differences were obtained in the level of IgA in saliva, but not in the level of cortisol. Systolic blood pressure decreased statistically significantly during the session (p = 0.003) and remained so until the end of the session. Diastolic pressure did not change significantly. The skin temperature did not change with the beginning of the session, but decreased significantly by the end of it (p = 0.02).
In a 2008 study by Baldwin et al. (Baldwin, Wagers, Schwartz, 2008) investigated the effect of Reiki on heart rate and blood pressure (BP) in rats exposed to loud noise. This study was aimed at overcoming the accusation of the subjectivity of CAM methods. Experiments in a strictly controlled laboratory environment were carried out on animals. Three rats were exposed to noise 90dB for 15 minutes a day for 8 days. In a preliminary study, the authors showed that such exposure leads to a statistically significant increase in heart rate and blood pressure (Baldwin, Schwartz, & Hopp, 2007). For the last 5 days of the experiment, the rats received 15 minutes of Reiki before exposure to the noise, as well as during the duration of the noise. The experiment was repeated using dummy Reiki instead. The results showed that Reiki, but not sham Reiki, significantly reduced the resting heart rate in rats (p 0.05) and significantly reduced the increase in heart rate caused by noise exposure (p 0.05). Neither Reiki nor sham Reiki had a significant effect on heart rate. nine0003
For the last 5 days of the experiment, the rats received 15 minutes of Reiki before exposure to the noise, as well as during the duration of the noise. The experiment was repeated using dummy Reiki instead. The results showed that Reiki, but not sham Reiki, significantly reduced the resting heart rate in rats (p 0.05) and significantly reduced the increase in heart rate caused by noise exposure (p 0.05). Neither Reiki nor sham Reiki had a significant effect on heart rate. nine0003
Theoretical basis of the study
The Lazarus and Cohen (1977) model of stress and coping was chosen as the theoretical basis for this project. Lazarus and Cohen noted the role of stress management, coping strategies, and general health, all of which are covered by the practice of interdisciplinary health care. The main emphasis in the model is on the perception of the situation and the choice of a productive coping strategy. Stress is experienced in a situation of interaction between a person and the environment and is determined by the impact of the stress factor on the individual. The response depends on the perception of this stressor and the socio-cultural resources at the person's disposal (Antonovsky & Kats, 1967; Cohen 1984; Lazarus & Cohen, 1977). The theory suggests that if a person is in a suboptimal emotional state (such as depression or anxiety), then they do not adequately assess the potential threat (primary assessment), and also inadequately perceive their resources to cope with this threat (secondary assessment), which leads to ineffective actions (Cohen, 1984). Thus, the Reiki intervention was aimed at helping the subjects cope with their depression, anxiety and pain, which would help to correct their primary and secondary assessment of the situation and make more adequate efforts to cope with stress. nine0003
The response depends on the perception of this stressor and the socio-cultural resources at the person's disposal (Antonovsky & Kats, 1967; Cohen 1984; Lazarus & Cohen, 1977). The theory suggests that if a person is in a suboptimal emotional state (such as depression or anxiety), then they do not adequately assess the potential threat (primary assessment), and also inadequately perceive their resources to cope with this threat (secondary assessment), which leads to ineffective actions (Cohen, 1984). Thus, the Reiki intervention was aimed at helping the subjects cope with their depression, anxiety and pain, which would help to correct their primary and secondary assessment of the situation and make more adequate efforts to cope with stress. nine0003
Method
Study design
An experiment was conducted to evaluate the effect of Reiki on pain, depression and anxiety in the elderly. In addition, heart rate and blood pressure were measured at baseline, before and after each treatment, and at the end of the study. In addition, face-to-face semi-structured interviews were conducted to analyze participants' experiences. Similar interviews were conducted with the control group (waiting list). These interviews were analyzed using the content analysis method. nine0003
In addition, face-to-face semi-structured interviews were conducted to analyze participants' experiences. Similar interviews were conducted with the control group (waiting list). These interviews were analyzed using the content analysis method. nine0003
Discussion of results and recommendations
Quantitative indicators showed significant improvements in the scales of pain, depression and anxiety in the experimental group, confirmed by qualitative data. There were no statistically significant results in heart rate and blood pressure. This is not surprising, since the majority of participants (85.5%) were not in the high risk group for AD and all participants were within the normal range for admission to the study. These results are consistent with Shore's (2004) data on reduction in psychological stress and Olson et al (Olson, Hanson, & Michaud, 2003) on pain reduction in the Reiki plus opioid medication group compared to the medication plus rest group. This is also consistent with the anxiety reduction results reported by Wardell and Engebretson (2001) and Baldwin et al. (Baldwin et al., 2008). Qualitative evidence suggests that Reiki may have the potential to improve health and shift to a more optimal (resource-saving) mode of functioning, which requires further study. nine0003
This is also consistent with the anxiety reduction results reported by Wardell and Engebretson (2001) and Baldwin et al. (Baldwin et al., 2008). Qualitative evidence suggests that Reiki may have the potential to improve health and shift to a more optimal (resource-saving) mode of functioning, which requires further study. nine0003
One of the key findings of the qualitative research is the widespread reports of relaxation during and after Reiki. This is consistent with the authors' experience with the use of Reiki and progressive muscle relaxation in the clinical setting. Another interesting result of the qualitative data was that many participants (with the exception of a few) reported that the relaxing effect of the sessions persisted after they ended. The comments of some participants suggest that the effect of Reiki is cumulative. These findings are important for future research. nine0003
Relaxation has long been recognized as an effective intervention for insomnia and chronic pain (National Institutes of Health Technology Assessment Panel on Integration of Behavioral and Relaxation Approaches into the Treatment of Chronic Pain and Insomnia, 1996). There is evidence that relaxation may be useful in the treatment of depression, but a systematic review of this evidence suggests that further research is needed (Jorm, Morgan, & Hetrick, 2008). Two meta-analyses have shown that relaxation reduces anxiety (Manzoni, Pagnini, Castelnuovo, Molinari, 2008; Thorp et al., 2009). It is possible that Reiki provides a therapeutic effect through deep relaxation. If this is the case, then Reiki research would correlate with the classical research of Benson, author of the Relaxation Response Model (1975, 2000), widely recognized for its pioneering research in psychophysiology and health (see, for example, Benson, 1979, 1984; Esch, Stefano , Fricchione, & Benson, 2002; Galvin, Benson, Deckro, Fricchione, & Dusek, 2006; Peters, Benson, & Porter, 1977). Benson (2000) notes that progressive muscle relaxation, meditation, and prayer have similar physiological and cognitive effects. A pilot study on Relaxation Response learning in a sample of healthy older adults demonstrated a statistically significant improvement over a simple attention task (Galvin et al.
There is evidence that relaxation may be useful in the treatment of depression, but a systematic review of this evidence suggests that further research is needed (Jorm, Morgan, & Hetrick, 2008). Two meta-analyses have shown that relaxation reduces anxiety (Manzoni, Pagnini, Castelnuovo, Molinari, 2008; Thorp et al., 2009). It is possible that Reiki provides a therapeutic effect through deep relaxation. If this is the case, then Reiki research would correlate with the classical research of Benson, author of the Relaxation Response Model (1975, 2000), widely recognized for its pioneering research in psychophysiology and health (see, for example, Benson, 1979, 1984; Esch, Stefano , Fricchione, & Benson, 2002; Galvin, Benson, Deckro, Fricchione, & Dusek, 2006; Peters, Benson, & Porter, 1977). Benson (2000) notes that progressive muscle relaxation, meditation, and prayer have similar physiological and cognitive effects. A pilot study on Relaxation Response learning in a sample of healthy older adults demonstrated a statistically significant improvement over a simple attention task (Galvin et al. , 2006), as well as a reduction in overall anxiety.
, 2006), as well as a reduction in overall anxiety.
This discovery sets important directions for further research. NCCAM characterizes Reiki as an energy medicine method that is a non-invasive complementary or alternative therapy. If relaxation is one of the responses to Reiki, then future research could build on the vast amount of existing research evaluating the physiological and cognitive effects of relaxation. If Reiki provides a different strategy for responding to stress, including negative physical and emotional states, then future research should test this and compare Reiki therapy with relaxation training to determine how they are similar to each other. Research comparing sessions to self and partner sessions, as well as studies comparing sessions given by working and non-clinical healers, will contribute to the understanding of the benefits of Reiki in both the clinical and "community" formats. nine0003
In addition, future research should have a theoretical basis. The study of Reiki versus sham Reiki per 100 subjects with fibromyalgia (Assefi et al., 2008) had no theoretical basis. Renowned researchers in pain (Dalton & Blau, 1996) and CAM (Astin, Shapiro, Eisenberg, and Forys, 2003) advocate the importance of a theoretical framework in the design, implementation, and interpretation of research results. Astin et al. (2003) note that "despite the widespread acceptance and support of the biopsychosocial model, psychosocial factors continue to be overlooked or overlooked in clinical research" (p. 131). nine0003
The study of Reiki versus sham Reiki per 100 subjects with fibromyalgia (Assefi et al., 2008) had no theoretical basis. Renowned researchers in pain (Dalton & Blau, 1996) and CAM (Astin, Shapiro, Eisenberg, and Forys, 2003) advocate the importance of a theoretical framework in the design, implementation, and interpretation of research results. Astin et al. (2003) note that "despite the widespread acceptance and support of the biopsychosocial model, psychosocial factors continue to be overlooked or overlooked in clinical research" (p. 131). nine0003
Conclusion
The small and voluntary nature of the sample may indicate biased results. It can be assumed that such people have a prior willingness to treat pain, depression or anxiety using additional methods, which threatens the internal validity of the project and the generalization of its results. Confounding variables such as the music used in the Reiki sessions and the therapeutic contact with the research team during the interviews may also have contributed to symptom relief. So, given the design of the study, it is not possible to judge whether Reiki exposure was the primary independent variable. However, many efforts were put into the study, including the use of a mixed method of data collection and analysis (qualitative-quantitative), treatment in an individualized form based on the needs of the participants, and the collection of an interdisciplinary research team. nine0003
So, given the design of the study, it is not possible to judge whether Reiki exposure was the primary independent variable. However, many efforts were put into the study, including the use of a mixed method of data collection and analysis (qualitative-quantitative), treatment in an individualized form based on the needs of the participants, and the collection of an interdisciplinary research team. nine0003
Recommendations for future research include the continued use of qualitative data to shed light on the supposed benefits of Reiki, the health problems that can be addressed in this way, and the conditions under which these improvements occur. Qualitative research must have a rigorous methodology and theoretical foundations, consider a biopsychosocial context, and involve recipients and Reiki practitioners. In addition, research may reveal similarities and differences between Reiki and relaxation, and research that will assess the impact of contextual factors on Reiki treatment is needed to determine the role of Reiki in alleviating physical and mental symptoms. nine0003
nine0003
References
- American Geriatrics Society Panel on Persistent Pain in Older Persons. (2002). The management of persistent pain in older persons. Journal of the American Geriatrics Society, 50. Retrieved from http://www.americangeriatrics.org/products/positionpapers/ JGS5071.pdf
- Antonovsky, A., & Kats, R. (1967). The life crisis history as a tool in epidemiologic research. Journal of Health and Social Behavior, 8, 15-20.
- Assefi, N., Bogart, A., Goldberg, J., & Buchwald, D. (2008). Reiki for the treatment of fibromyalgia: A randomized controlled trial. Journal of Alternative and Complementary Medicine, 14, 1115-1122. nine0024
- Astin, J.A., Shapiro, S.L., Eisenberg, D.M., & Forys, K.L. (2003). Mind-body medicine: State of the science, implications for practice. Journal of the American Board of Family Practice, 16, 131-147.
- Baldwin, A., Wagers, C., & Schwartz, G. (2008). Reiki improves heart rate homeostasis in laboratory rats.
 Journal of Alternative and Complementary Medicine, 14, 417-422.
Journal of Alternative and Complementary Medicine, 14, 417-422. - Baldwin, A.L., Schwartz, G.E., & Hopp, D.H. (2007). Are investigators aware of environmental noise in animal facilities and that such noise may affect experimental data? Journal of the American Association for Laboratory Animal Science, 46, 45-51. nine0024
- Benson, H. (1975). The response relaxation. New York: Morrow.
- Benson, H. (1979). The mind/body effect. New York: Simon and Schuster.
- Benson, H. (1984). Beyond the response relaxation. New York: Times Books.
- Benson, H. (2000). The response relaxation updated and expanded (25th anniversary ed.). New York: Avon.
- Bieri, D., Reeve, R.A., Champion, G.D., Addicoat, L., & Ziegler, J.B. (1990). The Faces Pain Scale for the self-assessment of the severity of pain experienced by children: Development, initial validation, and preliminary investigation for ratio scale properties. Pain, 41, 139-150.
- Buettner, L.
 , & Fitzsimmons, S. (2003). Dementia practice guidelines for recreational therapy: Treating disturbing behaviors. Alexandria, VA: American Therapeutic Recreation Association.
, & Fitzsimmons, S. (2003). Dementia practice guidelines for recreational therapy: Treating disturbing behaviors. Alexandria, VA: American Therapeutic Recreation Association. - Centers for Disease Control and Prevention, & National Association of Chronic Disease Directors. (2008). The state of mental health and aging in America. Issue brief 1: What do the data tell us? Retrieved from http://www.cdc.gov/aging/pdf/mental_health.pdf
- Cohen, F. (1984). Coping. In J.D. Matarazzo, S.M. Weiss, J.A. Herd, N.E. Miller, & S.M. Weiss (Eds.), Behavioral health: A handbook of health enhancement and disease prevention (pp. 3-40). New York: Wiley and Sons.
- Dalton, J., & Blau, W. (1996). Changing the practice of pain management: An examination of the theoretical basis of change. Pain Forum, 5, 266-272.
- Diefenbach, G.J., Stanley, M.A., Beck J.G., Novy, D.M., Verill, P., & Swann, A.C. (2001). Examination of the Hamilton Scales in assessment of anxious adults: A replication and extension.
 Journal of Psychopathology and Behavioral Assessment, 23, 117-127. nine0024
Journal of Psychopathology and Behavioral Assessment, 23, 117-127. nine0024 - Esch, T., Stefano, G. B., Fricchione, G. L., & Benson, H. (2002). The role of stress in neurodegenerative diseases and mental disorders. Neuro Endocrinology Letters, 23, 199-208.
- Gallo, J.J., & Lebowitz, B.D. (1999). The epidemiology of common late-life mental disorders in the community: Themes for the new century. Psychiatric Services, 50, 1158-1166.
- Galvin, J.A., Benson, H., Deckro, G.R., Fricchione, G.L., & Dusek, J.A. (2006). The response relaxation: Reducing stress and improving cognition in healthy aging adults. Complementary Therapies in Clinical Practice, 12, 186-191.
- Grzywacz, J.G., Suerken, C.K., Quandt, S.A., Bell, R.A., Lang, W., & Arcury, T.A. (2006). Older adults’ use of complementary and alternative medicine for mental health: Findings from the 2002 National Health Interview Survey. Journal of Alternative and Complementary Medicine, 12, 467-473.
- Hamilton, M.
 (1959). The assessment of anxiety states by rating. British Journal of Medical Psychology, 3, 50-55.
(1959). The assessment of anxiety states by rating. British Journal of Medical Psychology, 3, 50-55. - Herr, K. (2002). Chronic pain: Challenges and assessment strategies. Journal of Gerontological Nursing, 28(1), 20-27. nine0024
- Herr, K.A., Mobily, P.R., Kohout, F.J., & Wagenaar, D. (1998). Evaluation of the Faces Pain Scale for use with the elderly. Clinical Journal of Pain, 14(1), 29-38.
- Herron-Marx, S., Price-Knol, F., Burden, B., & Hicks, C. (2008). A systematic review of the use of reiki in health care. Alternative and Complementary Therapies, 14, 37-42.
- Hollander, M., & Wolfe, D.A. (1999). Nonparametric statistical methods (2nd ed.). New York: Wiley and Sons. nine0024
- Jorm, A.F., Morgan, A.J., & Hetrick, S.E. (2008). Relaxation for depression (Article No. CD007142). Cochrane Database of Systematic Reviews, Issue 4.
- Kennedy-Malone, L., Fletcher, K., & Plank, L. (2004). Management guidelines for nurse practitioners working with older adults (2nd ed.
 ). Philadelphia: Davis.
). Philadelphia: Davis. - Khechog, N. (2005). Music as medicine [CD]. Louisville, CO: Sounds True.
- Kovach, C.R., Noonan, P.E., Griffie, J., Muchka, S., & Weissman, D.E. (2002). The assessment of discomfort in dementia protocol. Pain Management Nursing, 3, 16-27. nine0024
- Kvale, S. (1996). Interviews: An introduction to qualitative research interviewing. Newbury Park, CA: Sage.
- Lazarus, R.S., & Cohen, J.B. (1977). environmental stress. In I. Altman & J.F. Wohlwill (Eds.), Human behavior and environment (Vol. 2, pp. 90-127). New York: Plenum.
- Lee, M. (2008). Is reiki beneficial for pain management? Focus on Alternative and Complementary Therapies, 13, 78-81.
- Lee, M., Pittler, H., & Ernst, E. (2008). Effects of reiki in clinical practice: A systematic review of randomized clinical trials. Journal of Clinical Practice, 62, 947-954.
- Manzoni, G. M., Pagnini, F., Castelnuovo, G., & Molinari, E. (2008). Relaxation training for anxiety: A ten-year systematic review with meta-analysis.
 BMC Psychiatry, 8, 41-53.
BMC Psychiatry, 8, 41-53. - Maxwell, A.E. (1970). Comparing the classification of subjects by two independent judges. British Journal of Psychiatry, 116, 651-655.
- McCaffery, M., & Pasero, C. (1999). Pain: Clinical manual (2nd ed.). St. Louis: Mosby.
- McNamara, C. (n.d.). General guidelines for conducting interviews. Retrieved from the Free Management Library website: http://www. managementhelp.org/evaluatn/intrview.htm nine0024
- Meeks, T., Wetherell, J., Irwin, M., Redwine, L., & Jeste, D. (2007). Complementary and alternative treatments for late-life depres- sion, anxiety, and sleep disturbance: A review of randomized controlled trials. Journal of Clinical Psychiatry, 68, 1461-1471.
- Murinson, B.B., Agarwal, A.K., & Haythornthwaite, J.A. (2008). Cognitive expertise, emotional development, and reflective capacity: Clinical skills for improved pain care. Journal of Pain, 9, 975-983.
- National Center for Complementary and Alternative Medicine.
 (2007). What is CAM? Retrieved from http://nccam.nih.gov/health/whatiscam/overview.htm
(2007). What is CAM? Retrieved from http://nccam.nih.gov/health/whatiscam/overview.htm - National Center for Complementary and Alternative Medicine. (2008). The use of complementary and alternative medicine in the United States. Retrieved from http://nccam.nih.gov/news/camstats/2007/camsurvey_fs1.htm
- National Institutes of Health Technology Assessment Panel on Integration of Behavioral and Relaxation Approaches into the Treatment of Chronic Pain and Insomnia. (nineteen96). Integration of behavioral and relaxation approaches into the treatment of chronic pain and insomnia. Journal of the American Medical Association, 276, 313-318.
- Olson, K., Hanson, J., & Michaud, M. (2003). Other complementary therapies, reiki effects on pain and quality of life in advanced cancer patients. Journal of Pain and Symptom Management, 26, 990-997.
- Peters, R.K., Benson, H., & Porter, D. (1977). Daily relaxation re-sponse breaks in a working population: Effects on self-reported measures of health, performance, and well-being.
 American Journal of Public Health, 67, 946-953.
American Journal of Public Health, 67, 946-953. - Rand, W.L. (2005). The reiki touch workbook. Louisville, CO: Sounds True.
- Shore, A. (2004). Long-term effects of energetic healing on symptoms of psychological depression and self-perceived stress. Alternative Therapies, 10(3), 42-48.
- Effects of Reiki Stein, D. (1995). Essential reiki: A complete guide to an ancient healing art. New York: Ten Speed Press.
- Stuart, A. (1955). A test for homogeneity of the marginal distributions in a two-way classification. Biometrika, 42, 412-416. nine0024
- Sun, X., & Yang, Z. (2008). Generalized McNemar's test for homogeneity of the marginal distributions. Retrieved from the SAS website: http://www2.sas.com/proceedings/forum2008/382-2008.pdf
- Thorp, S.R., Ayers, C.R., Nuevo, R., Stoddard, J.A., Sorrell, J.T., & Wetherell, J.L. (2009). Meta-analysis comparing different behavioral treatments for late-life anxiety. American Journal of General Psychiatry, 17, 105-115.

Learn more