Transference and countertransference in social work
Transference vs. Countertransference: What's the Difference?
Transference vs. Countertransference: What's the Difference? - Therapist Development Center Blog;
Search form
Search this site
Exam Prep Blog
- Home
- Blog
- Transference vs. Countertransference: What’s the Difference?
If you’re preparing for your ASWB Clinical Social Work Exam, transference and countertransference are two topics you definitely want to familiarize yourself with. As a coach I get a lot of questions on the differences between these two topics. Many social workers confuse the definitions of transference and countertransference and assume both warrant the same response. As we’ll discuss throughout this blog, transference and countertransference require very different actions both on the exam and in real life.
What is Transference?
Transference is a dynamic that occurs in therapy between the client and the therapist. Transference is when the client redirects (transfers) an unconscious feeling, desire, or expectation from another person toward their therapist. For example, a therapist may remind a client of her mother. Then, without the client even realizing it, she begins engaging with the therapist as she does her own mother. Transference can actually help the therapist identify patterns of relational interaction occurring in the client’s life.
Is Transference a Cause for Concern: How Should We Respond to Transference on the Exam?
When you see transference on the exam (or in real life), don’t panic! Transference is a common occurrence in therapy and is not a cause for alarm.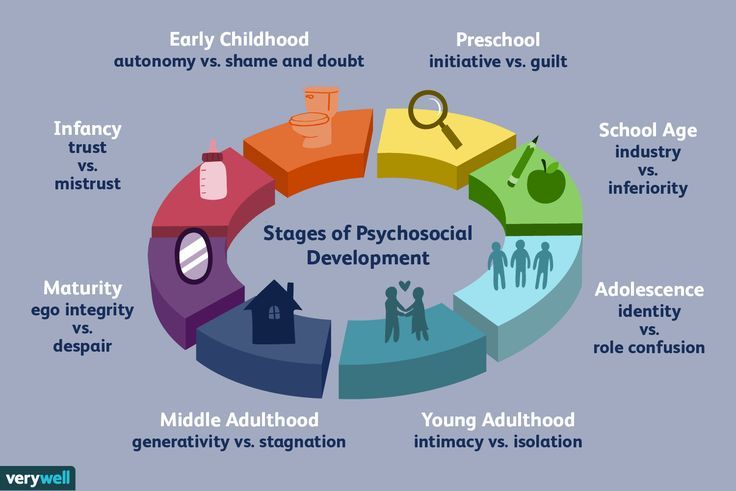 If you see a question on transference on the exam, you generally are not going to jump to anything drastic (like referring out to another therapist). Instead, you can actually use transference therapeutically. If a client is interacting with you as they interact with their mom (or dad or spouse or child or coworker, etc.), you can use this as an opportunity to explore these relational dynamics and patterns in therapy. Because transference is about
the client and not about us, it is okay to use it therapeutically.
If you see a question on transference on the exam, you generally are not going to jump to anything drastic (like referring out to another therapist). Instead, you can actually use transference therapeutically. If a client is interacting with you as they interact with their mom (or dad or spouse or child or coworker, etc.), you can use this as an opportunity to explore these relational dynamics and patterns in therapy. Because transference is about
the client and not about us, it is okay to use it therapeutically.
What is Countertransference?
So how does countertransference differ from transference? Countertransference is essentially the reverse of transference. In contrast to transference (which is about the client’s emotional reaction to the therapist), countertransference can be defined as the therapist’s emotional reaction to the client. Similarly to transference, countertransference is a common occurrence in therapy. Because of this, it is essential that we as therapists are aware of how countertransference may be showing up in therapy.![]() We may observe countertransference occurring when we have a strong emotional reaction towards a client. One common example of countertransference is when a therapist finds herself feeling protective and parental towards a client, as that client may be reminding her of her own child (or someone else she feels protective of in her life). Another example is when a client rubs you the wrong way. This may actually be you experiencing countertransference towards the client as they remind you of another person in your life who incites a similar emotional response from you.
We may observe countertransference occurring when we have a strong emotional reaction towards a client. One common example of countertransference is when a therapist finds herself feeling protective and parental towards a client, as that client may be reminding her of her own child (or someone else she feels protective of in her life). Another example is when a client rubs you the wrong way. This may actually be you experiencing countertransference towards the client as they remind you of another person in your life who incites a similar emotional response from you.
How Should We Respond to Countertransference on the Exam?
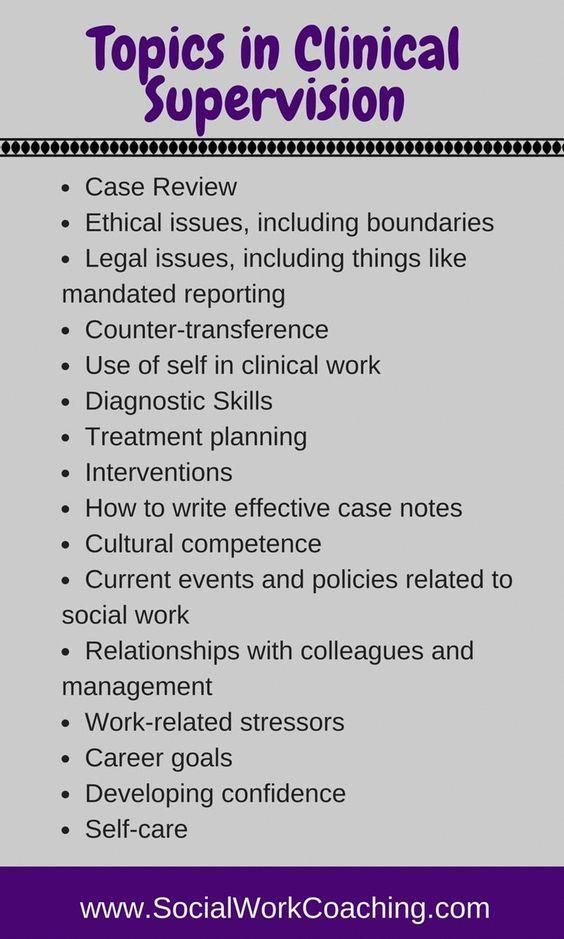
It is important to know that on the exam we are NOT going to respond to countertransference the same way we respond to transference. While we can use transference therapeutically with the client (because it is about the client) we do not use countertransference in therapy. Countertransference is about us, the therapist, so we are NOT going to discuss it with the client. On the exam, the most common FIRST action you will take in response to countertransference is seeking consultation/supervision. Seeking consultation/supervision allows you to work through your feelings of countertransference. This helps ensure our countertransference is dealt with appropriately and doesn’t impact our client or the therapeutic relationship.
On the exam, the most common FIRST action you will take in response to countertransference is seeking consultation/supervision. Seeking consultation/supervision allows you to work through your feelings of countertransference. This helps ensure our countertransference is dealt with appropriately and doesn’t impact our client or the therapeutic relationship.
Additionally, there may be times a therapist seeks their own therapy in response to countertransference issues that arise. The hope is that consultation/supervision and/or our own therapy will be enough to manage our countertransference. However, if both of these techniques are utilized and the therapist is still unable to manage their emotional reaction to the client, it may be necessary to refer the client to another therapist. Know that this is a last resort and not the first step we would take on an exam question.
Finally, we are going to use the same LMSW/LCSW practice question to look at two different ways a question on transference/countertransference could show up on the exam. Let’s see how you do on today’s practice question:
Let’s see how you do on today’s practice question:
ASWB Practice Question 1:
A social worker has been meeting with a 28-year-old woman for the past six months to work on issues of depression and suicidal ideation. The social worker observes that on days that she meets with this client, later in the day she spends a lot of time thinking about death and experiences a lower mood. What is this an example of?
A. Poor Boundaries.
B. Transference.
C. Countertransference.
D. Trauma Response.
(scroll down for answer)
The correct answer is C, countertransference. The therapist is having an emotional reaction to what the client is sharing.
ASWB Practice Question 2:
A social worker has been meeting with a 28-year-old woman for the past six months to work on issues of depression and suicidal ideation. The social worker observes that on days that she meets with this client, later in the day she spends a lot of time thinking about death and her mood is lower. What should the social worker do FIRST?
What should the social worker do FIRST?
A. Use her emotional reaction to explore how the client’s suicidal ideation may be impacting those around her.
B. Seek supervision.
C. Begin meeting with an individual therapist.
D. Refer the client to someone who specializes in depression and suicide.
(scroll down for answer)
The correct answer is B, to seek supervision. A is inappropriate because we should not be using countertransference (which is about our emotional reactions as the therapist) in therapy. Although it is possible that the therapist may begin their own therapy (C) at some point, this isn’t the FIRST thing we would do. Individual therapy is something that could be discussed in supervision as one way to manage the therapist’s countertransference. D is premature, as the therapist and client have been meeting for 6 months and have an established relationship. At this point, there is no need to refer out.
At this point, there is no need to refer out.
Masters and Clinical ASWB Exam Preparation
How did you do with these questions on transference/countertransference? Whether you’re preparing for your LMSW or LCSW exam, our ASWB social work exam prep programs will prepare you for any transference/countertransference questions on your exams. If you’re struggling with this topic (or any other topic), no worries! Every TDC customer is paired with a coach who you can email anytime you have questions or need additional explanations. TDC has helped THOUSANDS of social workers pass their ASWB clinical licensing exams and we can help you pass, too. If you haven’t already, be sure to check out our reviews from some of the THOUSANDS of social workers we have helped become LMSWs and LCSWs!
Social Work Exam
Prep Programs
Leave a Reply
Transference vs. Countertransference: What’s the big deal?
Transference vs. Countertransference: What’s the big deal? - Therapist Development Center Blog;
Search form
Search this site
Exam Prep Blog
- Home
- Blog
- Transference vs.
 Countertransference: What’s the big deal?
Countertransference: What’s the big deal?
You may be feeling overwhelmed by the number of new terms, theories, and practices you are learning. With all of the clinical information, you are consuming it can be easy to gloss over the concepts of transference and countertransference.
You know it makes sense that as a clinician you may be triggered by a client or you remind the client of someone they know. You may feel it’s common sense and it will be easy to identify in the clinical setting. However, transference and countertransference can be the areas that cause the most significant issues for you as a clinician. Here is why these concepts are a big deal and what you need to know.
What is transference?To define transference, start by thinking about the word transfer. When you transfer something, you move it from one place to another. The transference definition in psychology is when a client redirects their feelings from a significant other or person in their life to the clinician.
Think of it as the client projecting their feelings onto you as they would another person in their life. In most cases, the client experiences unconscious transference and is unaware that they are doing it. The client’s feelings transfer onto you and may be positive or negative. Transference in therapy is normal. Expect to experience transference in counseling and discuss any concerns you have with your supervisor.
Transference examples:- The client places unrealistic demands on you.
- A client admires you and tells you how much you remind them of their best friend.
- A client displaces anger onto you during a session when talking about his abusive parent.
Transference has benefits in the counseling session. The client can relax and be real during the session allowing themselves to experience growth. As a clinician, you can utilize the transference as a tool to help the client gain insight into their strength to handle situations outside of the session. You can help your client to see their reality of the event they are dealing with.
You can help your client to see their reality of the event they are dealing with.
Just as it can benefit the process, negative transference can hinder your client’s growth. If you become activated during transference and react negatively or defensively, it can stop the growth process. For example, if the client speaks to you in anger as they would to their partner and you personalize it, then you may miss an opportunity to help your client. Transference is a powerful way to improve your client’s ability to change their behavior and gain insight.
What is countertransference?Countertransference is when you as the clinician transfer your feelings onto your client. Often clinicians don’t realize when this happens. The countertransference definition can be thought of as the clinician’s response to a client’s transference.
Countertransference is an excellent reminder that clinicians are human beings with feelings and emotions. During a session, a client may open up and bare their souls causing a strong emotional reaction. The experience of the clinician during the session can affect the outcome. Clients can remind you of someone you know currently or in the past. As a clinician, you need to be aware of countertransference at all times.
The experience of the clinician during the session can affect the outcome. Clients can remind you of someone you know currently or in the past. As a clinician, you need to be aware of countertransference at all times.
- A clinician offers advice versus listening to the client’s experience.
- A clinician inappropriately discloses personal experiences during the session.
- A clinician doesn’t have boundaries with a client.
Countertransference can occur in many different ways and have adverse effects. It is a big deal when a clinician brings in their outside experiences and they lose their perspective which can lead to a reaction that hurts the client. Countertransference is common and can happen regardless of your years of clinical experience.
A crucial area to be aware of is erotic countertransference which is when the clinician experiences attraction, love, or sexual feelings towards a client. With strict ethical and legal guidelines, relationships with clients are prohibited. If you experience a strong reaction to a client, then you need to seek supervision for your countertransference.
With strict ethical and legal guidelines, relationships with clients are prohibited. If you experience a strong reaction to a client, then you need to seek supervision for your countertransference.
Your awareness of transference and countertransference is crucial in your growth as a clinician. Remember that these occurrences are normal and don’t be afraid to seek supervision when they happen. Don’t jeopardize your career as a clinician because of your pride. Your openness to accept feedback and guidance from a seasoned clinician can help you sharpen your skills in this area as well as prevent you from harming your client.
Dr. Kristie Overstreet is a clinical sexologist, certified sex therapist, licensed professional clinical counselor, author, speaker, and consultant. She holds a Ph.D. in Clinical Sexology, Master of Arts in Professional Counseling, and a Bachelor of Science in Biology. She is a licensed counselor in California, Florida, Georgia, and Louisiana. She is also a Certified Sex Therapist and Certified Addiction Professional.![]() She has over 12 years of clinical experience specializing in sex therapy, transgender healthcare, relationships, and helping counselors build their private practice. She is president of the Therapy Department, a private practice that provides counseling, training, speaking, and consulting services across the United States. For more information about Dr. Kristie’s work visit www.KristieOverstreet.com.
She has over 12 years of clinical experience specializing in sex therapy, transgender healthcare, relationships, and helping counselors build their private practice. She is president of the Therapy Department, a private practice that provides counseling, training, speaking, and consulting services across the United States. For more information about Dr. Kristie’s work visit www.KristieOverstreet.com.
Social Work Exam
Prep Programs MFT Exam
Prep Programs
Leave a Reply
Topic 5. Psychodynamic approach to social work
Psychology of personality
-
Criticism psychodynamic work
Literature:
Payne M. Social work: modern theory: educational allowance / Malcolm Payne; ed. J. Kampling; per. from English. – M., 2007
Psychodynamic approaches are considered individualistic, social changes they almost do not affect.
This approach based on the teachings of Freud and his followers. The name itself "psychodynamic approach" is associated with that builds dependency behavior from changes in the psyche.
The name itself "psychodynamic approach" is associated with that builds dependency behavior from changes in the psyche.
Psychodynamic theory explains how the mind stimulates action, psyche and behavior affect the social environment and are influenced by him.
These theories were tangible and influenced the theory social work in the 30-50s. 20th century. The psychodynamic approach presents is the main traditional social work to which many relate other theories and individual elements which continues to be used in practice.
Foreign authors highlight a number of practical issues and concepts.
-
Anxiety and uncertainty, the source of which is an inadequate resolution early childhood problems lead to the emergence of strong emotions, aggression, anger and love.
-
Coping - ability to deal with current problems without anxiety.
-
Protection and resistance – psychological barriers in overcoming life difficulties associated with inadequate problem solving past.

-
Transfer and countertransference in social work means the influence of past experience on behavioral models of the present and appear in the behavior of the client relation to the specialist. Specialist helps people see the connection problems of the past and present, and find real ways to overcome mental and practical barriers on the way to effective action.
-
In relationship with people are modeled effectively thinking and self-control, and gaining knowledge and confidence in understanding psychological problems. Modern authors often describe psychodynamic work "relational", by analogy with concept of "objective relations" in psychodynamic theory.
Psychoanalytic theory consists of three parts: theory human development, psychology personality and abnormal behavior, and as well as treatment theories. At the heart of the overall theory lie two fundamental ideas:
-
mental determinism - the principle that actions or behavior doesn't just happen, but arise as a result of the process human thinking;
-
performance about the unconscious - the notion that some forms of thinking and mental activity hidden from our consciousness.

All these ideas are widely known today. Yes, both principles accept that joke clauses reflect hidden or unconscious confusion in human thinking. However, generally accepted values are not always reveal the complexity of psychodynamic ideas. Thus, in the literature there is an example the term "unconscious" to demonstrate complexity of psychodynamic ideas. Resistance occurs at the moment when thoughts appear and feelings that are incompatible with others ideas that matter to us. IN In this case, the mind does not let into consciousness rejected thoughts. It's being done through a process called repression. Many repressed thoughts are dynamic they spur us to action, even if we are not aware of them. Psychodynamic the unconscious is made up of violently suppressed thoughts, which exist regardless of whether we are aware of them or not, and which often deeply hidden. Also important is concept aggression , denoting the process when people direct their destructive impulses against other people.
In psychoanalytic theories development children are expected to go through a series stages of development. These stages include various desires (instincts), which imply mental satisfaction pressure physiological needs such like hunger or thirst. The existence of such needs creates tension, or libido , that gives energy for action, realization of needs. In building attraction plays a very important role sexual tension - physiological manifestation, which is typical even for little children.
At every stage a certain type of behavior is formed, but in the process of moving to a new stage behavior associated with previous stages. Yes, early stage babies get satisfaction through the sucking process (for example, mother's breasts to satisfy need for food). At a later stages of sucking can also bring satisfaction (e.g. smoking cigarettes, sucking on sweets, etc.). Together meanwhile, adults have a wider range of behavioral manifestations gives them freedom of choice. Some people unconsciously choose the type of behavior, associated with certain stages. They are driven by the desire for satisfaction. any need, and therefore cannot use the entire repertoire behavior. This process is called fixation.
Some people unconsciously choose the type of behavior, associated with certain stages. They are driven by the desire for satisfaction. any need, and therefore cannot use the entire repertoire behavior. This process is called fixation.
At stage primary narcissism children only want to satisfy own needs. Thanks to social interaction before all communication with parents, they learn come to a compromise. On each stage focuses on separate need: oral (hunger), anal (excretion), phallic (identification with parents of the same sex), Oedipal (attraction to the parent opposite sex), latent (controlled cravings through permission Oedipus complex) and pubertal (social learning). The author of the concept about stages of development is Erickson. He suggested that at every stage rational consciousness overcomes crisis of growing up the circumstances of our lives. This concept of great importance in social work, especially in times of crisis interventions, draws attention to impact of cultural and social factors rather than intrinsic drives.
With stages of development related concept regression. Regression occurs when people who have reached advanced stages under the influence of stress return to behavior characteristic of earlier stages. Regression is different from fixation. In the latter case, individuals are unable to get out of the behavior inherent in the early stages.
In psychoanalytic personality theory is that people are a complex of desires, creating Id (It), indefinite pressure coming from the unknown source. It makes us act to satisfy our needs, but our actions do not always lead to expected results. Here arises The ego that shapes our perception and actions in relation to the environment the world. The ego controls the id. For example, children control fecal excretion, since the ego teaches that inappropriate actions are inconvenient. The ego controls the relationship people and things around us peace, i.e. object relations . The super ego develops general moral principles that guide action Ego.
An important property personality is the ability of the ego to conflict management. Ego Striving and Super Ego to control the It arising under the influence of social responsibility, provokes further conflicts. The result of such conflicts is alarm. The ego deals with anxiety by activating various defense mechanisms. mentioned above repression is one of them. Other important defense mechanisms are:
-
projection – unconscious thoughts that the ego seeks to protect. He and projected our consciousness on another person or object;
-
splitting - presence in various layers of the psyche conflicting thoughts and feelings whose impact leads to unpredictable consequences;
-
sublimation – redirection of energy (coming from It), originally aimed at unwanted behavior (often sexual), to more social acceptable actions:
-
rationalization - persuasion in the validity of the reasons causing certain actions, and emotional suppression of unreasonable reasons behavior.

Last Labor Freud focused on relationships Ego with objects. This topic has been developed and after his death (in the work of Anna Freud and Hartman). in personality psychology and object relations theory shows that children from an early age have ability to interact with external world (object relations). Development Ego denotes the growth of our ability learn from experience, based on rational possibilities of our consciousness, such as thinking (cognition), perception, memory.
Some theorists and practice of the psychodynamic approach had a significant impact on social work. Particularly interesting works by M. Klein, Salzberger-Wittenberg, Winnicot and Bowlby. These authors drew special attention to working with children. Klein discusses two emotional life "positions" that appear in early childhood: persecution position, arising from the fear of loneliness and inability to survive, and depression position associated with the fear of inflicting harm to the mother (appears later). Experience these two positions helps people learn to accept duality and avoid destructiveness. In work Winnicot analyzed object relationships are how children learn adapt by focusing less on the inner world and developing the ability interaction with the outside world. Bowlby translated the psychoanalytic mother-child relationship problem early stage research area and theoretical understanding of maternal deprivation. maternal deprivation, those. limiting the child's contact with mother, leads to developmental delay baby's personality. Later in the area research has formed a theory about the meaning of attachment. Attachment considered primarily as close relationship with mother, but not only. Attachment experience has influence on the development of subsequent relationships with other people. Consequences of loss attachments are extremely serious, whether death or separation from someone parents as a result of divorce. Proved that deprivation and the difficulties of early period are the most destructive for the child and have a negative impact on later human life.
Experience these two positions helps people learn to accept duality and avoid destructiveness. In work Winnicot analyzed object relationships are how children learn adapt by focusing less on the inner world and developing the ability interaction with the outside world. Bowlby translated the psychoanalytic mother-child relationship problem early stage research area and theoretical understanding of maternal deprivation. maternal deprivation, those. limiting the child's contact with mother, leads to developmental delay baby's personality. Later in the area research has formed a theory about the meaning of attachment. Attachment considered primarily as close relationship with mother, but not only. Attachment experience has influence on the development of subsequent relationships with other people. Consequences of loss attachments are extremely serious, whether death or separation from someone parents as a result of divorce. Proved that deprivation and the difficulties of early period are the most destructive for the child and have a negative impact on later human life. Here, however, plays a role not only maternal deprivation, but also the nature of the relationship between children and parents, and other factors, including the social environment. There are many social and psychological factors that protect from the destructive effects of deprivation.
Here, however, plays a role not only maternal deprivation, but also the nature of the relationship between children and parents, and other factors, including the social environment. There are many social and psychological factors that protect from the destructive effects of deprivation.
In psychoanalysis the theme of loss is considered very significant. Several concepts have been developed experiences of loss and grief. Mourning regarded as a response to any kind loss, not just the death of a loved one person. Parkes considers experience loss in many situations as a regression on children's experiences of stress about loss. Pinkus proves that in typical family reactions to death may be hidden feelings associated with the past relationships. Intensity of emotions of grief are a special topic in psychoanalysis. However, Smith believes that many actions in situations of loss and loss are explained social expectations of due behavior in such cases. She claims that the phenomenological or existential interpretation more suitable for explaining the situation loss.
Modern psychoanalytic works intersect with sociological concepts, especially with the idea that people are part of social systems and play social roles. recent research, written in the tradition of object relations, in particular the work of Kogut, show that children form perception his "I" and his difference from the surrounding the world at a very early age. Psychology "I" has been popular in literature since 80s 20th century
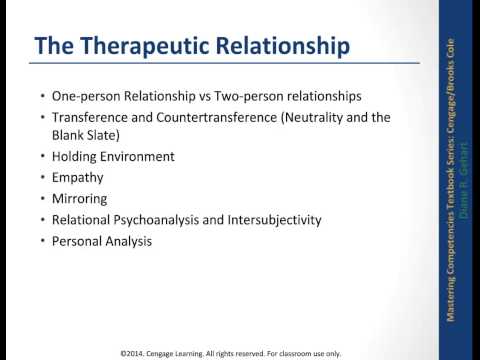
Treatment Theory in classical psychoanalysis built that therapists should be "empty screens" and strive for the greatest anonymity so that patients projected their fantasies onto them. Transfer occurs when the patient transfers unconscious feelings to his parents to the therapist and perceives him as one of them. Transfer is a way to release unconscious ideas. With the help of stimulation transfer reveals conflicts that stem from the difficulties of early relationships with parents and complexity of behavior in the present. IN social work these ideas are used in the sense that emotional memories of past relationships affect our behavior in the present, especially on relations with people. Countertransference occurs when psychoanalyst reacts irrationally on patients, bringing to the relationship past experience.
Countertransference occurs when psychoanalyst reacts irrationally on patients, bringing to the relationship past experience.
Some psychoanalytic techniques are directed to release hidden thoughts and feelings. Considered unacceptable behavior can be caused by depressed conflicts that come to the surface in a variety of ways. Opening reasons requires extraordinary efforts. Being at least once identified and correctly understood, conflicts no longer cause behavioral difficulties. Thus, traditional psychoanalytic tradition is connected with the motivation in people insights about their repressed feelings. Particular attention is paid to how people build relationships with the outside world, developing rational control skills over your life.
Influence psychodynamic theories for social work clearly exists. Understanding Psychodynamic Theory is a prerequisite for the analysis of other theories of social work because it influence is very widespread. Various scientific schools and practical technologies. Except In addition, there is interest in theorists who have departed far from Freud and main directions of psychoanalysis. Contemporary psychoanalytic theory no longer recognizes attraction as the main motive of behavior (Lounstein, 1985) and focuses on how the individual interacts with the social world; this theory has become social rather than biological. Brealey analyzes the main themes of psychoanalysis with the help of three key connections: between personality and significant others, between past and present experiences, between inner and external reality. Rasmusen and the Mishnah (2003) argue that in psychodynamic special attention to social work given to the social context interpersonal relationships through why approaches to perception are multiplying reality, as well as their differences. On against this background, the development of psychology personality (Goldstein), which is basis of the relational model (Horowitz, Meyer, Cooper, Lesser), aimed at strengthening interpersonal relationships.
Except In addition, there is interest in theorists who have departed far from Freud and main directions of psychoanalysis. Contemporary psychoanalytic theory no longer recognizes attraction as the main motive of behavior (Lounstein, 1985) and focuses on how the individual interacts with the social world; this theory has become social rather than biological. Brealey analyzes the main themes of psychoanalysis with the help of three key connections: between personality and significant others, between past and present experiences, between inner and external reality. Rasmusen and the Mishnah (2003) argue that in psychodynamic special attention to social work given to the social context interpersonal relationships through why approaches to perception are multiplying reality, as well as their differences. On against this background, the development of psychology personality (Goldstein), which is basis of the relational model (Horowitz, Meyer, Cooper, Lesser), aimed at strengthening interpersonal relationships. Emphasis on the interaction of the individual with environment means attention to intersubjectivity, i.e. interpersonal perception and response, and linguistic expression of human relationships. Psychology of Personality is the basis of ecosystem theory (Jemaine, Siporin) and crisis intervention.
Emphasis on the interaction of the individual with environment means attention to intersubjectivity, i.e. interpersonal perception and response, and linguistic expression of human relationships. Psychology of Personality is the basis of ecosystem theory (Jemaine, Siporin) and crisis intervention.
Role assessment psychoanalysis in social work indicates that psychoanalysis widely used in social work and in different countries there are various theoretical schools. Psychology personalities, for example, the most popular in the USA, object relations theory developed in the UK and the US.
Meaning Psychodynamic Theory .
Researchers distinguish three periods of influence of psychoanalysis on social work theory. Until the 1920s in the USA and under 1930s in the UK it the impact was minor. Then up until the 1960s. psychoanalysis took dominant position. During this period, his influence was so significant that formed with his using approaches applied in the social work to this day. After the 1960s psychoanalysis coexisted alongside other theories, although they were used only individual specialists. Some the authors consider the influence of psychoanalysis as "legacy". Influence of psychoanalysis is rather complex and indirect and is related to the role of Freud's research.
After the 1960s psychoanalysis coexisted alongside other theories, although they were used only individual specialists. Some the authors consider the influence of psychoanalysis as "legacy". Influence of psychoanalysis is rather complex and indirect and is related to the role of Freud's research.
Psychodynamic therapy caused an emergence in the social tolerant and open style work relationships, in which great importance attached to the client's hearing and in general - relationships, as opposed to directive, controlling style. She also contributed to the emergence striving to understand the individual, and not just take some action. Thanks to psychodynamic theory in social work, the emphasis shifted from events and thoughts on the feelings and forms of the unconscious. Many concepts, such as "unconscious", "insight", "aggression", "conflict", "anxiety", "relationship with mother", "transfer", borrowed from psychoanalytic theories. These terms form the general language vocabulary that is understood both in social work and in everyday life life. Significance of psychodynamic approach is constantly being confirmed practice. Important for social work emphasis on childhood, early relationships with people and maternal deprivations borrowed from psychodynamic theories, led to growing popularity of attachment theory. Attention of social workers to the study of mental and behavioral violations is explained by the close relationship social work with psychiatry and psychodynamic therapy 1920-1930s The increased attention of specialists in areas of social work to psychological and emotional factor (compared to with social factors) is also explained influenced by psychodynamic theory.
Significance of psychodynamic approach is constantly being confirmed practice. Important for social work emphasis on childhood, early relationships with people and maternal deprivations borrowed from psychodynamic theories, led to growing popularity of attachment theory. Attention of social workers to the study of mental and behavioral violations is explained by the close relationship social work with psychiatry and psychodynamic therapy 1920-1930s The increased attention of specialists in areas of social work to psychological and emotional factor (compared to with social factors) is also explained influenced by psychodynamic theory.
Transference and countertransference relationships: a mistake or inevitability of psychoanalytic practice
In the process of psychoanalytic practice between a whole system of relationships arises between the analyst and the client, in which the emotional component either contributes to the successful therapy or interfere with it. D. Pines writes about this: “They enter into an intense relationship with each other who bring their life experience, their perceived and unconscious feelings, dreams and desires, as well as circumstances of today's life, flowing outside the analytic space. <> ... the special structure of psychoanalysis, the conditions, imposed on the analyst in order to advance therapeutic work with problems of the patient, turn analytic interaction into a very special process. The analyst invites the patient to enter into fairly close and trusting relationship with him and at the same time time strictly excludes the possibility of physical contact and physical communication with the patient. He encourages the patient to open up, but himself, as far as possible, hides his feelings, facilitating the manifestation feelings of the patient associated with the most significant figures in his past and present, which he projects onto the analyst" [4, p. 69].
<> ... the special structure of psychoanalysis, the conditions, imposed on the analyst in order to advance therapeutic work with problems of the patient, turn analytic interaction into a very special process. The analyst invites the patient to enter into fairly close and trusting relationship with him and at the same time time strictly excludes the possibility of physical contact and physical communication with the patient. He encourages the patient to open up, but himself, as far as possible, hides his feelings, facilitating the manifestation feelings of the patient associated with the most significant figures in his past and present, which he projects onto the analyst" [4, p. 69].
These feelings experienced back in 1895 S. Freud gave the name - "transfer", which he regarded as reactions (direct allusions) patient on the personality of the analyst and the analyst's awareness of these reactions in its address, as a result of the influence of the repressed or suppressed libidinal feelings of the patient, and also as a source of resistance analytical process. In particular, he writes: "The one whose the need for love is not fully satisfied in reality, compelled to turn on every new face he encounters his libidinal hopes, and it is very likely that in this direction both parts of his libido are involved: both accessible to consciousness and unconscious. Therefore, it is quite natural and understandable that ready, the waiting active force of the libido, partly unsatisfied, also refers to the personality of the doctor" [9, With. 293].
In particular, he writes: "The one whose the need for love is not fully satisfied in reality, compelled to turn on every new face he encounters his libidinal hopes, and it is very likely that in this direction both parts of his libido are involved: both accessible to consciousness and unconscious. Therefore, it is quite natural and understandable that ready, the waiting active force of the libido, partly unsatisfied, also refers to the personality of the doctor" [9, With. 293].
Z. Freud distinguished transference positive and negative. Positive transfer was interpreted as a transfer to the psychoanalyst of various kinds of friendly and tender feelings acceptable to consciousness, with the continuation of these feelings in unconscious, negative - as a transfer to the psychoanalyst various kinds of hostile feelings and negative emotions [8].
With the accumulation of clinical experience, many analysts began to consider transference as the most significant means of understanding mental reality of the patient, in contrast to the initial understanding of his Z. Freud as resistance.
Freud as resistance.
In his work Psychoanalytic Dialogue: transference and countertransference” D. Pines analyzes later transfer definitions and indicates their extended and refined interpretation. So, according to R. Greenson, transference is “experiencing in present feelings, desires, relationships, fantasies and aspirations to defend themselves in relation to a person for whom all these feelings are not can relate, because they are repetition, a mixture of reactions, arising from attitudes towards persons who played an important role in human life during his early childhood”, i.e. so that the reaction can be considered a transference, it must be a repetition of the past and not have relationship to the present. In the interpretation of transfer W. Hoffer emphasizes the influence of childhood on the whole life of a person as a whole, arguing this position with the results of scientific observations, according to which people, building their relationships with real or imagined, positive or negative (and maybe ambivalent) objects, bring their memories of the most significant events past and thus change relationships with real objects, trying to build them in accordance with their life experience [4].
However, to date, a certain part of practitioners psychoanalysts recognizes the importance of mental changes arising at each stage of human maturation throughout life cycle after childhood - in youth, maturity and old age, without detracting from the influence of the past on the present and future. Based on this, Modern psychoanalysts are expanding their understanding of transference. During an analytic session, the patient in his communication with the analyst can relive feelings which he experienced in relation to significant people, not only from his childhood, but also from other age periods, including recent life events and the significance of certain persons in them.
If we turn to modern psychological, psychoanalytic and philosophical dictionaries, then the analysis of the definitions of concepts available there transfer, transfer, transfer shows the presence of largely coinciding interpretations, in which not only the influence of childhood experience is mentioned. So, in the latest philosophical dictionary and Dictionary of practical psychologist "transfer" (transfer; transfer) is described as "appearing in psychoanalysis the process and result of the spontaneous relationship of man to man, characterized by an unconscious transfer to him of the formed as a result of previous interactions with other people, positive or negative feelings [3, p. 512; 8, p. 219]. IN psychological dictionary-reference transfer (shift of affect) correlates with situation in which the patient recreates feelings and conflicts from one's own life (especially early feelings about relation to parents), and then transfers them to the therapist" [6, p. 220]. In the Dictionary of Analytical psychology, transference is interpreted as a “private a case of projection when describing an unconscious emotional connection, arising in the analysand in relation to the psychoanalyst" [1, With. 72]. This once again confirms that the psychoanalytic practice of recent decades has contributed certain changes in the understanding of the transfer phenomenon.
So, in the latest philosophical dictionary and Dictionary of practical psychologist "transfer" (transfer; transfer) is described as "appearing in psychoanalysis the process and result of the spontaneous relationship of man to man, characterized by an unconscious transfer to him of the formed as a result of previous interactions with other people, positive or negative feelings [3, p. 512; 8, p. 219]. IN psychological dictionary-reference transfer (shift of affect) correlates with situation in which the patient recreates feelings and conflicts from one's own life (especially early feelings about relation to parents), and then transfers them to the therapist" [6, p. 220]. In the Dictionary of Analytical psychology, transference is interpreted as a “private a case of projection when describing an unconscious emotional connection, arising in the analysand in relation to the psychoanalyst" [1, With. 72]. This once again confirms that the psychoanalytic practice of recent decades has contributed certain changes in the understanding of the transfer phenomenon. She also allowed us to take a different look at those problems that are carefully analyzed by Z. Freud and K. Jung when interpreting transference, understanding the essence of its nature and evaluation for psychotherapeutic practice is a pattern or a mistake that must be eradicate.
She also allowed us to take a different look at those problems that are carefully analyzed by Z. Freud and K. Jung when interpreting transference, understanding the essence of its nature and evaluation for psychotherapeutic practice is a pattern or a mistake that must be eradicate.
Z. Freud noted that the analytical process does not create a transfer (transference), but detects it. At This Z. Freud, as a practicing psychotherapist, was puzzled by several observations. First, he found that the transfer is more intense manifests itself in "analyzed persons" than in "not analyzed". Secondly, in the situation of analysis, the transference becomes the strongest resistance, "while outside analysis in transference, we must recognize the bearer of healing - guarantee of complete success” [9, With. 294]. So automatically arose the question is why in psychoanalysis the strongest lever of success becomes the strongest means of resistance? Isn't it for psychoanalysis "huge methodological damage"?
According to Freud, transference comes from erotic sources and, as a rule, distinctly dyed sexy. Transference acts the stronger, the less about guess it. K. Jung is not considered transference only as a projection of infantile-erotic fantasies, although they may be present at the beginning of the analysis, but subsequently, by reduction, they disintegrate and disappear. And then the main goal 9 becomes the theme and guiding thread0051 transfers. "Exclusively sexual interpretation of dreams and fantasies - serious violence against the psychological material of the patient: infantile sexual fantasy is by no means the whole story, but psychological material also contains a creative element, a goal which to outline the way out of the neurosis” [cit. according to 1, p. 73].
Transference acts the stronger, the less about guess it. K. Jung is not considered transference only as a projection of infantile-erotic fantasies, although they may be present at the beginning of the analysis, but subsequently, by reduction, they disintegrate and disappear. And then the main goal 9 becomes the theme and guiding thread0051 transfers. "Exclusively sexual interpretation of dreams and fantasies - serious violence against the psychological material of the patient: infantile sexual fantasy is by no means the whole story, but psychological material also contains a creative element, a goal which to outline the way out of the neurosis” [cit. according to 1, p. 73].
According to Z. Freud, “the most great difficulty for the psychoanalyst is the need to overcome the phenomena of transference, but not to forget that they do us an invaluable service by making real and explicit hidden and forgotten love feelings of the patient" [9, With. 301]. Transfer conjugation with resistance Z. Freud explains as follows: “Resistance at each step accompanies the treatment: each thought, taken separately, is sick, his every act has to be reckoned with resistances, since they are a compromise between forces, striving for recovery and opposing it" [9, With. 296]. And further: “... Transferring to doctor is only suitable for resistance in treatment, insofar as it is negative transfer or positive transfer repressed erotic mental movements. Eliminating theme migration that we make it conscious, we free the doctor's personality only from both of these components of feeling” [9, With. 298-299].
Freud explains as follows: “Resistance at each step accompanies the treatment: each thought, taken separately, is sick, his every act has to be reckoned with resistances, since they are a compromise between forces, striving for recovery and opposing it" [9, With. 296]. And further: “... Transferring to doctor is only suitable for resistance in treatment, insofar as it is negative transfer or positive transfer repressed erotic mental movements. Eliminating theme migration that we make it conscious, we free the doctor's personality only from both of these components of feeling” [9, With. 298-299].
K. Jung also considers the transfer phenomenon as "an inevitable companion of any meaningful analysis, since it is necessary that the doctor could, as clearly as possible, see the direction personal development of the patient”, while indicating an important feature of the analyst's work with the phenomenon of transference: "We are working not with a “transfer to the analyst”, but against him and, despite on him" [cit. according to 1, p. 72]. But in working with transference, according to K. Jung, it is important to take into account its modality (valency) and the patient's personality type. "For one type personality (called infantile-protesting) positive transfer is - to begin with - an important achievement with a healing effect; for another (infantile obedient) he - a dangerous apostasy, a convenient way to avoid, elude life obligations. For the first, negative carry means expansion of disobedience, and therefore apostasy and evasion of life obligations, for the second it is step towards healing” [Ibid.].
according to 1, p. 72]. But in working with transference, according to K. Jung, it is important to take into account its modality (valency) and the patient's personality type. "For one type personality (called infantile-protesting) positive transfer is - to begin with - an important achievement with a healing effect; for another (infantile obedient) he - a dangerous apostasy, a convenient way to avoid, elude life obligations. For the first, negative carry means expansion of disobedience, and therefore apostasy and evasion of life obligations, for the second it is step towards healing” [Ibid.].
In case of manifestation of transference, professionally a trained psychoanalyst should help the patient bring together consciousness and the unconscious, and in this way arrive at a new attitude. IN in psychoanalysis, the patient sees the face that seems to the patient promising renewal of his life attitude; he aspires to change, which is vital to him, even if he does not realizes that he is doing just that. Therefore, the patient "sticks" to the analyst, who seems to be an indispensable figure, absolutely necessary for life.
Therefore, the patient "sticks" to the analyst, who seems to be an indispensable figure, absolutely necessary for life.
P. King as professional analyst considers his true understanding of the phenomenon of transference, which includes not only the awareness of who or what symbolizes analyst, but also an awareness of how, from an emotional point of view, the patient perceives this or that person or object from the past, experiencing certain emotions towards him at that time, especially during the period infancy and early childhood. She also emphasized the importance determining for the analyst himself what traits of his parents the patient reproduces in the transference at the moment and ascribes them to the analyst [10].
In general, assess the occurrence of transfer in psychotherapeutic practice is possible, the following statement by K. Jung: “Transfer is never an advantage, it is always a hindrance. Transference medical treatment provides the patient with invaluable the opportunity to withdraw back their projections, to benefit from their losses and integrate your personality” [1, p. 73]. Therefore, the phenomenon of transfer is inevitable, in many ways it contributes therapy, only the methods used to work can be erroneous with him.
73]. Therefore, the phenomenon of transfer is inevitable, in many ways it contributes therapy, only the methods used to work can be erroneous with him.
But speaking of transference as a phenomenon that accompanies psychotherapeutic process, it is important to mention such a phenomenon as countertransference and evaluate its significance. Let's turn to dictionaries. The psychological dictionary-reference book explains this phenomenon as follows: “When conducting psychoanalysis The therapist may unconsciously project onto the patient's feelings or conflicts arising in his own life. Absolutely necessary. so that the therapist is aware of this possibility and not allowed its implementation” [6, p. 143]. The Dictionary of Psychoanalysis uses the term "countertransference" and is interpreted as "a set of unconscious reactions analytics on the personality of the analyzed person and especially on his transfer” [2, p. 212]. In the Dictionary of Analytical Psychology, countertransference (counter transfer) – “a special case of projection, used for description unconscious emotional response - the analyst's reaction to analysand in therapeutic relationship” [1, p. 52]. .
52]. .
In other words, countertransference can be defined as the analyst's observation and awareness of his own unconscious emotional reaction when communicating with one or another patient. The phenomenon of countertransference is also in most cases naturally. D. Pines finds the reason for the appearance of countertransference in the following: “... conflicts between children and adolescents age, living in an adult, can re-remind themselves and manifest itself in both the analyst and the patient, because now we view psychoanalysis as a two-way process in which two participants are involved” [4, p. 70].
Freud sees countertransference as a result "the influence of the patient on the unconscious feelings of the doctor" and emphasizes that "no analyst is able to go beyond the limits of what his own complexes and internal resistances", and hence the need for psychoanalyst to undergo a personal analysis [2, p. 212]. In 1912 Z. Freud wrote that the analyst should behave like a "surgeon who puts aside all his own feelings, including human sympathy, and concentrates his consciousness on one the sole purpose is to carry out the operation as best as possible. ” [eleven].
” [eleven].
According to modern analysts, in particular D. Pines, psychoanalysts must capture subtle emotional nuances own reaction, i.e. "distinguish identification with the patient and empathy for him”, in addition, they must “be aware that what is transferred to the patient and what the patient transfers to them as analytics” [4, p. 76]. Thus, when dealing with patients whose life experience was traumatic and whose pain is unbearable, analyst is forced to experience intolerable countertransference and the associated painful emotional state. However, as D. Pines points out, “It is impossible to experience unbearable feelings every time, arising from countertransference. Includes natural protection against someone else's pain, the countertransference meets with resistance. All that is possible to do in this situation is to accompany the patient on his journey into the past and keep him in the present in the hope that he can learn to live again” [Ibid.].
P. King notes the importance of distinguishing countertransference as pathological phenomenon and how the analyst's emotional response on communication with the patient, on various forms of transfer. It defines the analyst's emotional reaction as "the analyst's perception of feelings and moods that have no relationship to his own life, even alien to his usual way of responding, and those that, being placed in the context of all information reported by the patient and psychoanalytic environment, reveal the transference, as they were consciously or unconsciously expressed by the patient" [10, p. 332].
King notes the importance of distinguishing countertransference as pathological phenomenon and how the analyst's emotional response on communication with the patient, on various forms of transfer. It defines the analyst's emotional reaction as "the analyst's perception of feelings and moods that have no relationship to his own life, even alien to his usual way of responding, and those that, being placed in the context of all information reported by the patient and psychoanalytic environment, reveal the transference, as they were consciously or unconsciously expressed by the patient" [10, p. 332].
Important for the psychoanalyst is the ability to remain in a neutral positions, which Z. Freud also pointed out. However, experience shows that it is difficult for the psychoanalyst to be neutral, so he must constantly to catch the boundary between one's own feelings and feelings patients, “the analyst must be aware of the possibility over-identification with the patient and in the probability of projection onto patient of their own problems" [4, p.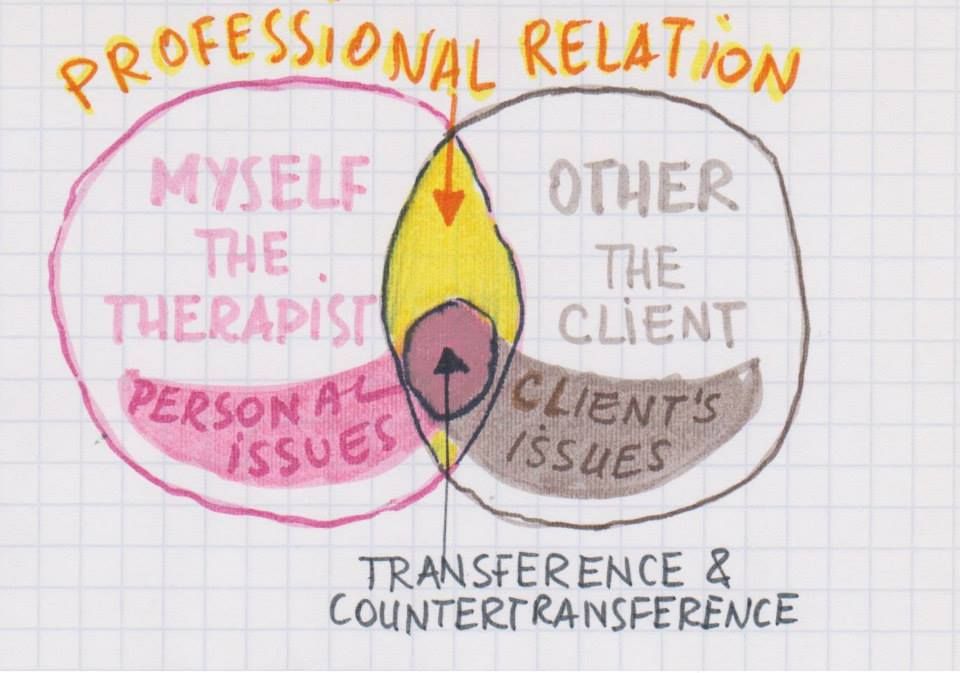 72].
72].
There are two possible exits when a transference or countertransference. The patient can accept the transfer or provide strong resistance to him, resisting the repetition of painful childhood experiences related to the relationship between persons significant to the patient. The therapist may also discover in himself strong unconscious resistance to accepting the countertransference that can touch his own deep-seated feelings and experiences. For example, if the patient in his transference demonstrates too positive assessment of the analyst and accepts all of his interpretation, the analyst may be misled by the sensation that this patient is "good" and the psychoanalysis is proceeding correctly.
To help the analyst cope with the phenomenon of countertransference, undergoing a personal analysis or cooperating with a supervisor. The most important task of supervision, from the point of view of D. Pines, is to teach future professionals to capture their own contribution to therapeutic interaction resulting from the transfer to analysis of the patient's feelings.
However, the significance of transference and countertransference for psychotherapeutic practice is essential. Modern researchers of this problem, they are unanimous in their opinion that the transfer and countertransference continues to be intriguing and confusing phenomena of therapeutic work. However, they are the ones who make analytics to constantly explore and discover your inner world and the inner world of the patient. D. Pines is right about this notes that "careful observation of the vast diversity transference and countertransference phenomena that are revealed during psychoanalysis, is one of the most creative and exciting aspects” of the work of a psychoanalyst.
- Literature:
-
Zelensky, V. Dictionary of analytical psychology / V. Zelensky. - M.: Higher. school, 2000. - 120 p.
-
Laplanche, J. Dictionary of Psychoanalysis / J. Laplanche, J.-B. Pontalis. - M.: Higher. school, 1996. - 623 p.
-
The latest philosophical dictionary / Comp.
 A.A. Gritsanov. - Mn.: Ed. V.M. Skakun, 1998. - 896 p.
A.A. Gritsanov. - Mn.: Ed. V.M. Skakun, 1998. - 896 p. -
Pines, D. Psychoanalytic dialogue: transference and countertransference / D. Pines // Questions of psychology. - 1997. - No. 6 - S. 69–76.
-
Psychological dictionary / under the general scientific. ed. P.S. Gurevich. - M.: OLMA Media Group, OLMA PRESS Education, 2007. - 800 p.
-
Psychology. A - Z: Dictionary-reference book / Per. from English. K. S. Tkachenko. - M.: FAIR-PRESS, 2000. - 448 p.
-
Psychology. A - Z: Dictionary-reference book / Per. from English. K. S. Tkachenko. - M.: FAIR-PRESS, 2000. - 448 p.
-
Dictionary of practical psychologist / comp. S.Yu. Golovin. – Minsk: Harvit, 1998 - 800 p.
-
Freud, Z. Beyond Pleasure / Z. Freud: Per. with him. - Minsk: Harvest, 2004. - 432 With.
-
King P. Affective response of the analyst to the patient's communication // Inter. J. Pxychoanal. 1978.
Learn more