Reactive hypoglycemia anxiety
Reactive hypoglycemia: Causes, symptoms, and treatment
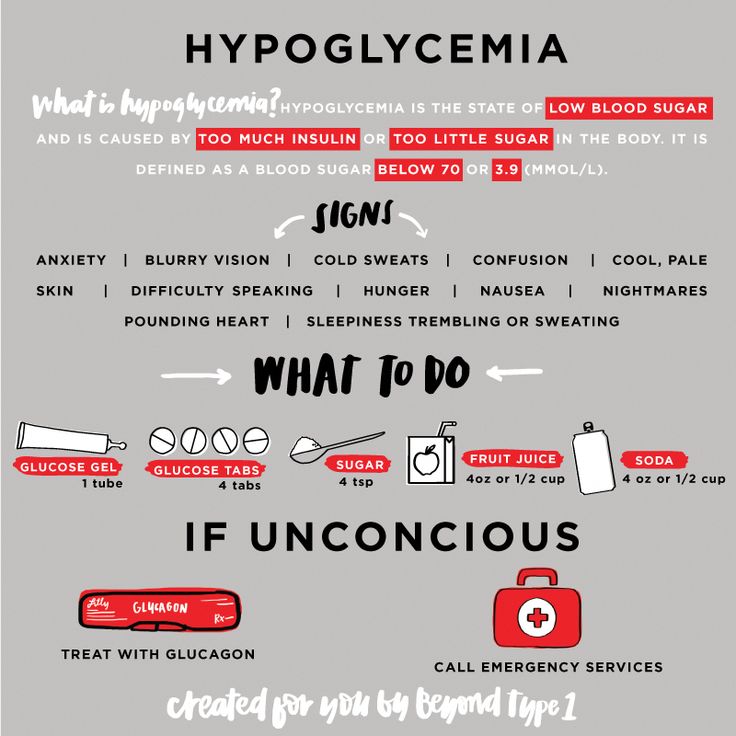
Reactive hypoglycemia is low blood sugar that occurs a few hours after eating a meal. It happens when a person has too much insulin in their blood at the wrong time.
Insulin is the hormone that enables sugar to enter cells from the bloodstream. Within cells, sugar serves as the primary source of energy.
Symptoms of reactive hypoglycemia may include confusion, shakiness, and anxiety. A person can reduce the risk of reactive hypoglycemia by taking dietary measures, such as eating small, frequent meals and limiting the intake of sugary foods.
Keep reading to learn more about reactive hypoglycemia, including the causes, symptoms, and treatment options available.
Hypoglycemia is the term for when blood sugar, or glucose, falls below the normal, healthy range. Some factors that affect blood sugar include:
- exercise
- the intake of sugar and other carbohydrates through the diet
- the amount of insulin in the body
When a person consumes carbohydrates, the body breaks them down to form glucose. In response, the pancreas secretes the hormone insulin, which helps glucose pass from the blood into cells in the muscles, liver, and brain. To function properly, these cells need glucose for fuel.
There are different types of hypoglycemia. One type occurs in people who have diabetes, and doctors classify this as diabetic hypoglycemia. It happens when the insulin injections or antidiabetic medication that a person takes removes too much sugar from the bloodstream.
Reactive hypoglycemia is a rare form of the condition, which doctors classify as nondiabetic hypoglycemia. It occurs when blood sugar levels are below 70 milligrams/deciliter. This often occurs approximately 2–4 hours after a meal. Symptoms subside quickly after eating or drinking carbohydrates.
Researchers have not yet fully identified the specific causes of reactive hypoglycemia. However, the condition stems from having too much insulin in the bloodstream at the wrong time.
Possible causes include:
- having prediabetes, which can make it hard for the pancreas to produce the right amount of insulin
- having rare enzyme deficiencies, which can make it difficult for the stomach and intestines to break down food
- having had stomach surgery, which can cause food to pass through the stomach into the intestines too fast
People with reactive hypoglycemia may experience some or all of the following symptoms 2–4 hours after a meal:
- hunger
- shakiness
- fatigue
- sweating
- weakness
- nausea or vomiting
- mood swings
- anxiety
- fast heart rate
- irritability
- headaches
- confusion
Most people who have reactive hypoglycemia do not require treatment.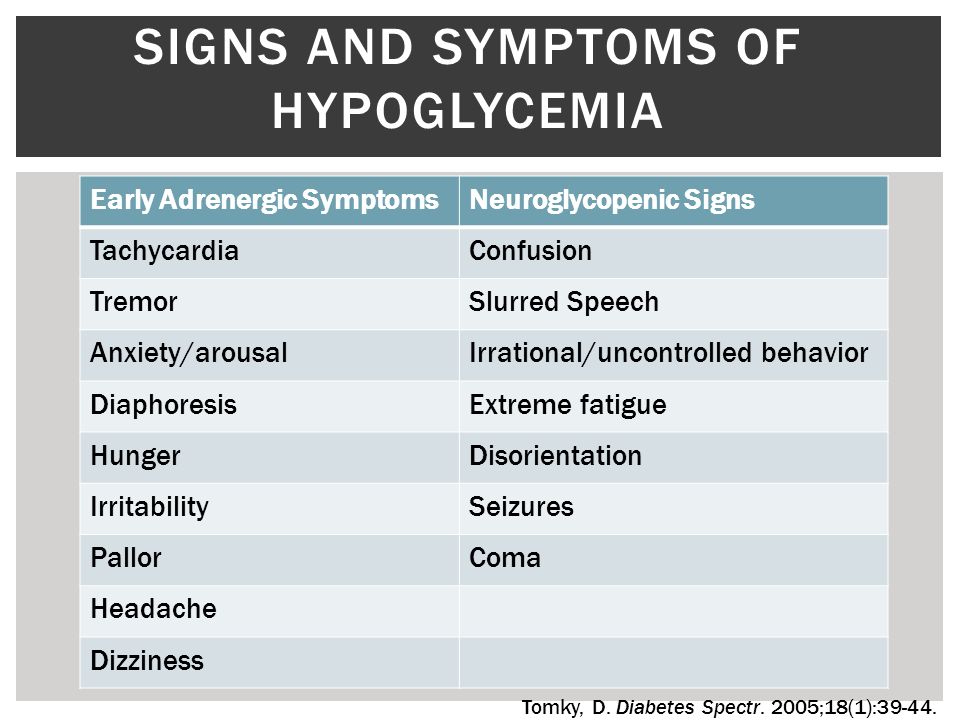 Rather, doctors recommend dietary changes to manage the symptoms.
Rather, doctors recommend dietary changes to manage the symptoms.
That said, if a person needs immediate treatment, doctors advise eating or drinking something that contains 15 grams of carbohydrates. Half a cup of juice contains this amount, but the juice should be the regular variety rather than a low calorie version that contains fewer carbohydrates.
One study reports that certain people with reactive hypoglycemia may also benefit from taking antidiabetic drugs, such as metformin. These individuals include those who doctors suspect may have prediabetes. Metformin may help reduce symptoms, as prediabetes is a possible cause of this type of hypoglycemia.
The dietary practices below may help prevent symptoms of reactive hypoglycemia:
- Eating small meals throughout the day: Eating a small amount of food every few hours can keep blood sugar from spiking as high as it does after eating a large meal.
- Limiting the intake of sugary foods and beverages, such as desserts, sweet tea, and fruit juices: These foods can trigger an excessive increase in insulin, which can result in a quick drop in blood sugar.

- Including lean protein and healthful fats in the diet: Examples of lean protein include fish and skinless poultry, while examples of healthful fats include avocados and olive oil.
- Eating high-fiber foods: These include fruits, vegetables, beans, and whole grains.
- Limiting or avoiding alcohol: Alcohol can cause low blood sugar. If a person wishes to drink alcohol, it is best to do so in small amounts and to eat something alongside it.
- Limiting or avoiding caffeine: Coffee, tea, and some sodas contain caffeine. This stimulant can cause the same symptoms of low blood sugar.
Learn more about what to eat for hypoglycemia here.
According to one study, certain people with reactive hypoglycemia may benefit from diabetes-prevention lifestyle practices. These people include individuals who have risk factors for diabetes, such as overweight and a family history of the disease.
In addition to helping prevent the onset of diabetes, these practices may reduce symptoms of hypoglycemia.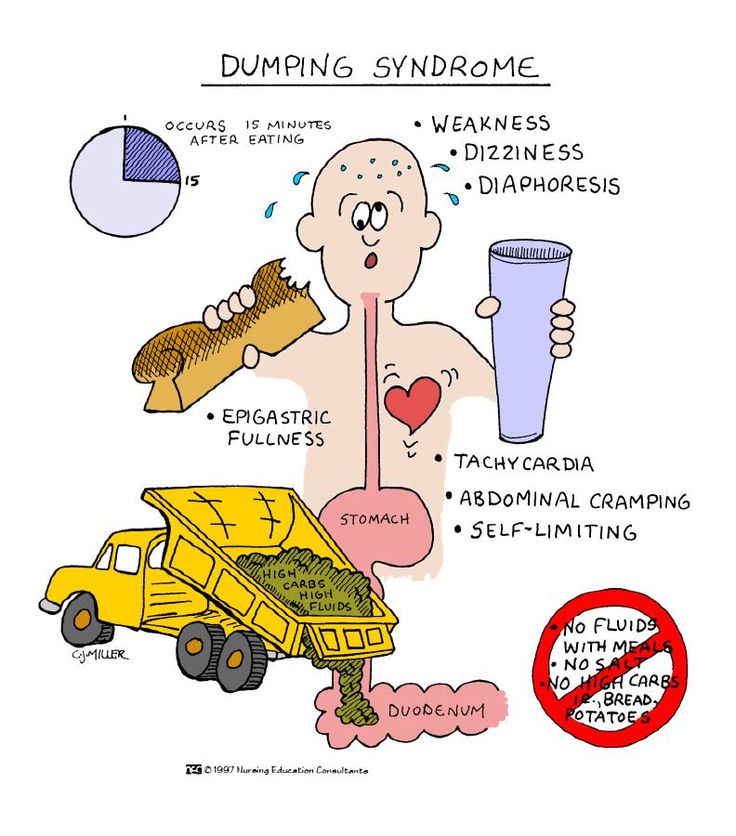 Aside from eating a healthful diet, the Centers for Disease Control and Prevention (CDC) recommend:
Aside from eating a healthful diet, the Centers for Disease Control and Prevention (CDC) recommend:
- increasing physical activity
- managing stress
- getting support from others with similar challenges
If a person is experiencing the symptoms of reactive hypoglycemia, they should consult a doctor.
This will enable them to find out whether they have the condition and, if so, to know its degree of severity. An examination and testing can rule out prediabetes or other conditions that may be causing the blood sugar to drop too much.
If necessary, a doctor may refer an individual to other healthcare professionals. These may include a registered dietitian or an endocrinologist, who is a specialist in hormone imbalances.
Reactive hypoglycemia is low blood sugar that occurs several hours after a meal. Doctors classify it as a nondiabetic variety of the condition.
When someone has symptoms of reactive hypoglycemia, the immediate treatment involves consuming a small amount of a sugary food or beverage, such as half a cup of fruit juice.
Following a healthful diet may help prevent the sugar spikes in the bloodstream that lead to sugar dips and symptoms of hypoglycemia.
Generalized Anxiety Disorder and Hypoglycemia Symptoms Improved with Diet Modification
Case Rep Psychiatry. 2016; 2016: 7165425.
Published online 2016 Jul 14. doi: 10.1155/2016/7165425
Author information Article notes Copyright and License information Disclaimer
Observational evidence suggests that a relationship may exist between high glycemic index diets and the development of anxiety and depression symptoms; however, as no interventional studies assessing this relationship in a psychiatric population have been completed, the possibility of a causal link is unclear. AB is a 15-year-old female who presented with concerns of generalized anxiety disorder and hypoglycemia symptoms. Her diet consisted primarily of refined carbohydrates. The addition of protein, fat, and fiber to her diet resulted in a substantial decrease in anxiety symptoms as well as a decrease in the frequency and severity of hypoglycemia symptoms.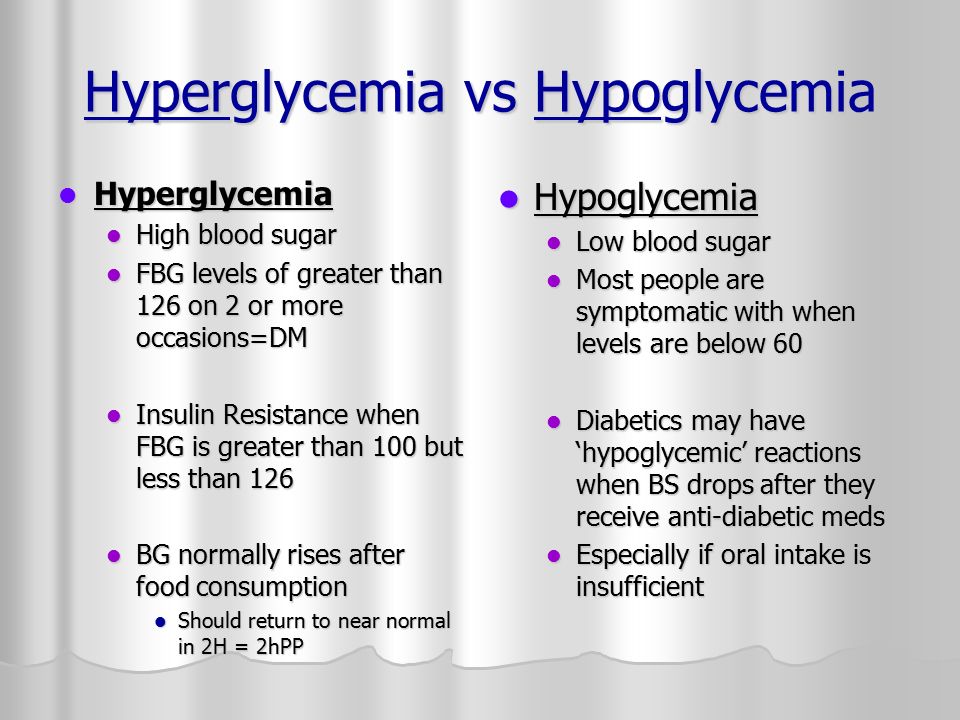 A brief return to her previous diet caused a return of her anxiety symptoms, followed by improvement when she restarted the prescribed diet. This case strengthens the hypothesis that dietary glycemic index may play a role in the pathogenesis or progression of mental illnesses such as generalized anxiety disorder and subsequently that dietary modification as a therapeutic intervention in the treatment of mental illness warrants further study.
A brief return to her previous diet caused a return of her anxiety symptoms, followed by improvement when she restarted the prescribed diet. This case strengthens the hypothesis that dietary glycemic index may play a role in the pathogenesis or progression of mental illnesses such as generalized anxiety disorder and subsequently that dietary modification as a therapeutic intervention in the treatment of mental illness warrants further study.
Generalized anxiety disorder (GAD) is a common and often disabling disease. It is characterized by fear, tension, and excessive worries regarding common events or problems for a minimum of six months [1] and is accompanied by physical symptoms such as heart palpitations, muscle tension, and chest tightness. Patients may experience nonspecific symptoms such as irritability and difficulty concentrating in addition to deterioration in the quality of their social, work, and personal experiences [1, 2]. Traumatic life experiences, dysfunctional serotonin, and epinephrine neurotransmitter systems and pernicious genetic influences are potentially involved in the development of GAD [3].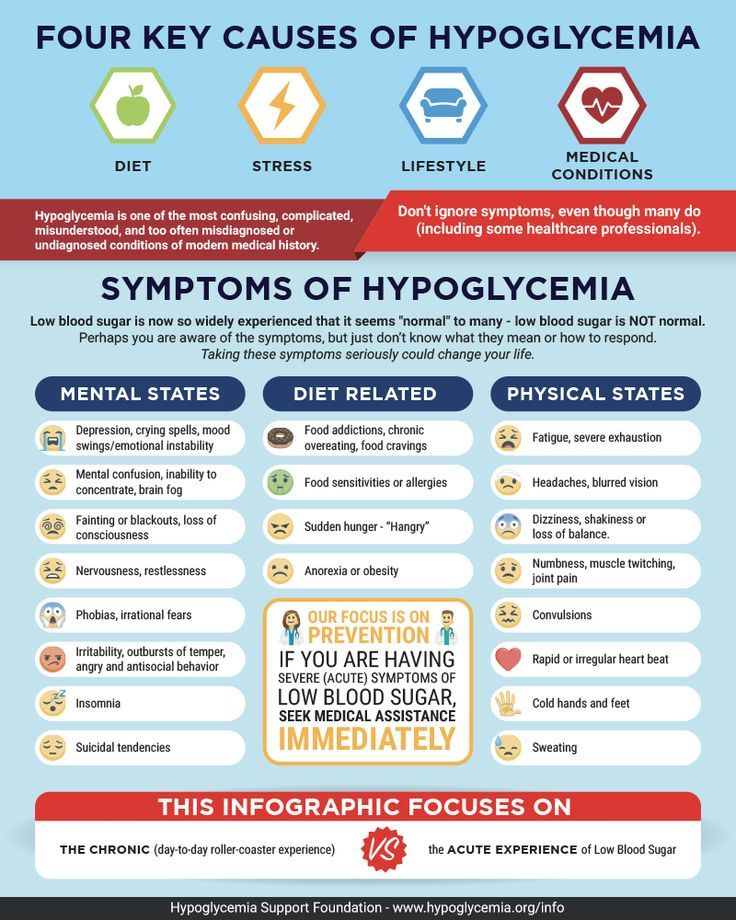 It is estimated that the lifetime prevalence is between 4.3% and 5.9% [1, 3] and 40–67% of patients experience comorbid depression [3].
It is estimated that the lifetime prevalence is between 4.3% and 5.9% [1, 3] and 40–67% of patients experience comorbid depression [3].
Conventional treatment of anxiety involves cognitive behavioural therapy in combination with pharmacologic interventions such as serotonin-norepinephrine reuptake inhibitors (SNRI), selective serotonin reuptake inhibitors (SSRI), or benzodiazepines [2, 3]. Despite appropriate treatment, many GAD patients cannot successfully achieve short term or long term remission. After five years, remission rates may remain as low as 38% [2]. Thus, the need for nonpharmacological approaches is evident [4].
Several studies suggest a relationship between improved nutrition and better mental health outcomes, both in general and adolescent populations. Epidemiological studies, including a recent meta-analysis, have shown that a diet including fruits, vegetables, fish, olive oil, nuts, and legumes may reduce the chance of developing depression [4, 5]. A prospective study found that a Mediterranean dietary pattern at baseline reduced the risk of depressive episodes 16.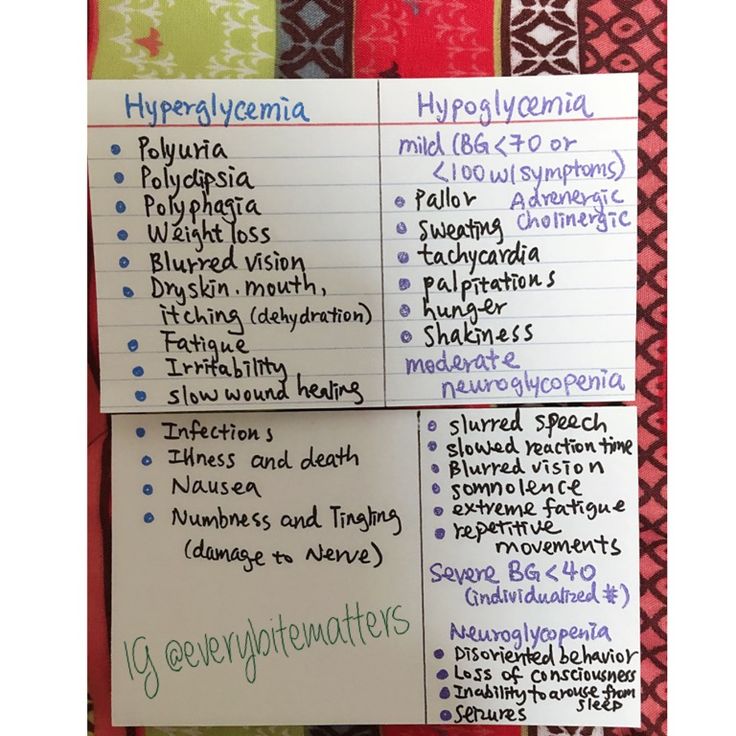 5 years later [6].
5 years later [6].
Despite evidence correlating a healthy diet with the maintenance of mental health, a trend towards a reduction in the quality of adolescent diets has been observed at the global level. This trend is characterized by an increased intake of fast foods, fried foods, sweets, refined grains, processed meat, and a reduction of fruit/vegetable intake [7]. The consumption of this Western-style diet has been independently associated with a greater risk for the development of anxiety and depression [7] and associated with a decline in the mental health status of adolescents [6]. Another study found an increased likelihood of psychological problems in adolescents associated with diets high in unhealthy foods [7].
A number of possible mechanisms have been proposed for the effect of diet on mental health including a role of inflammation and oxidation [6], deficiency of micronutrients such as folate, zinc, and magnesium [7], and glycemic balance.
The increase in global consumption of refined foods such as sweetened beverages, pastries, and refined carbohydrates impacts dietary glycemic index (GI), a measurement of the rate of blood glucose generation from specific food items.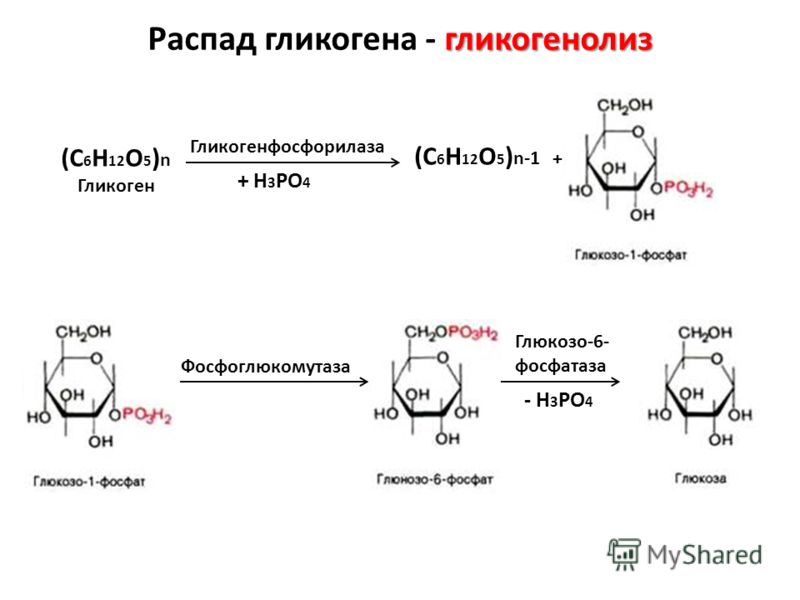 Glycemic load (GL) reflects both the glycemic index value and the total carbohydrate content of the food. Foods with a higher GI or GL create greater increases in blood sugar [8].
Glycemic load (GL) reflects both the glycemic index value and the total carbohydrate content of the food. Foods with a higher GI or GL create greater increases in blood sugar [8].
A recent cohort study showed that increasing odds of depression and anxiety have been associated with the consumption of foods that have a progressively higher GI and this relationship is maintained after controlling for micronutrients known to play a role in mental health [8]. Cross-sectional studies have demonstrated a correlation between the occurrence of depression/stress and higher intake of sweet foods [9] and a large prospective cohort study showed a positive correlation between a diet high in sweet desserts and refined grains and the risk for depression. Conversely, it was found that high consumption of fruits and vegetables, which contain fiber that lowers GI, was associated with a lower risk for depression [9].
In addition to the observational studies, a limited number of interventional studies have explored a potential relationship between blood sugar balance and emotional and cognitive health.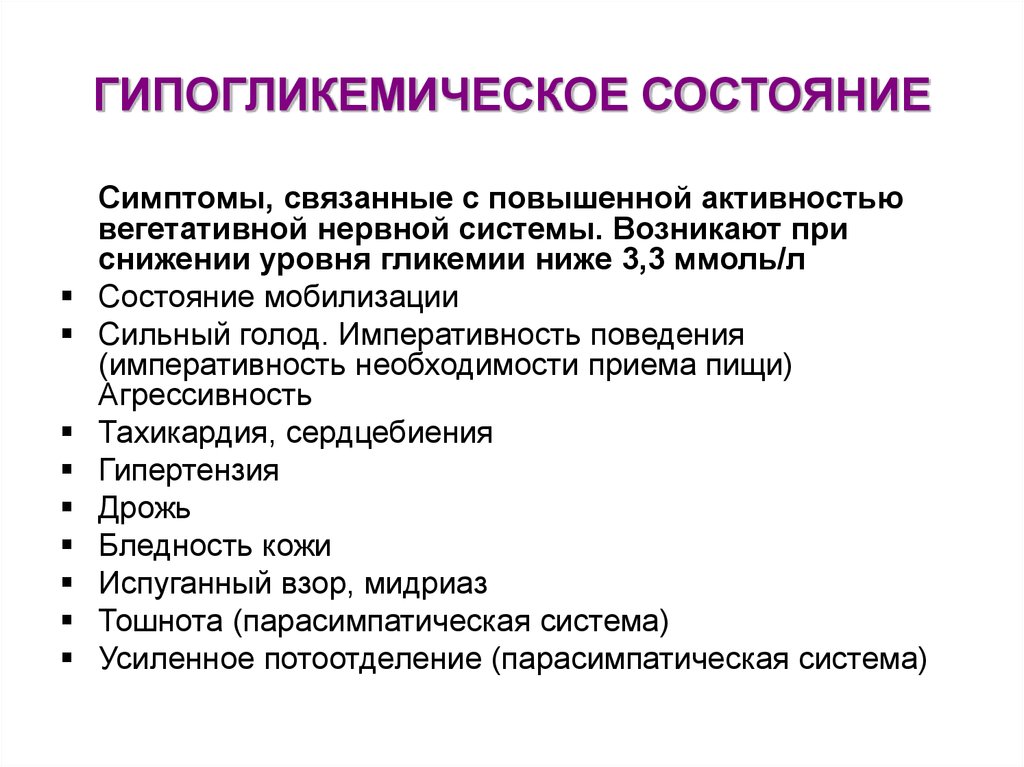 One clinical trial assigned healthy overweight subjects to high or low GI diets and found that the high GI diet resulted in worsening mood scores [10]. Two studies assessed the impact of high and low GI meals on cognitive performance in adults with type 2 diabetes and children, respectively, and found that the higher GI meal was related to poorer cognitive function [11, 12]. Conversely, two other intervention studies comparing high and low GI diets in patients with diabetes did not find a change in subclinical depression or cognitive function [9]. Despite this evidence that a relationship between dietary GI and emotional and cognitive functioning may exist, no interventional studies have assessed the impact of a low GI or low GL dietary intervention in psychiatric patient populations in order to assess causality of the relationship.
One clinical trial assigned healthy overweight subjects to high or low GI diets and found that the high GI diet resulted in worsening mood scores [10]. Two studies assessed the impact of high and low GI meals on cognitive performance in adults with type 2 diabetes and children, respectively, and found that the higher GI meal was related to poorer cognitive function [11, 12]. Conversely, two other intervention studies comparing high and low GI diets in patients with diabetes did not find a change in subclinical depression or cognitive function [9]. Despite this evidence that a relationship between dietary GI and emotional and cognitive functioning may exist, no interventional studies have assessed the impact of a low GI or low GL dietary intervention in psychiatric patient populations in order to assess causality of the relationship.
AB is a 15-year-old female student of south-Asian descent. She presented with concerns of anxiety and symptoms of hypoglycemia as well as difficulty concentrating, fatigue, headaches, asthma, and frequent urinary and vaginal infections.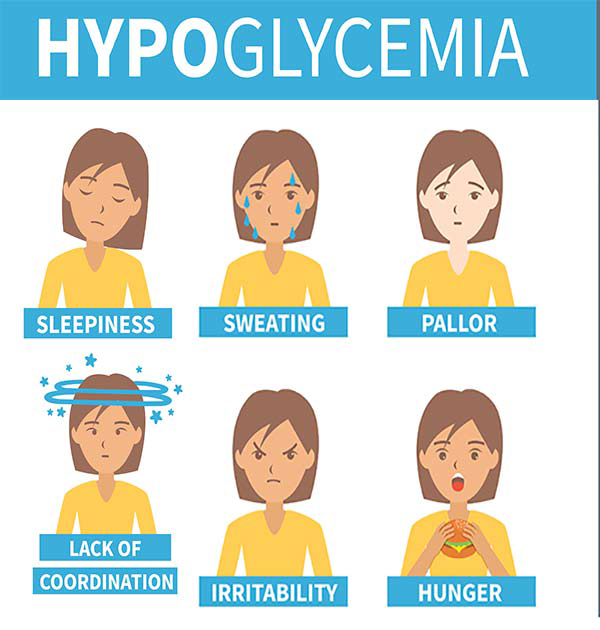
Her anxiety met criteria for GAD and she rated the intensity of anxiety as 8/10, with 10 being the highest level of anxiety possible. The anxiety started three months prior to the initial appointment and had worsened in the previous month. She described excessive worry that was difficult to control and impacted her daily functioning by causing her to be absent from school on several occasions. She experienced a number of somatic symptoms including heart palpitations, shakiness, discomfort in her stomach, and muscle tension. In response to the anxiety symptoms, she would eat foods like chocolate, chips, or fruit. AB was working with a counsellor to manage the anxiety symptoms and was finding some benefit.
AB had experienced episodes suggestive of hypoglycemia since 12 years of age. The symptoms included muscle weakness and shaking, headaches, nausea, anxiety, and loss of concentration. Her symptoms were ameliorated by eating sweet foods. AB reported that her hypoglycemia was at its worst at 12 years of age when she had to eat a granola bar hourly in order to concentrate.
2.1. Clinical Findings
A diet history revealed the following typical daily food intake:
Breakfast: fruit smoothie containing fruit, fruit juice, and water.
Morning snack: bagel with margarine.
Lunch: pasta or white rice with vegetables.
Afternoon snack: granola bar or cookies or gummy candies.
After school meal: white pasta; it may include meat.
Dinner: white rice or spaghetti; it may include meat.
Evening snack: cookies and toast.
Beverages: 2 liters of water, 1 cup of juice, 1 cup of lactose-free milk, and 1 cup of tea.
2.2. Past Medical History
Due to her difficulty concentrating, AB was prescribed dextroamphetamine 5 mg. While she found that it improved concentration, this medication caused her to lose weight. As the patient's weight was initially on the lower end of normal (weight: 115 lb., height: 5′6′′, and BMI: 18.6) the dose was reduced to 2 to 3 times per week, as needed.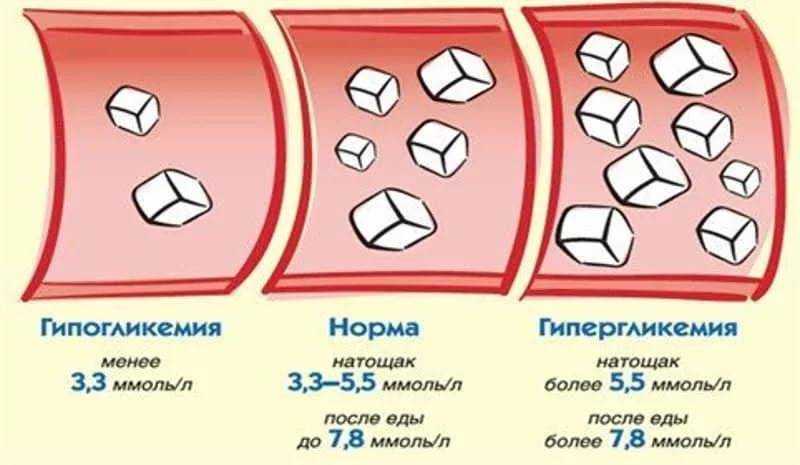
2.3. Psychosocial History
AB lives with her mother, father, and sister. AB's sister experienced mental health concerns in the previous years which created elevated stress levels in the family home.
2.4. Diagnostic Focus and Assessment
Repeated assessments of random and fasting blood glucose and screening physical examination were within normal range.
2.5. Therapeutic Approach
At the initial visit, the following dietary plan was prescribed:
Breakfast: it includes a smoothie containing fruit, water, 1 scoop of protein powder, and 1 tablespoon of flax seeds or olive oil.
Lunch and dinner: they include a serving of protein (meat, legume, and soy) and a serving of vegetables.
Snacks: they include protein when possible (e.g., apple with sunflower seed butter, vegetable sticks with hummus, and pumpkin seeds).
Continue to eat carbohydrate-containing snacks as needed for the management of hypoglycemia symptoms.

She was asked to follow these dietary guidelines daily until the follow-up visit. While eggs, nuts, and fish would have normally been recommended as well, the patient had an anaphylactic allergy to these foods.
2.6. Follow-Up and Outcomes
At the first follow-up, four weeks later, AB reported that she had complied with the dietary plan since the previous visit. She reported a significant decrease in anxiety (4 to 5/10), as well as improved energy, less-frequent and less intense hypoglycemia symptoms, and fewer headaches (once per week compared to daily) in addition to improved concentration and mood. She required fewer snacks during the day and decreased her intake of granola bars, cookies, and candies (1-2 servings per day). She also reported a cessation of chronic vaginal discharge. The substantial improvement in her anxiety symptoms prompted AB to temporarily discontinue her counselling sessions.
At a subsequent follow-up visit four weeks later, AB reported that she had briefly reverted back to her original diet for a period of one week and experienced a worsening of anxiety symptoms within one day. After returning to the dietary intervention prescribed, her anxiety symptoms decreased within two days.
After returning to the dietary intervention prescribed, her anxiety symptoms decreased within two days.
This case illustrates an example of improved anxiety and hypoglycemia symptoms in response to changes in the macronutrient composition of the diet. It suggests that dietary GI and blood sugar balance, within a physiologic range, may play a role in the development or clinical progression of anxiety. Subsequently, modifying the diet by reducing the consumption of refined carbohydrates and including more protein, fat, and fiber may be beneficial.
The proposed relationship is supported by observational studies demonstrating a relationship between higher GI/GL and increased incidence of mental illness as well as a potential mechanism. High GI foods result in an increase in blood glucose levels; however, a large compensatory insulin release may result in reactive hypoglycemia. Hypoglycemia is associated with an acute increase in epinephrine [13] which contributes to neuropsychiatric symptoms including anxiety [14] and symptoms associated with anxiety such as shakiness, sweating, and heart palpitations.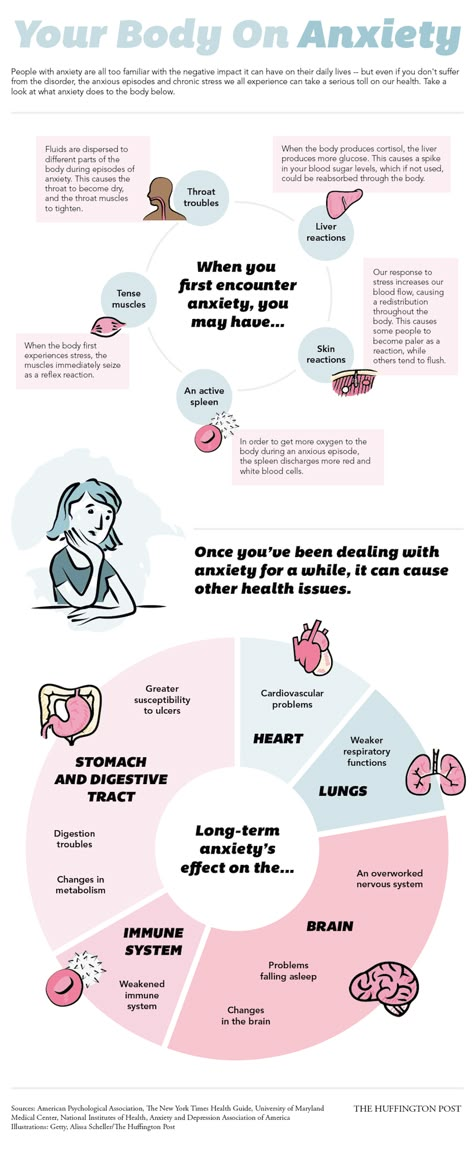 Induction of hypoglycemia in a laboratory setting has a negative impact on mood, hedonic tone, and energy levels as well as an increase in tense arousal [15]. The presence of both anxiety and hypoglycemia symptoms in AB's case, along with their concurrent response to treatment, lends support to the hypothesis that these conditions may be related.
Induction of hypoglycemia in a laboratory setting has a negative impact on mood, hedonic tone, and energy levels as well as an increase in tense arousal [15]. The presence of both anxiety and hypoglycemia symptoms in AB's case, along with their concurrent response to treatment, lends support to the hypothesis that these conditions may be related.
However, it is unclear if other macronutrient or micronutrient changes were, at least in part, responsible for the patient's symptom improvement as she had made several changes concurrently. A recent study found that the individuals in the highest third of GI had lower intake of magnesium, vitamin B6, vitamin B12, omega-3 fatty acids, and protein. Evidence shows that all of these nutrients may play a role in the prevention of mental illness [9].
Evidence suggests that adequate intake of protein may be required in the maintenance of mental health. Dietary protein provides amino acids, eight of which are essential. They cannot be synthesized by the body and must be supplied through the diet.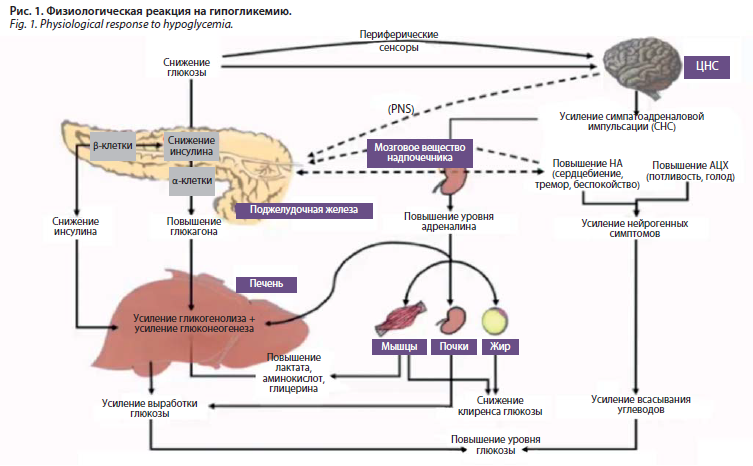 Amino acids form the building blocks of neurotransmitters. For example, the synthesis of serotonin requires the essential amino acid tryptophan and dopamine synthesis requires tyrosine, which is produced from the essential amino acid phenylalanine. The lack of tyrosine and tryptophan leads to deficiencies of the respective neurotransmitters and has been associated with psychiatric disturbances [16].
Amino acids form the building blocks of neurotransmitters. For example, the synthesis of serotonin requires the essential amino acid tryptophan and dopamine synthesis requires tyrosine, which is produced from the essential amino acid phenylalanine. The lack of tyrosine and tryptophan leads to deficiencies of the respective neurotransmitters and has been associated with psychiatric disturbances [16].
Micronutrient factors are also involved in neurotransmitter synthesis and may be involved in the development of mood and anxiety disorders. As in this case, a diet low in meat may be low in vitamin B12 and a diet low in green vegetables may lack folate. Because both nutrients are important for neurotransmitter synthesis [17], dietary intake may play a role in the development or progression of mood and anxiety disorders.
Dietary fat may also play a role in mental health. The dry weight of the brain is 60 percent fat [18] and low levels of omega-3 fats and cholesterol are significant risk factors for major depression and suicide [19].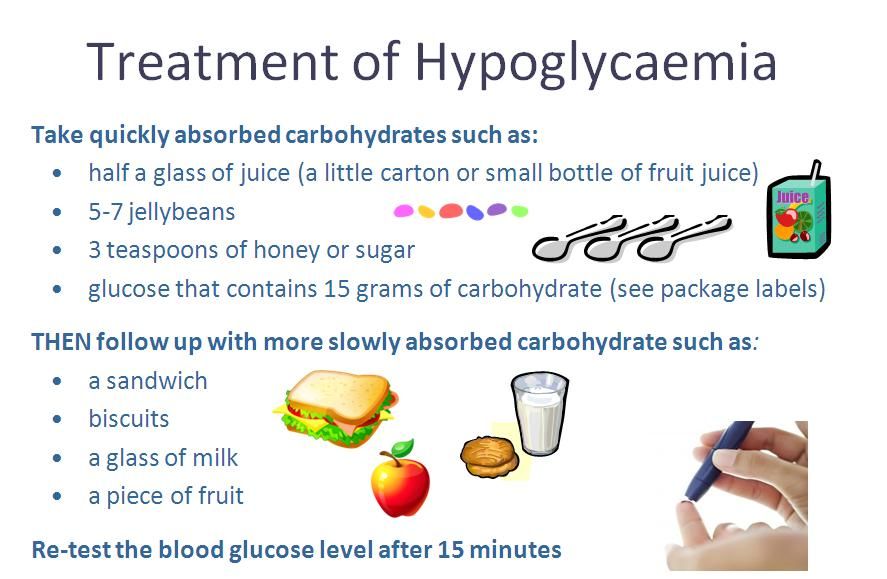 Omega-3 fats, which cannot be produced endogenously and must be obtained from the diet, affect the serotonergic system [19] and an inverse relationship between dietary omega-3 fatty acids and anxiety disorders has been demonstrated [7]. Preliminary evidence suggests that omega-3 supplementation may be beneficial in the treatment of anxiety [20].
Omega-3 fats, which cannot be produced endogenously and must be obtained from the diet, affect the serotonergic system [19] and an inverse relationship between dietary omega-3 fatty acids and anxiety disorders has been demonstrated [7]. Preliminary evidence suggests that omega-3 supplementation may be beneficial in the treatment of anxiety [20].
Despite these other potential factors, the concomitant improvement in both anxiety and hypoglycemia symptoms suggests that blood sugar balance may have been contributing to AB's anxiety disorder and that improvement in blood sugar management, as seen in the reduction of hypoglycaemic symptoms, may have been a significant factor in the response to treatment. In conjunction with the observational data [13], this may strengthen our understanding of the relationship between suboptimal blood sugar regulation, GI/GL, and mental illness.
One strength of this case report is that the dietary modifications were the only intervention initiated at the time during which the improvement in symptoms was observed.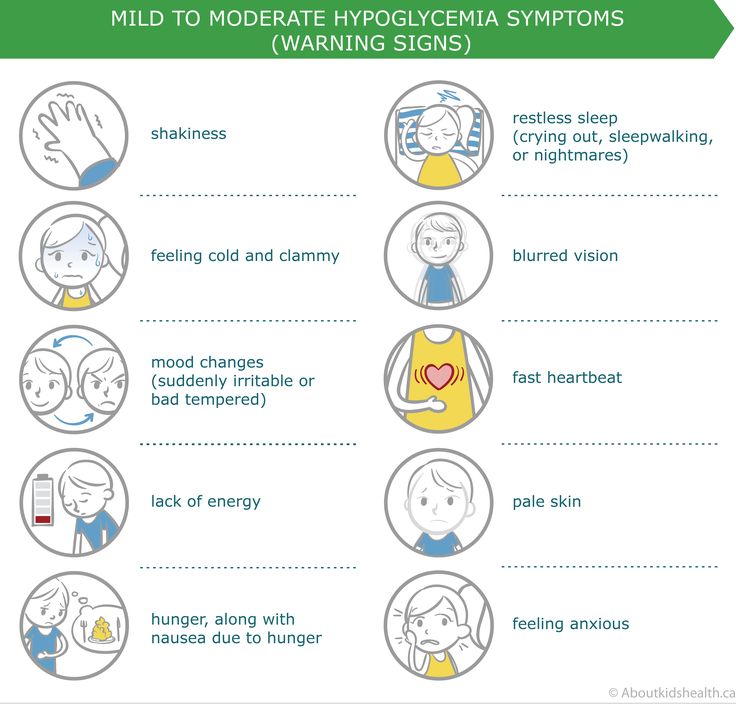 As well, the brief return to the patient's previous diet and subsequent worsening of symptoms lends support to the likelihood of a causal relationship.
As well, the brief return to the patient's previous diet and subsequent worsening of symptoms lends support to the likelihood of a causal relationship.
Some limitations exist as well. No validated assessment tool was used to monitor change in anxiety symptoms, only the patient's subjective report. Additionally, the patient was receiving counselling concurrently.
Blood sugar balance and dietary GI/GL appear to be important factors in a number of chronic illnesses. A recent meta-analysis found significant positive associations between higher GI or GL and higher incidence of diabetes, coronary heart disease, gallbladder disease, breast cancer, and all diseases combined [21]. As such, implementing a diet lower in refined carbohydrates in the treatment of anxiety may have substantial additional benefit with respect to risk of chronic disease.
Dietary carbohydrates may be significantly related to emotional and cognitive symptoms such as anxiety and difficulty concentrating. Further research into the potential role of GI in the pathogenesis and progression of mental health concerns in addition to the utility of dietary interventions in the treatment of these conditions is warranted.
Further research into the potential role of GI in the pathogenesis and progression of mental health concerns in addition to the utility of dietary interventions in the treatment of these conditions is warranted.
The authors declare that they have no competing interests.
1. Martin J. L. R., Sainz-Pardo M., Furukawa T. A., Martin-Sanchez E., Seoane T., Galan C. Review: benzodiazepines in generalized anxiety disorder: heterogeneity of outcomes based on a systematic review and meta-analysis of clinical trials. Journal of Psychopharmacology. 2007;21(7):774–782. doi: 10.1177/0269881107077355. [PubMed] [CrossRef] [Google Scholar]
2. Lalonde C. D., Van Lieshout R. J. Treating generalized anxiety disorder with second generation antipsychotics. Journal of Clinical Psychopharmacology. 2011;31(3):326–333. doi: 10.1097/jcp.0b013e31821b2b3f. [PubMed] [CrossRef] [Google Scholar]
3. Bandelow B., Boerner R. J., Kasper S., Linden M., Wittchen H.-U., Möller H.-J.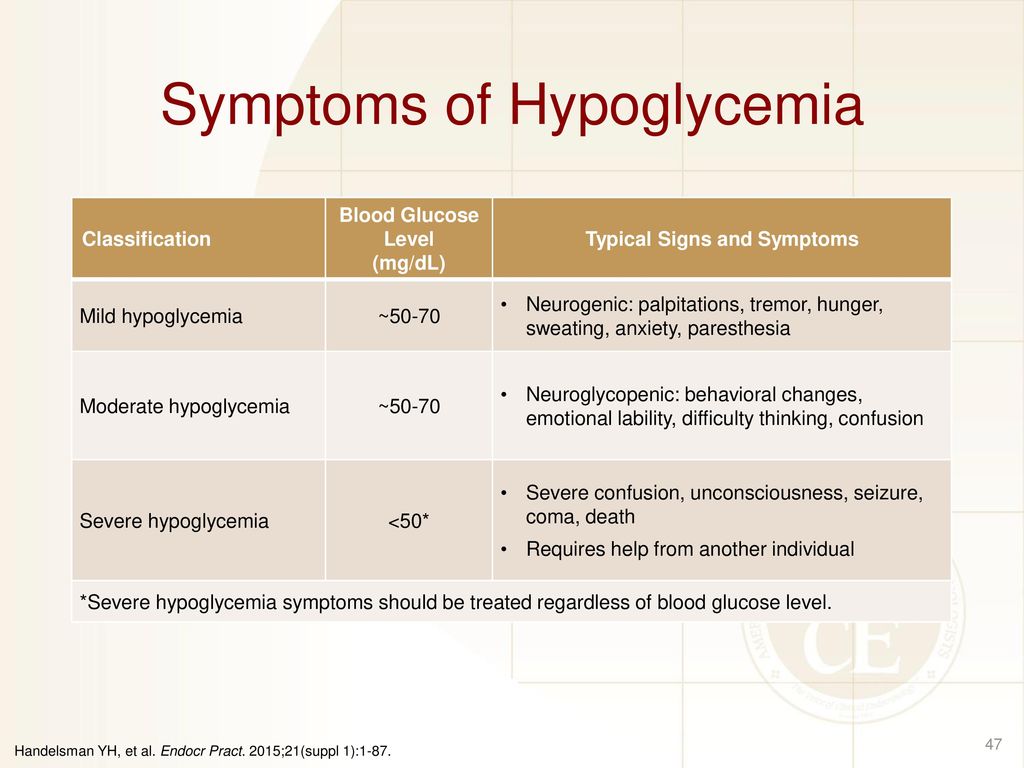 The diagnosis and treatment of generalized anxiety disorder. Deutsches Arzteblatt International. 2013;110(17):300–310. doi: 10.3238/arztebl.2013.0300. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
The diagnosis and treatment of generalized anxiety disorder. Deutsches Arzteblatt International. 2013;110(17):300–310. doi: 10.3238/arztebl.2013.0300. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
4. Opie R. S., O'Neil A., Itsiopoulos C., Jacka F. N. The impact of whole-of-diet interventions on depression and anxiety: a systematic review of randomised controlled trials. Public Health Nutrition. 2014;18(11):2074–2093. doi: 10.1017/s1368980014002614. [PubMed] [CrossRef] [Google Scholar]
5. Lai J. S., Hiles S., Bisquera A., Hure A. J., McEvoy M., Attia J. A systematic review and meta-analysis of dietary patterns and depression in community-dwelling adults. American Journal of Clinical Nutrition. 2014;99(1):181–197. doi: 10.3945/ajcn.113.069880. [PubMed] [CrossRef] [Google Scholar]
6. Ruusunen A., Lehto S. M., Mursu J., et al. Dietary patterns are associated with the prevalence of elevated depressive symptoms and the risk of getting a hospital discharge diagnosis of depression in middle-aged or older Finnish men. Journal of Affective Disorders. 2014;159:1–6. doi: 10.1016/j.jad.2014.01.020. [PubMed] [CrossRef] [Google Scholar]
Journal of Affective Disorders. 2014;159:1–6. doi: 10.1016/j.jad.2014.01.020. [PubMed] [CrossRef] [Google Scholar]
7. Kulkarni A. A., Swinburn B. A., Utter J. Associations between diet quality and mental health in socially disadvantaged New Zealand adolescents. European Journal of Clinical Nutrition. 2015;69(1):79–83. doi: 10.1038/ejcn.2014.130. [PubMed] [CrossRef] [Google Scholar]
8. Gangswisch J. E., Hale L., Garcia L., et al. High glycemic index diet as a risk factor for depression: analyses from the Women's Health Initiative. The American Journal of Clinical Nutrition. 2015;102(2):454–463. [PMC free article] [PubMed] [Google Scholar]
9. Haghighatdoost F., Azadbakht L., Keshteli A. H., et al. Glycemic index, glycemic load, and common psychological disorders. The American Journal of Clinical Nutrition. 2016;103(1):201–209. doi: 10.3945/ajcn.114.105445. [PubMed] [CrossRef] [Google Scholar]
10. Cheatham R. A., Roberts S. B., Das S. K., et al. Long-term effects of provided low and high glycemic load low energy diets on mood and cognition. Physiology and Behavior. 2009;98(3):374–379. doi: 10.1016/j.physbeh.2009.06.015. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
K., et al. Long-term effects of provided low and high glycemic load low energy diets on mood and cognition. Physiology and Behavior. 2009;98(3):374–379. doi: 10.1016/j.physbeh.2009.06.015. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
11. Ingwersen J., Defeyter M. A., Kennedy D. O., Wesnes K. A., Scholey A. B. A low glycaemic index breakfast cereal preferentially prevents children's cognitive performance from declining throughout the morning. Appetite. 2007;49(1):240–244. doi: 10.1016/j.appet.2006.06.009. [PubMed] [CrossRef] [Google Scholar]
12. Papanikolaou Y., Palmer H., Binns M. A., Jenkins D. J. A., Greenwood C. E. Better cognitive performance following a low-glycaemic-index compared with a high-glycaemic-index carbohydrate meal in adults with type 2 diabetes. Diabetologia. 2006;49(5):855–862. doi: 10.1007/s00125-006-0183-x. [PubMed] [CrossRef] [Google Scholar]
13. Sejling A.-S., Kjær T. W., Pedersen-Bjergaard U., et al. Hypoglycemia-associated changes in the electroencephalogram in patients with type 1 diabetes and normal hypoglycemia awareness or unawareness.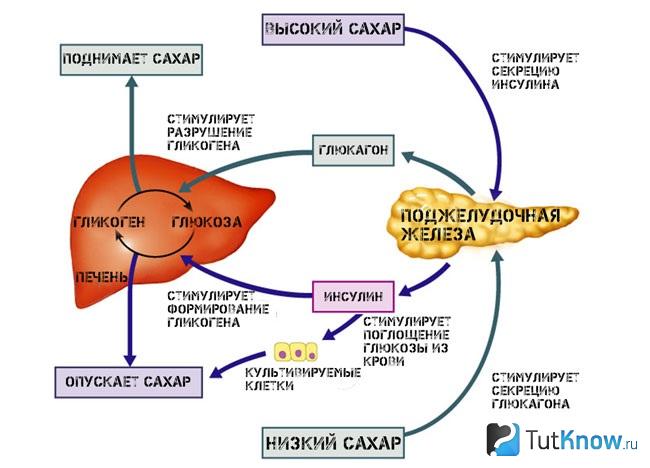 Diabetes. 2015;64(5):1760–1769. doi: 10.2337/db14-1359. [PubMed] [CrossRef] [Google Scholar]
Diabetes. 2015;64(5):1760–1769. doi: 10.2337/db14-1359. [PubMed] [CrossRef] [Google Scholar]
14. Paine N. J., Watkins L. L., Blumenthal J. A., Kuhn C. M., Sherwood A. Association of depressive and anxiety symptoms with 24-hour urinary catecholamines in individuals with untreated high blood pressure. Psychosomatic Medicine. 2015;77(2):136–144. doi: 10.1097/PSY.0000000000000144. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
15. Gold A. E., MacLeod K. M., Frier B. M., Deary I. J. Changes in mood during acute hypoglycemia in healthy participants. Journal of Personality and Social Psychology. 1995;68(3):498–504. doi: 10.1037/0022-3514.68.3.498. [PubMed] [CrossRef] [Google Scholar]
16. Sathyanarayana Rao T., Asha M. R., Ramesh B. N., Jagannatha Rao K. S. Understanding nutrition, depression and mental illnesses. Indian Journal of Psychiatry. 2008;50(2):77–82. doi: 10.4103/0019-5545.42391. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
17. Papakostas G. I., Petersen T., Mischoulon D., et al. Serum folate, vitamin B12, and homocysteine in major depressive disorder, part 2: Predictors of relapse during the continuation phase of pharmacotherapy. Journal of Clinical Psychiatry. 2004;65(8):1096–1098. doi: 10.4088/JCP.v65n0811. [PubMed] [CrossRef] [Google Scholar]
Papakostas G. I., Petersen T., Mischoulon D., et al. Serum folate, vitamin B12, and homocysteine in major depressive disorder, part 2: Predictors of relapse during the continuation phase of pharmacotherapy. Journal of Clinical Psychiatry. 2004;65(8):1096–1098. doi: 10.4088/JCP.v65n0811. [PubMed] [CrossRef] [Google Scholar]
18. Chang C.-Y., Ke D.-S., Chen J.-Y. Essential fatty acids and human brain. Acta Neurologica Taiwanica. 2009;18(4):231–241. [PubMed] [Google Scholar]
19. Huan M., Hamazaki K., Sun Y., et al. Suicide attempt and n-3 fatty acid levels in red blood cells: a case control study in China. Biological Psychiatry. 2004;56(7):490–496. doi: 10.1016/j.biopsych.2004.06.028. [PubMed] [CrossRef] [Google Scholar]
20. Su K.-P., Matsuoka Y., Pae C.-U. Omega-3 polyunsaturated fatty acids in prevention of mood and anxiety disorders. Clinical Psychopharmacology and Neuroscience. 2015;13(2):129–137. doi: 10.9758/cpn.2015.13.2.129. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
21. Barclay A. W., Petocz P., McMillan-Price J., et al. Glycemic index, glycemic load, and chronic disease risk—a meta-analysis of observational studies. The American Journal of Clinical Nutrition. 2008;87(3):627–637. [PubMed] [Google Scholar]
Barclay A. W., Petocz P., McMillan-Price J., et al. Glycemic index, glycemic load, and chronic disease risk—a meta-analysis of observational studies. The American Journal of Clinical Nutrition. 2008;87(3):627–637. [PubMed] [Google Scholar]
REACTIVE HYPOGLYCEMIA in people with and without diabetes | Sugar Magazine
Did you know that post-eating hypo is not just for people with diabetes?
What is reactive hypoglycemia? Main causes and symptoms? How to treat? What to do in case of occurrence?
Let's figure it out together!
- Author: Anastasia Tsvigun, editor
- access_time
Reactive hypoglycemia - decrease in blood glucose after a certain period of time after eating a meal to a dangerously low value.
At the same time, episodes of falling SC usually recur and occur within four hours after eating.
Reactive hypo is thought to be more common in people who are overweight or who have had stomach and upper small intestine surgery, and as a result, food may not stay in the stomach as it normally does.
✅ REASONS
Scientists believe that the problem is the production of too much insulin produced and released by the pancreas after a heavy carbohydrate meal.
This excess production and secretion of insulin continues after food-derived glucose is digested, causing the amount of glucose in the bloodstream to drop to a lower than normal level.
What causes this increased activity of the pancreas is not yet clear.
One of the possible causes of - is a benign tumor in the pancreas. Another explanation is that reactive hypoglycemia is caused by a lack of glucagon secretion.
National Institutes of Health (NIH) USA states that "the cause of most cases of reactive hypoglycemia is still open to debate. "
"
✅ SYMPTOMS
Major symptoms of reactive hypoglycemia may include:
- unreasonable anxiety
- blurred vision
- dizziness
- fatigue
- headache
- palpitations
- increased hunger
- irritability
- sweating
IMPORTANT note that many of these symptoms can occur even without low blood sugar. And the actual cause for most people is often related to what food was eaten, or to changes in the transit time of food through the stomach and intestinal tract.
If there are no symptoms of hypoglycemia at the time of onset, you may have what is known as "postprandial syndrome".
✅ PREVENTION AND TREATMENT
Reactive hypo usually does not require any medical treatment.
The following is recommended to patients for prevention:
1. Eat a well-balanced diet including meat, poultry, fish, non-meat sources of protein, dairy products, and fiber-rich foods such as whole grains, fruits, and vegetables.
2. Eat often and in small portions. Divide your daily diet into several small meals and low-carb snacks, no more than 3 hours apart.
3. Reduce consumption of unhealthy carbohydrates: store-bought sweets, baked goods, soft drinks rich in glucose or sucrose.
4. Exercise regularly! Physical activity increases sugar intake, which in turn reduces the excessive release of insulin.
5. When drinking alcohol, eat food and do not mix with sugary soft drinks.
Some people, such as those who have had bowel surgery, may need further evaluation by a doctor.
✅ IMPROVE HYPO-CONSCIOUSNESS
If you suffer from frequent hypoglycemia, it can be potentially dangerous not only for you, but also for those around you.
Examples where hypo and not being aware of it can be particularly dangerous include driving, operating dangerous machinery at work, and even simple everyday tasks such as cooking or crossing a road.
If you do not feel any symptoms of hypoglycemia, you may need to check your CK levels more often to recognize the onset of hypoglycemia. Also try to record what events lead to hypo so you can identify trends and prevent them in the future.
SAVE YOURSELF!
Caring Your Sugar OK
***Source: diabetes.co.uk
Helpful Hints to Manage Hypoglycemia Naturally
The information in this blog has not been verified by your country's public health authority and is not intended for diagnosis, treatment, or medical advice. Read more
Hypoglycemia, or low blood sugar, has been experienced by all of us at some point in our lives. However, if hypoglycemia persists, it can be a sign of more serious conditions such as diabetes and even arthritis. So what is hypoglycemia - and how do we deal with this phenomenon that has existed for many centuries? I believe that we should take a comprehensive approach to the treatment of hypoglycemia, focusing on the phenomena of imbalance in the body. Our task is to help the body maintain normal blood sugar levels and improve overall health.
Our task is to help the body maintain normal blood sugar levels and improve overall health.
What is hypoglycemia?
Hypoglycemia is a condition that occurs when the body's blood sugar or glucose levels are low. Glucose is the body's source of energy and nutrients, so low glucose levels prevent the body from functioning optimally and can lead to many symptoms, including dizziness, fainting, blurred consciousness, and muscle weakness.
When we eat foods high in glucose, such as sweets, bread, pasta, and some fruits, glucose is absorbed into the bloodstream and transported to various parts of the body, including the heart and brain for energy. Our pancreas responds to this sugar intake by releasing the hormone insulin, which helps process and break down glucose in the body. Insulin also helps cells absorb glucose, and the excess is sent to the liver for storage and metabolism.
Under normal circumstances, when blood glucose levels are low, a hormone called glucagon signals the liver to release stored glucose stores and keeps blood sugar levels stable. But when at any stage of this process there is a stop or disturbance, the level of sugar in the blood becomes unbalanced and symptoms of hypoglycemia develop.
Hypoglycemia is generally divided into two types: reactive and non-reactive.
- Symptoms of reactive hypoglycemia are usually caused by an overproduction of insulin, which may result from consumption of foods or drinks high in sugar and refined carbohydrates. This forces the body to overwork, produce insulin and break down all the sugar eaten. Such symptoms may occur within a few hours after eating.
- Non-reactive hypoglycemia not related to food intake. It is influenced by factors such as family history and other diseases that your body fights. If you have any disorder that affects your liver, kidneys, or heart, your body may not process glucose properly, resulting in hypoglycemia.
Signs and symptoms of hypoglycemia
The causes of hypoglycemia are varied and individual. The same can be said about her symptoms. However, there is something in common that most patients with hypoglycemia have in common - at some point they have experienced symptoms of low blood sugar levels. The most common of these symptoms are:
- Hunger. Does your stomach growl during the day? This is usually a sign that your blood sugar is low and your body is very hungry.
- Foggy mind. If you lose focus easily at work, hypoglycemia may be the cause. Patients who experience cloudy consciousness describe this condition as follows: confused consciousness, "porridge in the head", it is difficult to think.
- Fatigue . And what else! Feeling tired, exhausted, having trouble falling asleep, and even having body aches at the end of the day can mean you have low blood sugar.
- Mood swings. If you often experience mood swings during the day, or even if such swings give you a headache, this indicates an imbalance in your blood sugar levels.
- Dizziness. Have you ever felt dizzy at school or at work? Did you have fainting? These symptoms may be caused by low blood sugar.
- Anxiety. Did you have a nervous day? Each of us has a lot of stress in life, but if anxiety and worry do not let you go all day, you probably have low blood sugar. Hypoglycemia can also be caused by skipping meals, which causes fluctuations in blood sugar throughout the day. Heavy drinking, paradoxically, can also lower blood sugar levels over time. Alcohol can lead to a temporary spike in blood sugar, but after a few hours, the body's sugar levels plummet.
Who is at risk for hypoglycemia?
Strictly speaking, everyone is at risk of hypoglycemia. In both children and adults, symptoms of hypoglycemia can occur at any age, especially if their diet is high in sugar and carbohydrates. Also, keep in mind that hypoglycemia, like diabetes, is inherited, so you may be predisposed to insulin resistance, and with it, to low blood sugar.
Conventional treatment for hypoglycemia
The American Diabetes Association recommends taking 15-20 grams of carbohydrates (to provide glucose) and then monitoring blood sugar levels for 15 minutes to detect a spike in sugar levels. If low blood sugar levels persist, repeat this procedure until blood sugar levels stabilize. As soon as the blood sugar level is normal, it is recommended to have a snack or meal so that the body receives nutrients and the stomach is not empty.
Integrative approach to the treatment of hypoglycemia
Conventional therapies are aimed at treating or controlling hypoglycemia, while the integrative approach is more focused on prevention. There are a few things you can do to stay healthy and avoid or reduce the effects of hypoglycemia:
1. Remember to eat foods that are high in protein and fiber and low in sugar.
- Include protein in every meal - fish, eggs, tofu, tempeh; - any meat or its vegetarian alternatives that you include in your diet will be useful.
When cooking, swap out butter and margarine for coconut oil, olive oil, or avocado oil to add healthy fats that keep blood sugar levels stable longer.
- Try to eat less but more often during the day. I recommend nuts or dried fruit and nut mix (not M&Ms) as a snack at school and work because they are high in protein and filling.
- Reduce the amount of sugary drinks and sweets in your diet, and this will increase your insulin resistance.
2. Eat healthy carbohydrates.
- Not all carbs are bad! Healthy carbohydrates to include in your diet are brown rice, legumes, sweet potatoes, and beans. To keep your blood sugar stable throughout the day, replace refined carbs like ice cream or cookies with these alternatives.
- Feed your body with healthy carbohydrates so that while walking or exercising in the gym your body has reserves of glucose, and you would not feel dizzy or unwell.
- Avoid fast food and fried foods, sugary drinks, sugary alcoholic beverages, and highly processed foods because all of these can raise glucose levels.
3. Take natural supplements.
There are nutritional supplements that can help raise blood sugar levels and keep insulin levels stable. Here are my favorites:
- Chrome. This microelement interacts with insulin, helping to reduce insulin resistance and effectively break down glucose. Chromium is known for its anti-inflammatory and antihypoglycemic effects on the body. A supplement like chromium picolinate or GTF-chromium will give you the dose of chromium you need to maintain normal blood sugar levels. These supplements should be taken after meals.
- Spirulina. Spirulina supplements are great at reducing sugar cravings and helping to normalize fluctuating blood sugar levels. This product, in both powder and tablet form, is an effective remedy for low blood sugar, and I love adding spirulina to my morning smoothies with banana, strawberry, protein powder, and coconut oil to keep my blood sugar stable with very morning.
- Whey protein.
Whey protein supplies the body with essential amino acids such as glutamine, which helps stabilize the body's sugar stores. It can help prevent blood sugar spikes. If you can't tolerate whey protein, try rice protein or hemp protein.
- Omega-3. Healthy fats like omega 3s help your body store nutrients more efficiently so you don't experience blood sugar spikes. Omega-3 fatty acids, such as fish oil, also reduce inflammation that can result from hypoglycemia and low blood sugar.
- Dandelion root. Dandelion root is great for maintaining blood sugar levels and is good for the pancreas. Try drinking dandelion tea several times a day or adding dandelion to your favorite smoothies.
- Milk thistle. It is also useful for the liver and pancreas and is able to normalize blood glucose levels. A standard dose of 200 mg is recommended.
Sources:
- http://www.diabetes.org/living-with-diabetes/treatment-and-care/blood-glucose-control/hypoglycemia-low-blood.
Learn more