Ritalin sex drive
Managing Your Sex Life With ADHD
ADHD doesn't disappear in the bedroom. In fact, research suggests that people with ADHD have a lower sex drive than those without the condition. Some may find themselves unable to concentrate on sex long enough to fully enjoy it, while others may become overly sexually active to the point that it appears to be a sexual addiction. And some may engage in risky sexual behavior as a result of their ADHD symptoms.
Sexual problems can stem from symptoms or even ADHD treatment. Certain features of the disorder can have a direct effect on a person's sexual function, as can side effects of medications prescribed for ADHD.
How ADHD Affects Your Sex LifeADHD symptoms that can cause problems with your sex life include:
- Impulsivity. Adults with ADHD may impulsively pursue sexual activity. That same impulsiveness may prompt risky sexual behaviors such as unprotected sex. Adults with ADHD may find that their impulsive nature make them poor lovers, as they are anxious to move quickly to the next activity in their lives.
"They want to get through it as fast as they can, not considering their partner," says Constance Wood, PhD, a psychologist in Houston.
- Inability to pay attention. ADHD adults jump from one thought to the next and find it hard to exist in the moment. They may find that other thoughts keep them from fully enjoying sexual activity. "Sex requires a certain amount of attention and good judgment," Wood says. "Problems with their lives race through their heads while they are having sex and distract them." People with ADHD may even find themselves unable to complete the sex act as they become diverted and lose interest.
- Hyperactivity. Researchers believe that hyperactivity can affect the sex drives of people who suffer from the disorder, creating a high level of arousal that leads to frantic sexual pursuit in order to relieve their inner tensions. Adult ADHD patients experiencing hyperactive sexuality may find themselves drawn to edgier sexual practices such as fetishism and exhibitionism.
Some ADHD medications can have an effect on a person's sex drive, as well. Antidepressants like bupropion (Wellbutrin) used to treat ADHD can cause reduced sexual desire. ADHD stimulants (Adderall, Ritalin) also can affect a person's libido, although reports vary regarding that effect — some sources say stimulants increase libido, while others say they reduce sex drive and cause erectile dysfunction.
Overcoming ADHD-Related Sexual ProblemsSolving sexual issues brought on by ADHD often involves successfully treating the disorder itself. ADHD treatments include:
- Medication. Finding a medication that can quell the impulses and hyperactivity of ADHD without affecting your sex drive may be a process of trial and error, but ultimately you should be better able to focus on — and enjoy — sex. "If you're taking your medication, that's certainly going to help sexually and otherwise," Wood says.
- Therapy. Different types of therapy can help adults with ADHD.
 Cognitive-behavioral therapy can help you better understand how adult ADHD is controlling your behavior and take steps to prevent it from recurring. Psychotherapy can help you get to the root of the disorder and the damage it has done to your life. "Psychotherapy allows [patients to] talk about what's lying underneath, the problems or difficulties with the marriage and themselves," Wood says.
Cognitive-behavioral therapy can help you better understand how adult ADHD is controlling your behavior and take steps to prevent it from recurring. Psychotherapy can help you get to the root of the disorder and the damage it has done to your life. "Psychotherapy allows [patients to] talk about what's lying underneath, the problems or difficulties with the marriage and themselves," Wood says.
Regardless of the sexual problem, be it low libido or an overactive sex drive, adults with ADHD can find a solution through any number of personalized treatment plans.
Does Ritalin have sexual side effects?
Dear Reader,
Sexual side effects associated with medications can certainly be frustrating, and while they aren't the most common reported concern for those taking Ritalin (generic name: methylphenidate), it can impact some folks in this way. Methylphenidate is a medication used to treat attention deficit/hyperactivity disorder (ADHD), but methylphenidate isn’t just for ADHD. It’s also used to treat narcolepsy, Parkinson's disease, and depression. Though these meds may hamper the bedroom vibe for some people because it may decrease sex drive, there could be other reasons for not experiencing the "big bang" — such as stress, a psychological condition, or other medications that are taken simultaneously. Some other drugs prescribed for mental health conditions — including selective serotonin reuptake inhibitors (SSRIs) — have been shown to have sexual side effects, too. Therefore, there are a lot of possible reasons why someone may experience a hard time getting... um... hard.
It’s also used to treat narcolepsy, Parkinson's disease, and depression. Though these meds may hamper the bedroom vibe for some people because it may decrease sex drive, there could be other reasons for not experiencing the "big bang" — such as stress, a psychological condition, or other medications that are taken simultaneously. Some other drugs prescribed for mental health conditions — including selective serotonin reuptake inhibitors (SSRIs) — have been shown to have sexual side effects, too. Therefore, there are a lot of possible reasons why someone may experience a hard time getting... um... hard.
To answer your question more specifically: do problems reaching orgasm or ejaculating make the list of side effects? Not exactly. Rather, the documented sexual side effects from methylphenidate include decreased sex drive, frequent or painful erections, and priapism (when an erection is sustained for several hours). Priapism is quite a rare and serious side effect. If the condition is suspected, it requires immediate medical attention.
While methylphenidate may impact some folks' sex lives more directly, some of the other possible side effects might be indirectly affecting a person's life in the bedroom. Common side effects include:
- Nervousness
- Irritability
- Insomnia or restlessness
- Nausea, vomiting, stomach pain, heartburn, or loss of appetite
- Diarrhea
- Headaches
- Slowed growth
- Dry mouth
- Numbness or tingling in the hands or feet
- Increased heart rate
- Elevated blood pressure
List adapted from MedlinePlus.
If someone taking methylphenidate experiences chest pain, irregular heart rates, fainting, seizures, fevers, and hives or rashes, they may benefit from getting it checked out. Researchers are constantly learning more about the short- and long-term effects of medications, so there may be more research in the future to indicate whether libido or sexual performance may be affected. Additionally, while methylphenidate can treat a number of conditions guided by a health care provider, taking an amount other than the dose prescribed or using it when it hasn’t been specifically prescribed for you might increase the risk of adverse effects, including those affecting desire and sexual functioning.
Additionally, while methylphenidate can treat a number of conditions guided by a health care provider, taking an amount other than the dose prescribed or using it when it hasn’t been specifically prescribed for you might increase the risk of adverse effects, including those affecting desire and sexual functioning.
In any case, there are a range of possible explanations for experiencing sexual difficulties both related to using this medication and sans pharmaceutical interference. As such, it’s good to know that a health care provider can be a great resource in figuring out the most beneficial and safest dose and combination of treatments to keep the libido as alive and kickin’ as possible.
Secrets of the libido: why is sex enough for someone once a month, and someone does not mind three times a day?
Why do we all need different amounts of sex, where do asexuals come from (and who are demisexuals?!), how do sports, drugs and psychological state affect libido? All this is told by Daria Varlamova and Elena Foer in the book “Sex. From the neuroscience of libido to virtual porn. Popular Science Guide” is a novelty from Alpina Non-Fiction and the Evolution Foundation.
From the neuroscience of libido to virtual porn. Popular Science Guide” is a novelty from Alpina Non-Fiction and the Evolution Foundation.
Is there a "normal libido"?
Each of us is naturally given a certain sexual temperament: for some, two times a month is enough, and for others, even three times a day. We compare ourselves to others all the time, and that goes for our sex life as well. Do other people want sex as often as we do? Do they do it that often? What level of libido makes you "cold" and what makes you "worried"? As with all questions of normality, here we run into a duality of methods of assessment: there is a statistical norm (“I want sex about as often as most people of my sex and age group”) and a functional one (“I want sex often enough that he was an important part of my life, but it does not distract me from self-realization, friendship and other useful things”). The statistical norm is simpler and clearer, but the functional norm reflects the most important thing - how comfortable you are with you. nine0005
nine0005
First, dry numbers: according to a large international survey (26,000 people) conducted by Durex (it is worth noting here that the condom manufacturer clearly had its own interest, so the data should be treated accordingly) in 2008, Russians on average had sex 143 times a year. That is almost three times a week. Not bad, right? We were in third place after the Brazilians and the Greeks. By comparison, Americans only had sex 85 times a year. True, there is not so much benefit from this information - for someone this particular year could be unsuccessful (or, conversely, very successful), and the average indicators do not say anything about the scatter of options. nine0005
It happens that ideally matched partners have hormones raging with different intensity.
No one undertakes to determine the universal norm of the need for sex - even the so-called hypoactive disorder of sexual desire, which we will talk about later, appeared in psychiatric reference books because some people experienced discomfort due to their unwillingness to make love. If all these citizens said: “Great! This gives me a lot of free time for reading, sports and other pleasant things. Also, you don't have to worry about protection. How lucky I am!” (which is exactly what some asexuals do), no one could attribute a pathological condition to them, because, as psychiatrists like to say: "No complaints - no diagnosis." nine0005
If all these citizens said: “Great! This gives me a lot of free time for reading, sports and other pleasant things. Also, you don't have to worry about protection. How lucky I am!” (which is exactly what some asexuals do), no one could attribute a pathological condition to them, because, as psychiatrists like to say: "No complaints - no diagnosis." nine0005
So everything depends on the subjective assessment of the quality of life. Which is partly related to how your temperament coincides with the temperament of your partner (s) - after all, it happens that people who are very close in spirit and ideally suited to each other in everything else have hormones raging with different powers. And one more thing - with the ideas of “normal” sexuality accepted in society.
Now is the time to remember Dr. House's famous phrase: "Everyone lies." And they lie a lot about sex - to friends, partners and even scientists during sociological surveys. For example, The New York Times columnist, economist Seth Stevens-Davidowitz, was not too lazy and compared the data of a large American General Social Survey study on the frequency of sex and condom use. According to men's responses, it turned out that heterosexual Americans over 18 used approximately 1.6 billion condoms per year. nine0005
According to men's responses, it turned out that heterosexual Americans over 18 used approximately 1.6 billion condoms per year. nine0005
Libido is a fragile and capricious thing.
Heterosexual women in the same age group used 1.1 billion condoms during the same period. Who was telling the truth? But no one: according to economic statistics, no more than 600 million condoms are sold in the United States a year. Therefore, trying to determine the "normality" of one's temperament by comparing oneself with other people is an idea that is obviously a failure. It is much more important to monitor whether you are comfortable with your own libido and whether there are any sudden, incomprehensible changes with it. But this is a fragile and capricious thing, and even within the framework of one organism it can fluctuate greatly depending on the following factors. nine0005
Balance of hormones and neurotransmitters
We are accustomed to associate attraction with chemistry, and, indeed, the balance of neurotransmitters plays a critical role in this mechanism. First of all, dopamine, on which our reward system works: we have already said that this neurotransmitter is “responsible” for the persistent desire for something. Dopamine levels can be increased by new bright stimuli, and psychostimulants (primarily amphetamines, Ritalin and cocaine) also affect dopamine metabolism. Testosterone, estrogen, and oxytocin are also directly related to libido, and indirectly, progesterone and serotonin. nine0005
First of all, dopamine, on which our reward system works: we have already said that this neurotransmitter is “responsible” for the persistent desire for something. Dopamine levels can be increased by new bright stimuli, and psychostimulants (primarily amphetamines, Ritalin and cocaine) also affect dopamine metabolism. Testosterone, estrogen, and oxytocin are also directly related to libido, and indirectly, progesterone and serotonin. nine0005
Fluctuations in sexual temperament can be a symptom of a mental disorder: for example, in the hypomanic or manic phase of bipolar affective disorder, interest in sex increases, while in anxiety disorders and depression it decreases. The catch is that the newest generation of
antidepressants - selective serotonin reuptake inhibitors - also often lead to a decrease in libido. Testosterone is somehow connected with the desire for a variety of partners - in polygamous men and women, the level of this hormone is higher than in monogamous ones. A weak libido can also be associated with problems with the thyroid gland - a lack of thyroid hormones leads to both depression and a decrease in interest in sex. nine0005
A weak libido can also be associated with problems with the thyroid gland - a lack of thyroid hormones leads to both depression and a decrease in interest in sex. nine0005
Women's cycle
In women, desire is associated with the menstrual cycle - a few days before ovulation, you begin to want sex more and more, and the peak of love comes a couple of days before or after the release of the egg. Interestingly, this pattern is associated with an increase in the level of not only estrogen, but also, according to some sources, testosterone, which is considered to be the “male” hormone. But in the second half of the cycle, estrogen and testosterone become less, and progesterone levels begin to rise, which reduces a woman's chances of having an orgasm. nine0005
Bad habits
It is commonly believed that alcohol increases libido. Almost every one of us has come across this phenomenon in a bar or at a corporate party - it is no coincidence that there were jokes about “beer glasses” through which everyone around starts to look attractive. But if we discard everyday experience (which from the point of view of science does not prove anything), the data on this topic is very contradictory - there are studies confirming that alcohol lowers testosterone levels in both women and men (which should have a negative effect on attraction), and There are studies that say otherwise. While sexologists agree that a glass of wine on a date won't hurt, regular use of alcohol as an aphrodisiac is not recommended. nine0005
But if we discard everyday experience (which from the point of view of science does not prove anything), the data on this topic is very contradictory - there are studies confirming that alcohol lowers testosterone levels in both women and men (which should have a negative effect on attraction), and There are studies that say otherwise. While sexologists agree that a glass of wine on a date won't hurt, regular use of alcohol as an aphrodisiac is not recommended. nine0005
With regard to smoking, nicotine is a vascular aggravator and, with long-term use, can contribute to erectile dysfunction and clitoral desensitization, but much less is known about its effects on libido and psychological arousal. A small study by researchers at the University of Texas at Austin found that subjective psychological arousal while watching erotic movies was reduced by almost a quarter when exposed to nicotine. Another bad habit that kills desire is lack of sleep: lack of sleep leads to a decrease in testosterone levels. nine0005
nine0005
A few days before ovulation, a woman begins to want sex more and more.
Sports
Moderate exercise increases sexual desire, but if you overdo it, problems may arise: with heavy physical exertion, the level of the hormone cortisol increases. The basic task of cortisol is to adjust the metabolism in case of stress in such a way as to conserve the energy resources of the body. With prolonged elevated levels of cortisol, the body stops responding to testosterone, and a person's interest in sex decreases. nine0005
Age
In men, the peak of temperament occurs in adolescence, in women - in 30+. This well-known fact (unlike many other well-known facts) is generally confirmed by science, although not all men and women fit into such an “activity schedule”.
Presence of psychological problems
Depression (as well as taking some antidepressants), anxiety, increased stress (in which, again, cortisol levels increase), low self-esteem, dysmorphophobic disorders (rejection of one's own appearance), can lead to a decrease in desire, difficulties in relationships with a partner (there are many nuances - the balance of power, the level of trust and respect, repressed aggression, the presence of past grievances, emotional intimacy and, of course, the partner's sexual attractiveness and technique) plus psychological trauma on sexual grounds (experience of violence or harassment). nine0005
nine0005
Aphrodisiacs
Just last year, scientists from California published a review of studies on the most popular natural aphrodisiacs. It turned out that chocolate and oysters, despite their excellent taste, do not affect libido. Ginkgo biloba, beloved by the Chinese, has been shown in one experiment to improve those whose libido had dropped due to antidepressants, but further research did not confirm this. Ginseng has proven to be beneficial for women during menopause. The effect of the Peruvian maca root has also been confirmed, which both stimulates sexual desire and fights erectile dysfunction. nine0005
Ridiculous body movements: where asexuals come from
Jokes about cold British lords and ladies may soon be considered a manifestation of intolerance: more and more people began to openly admit that they are not interested in sex and are quite comfortable with it. They may fall in love and have sexual intercourse to please their partner, but they themselves do not feel any need for sex.
The issue of considering asexuality as another type of orientation is on the agenda. But here a snag arises with definitions: who, in fact, should be considered asexual and how to distinguish people with a natural "zero" temperament in this area from those who have lost interest in "ridiculous body movements" after a psychological trauma? nine0005
In the DSM Diagnostic Handbook of Mental Disorders, the so-called “hypoactive sexual desire disorder” still exists, the diagnostic criteria for which are a reduced level of sexual desire, a decrease in the number of sexual fantasies and, as a result of all this, stress or a deterioration in relationships with a partner. All this must occur for at least six months and in more than 75% of sexual experiences (and not be explained by other problems, such as drug use or physical illness). There is no known objective "norm" of attraction (frequency, intensity, stability, severity, etc.). The specialist compares the current state with the person's previous experience, and for a diagnosis to be made, the patient must be experiencing distress, both personal and interpersonal. The symptoms of hypoactive sexual desire disorder may be similar to those experienced by asexuals, but the line between these conditions is very blurred and controversial. nine0005
The symptoms of hypoactive sexual desire disorder may be similar to those experienced by asexuals, but the line between these conditions is very blurred and controversial. nine0005
Asexuality can be singled out as another type of orientation.
Asexuality is as yet a poorly understood phenomenon, and people who identify as asexual vary widely in their experience and interest in masturbation, petting, porn, and being attractive to people of any gender. A joint study by scientists from England and the United States showed that people who consider themselves asexual are less likely to show both sexual attraction and the ability to be physically aroused. nine0005
Interestingly, however, asexuals showed no less interest in masturbation than non-asexuals and showed no difference in sexual suppression (the same inhibitory SIS we talked about at the beginning of the chapter). From this we can conclude that asexuals are indifferent not to sex itself, but to interaction with other people, and this is not due to psychological frustration.![]() True, the disadvantage of the study is that it was a questionnaire and objective measurements of physiological reactions to various stimuli were not carried out. So, there is an alternative explanation - asexuals may simply be less aware of their physical arousal. In addition, there were studies that showed that some asexuals were unable to even masturbate. nine0005
True, the disadvantage of the study is that it was a questionnaire and objective measurements of physiological reactions to various stimuli were not carried out. So, there is an alternative explanation - asexuals may simply be less aware of their physical arousal. In addition, there were studies that showed that some asexuals were unable to even masturbate. nine0005
Many asexuals were no less interested in masturbation than non-asexuals
Antisexuals bring additional confusion to this picture - people who, for ideological reasons, are not in the mood to have sex and suggest that others also give up this bad habit (the typical logic of such reasoning is well described "Kreutzer Sonata" by Leo Tolstoy: sex is greatly overrated, prevents a thinking being from thinking calmly and complicates relationships). Among them can be both asexuals, for some reason even in theory opposed to sexual relations, and individuals with a powerful libido, which can create great difficulties for them in implementing their own ideas in practice. nine0005
nine0005
In any case, there is still no consensus in the scientific community regarding the definition of asexuality and whether it should be considered a separate orientation, lack of orientation, dysfunction or a variant of the norm and a manifestation of sexual diversity. There are not even exact statistics on the proportion of asexuals among the population - various (and still few) polls give from 0.4 to 5% (at the same time, such self-identification is more common among women). As a result, it becomes very difficult to conduct quantitative research on asexuality - in such a modest and heterogeneous field, you can’t work very well with large samples. Therefore, the main information that we have at the moment is the results of small-scale qualitative studies (in-depth interviews and focus groups), which so far raise more questions than they give answers. nine0005
Only for love: who are demisexuals?
Almost simultaneously with asexuals in discussions about sex, another interesting category emerged - demisexuals. These are people who do not experience sexual attraction until they feel a strong emotional attachment to a partner. Such a person can abstractly evaluate the external attractiveness of other people, but his sexuality seems to be in a “sleep mode” and is activated only when strong emotions arise. From the outside it seems that there are many of them, especially among women. But still, many experience sexual attraction outside of an emotional connection, although they give it a go only in the presence of feelings or at least strong alcohol. But demisexuals claim that, in principle, they are not able to fantasize about a stormy night with a stranger. nine0005
These are people who do not experience sexual attraction until they feel a strong emotional attachment to a partner. Such a person can abstractly evaluate the external attractiveness of other people, but his sexuality seems to be in a “sleep mode” and is activated only when strong emotions arise. From the outside it seems that there are many of them, especially among women. But still, many experience sexual attraction outside of an emotional connection, although they give it a go only in the presence of feelings or at least strong alcohol. But demisexuals claim that, in principle, they are not able to fantasize about a stormy night with a stranger. nine0005
Demisexuals are interested in sex as a way to express affection, and not as a process in itself.
Of course, it is not very clear where the boundary lies - many are not ready to sleep with "anyone" (although the definition of "anyone" varies greatly - for someone, a couple of hours of heart-to-heart talk is enough to transfer a person into the category of acceptable sexual partners, and some require marriage for this), and emotional attachment can vary in strength and is not always associated with a good knowledge and understanding of a partner (some, for example, tend to project attractive images onto unfamiliar people and fall in love with them). At the same time, demisexuals position themselves in the so-called "gray zone" between asexuality and the average level of involvement in sex: they are still interested in it, but rather as a way to express affection, and not as a valuable process in itself. Since the concept is relatively new, scientific articles with the word “demisexuality” in the title are now not particularly found. But the connection between emotional attachment and sexual attraction has been studied for a long time, and scientists already have some ideas on this topic. nine0005
At the same time, demisexuals position themselves in the so-called "gray zone" between asexuality and the average level of involvement in sex: they are still interested in it, but rather as a way to express affection, and not as a valuable process in itself. Since the concept is relatively new, scientific articles with the word “demisexuality” in the title are now not particularly found. But the connection between emotional attachment and sexual attraction has been studied for a long time, and scientists already have some ideas on this topic. nine0005
According to popular belief, sex "for love" is more important for women, while men are more willing to embark on erotic adventures without too much sentimentality. The most popular study supporting this view was conducted back in 1989 by scientists from the University of Florida: pretty students and students approached students of the opposite sex and offered non-committal sex that same evening. About 75% of the guys agreed immediately, and many of those who refused suggested rescheduling the meeting. But none of the girls said, “Yes, great idea!” True, it is not very clear here where real desires intersect with gender expectations, perhaps the girls wanted frivolous adventures, but they were too shy to agree for fear of putting their reputation at risk. nine0005
But none of the girls said, “Yes, great idea!” True, it is not very clear here where real desires intersect with gender expectations, perhaps the girls wanted frivolous adventures, but they were too shy to agree for fear of putting their reputation at risk. nine0005
Both emotional attachment and physical attraction originate in the same areas of the brain.
In addition, in sex it is quite difficult to filter out "pleasure and nothing personal" from sympathy that can grow into a relationship. A 2012 study by Concordia University in Montreal found that both emotional attachment and physical attraction originate in the same brain regions, the insula and striatum. According to Canadian scientists, these sensations are rather different parts of the same spectrum of neurobiological reactions than completely different phenomena. “Love is a habit that forms when desire is rewarded,” says study author and psychologist Jim Pfaus. nine0005
Follow our news on Telegram
Author:
Katerina Reznikova,
Ritalin: Teachers - calm students.
 Government obedient citizens.
Government obedient citizens. Do children bother you? Ritalin is here to help you.
Adults also suffer from hyperactivity. ADHD syndromes have also been found in adults. Now the true reasons for the behavior of the "orange hooligans" are clear. nine0005
The Parliamentary Commission held a special meeting devoted to citizens' appeals regarding the use of addictive drugs by children, such as Ritalin,
Pharmacological correction of social maladjustment is from the developments of Soviet punitive psychiatry
medicine as social control
http://bankrabot .com/work/work_40593.html
The third major force in supporting medicalization is the pharmaceutical industry. This industry has an economic interest in medicalization, since medication is most often treated as treatment. Medicalization is also interpreted as taking drugs (Vert,1991).
Neither doctors, nor various groups, nor pharmaceutical companies alone have sufficient influence on the spread of medicalization. Therefore, successful medicalization depends on mutual interests in the activities of these and some other groups. The history of hyperkinesis illustrates this process. By the original definition, hyperkinesis lacks clear biological signs, but is known to occur in children over 5 years of age who are overly active, impulsive, and easily distracted, but who have no brain damage (Diller, 1998). Since the late 1930s, physicians have learned that amphetamines (including methamphetamine) can reduce attention deficits in adults and children, regardless of their mental status. In addition, even if biological amphetamines are stimulated, they provide an intense concentration that can cause users to become less active. These characteristics make amphetamines a natural choice for treating hyperkinesis. However, due to the fact that amphetamine is highly addictive and has dangerous side effects, doctors avoid recommending it to patients. In the absence of a viable treatment, physicians rarely made a diagnosis of hyperkinesis.
Therefore, successful medicalization depends on mutual interests in the activities of these and some other groups. The history of hyperkinesis illustrates this process. By the original definition, hyperkinesis lacks clear biological signs, but is known to occur in children over 5 years of age who are overly active, impulsive, and easily distracted, but who have no brain damage (Diller, 1998). Since the late 1930s, physicians have learned that amphetamines (including methamphetamine) can reduce attention deficits in adults and children, regardless of their mental status. In addition, even if biological amphetamines are stimulated, they provide an intense concentration that can cause users to become less active. These characteristics make amphetamines a natural choice for treating hyperkinesis. However, due to the fact that amphetamine is highly addictive and has dangerous side effects, doctors avoid recommending it to patients. In the absence of a viable treatment, physicians rarely made a diagnosis of hyperkinesis. The situation changed only at 1960 when the amphetamine Ritalin (methylphenidate) was introduced to the market (Conrad and Schneider, 1992). Ritalin has fewer short-term side effects than other amphetamines, and in the short term improves the ability to concentrate, reduces the tendency to act impulsively, and increases the desire to obey discipline. By producing Ritalin, pharmaceutical companies launched a massive campaign to sell it. According to Peter, Conrad, and Joseph Schneider, after the mid-1960s, it is practically impossible to read a medical journal or free junk magazines (sent by pharmaceutical companies to doctors) without looking at some carefully crafted advertisements such as Retalin and Dexedrine (another amphetamine). These promotional materials explain the benefits of treating hyperkinesis... and encourage doctors to diagnose and treat childhood hypermobility. Advertisements can be from one to six pages. She often advises physicians that hyperkinetic syndrome exists as a separate medical entity and that the syndrome is fully diagnosed through the patient's history, psychometric testing, and is classified on an expert scale by the Department of Health, Education and Welfare as MDM (minimal brain dysfunction).
The situation changed only at 1960 when the amphetamine Ritalin (methylphenidate) was introduced to the market (Conrad and Schneider, 1992). Ritalin has fewer short-term side effects than other amphetamines, and in the short term improves the ability to concentrate, reduces the tendency to act impulsively, and increases the desire to obey discipline. By producing Ritalin, pharmaceutical companies launched a massive campaign to sell it. According to Peter, Conrad, and Joseph Schneider, after the mid-1960s, it is practically impossible to read a medical journal or free junk magazines (sent by pharmaceutical companies to doctors) without looking at some carefully crafted advertisements such as Retalin and Dexedrine (another amphetamine). These promotional materials explain the benefits of treating hyperkinesis... and encourage doctors to diagnose and treat childhood hypermobility. Advertisements can be from one to six pages. She often advises physicians that hyperkinetic syndrome exists as a separate medical entity and that the syndrome is fully diagnosed through the patient's history, psychometric testing, and is classified on an expert scale by the Department of Health, Education and Welfare as MDM (minimal brain dysfunction). These same pharmaceutical companies also support sophisticated hyperkinesis diagnostic and treatment information packages for doctors, pay for professional conferences on the subject, and support research into the identification and treatment of hyperkinesis (1992: 159-160). In addition, pharmaceutical companies promoted Ritalin to the public, spending $610 million on direct advertising in 1996 and up to $44 million in 1990. (Diller, 1998:139). As already noted, pediatricians were a ready audience for a marketing campaign that promised to support their declining income and declining prestige. This market expanded in the late 1980s when the diagnosis of hyperkinesia was replaced with "attention deficit disorder" (ADD). Unlike hyperkinesis, the definition of NDV does not set age limits and includes girls, whose dissatisfaction is the same in nature as that of boys, and who fulfill themselves through physical activity. Many teachers, as well as paediatricians, readily adapted the concept of NDV to different situations (Diller, 1998).
These same pharmaceutical companies also support sophisticated hyperkinesis diagnostic and treatment information packages for doctors, pay for professional conferences on the subject, and support research into the identification and treatment of hyperkinesis (1992: 159-160). In addition, pharmaceutical companies promoted Ritalin to the public, spending $610 million on direct advertising in 1996 and up to $44 million in 1990. (Diller, 1998:139). As already noted, pediatricians were a ready audience for a marketing campaign that promised to support their declining income and declining prestige. This market expanded in the late 1980s when the diagnosis of hyperkinesia was replaced with "attention deficit disorder" (ADD). Unlike hyperkinesis, the definition of NDV does not set age limits and includes girls, whose dissatisfaction is the same in nature as that of boys, and who fulfill themselves through physical activity. Many teachers, as well as paediatricians, readily adapted the concept of NDV to different situations (Diller, 1998). In the face of downsizing and a simultaneous increase in the number of students, as well as the introduction of testing and competitive tasks for younger students, teachers could hardly be accused of addicting pills that make their students more capable. At the same time, teachers themselves began to diagnose NDV based on one fact of poor academic performance. Not surprisingly, the suggestion for a child to take Retalin now often comes from the teacher (Diller, 1998).
In the face of downsizing and a simultaneous increase in the number of students, as well as the introduction of testing and competitive tasks for younger students, teachers could hardly be accused of addicting pills that make their students more capable. At the same time, teachers themselves began to diagnose NDV based on one fact of poor academic performance. Not surprisingly, the suggestion for a child to take Retalin now often comes from the teacher (Diller, 1998).
Parents are also more willing to attribute their children's behavioral and educational problems to NDV than to simply bad parenting. Thus, just as those who argue that alcoholism or gambling is a disease, parents who seek to elevate their child's status without putting in the effort are spurring research into the treatment of NAD. Finally, recent changes in laws have encouraged parents to promote the diagnosis of NDD as a means of obtaining educational support for their children (Diller, 1998). Since 1991, it has been officially recognized that NDV is the basis for the assignment of federal anti-discrimination status. These statuses are established in the context of an individual educational assistance program for disabled children, as well as for children with any behavioral problems that can be regarded as a manifestation of disability. Thus, many parents have found that having their child diagnosed with NDD increases educational opportunities while decreasing the chances that the child may be expelled or expelled from educational institutions. In the same way, adults with NDV can qualify for
These statuses are established in the context of an individual educational assistance program for disabled children, as well as for children with any behavioral problems that can be regarded as a manifestation of disability. Thus, many parents have found that having their child diagnosed with NDD increases educational opportunities while decreasing the chances that the child may be expelled or expelled from educational institutions. In the same way, adults with NDV can qualify for
17
Year: 2005
WHAT ARE THEY TRYING TO "CURE" WITH RITALIN
http://www.narcom.ru/parents/parents/9.html
Deviant behavior of children and adolescents
The behavior of some children and adolescents attracts attention as a violation of norms , inconsistency with the advice and recommendations received, differs from the behavior of those who fit into the normative requirements of the family, school and society. This behavior, characterized by a deviation from accepted moral, and in some cases legal norms, is called deviant. It includes anti-disciplinary, anti-social, delinquent illegal and auto-aggressive (suicidal and self-damaging) acts. By their origin, they can be caused by various deviations in the development of the personality and its response. More often, this behavior is the reaction of children and adolescents to difficult life circumstances. It is on the verge of normal and disease and therefore should be evaluated not only by a teacher, but also by a doctor. The possibility of the appearance of deviations in behavior is also associated with the peculiarities of physical development, the conditions of education and the social environment. nine0005
It includes anti-disciplinary, anti-social, delinquent illegal and auto-aggressive (suicidal and self-damaging) acts. By their origin, they can be caused by various deviations in the development of the personality and its response. More often, this behavior is the reaction of children and adolescents to difficult life circumstances. It is on the verge of normal and disease and therefore should be evaluated not only by a teacher, but also by a doctor. The possibility of the appearance of deviations in behavior is also associated with the peculiarities of physical development, the conditions of education and the social environment. nine0005
Evaluating his body, a teenager states his physical superiority, norm or inferiority and draws a conclusion about his social value. Understanding your body is a refraction in the mind of your own abilities, as well as the perceptions and assessments of others. There may be a passive attitude towards physical weakness, or a desire to compensate for their shortcomings in another area, or try to correct them, rapid growth during puberty leads to a change in the skeleton. The delay in the formation of the neuromuscular apparatus in this case can disrupt the coordination of movements, which will manifest itself in clumsiness. Hints or reproaches of others about appearance or awkwardness cause violent affects, distort behavior. Accelerated tall boys are convinced of their masculinity and strength. They may not fight for the respect of others. Their self-confidence is also helped by the fact that they are perceived as intelligent. In this regard, they are more natural, more obedient and require less attention. Lagging behind in development, thin and undersized boys appear to others as small, immature and unadapted. They feel the need for guardianship, show rebelliousness. In order to change an unfavorable impression of themselves, they are forced to constantly show ingenuity, enterprise, “bravery”, be in sight, and by their “achievements” prove their usefulness and even indispensability in the group to which they belong. Such activity leads to communication difficulties and emotional stress, which create conditions for deviant behavior.
The delay in the formation of the neuromuscular apparatus in this case can disrupt the coordination of movements, which will manifest itself in clumsiness. Hints or reproaches of others about appearance or awkwardness cause violent affects, distort behavior. Accelerated tall boys are convinced of their masculinity and strength. They may not fight for the respect of others. Their self-confidence is also helped by the fact that they are perceived as intelligent. In this regard, they are more natural, more obedient and require less attention. Lagging behind in development, thin and undersized boys appear to others as small, immature and unadapted. They feel the need for guardianship, show rebelliousness. In order to change an unfavorable impression of themselves, they are forced to constantly show ingenuity, enterprise, “bravery”, be in sight, and by their “achievements” prove their usefulness and even indispensability in the group to which they belong. Such activity leads to communication difficulties and emotional stress, which create conditions for deviant behavior. nine0005
nine0005
Puberty also affects behavior. With premature sexual development, in some cases, predominantly emotional disorders occur, in others - behavioral disorders (pretentiousness, irascibility, aggressiveness), a disorder of drives; especially sexual. With delayed sexual development, slowness, lack of concentration, uncertainty, impulsiveness and difficulties in adaptation appear.
The occurrence of deviant behavior may be due to psychological characteristics. In younger adolescents, there are disproportions in the level and pace of personality development. The emerging feeling of adulthood leads to an overestimated level of claims, emotionality becomes unstable, characterized by sharp mood swings, rapid transitions from exaltation to a lowered mood. When a teenager encounters a lack of understanding of his aspirations for independence, as well as in response to criticism of physical abilities or external data, flashes of affect arise. The most unstable mood is observed at 11-13 years old in boys and 13-15 years old in girls. The most pronounced stubbornness falls on the same age. Older teenagers are concerned about the right to independence, they are looking for their place in life. There is a differentiation of abilities, interests, a worldview is developed, a psychosexual orientation is determined. However, purposefulness and perseverance at this age still coexist with impulsiveness and instability. Excessive self-confidence and categoricalness are combined with sensitivity and self-doubt. The desire for wide contacts coexists with the desire to be alone, arrogance with shyness, romanticism with pragmatism and cynicism, the need for tenderness with sadism. nine0005
The most pronounced stubbornness falls on the same age. Older teenagers are concerned about the right to independence, they are looking for their place in life. There is a differentiation of abilities, interests, a worldview is developed, a psychosexual orientation is determined. However, purposefulness and perseverance at this age still coexist with impulsiveness and instability. Excessive self-confidence and categoricalness are combined with sensitivity and self-doubt. The desire for wide contacts coexists with the desire to be alone, arrogance with shyness, romanticism with pragmatism and cynicism, the need for tenderness with sadism. nine0005
The development of a teenager's personality occurs under the influence of the culture and society that brought him up, is associated with socio-economic status and gender. Puberty in modern adolescents ends before the onset of social maturity. The existing freedom to choose a life path lengthens the time for adaptation. At the same time, social maturation occurs unevenly and depends on the completion of education, material independence or the onset of adulthood. A teenager in some areas of life may be unadapted and it is hard to experience his failure. For example, having authority in a group of athletes, a teenager may be completely immature in relationships with people of the opposite sex. nine0005
A teenager in some areas of life may be unadapted and it is hard to experience his failure. For example, having authority in a group of athletes, a teenager may be completely immature in relationships with people of the opposite sex. nine0005
During the life of a teenager, the range of social roles expands: a student, a participant in amateur performances, a member of a sports team, etc. However, their development is difficult, which can lead to great emotional stress and behavioral disorders. Behavioral disorders may include the following:
Hyperkinetic conduct disorder. It is characterized by a lack of persistence in activities requiring mental exertion, a tendency to jump from one activity to another without completing any of them, along with loosely regulated and excessive activity. This can be combined with recklessness, impulsiveness, a tendency to get into accidents, receive disciplinary action due to a thoughtless or defiant violation of the rules. In relationships with adults, they do not feel distance, children do not like them, they refuse to play with them. There may also be conduct disorder and low self-esteem. nine0005
There may also be conduct disorder and low self-esteem. nine0005
Conduct disorder limited to the family. It includes antisocial or aggressive behavior (protesting, rude), which manifests itself only at home in relationships with parents and relatives. There may be theft from the house, destruction of things, cruelty towards them, arson of the house.
Unsocialized conduct disorder. It is characterized by a combination of persistent antisocial or aggressive behavior with violation of social norms and with significant violations of relationships with other children. It is characterized by a lack of productive communication with peers and manifests itself in isolation from them, rejection by them or unpopularity, as well as in the absence of friends or empathic mutual bonds with peers. In relation to adults, they show disagreement, cruelty and indignation, less often the relationship is good, but without due trust. There may be associated emotional disturbances. Usually the child or teenager is alone. Typical behaviors include pugnacity, disorderly conduct, extortion or assault with violence and cruelty, disobedience, rudeness, individualism and resistance to authority, severe outbursts of anger and uncontrollable rage, destructive acts, arson,
Typical behaviors include pugnacity, disorderly conduct, extortion or assault with violence and cruelty, disobedience, rudeness, individualism and resistance to authority, severe outbursts of anger and uncontrollable rage, destructive acts, arson,
Socialized conduct disorder. It differs in that persistent antisocial (stealing, lying, skipping school, leaving home, extortion, rudeness) or aggressive behavior occurs in sociable children and adolescents. Often they are part of a group of antisocial peers, but they can also be part of a non-delinquent company. Relations with adults representing power are bad.
Mixed, behavioral and emotional disorders combination of persistently aggressive antisocial or defiant behavior with severe symptoms of depression or anxiety. in self-accusations and hopelessness, in others - behavioral disorders are accompanied by anxiety, timidity, fears, obsessions or worries about their health. nine0005
Delinquent behavior. Misdemeanors, petty offenses that do not reach the degree of crime punishable in court are implied. It manifests itself in the form of absenteeism from classes, communication with anti-social companies, hooliganism, mockery of the small and weak, extortion of money, theft from bicycles and motorcycles. Often there are fraud, speculation, home theft. The reasons are social - the shortcomings of education. 30% -80% of delinquent children have an incomplete family, 70% of adolescents have serious character disorders, 66% are accentuators. Among hospital patients without psychosis, 40% have delinquent behavior. In half of them, it was combined with psychopathy. Runaways from home and vagrancy in a third of cases are combined with delinquency. A quarter of those hospitalized - with shoots. nine0005
It manifests itself in the form of absenteeism from classes, communication with anti-social companies, hooliganism, mockery of the small and weak, extortion of money, theft from bicycles and motorcycles. Often there are fraud, speculation, home theft. The reasons are social - the shortcomings of education. 30% -80% of delinquent children have an incomplete family, 70% of adolescents have serious character disorders, 66% are accentuators. Among hospital patients without psychosis, 40% have delinquent behavior. In half of them, it was combined with psychopathy. Runaways from home and vagrancy in a third of cases are combined with delinquency. A quarter of those hospitalized - with shoots. nine0005
The first escapes occur in fear of punishment or as a reaction of protest, and then turn into a conditioned reflex stereotype. Shoots occur:
as a result of insufficient supervision;
for entertainment purposes;
as a protest reaction to excessive demands in the family;
as a reaction to insufficient attention from loved ones;
as a reaction of anxiety and fear to punishment;
due to fantasy and daydreaming;
to get rid of the guardianship of parents or caregivers; nine0135 as a result of ill-treatment by comrades;
as an unmotivated desire to change the situation, which is preceded by boredom, melancholy.
Early alcoholization and drug addiction (addictive behavior). This is the teenage equivalent of adult drinking and the onset of drug addiction. In half of the cases, alcoholism and drug addiction begin in adolescence. More than a third of delinquent adolescents abuse alcohol and are familiar with drugs. Motives for use - to be one's own in the company, curiosity, the desire to become an adult or change one's mental state. In the future, they drink, take drugs for a cheerful mood, for greater looseness, self-confidence, etc. Addictive behavior can be judged first by the appearance of mental (the desire to survive the rise, oblivion) dependence, and then physical dependence (when the body cannot function without alcohol or drugs). The emergence of group mental dependence (the desire to get drunk at every meeting) is a threatening precursor to alcoholism. The desire of a teenager to find a reason for drinking or drug addiction, the constant search for alcohol-containing drinks or drugs, is already an early sign of alcoholism, and in other cases of drug addiction. nine0005
nine0005
Deviations in sexual behavior. Adolescents have insufficiently conscious and increased sexual desire. Gender identification has not yet been completed. Therefore, deviations in sexual behavior easily occur. Adolescents with accelerated and delayed maturation are especially susceptible to them. For the former, a strong sexual desire arises long before social maturity, for the latter, there is a desire to assert themselves, overtaking peers in sexual activity. In addition, those who are lagging behind in development may become the object of seduction by their older comrades. Sexual deviations in adolescents depend on the situation and are transient. Among them may be visionism (peeping at the naked), exhibitionism (demonstration of one's nudity), manipulation of the genitals of younger children or animals. nine0005
As they grow older and with the transition to a normal sexual life, deviations disappear completely. In unfavorable cases, they become a bad habit and persist along with normal sexual behavior or resume in the absence of a normal sexual life, seductive influence.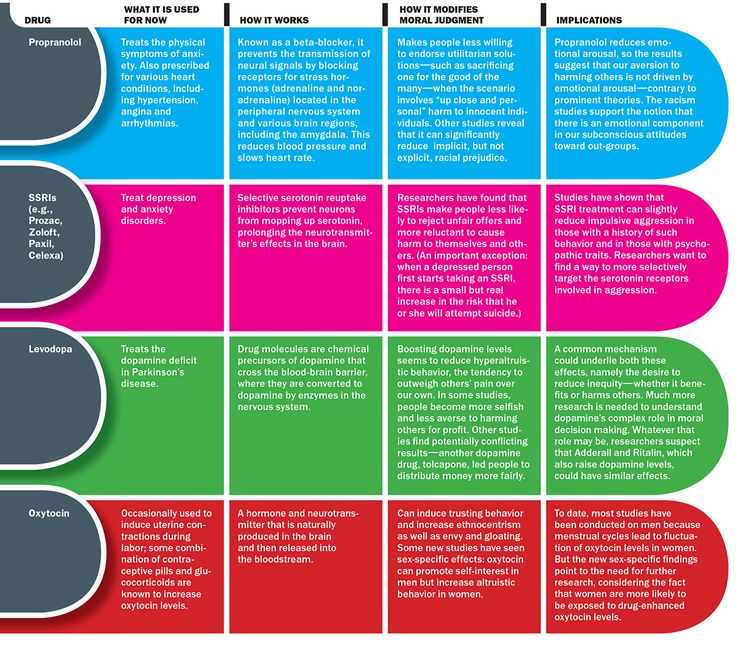 If masturbation appears before puberty, reaches a high frequency, is accompanied by neurotic symptoms or depressive experiences due to one's behavior, it should be considered as a deviation. Petting, i.e. mutual affection without sexual intercourse, to achieve orgasm, is used by adolescents in order to avoid defloration and pregnancy. It can be considered deviant if practiced before the age of puberty. The emergence of sexual relations before full physical maturation can be considered as a deviation. Adolescent promiscuity (repeated change of partners and frequent sexual intercourse) is a sexual deviation. It is often combined with alcoholism, which in some disinhibits drives, while in others leads to passive obedience. nine0005
If masturbation appears before puberty, reaches a high frequency, is accompanied by neurotic symptoms or depressive experiences due to one's behavior, it should be considered as a deviation. Petting, i.e. mutual affection without sexual intercourse, to achieve orgasm, is used by adolescents in order to avoid defloration and pregnancy. It can be considered deviant if practiced before the age of puberty. The emergence of sexual relations before full physical maturation can be considered as a deviation. Adolescent promiscuity (repeated change of partners and frequent sexual intercourse) is a sexual deviation. It is often combined with alcoholism, which in some disinhibits drives, while in others leads to passive obedience. nine0005
Transient adolescent homosexuality is usually situational. Often it manifests itself in closed educational institutions, where adolescents of the same sex are concentrated. In younger adolescents, this deviation can be caused by seduction, corruption, imitation and coercion. This deviation is more often found in male adolescents than in girls. The possibility of transient homosexuality is explained by the insufficient maturity of sexual desire. Unlike true homosexuality, an object of the opposite sex is always attractive. nine0005
This deviation is more often found in male adolescents than in girls. The possibility of transient homosexuality is explained by the insufficient maturity of sexual desire. Unlike true homosexuality, an object of the opposite sex is always attractive. nine0005
Psychogenic pathological personality formation. This is an abnormal formation of the immature personality of children and adolescents under the influence of:
ugly upbringing and chronic psychotraumatic situations;
severe experiences of life's difficulties;
protracted neuroses;
sensory and body defects or chronic diseases.
Incorrect upbringing plays a role in their development, as a result of which behavioral disorders are often added.
The behavioral disorders described here often baffle not only parents, but also experienced teachers, since educational measures are insufficient to correct adolescents. In these cases, noticeable success can be achieved with the help of psychologists who are able to uncover the true causes of frustrated behavior and give the necessary recommendations.