A key feature of the mmpi 2 is that
Minnesota Multiphasic Personality Inventory - StatPearls
Augustus E. Floyd; Vikas Gupta.
Author Information
Last Update: April 28, 2022.
Definition/Introduction
The Minnesota Multiphasic Personality Inventory (MMPI) is the most common psychometric test devised to assess personality traits and psychopathology. This data can be used to draw conclusions about the test taker’s psychopathy or to interpret psychological characteristics compared to the norm.[1] The most common treatment application of the test by providers is establishing or reevaluating care for an ambiguous clinical picture.[2] For psychiatric management, this aids in creating generalizable data relevant to a plethora of possible conditions.[1][2]
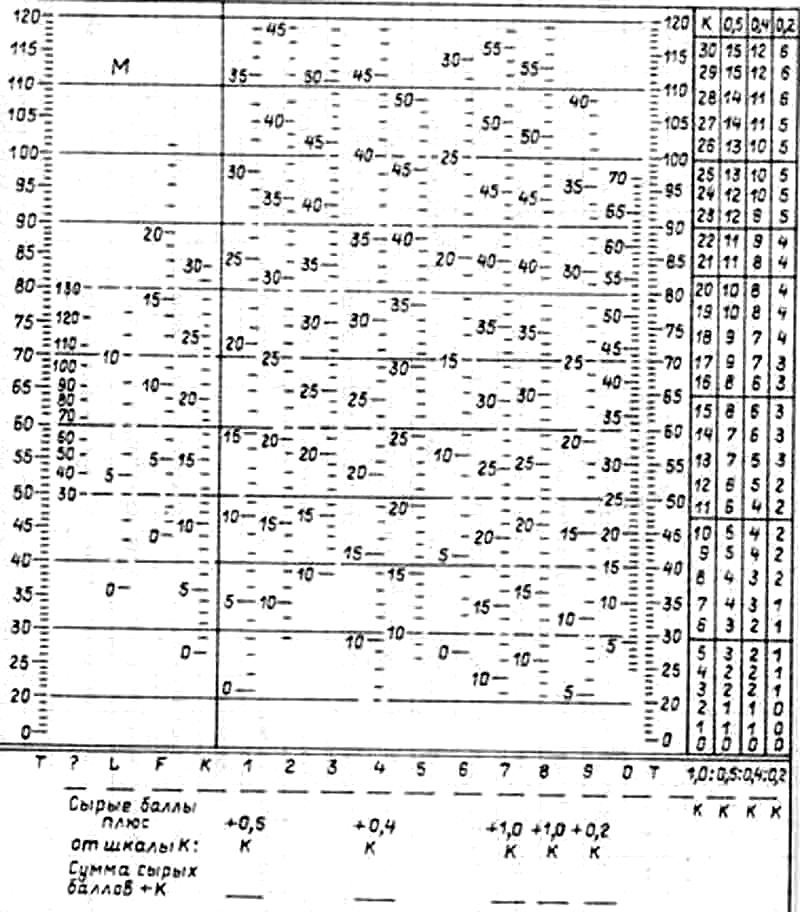
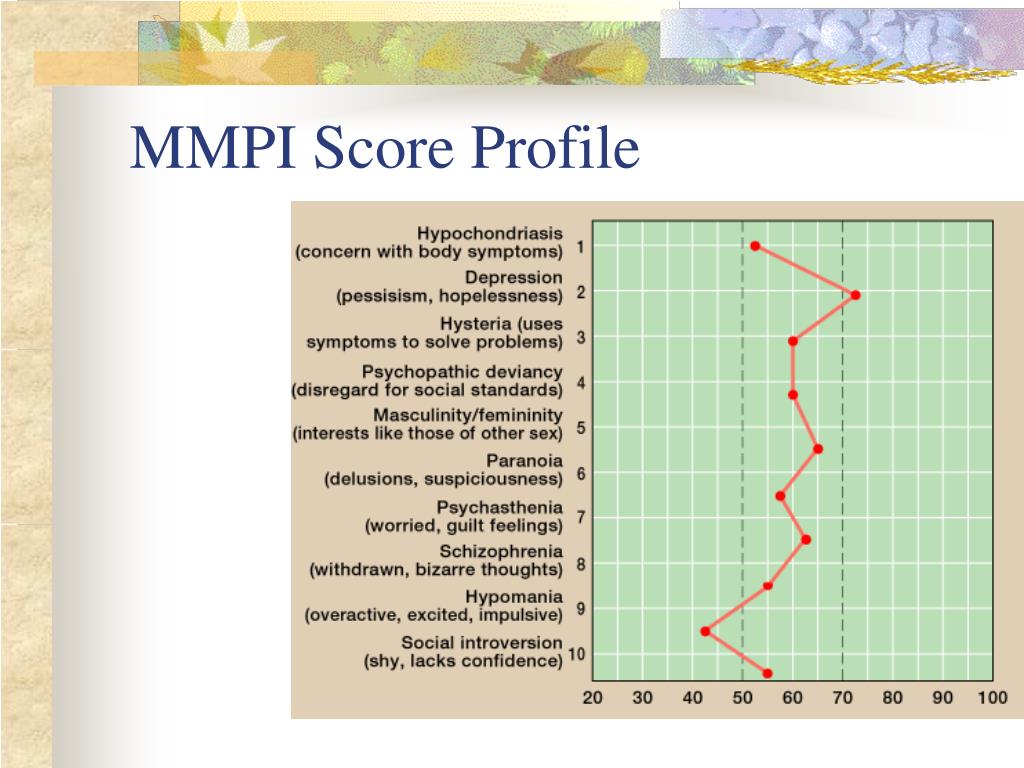
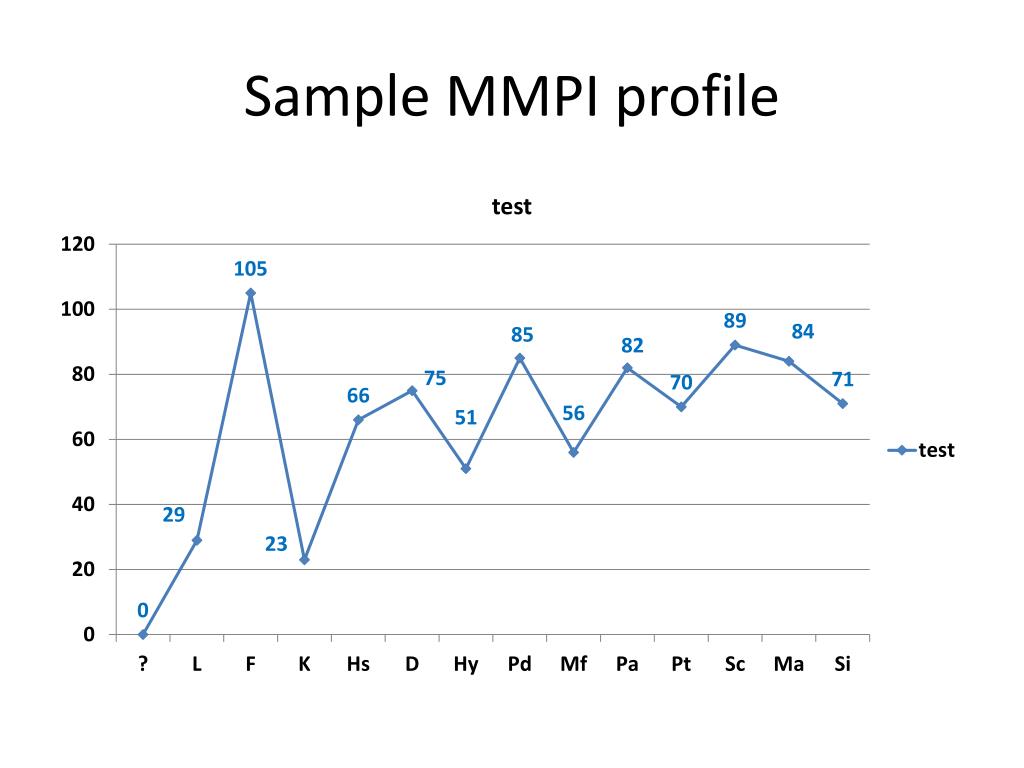
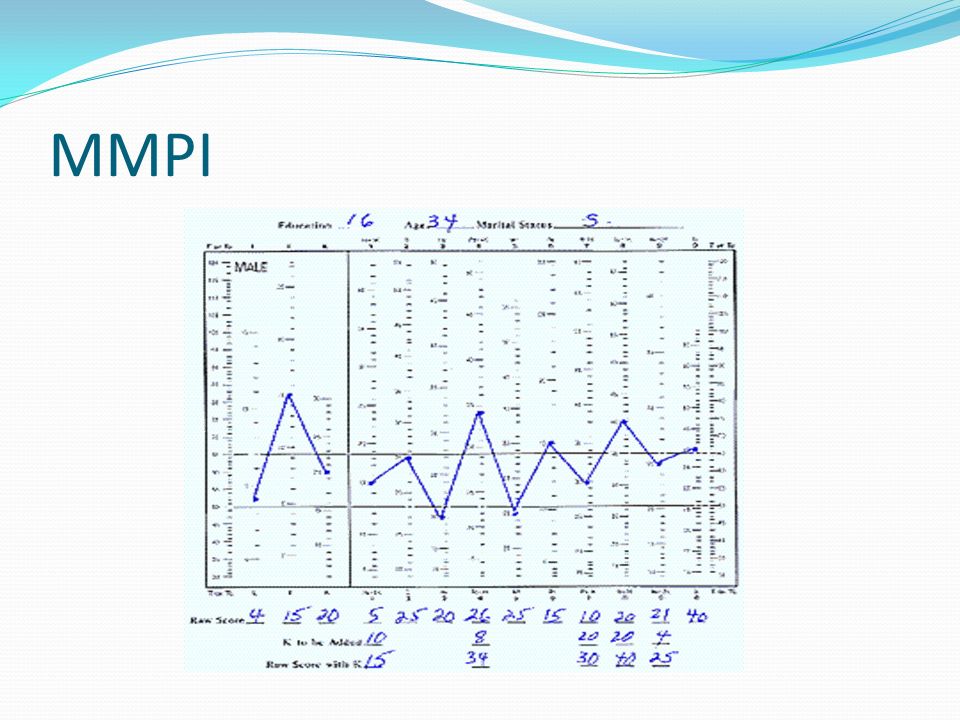
The MMPI was developed in the 1930s and published through the University of Minnesota in 1942 by Stuart Hathaway and Charley McKinley using visitors of patients at the University of Minnesota hospital as a base sample in both theorizing constructs of psychiatric illness and fielding the instrument. Testing is administered through 567 true or false items using a booklet with an accompanying answer sheet. The responses are then hand-scored and plotted on an X-Y graph; a separate version is used for male and female respondents.[3]
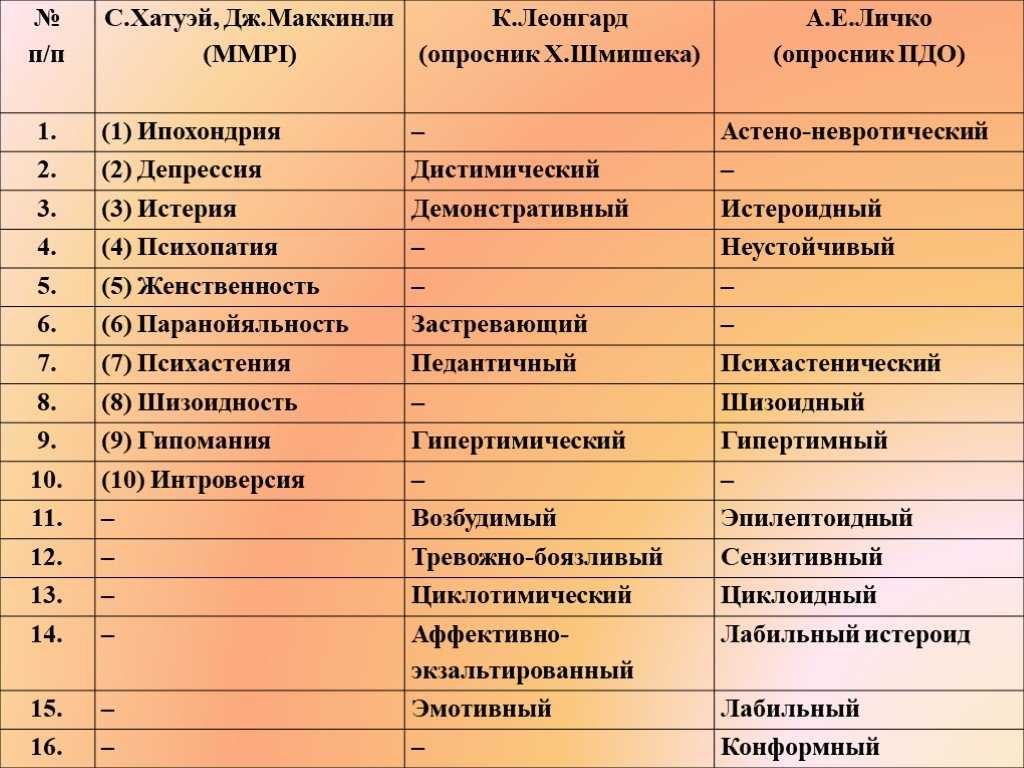
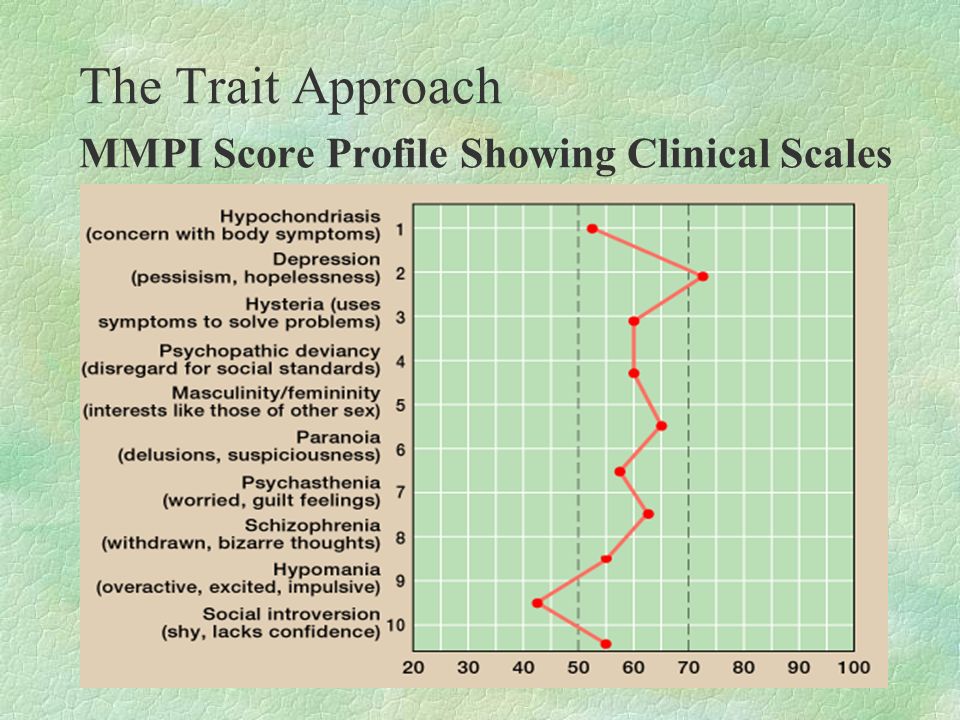
The X-axis is comprised of 14 scales. The first four ‘content scales’ judge the validity of the test attempt and include:
? to represent the number of questions completed incorrectly, either with no attempt or both ‘true’ and ‘false’ selected
L for ‘Lie’ to represent an attempt by the respondent to misrepresent themselves in a more positive light
F or ‘frequency’ to gauge random response as well as the respondent’s exaggeration or downplaying of symptoms
K to gauge ‘defensiveness,’ or evasion of stressful content
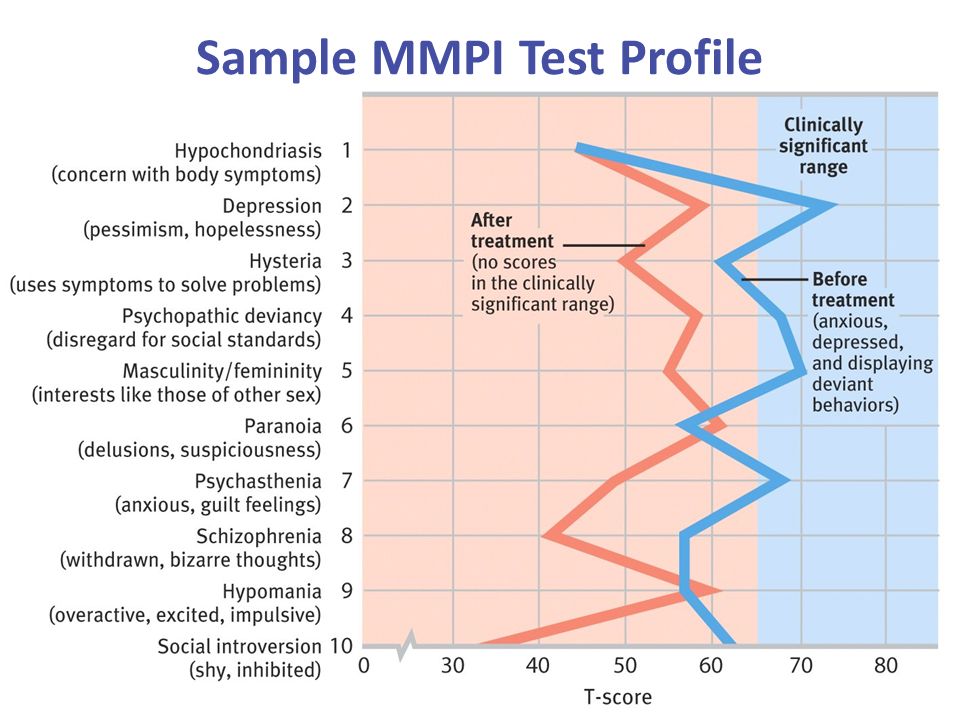
The 10 remaining scales known as ‘clinical scales’ are designed to measure for the presence of psychiatric syndromes, including:
1 or ‘Hs’ for hypochondriasis
2 or ‘D’ for depression
3 or ‘Hy’ for hysteria
4 or ‘Pd’ for psychopathic deviate
5 or ‘Mf’ for the continuum of masculinity-femininity
6 or ‘Pa’ for paranoia
7 or ‘Pt’ for psychasthenia or obsessive-compulsive tendency
8 or ‘Sc’ for schizophrenia
9 or ‘Ma’ for mania
0 or ‘Si’ for social introversion.

The Y-axis statistically standardizes the grading received on each scale in a range of T-scores from 0 to 120. A mean score is 50, and 82% of respondents are considered the normal population falling between 30 and 70. A T-score greater than 70 indicates psychopathy in that category.
Issues of Concern
The existence of the MMPI has been concurrent with vast reforms in societal convention and increased understanding of behavioral health.[3] Likewise, the instrument has been adapted to reflect such changes. Overarching criticisms to the original test center on its disparity in addressing psychopathy in social and ethnic minorities.[1] This has been attributed to the original sample being a small group, mainly consisting of young rural Caucasian subjects from the Midwestern United States.[4] Studies have established biases in which misunderstanding or failure to identify with the content of questions culturally has led to underreporting or overreporting mental illness. [5][1]
[5][1]
These shortcomings led to the release of the MMPI-2 by James N. Butcher, W. Grant Dahlstrom, John R. Graham, Auke Tellegen, and Beverly Kaemme in 1989.[6] This assessment retains the original total of 567 items with the same corresponding 14 scales with the original number of questions from the test.[6] Test items were revised based upon a larger and more diverse sample size of 2600 attuned to a 6th-grade reading level.[6] Gendered differences were replaced with a nongendered standardized scoring.[6] Despite further advancements, the MMPI-2 is still the most commonly administered version and has been translated into over 40 languages.[1]
In 2003, 9 restructured clinical or ‘RC’ scales were introduced as a prospective replacement for the original clinical scales.[1] These include:
RCd, or ‘demoralization’ – misery or depression
RC1 or ‘somatic complaints, – the fixation on bodily symptoms of illness or somatization
RC2 or ‘low positive emotions’ – weakened positivity, lack of enjoyment
RC3 or ‘cynicism’ – low regard for the merit of others and their actions
RC4 or ‘antisocial behavior’ – selfish and sociopathic conduct
RC6 or ‘ideas of persecution’ – belief in the malintent of others toward oneself
RC7 or ‘dysfunctional negative emotions’ – experiences on a spectrum of anxiety and irritability
RC8 or ‘aberrant experiences’ – uncommon beliefs or interpretation of experiences
RC9 or ‘hypomanic activation’ – energetic drive and desire for exertion
The RC scales were devised to provide a streamlined interpretation and less overlap with an increased focus on the growth in understanding within psychiatry over the past 70 years.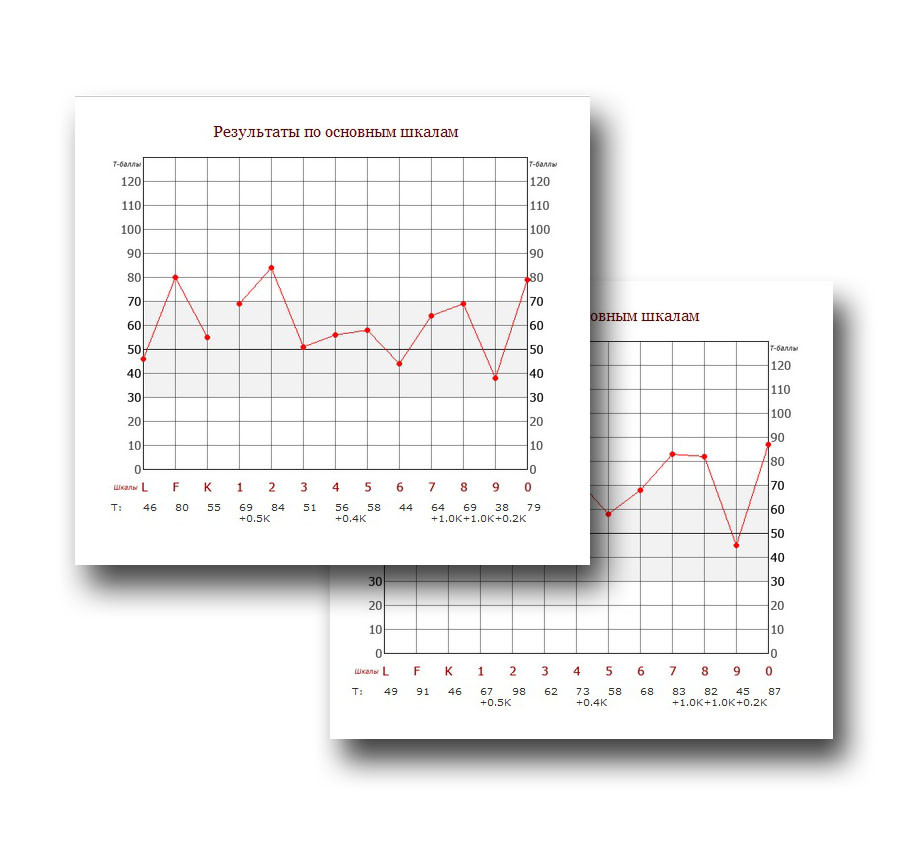 Combinations of high-scoring categories represent distinct psychiatric constructs rather than the nebulous findings of the original clinical scales tying the patient to a specific diagnosis. Arguments also exist that this information is limited in that it categorizes the responder rather than providing data on an individual patient within a personalized spectrum of behavior.[1]
Combinations of high-scoring categories represent distinct psychiatric constructs rather than the nebulous findings of the original clinical scales tying the patient to a specific diagnosis. Arguments also exist that this information is limited in that it categorizes the responder rather than providing data on an individual patient within a personalized spectrum of behavior.[1]
The RC scales were incorporated into the most current form of the MMPI, known as the Minnesota Multiphasic Personality Inventory-2 Revised Form, or the MMPI-2-RF, which was released in 2008 by Yossef Ben-Porath and Auke Telleger of the University of Minnesota. The MMPI-2-RF is composed of 338 items measured by 51 scales broken into 9 validity scales, 3 higher-order scales, the 9 RC scales, 23 specific problem scales, 2 interest scales, and 5 revised personality psychopathy scales.[1]
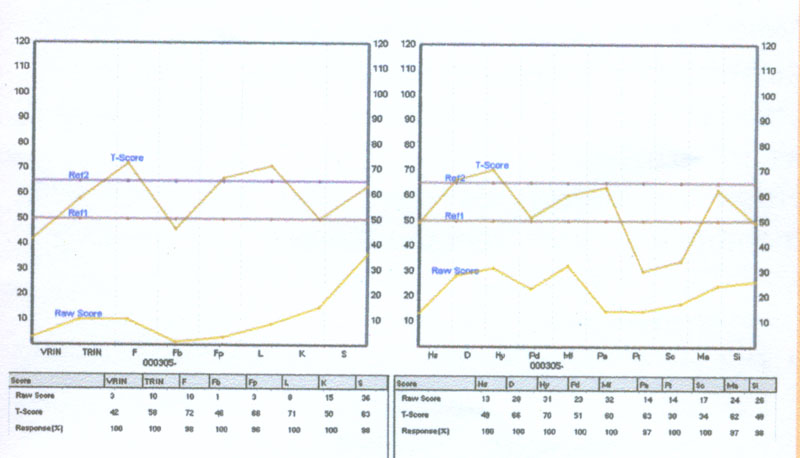
The 9 validity scales assess incongruent answering or deceptive test-taking and include:
VRIN-r or ‘variable response inconsistency’ – inconsistent reporting of items
TRIN-r or ‘true response inconsistency’ careless reporting of items
F-r or ‘infrequent responses,’ – overreporting of infrequent responses compared to the norm
Fp-r or ‘infrequent psychopathology responses’ – overreporting of infrequent responses compared to those with psychopathy
Fs or ‘infrequent somatic responses’ – overreporting of infrequent responses compared to medical patients
FBS-r or ‘symptom validity’ – overreporting of nonvalid symptoms compared to both physical and mental standard symptomology
RBS or ‘response bias’ – overreporting associated with a statistically invalidated presentation of the disease
L-r or ‘uncommon virtues’ – underreporting through infrequently declared values or actions
K-r or ‘adjustment validity’ – underreporting by tailoring answers to give the impression of healthy psychological adjustment
The 3 higher-order scales broadly categorize psychopathic presentation and include:
EID or ‘emotional/internalizing dysfunction’ – problems concerning mood and affect
THD or ‘thought dysfunction’ – problems concerning disorganization of thought
BXD or ‘behavioral/external dysfunction’ – problems concerning impulsive or inappropriate behavior
The problem scales highlight responses consistent with the presence of specific psychopathic and psychosomatic presentations and include:
MLS or ‘malaise’
GIC or ‘gastrointestinal complaints’
HPC or ‘head pain complaints'
NUC or ‘neurological complaints’
COG or ‘cognitive complaints’
SUI or ‘suicidal/death ideation’
HLP or ‘helplessness/hopelessness’
SFD or ‘self-doubt’
NFC or ‘inefficacy’
STW or ‘stress/worry’
AXY or ‘anxiety’
ANP or ‘anger proneness’
BRF or ‘behavior-restricting fears’
MSF or ‘multiple specific fears’
JCP or ‘juvenile conduct problems’
SUB or ‘substance abuse’
AGG or ‘aggression’
ACT or ‘activation’
FML or ‘family problems’
IPP or ‘interpersonal passivity’
SAV or ‘social avoidance’
SHY or ‘shyness’
DSF or ‘disaffiliativeness’
The interest scales are designed to assess cognitive skills, aptitude, and learning preferences which include:
AES or aesthetic-literary interests – pursuits related to fine art
MEC or mechanical-physical interests – pursuits related to kinesthetic activities
The revised personality/psychopathology five scales are based on 107 distinct items and include:
AGG-r or ‘aggressiveness-revised’ – preference for excess and antagonism
PSYCH-r or ‘psychoticism-revised’ – preference for disconnection from reality
DISC-r or ‘disconstraint-revised’ – preference for impulsion and compulsion
NEGE-r or ‘negative emotionality/neuroticism-revised’ – preference for anxiety
INTR-r or ‘introversion/low positive emotional-revised’ – flat affect and timidity
It has been suggested that while the MMPI-2-RF has many additional metrics, the reduction in question number limits the amount of information about psychiatric diseases to about 60% of the original test. There has also been considerable debate over whether the new metrics are inaccurate in detecting psychopathy.[1] In separating genuine psychopathy from attempts to feign a diagnosis for personal incentive, some studies have noted the new validity scales to be overly sensitive to overreporting symptoms to achieve a specific result. It has conversely been found that the L-r and K-r scales are particularly reliable at detecting underreporting of mental illness.[7][8] Overall, literature has supported the MMPI-2-RF in identifying the accuracy of reporting psychiatric information in those who complete it.[1]
There has also been considerable debate over whether the new metrics are inaccurate in detecting psychopathy.[1] In separating genuine psychopathy from attempts to feign a diagnosis for personal incentive, some studies have noted the new validity scales to be overly sensitive to overreporting symptoms to achieve a specific result. It has conversely been found that the L-r and K-r scales are particularly reliable at detecting underreporting of mental illness.[7][8] Overall, literature has supported the MMPI-2-RF in identifying the accuracy of reporting psychiatric information in those who complete it.[1]
Clinical Significance
The MMPI maintains an enduring presence in the field of mental health, and its current adaption has been widely evaluated by the standard of modern behavioral health practices.[1] It continues to receive widespread application as a threshold of determining the presence of psychopathy, as a means of constructing a differential diagnosis for mental health problems, and as a versatile test to achieve transferrable psychological data. These data points indicate a category, which gives behavioral health professionals a starting point to explore plausible diagnoses and initiate appropriate treatment. Completion may also offer therapeutic benefits to patients in reflecting upon their issues and improving personal understanding of their psychology.[3]
These data points indicate a category, which gives behavioral health professionals a starting point to explore plausible diagnoses and initiate appropriate treatment. Completion may also offer therapeutic benefits to patients in reflecting upon their issues and improving personal understanding of their psychology.[3]
In addition to its predominant clinical application, an extensive body of research exists to assess the MMPI in all its versions for the use in criminology, population studies, and prediction of aptitude in a particular role. Several studies on the MMPI-2-RF have compared those with a criminal history to those who have undergone rehabilitation and found that high scores on externalizing scales were predictive of violent behavior.[9] The MMPI-2-RF has also been used to prescreen applicants for law enforcement to obtain baseline mental health or flagging for aggressive tendencies.[1][10] There has also been usage evaluating parenting suitability in custody battles over children and in predicting the course of domestic disputes in couples.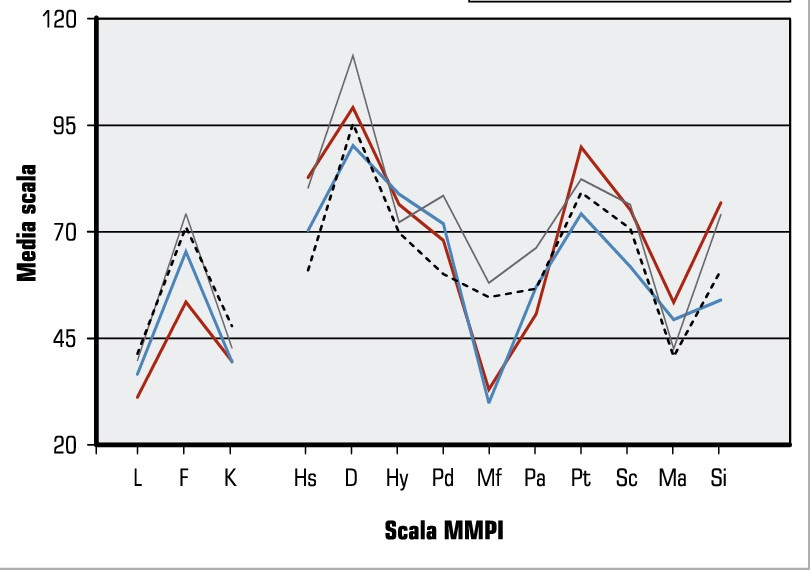 [11][12] Interpretations of the test have also been used to establish criminal intent in defendants.[1][9]
[11][12] Interpretations of the test have also been used to establish criminal intent in defendants.[1][9]
A major consensus of the MMPI in its current form is that increased accessibility for being tested improves retention without compromising outcomes. Prevailing criticisms of the original format were the extensive span of questioning and difficulty of paper administration for both completion and grading, with efforts to provide a more efficient medium well-documented since the 1980s.[13] When evaluating the use of tablet devices compared to conventional forms of electronic administration using a home computer or laptop for taking the MMPI-RF-2, the difference in reliability of results between the two mediums was insignificant.[14] There have also been motions to use the MMPI-2-RF to assess psychopathy utilizing an algorithm using a high score on a higher-order scale and then tailoring the remaining assessment to similar questions to the indicated higher order.[15] To aid in administration to pediatric patients, an adolescent form exists known as the Minnesota Multiphasic Personality Inventory-Adolescent-Restructured Form (MMPI-A-RF). [16]
[16]
Clinical Pearls
The MMPI provides broad information about aspects of personality and the existence of components of psychopathology.
The MMPI is completed by indicating true/false to a series of declarative statements that identify personal beliefs or symptomology.
Interpretation is based upon scoring reasonably truthfully and consistently within the outlined scales of the test.
Scales in older versions represented clinical syndromes, while more recently developed scales are based on identifying symptoms that can be applied to appropriate conditions or disorders.
The MMPI is effective at distinguishing psychopathy from malingering or purposeful test-taking as well as from medical conditions.
The MMPI has been revised to make the test more efficient, reproducible to test-takers in a broader societal demographic, and more grounded in current theory.
The MMPI can be taken by an individual patient to provide evidence of their symptoms but can also be fielded to a population fitting a known category to observe trends within their scoring.
The MMPI has been applied to a variety of non-clinical settings, including legal evidence in criminal and civil cases and screening for employment.
The completion of the MMPI holds value in determining care throughout a variety of treatment considerations. The test should be administered by a licensed psychotherapist, usually a psychiatrist or clinical psychologist, with informed consent obtained by discussing the risks and benefits of completion. Analysis of the results by the psychotherapist interpreting scoring should be attached with a working diagnosis to assess for treatment response. The presence of conditions associated with high-scoring categories will ultimately guide the necessity for pharmacological or non-pharmacological treatment options. This will, in turn, outline the need for referral to appropriate mental healthcare, from continuing outpatient follow-up to institutionalization with fully-staffed nursing and rehabilitative care. Transfer of care should involve appropriate discussion of MMPI data correlated with a summary of interventions. High-scoring in concerning scales such as suicidality highlights an existing need for acute observation or placement. The validity of symptoms should also be corroborated to demonstrate whether a patient is malingering or suffering from organic disorders requiring medical management by a treatment team. The bio-ethical implications of the MMPI should also be identified if the patient is completing the test in concurrence or stipulation with legal charges, and they should be counseled on what findings might hold concerning criminality. The basis for the use of test data in determining adherence has also been documented in a sample consisting of 471 psychiatric patients, with externalizing scales predictive of whether a patient will be more likely to terminate treatment.[1] [Level 3] This illustrates the need for multi-level involvement in facilitating outreach and patient compliance.
High-scoring in concerning scales such as suicidality highlights an existing need for acute observation or placement. The validity of symptoms should also be corroborated to demonstrate whether a patient is malingering or suffering from organic disorders requiring medical management by a treatment team. The bio-ethical implications of the MMPI should also be identified if the patient is completing the test in concurrence or stipulation with legal charges, and they should be counseled on what findings might hold concerning criminality. The basis for the use of test data in determining adherence has also been documented in a sample consisting of 471 psychiatric patients, with externalizing scales predictive of whether a patient will be more likely to terminate treatment.[1] [Level 3] This illustrates the need for multi-level involvement in facilitating outreach and patient compliance.
Nursing, Allied Health, and Interprofessional Team Interventions
The MMPI can be a valuable tool in assessing the psychological status of a patient.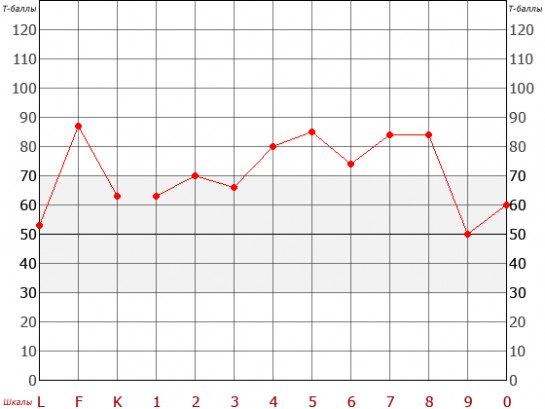 It will be ordered by a psychologically trained clinician but can provide crucial information to many members of the interprofessional healthcare team, including family clinicians, psychologically trained nursing staff, social workers, and counselors. Specifics regarding its use will vary depending on the clinical situation, and it needs to be part of a more complete evaluation to help direct therapeutic interventions and drive optimal patient outcomes. [Level 5]
It will be ordered by a psychologically trained clinician but can provide crucial information to many members of the interprofessional healthcare team, including family clinicians, psychologically trained nursing staff, social workers, and counselors. Specifics regarding its use will vary depending on the clinical situation, and it needs to be part of a more complete evaluation to help direct therapeutic interventions and drive optimal patient outcomes. [Level 5]
Review Questions
Access free multiple choice questions on this topic.
Comment on this article.
References
- 1.
Sellbom M. The MMPI-2-Restructured Form (MMPI-2-RF): Assessment of Personality and Psychopathology in the Twenty-First Century. Annu Rev Clin Psychol. 2019 May 07;15:149-177. [PubMed: 30601687]
- 2.
Butcher JN. Personality assessment from the nineteenth to the early twenty-first century: past achievements and contemporary challenges.
 Annu Rev Clin Psychol. 2010;6:1-20. [PubMed: 20192801]
Annu Rev Clin Psychol. 2010;6:1-20. [PubMed: 20192801]- 3.
Schilling R, Casper ST. Of psychometric means: Starke R. Hathaway and the popularization of the Minnesota Multiphasic Personality Inventory. Sci Context. 2015 Mar;28(1):77-98. [PubMed: 25832571]
- 4.
Carter JH. Racism's impact on mental health. J Natl Med Assoc. 1994 Jul;86(7):543-7. [PMC free article: PMC2607595] [PubMed: 8064907]
- 5.
Dennis PH. A comparative study of Minnesota Multiphasic Personality Inventory (MMPI) scores of four apparently different black populations. J Natl Med Assoc. 1974 May;66(3):244-7 passim. [PMC free article: PMC2609171] [PubMed: 4151276]
- 6.
Drayton M. The Minnesota Multiphasic Personality Inventory-2 (MMPI-2). Occup Med (Lond). 2009 Mar;59(2):135-6. [PubMed: 19233834]
- 7.
Ingram PB, Ternes MS. The detection of content-based invalid responding: a meta-analysis of the MMPI-2-Restructured Form's (MMPI-2-RF) over-reporting validity scales.
 Clin Neuropsychol. 2016 May;30(4):473-96. [PubMed: 27214667]
Clin Neuropsychol. 2016 May;30(4):473-96. [PubMed: 27214667]- 8.
Tarescavage AM, Scheman J, Ben-Porath YS. Reliability and validity of the Minnesota Multiphasic Personality Inventory-2-Restructured Form (MMPI-2-RF) in evaluations of chronic low back pain patients. Psychol Assess. 2015 Jun;27(2):433-446. [PubMed: 25436662]
- 9.
Whitman MR, Tarescavage AM, Glassmire DM, Burchett D, Sellbom M. Examination of differential validity of MMPI-2-RF scores by gender and ethnicity in predicting future suicidal and violent behaviors in a forensic sample. Psychol Assess. 2019 Mar;31(3):404-409. [PubMed: 30520653]
- 10.
Marshall RE, Milligan-Saville JS, Steel Z, Bryant RA, Mitchell PB, Harvey SB. A prospective study of pre-employment psychological testing amongst police recruits. Occup Med (Lond). 2020 May 27;70(3):162-168. [PubMed: 32040153]
- 11.
Lee TTC, Taylor AM, Holbert AM, Graham JR. MMPI-2-RF predictors of interpersonal relationship characteristics in committed couples.
 Psychol Assess. 2019 Sep;31(9):1118-1124. [PubMed: 31192629]
Psychol Assess. 2019 Sep;31(9):1118-1124. [PubMed: 31192629]- 12.
Fariña F, Redondo L, Seijo D, Novo M, Arce R. A meta-analytic review of the MMPI validity scales and indexes to detect defensiveness in custody evaluations. Int J Clin Health Psychol. 2017 May-Aug;17(2):128-138. [PMC free article: PMC6220924] [PubMed: 30487888]
- 13.
Deskovitz MA, Weed NC, McLaughlan JK, Williams JE. Interpretive Reliability of Six Computer-Based Test Interpretation Programs for the Minnesota Multiphasic Personality Inventory-2. Assessment. 2016 Apr;23(2):250-61. [PubMed: 25944798]
- 14.
Menton WH, Crighton AH, Tarescavage AM, Marek RJ, Hicks AD, Ben-Porath YS. Equivalence of Laptop and Tablet Administrations of the Minnesota Multiphasic Personality Inventory-2 Restructured Form. Assessment. 2019 Jun;26(4):661-669. [PubMed: 28618858]
- 15.
Tarescavage AM, Ben-Porath YS. Examination of the feasibility and utility of flexible and conditional administration of the Minnesota Multiphasic Personality Inventory-2-Restructured Form.
 Psychol Assess. 2017 Nov;29(11):1337-1348. [PubMed: 28165271]
Psychol Assess. 2017 Nov;29(11):1337-1348. [PubMed: 28165271]- 16.
Handel RW. An Introduction to the Minnesota Multiphasic Personality Inventory-Adolescent-Restructured Form (MMPI-A-RF). J Clin Psychol Med Settings. 2016 Dec;23(4):361-373. [PubMed: 27752979]
Minnesota Multiphasic Personality Inventory - StatPearls
Augustus E. Floyd; Vikas Gupta.
Author Information
Last Update: April 28, 2022.
Definition/Introduction
The Minnesota Multiphasic Personality Inventory (MMPI) is the most common psychometric test devised to assess personality traits and psychopathology. This data can be used to draw conclusions about the test taker’s psychopathy or to interpret psychological characteristics compared to the norm.[1] The most common treatment application of the test by providers is establishing or reevaluating care for an ambiguous clinical picture.[2] For psychiatric management, this aids in creating generalizable data relevant to a plethora of possible conditions. [1][2]
[1][2]
The MMPI was developed in the 1930s and published through the University of Minnesota in 1942 by Stuart Hathaway and Charley McKinley using visitors of patients at the University of Minnesota hospital as a base sample in both theorizing constructs of psychiatric illness and fielding the instrument. Testing is administered through 567 true or false items using a booklet with an accompanying answer sheet. The responses are then hand-scored and plotted on an X-Y graph; a separate version is used for male and female respondents.[3]
The X-axis is comprised of 14 scales. The first four ‘content scales’ judge the validity of the test attempt and include:
? to represent the number of questions completed incorrectly, either with no attempt or both ‘true’ and ‘false’ selected
L for ‘Lie’ to represent an attempt by the respondent to misrepresent themselves in a more positive light
F or ‘frequency’ to gauge random response as well as the respondent’s exaggeration or downplaying of symptoms
K to gauge ‘defensiveness,’ or evasion of stressful content
The 10 remaining scales known as ‘clinical scales’ are designed to measure for the presence of psychiatric syndromes, including:
1 or ‘Hs’ for hypochondriasis
2 or ‘D’ for depression
3 or ‘Hy’ for hysteria
4 or ‘Pd’ for psychopathic deviate
5 or ‘Mf’ for the continuum of masculinity-femininity
6 or ‘Pa’ for paranoia
7 or ‘Pt’ for psychasthenia or obsessive-compulsive tendency
8 or ‘Sc’ for schizophrenia
9 or ‘Ma’ for mania
0 or ‘Si’ for social introversion.
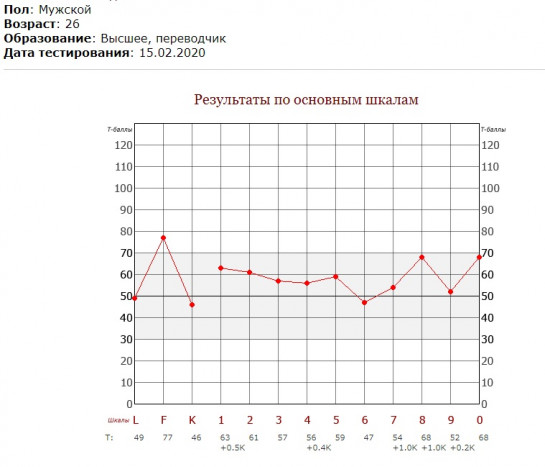
The Y-axis statistically standardizes the grading received on each scale in a range of T-scores from 0 to 120. A mean score is 50, and 82% of respondents are considered the normal population falling between 30 and 70. A T-score greater than 70 indicates psychopathy in that category.
Issues of Concern
The existence of the MMPI has been concurrent with vast reforms in societal convention and increased understanding of behavioral health.[3] Likewise, the instrument has been adapted to reflect such changes. Overarching criticisms to the original test center on its disparity in addressing psychopathy in social and ethnic minorities.[1] This has been attributed to the original sample being a small group, mainly consisting of young rural Caucasian subjects from the Midwestern United States.[4] Studies have established biases in which misunderstanding or failure to identify with the content of questions culturally has led to underreporting or overreporting mental illness.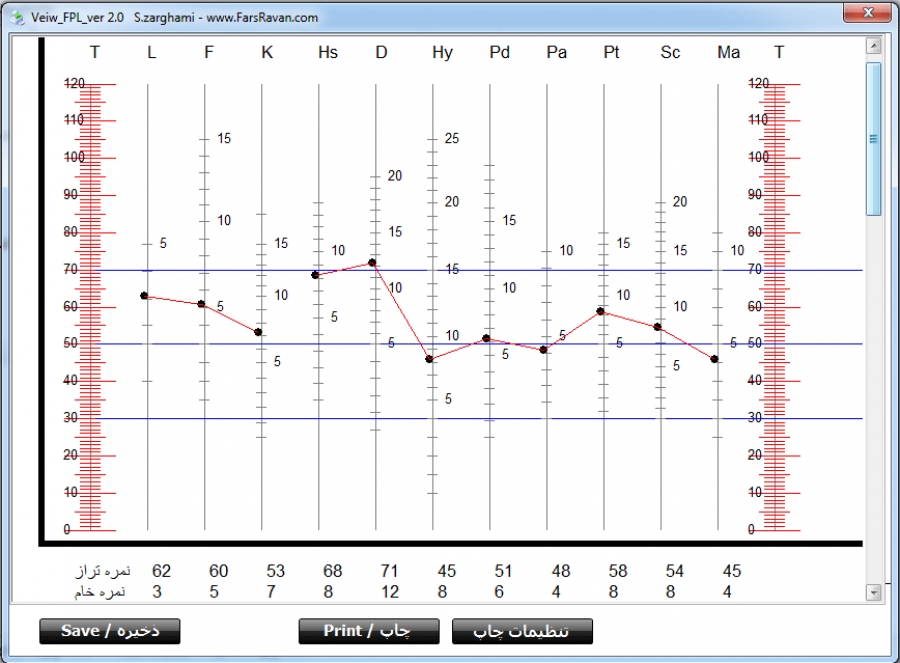 [5][1]
[5][1]
These shortcomings led to the release of the MMPI-2 by James N. Butcher, W. Grant Dahlstrom, John R. Graham, Auke Tellegen, and Beverly Kaemme in 1989.[6] This assessment retains the original total of 567 items with the same corresponding 14 scales with the original number of questions from the test.[6] Test items were revised based upon a larger and more diverse sample size of 2600 attuned to a 6th-grade reading level.[6] Gendered differences were replaced with a nongendered standardized scoring.[6] Despite further advancements, the MMPI-2 is still the most commonly administered version and has been translated into over 40 languages.[1]
In 2003, 9 restructured clinical or ‘RC’ scales were introduced as a prospective replacement for the original clinical scales.[1] These include:
RCd, or ‘demoralization’ – misery or depression
RC1 or ‘somatic complaints, – the fixation on bodily symptoms of illness or somatization
RC2 or ‘low positive emotions’ – weakened positivity, lack of enjoyment
RC3 or ‘cynicism’ – low regard for the merit of others and their actions
RC4 or ‘antisocial behavior’ – selfish and sociopathic conduct
RC6 or ‘ideas of persecution’ – belief in the malintent of others toward oneself
RC7 or ‘dysfunctional negative emotions’ – experiences on a spectrum of anxiety and irritability
RC8 or ‘aberrant experiences’ – uncommon beliefs or interpretation of experiences
RC9 or ‘hypomanic activation’ – energetic drive and desire for exertion
The RC scales were devised to provide a streamlined interpretation and less overlap with an increased focus on the growth in understanding within psychiatry over the past 70 years. Combinations of high-scoring categories represent distinct psychiatric constructs rather than the nebulous findings of the original clinical scales tying the patient to a specific diagnosis. Arguments also exist that this information is limited in that it categorizes the responder rather than providing data on an individual patient within a personalized spectrum of behavior.[1]
Combinations of high-scoring categories represent distinct psychiatric constructs rather than the nebulous findings of the original clinical scales tying the patient to a specific diagnosis. Arguments also exist that this information is limited in that it categorizes the responder rather than providing data on an individual patient within a personalized spectrum of behavior.[1]
The RC scales were incorporated into the most current form of the MMPI, known as the Minnesota Multiphasic Personality Inventory-2 Revised Form, or the MMPI-2-RF, which was released in 2008 by Yossef Ben-Porath and Auke Telleger of the University of Minnesota. The MMPI-2-RF is composed of 338 items measured by 51 scales broken into 9 validity scales, 3 higher-order scales, the 9 RC scales, 23 specific problem scales, 2 interest scales, and 5 revised personality psychopathy scales.[1]
The 9 validity scales assess incongruent answering or deceptive test-taking and include:
VRIN-r or ‘variable response inconsistency’ – inconsistent reporting of items
TRIN-r or ‘true response inconsistency’ careless reporting of items
F-r or ‘infrequent responses,’ – overreporting of infrequent responses compared to the norm
Fp-r or ‘infrequent psychopathology responses’ – overreporting of infrequent responses compared to those with psychopathy
Fs or ‘infrequent somatic responses’ – overreporting of infrequent responses compared to medical patients
FBS-r or ‘symptom validity’ – overreporting of nonvalid symptoms compared to both physical and mental standard symptomology
RBS or ‘response bias’ – overreporting associated with a statistically invalidated presentation of the disease
L-r or ‘uncommon virtues’ – underreporting through infrequently declared values or actions
K-r or ‘adjustment validity’ – underreporting by tailoring answers to give the impression of healthy psychological adjustment
The 3 higher-order scales broadly categorize psychopathic presentation and include:
EID or ‘emotional/internalizing dysfunction’ – problems concerning mood and affect
THD or ‘thought dysfunction’ – problems concerning disorganization of thought
BXD or ‘behavioral/external dysfunction’ – problems concerning impulsive or inappropriate behavior
The problem scales highlight responses consistent with the presence of specific psychopathic and psychosomatic presentations and include:
MLS or ‘malaise’
GIC or ‘gastrointestinal complaints’
HPC or ‘head pain complaints'
NUC or ‘neurological complaints’
COG or ‘cognitive complaints’
SUI or ‘suicidal/death ideation’
HLP or ‘helplessness/hopelessness’
SFD or ‘self-doubt’
NFC or ‘inefficacy’
STW or ‘stress/worry’
AXY or ‘anxiety’
ANP or ‘anger proneness’
BRF or ‘behavior-restricting fears’
MSF or ‘multiple specific fears’
JCP or ‘juvenile conduct problems’
SUB or ‘substance abuse’
AGG or ‘aggression’
ACT or ‘activation’
FML or ‘family problems’
IPP or ‘interpersonal passivity’
SAV or ‘social avoidance’
SHY or ‘shyness’
DSF or ‘disaffiliativeness’
The interest scales are designed to assess cognitive skills, aptitude, and learning preferences which include:
AES or aesthetic-literary interests – pursuits related to fine art
MEC or mechanical-physical interests – pursuits related to kinesthetic activities
The revised personality/psychopathology five scales are based on 107 distinct items and include:
AGG-r or ‘aggressiveness-revised’ – preference for excess and antagonism
PSYCH-r or ‘psychoticism-revised’ – preference for disconnection from reality
DISC-r or ‘disconstraint-revised’ – preference for impulsion and compulsion
NEGE-r or ‘negative emotionality/neuroticism-revised’ – preference for anxiety
INTR-r or ‘introversion/low positive emotional-revised’ – flat affect and timidity
It has been suggested that while the MMPI-2-RF has many additional metrics, the reduction in question number limits the amount of information about psychiatric diseases to about 60% of the original test. There has also been considerable debate over whether the new metrics are inaccurate in detecting psychopathy.[1] In separating genuine psychopathy from attempts to feign a diagnosis for personal incentive, some studies have noted the new validity scales to be overly sensitive to overreporting symptoms to achieve a specific result. It has conversely been found that the L-r and K-r scales are particularly reliable at detecting underreporting of mental illness.[7][8] Overall, literature has supported the MMPI-2-RF in identifying the accuracy of reporting psychiatric information in those who complete it.[1]
There has also been considerable debate over whether the new metrics are inaccurate in detecting psychopathy.[1] In separating genuine psychopathy from attempts to feign a diagnosis for personal incentive, some studies have noted the new validity scales to be overly sensitive to overreporting symptoms to achieve a specific result. It has conversely been found that the L-r and K-r scales are particularly reliable at detecting underreporting of mental illness.[7][8] Overall, literature has supported the MMPI-2-RF in identifying the accuracy of reporting psychiatric information in those who complete it.[1]
Clinical Significance
The MMPI maintains an enduring presence in the field of mental health, and its current adaption has been widely evaluated by the standard of modern behavioral health practices.[1] It continues to receive widespread application as a threshold of determining the presence of psychopathy, as a means of constructing a differential diagnosis for mental health problems, and as a versatile test to achieve transferrable psychological data. These data points indicate a category, which gives behavioral health professionals a starting point to explore plausible diagnoses and initiate appropriate treatment. Completion may also offer therapeutic benefits to patients in reflecting upon their issues and improving personal understanding of their psychology.[3]
These data points indicate a category, which gives behavioral health professionals a starting point to explore plausible diagnoses and initiate appropriate treatment. Completion may also offer therapeutic benefits to patients in reflecting upon their issues and improving personal understanding of their psychology.[3]
In addition to its predominant clinical application, an extensive body of research exists to assess the MMPI in all its versions for the use in criminology, population studies, and prediction of aptitude in a particular role. Several studies on the MMPI-2-RF have compared those with a criminal history to those who have undergone rehabilitation and found that high scores on externalizing scales were predictive of violent behavior.[9] The MMPI-2-RF has also been used to prescreen applicants for law enforcement to obtain baseline mental health or flagging for aggressive tendencies.[1][10] There has also been usage evaluating parenting suitability in custody battles over children and in predicting the course of domestic disputes in couples. [11][12] Interpretations of the test have also been used to establish criminal intent in defendants.[1][9]
[11][12] Interpretations of the test have also been used to establish criminal intent in defendants.[1][9]
A major consensus of the MMPI in its current form is that increased accessibility for being tested improves retention without compromising outcomes. Prevailing criticisms of the original format were the extensive span of questioning and difficulty of paper administration for both completion and grading, with efforts to provide a more efficient medium well-documented since the 1980s.[13] When evaluating the use of tablet devices compared to conventional forms of electronic administration using a home computer or laptop for taking the MMPI-RF-2, the difference in reliability of results between the two mediums was insignificant.[14] There have also been motions to use the MMPI-2-RF to assess psychopathy utilizing an algorithm using a high score on a higher-order scale and then tailoring the remaining assessment to similar questions to the indicated higher order.[15] To aid in administration to pediatric patients, an adolescent form exists known as the Minnesota Multiphasic Personality Inventory-Adolescent-Restructured Form (MMPI-A-RF). [16]
[16]
Clinical Pearls
The MMPI provides broad information about aspects of personality and the existence of components of psychopathology.
The MMPI is completed by indicating true/false to a series of declarative statements that identify personal beliefs or symptomology.
Interpretation is based upon scoring reasonably truthfully and consistently within the outlined scales of the test.
Scales in older versions represented clinical syndromes, while more recently developed scales are based on identifying symptoms that can be applied to appropriate conditions or disorders.
The MMPI is effective at distinguishing psychopathy from malingering or purposeful test-taking as well as from medical conditions.
The MMPI has been revised to make the test more efficient, reproducible to test-takers in a broader societal demographic, and more grounded in current theory.
The MMPI can be taken by an individual patient to provide evidence of their symptoms but can also be fielded to a population fitting a known category to observe trends within their scoring.

The MMPI has been applied to a variety of non-clinical settings, including legal evidence in criminal and civil cases and screening for employment.
The completion of the MMPI holds value in determining care throughout a variety of treatment considerations. The test should be administered by a licensed psychotherapist, usually a psychiatrist or clinical psychologist, with informed consent obtained by discussing the risks and benefits of completion. Analysis of the results by the psychotherapist interpreting scoring should be attached with a working diagnosis to assess for treatment response. The presence of conditions associated with high-scoring categories will ultimately guide the necessity for pharmacological or non-pharmacological treatment options. This will, in turn, outline the need for referral to appropriate mental healthcare, from continuing outpatient follow-up to institutionalization with fully-staffed nursing and rehabilitative care. Transfer of care should involve appropriate discussion of MMPI data correlated with a summary of interventions. High-scoring in concerning scales such as suicidality highlights an existing need for acute observation or placement. The validity of symptoms should also be corroborated to demonstrate whether a patient is malingering or suffering from organic disorders requiring medical management by a treatment team. The bio-ethical implications of the MMPI should also be identified if the patient is completing the test in concurrence or stipulation with legal charges, and they should be counseled on what findings might hold concerning criminality. The basis for the use of test data in determining adherence has also been documented in a sample consisting of 471 psychiatric patients, with externalizing scales predictive of whether a patient will be more likely to terminate treatment.[1] [Level 3] This illustrates the need for multi-level involvement in facilitating outreach and patient compliance.
High-scoring in concerning scales such as suicidality highlights an existing need for acute observation or placement. The validity of symptoms should also be corroborated to demonstrate whether a patient is malingering or suffering from organic disorders requiring medical management by a treatment team. The bio-ethical implications of the MMPI should also be identified if the patient is completing the test in concurrence or stipulation with legal charges, and they should be counseled on what findings might hold concerning criminality. The basis for the use of test data in determining adherence has also been documented in a sample consisting of 471 psychiatric patients, with externalizing scales predictive of whether a patient will be more likely to terminate treatment.[1] [Level 3] This illustrates the need for multi-level involvement in facilitating outreach and patient compliance.
Nursing, Allied Health, and Interprofessional Team Interventions
The MMPI can be a valuable tool in assessing the psychological status of a patient. It will be ordered by a psychologically trained clinician but can provide crucial information to many members of the interprofessional healthcare team, including family clinicians, psychologically trained nursing staff, social workers, and counselors. Specifics regarding its use will vary depending on the clinical situation, and it needs to be part of a more complete evaluation to help direct therapeutic interventions and drive optimal patient outcomes. [Level 5]
It will be ordered by a psychologically trained clinician but can provide crucial information to many members of the interprofessional healthcare team, including family clinicians, psychologically trained nursing staff, social workers, and counselors. Specifics regarding its use will vary depending on the clinical situation, and it needs to be part of a more complete evaluation to help direct therapeutic interventions and drive optimal patient outcomes. [Level 5]
Review Questions
Access free multiple choice questions on this topic.
Comment on this article.
References
- 1.
Sellbom M. The MMPI-2-Restructured Form (MMPI-2-RF): Assessment of Personality and Psychopathology in the Twenty-First Century. Annu Rev Clin Psychol. 2019 May 07;15:149-177. [PubMed: 30601687]
- 2.
Butcher JN. Personality assessment from the nineteenth to the early twenty-first century: past achievements and contemporary challenges.
 Annu Rev Clin Psychol. 2010;6:1-20. [PubMed: 20192801]
Annu Rev Clin Psychol. 2010;6:1-20. [PubMed: 20192801]- 3.
Schilling R, Casper ST. Of psychometric means: Starke R. Hathaway and the popularization of the Minnesota Multiphasic Personality Inventory. Sci Context. 2015 Mar;28(1):77-98. [PubMed: 25832571]
- 4.
Carter JH. Racism's impact on mental health. J Natl Med Assoc. 1994 Jul;86(7):543-7. [PMC free article: PMC2607595] [PubMed: 8064907]
- 5.
Dennis PH. A comparative study of Minnesota Multiphasic Personality Inventory (MMPI) scores of four apparently different black populations. J Natl Med Assoc. 1974 May;66(3):244-7 passim. [PMC free article: PMC2609171] [PubMed: 4151276]
- 6.
Drayton M. The Minnesota Multiphasic Personality Inventory-2 (MMPI-2). Occup Med (Lond). 2009 Mar;59(2):135-6. [PubMed: 19233834]
- 7.
Ingram PB, Ternes MS. The detection of content-based invalid responding: a meta-analysis of the MMPI-2-Restructured Form's (MMPI-2-RF) over-reporting validity scales.
 Clin Neuropsychol. 2016 May;30(4):473-96. [PubMed: 27214667]
Clin Neuropsychol. 2016 May;30(4):473-96. [PubMed: 27214667]- 8.
Tarescavage AM, Scheman J, Ben-Porath YS. Reliability and validity of the Minnesota Multiphasic Personality Inventory-2-Restructured Form (MMPI-2-RF) in evaluations of chronic low back pain patients. Psychol Assess. 2015 Jun;27(2):433-446. [PubMed: 25436662]
- 9.
Whitman MR, Tarescavage AM, Glassmire DM, Burchett D, Sellbom M. Examination of differential validity of MMPI-2-RF scores by gender and ethnicity in predicting future suicidal and violent behaviors in a forensic sample. Psychol Assess. 2019 Mar;31(3):404-409. [PubMed: 30520653]
- 10.
Marshall RE, Milligan-Saville JS, Steel Z, Bryant RA, Mitchell PB, Harvey SB. A prospective study of pre-employment psychological testing amongst police recruits. Occup Med (Lond). 2020 May 27;70(3):162-168. [PubMed: 32040153]
- 11.
Lee TTC, Taylor AM, Holbert AM, Graham JR. MMPI-2-RF predictors of interpersonal relationship characteristics in committed couples.
 Psychol Assess. 2019 Sep;31(9):1118-1124. [PubMed: 31192629]
Psychol Assess. 2019 Sep;31(9):1118-1124. [PubMed: 31192629]- 12.
Fariña F, Redondo L, Seijo D, Novo M, Arce R. A meta-analytic review of the MMPI validity scales and indexes to detect defensiveness in custody evaluations. Int J Clin Health Psychol. 2017 May-Aug;17(2):128-138. [PMC free article: PMC6220924] [PubMed: 30487888]
- 13.
Deskovitz MA, Weed NC, McLaughlan JK, Williams JE. Interpretive Reliability of Six Computer-Based Test Interpretation Programs for the Minnesota Multiphasic Personality Inventory-2. Assessment. 2016 Apr;23(2):250-61. [PubMed: 25944798]
- 14.
Menton WH, Crighton AH, Tarescavage AM, Marek RJ, Hicks AD, Ben-Porath YS. Equivalence of Laptop and Tablet Administrations of the Minnesota Multiphasic Personality Inventory-2 Restructured Form. Assessment. 2019 Jun;26(4):661-669. [PubMed: 28618858]
- 15.
Tarescavage AM, Ben-Porath YS. Examination of the feasibility and utility of flexible and conditional administration of the Minnesota Multiphasic Personality Inventory-2-Restructured Form.
 Psychol Assess. 2017 Nov;29(11):1337-1348. [PubMed: 28165271]
Psychol Assess. 2017 Nov;29(11):1337-1348. [PubMed: 28165271]- 16.
Handel RW. An Introduction to the Minnesota Multiphasic Personality Inventory-Adolescent-Restructured Form (MMPI-A-RF). J Clin Psychol Med Settings. 2016 Dec;23(4):361-373. [PubMed: 27752979]
MMPI scale 4 Impulsivity
Doctor Demkin's blog
Articles about psychology and psychodiagnostics
- Are you here:
- Home
- Blog
- Psychodiagnostics
- 4th scale MMPI (SMIL) Psychopathic deviations
Psychodiagnostics
The 4th scale of the MMPI methodology and its clone adaptations (SMIL, SKLO, MMIL, MLO) is a complex heterogeneous scale with a multi-variant interpretation and a large number of descriptors.
Using the 4th scale, the overall level of social adaptation of a person is assessed:
- degree of self-alienation and alienation from family and society,
- compliance with generally accepted moral and ethical standards, laws,
- respect for the interests of other people,
- the ability to obey.
This scale makes it possible to identify manifestations of such a significant deficiency in the consciousness, actions and behavior of a person as lack of understanding of the negative consequences of one's actions for other people , which leads to deviant behavior, recurring problems and conflicts in the family, at school or work, clashes with the law.
Along with the F scale and the 9th scale, forms the aggression index , which, when the sum of the F + 4 + 9 scales > 200 T points, is a predictor of open physical aggression.
The original goal of developing the scale was to identify individuals who have constant problems with the law , but at the same time have normal cognitive (mental) abilities and satisfactory social and psychological adaptation.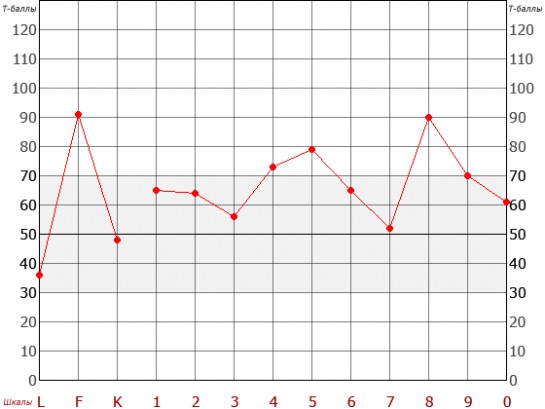 This is a target group of people who do not care about the social consequences of their behavior, but at the same time they do not have neurotic or psychotic disorders, do not show signs of aggressive or deviant behavior during the examination or interview. However, in a state of stress or when faced with a situation that requires consistent and responsible behavior, such people act solely in their own interests, including in rebellious antisocial forms with the manifestation of heteroaggression.
This is a target group of people who do not care about the social consequences of their behavior, but at the same time they do not have neurotic or psychotic disorders, do not show signs of aggressive or deviant behavior during the examination or interview. However, in a state of stress or when faced with a situation that requires consistent and responsible behavior, such people act solely in their own interests, including in rebellious antisocial forms with the manifestation of heteroaggression.
The task of identifying people with similar characteristics during professional selection is especially relevant due to the fact that such people, having well-developed communication skills, developed intuition (with a moderate increase in the scale) and the ability to manipulate others, are able to make the most favorable first impression , may seem friendly and very interesting to talk to (especially as the scale goes down to 0). Their recent acquaintances often cannot believe that such "nice" people are capable of antisocial behavior or crime.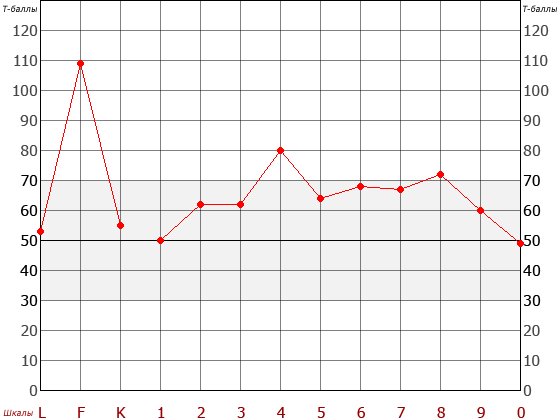 Quite often such people reveal traits of the Dark Triad of Personality.
Quite often such people reveal traits of the Dark Triad of Personality.
The hallmark of people in this group is an inability to learn from their own mistakes , even if this results in repeated punishments or loss of benefits. People in this category are capable of experiencing some degree of guilt when they are caught or caught (especially if this avoids or reduces punishment), but the guilt quickly passes and the cycles of antisocial behavior repeat.
The core of the problems in individuals with high scores on the scale of Psychopathic Deviations - Impulsivity
- Difficult or inhibited social learning,
- Low sensitivity to social feedback,
- Low empathy,
- High impulsiveness in actions, reactions, decisions,
- Inability to delay reward (pleasure),
- Risk preparedness and search (due to blocking information about threats),
- Unmotivated antagonistic competition,
- Aggressive behavior and reactions, bullying
- Miscellaneous deviant behavior
- Possible criminal orientation and activity,
- Possible alcohol, drug, gambling addiction.
Neurophysiological features
- Decreased activity of stress-regulating systems
- Low serotonergic and dopaminergic activity
What does an increase in scores on the 4th scale of MMPI mean
In general cases, an increase in scores on the 4th scale can be described by the following personality descriptors:
- Difficulties in accepting the values, rules and standards of society (characteristic of deviant behavior) .
- Impulsiveness of behavior, desire for immediate satisfaction of impulses and needs (for example, characteristic of aggressive drivers, for counterproductive behavior at work) .
- Insensitivity to the needs and feelings of others (for example, characteristic of despotic politicians) .
- Possible manifestation of antisocial behavior, including lying, cheating, stealing, sexual deviations, direct physical aggression, violence.
- Conflicts with authority figures, difficulties with submission.
- Probable alcohol and/or drug abuse.
- Stormy family relationships and marital problems, including infidelity.
- Blaming family members and the environment for their own difficulties (typical for toxic partners).
- Insufficient or missed life achievements.
- Myopia, difficulty planning actions and long-term strategies.
- Action without regard for consequences. The inability to learn from negative experiences.
- Acceptance of risks, including unreasonable ones. Seeking thrills.
- Impatience, difficulty waiting, reduced frustration tolerance.
- Immaturity of emotions, infantilism, childishness.
- Narcissistic self-centeredness and selfishness. Demonstrativeness and exhibitionist tendencies.
- The ability to make a good first impression as smart and self-confident people (especially at a low 0-th scale), which is typical for manipulators.
- Sociability, contact, talkativeness.
- Manipulation of people. Interest only in those who can benefit or give pleasure.
- The superficiality of interpersonal relationships. Inability to have deep emotional attachments. Resentment and ease of breaking relationships.
- They are distinguished by sarcasm and cynicism in relationships. They joke a lot, “humor”, “taunt”.
- Show hostility, aggressiveness, rebelliousness. Opposition to any restrictions or dominant authoritarian figures.
- Men show direct verbal and physical aggression.
 Women are more likely to show passive or indirect aggression.
Women are more likely to show passive or indirect aggression. - A wide range of interests without a clear focus.
- Activity, enterprise, energy and spontaneity.
- Creativity and innovation.
- Can feign guilt and remorse when it helps to extricate themselves from problems.
- There is no deep emotional reaction during experiences.
- They rarely admit to feeling sadness, fear and worry about the future.
- Most often they feel boredom and inner emptiness, which they seek to fill with activity, entertainment and rewards of various kinds.
- Have a poor prognosis for psychotherapy, but may agree to treatment to avoid trouble. In the process, they tend to over-intellectualize problems and blame others for their own difficulties. As a rule, interrupt the course prematurely.
Main complaints:
Problems with authoritarian persons, parents, delinquency, emotional difficulties in intimate relationships, physical aggression, anger, outbursts of emotions, protest and rebellious behavior, potential for developing addictions to psychoactive substances.
Dominant thoughts:
Distrust, alienation, anger, boredom, how to "stab" everyone, get a benefit, how to please yourself and immediately!
Emotional sphere:
Emotional impulses, social fearlessness, superficial feelings, emotional detachment, accusations, stimulus seeking, tirelessness.
Assessing the level of problems when increasing the 4th MMPI scale (SMIL)
| Level of likely psychopathological manifestations T ≥ 75 ( MMPI -2) ≥ 80 ( MMPI ) Antisocial behavior, direct aggression, violence, instability of behavior, irresponsibility, low tolerance for boredom, problems with the law, alcohol, drug abuse, complete self-forgiveness. |
| Level of pronounced accentuation and possible psychopathological manifestations T = 65-74 ( MMPI -2) T = 70-79 ( MMPI ) Rebelliousness, protests against restrictions and authoritarian figures, difficulty obeying, insecurity, impulsiveness, irritability, conflict, spitefulness, aggressiveness, problems at work, family problems, manipulation of others, narcissism, selfishness, possible alcohol abuse, less often drugs. Periodic outbursts of irresponsible antisocial behavior. They may feel genuine remorse, albeit for a short time. |
| Level of character traits and latent personality accentuation T=55-64 ( MMPI -2) T=55-69 ( MMPI ) Non-standard, creativity, sociability, immaturity, self-centeredness, superficiality, passive and indirect aggression, opposition to restrictions, constant search for pleasure, egocentrism, possible development of addictions, increased sexuality. |
| Average T= 45-54 Compliance with the requirements of society. |
| Low performance T < 45 Morality, self-criticism, conformity, manageability, mediocrity, problems with self-identification, low sexuality. |

When evaluating profiles with increasing scores on the 4th scale, it is important to take into account all the factors that may prompt the researcher, whether the results obtained are characterological or whether they reflect a situational adaptive reaction . The profile also needs to be assessed, taking into account the level of education, the cultural aspect and the socioeconomic status of the subject.
For example, elevated scores on Scale 4 in a manager may reflect a Machiavellian leadership style, egocentric nature, careerism, and a high degree of politicization, rather than conflicts with authoritarian figures and problems with the law.
Top managers, stock market players, financiers and businessmen, politicians who are able to instantly make independent decisions and bear significant risks for the sake of personal success, manipulate not only individuals, but also large communities, will also experience an increase in the 4th scale SMIL. Such individuals are unlikely to have criminal problems, apart from possible economic and political machinations. However, they will also show characteristic features: the ability and desire to manipulate people in their own interests, pronounced narcissism, lack of empathy, the desire to bypass or “bend” the law for their own benefit, an expressed protest against any kind of control of their freedom and independence, which can lead to interpersonal problems and conflicts. Taking into account the high socioeconomic, cultural and educational level of the subjects, the prediction of antisocial behavior seems unlikely. However, it can be done when revealing a history of manifestations of physical aggression, explosive reactions and socially dangerous actions, conflicts, acts of armed self-defense. In this case, it is unlikely that the history of active direct physical aggression will stop on its own, and will not develop progressively.
In this case, it is unlikely that the history of active direct physical aggression will stop on its own, and will not develop progressively.
The main social groups characterized by an increase in indicators on the 4th scale
- Orphans, children of divorced parents, victims of domestic violence, residents of boarding schools, shelters, orphanages.
- Teenagers, students.
- Prisoners of colonies and prisons.
- Employees of law enforcement agencies with work experience.
- Businessmen, politicians.
- People in search of work, in the process of solving vital tasks.
- People in distress.
- Family conflicts (spouses, parents), recent divorce, deprivation of work or property.
- Graduates of educational institutions.

- Immigrants, visitors.
- Adherents of the counterculture.
During mass psychodiagnostic examinations, stable types were identified, characterized by an increase in the indicators of the 4th scale. [Astin, A. W. (1959). A factor study of the MMPI psychopathic deviate scale. Journal of Consulting Psychology, 23(6), 550-554., Comrey, A. L. (1958). A factor analysis of items on the MMPI Psychopathic Deviate Scale. Educational and Psychological Measurement, 18,91-98.]
| No. | Type | Description | |
| 1 | "Golden" youth. Bohemia | Disorganized and irresponsible hedonist - "free artist" with impulsive behavior, living in the moment. | |
| 2 | Politician. | Egocentric Machiavellian, steadily and disciplined (with a concomitant increase in K) following his goals with a well-thought-out strategy. | |
| 3. | "Cool" macho | A charming, impulsive hedonist whose tough temper and aggressiveness can be exacerbated by alcohol and drugs, but are quickly replaced by frustration. He fills the void with promiscuity, drinking, fighting and looking for trouble with the law. | |
| 4. | Henpecked | Passive, dependent, self-forgiving and disorganized quiet alcoholic, hunted down by a dominant partner who gives him some necessary support. |
 Businessman. Careerist.
Businessman. Careerist. Formative factors (evolutionary psychological theory)
- Hostile environment.

- Genetic predisposition.
- Rejection, inattention, coldness on the part of parents (unwanted child, indifferent, emotionally cold, hostile parents, incomplete family) or educators (orphan, orphanage child, cadet, prisoner).
- Constant conflicts, tension and stress in the parental family, educational or educational institution, organized team.
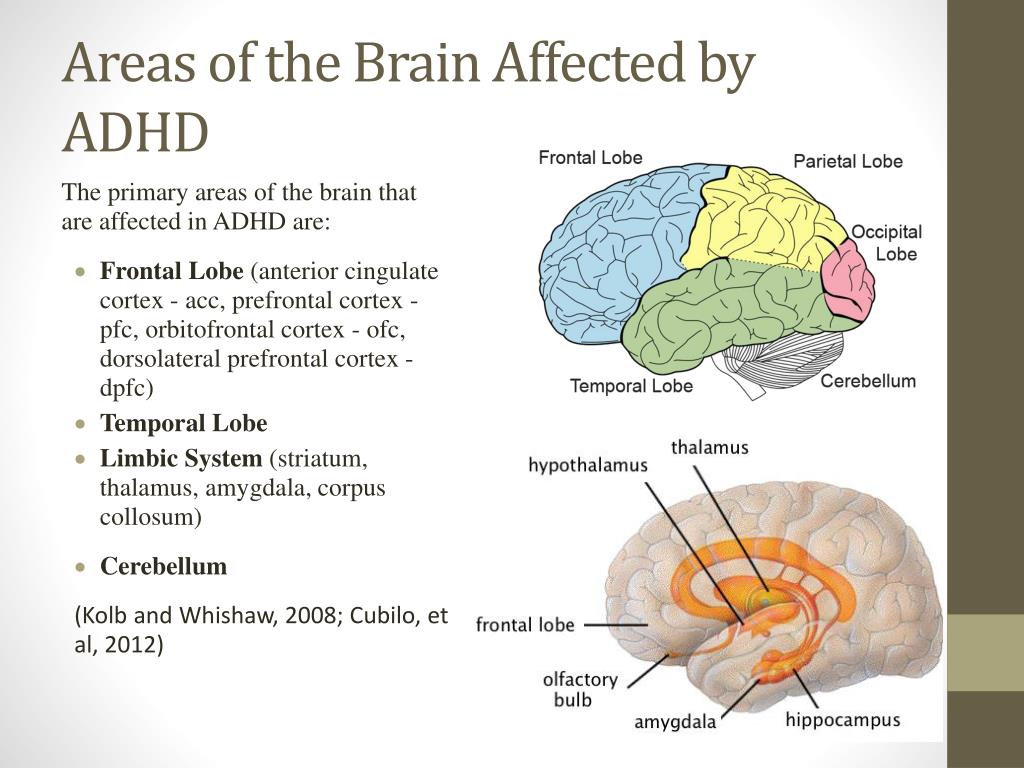
- Attention deficit hypermobility syndrome (ADHD).
- Decreased cortisol levels as a result of previous trauma.
Adaptive functions:
- Hostile environment survival
- Stress tolerance and minor threats
- Maintaining vigilance in dangerous environments
Basic psychological needs of people with high scores on the 4th SMIL scale
- In sensual pleasures, rewards, achievements (search for compensation for problems and suffering in childhood and adolescence).
- In dominance, to avoid anxiety due to falling under someone's control.
- Emotional distance due to unwillingness to become vulnerable.
- Pathological desire for lack of attention and love through aggressive and provocative behavior.
Sources of stress and situations of frustration
- Obstacles, coercion, lack of freedom, monotony, routine, lack of attention and recognition.
Typical stress response : Stenic reactions, heteroaggression.
Basic psychological defense mechanisms:
- Repression with behavioral response (criticism, protest, aggression of any kind).
- Projection
- Regression (care in childhood, infantilization).
- Isolation (alienation), distancing.
- Humor, cynicism
- Intellectualization
Cognitive distortions
- Close relationships can be traumatic.
- You have to be stronger than others to be safe.
- People just use each other for their own purposes.
Sexual activity
- Increased sexuality,
- Frequent change of partners,
- Surface relations,
- Debauchery. Sexual perversions, desire for non-standard or aggressive sex are possible.
- Severe difficulty in establishing deep emotional relationships, neglect of partner's needs.
- Inability to receive emotional satisfaction.
Governing life mottos
- My life - my rules.
- We only live once.
- Live fast, die young.
- Man to man is a wolf.
- From a black sheep - at least a tuft of wool.
- If you don't cheat, you won't sell.
Risks to life and life expectancy
Violent death, injuries, accidents, aggressive driving and traffic accidents, accidents, suicides, drug overdose, alcoholism and related diseases and acute conditions.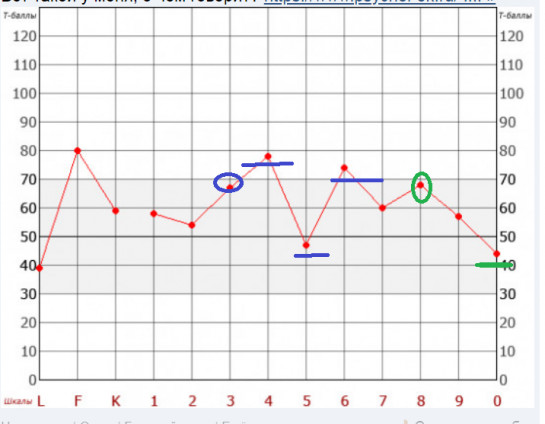
Life expectancy is less than in the group with normal or low scores on the 4th scale.
Peculiarities of interpretation of personality profiles with an increased 4th scale
To accurately describe the personality of the subject, it is necessary to evaluate the personality profile as a whole, in relation to the indicators of other MMPI scales. Even within the same profile, scores may differ depending on age, gender, education, and socioeconomic status. Examples of typical profiles are shown in the table below:
| Profile code | Key features at the level of violations |
| 49/94 | Impulsivity, anger, aggression. Enough energy for direct physical aggression and violent actions (fights, beatings, rape). Alcohol, drugs. |
| 48/84 | Psychotic variants of antisocial behavior. |
| 47/74 | Alternation of periods of complete irresponsibility for actions with periods of temporary guilt and self-flagellation. Persistent high level of anxiety. Need for ongoing self-assessment. |
| 46/64 | Immature passive dependent narcissistic personality. Suspicion and incredulity. Suppressed aggression and hostility. |
| 45/54 | Men: narcissistic individuals, with episodes of deviant behavior, participants in social and anti-government protests. Sometimes explicit homosexuals. Women: rejection of the female role, acceptance of male roles. Protest and criminal activity. Possible homosexuality (lesbianism). |
| 43/34 | Chronic intense passive aggression (often towards family members). Hidden and disguised anti-social actions. Manipulation of people. Treason. Episodes of violence are possible. |
| 42/24 | Unable to defer self-reward. Temporary guilt in those recently caught or convicted of deviant behavior. Repeating cycles: "action - capture - guilt - self-forgiveness - action." Suicidal thoughts. Alcohol, drugs. |
| 41/14 | Intense hypochondriacal symptoms (headaches). Hidden passive aggression. Alcohol, hard drugs as self-medication. |
 criminal behavior. Religious or political bigotry and likely extremism. Sexual perversions, sexual crimes. Alcohol, drugs (mainly hallucinogens).
criminal behavior. Religious or political bigotry and likely extremism. Sexual perversions, sexual crimes. Alcohol, drugs (mainly hallucinogens). 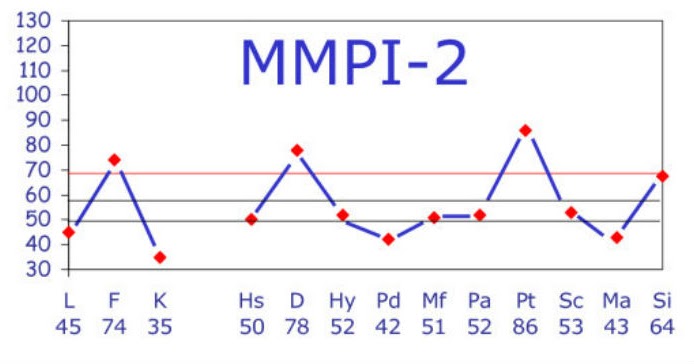
Personality profiles of offenders with increased scores on the 4th scale
[Hall H.V. Fornestic Psychology and Neuropsychology for Criminal and Civil cases. CRS Press, - 2008. pp. 402-404]
| Profile name, (frequency) | T points (MMPI-2) | Profile code | Leading Features |
| Able (17%) | Peaks up to 70 | 49 | Pleasant, seems natural, popular, impulsive, manipulative. |
| Baker (4%) | Peaks up to 70 | 42 right side down | Inadequate, anxious, defensive, repressed, dogmatic, addicted to alcohol but not to drugs. |
| Charlie (9%) | Peak over 80, slightly above 70 | 864 right lift | Aggressive rapist, misanthrope, suspicious, maladaptive, serious criminal history, alcohol and drug addiction, aloof, antagonistic ("negative"), antisocial. |
| Delta (10%) | Pd 70-80-90 | peak 4 scale with others less than 70 | Immoral, hedonistic egocentric, flamboyant, manipulative, impulsive, constant pleasure seeking. Bad relationships with authoritarians and equals, frequent offending. |
| Easy (7%) | Low profile, peaks up to 70-80 | 43 right hand reduction | Bright, stable, well educated middle class, well adapted and resourced. Has not achieved desired life goals, but has good interpersonal relationships with others Has not achieved desired life goals, but has good interpersonal relationships with others |
| Foxtrot (8%) | Peaks above 80, other scales above 70 | 489 right lift | Rigid, demonstratively daring, dominating, space-filling, cynical, anti-social. Rich criminal history, poor adaptability to places of deprivation of liberty. |
| George (7%) | Peak Lift 70+ | 4123 | Hard worker, anxious and submissive "muzhik", accepting criminal values, who grew up in a deviant family. Getting an education, dealing with basic psychological problems, and rest improve the prognosis for correcting criminal behavior. |
| How (13%) | Very high peaks over 80-90 | code not defined | Unstable, agitated, anxious, background mental disorders. Has problems in all areas of life. |
| Item (19%) | Low profile, less than 70 peaks | code not defined | Stable, functioning well with no apparent problems |
| Jupiter (3%) | Peaks over 70 | 789 sloping right up | Recovering type, but having numerous conflicts with prison staff and inmates.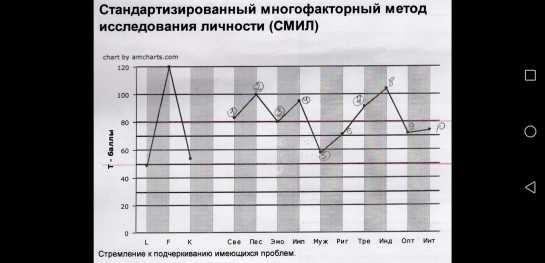 Well adapted to life in the wild. Well adapted to life in the wild. |
 The representative of the middle class, focused on achievements, occupies a good position in society.
The representative of the middle class, focused on achievements, occupies a good position in society. Elevated scores on the 4th scale in people without psychopathological disorders
Elevated scores on the 4th scale of SMIL do not in all cases suggest aggressive and antisocial tendencies. A moderate increase in the scores of the 4th scale can be observed in people without significantly pronounced or absent antisocial tendencies. In these cases, increases reflect sthenic and adaptive reactions, a temporary protective shutdown of empathy, and distancing. A moderate increase in the scale is observed in a state of stress and distress, during hard work or activities aimed at achieving a specific goal:
- When adapting to new conditions (graduates, immigrants who have changed their social stratum, environment, place of residence).
- With dissatisfaction with mass culture, politics.
- With dissatisfaction with professional activities, achievements.

- In conflicts with parents, management.
- In age-related crises.
- People in search of work, passing entrance tests and interviews.
- Recently divorced, laid-off people.
- When participating in court hearings on guardianship, division of property.
- In those who are unjustly accused, experiencing an acute sense of resentment.
For some people, an increase in the 4th scale of SMIL may be a consequence of the characteristics of professional activity or a sign of professional burnout syndrome:
- Warriors, bodyguards, employees of law enforcement agencies.
- Athletes of "extreme" sports, boxers.
- Entrepreneurs, politicians.
Character strengths in people with a moderate increase in scores on the 4th scale
In a positive way, a moderate increase in scores on the 4th MMPI scale in people with a sufficient level of education and general culture reflects such characteristics as:
- Activity and purposefulness, independence and self-sufficiency, self-confidence and self-confidence,
- Non-conformity of thinking and behavior, innovation,
- Ability to face challenges, take risks, be fearless.
- Good communication skills, ability to please and charm, flirt, friendliness.
- Developed intuition, heuristic style of thinking.
However, they may still have superficial relationships, problems with emotional involvement, empathy and deep rapprochement with people.
They work best in the absence of constant control and instructions, with the possibility of showing initiative and independence. However, their activities may be impulsive, chaotic and disorderly.
Low scores on the 4th scale of SMIL
Reduced scores on the scale (below 45 T-scores) most often do not suggest the presence of psychopathological abnormalities. Men with low scores:
- Balanced, modest, but somewhat passive.
- Have difficulty asserting themselves. They identify with their social status.
- Show reduced interest in heterosexual activity.

- Ordinary, standard, mediocre and boring, can tolerate next to the same unassuming, passive.
- Overly moralistic, self-critical and overly controlled.
- Not sad, not irritated, not touchy, well-managed, less capricious, swear less, resent less, have little chance of getting into trouble with the law.
Women with low scores:
- Cooperative, pleasant and relaxed,
- Have few problems, are not quick-tempered, not stubborn, love to be taken care of, do not argue, do not tend to shout or get angry, are less envious or jealous.
- Not overly sensitive, less hostile or unfriendly, not giving advice.
- Tend to correct other people's mistakes.
Peculiarities of indicators of the 4th SMIL scale (MMPI) in adolescents
For psychodiagnostics of adolescents under 18 years of age, the MMPI-A form is used.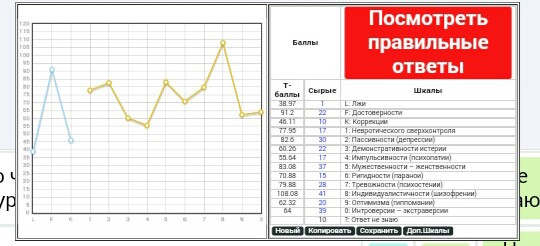 Every third teenager has elevated scores on the 4th scale. The high scores most likely reflect their often frantic attempts to form a sense of self-identity and achieve psychological independence from their parents, which is more often than not a natural phase of their development rather than a permanent, enduring trait. However, high and very high scores will still reflect the likely level of pathology. Such indicators are most often observed in "difficult" adolescents who commit antisocial acts, are in conflict with their families, have problems in educational institutions, use drugs and / or alcohol. For such teenagers, guilt for misconduct is uncharacteristic, and they are usually immune to punishment. With moderate increases, there may be problems with school, deviant behavior (lying, cheating, stealing, outbursts of anger, jealousy). Typically, an increase in rates is observed in sexually active adolescents.
Every third teenager has elevated scores on the 4th scale. The high scores most likely reflect their often frantic attempts to form a sense of self-identity and achieve psychological independence from their parents, which is more often than not a natural phase of their development rather than a permanent, enduring trait. However, high and very high scores will still reflect the likely level of pathology. Such indicators are most often observed in "difficult" adolescents who commit antisocial acts, are in conflict with their families, have problems in educational institutions, use drugs and / or alcohol. For such teenagers, guilt for misconduct is uncharacteristic, and they are usually immune to punishment. With moderate increases, there may be problems with school, deviant behavior (lying, cheating, stealing, outbursts of anger, jealousy). Typically, an increase in rates is observed in sexually active adolescents.
Young men with an increase of the 4th scale are often victims of physical violence (parents, peers), leave their homes, skip school.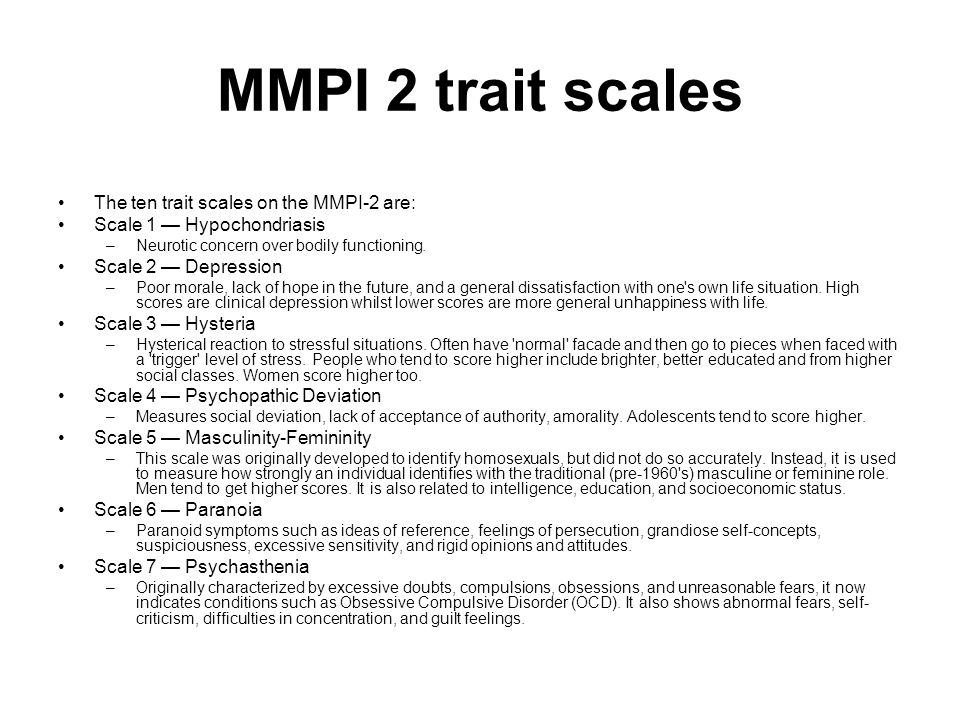 Girls are also often victims of sexual violence. Everyone, most often, lacks the motivation to receive help.
Girls are also often victims of sexual violence. Everyone, most often, lacks the motivation to receive help.
Issues of professional psychological selection
Leading EQS (professionally important qualities)
Leadership, initiative, competition, originality , patience, restraint
Recommended types of professional tasks
Solving various and non-standard tasks.
Recommended and possible areas of activity
Production, advertising, art, creative.
Professional incompetence by areas of interaction
Man - man, man - sign system
Contraindicated types of professional activity
- Work with children, teenagers.
- Work with personnel.
- Work with clients.
- Teaching and educational activities
- Monotonous and monotonous work.
- Scientific and research activities
- Work that requires endurance, stress resistance, reliability.
- Performing activity.
- Work requiring teamwork.
- Activities related to moral and material responsibility (salespeople, financiers, accountants, civil servants)
- Work that gives uncontrolled power over people (officials, deputies, regulatory bodies, law enforcement agencies).
- Work with weapons, mechanisms, vehicles.
- Operator activity. Critical zones in professional activity in relation to obstacles and leaders, non-compliance with regulations, routine, problems with bringing the case to the end
- Back
Recommendations on the style of working in a team
Individual work in a competitive environment
Recommendations on the optimal management style
External control and clear regulation of activities. Dependence of encouragement on concrete results of work.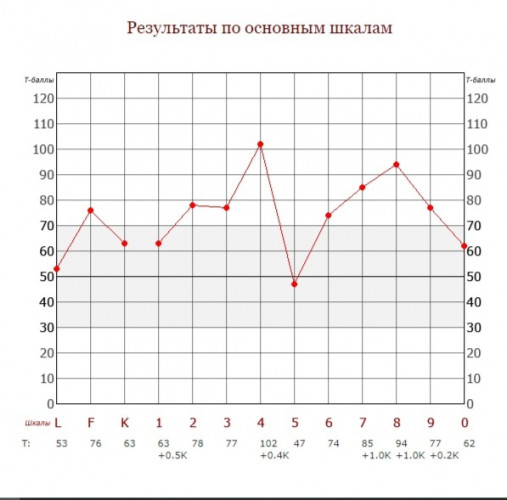 Immediate reward based on results. Unfulfilled or altered reward promises are not allowed. Emphasizing the special status of the employee.
Immediate reward based on results. Unfulfilled or altered reward promises are not allowed. Emphasizing the special status of the employee.
Recommendations for optimal working conditions
Clear regulation of the work process, place and schedules. Calm conditions and physical comfort. The possibility of obtaining aesthetic pleasure from the work performed.
Prognosis of success in psychotherapy and behavior correction
Low .
Due to their communication skills, enthusiasm and intelligence, they may initially be perceived as good candidates for psychotherapy. However, their personality is based on hostility, impulsiveness and a sense of alienation, which eventually surface. They tend to blame others for their problems. As a result, they will resist therapy and stop it as soon as possible . Part of their resistance is due to the fact that they have difficulty committing themselves to any, including therapeutic, relationships.
If they do not experience any subjective suffering (scales 2 and 7), then their motivation to change will be especially low. In addition, their initial motivation is more often not to actually change, but rather to avoid some form of punishment or trouble. In therapy, they tend to intellectualize problems and blame others.
The long-term prognosis of therapy is unsatisfactory. The short-term goal is to focus on clear changes in 's behavior (rather than just verbalizing them). External pressure can increase the motivation to undergo therapy.
Outside of therapeutic conditions, behavior modification is extremely difficult, subject only to superior force or for immediate gain. Correction in correctional institutions is almost impossible.
Andrey Demkin, MD, LCP
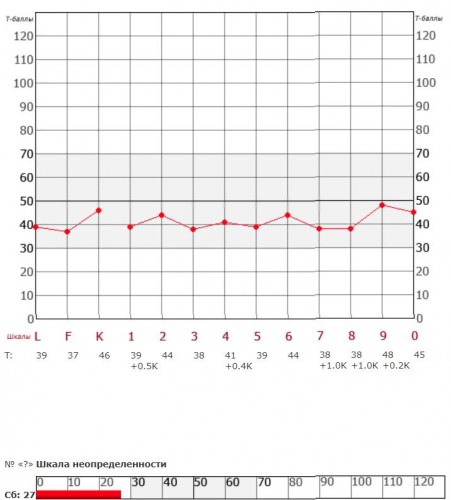
L - False F - Reliability K - Correction 1 - Hypochondria 2 - Depression 3 - Hysteria 4 - Psychopathy 6 - Paranoia 7 - Psychathenia 8 - Schizophrenia 9 - Hypomania 0 - Introversion
New Articles
Related Articles:
Dr. Andrey Demkin
Andrey Demkin
Dr. Andrey Demkin
Dr. Andrey Demkin
Dr. Andrey Demkin
Dr. Andrey Demkin
Dr. Andrey
Annotated Index of Articles of the National Psychological Journal
How Our Word Will Respond
National Psychological Journal 2022. No. 3. p.126-130
Tsukerman G.A.
moreDownload PDF
497
Life with love as the meaning of being in the existential paradigm of relationships
National Psychological Journal 2022. No. 3. c.119-125
Utrobina V.G.
moreDownload PDF
508
Ecopsychological interactions of young children with other subjects of the social environment
National Psychological Journal 2022. No. 3. p.108-118
Lidskaya E. V. Panov V.I.
V. Panov V.I.
detailsDownload PDF
467
Application of the method "Diagnostics of the mental development of children from birth to three years" in clinical psychology and psychiatry
National Psychological Journal 2022. No. 3. p.97-107
Trushkina S.V. Skoblo G.V.
moreDownload PDF
490
The Russian Museum of Childhood: On the Development of a Scientific Concept
National Psychological Journal 2022. No. 3. p.89-96
Sobkin V. S. Kalashnikova E. A. Lykova T. A.
moreDownload PDF
366
From Responsiveness to Self-Organization: A Comparison of Approaches to the Child in Waldorf and Directive Pedagogy
National Psychological Journal 2022. No. 3. p.77-88
No. 3. p.77-88
Abdulaeva E.A.
detailsDownload PDF
280
E.O. Smirnova on the moral education of children
National Psychological Journal 2022. No. 3. c.69-76
Burlakova I.A.
moreDownload PDF
290
Modern childhood and preschool education are on the protection of the rights of the child: on the occasion of the 75th anniversary of E.O. Smirnova
National Psychological Journal 2022. No. 3. p.60-68
Karabanova O.A.
moreDownload PDF
296
E.O. Smirnova in the practice of education
National Psychological Journal 2022. No. 3. c.52-59
Galiguzova L.N. Meshcheryakova S.Yu.
moreDownload PDF
274
Funny and scary in children's narratives: a cognitive aspect
National Psychological Journal 2022.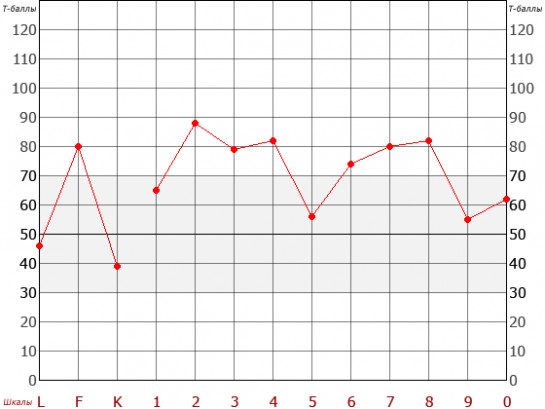 No. 3. p.44-51
No. 3. p.44-51
Shiyan O.A.
moreDownload PDF
375
Approach E.O. Smirnova to the assessment of toys for children
National Psychological Journal 2022. No. 3. c.35-43
Ryabkova I.A. Sheina E.G.
moreDownload PDF
347
The Artist in the Child
National Psychological Journal 2022. No. 3. p.26-34
Melik-Pashaev A.A.
moreDownload PDF
309
Children's play as a territory of freedom
National Psychological Journal 2022. No. 3. c.13-25
Yudina E.G.
moreDownload PDF
322
The Dialectical Structure of Preschooler Play
National Psychological Journal 2022.