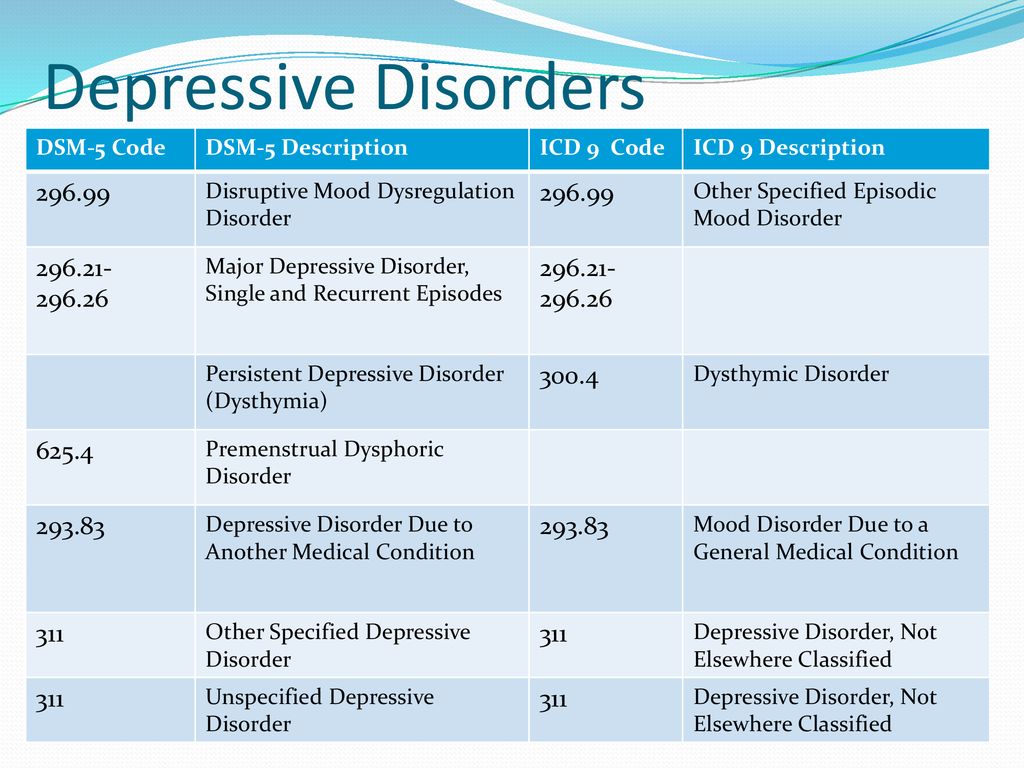
Diagnostic code for major depressive disorder
Major depressive disorder, recurrent severe without psychotic features
F32.4 Major depressive disorder, single episode, in partial remission
F32.5 Major depressive disorder, single episode, in full remission
F32.8 Other depressive episodes
F32.81 Premenstrual dysphoric disorder
F32. 89 Other specified depressive episodes
F32.9 Major depressive disorder, single episode, unspecified
F32.A Depression, unspecified
F33 Major depressive disorder, recurrent
F33.0 Major depressive disorder, recurrent, mild
F33.1 Major depressive disorder, recurrent, moderate
F33. 2
Major depressive disorder, recurrent severe without psychotic features
2
Major depressive disorder, recurrent severe without psychotic features
F33.3 Major depressive disorder, recurrent, severe with psychotic symptoms
F33.4 Major depressive disorder, recurrent, in remission
F33.40 …… unspecified
F33.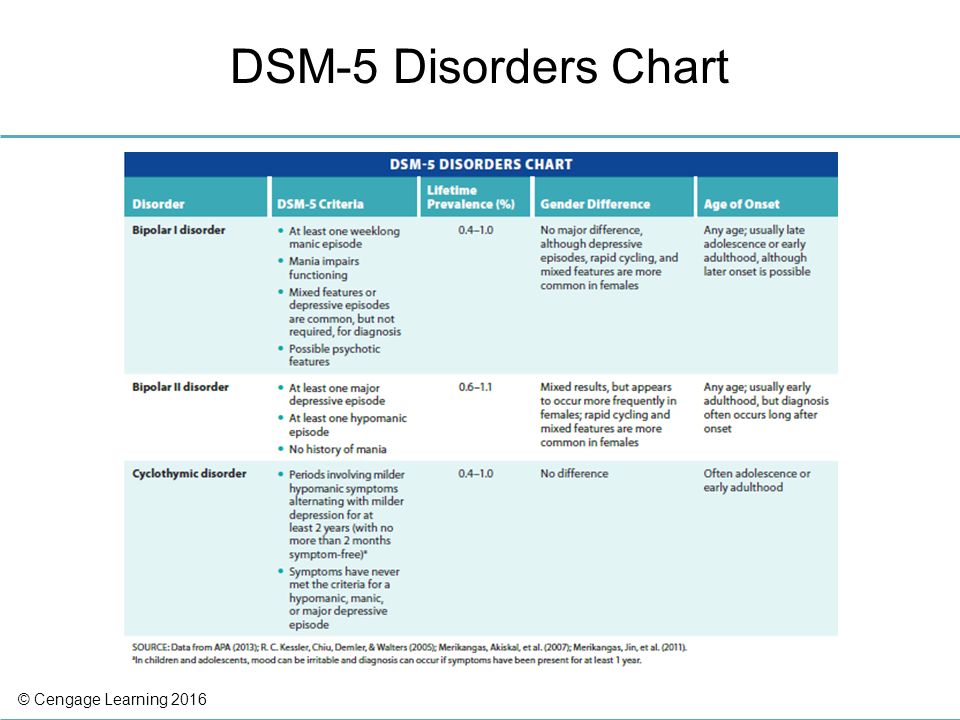 41 Major depressive disorder, recurrent, in partial remission
41 Major depressive disorder, recurrent, in partial remission
F33.42 Major depressive disorder, recurrent, in full remission
F33.8 Other recurrent depressive disorders
F33.9 Major depressive disorder, recurrent, unspecified
F34 Persistent mood [affective] disorders
F34. 0 Cyclothymic disorder
0 Cyclothymic disorder
F34.1 Dysthymic disorder
Reimbursement claims with a date of service on or after October 1, 2015 require the use of ICD-10-CM codes.
Major depressive disorder, recurrent, unspecified
- ICD-10-CM Codes ›
- F01-F99 ›
- F30-F39 ›
- F33- ›
- 2023 ICD-10-CM Diagnosis Code F33.9
Major depressive disorder, recurrent, unspecified
- 2016 2017 2018 2019 2020 2021 2022 2023 Billable/Specific Code
- F33.9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
- The 2023 edition of ICD-10-CM F33.9 became effective on October 1, 2022.
- This is the American ICD-10-CM version of F33.9 - other international versions of ICD-10 F33.9 may differ.
Applicable To
- Monopolar depression NOS
The following code(s) above F33.9 contain annotation back-references
Annotation Back-References
In this context, annotation back-references refer to codes that contain:
- Applicable To annotations, or
- Code Also annotations, or
- Code First annotations, or
- Excludes1 annotations, or
- Excludes2 annotations, or
- Includes annotations, or
- Note annotations, or
- Use Additional annotations
that may be applicable to F33.9:
- F01-F99
2023 ICD-10-CM Range F01-F99
Mental, Behavioral and Neurodevelopmental disorders
Includes
- disorders of psychological development
Type 2 Excludes
- symptoms, signs and abnormal clinical laboratory findings, not elsewhere classified (R00-R99)
- F33
ICD-10-CM Diagnosis Code F33
Major depressive disorder, recurrent
- 2016 2017 2018 2019 2020 2021 2022 2023 Non-Billable/Non-Specific Code
Includes
- recurrent episodes of depressive reaction
- recurrent episodes of endogenous depression
- recurrent episodes of major depression
- recurrent episodes of psychogenic depression
- recurrent episodes of reactive depression
- recurrent episodes of seasonal affective disorder
- recurrent episodes of seasonal depressive disorder
- recurrent episodes of vital depression
Type 1 Excludes
- bipolar disorder (F31.
 -)
-) - manic episode (F30.-)
Approximate Synonyms
- Depression, major, recurrent
- Major depression, recurrent
- Major depressive disorder, recurrent episode
- Major depressive disorder, seasonal
- Recurrent major depression
- Severe recurrent seasonal major depression
Clinical Information
- A disorder characterized by melancholic feelings of grief or unhappiness.
- A melancholy feeling of sadness and despair.
- A mental condition marked by ongoing feelings of sadness, despair, loss of energy, and difficulty dealing with normal daily life. Other symptoms of depression include feelings of worthlessness and hopelessness, loss of pleasure in activities, changes in eating or sleeping habits, and thoughts of death or suicide.
 Depression can affect anyone, and can be successfully treated. Depression affects 15-25% of cancer patients.
Depression can affect anyone, and can be successfully treated. Depression affects 15-25% of cancer patients. - Depression is a serious medical illness that involves the brain. It's more than just a feeling of being "down in the dumps" or "blue" for a few days. If you are one of the more than 20 million people in the United States who have depression, the feelings do not go away. They persist and interfere with your everyday life. Symptoms can include
- sadness
- loss of interest or pleasure in activities you used to enjoy
- change in weight
- difficulty sleeping or oversleeping
- energy loss
- feelings of worthlessness
- thoughts of death or suicide
 Some people get seasonal affective disorder in the winter. Depression is one part of bipolar disorder.there are effective treatments for depression, including antidepressants and talk therapy. Most people do best by using both.
Some people get seasonal affective disorder in the winter. Depression is one part of bipolar disorder.there are effective treatments for depression, including antidepressants and talk therapy. Most people do best by using both. - Depressive states usually of moderate intensity in contrast with major depression present in neurotic and psychotic disorders.
- Mild depression that is not considered clinical depression. For clinical depression, use major depression.
- Unpleasant, but not necessarily irrational or pathological, mood state characterized by sadness, despair, or discouragement; "the blues"; may also involve low self-esteem, social withdrawal, and somatic symptoms such as eating and sleep disturbance.
ICD-10-CM F33.9 is grouped within Diagnostic Related Group(s) (MS-DRG v40.0):
- 885 Psychoses
Convert F33. 9 to ICD-9-CM
9 to ICD-9-CM
Code History
- 2016 (effective 10/1/2015): New code (first year of non-draft ICD-10-CM)
- 2017 (effective 10/1/2016): No change
- 2018 (effective 10/1/2017): No change
- 2019 (effective 10/1/2018): No change
- 2020 (effective 10/1/2019): No change
- 2021 (effective 10/1/2020): No change
- 2022 (effective 10/1/2021): No change
- 2023 (effective 10/1/2022): No change
Diagnosis Index entries containing back-references to F33.9:
- Depression (acute) (mental) F32.A
ICD-10-CM Diagnosis Code F32.A
Depression, unspecified
- 2022 - New Code 2023 Billable/Specific Code
Applicable To
- Depression NOS
- Depressive disorder NOS
- monopolar F33.
 9
9
- Disorder (of) - see also Disease
- depressive F32.A
ICD-10-CM Diagnosis Code F32.A
Depression, unspecified
- 2022 - New Code 2023 Billable/Specific Code
Applicable To
- Depression NOS
- Depressive disorder NOS
- major F32.9
ICD-10-CM Diagnosis Code F32.9
Major depressive disorder, single episode, unspecified
- 2016 2017 2018 2019 2020 2021 2022 2023 Billable/Specific Code
Applicable To
- Major depression NOS
- recurrent F33.9
- recurrent F33.9
- depressive F32.A
- Episode
- Involution, involutional - see also condition
- Melancholia F32.A
ICD-10-CM Diagnosis Code F32.A
Depression, unspecified
- 2022 - New Code 2023 Billable/Specific Code
Applicable To
- Depression NOS
- Depressive disorder NOS
- recurrent F33.
 9
9
- Menopause, menopausal (asymptomatic) (state) Z78.0
ICD-10-CM Diagnosis Code Z78.0
Asymptomatic menopausal state
- 2016 2017 2018 2019 2020 2021 2022 2023 Billable/Specific Code Adult Dx (15-124 years) Female Dx POA Exempt
Applicable To
- Menopausal state NOS
- Postmenopausal status NOS
Type 2 Excludes
- symptomatic menopausal state (N95.1)
- depression (single episode) F32.89
ICD-10-CM Diagnosis Code F32.89
Other specified depressive episodes
- 2017 - New Code 2018 2019 2020 2021 2022 2023 Billable/Specific Code
Applicable To
- Atypical depression
- Post-schizophrenic depression
- Single episode of 'masked' depression NOS
- agitated (single episode) F32.2
ICD-10-CM Diagnosis Code F32.2
Major depressive disorder, single episode, severe without psychotic features
- 2016 2017 2018 2019 2020 2021 2022 2023 Billable/Specific Code
- recurrent episode F33.
 9
9
- recurrent episode F33.
- psychotic (single episode) F32.89
ICD-10-CM Diagnosis Code F32.89
Other specified depressive episodes
- 2017 - New Code 2018 2019 2020 2021 2022 2023 Billable/Specific Code
Applicable To
- Atypical depression
- Post-schizophrenic depression
- Single episode of 'masked' depression NOS
- recurrent episode F33.9
- Reaction - see also Disorder
- depressive (single episode) F32.9
ICD-10-CM Diagnosis Code F32.9
Major depressive disorder, single episode, unspecified
- 2016 2017 2018 2019 2020 2021 2022 2023 Billable/Specific Code
Applicable To
- Major depression NOS
- affective (single episode) F31.4
ICD-10-CM Diagnosis Code F31.4
Bipolar disorder, current episode depressed, severe, without psychotic features
- 2016 2017 2018 2019 2020 2021 2022 2023 Billable/Specific Code
- recurrent episode F33.
 9
9
- recurrent episode F33.
- depressive (single episode) F32.9
ICD-10-CM Codes Adjacent To F33.9
F33 Major depressive disorder, recurrent
F33.0 Major depressive disorder, recurrent, mild
F33.1 Major depressive disorder, recurrent, moderate
F33.2 Major depressive disorder, recurrent severe without psychotic features
F33. 3 Major depressive disorder, recurrent, severe with psychotic symptoms
3 Major depressive disorder, recurrent, severe with psychotic symptoms
F33.4 Major depressive disorder, recurrent, in remission
F33.40 …… unspecified
F33.41 Major depressive disorder, recurrent, in partial remission
F33.42 Major depressive disorder, recurrent, in full remission
F33. 8 Other recurrent depressive disorders
8 Other recurrent depressive disorders
F33.9 Major depressive disorder, recurrent, unspecified
F34 Persistent mood [affective] disorders
F34.0 Cyclothymic disorder
F34.1 Dysthymic disorder
F34. 8 Other persistent mood [affective] disorders
8 Other persistent mood [affective] disorders
F34.81 Disruptive mood dysregulation disorder
F34.89 Other specified persistent mood disorders
F34.9 Persistent mood [affective] disorder, unspecified
F39 Unspecified mood [affective] disorder
F40 Phobic anxiety disorders
F40. 0 Agoraphobia
0 Agoraphobia
Reimbursement claims with a date of service on or after October 1, 2015 require the use of ICD-10-CM codes.
Validation of a screening test based on DSM-5 criteria by digital phenotyping in the Russian population
Validation of a screening test based on DSM-5 criteria by digital phenotyping in the Russian population Website of the publishing house "Media Sfera"
contains materials intended exclusively for healthcare professionals. By closing this message, you confirm that you are a registered medical professional or student of a medical educational institution. nine0006
Kasyanov E.D.
National Medical Research Center for Psychiatry and Neurology named after N.N. V.M. Bekhterev” of the Ministry of Health of the Russian Federation
Verbitskaya E.V.
First Saint-Petersburg State Medical University. acad. I.P. Pavlova
Rakitko A.S.
Genotek LLC
Ilyinsky V. V.
V.
Genotek LLC
Rukavishnikov G.V.
National Medical Research Center for Psychiatry and Neurology named after N.N. V.M. Bekhterev” of the Ministry of Health of the Russian Federation
Neznanov N.G.
National Medical Research Center for Psychiatry and Neurology. V.M. Bekhtereva
Kibitov A.O.
National Medical Research Center for Psychiatry and Neurology named after N.N. V.M. Bekhterev” of the Ministry of Health of the Russian Federation;
National Medical Research Center for Psychiatry and Narcology named after N.N. V.P. Serbian Ministry of Health of the Russian Federation
Mazo G.E.
National Medical Research Center for Psychiatry and Neurology named after N.N. V.M. Bekhterev"
Validation of a screening test based on DSM-5 criteria by digital phenotyping on the Russian population G.V., Neznanov N.G., Kibitov A.O., Mazo G.E.
More about the authors
Magazine: Journal of Neurology and Psychiatry. S.S. Korsakov. Special issues. 2022;122(6‑2): 64‑70 nine0006
S.S. Korsakov. Special issues. 2022;122(6‑2): 64‑70 nine0006
DOI: 10.17116/jnevro202212206264
How to quote:
Kasyanov E.D., Verbitskaya E.V., Rakitko A.S., Ilyinsky V.V., Rukavishnikov G.V., Neznanov N.G., Kibitov A.O., Mazo G.E. Validation of a screening test based on DSM-5 criteria by digital phenotyping on the Russian population. nine0055 Journal of Neurology and Psychiatry. S.S. Korsakov. Special issues. 2022;122(6‑2):64‑70.
Kasyanov ED, Verbitskaya EV, Rakitko AS, Ilinsky VV, Rukavishnikov GV, Neznanov NG, Kibitov AO, Mazo GE. Validation of a DSM-5-based screening test using digital phenotyping in the Russian population. Zhurnal Nevrologii i Psikhiatrii imeni S.S. Korsakova. 2022;122(6‑2):64‑70. (In Russ.).
https://doi.org/10.17116/jnevro202212206264 nine0006
Close metadata
PURPOSE OF THE STUDY
To assess the ability of the depression and anxiety screening test, based on DSM-5 diagnostic criteria, to detect cases of these conditions, assessed using the validated Hospital Anxiety and Depression Scale (HADS), in a population sample through digital phenotyping.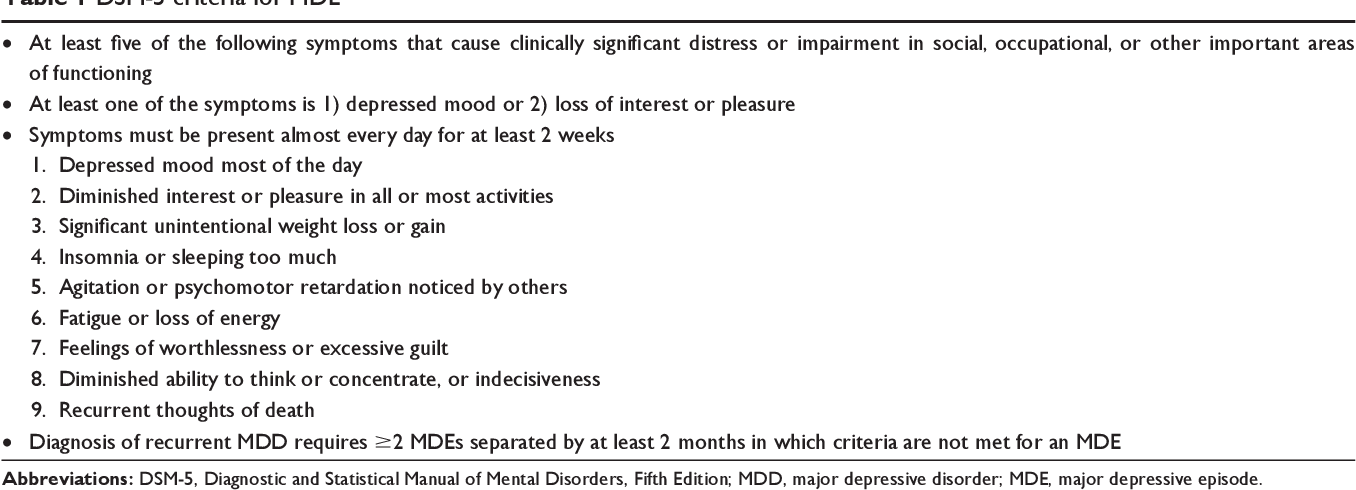
MATERIAL AND METHODS
This cross-validation study included 5116 respondents (mean age 36.9(9.8) years), of which 49.4% (2526) were women. The study screening test for depression and anxiety was created based on the DSM-5 diagnostic criteria for major depressive disorder and generalized anxiety disorder electronically. The validated HADS scale was used as a standard test. Categories of depression (HADS-D) and anxiety (HADS-A) phenotypes were formed with a cut-off of ≥8 and ≥11 points. The main indicators of the validity of the study test were calculated, including accuracy (Ac), sensitivity (Sn) and specificity (Sp) with 9 of them5% confidence intervals (CI).
RESULTS
The frequency of current depression and anxiety on the screening test was 7.8% ( n = 400) and 12.5% ( n = 639), respectively, the frequency of depression during the lifetime was 25.9% ( n =1327). On the HADS-D depression subscale for cutoffs of ≥11 and ≥8 points, the frequency of depression was 3. 4% ( n =174) and 15% ( n =766), respectively, for the HADS-A anxiety subscale for cutoffs in ≥11 and ≥8 points, the frequency of anxiety was 8.9% ( n =456) and 31.8% ( n =1628), respectively. At a cut-off of ≥11 points for HADS-D and HADS-A, current depression scores were Ac=92%, Sn=47% (95% CI [39-54]), Sp=94% (95% CI [93-94]) ), lifetime depression — Ac=75%, Sn=63% (95% CI [56-70]), Sp=75% (95% CI [74-77]) and current anxiety — Ac=88%, Sn=54% (95% CI [50–59]) and Sp=92% (95% CI [90–92]). At a cut-off of ≥8 points for HADS-D and HADS-A, current depression rates were Ac=86%, Sn=30% (95% CI [27–33]), Sp=96% (95% CI5% [95-97]), lifetime depression - Ac=74%, Sn=51% (95% CI [48-55]), Sp=79% (95% CI [77-80]) and current anxiety — Ac=75%, Sn=31% (95% CI [29-33]), Sp=96% (95% CI [95-97]).
4% ( n =174) and 15% ( n =766), respectively, for the HADS-A anxiety subscale for cutoffs in ≥11 and ≥8 points, the frequency of anxiety was 8.9% ( n =456) and 31.8% ( n =1628), respectively. At a cut-off of ≥11 points for HADS-D and HADS-A, current depression scores were Ac=92%, Sn=47% (95% CI [39-54]), Sp=94% (95% CI [93-94]) ), lifetime depression — Ac=75%, Sn=63% (95% CI [56-70]), Sp=75% (95% CI [74-77]) and current anxiety — Ac=88%, Sn=54% (95% CI [50–59]) and Sp=92% (95% CI [90–92]). At a cut-off of ≥8 points for HADS-D and HADS-A, current depression rates were Ac=86%, Sn=30% (95% CI [27–33]), Sp=96% (95% CI5% [95-97]), lifetime depression - Ac=74%, Sn=51% (95% CI [48-55]), Sp=79% (95% CI [77-80]) and current anxiety — Ac=75%, Sn=31% (95% CI [29-33]), Sp=96% (95% CI [95-97]).
CONCLUSION
The high accuracy and specificity of the study test allow it to be used for screening purposes to detect (but not exclude) cases of depression and anxiety in the population. However, further research is needed to validate the study test using a diagnostic interview with a physician. nine0006
However, further research is needed to validate the study test using a diagnostic interview with a physician. nine0006
Keywords:
digital phenotyping
depression
anxiety
screening
HADS
DSM
Authors:
Kasyanov E.D.
National Medical Research Center for Psychiatry and Neurology named after N.N. V.M. Bekhterev” of the Ministry of Health of the Russian Federation
Verbitskaya E.V.
First Saint-Petersburg State Medical University. acad. I.P. Pavlova
Rakitko A.S.
Genotek LLC
Ilyinsky V.V.
Genotek LLC
Rukavishnikov G.V.
National Medical Research Center for Psychiatry and Neurology named after N.N. V.M. Bekhterev” of the Ministry of Health of the Russian Federation
Neznanov N.G.
National Medical Research Center for Psychiatry and Neurology. V.M. Bekhterev
- SPIN RSCI: 9772-0024
- Scopus AuthorID: 35593613200
- ORCID: 0000-0001-5618-4206
Kibitov A.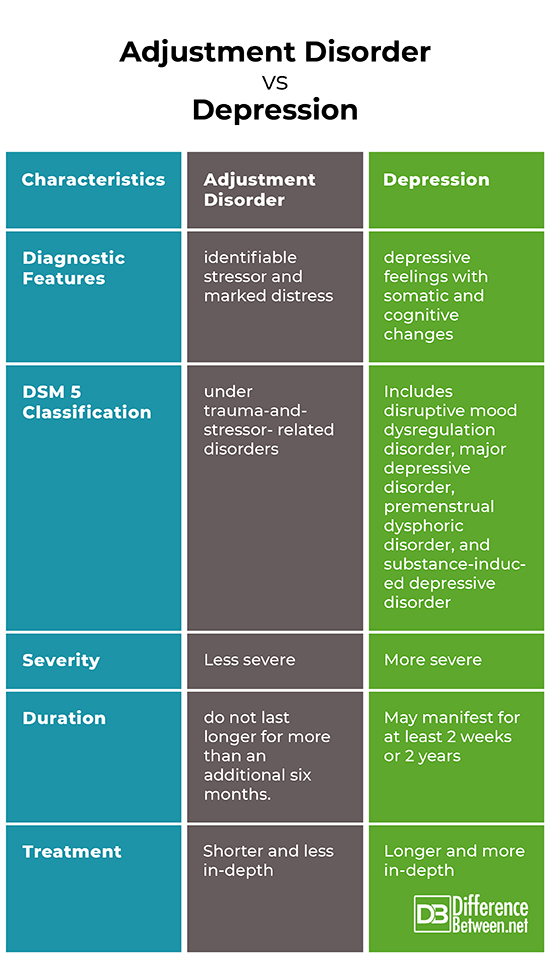 O.
O.
National Medical Research Center for Psychiatry and Neurology named after N.N. V.M. Bekhterev” of the Ministry of Health of the Russian Federation;
National Medical Research Center for Psychiatry and Narcology named after N.N. V.P. Serbian Ministry of Health of the Russian Federation
Mazo G.E.
National Medical Research Center for Psychiatry and Neurology named after N.N. V.M. Bekhterev"
References:
- Weissman MM. Big Data Begin in Psychiatry. JAMA Psychiatry. 2020;77(9):967-973. PMID: 32401285. https://doi.org/10.1001/jamapsychiatry.2020.0954
- Howard DM, Adams MJ, Shirali M, Clarke TK, Marioni RE, et al. Genome-wide association study of depression phenotypes in UK Biobank identifies variants in excitatory synaptic pathways. NatCommun. 2018;9:1:1-10. https://doi.org/10.1038/s41467-018-03819-3
- Cai N, Revez JA, Adams MJ, et al. MDD Working Group of the Psychiatric Genomics Consortium, Kendler K.S., Flint J. Minimal phenotyping yields genome-wide association signals of low specificity for major depression.
 Nat Genet. 2020;52:4:437-447. https://doi.org/10.1038/s41588-020-0594-5
Nat Genet. 2020;52:4:437-447. https://doi.org/10.1038/s41588-020-0594-5 - Insel TR. Digital phenotyping: a global tool for psychiatry. World Psychiatry. 2018;17(3):276-277. PMID: 30192103; PMCID: PMC6127813. https://doi.org/10.1002/wps.20550
- Lydon-Staley DM, Barnett I, Satterthwaite TD, et al. Digital phenotyping for psychiatry: Accommodating data and theory with network science methodologies. Curr Opin Biomed Eng. 2019;9:8-13. Epub 2018 Dec 14. PMID: 31650093; PMCID: PMC6812649. https://doi.org/10.1016/j.cobme.2018.12.003
- Sequeira L, Battaglia M, Perrotta S, et al. Digital Phenotyping With Mobile and Wearable Devices: Advanced Symptom Measurement in Child and Adolescent Depression. J Am Acad Child Adolesc Psychiatry. 2019;58(9):841-845. Erratum in: J Am Acad Child Adolesc Psychiatry. 2020;59(12):1408. PMID: 31445619. https://doi.org/10.1016/j.jaac.2019.04.011
- Melcher J, Hays R, Torous J. Digital phenotyping for mental health of college students: a clinical review.
 Evidence Based Mental Health. 2020;23(4):161-166. Epub 2020 Sep 30. PMID: 32998937. https://doi.org/10.1136/ebmental-2020-300180
Evidence Based Mental Health. 2020;23(4):161-166. Epub 2020 Sep 30. PMID: 32998937. https://doi.org/10.1136/ebmental-2020-300180 - Stanghellini G, Leoni F. Digital Phenotyping: Ethical Issues, Opportunities, and Threats. Front Psychiatry. 2020;11:473. PMID: 32536882; PMCID: PMC7267063. https://doi.org/10.3389/fpsyt.2020.00473
- Hieronymus F, Østergaard S. Rating, berating or overrating antidepressant efficacy? The case of the Hamilton depression rating scale. European neuropsychopharmacology. 2021;52:12-14.
- Kidron CA, Kirmayer LJ. Global Mental Health and Idioms of Distress: The Paradox of Culture-Sensitive Pathology of Distress in Cambodia. Cult Med Psychiatry. 2019;43(2):211-235. PMID: 30515681. https://doi.org/10.1007/s11013-018-9612-9
- Wang YP, Gorenstein C. Psychometric properties of the Beck Depression Inventory-II: a comprehensive review. Braz J Psychiatry. 2013;35(4):416-41. Epub 2013 Dec 23. PMID: 24402217. https://doi.org/10.1590/1516-4446-2012-1048
- Smoller JW, Andreassen OA, Edenberg HJ, et al.
 Psychiatric genetics and the structure of psychopathology. Mol Psychiatry. 2019;24:409-420. https://doi.org/10.1038/s41380-017-0010-4
Psychiatric genetics and the structure of psychopathology. Mol Psychiatry. 2019;24:409-420. https://doi.org/10.1038/s41380-017-0010-4 - Hyde CL, Nagle MW, Tian C, et al. Identification of 15 genetic loci associated with risk of major depression in individuals of European descent. Nat Genet. 2016;48(9):1031-1036. Epub 2016 Aug 1. PMID: 27479909; PMCID: PMC5706769. https://doi.org/10.1038/ng.3623
- Brennan C, Worrall-Davies A, McMillan D, et al. The hospital anxiety and depression scale: A diagnostic meta-analysis of case-finding ability. J Psychosom Res. 2010;69(4):371-378.
- Kibitov AO, Mazo GE, Rakitko AS, et al. GWAS-based polygenic risk scores for depression with clinical validation: methods and study design in the Russian population. Zhurnal Nevrologii i Psikhiatriii im. S.S. Korsakova. 2020;120(11):131-140. https://doi.org/10.17116/jnevro2020120111131
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, DSM-5.
 American Psychiatric Publishing. 2013.
American Psychiatric Publishing. 2013. - Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67:6:361-370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x
- Irwig L, Tosteson AN, Gatsonis C, et al. Guidelines for meta-analyses evaluating diagnostic tests. Ann Intern Med. 1994;120:667-676.
- Leeflang MM. Systematic reviews and meta-analyses of diagnostic test accuracy. Clin Microbiol Infect. 2014;20(2):105-113. PMID: 24274632. https://doi.org/10.1111/1469-0691.12474
- Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: Hot to practice and teach EBM, 2nd Edition. New York, Churchill Livingstone; 2000.
- Kibitov AA, Rakitko AS, Kasyanov ED, Rukavishnikov GV, Kozlova KA, et al. Screening of Depressive Symptoms in a Russian General Population Sample: A Web-based Cross-sectional Study. Clinical Practice & Epidemiology in Mental Health. 2021;17:205-211. https://doi.org/10.2174/1745017
7010205
- Thombs BD, Kwakkenbos L, Levis AW, et al.
 Addressing overestimation of the prevalence of depression based on self-report screening questionnaires. CMAJ. 2018;190(2):44-49. https://doi.org/10.1503/cmaj.170691
Addressing overestimation of the prevalence of depression based on self-report screening questionnaires. CMAJ. 2018;190(2):44-49. https://doi.org/10.1503/cmaj.170691
Close metadata
Types of depression and their classification
Depression - what is it, what is its etiology, what is the relevance of depressive disorders. Symptoms and classification of depression. What are the characteristics of certain types of depression? These topics formed the basis of our interview with the Chief Physician of the Health Harmony Medical Center, psychiatrist, psychiatrist-narcologist and psychotherapist Vladislav Sipovich. nine0006
What is depression, how common is it and what are its causes?
Depression in Latin means to suppress, put pressure on something. As a medical term, it is used to define a mental disorder characterized by low mood, manifested by a depressed, depressed, sad, anxious, or indifferent state. Accompanied by anhedonia - a reduced or completely lost ability to enjoy life and have fun.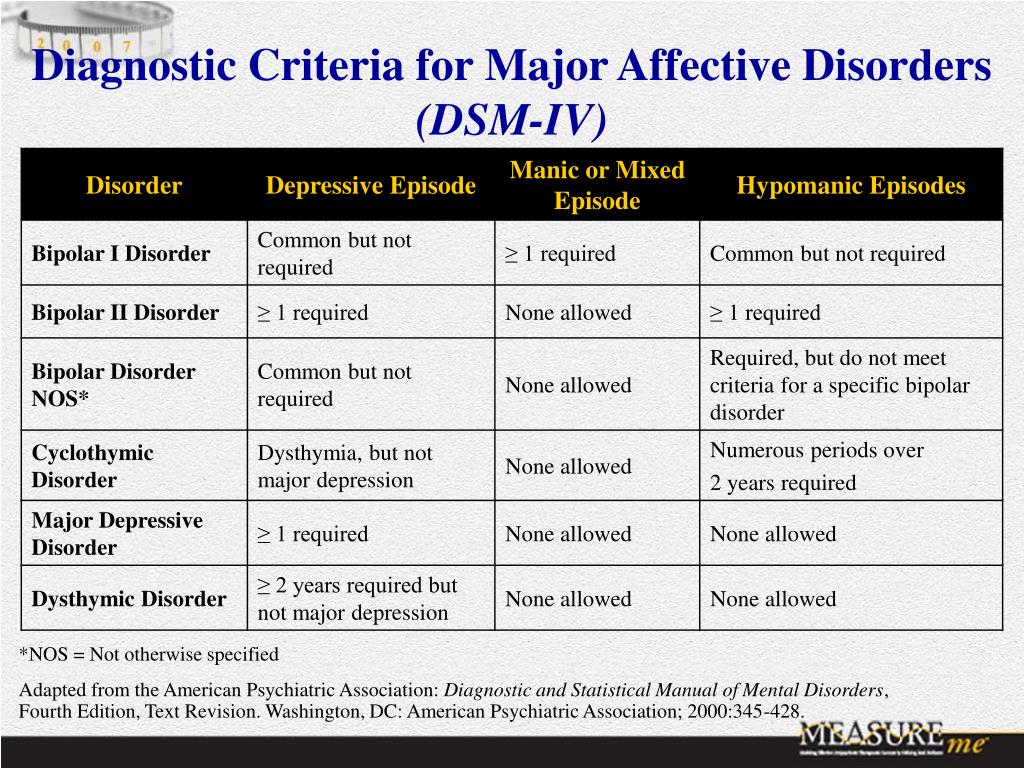 nine0006
nine0006
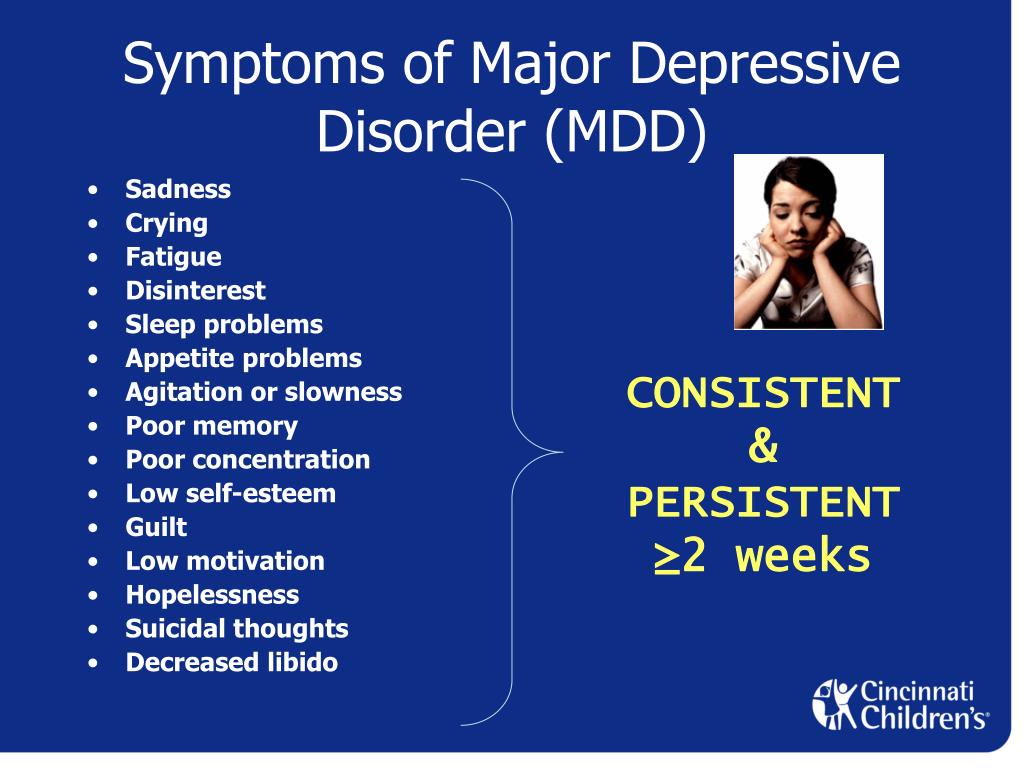
The main symptoms of depression are:
• Low self-esteem.
• Loss of interest in normal activities.
• Exaggerated sense of guilt.
• Decreased mood.
• Pessimistic outlook on life.
• Fatigue and lack of energy.
• Violation of concentration, sleep and appetite.
• Suicidal thoughts.
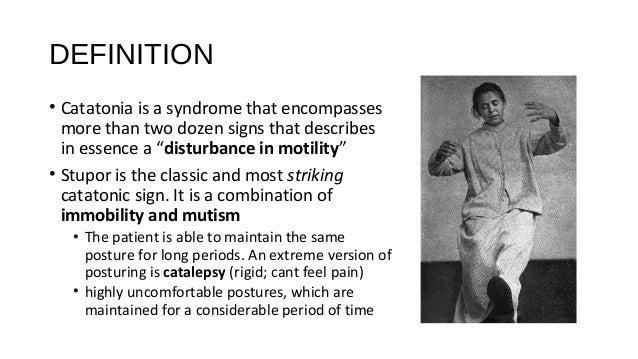
Severe forms of depression are characterized by the so-called depressive triad:
• Low mood. nine0005 • Inhibited thinking.
• Decreased motor activity with a predominance of inhibition processes.
Temporary depression can be a normal response to negative life circumstances such as job loss, divorce, financial loss, illness or loss of loved ones. In such cases, a person sometimes begins to abuse alcohol, drugs, antidepressants and other psychoactive substances.
Depressive disorder may be a symptom of physical illness or a side effect of certain medications. If the cause of depression is not identified, then it is differentiated as endogenous.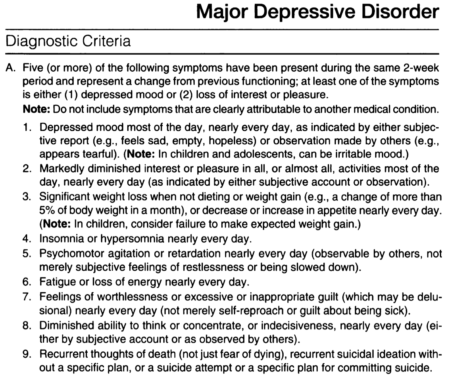 Screening for types of depression is done using self-assessment tests such as the Zang or Beck scale, a large depression questionnaire. By the way, the main symptoms of depression were described by Hippocrates, who defined this condition as melancholy. nine0006
Screening for types of depression is done using self-assessment tests such as the Zang or Beck scale, a large depression questionnaire. By the way, the main symptoms of depression were described by Hippocrates, who defined this condition as melancholy. nine0006
The relevance of identifying and diagnosing depression is explained not only by the fact that it significantly reduces the quality of life of a person, but is also the most common mental disorder. Every tenth person over the age of 40 suffers from it, and 2/3 of them are women. Children are less susceptible to depression, but nevertheless, 5% of adolescents aged 10-16 experience a depressive disorder. Depression is a major cause of morbidity and disability in children and young people, and significantly increases the risk of suicide in these age groups. nine0006
The etiology of depression is multifactorial. The main causes can be combined into the following groups:
• Social and psychological leading to the so-called reactive (psychogenic) depression.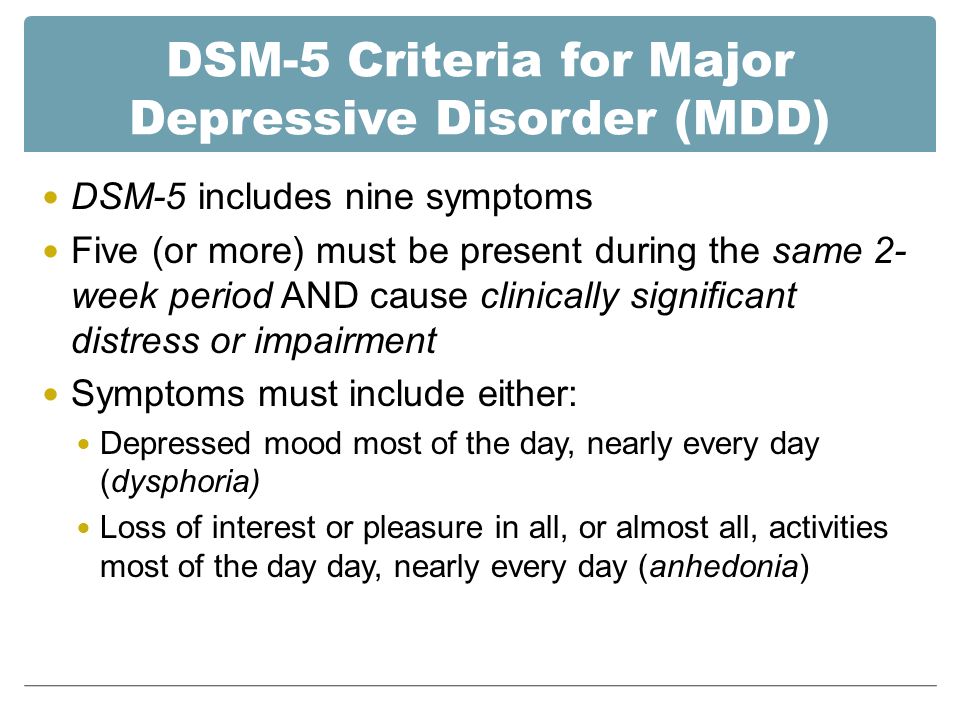 Depression in this case develops as a response to the external impact of events, situations and stress.
Depression in this case develops as a response to the external impact of events, situations and stress.
• Somatic , more precisely somatogenic. An example is Alzheimer's disease, atherosclerosis of the cerebral arteries, TBI, viral infections, endocrinological disorders, especially in hypothyroidism (7 times higher than in healthy people), etc.
• Iatrogenic developing in response to taking certain drugs - corticosteroids, benzodiazepines, neuroleptics, sedatives and hypnotics. This group also includes depressions provoked by the abuse of alcohol, cocaine, opiates, and other psychostimulants. They usually heal on their own or go away when the drugs are stopped.
• Endogenous , arising without any apparent external cause, as if from within the body. About 35% of depressions develop autochthonously without any external influences. nine0005 Risk factors for depression are:
• Dramatic childhood experiences including abuse, loss of parents or their antisocial behavior, physical anomalies in the child, bullying and cyberbullying by peers or teachers.
• Personal characteristics of the patient , for example, perfectionism.
• Periods of hormonal adjustment - adolescence, menopause, as well as pregnancy and childbirth. About 10% of pregnant women may suffer from depression, and postpartum depression occurs in 12-16% of women who have given birth. nine0006
As for the neurobiological mechanisms of the development of major depressive disorder, there are several hypotheses, among which the most popular is monoamine, linking depression with a lack of amine neurotransmitters - serotonin, norepinephrine, dopamine. This theory has not yet received a convincing evidence base.
There is also an evolutionary theory of depression, which considers it as a survival mechanism and the possibility of the least painful solution to urgent problems. Avoidance behavior in depression helps to solve problems such as:
• avoid unpleasant moments in the process of understanding negative situations and making often forced compromise decisions;
• adapt to unpleasant circumstances, and in a social environment in which there are opportunities for avoiding them.
Also noteworthy is such a type of depression as seasonal affective disorder, which develops as a result of prolonged sunless weather in autumn and winter, as well as in people who are in rooms with twilight lighting for a long time. Seasonal depression is treated with walks in the sun or light therapy. Perhaps the seasonality of the disease is due to a deficiency in the formation of vitamin D in the skin with a lack of sunlight in the UV spectrum. nine0006
According to the cognitive model of depression, it is caused by dysfunctional beliefs that are formed in childhood and activated in adulthood under certain life circumstances. According to this theory, the distortion of thinking in depression manifests itself in the form of a cognitive triad:
• Low self-esteem, confidence in one's own worthlessness.
• Low opinion of the surrounding reality.
• Disbelief in one's own "bright" future.
Distorted thinking and ideas also manifest themselves in the “tyranny of duties” characteristic of depressive patients in the form of a firm conviction that they should know everything, understand, foresee, make quick and correct decisions, etc. At the same time, there are random inferences, exaggerations, generalization or selective abstraction from events and situations. nine0006
At the same time, there are random inferences, exaggerations, generalization or selective abstraction from events and situations. nine0006
What is the diagnosis of depression based on?
Difficulties in diagnosing depressive disorders are primarily due to the fact that patients try not to advertise their condition and often hide the symptoms of depression. This is explained by the fear of prescribing antidepressants and the occurrence of side effects from taking them, as well as fixing the diagnosis in the medical record, followed by referral to a psychiatrist or psychotherapist and a possible report to the employer.
Depression is diagnosed in the following areas:
• Screening for the presence of a disorder.
• Test and clinician's clinical evaluation.
• Determination of the severity of individual symptoms - anxiety, anhedonia, suicidal tendencies.
As I said, various tests (Zange or Beck scale) and questionnaires (short and long) are used to screen and determine the severity of depression.
Clinical judgment is important in the choice of treatment and management. Based mainly on medical experience, the role of instrumental or laboratory criteria is relevant only in the diagnosis of somatic depression caused by diseases of an infectious, neurological, endocrinological nature. To differentiate the latter, it is important in depressed patients to conduct an examination of the thyroid gland to diagnose hypo- or hyperthyroidism. nine0006
According to ICD-10 (International Classification of Diseases, 10th Revision), symptoms of depression are divided into major and minor symptoms. To make a diagnosis, you must have 2 main and at least 3 additional.
The main (typical) symptoms of depression are:
• Unreasonably depressed mood for more than 2 weeks.
• Anhedonia with loss of interest in life and inability to enjoy previously pleasant moments and activities. nine0005 • Loss of strength, increased fatigue, stably fixed for a month.
Additional symptoms include:
• Pessimistic outlook on life.
• Anxiety, fear, sense of worthlessness and pronounced guilt.
• Low self-esteem.
• Decreased ability to concentrate and make decisions.
• Appetite disorders, decreased or increased weight.
• Sensation of a sweet taste in the mouth (glycogeusia). nine0005 • Suicidal thoughts and obsessive thoughts about death.
• Sleep disorders in the form of insomnia or, conversely, drowsiness and oversleeping.
The duration of symptoms for a reliable diagnosis should be at least 2 weeks, although a shorter period of their manifestation is allowed with especially pronounced severity and intensity.
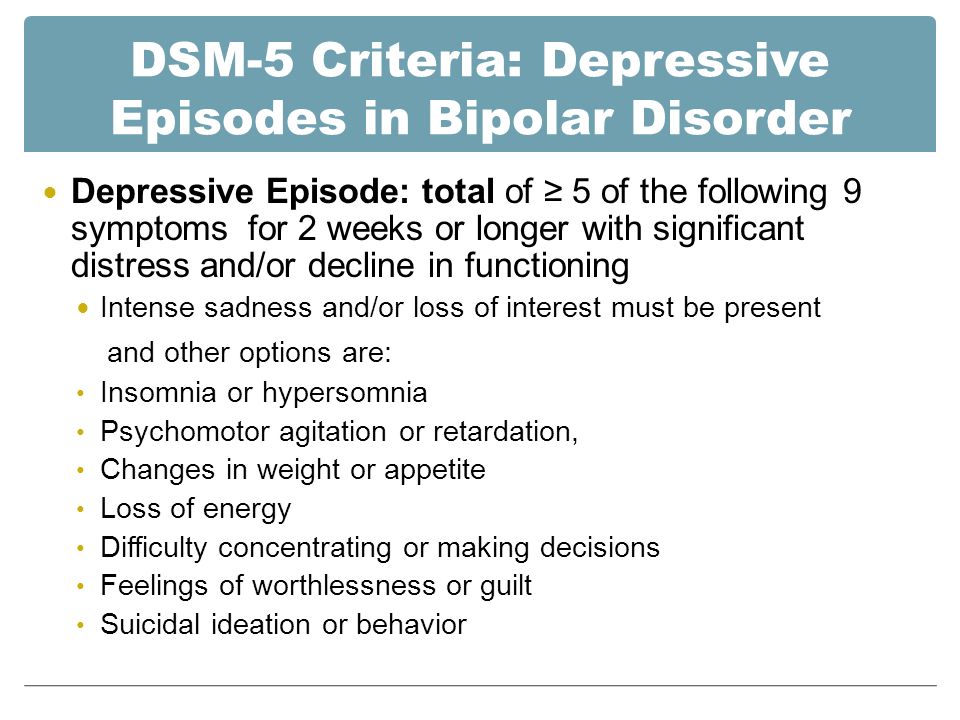
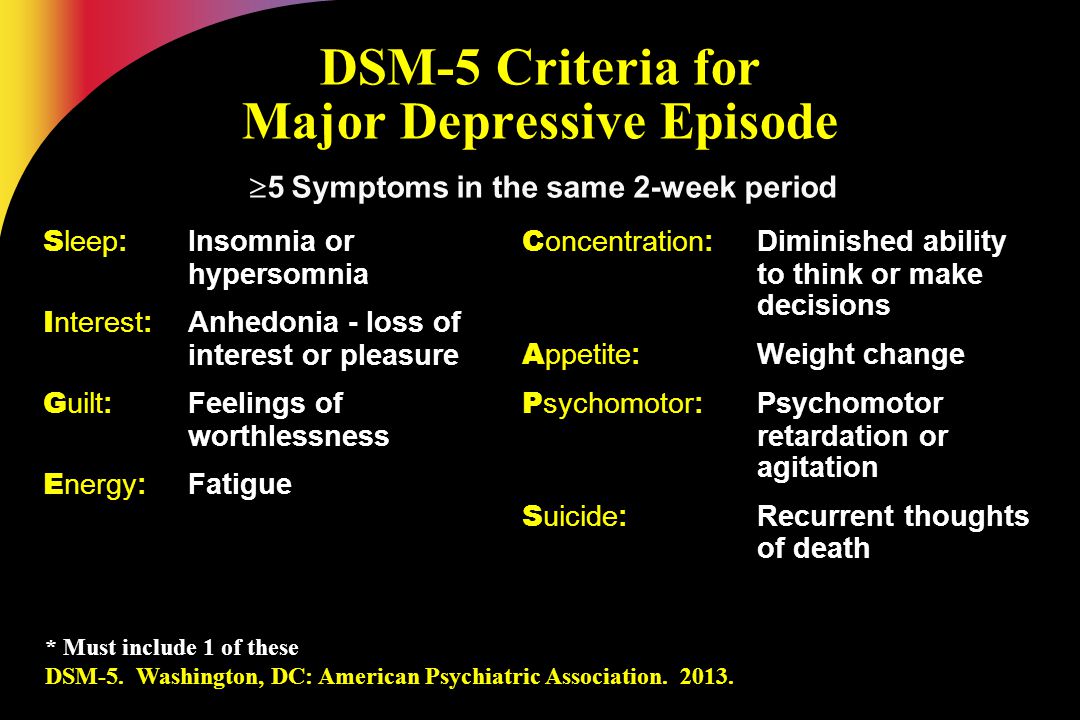
According to the diagnostic criteria of the American classification of mental illness DSM-IV-TR, it is necessary to identify and save for 2 weeks 5 of these 9Symptoms:
• Suppressed depressive mood, which in adolescence may be manifested by irritability.
• Anhedonia.
• Increase or decrease in appetite and weight.
• Insomnia - difficulty falling asleep, dissatisfaction with the quality of sleep, and hypersomnia (sleep intoxication), manifested by difficulty in the transition from sleep to wakefulness.
• Psychomotor inhibition or excitation.
• Inhibition of thought processes and decreased attention, especially the ability to concentrate. nine0005 • Feelings of insignificance, low self-esteem, inflated guilt.
• Increased fatigue, loss of energy, decreased vitality.
• Persistent thoughts of death and suicide, marked suicidal tendencies.
As part of the 5 significant symptoms, at least one of the 2 main symptoms must be present - anhedonia and / or depressive mood.
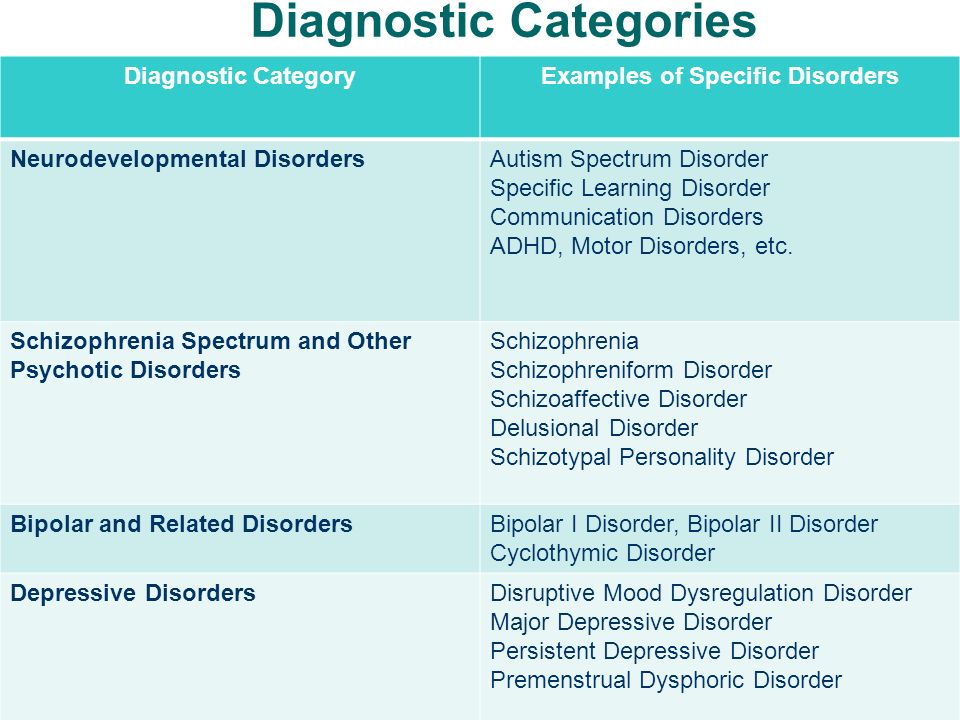
How are different types of depression classified?
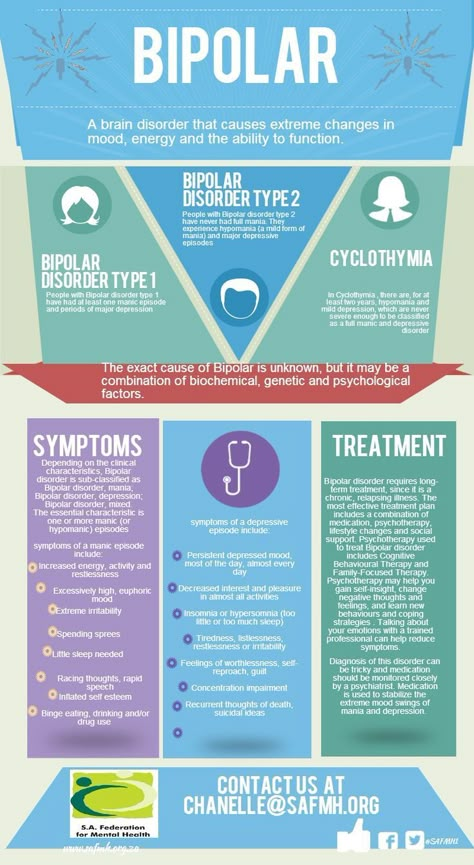
The classification of the main types of depression is based on the etiology, clinical picture, prevailing symptoms, frequency of occurrence, duration of the course and other features. nine0005 If the mood remains stably lowered, then such depressive disorders are referred to as unipolar, if episodes of depression are interspersed with manic (enthusiastic mood and arousal) - they speak of mixed or bipolar depression, more likely related to bipolar disorder (OCD).
The following types of unipolar depression are classified in the DSM-IV:
• Major depressive disorder (clinical depression) with all of the characteristic symptoms described above. nine0006
• Minor depression in which not all symptoms of clinical depression are present, but 2 major depression criteria are present for at least 2 weeks.
• Atypical form , in which, along with the typical symptoms of a depressive disorder, there are also atypical ones - increased appetite, weight gain, emotional reactivity.
• Recurrent transient form depression (RBD) with a characteristic course. Episodes develop about once a month and last less than 2 weeks, most often 2-3 days. Diagnosis requires regular occurrence of episodes throughout the year without reference to MC in women. nine0006
• Dysthymia is a mild form of mood disorder characterized by milder and less severe symptoms than clinical depression. Despite this, it has a protracted course, lasts much longer, at least 2 years, sometimes stretches for decades. Therefore, it is often referred to as chronic depression. Sometimes it develops into major depressive disorder, in which case it is called double depression.
Despite this, it has a protracted course, lasts much longer, at least 2 years, sometimes stretches for decades. Therefore, it is often referred to as chronic depression. Sometimes it develops into major depressive disorder, in which case it is called double depression.
• In domestic medicine, the concept of 9 is widespread0234 vital, i.e. life depression . It is characterized by pronounced melancholy and anxiety, which can manifest itself even at the physical level, for example, pain in the solar plexus, lack of need for food and sleep. Therefore, it is also called "dreary depression." It proceeds quite hard, but has a favorable prognosis, as it responds well to treatment with antidepressants.
• The resistant form , in contrast to the vital form, does not give a pronounced clinical effect when even two 4-week courses of antidepressants are used. nine0006
• Anxiety and depressive disorder . Reminds depressive, but in contrast to it, anxiety and depressive syndromes in the clinical picture are equally represented.
• The neurotic form of is characterized by low self-esteem, lack of confidence in one's strengths and abilities, and an acute sense of guilt.
• Autonomic depression with severe physical symptoms such as tachycardia, BP fluctuations, tinnitus. nine0006
• Masked with hidden, mild signs of apathy, with a desire for solitude and self-isolation, reduced interest in life. It masquerades as chronic fatigue.
• Asthenic . It proceeds with weakness, lethargy, sleep disturbances, emotional instability, aggravated by stress, physical and mental overload.
• Postpartum . It develops 10-14 days after childbirth against the background of hormonal changes, anxiety for the baby, constant lack of sleep and excessive fatigue. nine0006
• Somatogenic . It is a consequence of endocrine disorders, neoplasms, brain injuries, impaired blood supply, and some psychotic conditions.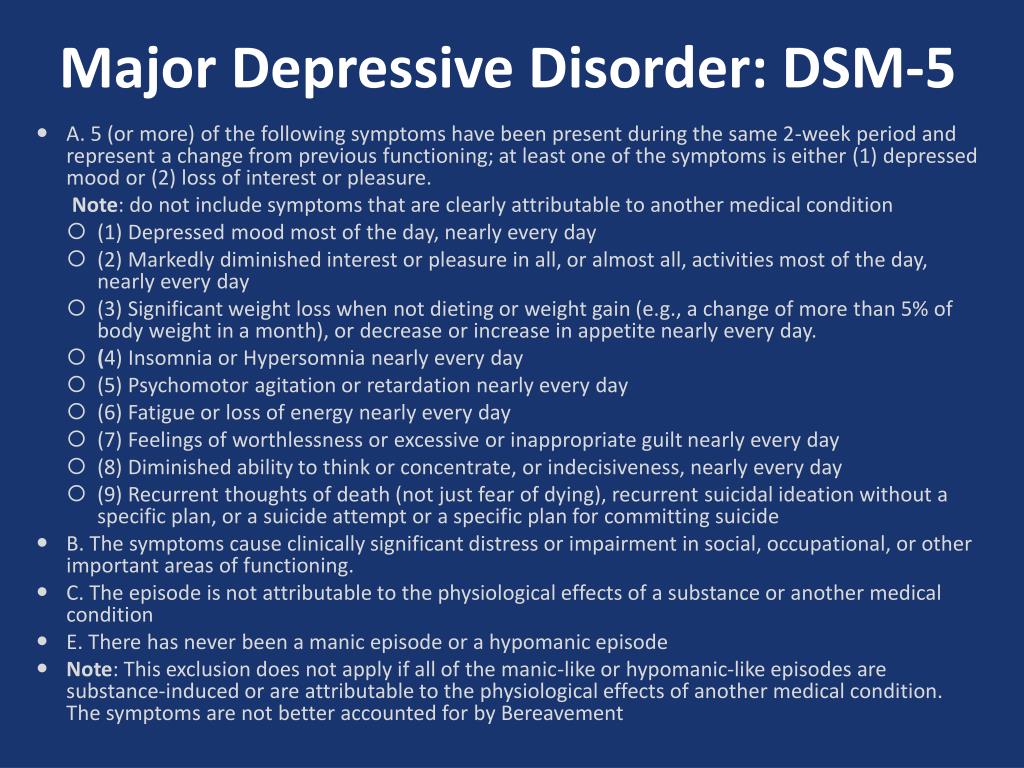
• Alcoholic depression . It is a mental disorder, accompanied by dependence on alcohol, detachment, non-recognition of the problem and often self-flagellation, an acute sense of guilt. Women are at particular risk due to their increased emotionality.
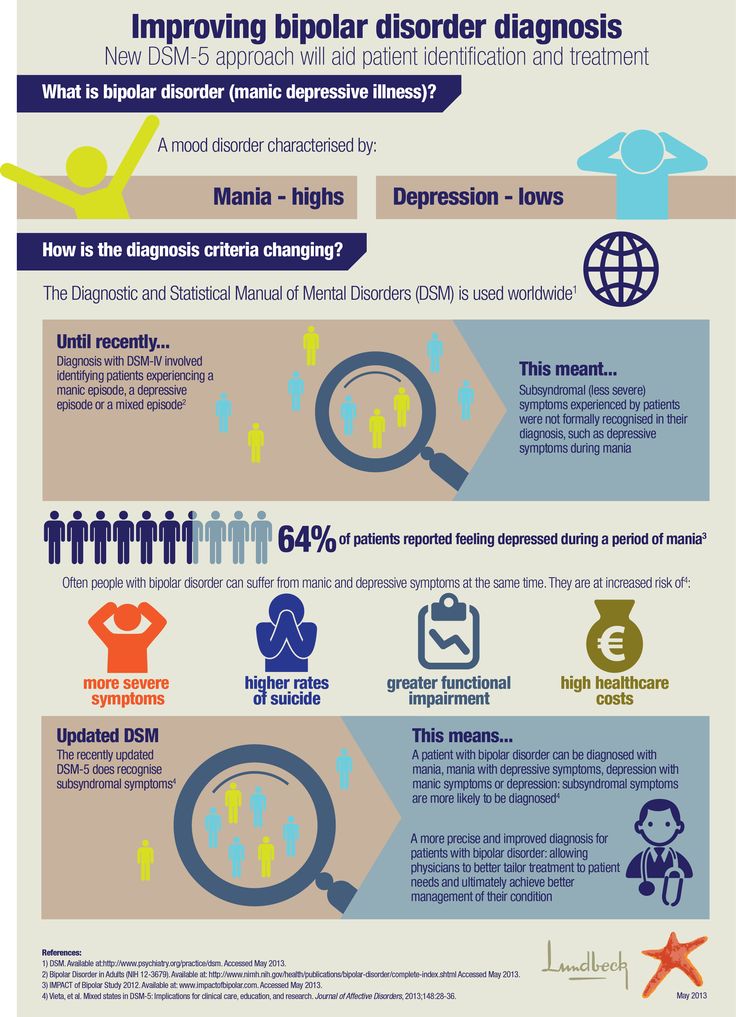
The following forms are distinguished among bipolar depressive disorders:
• Type I bipolar depression. Rare, characterized by alternating phases of depression, normal mood and manic phases. The latter are characterized by an elevated, almost euphoric mood, hyperactivity, increased excitability, and reduced need for sleep. In the manic phase, a person often commits rash acts, engages in casual sexual relationships, and often takes irrational financial steps. In fact, bipolar depression can be characterized as being periodically on top of the world, followed by a plunge into the abyss of despair. nine0005 • Bipolar depression type II. More similar to recurrent depression in terms of milder symptoms and frequency of episodes.