Psychology behind plastic surgery
Cosmetic Surgery and Psychological Issues
Psychiatry (Edgmont). 2007 Dec; 4(12): 65–68.
Published online 2007 Dec.
, MD and , MD
Author information Copyright and License information Disclaimer
This ongoing column is dedicated to the challenging clinical interface between psychiatry and primary care—two fields that are inexorably linked. In this edition of The Interface, we review two psychiatric concerns related to cosmetic surgery patients.
Cosmetic surgery continues to grow in popularity in the United States, perhaps stimulated by the impressive physical rejuvenations exhibited by media figures and/or the spate of provocative television shows illustrating the “miracle” of drastic surgical self-transformation. Regardless of the reasons, cosmetic procedures are on the rise—up 34 percent from 2005 to 2006.
1 According to the 2006 membership survey of the American Academy of Facial Plastic and Reconstructive Surgery,1 these increases were largely attributed to non-surgical cosmetic procedures (e. g., Botox injections, microdermabrasion treatments, hyaluronic acid injections, chemical peels, dermal fillers, fat injections).
Additional findings of the 2006 membership survey1 indicate that blepharoplasty was the most commonly performed cosmetic surgical procedure, followed by rhinoplasty and rhytidectomy. These procedures were followed, in turn, by hair transplantation, lip augmentation, laser resurfacing, forehead lifts, and breast enhancement. Nearly 80 percent of the recipients of these cosmetic undertakings were Caucasian. As for the prevalence of specific cosmetic procedures among other ethnic groups, rhinoplasty was most common among African-American and Hispanic subgroups, whereas blepharoplasty was most common among Asian Americans. Nearly 60 percent of the patients reported in this survey underwent multiple facial procedures in the same year.
Clearly, cosmetic procedures are on the increase in the US. As a result, these patients are not uncommon in primary care and psychiatric settings. But, how much do we really know about the psychological issues related to these individuals? In this article, we focus on two important psychiatric phenomena among cosmetic surgery patients: 1) the suicide risk among women who have undergone breast augmentation surgery and 2) body dysmorphic disorder (BDD).
But, how much do we really know about the psychological issues related to these individuals? In this article, we focus on two important psychiatric phenomena among cosmetic surgery patients: 1) the suicide risk among women who have undergone breast augmentation surgery and 2) body dysmorphic disorder (BDD).
In the past seven years, a series of studies have consistently suggested an increased risk of suicide among women who have undergone cosmetic breast augmentation surgery. In the only available US study, Brinton and colleagues2 retrospectively examined the risk for completed suicide in a cohort of over 13,000 women who had received cosmetic breast augmentation surgery. During the study period, on average about 14 years after the procedure, the standardized mortality rate (SMR) (i.e., the ratio of the observed mortality rate to the predicted mortality rate in the general population) for suicide in this study sample was 1.54 (95% confidence interval, 1.0–2.4). In a subsequent examination of these participants approximately five years later,
3 the SMR for suicide was 1. 63 (95% confidence interval, 1.1–2.3). In a prospective study by Koot and colleagues4 of over 3500 Swedish women who had undergone cosmetic breast augmentation surgery, investigators again found an increased risk of suicide (SMR of 2.9; 95-percent confidence interval, 1.6–4.8). In studies among Finnish5 and Danish6 women, the SMRs for suicide following breast augmentation surgery were 4.26 (95% confidence interval, 1.56–9.26) and 3.1 (95% confidence interval, 1.7–5.2), respectively. Finally, in a retrospective study of Canadian women who had cosmetic breast augmentation surgery, Villenueve and colleagues7 found a SMR for suicide of 1.73 (95% confidence interval, 1.31–2.24). Rohrich and colleagues8 caution that these findings may be related to random chance, given the small absolute number of deaths among the various samples. However, these studies entailed different methodologies, varying patient characteristics, and various research groups, yet each came to the same conclusion: There is a slightly higher risk (just over twice that found in the general population) of suicide among women with breast implants.
63 (95% confidence interval, 1.1–2.3). In a prospective study by Koot and colleagues4 of over 3500 Swedish women who had undergone cosmetic breast augmentation surgery, investigators again found an increased risk of suicide (SMR of 2.9; 95-percent confidence interval, 1.6–4.8). In studies among Finnish5 and Danish6 women, the SMRs for suicide following breast augmentation surgery were 4.26 (95% confidence interval, 1.56–9.26) and 3.1 (95% confidence interval, 1.7–5.2), respectively. Finally, in a retrospective study of Canadian women who had cosmetic breast augmentation surgery, Villenueve and colleagues7 found a SMR for suicide of 1.73 (95% confidence interval, 1.31–2.24). Rohrich and colleagues8 caution that these findings may be related to random chance, given the small absolute number of deaths among the various samples. However, these studies entailed different methodologies, varying patient characteristics, and various research groups, yet each came to the same conclusion: There is a slightly higher risk (just over twice that found in the general population) of suicide among women with breast implants.
The explanation for these findings remains unknown. However, previous studies indicate that there may be meaningful differences between women with breast implants and women in the general population. For example, in contrast to women in the general population, women with breast implants have been found to have significantly lower body mass indices and greater likelihoods of cigarette smoking;9 more induced abortions and fewer live births;10 and lower educational levels, earlier ages at first delivery, and more screenings for breast disease.11 However, other potential differences warrant further study, including the prevalence of Axis I and II disorders. Interestingly, in the PsycINFO database, we were unable to locate any articles relating to breast augmentation patients and Axis II disorders.
According to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, BDD is designated as an Axis I disorder that is characterized by an individual's intense preoccupation with an imagined defect in appearance. If a physical anomaly is actually present, the individual's preoccupation with it is markedly excessive. As with many other Axis I disorders, the individual must experience significant distress and/or functional impairment.
If a physical anomaly is actually present, the individual's preoccupation with it is markedly excessive. As with many other Axis I disorders, the individual must experience significant distress and/or functional impairment.
BDD occurs in up to one percent of the general population,12 but appears to be much more prevalent in patients seeking cosmetic surgery. For example, in a review of the cosmetic-surgery literature, Glaser and Kaminer found prevalence rates of BDD between 7 and 15 percent. As for specific studies among cosmetic surgery patients, Sarwer and colleagues13 found a seven-percent prevalence rate of BDD. In an Italian sample, Altamura and colleagues14 found that the prevalence of formal BDD was 6.3 percent; however, the prevalence of subclinical or subthreshold BDD among these patients was 18.4%. Finally, in a Dutch sample consisting of patients from both dermatology and plastic surgery clinics, 8.5 percent screened positively for BDD. 15
15
Comorbidity in psychiatric patients with BDD. Among general psychiatric patients with BDD, past investigators have examined the prevalence of comorbid psychological characteristics as well as formal Axis I and II psychiatric disorders. Compared with non-BDD samples, psychiatric patients with BDD appear to have higher levels of anger and hostility;16 lower self esteem and higher levels of perfectionism;17 higher frequencies of childhood abuse and neglect;18 and more frequent suicidal ideation and attempts.19 Comorbid Axis I disorders include major depression (74%),20 substance use disorders (49%),21 social phobia (39%),22 eating disorders (33%),23 and obsessive-compulsive disorder (30%).24 There are also psychotic and nonpsychotic variants of BDD,25 further broadening Axis I possibilities. Axis II disorders are also apparently common, particularly Cluster C disorders. 26
26
Comorbidity in cosmetic-surgery-seeking patients with BDD. Psychiatric disorders have also been investigated in BDD patients who are seeking cosmetic surgery. These patients appear to have high prevalence rates of several comorbid Axis I disorders including major depression, social phobia, and obsessive-compulsive disorder.22 Compared to patients without BDD seeking cosmetic surgery, those with BDD also have significantly higher rates of Axis II disorders including borderline, avoidant, paranoid, schizotypal, and obsessive-compulsive personality disorders.26
Both psychiatrists and primary care physicians are likely to encounter increasing numbers of patients in their practices who are either seeking or have undergone cosmetic surgery. Two psychiatric phenomena are of potential concern: 1) the heightened risk of suicide among women following breast augmentation surgery and 2) the high prevalence of BDD and its associated psychiatric comorbidities. Being alert to these specific psychiatric maladies in cosmetic surgery patients will hopefully enhance prompt diagnosis and effective treatment in both practice settings.
Being alert to these specific psychiatric maladies in cosmetic surgery patients will hopefully enhance prompt diagnosis and effective treatment in both practice settings.
Randy A. Sansone, Dr. R. Sansone is a professor in the Departments of Psychiatry and Internal Medicine at Wright State University School of Medicine in Dayton, Ohio, and Director of Psychiatry Education at Kettering Medical Center in Kettering, Ohio.
Lori A. Sansone, Dr. L. Sansone is a family medicine physician in practice (government service) at Wright-Patterson Air Force Base. The views and opinions expressed in this column are those of the authors and do not reflect the official policy or the position of the United States Air Force, Department of Defense, or US government.
1. American Society of Facial Plastic and Reconstructive Surgeons (AAFPRS) 2006 Membership Survey: Trends in Facial Plastic Surgery. Alexandria, VA: American Society of Facial Plastic and Reconstructive Surgeons; 2006. [Google Scholar]
2. Brinton LA, Lubin JH, Burich MC, et al. Mortality among augmentation mammoplasty patients. Epidemiol. 2001;12:321–6. [PubMed] [Google Scholar]
Brinton LA, Lubin JH, Burich MC, et al. Mortality among augmentation mammoplasty patients. Epidemiol. 2001;12:321–6. [PubMed] [Google Scholar]
3. Brinton LA, Lubin JH, Murray MC, et al. Mortality rates among augmentation mammoplasty patients: An update. Epidemiology. 2006;17:162–9. [PubMed] [Google Scholar]
4. Koot VCM, Peeters PHM, Granath F, et al. Total and cause specific mortality among Swedish women with cosmetic breast implants: Prospective study. BMJ. 2003;326:527–8. [PMC free article] [PubMed] [Google Scholar]
5. Pukkala E, Kulmala I, Hovi SL, et al. Causes of death among Finnish women with cosmetic breast implants, 1971–2001. Ann Plast Surg. 2003;51:339–42. [PubMed] [Google Scholar]
6. Jacobsen PH, Holmich LR, McLaughlin JK, et al. Mortality and suicide among Danish women with cosmetic breast implants. Arch Int Med. 2004;164:2450–5. [PubMed] [Google Scholar]
7. Villeneuve PJ, Holowaty EJ, Brisson J, et al. Mortality among Canadian women with cosmetic breast implants. Am J Epidemiol. 2006;164:334–41. [PubMed] [Google Scholar]
Am J Epidemiol. 2006;164:334–41. [PubMed] [Google Scholar]
8. Rohrich RJ, Adams WP, Potter JK. A review of psychological outcomes and suicide in aesthetic breast augmentation. Plast Reconstr Surg. 2007;119:401–8. [PubMed] [Google Scholar]
9. Kjoller K, Holmich LR, Fryzek JP, et al. Characteristics of women with cosmetic breast implants compared with women with other types of cosmetic surgery and population-based controls in Denmark. Ann Plast Surg. 2003;50:6–12. [PubMed] [Google Scholar]
10. Fryzek JP, Weiderpass E, Signorello LB, et al. Characteristics of women with cosmetic breast augmentation surgery compared with breast reduction surgery patients and women in the general population of Sweden. Ann Plast Surg. 2000;45:349–56. [PubMed] [Google Scholar]
11. Brinton LA, Brown SL, Colton T, et al. Characteristics of a population of women with breast implants compared with women seeking other types of plastic surgery. Plast Reconstr Surg. 2000;105:919–27. [PubMed] [Google Scholar]
12. Glaser DA, Kaminer MS. Body dysmorphic disorder and the liposuction patient. Dermatol Surg. 2005;31:559–60. [PubMed] [Google Scholar]
Glaser DA, Kaminer MS. Body dysmorphic disorder and the liposuction patient. Dermatol Surg. 2005;31:559–60. [PubMed] [Google Scholar]
13. Sarwer DB, Wadden TA, Pertschuk MJ, Whitaker LA. Body image dissatisfaction and body dysmorphic disorder in 100 cosmetic surgery patients. Plast Reconstr Surg. 1998;101:1644–49. [PubMed] [Google Scholar]
14. Altamura C, Paluello MM, Mundo E, et al. Clinical and subclinical body dysmorphic disorder. Eur Arch Psychiatry Clin Neurosci. 2001;251:105–8. [PubMed] [Google Scholar]
15. Vulink NC, Sigurdsson V, Kon M, et al. Body dysmorphic disorder in 3 to 8% of patients in outpatient dematology and plastic surgery clinics. Ned Tijdschr Geneeskd. 2006;150:97–100. [PubMed] [Google Scholar]
16. Phillips KA, Siniscalchi JM, McElroy SL. Depression, anxiety, anger, and somatic symptoms in patients with body dysmorphic disorder. Psychiatr Q. 2004;75:309–20. [PMC free article] [PubMed] [Google Scholar]
17. Bartsch D. Prevalence of body dysmorphic disorder symptoms and associated clinical features among Australian university students. Clin Psychol. 2007;11:16–23. [Google Scholar]
Clin Psychol. 2007;11:16–23. [Google Scholar]
18. Didie ER, Tortolani CC, Pope CG, et al. Childhood abuse and neglect in body dysmorphic disorder. Child Abuse Negl. 2006;30:1105–15. [PMC free article] [PubMed] [Google Scholar]
19. Phillips KA, Menard W. Suicidality in body dysmorphic disorder: A prospective study. Am J Psychiatry. 2006;163:1280–2. [PMC free article] [PubMed] [Google Scholar]
20. Phillips KA, Didie ER, Menard W. Clinical features and correlates of major depressive disorder in individuals with body dysmorphic disorder. J Affect Disord. 2007;97:129–35. [PMC free article] [PubMed] [Google Scholar]
21. Grant JE, Menard W, Pagano ME, et al. Substance use disorders in individuals with body dysmorphic disorder. J Clin Psychiatry. 2005;66:309–16. [PMC free article] [PubMed] [Google Scholar]
22. Coles ME, Phillips KA, Menard W, et al. Body dysmorphic disorder and social phobia: Cross-sectional and prospective data. Depress Anxiety. 2006;23:26–33. [PMC free article] [PubMed] [Google Scholar]
23. Ruffolo JS, Phillips KA, Menard W, et al. Comorbdity of body dysmorphic disorder and eating disorders: Severity of psychopathology and body image disturbance. Int J Eat Disord. 2006;39:11–19. [PubMed] [Google Scholar]
Ruffolo JS, Phillips KA, Menard W, et al. Comorbdity of body dysmorphic disorder and eating disorders: Severity of psychopathology and body image disturbance. Int J Eat Disord. 2006;39:11–19. [PubMed] [Google Scholar]
24. Pavan C, Vindigni V, Semenzin M, et al. Personality, temperament and clinical scales in an Italian plastic surgery setting: What about body dysmorphic disorder? Int J Psychiatry Clin Pract. 2006;10:91–6. [PubMed] [Google Scholar]
25. Phillips KA. Psychosis in body dysmorphic disorder. J Psychiatr Res. 2004;38:63–72. [PubMed] [Google Scholar]
26. Bellino S, Zizza M, Paradiso E, et al. Dysmorphic concern symptoms and personality disorders: A clinical investigation in patients seeking cosmetic surgery. Psychiatry Res. 2006;144:73–8. [PubMed] [Google Scholar]
Plastic surgery: Beauty or beast?
Before the makeover, DeLisa Stiles--a therapist and captain in the Army Reserves--complained of looking too masculine. But on Fox's reality TV makeover show, "The Swan 2," she morphed into a beauty queen after a slew of plastic surgery procedures--a brow lift, lower eye lift, mid-face lift, fat transfer to her lips and cheek folds, laser treatments for aging skin, tummy tuck, breast lift, liposuction of her inner thighs and dental procedures. The Fox show gives contestants plastic surgery and then has them compete in a beauty pageant, which last year Stiles won.
The Fox show gives contestants plastic surgery and then has them compete in a beauty pageant, which last year Stiles won.
"The Swan" and other such plastic-surgery shows, including ABC's "Extreme Makeover" and MTV's "I Want a Famous Face," are gaining steam, but some psychologists are concerned about the psychological impact on those who undergo such drastic cosmetic surgery--and also on those who don't and may feel inadequate as a result. While such radical transformations are rare, some psychologists plan to investigate the surge in cosmetic procedures and whether these surgeries have any lasting psychological consequences.
The number of cosmetic procedures increased by 44 percent from 2003 to 2004, according to the American Society for Aesthetic Plastic Surgery. Plastic surgeons conducted a record 11.9 million procedures last year, including nonsurgical procedures like Botox and surgical procedures like breast augmentation or liposuction (see chart).
How do such procedures affect patients psychologically? A recent analysis of 37 studies on patients' psychological and psychosocial functioning before and after cosmetic surgery by social worker Roberta Honigman and psychiatrists Katharine Phillips, MD, and David Castle, MD, suggests positive outcomes in patients, including improvements in body image and possibly a quality-of-life boost too. But the same research--published in the April 2004 issue of Plastic and Reconstructive Surgery (Vol. 113, No. 4, pages 1,229-1,237)--also found several predictors of poor outcomes, especially for those who hold unrealistic expectations or have a history of depression and anxiety. The researchers found that patients who are dissatisfied with surgery may request repeat procedures or experience depression and adjustment problems, social isolation, family problems, self-destructive behaviors and anger toward the surgeon and his or her staff.
But the same research--published in the April 2004 issue of Plastic and Reconstructive Surgery (Vol. 113, No. 4, pages 1,229-1,237)--also found several predictors of poor outcomes, especially for those who hold unrealistic expectations or have a history of depression and anxiety. The researchers found that patients who are dissatisfied with surgery may request repeat procedures or experience depression and adjustment problems, social isolation, family problems, self-destructive behaviors and anger toward the surgeon and his or her staff.
Overall, there are more questions than answers regarding psychological effects of cosmetic surgery: There are few longitudinal studies and many contradictory findings, researchers note. Many studies also contain small sample sizes and short follow-ups with patients, says Castle, a professor and researcher at the Mental Health Research Institute of Victoria in Victoria, Australia.
"We really need good, large prospective studies of representative samples of patients, using well-established research instruments," Castle says. "While most people do well in terms of psychosocial adjustment after such procedures, some do not, and the field needs to be aware of this and to arrange screening for such individuals."
"While most people do well in terms of psychosocial adjustment after such procedures, some do not, and the field needs to be aware of this and to arrange screening for such individuals."
In particular, the extent to which cosmetic surgery affects patients' relationships, self-esteem and quality of life in the long-term offers many research opportunities for psychologists, says psychologist Diana Zuckerman, PhD, president of the National Research Center for Women and Families, a think tank that focuses on health and safety issues for women, children and families.
"These are fascinating issues for psychologists to look at--from the cultural phenomena to the interpersonal phenomena to the mental health and self-esteem issues," Zuckerman says.
In addition, plastic-surgery issues will increasingly affect clinician psychologists, and the area will offer new roles for them--such as conducting pre- and post-surgical patient assessments, says psychologist David Sarwer, PhD, director of the Education, Weight and Eating Disorders Program at the University of Pennsylvania. He has studied appearance-related psychological issues, including cosmetic surgery, for the last 10 years.
He has studied appearance-related psychological issues, including cosmetic surgery, for the last 10 years.
"As the popularity of plastic surgery continues to grow, many psychologists likely already have--or will encounter--a patient that has thought about or undergone a cosmetic procedure," he says. Therefore it will be increasingly important for psychologists to be able to talk with patients about their appearance concerns and what may make some one a good or bad candidate for cosmetic surgery, he says.
Research directions
Equally pressing, however, is the need for research that sheds light on plastic surgery's psychosocial effects, many psychologists agree. To help fill in the gaps, researchers suggest further studies on the following questions:
-
Does plastic surgery make patients feel better? Studies have shown that people report increased satisfaction with the body part they had surgery on, but results are mixed on whether plastic surgery boosts their self-esteem, quality of life, self-confidence and interpersonal relationships in the long term.

In a recent study, Sarwer--also an associate professor of psychology at the Center for Human Appearance at the University of Pennsylvania School of Medicine--found that a year after receiving cosmetic surgery, 87 percent of patients reported satisfaction following their surgery, including improvements in their overall body image and the body feature altered. They also experienced less negative body image emotions in social situations. The study, which was supported by a grant from the Aesthetic Surgery Education and Research Foundation, appeared in the May/June issue of the Aesthetic Surgery Journal (Vol. 25, No. 3, pages 263-269). Sarwer and his colleagues plan to follow up with the patients next year.
However, Castle's team found in their literature review--besides some positive outcomes--a link between plastic surgery and poor post-surgical outcomes for some patients, particularly for those with a personality disorder, those who thought the surgery would save a relationship and those who held unrealistic expectations about the procedure.
Some studies have even gone as far as linking dissatisfaction with cosmetic surgery procedures to suicide. For example, in one study, the National Cancer Institute found in 2001 that women with breast implants were four times more likely to commit suicide than other plastic surgery patients of the same age as the women who underwent breast implants, says Zuckerman, who in April testimony to the Food and Drug Administration (FDA) urged the FDA to deny approval of silicone gel breast implants because of a lack of longitudinal research ensuring their safety.
The other three studies on the topic found the suicide rate to be two to three times greater. Neither of the studies, however, identified a causal relationship between breast implants and suicide. Some researchers speculate that some of the surgery recipients may hold unrealistic expectations of it or have certain personality characteristics that predispose them to suicide.
-
How does cosmetic surgery affect those around the recipients? Physically attractive people often receive preferential treatment and are perceived by others as more sociable, dominant, mentally healthy and intelligent than less attractive people, according to research by psychologist Alan Feingold, PhD, in the March 1992 issue of APA's Psychological Bulletin (Vol.
111, No. 2, pages 304-341).
"It's not like looking good doesn't have real advantages--it does," Zuckerman says. "If some people get plastic surgery and other people don't, is that going to put the people who don't at all kinds of disadvantages, such as in finding a job or spouse?"
Nearly 30 years ago, many mental health professionals viewed patients who sought cosmetic surgery as having psychiatric issues, but many studies since then suggest that those who seek cosmetic surgery have few differences pathologically with those who don't have surgery, Sarwer says.
Most people are motivated to undergo cosmetic surgery because of body-image dissatisfaction, says Susan Thorpe, a lecturer in psychology at the University of Surrey in Guildford, Surrey, who conducts cosmetic surgery research.
"They want to look normal--that is, they don't want to stand out in an obvious way or to have features which cause comment or make them feel self-conscious," Thorpe says. "They also want their physical appearance to be more in line with their personalities and feel that they want all the bits of their bodies to match."
-
What effect does plastic surgery have on children and teenagers? In 2004, about 240,682 cosmetic procedures were performed on patients 18 years old or younger, and the top surgical procedures were nose reshaping, breast lifts, breast augmentation, liposuction and tummy tucks. However, very few studies have been conducted to examine the safety and long-term risks of these procedures on adolescents--an age in which teenagers are still developing mentally and physically, Zuckerman says.
-
When does changing your appearance qualify as body dysmorphic disorder (BDD)? BDD, first introduced in the revised third edition of the Diagnostic and Statistical Manual of Mental Disorders in 1987, is characterized by a preoccupation with an aspect of one's appearance.
 People with BDD repeatedly change or examine the offending body part to the point that the obsession interferes with other aspects of their life. Several studies show that 7 to 12 percent of plastic surgery patients have some form of BDD. Plus, the majority of BDD patients who have cosmetic surgery do not experience improvement in their BDD symptoms, often asking for multiple procedures on the same or other body features.
People with BDD repeatedly change or examine the offending body part to the point that the obsession interferes with other aspects of their life. Several studies show that 7 to 12 percent of plastic surgery patients have some form of BDD. Plus, the majority of BDD patients who have cosmetic surgery do not experience improvement in their BDD symptoms, often asking for multiple procedures on the same or other body features.
Sarwer often works with plastic surgeons to help them identify such psychological issues as BDD, so surgeons then can refer patients to mental health professionals. He encourages them to look for the nature of the person's appearance concern, such as whether a patient has an excessive concern with a body feature that appears normal to nearly anyone else. Part of that also includes accounting for patients' internal motivations for surgery--are they doing it for themselves or out of pressure from a romantic partner or friend? And, he encourages surgeons to ensure patients hold realistic expectations about the procedures, rather than expecting the surgery to end long-standing personal issues.
Psychology's role
Apart from research, psychologists can find clinical roles in aiding cosmetic surgery patients too, such as helping plastic surgeons conduct such assessments. For example, they can help plastic surgeons identify patients who may not adjust well psychologically or psychosocially after surgery, researchers say.
Castle says that empirically based screening questionnaires will help plastic surgeons select cosmetic surgery patients likely to experience positive psychosocial outcomes.
Sarwer has teamed with other psychologists and plastic surgeons to develop such screening questionnaires, which are included in the book "Psychological Aspects of Reconstructive and Cosmetic Plastic Surgery: Clinical, Empirical and Ethical Perspectives" (Lippincott Williams & Wilkins, 2005). The book, to be published this month, features a chapter on how to help both surgeons and mental health professionals screen for BDD, as well as explore the relationships among physical appearance, body image and psychosocial functioning.
Sarwer believes more psychologists will begin to examine issues related to cosmetic surgery because of its increasing popularity and the link between appearance, body image and many psychiatric disorders, such as eating disorders, social phobia and sexual functioning. "Scientifically, we're just starting to catch up to the popularity of [cosmetic surgery] in the population," Sarwer says.
And, as more studies commence, Castle says they need to characterize the population being studied, clearly identify outcome variables and use standardized and state-of-the-art measures.
"There may be strong cultural pressures that are so unrealistic in terms of how we're supposed to look," Zuckerman adds. "Psychologists should...figure out why this is happening and what we need to know to make sure that people aren't going to be harmed by this."
Psychology and plastic surgery
Plastic surgery
Tags:
Yu. Titova:
Titova:
Hello, the MediaDoctor channel is on the air, the program “Plastic Surgery with Dr. Zakharov”. Today we have a premiere, the first issue, so I am pleased to introduce our presenter, a plastic surgeon, already known to many in the capital, Anton, I welcome you. nine0003
A. Zakharov:
Good morning, dear listeners.
Y. Titova:
Finally, we have launched your author's program in this studio. My name is Yulia Titova, and Ekaterina Kryukova, my co-host, colleague.
E. Kryukova:
Hello.
Y. Titova:
Today we will talk about plastic surgery together with psychology. Let's figure out when a plastic surgery is necessary for a patient or is it an ill-considered impulse. And do doctors dissuade patients from surgery when they realize that it is currently inappropriate. nine0003
So, let's start with, is it possible to categorize patients in psychology? Maybe, by type, impulsive, rational, or there are patients with some kind of deviations, psychological illnesses. What do you meet in your practice?
What do you meet in your practice?
A. Zakharov:
The main visitors of the plastic surgeon are absolutely normal people with adequate self-esteem, adequate perception of their own appearance, who have some wishes regarding the improvement of the composition of their own face and body. Their needs in this case are based on an absolutely objective assessment. But this is only a part of those people who come to the reception. nine0003
There are others, there are people who have a pathologically altered perception of themselves. For example, patients with body dysmorphic disorders who cannot objectively evaluate their appearance cannot form an objective image of themselves. And such changes in the psyche are only part of a much larger violation of the mental health of a person. Most often, these are changes in the structure of a psychotic disorder of one form or another, and, of course, surgical care is never indicated for such patients. They require, first of all, an examination by a psychiatrist, the aesthetic surgeon identifies these patients at the appointment and must assess the adequacy of the perception of this person by conducting a targeted conversation, discussing the details. If it does not fit into the normal framework, then he must ensure that he is provided with full-fledged psychiatric care. In no case should such patients be operated on, because the operation cannot bring them satisfaction, cannot bring reassurance, cannot give them, in principle, anything, only further stimulate their disturbance in the perception of their own appearance. nine0003
If it does not fit into the normal framework, then he must ensure that he is provided with full-fledged psychiatric care. In no case should such patients be operated on, because the operation cannot bring them satisfaction, cannot bring reassurance, cannot give them, in principle, anything, only further stimulate their disturbance in the perception of their own appearance. nine0003
E. Kryukova:
What specific markers of the patient's inadequacy will you find during the conversation? Maybe there are examples from practice?
A. Zakharov:
There are a lot of criteria for evaluating a person, and personal contact with the patient is very important for an aesthetic surgeon. This concerns not only the identification of some violations in his mental status, but also mutual understanding. Because only by understanding the true needs of a person, it is possible to draw up a treatment plan that suits him and achieve good results. nine0003
What do we pay attention to? The dialogue goes on for quite a long time, and we evaluate how focused he is on the specific details of his appearance, how much his assessment of the composition of his own face correlates with classical ideas about aesthetics and composition. How does he motivate his desire to see a surgeon? How he sees his long-term result, how ready he is to go through the rehabilitation process, how rationally he approaches the process of receiving surgical care. nine0003
How does he motivate his desire to see a surgeon? How he sees his long-term result, how ready he is to go through the rehabilitation process, how rationally he approaches the process of receiving surgical care. nine0003
Only by understanding the true needs of a person, it is possible to draw up a treatment plan that suits him and achieve good results.
E. Kryukova:
Most likely, you mean the case when the patient draws some grotesque forms of his appearance, and this becomes the main factor for refusing the operation.
A. Zakharov:
No, not only. Without a doubt, the degree of severity of self-perception disorders can be different. These can be either severe disorders that are visible immediately at the first words of the patient, and they can lead the doctor to such thoughts, or a more superficial disorder of perception, not of a psychotic level, but of a neurotic one, in which it is clear that a person is pathologically focused on his imperfections. He sees many of them in himself, he immediately wants to change one, and the second, and the third. And these needs are clearly not of an objective nature, based on some imperfections, but of a neurotic nature, when a person does not accept what is in his appearance. It can be seen that these are introduced sensations, that this is not a need formed by a long assessment, but an impulse impulse. Most often, against the background of acute stress, which changes his perception of himself for a certain period of time, he becomes dissatisfied with himself in almost everything. And, of course, this allows you to identify a person in a state of such a neurotic disorder. nine0003
He sees many of them in himself, he immediately wants to change one, and the second, and the third. And these needs are clearly not of an objective nature, based on some imperfections, but of a neurotic nature, when a person does not accept what is in his appearance. It can be seen that these are introduced sensations, that this is not a need formed by a long assessment, but an impulse impulse. Most often, against the background of acute stress, which changes his perception of himself for a certain period of time, he becomes dissatisfied with himself in almost everything. And, of course, this allows you to identify a person in a state of such a neurotic disorder. nine0003
E. Kryukova:
Do you recommend such patients to sleep over and think about this idea?
A. Zakharov:
Any patient has an opportunity to think, because an aesthetic operation is not a trip to a hairdresser's or a manicure salon. This is a rather serious event, which implies a full scope of examination and preoperative preparation, a full assessment of all vital systems in order to make anesthesia safe. It all takes time. nine0003
It all takes time. nine0003
There is a fairly large time gap between when the patient gets to the initial appointment and when he gets to the operating room. Because recovery takes time. This is, most often, a few weeks, for this the patient needs to take a vacation, find this time. Any actively practicing surgeon has a fairly large record ahead, this also leaves some kind of imprint. Therefore, from admission to surgery, patients take from a month to a year. Sometimes those who were at the reception a year ago come to the operating room and decide that they want to perform an aesthetic operation, and only a year later this is realized. There is time to think. And without a doubt, if we see a person in such a state of stress, then we simply appoint a second consultation, offer a preliminary treatment plan, but give the opportunity to discuss it in a month so that the person, in a state of psychological comfort, can assess our capabilities, his needs, once again clarify some of your details. And then implement something according to the corrected treatment plan, if it still needs it. nine0003
And then implement something according to the corrected treatment plan, if it still needs it. nine0003
Y. Titova:
Today, natural beauty is valued more, it's no secret to anyone, and men scream about it very loudly, begging modern girls not to go under the plastic surgeon's knife. But a little earlier, just a few years ago, plastic surgery was very popular, and almost every second girl went under the knife, everyone dreamed about it, but maybe not always had the opportunity. But today, as you have already noticed, there are victims of plastic surgery who overdid it, did everything they could and everything they could not. And in the end they come to terrifying results. How does the doctor decide to still make some more adjustments to the girl's appearance, while realizing that this will not bring improvements? nine0003
A. Zakharov:
A very big, global question. I will try to answer it in parts, because each of these parts is interesting in its own way. Firstly, natural beauty is always valuable, and it is not a matter of fashion that some time ago unnatural changes were fashionable, now they are natural again, this is not so. Natural beauty always comes first. The consequence of this fact is that surgeons always try to get exactly natural results. We are talking about professional surgeons. The question is whether these results are achievable for them, because a high-quality aesthetic operation performed by a good specialist, on good equipment, correctly selected tactically for a particular person, is an operation that leads to improvement towards natural beauty, and not towards certain disharmony. Therefore, it is more a question of the quality of the services provided than of trends or fashion. nine0003
Firstly, natural beauty is always valuable, and it is not a matter of fashion that some time ago unnatural changes were fashionable, now they are natural again, this is not so. Natural beauty always comes first. The consequence of this fact is that surgeons always try to get exactly natural results. We are talking about professional surgeons. The question is whether these results are achievable for them, because a high-quality aesthetic operation performed by a good specialist, on good equipment, correctly selected tactically for a particular person, is an operation that leads to improvement towards natural beauty, and not towards certain disharmony. Therefore, it is more a question of the quality of the services provided than of trends or fashion. nine0003
Let's say that in my practice I perform only interventions that lead a person to more harmonious, natural features. What does harmonious, natural mean? Those that fit into the canonical ideas about beauty, the correct ratios, the golden ratio, and those features of appearance that have been described since Ancient Greece, Ancient Rome about how it should be right in terms of aesthetics. A high-quality aesthetic operation brings a person closer to this image, and does not move away from it. nine0003
A high-quality aesthetic operation brings a person closer to this image, and does not move away from it. nine0003
The second question: is it necessary, if a person has multiple operations, to take him for another operation. If this is a person who is currently far from the idea of natural beauty, I believe that this is only possible if this is some kind of correction that brings him closer to the true ideas of harmony, to classical ideas, and does not aggravate the existing situation due to those disharmony , which are. Is it possible to operate on the 10th, 12th time? Of course, you can, once it has to be done correctly. If the surgeon sees that he cannot improve the composition, cannot bring the face or body closer to harmonious combinations, then, probably, you should not do this. And the professional will always refuse in this case. nine0003
You know, this is a very important criterion, all surgeons, working at a high level of quality, select patients, they do not take everyone, persuading every first visitor to their clinic to do some kind of operation. On the contrary, they select from those who want, only those whom they can really help, make them happy, objectively improve their appearance. This is the meaning of selection and the meaning of interaction with all this large patient society in order to take only those who can be helped. nine0003
On the contrary, they select from those who want, only those whom they can really help, make them happy, objectively improve their appearance. This is the meaning of selection and the meaning of interaction with all this large patient society in order to take only those who can be helped. nine0003
If the surgeon sees that he cannot improve the composition, cannot bring the face or body closer to harmonious combinations, then it is probably not worth it. And the professional will always refuse in this case.
Y. Titova:
But then such an ethical moment immediately arises in my head - after all, to cut and get money for it, or to take a patient and communicate with him in an accessible way and make it clear that he does not need it.
A. Zakharov:
Ethical issues are relevant for any medical activity. And without a doubt, for aesthetic surgery, as for piece work, they are also extremely relevant.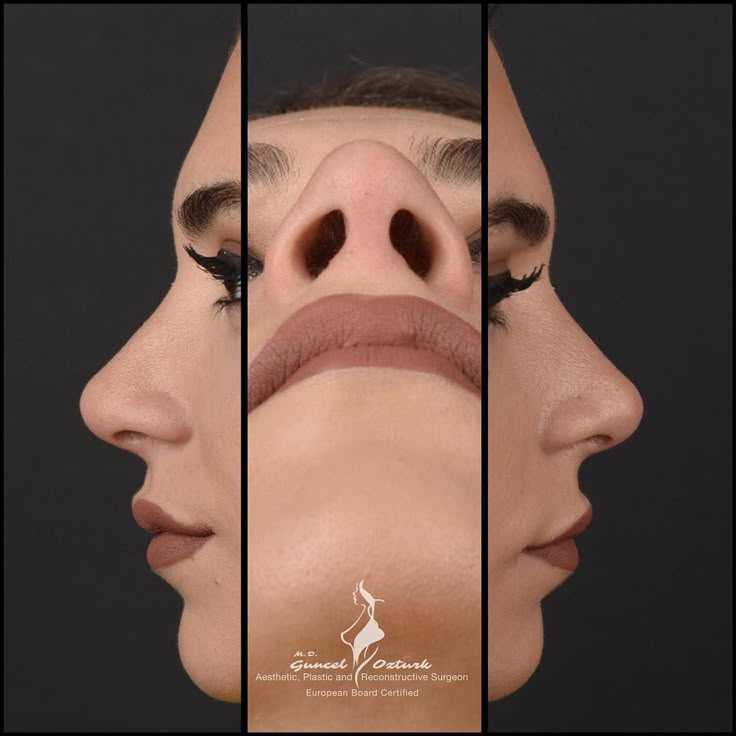 A professional will never go against his principles, as a specialist, for the sake of some momentary profits. If a patient turns to a surgeon with deliberately irrational demands, and the surgeon immediately agrees, this should be very alarming. Most of our patients, before choosing a specialist to whom they are ready to entrust their appearance, bypass 5-10 consultations of different surgeons and choose exactly the canvas that is closer to their needs. nine0003
A professional will never go against his principles, as a specialist, for the sake of some momentary profits. If a patient turns to a surgeon with deliberately irrational demands, and the surgeon immediately agrees, this should be very alarming. Most of our patients, before choosing a specialist to whom they are ready to entrust their appearance, bypass 5-10 consultations of different surgeons and choose exactly the canvas that is closer to their needs. nine0003
Without a doubt, if a person is aggressively disposed to perform some kind of operation, having received a number of refusals, he will sooner or later find that person who will easily compromise with professional ethics and his own conscience and do what a person does not need to do for his own sake. income. But this is the choice of each person. In a global sense, such tactics are not very promising for surgeons who take everyone, because the pool of negative cases and unsatisfactory results is significantly increasing. To be honest, it would be very unpleasant for me if a patient with a negative result of the operation, whom I took by some coincidence, had a place to be and thereby created a negative information background for me. I wouldn't like it. Therefore, in my practice, I do my best to prevent this from happening. And maybe even my rejection rate is too high, but I know that all those people I take for surgery will definitely look better than before, and they really need it. nine0003
I wouldn't like it. Therefore, in my practice, I do my best to prevent this from happening. And maybe even my rejection rate is too high, but I know that all those people I take for surgery will definitely look better than before, and they really need it. nine0003
If a patient approaches a surgeon with obviously irrational demands, and the surgeon immediately agrees, this should be very alarming.
Y. Titova:
Katya mentioned the moment of the second operation, we have already talked about it a little. An interesting point: we talked with the patient, who is absolutely adequate, aware of what he is doing, his choice is correct and, perhaps, at some point will improve the elements of his appearance. But after the operation, already when the rehabilitation has passed, the person has an internal conflict. He understands that this is not quite the same, although visually everything is quite harmonious and beautiful. There are such cases, and what to do? It seems that a second operation is not needed, you just need to wait, get used to it, or quickly fix everything back? nine0003
There are such cases, and what to do? It seems that a second operation is not needed, you just need to wait, get used to it, or quickly fix everything back? nine0003
A. Zakharov:
A very interesting question is the acceptance of one's own appearance after aesthetic intervention, how ready a person is to adapt to this new look. If he really wanted this, this was his true need, and this is exactly what we revealed at the initial appointment, then, of course, he will easily perceive these changes. Because this is the realization of his fantasies, his desires, his appearance, which he imagined. That is, it easily adapts to his system of perception. If he cannot accept himself in the early period, then this indicates our shortcomings in the selection. This means that not all details were agreed upon, not all points were discussed, and we are trying to ensure that such cases do not occur. nine0003
But there is another aspect here. All those changes that we see in relation to aesthetics do not occur at once, they take time.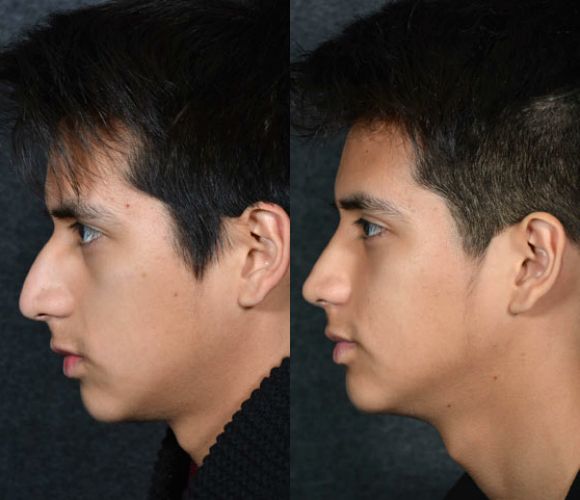 Rehabilitation after any plastic surgery takes time until the swelling subsides, while the person is recovering, everything manifests itself gradually. This is not a sudden change of image, and this gradual rehabilitation allows a person to smoothly enter into these new sensations. That is, nature itself does not allow everything to be done so quickly, thus adaptation is much easier. There are operations with a very long rehabilitation due to their technological features, and this allows you to get used to it. nine0003
Rehabilitation after any plastic surgery takes time until the swelling subsides, while the person is recovering, everything manifests itself gradually. This is not a sudden change of image, and this gradual rehabilitation allows a person to smoothly enter into these new sensations. That is, nature itself does not allow everything to be done so quickly, thus adaptation is much easier. There are operations with a very long rehabilitation due to their technological features, and this allows you to get used to it. nine0003
E. Kryukova:
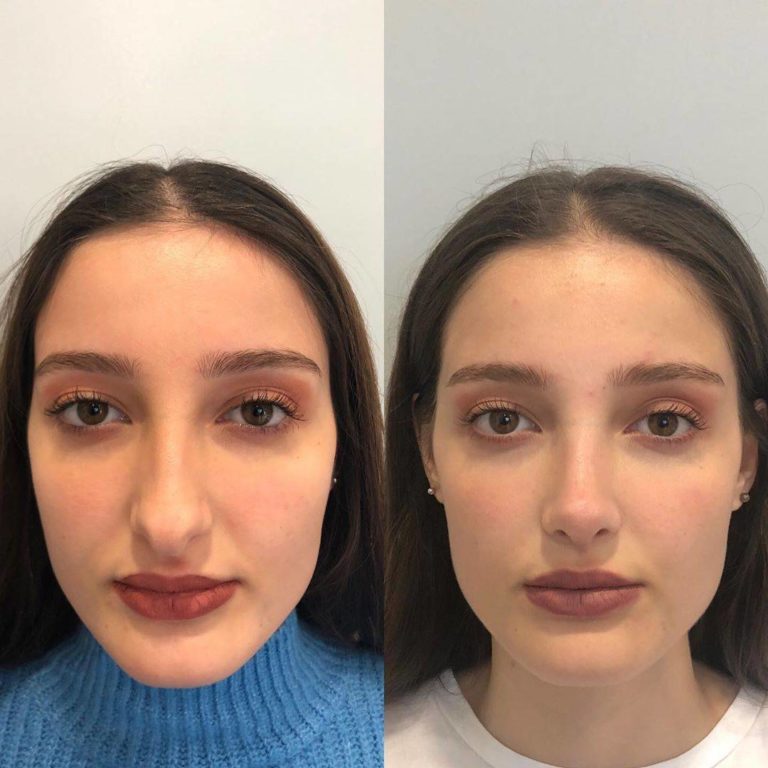
If we talk about specific operations, in rhinoplasty there is a very high percentage of repeated operations, secondary ones. It depends on the patient or on the doctor, whose fault is it?
A. Zakharov:
There is no one's fault here, there is nature, its laws. The fact is that all rhinoplasty operations have such an instability factor as scarring between the bone and cartilage framework and the integumentary soft tissues, which are difficult to predict. And most of the difficulties with rhinoplasty are connected precisely with this, because even with an ideally created bone and cartilage framework of the nose and a favorable prognosis, rough scarring can always intervene and disrupt our composition, on the one hand. nine0003
And most of the difficulties with rhinoplasty are connected precisely with this, because even with an ideally created bone and cartilage framework of the nose and a favorable prognosis, rough scarring can always intervene and disrupt our composition, on the one hand. nine0003
On the other hand, the nose is the central part of the face, and the demands of patients on ideal proportions and contours in relation to the nose are very high. Therefore, the combination of these factors - the natural complexity with scarring and the impossibility of predicting it, although we can influence it during the treatment process, is our main task after the operation, and the peculiarities of patients' assessment of their appearance make this manipulation so unpredictable in terms of long-term results. Because there may be a great nose, but a person does not like it. And the situation may be reversed: everything seems to be pleasant, but the surgeon sees that there are some elements of asymmetry, elements of contour violations. So there has to be a compromise here. Unfortunately, in relation to any aesthetic operation, there is no absolute that we get everything perfect, as in the picture. We live in the real world, and surgery, despite its active development, despite the high technologies that are in our hands, the huge perfectionism of specialists that they put into their work, still remains medicine, and not an exact science with its own characteristics. nine0003
So there has to be a compromise here. Unfortunately, in relation to any aesthetic operation, there is no absolute that we get everything perfect, as in the picture. We live in the real world, and surgery, despite its active development, despite the high technologies that are in our hands, the huge perfectionism of specialists that they put into their work, still remains medicine, and not an exact science with its own characteristics. nine0003
Most of the difficulties with rhinoplasty are due to the fact that even with an ideally created bone and cartilage framework of the nose and a favorable prognosis, rough scarring can always intervene and disrupt the composition
E. Kryukova:
You correctly said that the nose is the central part of the face, and a person is very picky about this area. Do they often come unreasonably on this account?
A. Zakharov:
Aesthetic surgeons are often visited unreasonably, both in relation to rhinoplasty and in relation to all other operations. Regarding some excessive complexity of this operation, I am not ready to agree with you, because in our practice there are much more complex operations than rhinoplasty. A number of reconstructive interventions, a number of anti-aging interventions on the face are technologically much more complicated than rhinoplasty, they have more nuances, more risks. It's just that this is such a trend in the perception of our activities that rhinoplasty is a kind of calling card, the biggest difficulty. In no case. This is more due to the fact that the contingent of people who want this operation are mostly young females with an increased aesthetic sense, with increased demands on themselves and often making excessive demands on their own appearance. This is what is broadcast in the information field and the subsequent attitude to these manipulations. Although technologically this is not the most difficult operation, and rehabilitation is not the most difficult operation, and there are a lot of them, with good results.
Regarding some excessive complexity of this operation, I am not ready to agree with you, because in our practice there are much more complex operations than rhinoplasty. A number of reconstructive interventions, a number of anti-aging interventions on the face are technologically much more complicated than rhinoplasty, they have more nuances, more risks. It's just that this is such a trend in the perception of our activities that rhinoplasty is a kind of calling card, the biggest difficulty. In no case. This is more due to the fact that the contingent of people who want this operation are mostly young females with an increased aesthetic sense, with increased demands on themselves and often making excessive demands on their own appearance. This is what is broadcast in the information field and the subsequent attitude to these manipulations. Although technologically this is not the most difficult operation, and rehabilitation is not the most difficult operation, and there are a lot of them, with good results. But here the issue of preliminary study of the composition, the correct understanding of the results by both the doctor and the patient before the operation is fundamentally important. And in no case should the surgeon make decisions that lead the patient to deviate from the classical proportions of the face after performing rhinoplasty. nine0003
But here the issue of preliminary study of the composition, the correct understanding of the results by both the doctor and the patient before the operation is fundamentally important. And in no case should the surgeon make decisions that lead the patient to deviate from the classical proportions of the face after performing rhinoplasty. nine0003
E. Kryukova:
But very often a person loses his individuality after nose correction.
A. Zakharov:
Without a doubt, typical manipulations are not suitable for work in aesthetic surgery, this applies not only to rhinoplasty, but to all interventions. Of course, what suits a person with one appearance may not work at all for a person with another appearance. The high level of professional approach of an aesthetic surgeon implies individual work in each individual case. It seems to me that some kind of standardization of appearance through standard interventions with typical results is a very superficial approach, and patients see it the same way. Each person wants to preserve the individuality of his face after any operation, to remain recognizable, not to be similar in some individual features to dozens of other people, so in each case this is an individual plan. There are people who need a straight, long nose; in no case will a small nose suit them, and vice versa. It is in a preliminary dialogue with the patient that a common understanding of composition, a common understanding of aesthetics is born, and then it is simply realized in the operating room. nine0003
Each person wants to preserve the individuality of his face after any operation, to remain recognizable, not to be similar in some individual features to dozens of other people, so in each case this is an individual plan. There are people who need a straight, long nose; in no case will a small nose suit them, and vice versa. It is in a preliminary dialogue with the patient that a common understanding of composition, a common understanding of aesthetics is born, and then it is simply realized in the operating room. nine0003
Each person wants to preserve the individuality of his face after any operation, to remain recognizable, not to be similar in some individual features to dozens of other people, so in each case this is an individual plan.
Y. Titova:
Don't people come to a plastic surgeon like they go to a beauty salon: can I, like hers?
A. Zakharov:
They come with a photo or someone's Instagram and say: "I want like this. " And this is one of the actions that immediately alarms the surgeon, because it indicates that a person has a lack of self-identification, he wants to be not himself, he wants to be like someone else. This is already very suspicious, and further dialogue will reveal the true motives for the operation. This is a worrying factor, because the patient, who is really shown the operation, comes with completely different words. He says: “You know, doctor, I don’t like the fact that my nose is crooked, that it is asymmetrical, that it has a large, heavy tip. I don’t like this hunchback, it seems to me that it doesn’t make my face so winning compositionally, I would like to look better. Tell me, can I somehow improve my overall composition by working with my nose? Next, the surgeon tries to realize his vision and coordinate it with the patient. When I want to, like a neighbor or neighbor, this is a bad sign. nine0003
" And this is one of the actions that immediately alarms the surgeon, because it indicates that a person has a lack of self-identification, he wants to be not himself, he wants to be like someone else. This is already very suspicious, and further dialogue will reveal the true motives for the operation. This is a worrying factor, because the patient, who is really shown the operation, comes with completely different words. He says: “You know, doctor, I don’t like the fact that my nose is crooked, that it is asymmetrical, that it has a large, heavy tip. I don’t like this hunchback, it seems to me that it doesn’t make my face so winning compositionally, I would like to look better. Tell me, can I somehow improve my overall composition by working with my nose? Next, the surgeon tries to realize his vision and coordinate it with the patient. When I want to, like a neighbor or neighbor, this is a bad sign. nine0003
Y. Titova:
Today there are a lot of young girls who look great, but are so unsure of themselves that it's just horror. They are constantly trying to do something with themselves, various manipulations, up to plastic surgery. Will the plastic surgeon stop such a patient? After all, having done something irreversible, it still won’t make this or that person happier, how to be in this case?
They are constantly trying to do something with themselves, various manipulations, up to plastic surgery. Will the plastic surgeon stop such a patient? After all, having done something irreversible, it still won’t make this or that person happier, how to be in this case?
A. Zakharov:
In this case, of course, the operation is not necessary. nine0003
Y. Titova:
But how do you discuss it with him, you say: “You are beautiful, are you the best?”
A. Zakharov:
No, if I see that the patient has no objective indications for intervention, his requests, his needs do not correspond to our technological capabilities, and we do not have the opportunity to improve the composition through our manipulations, then This is an absolutely clear, motivated refusal. If a person continues to insist or expresses his clear confidence that he needs it, then everything depends on how he motivates such behavior. If these motives are based on objective assessments, then we can conduct a constructive dialogue and, through persuasion in this dialogue, dissuade a person. And thus: a) help him do what he does not need; b) to help ourselves not to get an unsatisfied patient, in whom we still cannot achieve the correct degree of satisfaction, why do it then. And if we see that the arguments are irrational, that this is already connected with a violation of self-perception, then here the profile specialist should work further, the profile specialist in this case is a psychiatrist. nine0003
If these motives are based on objective assessments, then we can conduct a constructive dialogue and, through persuasion in this dialogue, dissuade a person. And thus: a) help him do what he does not need; b) to help ourselves not to get an unsatisfied patient, in whom we still cannot achieve the correct degree of satisfaction, why do it then. And if we see that the arguments are irrational, that this is already connected with a violation of self-perception, then here the profile specialist should work further, the profile specialist in this case is a psychiatrist. nine0003
E. Kryukova:
Aren't you tired of such long conversations? Maybe plastic surgery needs a filter in the person of mental workers, as, for example, a psychological examination is required for sex reassignment operations, something like that, which would make your life and work easier?
A. Zakharov:
First of all, this is part of my work. And it is unlikely that anyone except me can accurately assess where I can solve the problem with my surgical capabilities, where I cannot. Let's put it this way, despite the fact that it is very emotional and time-consuming, it allows me to form the right pool of patients already for the direct surgical intervention. Of course, in borderline cases, when the surgeon cannot figure it out exactly, after all, the plastic surgeon is not a psychiatrist, and he cannot fully appreciate everything, as a specialized specialist. Although we are all close in some way to the evaluative approaches that are used in psychiatry, this is also a necessity in our work. However, there are cases when we doubt, when we are not sure, and we collectively, already with a psychiatrist, decide to perform the operation or not. nine0003
Let's put it this way, despite the fact that it is very emotional and time-consuming, it allows me to form the right pool of patients already for the direct surgical intervention. Of course, in borderline cases, when the surgeon cannot figure it out exactly, after all, the plastic surgeon is not a psychiatrist, and he cannot fully appreciate everything, as a specialized specialist. Although we are all close in some way to the evaluative approaches that are used in psychiatry, this is also a necessity in our work. However, there are cases when we doubt, when we are not sure, and we collectively, already with a psychiatrist, decide to perform the operation or not. nine0003
Almost all aesthetic surgeons work with a psychiatrist to support their own opinion with a specialized specialist in difficult situations. Some kind of preliminary filter is hard, if you pass, you will communicate with the surgeon, if you don’t pass, you won’t, in my opinion, this is unnecessary. This is way too harsh. Still, the majority of patients who apply are absolutely normal, adequate people who want rational changes for the better.
Still, the majority of patients who apply are absolutely normal, adequate people who want rational changes for the better.
Almost all aesthetic surgeons work with a psychiatrist to support their own opinion with a specialized specialist in difficult situations. nine0008
E. Kryukova:
I agree with everything, but the only point is that there are no objective medical indications in plastic surgery.
A. Zakharov:
Of course.
E. Kryukova:
This is done according to aesthetic criteria. Here you have a measure of beauty - these are ancient standards.
A. Zakharov:
Of course.
E. Kryukova:
And for other doctors it can be something completely strange. How to be here? nine0003
A. Zakharov:
You know, it's a matter of taste. In general, taste is a very light concept, somewhat ephemeral. We see that there are different brands of cars, different brands of clothing, there is a different approach to the implementation of the same tasks, but with a different aesthetic, functional component. It's the same with aesthetic surgery. Let's say I like operations that are not visible. In my perception, a high-quality aesthetic operation is one that has obvious aesthetic improvements, but it is not visible, the face does not seem to be operated on. This is the top of what I strive for in my practice, and in the vast majority of cases, this is achieved. nine0003
We see that there are different brands of cars, different brands of clothing, there is a different approach to the implementation of the same tasks, but with a different aesthetic, functional component. It's the same with aesthetic surgery. Let's say I like operations that are not visible. In my perception, a high-quality aesthetic operation is one that has obvious aesthetic improvements, but it is not visible, the face does not seem to be operated on. This is the top of what I strive for in my practice, and in the vast majority of cases, this is achieved. nine0003
Some surgeons see things differently. But every product, every service has its own consumer. Someone chooses a classic suit, someone chooses a clown nose and clown pants with long boots. Everyone has the right to their own choice, everyone gets what he wants. And the question is more to the patients. If the patient's aesthetic perception is developed, and he acts from his true motives, his needs, not introduced trends, because this is a very superficial judgment, but his true needs, then most likely he will choose something very conservative. If the patient's aesthetic perception is not developed, or these are some externally introduced superficial judgments, he has needs even for grotesque changes in appearance, again, if he turns to me, I will refuse him intervention, because I do not want such a result to be a product my labor. But he, no doubt, will find someone who realizes his wishes, and, God forbid, everyone will be happy in this situation. nine0003
If the patient's aesthetic perception is not developed, or these are some externally introduced superficial judgments, he has needs even for grotesque changes in appearance, again, if he turns to me, I will refuse him intervention, because I do not want such a result to be a product my labor. But he, no doubt, will find someone who realizes his wishes, and, God forbid, everyone will be happy in this situation. nine0003
In my perception, a high-quality aesthetic operation is one that has obvious aesthetic improvements, but it is not visible, the face does not seem to be operated on.
Y. Titova:
In fact, this idea has now been confirmed that every doctor has his own style of plastic surgeon. And when communicating with young girls who are interested in plastic surgery, looking at the photo, they can say: this is the hand of Dr. Ivanov, this is the hand of Dr. Petrov. I don’t see much difference, I just see it’s done here, the girl is not done here, or it’s imperceptible. nine0003
nine0003
A. Zakharov:
I don't quite agree with you, because when everything is done really cool, no one will say that this is someone's hand. If everything is on the level, there is no feeling that someone has done something here, someone has worked. Everything is just beautiful, everything is aesthetically pleasing, thanks to mom and dad for this.
E. Kryukova:
But from our conversation I have a feeling that plastic surgery is about feelings. You talked about 5-10 consultations that patients usually go through. What do we need to achieve in finding our surgeon? What do you recommend focusing on? nine0003
A. Zakharov:
First, without a doubt, this is a common vision of the result, a common perception of what we want to get as a result. Secondly, this is a sense of security, that is, an absolutely clear understanding by both the doctor and the patient of all these processes, all the risks and work with these risks. Because you can see everything correctly, but besides what you see, you need to implement it. Implementation is technologically correct and safe for the patient, because there are a lot of criteria: there must be a normal clinic, fully equipped, it must be in compliance with all standards, because this is surgery, this is not a pure art that exists in medicine, in medical activity. Compliance with all, without a doubt, safety standards in relation to anesthesia, because not everything depends on the surgeon. There are other services that are responsible for the life of the patient. And, probably, the combination of a general vision of aesthetics with understandable security guarantees is the right alloy that allows you to choose your specialist. nine0003
Because you can see everything correctly, but besides what you see, you need to implement it. Implementation is technologically correct and safe for the patient, because there are a lot of criteria: there must be a normal clinic, fully equipped, it must be in compliance with all standards, because this is surgery, this is not a pure art that exists in medicine, in medical activity. Compliance with all, without a doubt, safety standards in relation to anesthesia, because not everything depends on the surgeon. There are other services that are responsible for the life of the patient. And, probably, the combination of a general vision of aesthetics with understandable security guarantees is the right alloy that allows you to choose your specialist. nine0003
Combining a shared vision of aesthetics with clear safety guarantees is the right mix to choose your specialist.
E. Kryukova:
How do you predict the result? Just communicating with text, maybe you draw something, do diagnostics with photographs?
A. Zakharov:
Zakharov:
I prefer dialogue and drawing. It is these living methods that allow you to better feel the person, the patient to understand the vision of the doctor. I am not a supporter of all sorts of computer simulations and diagnostics. It seems to me that this is some kind of manipulation of consciousness, because not a single computer simulation that exists today takes into account the real biomechanics of tissues, skin extensibility, displacement of anatomical structures, but this applies to any part of the body. That is, this is just a variant of a graphic editor that allows you to see a picture in two or three dimensions, but what does this have to do with real practice. nine0003
E. Kryukova:
It seems to me that it would be useful for the patient to see himself with a new element. Here we said at the beginning of the dialogue that after the operation something is wrong, the patient may not like it during rehabilitation. And here, when modeling, something new has already been screwed in, he appreciated - like it, don't like it, maybe it's time for me to leave.
Y. Titova:
It will be worse if he likes the simulation, but it will disagree with the result.
A. Zakharov:
You just read my thoughts in this situation. Drawing something is not enough, you need to have the technological ability to implement it in the operating room exactly as it was drawn. This just relies on the real possibilities of tissues, and this is not always possible. Therefore, often, such a perfectionistic approach to predicting the result due to the model generates an unrealizable expectation. That is, the patient wants to get exactly what he saw in the simulation, and this is technologically impossible, not at all. nine0003
Y. Titova:
But at least you can understand whether you are ready to part with your nose or not.
A. Zakharov:
And in the aggregate it turns out that there is a dissonance between excessive expectations due to modeling and a certain reality.
E. Kryukova:
Do men also turn to plastic surgeons? Still, men are more rational in this regard, or, on the contrary, are they more impulsive?
A. Zakharov:
No, on the contrary. The male contingent is the most difficult to work with, aesthetic operations for men are technologically more complicated than for women, they are much more complex in terms of composition. Almost all aesthetic manipulations from our practice are aimed at improving the aesthetics of a woman's face with elements of feminization. According to the technical process, they lead to a certain feminization. And to modify such an operation in relation to a male face in order to obtain either the absence of changes in terms of masculinization or feminization, or to obtain, on the contrary, the opposite change. This is a special approach, more individual planning, many technological additional complexities. nine0003
Secondly, men are much more demanding than women, this is a problem, because they cannot disguise themselves with cosmetics, they cannot divert attention from the rehabilitation areas with hair. And in this regard, the exactingness for implementation, for manipulation is much higher. In general, the male contingent who seeks the help of an aesthetic surgeon is psychologically more complex. The path of a man to an aesthetic surgeon is much more tortuous and difficult in terms of making this decision. And, of course, each patient, a man, in our practice they are 5-7 percent of the total number of visitors, this is a separate case that requires even more attention than a female patient. nine0003
And in this regard, the exactingness for implementation, for manipulation is much higher. In general, the male contingent who seeks the help of an aesthetic surgeon is psychologically more complex. The path of a man to an aesthetic surgeon is much more tortuous and difficult in terms of making this decision. And, of course, each patient, a man, in our practice they are 5-7 percent of the total number of visitors, this is a separate case that requires even more attention than a female patient. nine0003
The male contingent is the most difficult to work with, aesthetic surgeries for men are technologically more complicated than for women. Almost all aesthetic manipulations from our practice are aimed at improving the aesthetics of a woman's face with elements of feminization.
E. Kryukova:
What brings a man to a plastic surgeon?
A. Zakharov:
There are absolutely objective testimonies. For example, traumatic deformities of the nose after injuries of a sports or domestic nature, everything happens. There is a desire to look younger, or not so much younger as fresher, more familiar to oneself, let's say, in earlier years. Often these are public people, for whom the appearance and aesthetics of their own face is fundamentally important due to the presence of public speaking, an active social life. Therefore, very different paths, but they are similar to those that lead women to us. nine0003
For example, traumatic deformities of the nose after injuries of a sports or domestic nature, everything happens. There is a desire to look younger, or not so much younger as fresher, more familiar to oneself, let's say, in earlier years. Often these are public people, for whom the appearance and aesthetics of their own face is fundamentally important due to the presence of public speaking, an active social life. Therefore, very different paths, but they are similar to those that lead women to us. nine0003
Y. Titova:
Interesting. Do men want to become more brutal in the face?
A. Zakharov:
There are some.
Yu. Titova:
What interesting things can a doctor offer in this respect?
A. Zakharov:
Often the operation is precisely masculinizing, making the face more masculine, this is a hobby, chin structuring for patients with deficient height of the lower third of the face, deficient projection of the lower jaw in the frontal plane. This is an option, given that they certainly have pre-orthodontic treatment, and they have a normal bite, and they have already done everything that the dentist needs in order to get the right composition, as a refinement in this direction, this can be an increase in the projection of the chin, a change in its shape. nine0003
This is an option, given that they certainly have pre-orthodontic treatment, and they have a normal bite, and they have already done everything that the dentist needs in order to get the right composition, as a refinement in this direction, this can be an increase in the projection of the chin, a change in its shape. nine0003
Y. Titova:
Unfortunately, our broadcast has come to an end. Dear friends, I still allow myself the following phrase, which I read on the Internet today in relation to our broadcast: measure seven times, cut once.
A. Zakharov:
Absolutely correct.
Y. Titova:
Therefore, you need to be as objective as possible in this respect and not make hasty conclusions about your appearance. And, for sure, you do not need to listen to third parties who impose something. nine0003
A. Zakharov:
Without a doubt.
Y. Titova:
Dear friends, Anton Zakharov, a plastic surgeon, was on the air today. Thank you very much, very interesting, I hope we have conveyed the correct information to many, which will be applied. Ekaterina Kryukova, I, Yulia Titova, this is the program "Plastic Surgery with Dr. Zakharov". Be healthy, all the best.
Thank you very much, very interesting, I hope we have conveyed the correct information to many, which will be applied. Ekaterina Kryukova, I, Yulia Titova, this is the program "Plastic Surgery with Dr. Zakharov". Be healthy, all the best.
A. Zakharov:
Thank you. nine0003
what you need to know about a comprehensive examination for women
For many people, the starting point for making a decision about plastic surgery is psychological aspects, including uncertainty, the desire to radically change oneself, become like an idol, and so on. Every year, innovations appear in the field of beauty that cannot leave you indifferent, and for many they become the only option to improve the quality of life. But is this really so and is plastic surgery capable of solving psychological problems, we will consider further. nine0003
It is worth noting that not only women, but also men tend to remove certain imperfections by surgery. But changes are not always based on the desire to prolong youth and remove cosmetic defects. Complexes about appearance are largely to blame.
Complexes about appearance are largely to blame.
.
Defects in appearance and psychological complexes
Very often the desire to improve appearance is directly related to self-doubt. It happens that behind the urgent need to have an operation there are needs for love, recognition, attention. nine0003
If a person often thinks about plastic surgery, he should analyze a few points and honestly answer the questions:
- What is the operation for, what problems will it help solve?
- Are there feelings of dissatisfaction? It is important to understand that changing appearance does not always mean solving psychological problems. For example, new lips or a facelift will not fix loneliness, lack of communication with friends, and will not help cope with depression. nine0483
- Do you really want to sign up for an operation, or is this desire dictated by a loved one, acquaintances and other people who influence you.
Complexes of appearance often lead a person to the idea of undergoing plastic surgery. This helps to increase the perception of one's own "I".
This helps to increase the perception of one's own "I".
Cases in which plastic surgery is applicable
A person's physical condition is not the only criterion for a candidate's eligibility for plastic surgery. Experienced surgeons can still consider concerned clients during the consultation. Many of them prescribe recommendations for psychological rehabilitation. nine0003
However, there is a group of patients for whom plastic surgery is indicated:
- A person needs plastic surgery if there is skin ptosis, a change in skin relief, new features appear that were not there before (bags under the eyes, “bulldog cheeks”).
- Reconstructive plastic surgery is necessary in case of injuries, accidents.
- Breast augmentation is required for asymmetries, too large breasts, resulting in problems with posture.
- Plastic surgery of the lips, nose to eliminate visible defects due to age-related changes and after injuries.
 nine0483
nine0483 - A tummy tuck will help women who have given birth to feel more attractive and more confident if they have not returned to shape with the help of physical activity.
- Intimate plastic surgery is indicated for women after childbirth, in case of discomfort during intimacy.
The first changes on the face are noticeable after 25 years, so cosmetic and surgical interventions are not performed on patients under 18 years of age. Except for the correction of congenital defects (including the plastic of the auricles). Everything is individual - a plastic surgeon will help to decide on the need for the procedure. nine0003
Contraindications to plastic surgery treatment
There are not only physical contraindications associated with infectious, chronic and other diseases, but also psychological ones. Let's consider them in more detail.
A small percentage of disharmony in appearance
Not every person who turns to a surgeon should undergo surgery. Patients can be conditionally divided into 2 categories:
Patients can be conditionally divided into 2 categories:
Representatives of the first group are characterized by high self-esteem. For them, the aesthetic component of appearance is above all. In such patients, there is a need to improve themselves in something. Thanks to the emotional mood and the conviction that the intervention is necessary, the postoperative period is easy. This contributes to the formation of a positive image in their own eyes. nine0003
The second group of people has physical defects and cosmetic defects that have contributed to a decrease in self-esteem for a long time.
Rehabilitation in such patients is slower, since it takes more time to restore confidence in oneself and one's own "I".
Obsessive states of the patient regarding appearance
It is important to objectively assess the need for surgery. If there are physical defects that can be removed with the help of surgery, it is worth going to plastic surgery abroad. The main thing is to choose the right clinic, taking into account the rating of the medical facility and patient reviews. nine0003
The main thing is to choose the right clinic, taking into account the rating of the medical facility and patient reviews. nine0003
For example, if a woman decides to have mammoplasty after breastfeeding, her desire is quite justified and understandable. After all, at any age you can remain attractive and confident. Another thing is when a young girl with a small but firm and neat bust decides to put implants. Most likely, she has complexes because of her appearance due to various reasons. Perhaps the ex-boyfriend said this shortcoming, or the problem goes deep into adolescence, when buxom classmates accepted compliments from guys, and thin, slender girls remained in the shadows. Everything has long been forgotten and experienced, but the mind set aside that small breasts look ugly. nine0003
Before you sign up for an operation to change your appearance, you need to deal with psychological problems: learn how to overcome appearance complexes and learn to love yourself.
Excessive fixation on ideal forms
Idealization of appearance can become an invisible enemy, pushing you to decide on plastic surgery without medical indications. A person involuntarily compares himself with other people, looking for his weaknesses. All this leads to the formation of complexes. The patient turns to a plastic surgeon to make his appearance ideal, corresponding to someone's (or his) expectations. But even after the intervention, your own appearance will not seem perfect, because there is no limit to perfection. This is fraught with constant changes, the so-called experiments on oneself. nine0003
A person involuntarily compares himself with other people, looking for his weaknesses. All this leads to the formation of complexes. The patient turns to a plastic surgeon to make his appearance ideal, corresponding to someone's (or his) expectations. But even after the intervention, your own appearance will not seem perfect, because there is no limit to perfection. This is fraught with constant changes, the so-called experiments on oneself. nine0003
Plastic surgery in Istanbul will solve aesthetic problems of any complexity, but only after the harmonization of psychological health.
Exaggerated expectations from surgery
Many patients find it easy to decide on plastic surgery because they have high expectations from surgery. It seems to them that after a facelift, the face will be completely renewed and young, despite their age. The desire to get eyes or lips like a celebrity is actually associated with the desire for publicity. nine0003
It is important to assess the situation objectively. Indeed, after the intervention of the patient, edema, sutures, a rehabilitation period are expected, and only after a little time you can evaluate the result, for which you also need to be prepared.
Indeed, after the intervention of the patient, edema, sutures, a rehabilitation period are expected, and only after a little time you can evaluate the result, for which you also need to be prepared.
Exclusively psychological problems in a person's life
During the period of temporary life difficulties, one should not decide on an operation. For each they are their own. However, you should not make an appointment with a plastic surgeon, being in a state of crisis due to the death of a loved one, divorce and other life metamorphoses. nine0003
Real goals for the operation - the key to success in eliminating psychological complexes
During the consultation, the plastic surgeon listens to the wishes and doubts of the client regarding the operation, and also finds out the true vision of one's own appearance. The key to success is honesty with yourself and the attending physician, determining the real goals of the procedure. You should speak as clearly and frankly as possible about your feelings and feelings.
You should speak as clearly and frankly as possible about your feelings and feelings.
It is unreasonable for the patient to exaggerate when talking about problem parts of the body if the operation is only aesthetic. Misleading the doctor can lead to negative consequences after the procedure. nine0003
Comprehensive examination of women
The importance of objective self-assessment Objective self-assessment is very important in making a decision about surgery. A simple example: a girl does not like her lips, she considers them too thin or asymmetrical and lives with this thought. Over time, this state of affairs leads to the appearance of complexes due to the appearance of and it seems that there is only one way out - to increase the lips. But the desire to improve oneself does not always end with one procedure. A person has a desire to further improve and change himself. It is important to fall into the hands of a qualified surgeon, but the most important thing is to learn to objectively evaluate yourself.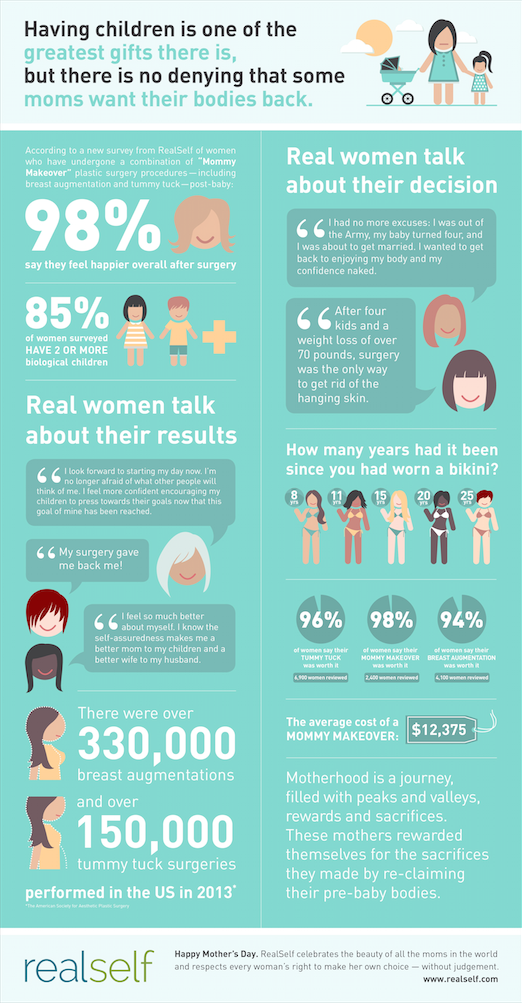 nine0003
nine0003
Responsibility to yourself and others
Plastic surgery changes the external and internal world. An operation done for the sake of someone can lead to great disappointment. Others are able to respond well to positive changes, but are unlikely to be able to accept the negative consequences of the operation.
The results of surgical correction may be subject to criticism from others, which must be skillfully screened out. For many, the instruction helps: “I did it for myself and I like everything!”. You need to mentally prepare for the fact that even in a new look you will not be liked by everyone. But since all people are different, with their own opinions and worldviews, this is normal. nine0003
During their activity, Turkish surgeons have become partly psychologists. In the process of consultation, in addition to assessing the anamnesis, they determine the moral state of a person, his psychological readiness for surgical intervention.