Non ssri for anxiety
Non-Antidepressant Treatment of Generalized Anxiety Disorder
. 2015;10(2):86-96.
doi: 10.2174/15748847113089990058.
Nada Zahreddine, Sami Richa 1
Affiliations
Affiliation
- 1 Hôtel-Dieu de France University Hospital, Achrafieh, Lebanon.
- PMID: 23438725
- DOI: 10.2174/15748847113089990058
Nada Zahreddine et al. Curr Clin Pharmacol. 2015.
. 2015;10(2):86-96.
doi: 10.2174/15748847113089990058.
Authors
Nada Zahreddine, Sami Richa 1
Affiliation
- 1 Hôtel-Dieu de France University Hospital, Achrafieh, Lebanon.
- PMID: 23438725
- DOI: 10.2174/15748847113089990058
Abstract
Introduction: Generalized anxiety disorder (GAD) is a prevalent and very disabling anxiety disorder. First-line medications are antidepressants such as selective serotonin reuptake inhibitors (SSRIs) and selective serotonin and noradrenalin reuptake inhibitors (SNRIs). However, a substantial number of patients do not reach remission while on antidepressants and they may develop troublesome side effects, which highlights the necessity of new therapeutic options for GAD.
However, a substantial number of patients do not reach remission while on antidepressants and they may develop troublesome side effects, which highlights the necessity of new therapeutic options for GAD.
Methods: The purpose of this review is to discuss all non-antidepressant treatments studied in GAD. We searched MedLine for English articles published between 1980 and 2012, containing the following keywords: "generalized (or generalised) anxiety disorder" OR "anxiety disorder", AND "drug therapy" OR "herbal medicine". 76 articles were finally selected.
Results: Pregabalin is the anticonvulsant with the most robust level of evidence in GAD. It rapidly reduces anxiety, has a safe side effect profile and presents a low potential for abuse. Among antipsychotics, quetiapine is the one of choice in GAD, with similar efficacy to SSRIs in low dosages, yet with lower overall tolerability. Benzodiazepines, buspirone and hydroxyzine are Food and Drugs administration (FDA) approved for GAD and have relatively good evidence of efficacy. Other drugs (betablockers, zolpidem, riluzole, etc.) and natural remedies (e.g. Piper methysticum) could be potential treatment options, yet additional research is warranted.
Benzodiazepines, buspirone and hydroxyzine are Food and Drugs administration (FDA) approved for GAD and have relatively good evidence of efficacy. Other drugs (betablockers, zolpidem, riluzole, etc.) and natural remedies (e.g. Piper methysticum) could be potential treatment options, yet additional research is warranted.
Conclusion: Pregabalin and quetiapine are the two most promising non-antidepressant treatments for GAD.
Keywords: Anticonvulsants; antipsychotics; drug therapy; generalized anxiety; herbal treatment; pregabalin; quetiapine.
Copyright© Bentham Science Publishers; For any queries, please email at [email protected].
Similar articles
-
New approaches to the pharmacological management of generalized anxiety disorder.

Buoli M, Caldiroli A, Caletti E, Paoli RA, Altamura AC. Buoli M, et al. Expert Opin Pharmacother. 2013 Feb;14(2):175-84. doi: 10.1517/14656566.2013.759559. Epub 2013 Jan 3. Expert Opin Pharmacother. 2013. PMID: 23282069 Review.
-
Selecting pharmacotherapy for generalized anxiety disorder.
Goodman WK. Goodman WK. J Clin Psychiatry. 2004;65 Suppl 13:8-13. J Clin Psychiatry. 2004. PMID: 15384931 Review.
-
Treatment of generalized anxiety disorder: a comprehensive review of the literature for psychopharmacologic alternatives to newer antidepressants and benzodiazepines.
Huh J, Goebert D, Takeshita J, Lu BY, Kang M. Huh J, et al. Prim Care Companion CNS Disord. 2011;13(2):PCC.
 08r00709. doi: 10.4088/pcc.08r00709blu. Prim Care Companion CNS Disord. 2011. PMID: 21977338 Free PMC article.
08r00709. doi: 10.4088/pcc.08r00709blu. Prim Care Companion CNS Disord. 2011. PMID: 21977338 Free PMC article. -
Pharmacotherapy for generalized anxiety disorder in adult and pediatric patients: an evidence-based treatment review.
Strawn JR, Geracioti L, Rajdev N, Clemenza K, Levine A. Strawn JR, et al. Expert Opin Pharmacother. 2018 Jul;19(10):1057-1070. doi: 10.1080/14656566.2018.1491966. Expert Opin Pharmacother. 2018. PMID: 30056792 Free PMC article. Review.
-
Pharmacological treatment of generalized anxiety disorder.
Reinhold JA, Mandos LA, Rickels K, Lohoff FW. Reinhold JA, et al. Expert Opin Pharmacother. 2011 Nov;12(16):2457-67. doi: 10.1517/14656566.2011.618496. Epub 2011 Sep 28. Expert Opin Pharmacother.
 2011. PMID: 21950420 Review.
2011. PMID: 21950420 Review.
See all similar articles
Cited by
-
AVN-101: A Multi-Target Drug Candidate for the Treatment of CNS Disorders.
Ivachtchenko AV, Lavrovsky Y, Okun I. Ivachtchenko AV, et al. J Alzheimers Dis. 2016 May 25;53(2):583-620. doi: 10.3233/JAD-151146. J Alzheimers Dis. 2016. PMID: 27232215 Free PMC article. Review.
-
Anxiolytic and antidepressant-like activities of the novel and potent non-imidazole histamine H₃ receptor antagonist ST-1283.
Bahi A, Schwed JS, Walter M, Stark H, Sadek B. Bahi A, et al. Drug Des Devel Ther. 2014 May 28;8:627-37. doi: 10.2147/DDDT.S63088. eCollection 2014. Drug Des Devel Ther. 2014. PMID: 24920886 Free PMC article.
What alternative anxiety medication can be used if you cannot tolerate an SSRI?
Generalized anxiety disorder (GAD) is often treated with Selective Serotonin Reuptake Inhibitors (SSRIs). Normally, people are first prescribed the SSRIs citalopram, escitalopram or sertraline. Trials show that only 50% to 60% of people respond to these medications, remission rates between 25% and 35% are achieved, and a large proportion of patients experience significant SSRI side effects. Pharmacogenetic testing, which determines how you respond to medications based on your unique DNA, can help individuals and their healthcare providers to understand why some cannot tolerate SSRIs and help predict how other anxiety medications will work for them. Pharmacogenetic testing will indicate if an individual is a normal, intermediate, ultrarapid, or poor metabolizer for commonly prescribed medications. It can help determine which of the other possible treatment options for GAD are right for an individual. These include serotonin-norepinephrine reuptake inhibitors (SNRIs), buspirone, hydroxyzine, pregabalin, and bupropion. A prescribing algorithm, or process to be followed for GAD treatment is available at: psychopharm.mobi.
These include serotonin-norepinephrine reuptake inhibitors (SNRIs), buspirone, hydroxyzine, pregabalin, and bupropion. A prescribing algorithm, or process to be followed for GAD treatment is available at: psychopharm.mobi.
Some patients with GAD frequently experience SSRI-induced sexual side effects, worsening of anxiety or sleep disruption. There are multiple reasons for SSRI intolerance – you can find more details here.
Below we provide an overview of some alternative medications that can be used for treatment of anxiety and the role of pharmacogenetic variations that have an impact on tolerability and response.
Duloxetine and Venlafaxine
Duloxetine (Cymbalta) and venlafaxine (Effexor) come from another family of medications called SNRIs that are FDA-approved for the treatment of GAD. Duloxetine may also be useful for patients suffering from neuropathic pain and fibromyalgia. Duloxetine is ususally preferred because it may have less sexual side effects than venlafaxine does. Duloxetine is cleared in the liver by two important enzymes in drug metabolism called CYP2D6 and CYP1A2. Sometimes, duloxetine and the drug fluvoxamine are prescribed together. Fluvoxamine is used to treat obsessive-compulsive disorder which often occurs with GAD. People who do not metabolize duloxetine normally based on their pharmacogenetic profile may experience serious side effects because fluvoxamine interferes with CYP1A2 enzymes and is also metabolized by CYP2D6. In one study, poor CYP2D6 metabolizers of duloxetine experienced a six-fold increase of the the drug in their blood versus those who metabolize it normally. Excessive drug dose is one of the most common reasons why some people cannot tolerate SSRIs.
Duloxetine is cleared in the liver by two important enzymes in drug metabolism called CYP2D6 and CYP1A2. Sometimes, duloxetine and the drug fluvoxamine are prescribed together. Fluvoxamine is used to treat obsessive-compulsive disorder which often occurs with GAD. People who do not metabolize duloxetine normally based on their pharmacogenetic profile may experience serious side effects because fluvoxamine interferes with CYP1A2 enzymes and is also metabolized by CYP2D6. In one study, poor CYP2D6 metabolizers of duloxetine experienced a six-fold increase of the the drug in their blood versus those who metabolize it normally. Excessive drug dose is one of the most common reasons why some people cannot tolerate SSRIs.
Venlafaxine is also metabolized by CYP2D6. For CYP2D6 poor and intermediate metabolizers, the Royal Dutch Pharmacists Association – Pharmacogenetics Working Group (DPWG) guidelines recommend an alternative to venlafaxine or to adjust the dose to and to monitor the patient’s plasma metabolite level. For CYP2D6 ultrarapid metabolizers, the DPWG guidelines suggest prescribing a dose to a maximum of 150% of the normal dose or to select an alternative to venlafaxine.
For CYP2D6 ultrarapid metabolizers, the DPWG guidelines suggest prescribing a dose to a maximum of 150% of the normal dose or to select an alternative to venlafaxine.
Ethnic Background and SNRIs
Depending on ethnic background, 30-50% of people in North America have inherently altered CYP2D6 activity and may experience side effects when treated with duloxetine or venlafaxine, and also cannot tolerate SSRIs such as fluoxetine and paroxetine. Poor and Ultrarapid metabolizers should not be prescribed these medications due to the availability of other, better alternatives. Other SNRIs, such as desvenlafaxine and levomilnacipran, are metabolized by the CYP3A4 enzyme, not the CYP2D6 and could be prescribed instead if a person’s pharmacogenetic profile indicates they are good alternatives.
General Side Effects
SNRIs may cause headaches, drowsiness or insomnia, nervousness, nausea, dry mouth, weight loss and increased sweating. Patients starting an SNRI should be monitored for efficacy of treatment as well as tolerability. When starting an SNRI, the patient’s other health problems should also be assessed by the healthcare provider to ensure that it is the correct medication.
When starting an SNRI, the patient’s other health problems should also be assessed by the healthcare provider to ensure that it is the correct medication.
The SNRI Buspirone (Buspar) is used for treatment of GAD and depression. Buspirone is metabolized by the CYP3A4 enzyme, which is involved in the metabolism of multiple medications. The activity of CYP3A4 can vary by a factor of 10-100 between individuals. About 15% of people in North America have inherently reduced CYP3A4 function; people carrying inactive alleles are at increased risk of drug-induced toxicity, especially when buspirone is co-prescribed with CYP3A4 substrate or inhibitors.
Generalized Anxiety Drugs not affected by Pharmacogenetics
Pregabalin (Lyrica) is an antiepileptic medication that commonly prescribed for anxiety in Europe and South America where it is approved for GAD, but in Canada and US it is approved for treatment of neuropathic pain in patients with diabetic peripheral neuropathy and postherpetic neuralgia. Pregabalin is more sedating than SSRIs and might be beneficial for anxiety patients experiencing insomnia. Furthermore, it has a faster response profile than SSRIs. Pregabalin should be used with caution in the elderly however because of increased risk of falls and somnolence. Gabapentin is another antiepileptic medication prescribed for neuropathic pain and seizures, but also frequently used off-label as an anti-anxiety treatment. Gabapentin and pregabalin are mostly eliminated through the kidneys or renally and not through the liver like SNRIs and SSRIs and are therefore unlikely to be influenced by a person’s pharmacogenetic profile.
Pregabalin is more sedating than SSRIs and might be beneficial for anxiety patients experiencing insomnia. Furthermore, it has a faster response profile than SSRIs. Pregabalin should be used with caution in the elderly however because of increased risk of falls and somnolence. Gabapentin is another antiepileptic medication prescribed for neuropathic pain and seizures, but also frequently used off-label as an anti-anxiety treatment. Gabapentin and pregabalin are mostly eliminated through the kidneys or renally and not through the liver like SNRIs and SSRIs and are therefore unlikely to be influenced by a person’s pharmacogenetic profile.
Other less-common alternatives
Although the FDA has approved the tranquilizer alprazolam for generalized anxiety disorder, benzodiazepines, the class of drugs that alprazolam belongs to, are generally not recommended as alternatives to SSRIs for treatment of anxiety. This is because of their sedative effects, which can lead to automobile accidents, increased risk of falls and impaired memory. Benzodiazepines are also associated with the potential for abuse.
Benzodiazepines are also associated with the potential for abuse.
In patients with severe uncontrolled anxiety, antipsychotic augmentation might also be considered. Medications that have been evaluated in this context include risperidone, olanzapine and quetiapine.
Summary
- Pharmacogenetic test results can provide insight to which of the SSRIs and SNRIs should be used for the treatment of anxiety.
- Pharmacogenetic testing can help to reduce the number of SSRI trials an individual requires, improve tolerability, and the adherence to treatment.
- Clinical pharmacists can assist physicians to optimize medication management, particularly for patients with complex drug metabolic profiles who are frequently “treatment resistant” or cannot tolerate SSRIs.
References:
http://psychopharm.mobi/algo_live/
Roy-Byrne, P., MD. Treatment-refractory anxiety; definition, risk factors, and treatment challenges. Dialogues Clin Neurosci. 2015 Jun; 17(2): 191–206.
Dialogues Clin Neurosci. 2015 Jun; 17(2): 191–206.
Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders. Katzman MA, Bleau P, Blier P, Chokka P, Kjernisted K, Van Ameringen M; Canadian Anxiety Guidelines Initiative Group on behalf of the Anxiety Disorders Association of Canada/Association Canadienne des troubles anxieux and McGill University, Antony MM, Bouchard S, Brunet A, Flament M, Grigoriadis S, Mendlowitz S, O’Connor K, Rabheru K, Richter PM, Robichaud M, Walker JR. BMC Psychiatry. 2014;14 Suppl 1:S1. doi: 10.1186/1471-244X-14-S1-S1. Epub 2014 Jul 2. Review.
Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 6. Special Populations: Youth, Women, and the Elderly. MacQueen GM, Frey BN, Ismail Z, Jaworska N, Steiner M, Lieshout RJ, Kennedy SH, Lam RW, Milev RV, Parikh SV, Ravindran AV; CANMAT Depression Work Group. Can J Psychiatry. 2016 Sep;61(9):588-603. doi: 10.1177/0706743716659276. Epub 2016 Aug 2. Review. Erratum in: Can J Psychiatry. 2017 May;62(5):356.
Can J Psychiatry. 2016 Sep;61(9):588-603. doi: 10.1177/0706743716659276. Epub 2016 Aug 2. Review. Erratum in: Can J Psychiatry. 2017 May;62(5):356.
Jakubovski E, Johnson JA, Nasir M, Müller-Vahl K, Bloch MH. Systematic review and meta-analysis: Dose-response curve of SSRIs and SNRIs in anxiety disorders. Depress Anxiety. 2019 Mar;36(3):198-212.
Hicks JK et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors. Clin Pharmacol Ther. 2015 Aug; 98(2): 127–134.
-
Ruslan Dorfman, PhD, MBA
Founder and CSO Ruslan Dorfman is a trailblazer in personalized medicine, a molecular geneticist, and technology builder.
 Inspired by direct interactions with Cystic Fibrosis families from all over the world, Dr. Dorfman co-founded GeneYouIn to facilitate access to advanced genetics for the general public. He managed large-scale R&D programs at Sick Kids Hospital, Toronto. He advised Bridgepoint and Mount Sinai hospitals on the implementation of personalized medicine programs. Dr. Dorfman has published thirty peer-reviewed papers on the genetics of Cystic Fibrosis and Pain.
Inspired by direct interactions with Cystic Fibrosis families from all over the world, Dr. Dorfman co-founded GeneYouIn to facilitate access to advanced genetics for the general public. He managed large-scale R&D programs at Sick Kids Hospital, Toronto. He advised Bridgepoint and Mount Sinai hospitals on the implementation of personalized medicine programs. Dr. Dorfman has published thirty peer-reviewed papers on the genetics of Cystic Fibrosis and Pain.
What you should know about antidepressants
Ekaterina Kushnir
treats anxiety disorder
I have generalized anxiety disorder.
For a long time I coped without pills and other help, but one day I got tired of constant anxiety and began to interfere with my normal life. As a result, I turned to a private psychiatrist.
The doctor prescribed an antidepressant from the SSRI group - these are selective serotonin reuptake inhibitors. Such drugs are the first thing prescribed in the treatment of depression and a number of other conditions, including my illness. nine0003
The doctor immediately warned me about some peculiarities associated with taking the drug. Some of them I then felt on myself. I think everyone who plans to be treated with antidepressants should know about them.
At the same time, it should be taken into account that most of the negative effects of therapy are temporary and not dangerous, and if they do not go away, one medicine can be replaced with another. Antidepressants help many people with mental disorders and other illnesses get rid of their symptoms and return to a full life, so you definitely should not be afraid of them. The main thing is to take such drugs when they are really needed: as prescribed by a competent doctor and under his control. nine0003
See a doctor
Our articles are written with love for evidence-based medicine.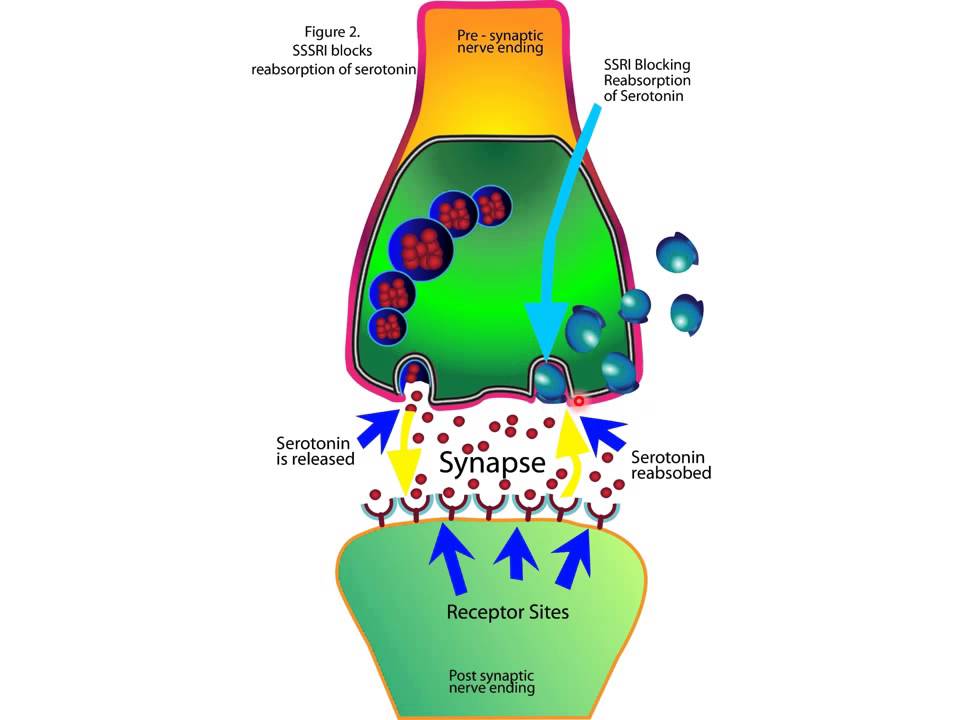 We refer to authoritative sources and go to doctors with a good reputation for comments. But remember: the responsibility for your health lies with you and your doctor. We don't write prescriptions, we make recommendations. Relying on our point of view or not is up to you.
We refer to authoritative sources and go to doctors with a good reputation for comments. But remember: the responsibility for your health lies with you and your doctor. We don't write prescriptions, we make recommendations. Relying on our point of view or not is up to you.
Fact No. 1
Antidepressants may make symptoms worse at firstAntidepressants can increase anxiety in anxiety disorders, as well as cause irritability and agitation - this is the name for causeless motor arousal, the inability to sit still. It's not dangerous, but rather unpleasant. This condition is sometimes referred to as initial anxiety, that is, the anxiety of starting therapy. Up to 65% of people face it. nine0003
Antidepressant-induced anxiety syndrome - a systematic review in the British Journal of Psychiatry
There is also evidence that some classes of antidepressants, including SSRIs, may increase suicidal ideation in depression in young people aged 18 to 24 years. These data are not very reliable, and in older people, the risk of suicide no longer increases and even decreases.
Without treatment, depression is more likely to lead to suicidal thoughts, and in case of anxiety, you just need to prepare for such an effect, then it will be easier to survive the attacks. nine0003
The doctor told me that in the first two or three weeks there may be an increase in anxiety, but I did not take it too seriously.
Everything was fine for the first week. After about seven days, I became nervous and irritable. And then I woke up at night and after a while I felt an incomprehensible fear. My heartbeat increased, my head was spinning, my throat was constricted. Because of this, I felt a real panic - I spent the rest of the night fighting terrible thoughts, in the morning I got up completely broken. nine0003
/list/antidepressant-myths/
8 myths about antidepressants
I have never had such panic attacks before medication - my anxiety was background, general. I got scared and wrote to the doctor, who reassured me and said that it was not dangerous and would pass soon.
After that, I already expected these panic attacks, immediately tried to relax, calm down, remember that this was just a temporary effect of the drugs. And they ended faster, and then they completely disappeared.
My letter to a psychiatrist. I was scared: I expected an increase in background anxiety, but not panic attacks. I even thought about giving up the medicineFact No. 2
The effect of antidepressant treatment will not be immediateIncrease the dose of antidepressants gradually to reduce side effects. They usually start with the minimum, and then bring it up to the working one. For example, for SSRIs with the active ingredient "sertraline", the working dose is from 100 mg per day. I started taking such a drug with 25 mg, and then gradually, in several steps, under the supervision of a doctor, raised the dose to 100 mg.
SSRI dosage - NHS
What doses of antidepressants will be optimal - an article in The Lancet
The process of reaching a working dose can take from two weeks to a month or more. It depends on the drug and its tolerance. I turned out to be sensitive to the medicine, it was hard for me to survive every increase in dosage: anxiety increased again, there were other side effects that then stopped. However, this is not the case for everyone, sometimes the process goes faster.
It depends on the drug and its tolerance. I turned out to be sensitive to the medicine, it was hard for me to survive every increase in dosage: anxiety increased again, there were other side effects that then stopped. However, this is not the case for everyone, sometimes the process goes faster.
The full therapeutic effect, that is, the disappearance or a strong improvement in the symptoms of the disease, occurs some time after reaching the working dosage. As a rule, this is a week or two, although some positive changes may be earlier. For some people, this process stretches for a longer period: 6-12 weeks. Minimum initial doses of drugs usually do not work. nine0003
It is better to prepare for the fact that the symptoms of the disease will not disappear in the first weeks of treatment. And remember - this does not always mean that the drug needs to be changed, sometimes you just need to wait or further increase the dosage under the supervision of a doctor.
Fact No. 3
3
Another way to mitigate the side effects of antidepressants is to prescribe an additional drug along with them: for example, from the group of tranquilizers. Such drugs may have their own side effects, they should not be taken for a long time. Unlike antidepressants, some of them can be addictive. They are usually appointed for a month, but this period may be shorter or longer. nine0003
Antidepressants together with benzodiazepines work better for depression - BMJ magazine
My doctor prescribed a rather mild drug for me. However, he did not suit me. At first, it caused increased drowsiness: during the period of increased anxiety, it went away for a while, but then returned - even with half a pill I turned off and could sleep all day. And if I drank at night, I woke up with difficulty in the morning. The psychiatrist prescribed another medicine, but I could not buy it: the drug was not available in any pharmacy nearby. nine0003
nine0003
As a result, I simply endured all the side effects of therapy - they were unpleasant, but tolerable. When discussing with the doctor, she called this option acceptable if the side effects of the second medicine only worsen the situation.
My prescriptions for drugs. I never used one, because there was no such medicine in pharmaciesFact No. 4
Side effects are not always, but they areModern antidepressants, including SSRIs, are mild and have almost no side effects. Older drugs - tricyclic antidepressants and monoamine oxidase inhibitors - cause more side effects. Doctors usually use them when milder first-line drugs don't work or when they can't be prescribed. nine0003
Side effects of antidepressants - the National Health Service of the UK
Side effects of various antidepressants - Uptodate
Side effects of antidepressants and their impact on the treatment of a large depressive disorder - the journal NATURE
STRICTIC STRICTION OF REDICAL
.![]() effects of antidepressants - advice from the Mayo Clinic staff
effects of antidepressants - advice from the Mayo Clinic staff
Choosing an SSRI drug does not guarantee the absence of side effects - many people tolerate treatment easily, but sometimes a change in drug may be necessary. nine0003
The first couple of weeks of taking there is a risk that the state of health will be so-so - it's worth thinking about. It may be worth scheduling the start of therapy on vacation.
I work remotely, and it was easier for me: the first pill was taken on Saturday, I slept through the weekend. Then she continued to work, but refused any additional loads: housework, part-time jobs, training and everything else.
It was hard work: I wanted to sleep, then I began to worry and get distracted. I also had diarrhea, nausea, headaches, tremors, i.e. hand trembling, hot flashes, sweating, palpitations. At night, panic attacks began, in the morning I had difficulty getting up because I was in pain and dizzy. nine0003
There are mixed data on how common the side effects of antidepressants are. If we summarize them, then the numbers look something like this:
If we summarize them, then the numbers look something like this:
- nausea - about 25% feel it;
- diarrhea - it happens in 15% of people, and 5%, on the contrary, will have constipation;
- sweating and a feeling of heat occur in about 20% of people;
- sexual dysfunction, decreased libido may occur in 80% of cases;
- insomnia - in 11% of cases;
- headache and dizziness - in about 10-11% of cases; nine0100
- weight gain - not all drugs give this effect. Some, on the contrary, can reduce weight. On my medicine, I lost 2 kilograms in the first month, despite the fact that I quit training due to poor health. True, then they returned back.
It can be seen that most side effects occur in less than half of the cases. In addition, in most cases they pass in the first weeks and are not dangerous.
Side effects not listed above are very rare. I was "lucky", and I faced one such - a decrease in visual acuity. Once in the morning I noticed that I see worse without glasses. A little later, I realized that something was wrong with the glasses. nine0003
I was "lucky", and I faced one such - a decrease in visual acuity. Once in the morning I noticed that I see worse without glasses. A little later, I realized that something was wrong with the glasses. nine0003
I wrote to the doctor, she replied that this happens, as a rule, is not dangerous and passes, but it is better to visit an ophthalmologist. I went to the ophthalmologist, everything was fine with my eyes, there was nothing terrible, but my vision really worsened - it was not a subjective feeling. On the right eye, it was -0.5 diopters, it became -0.75, and on the left eye it was -1.5, and it became -3.5.
I was offered to try changing the drug, but I decided to wait. Vision was then restored. I have not yet gone to the doctor to have it measured, but according to subjective feelings, it is at the same level as before: I am comfortable again in my glasses. nine0003
Side effects should not be tolerated - if something greatly worries, scares or interferes with life, it is better to tell the doctor right away. The psychiatrist will be able to determine whether the side effect of the drug is dangerous and whether it is worth continuing to take it. There are several antidepressants of the SSRI group, in addition, there are groups of drugs with a slightly different mechanism of action. As a rule, doctors manage to find a medicine that gives a good effect without side effects.
The psychiatrist will be able to determine whether the side effect of the drug is dangerous and whether it is worth continuing to take it. There are several antidepressants of the SSRI group, in addition, there are groups of drugs with a slightly different mechanism of action. As a rule, doctors manage to find a medicine that gives a good effect without side effects.
If there is no danger, the doctor can adjust the dose or increase it more gradually - this often helps to cope with unpleasant effects. nine0003 I wrote to the doctor again when my visual acuity decreased
Fact No. 5
Antidepressants need to be taken long termAntidepressants are not drugs that you can stop drinking as soon as you get better. They are taken for a long time: usually from several months, less often several years.
Anxiety Therapy - UpToDate
For example, for generalized anxiety disorder, the duration of treatment is at least a year. Moreover, the date is not counted from the very beginning, but from the moment when a lasting effect appeared from the pills. In fact, they will have to be drunk for about 1.5 years - it depends on how long it takes to reach the working dosage of the medicine. nine0003
In fact, they will have to be drunk for about 1.5 years - it depends on how long it takes to reach the working dosage of the medicine. nine0003
The cost of a package of the most famous antidepressant "Zoloft" is about 700 R, enough for about a month. That is, a course of therapy will cost about 10,000 R - maybe more or less, depending on which drug is selected.
Psychotherapy review - UpToDate
Another drug of the same group already costs more than 2000 R per pack. Source: rigla.ruThe cost of an appointment with a good psychiatrist in Moscow is 3000-5000 R. At first, you will need to visit him about once every 1-1.5 months, then less often. nine0003
You can apply to the psycho-neurological dispensary at the place of residence under compulsory medical insurance - it's free. At the same time, they will not put you on psychiatric registration: it was canceled in 1993. People with disorders that do not threaten their lives or those around them are on consultative and diagnostic care. If you stop going to the doctor, he will not find out what happened: a person seeks help at will.
If you stop going to the doctor, he will not find out what happened: a person seeks help at will.
Psychotherapy, usually cognitive-behavioral, is also commonly prescribed to enhance and sustain the effects of antidepressants. In many cases, it improves the effectiveness of drugs, including depression and generalized anxiety disorder. An appointment with a psychotherapist in Moscow costs an average of 5000 R. For treatment, you will need about 10 sessions or more. nine0003
/psychotherapy/
How psychotherapy works
Fact No. 6
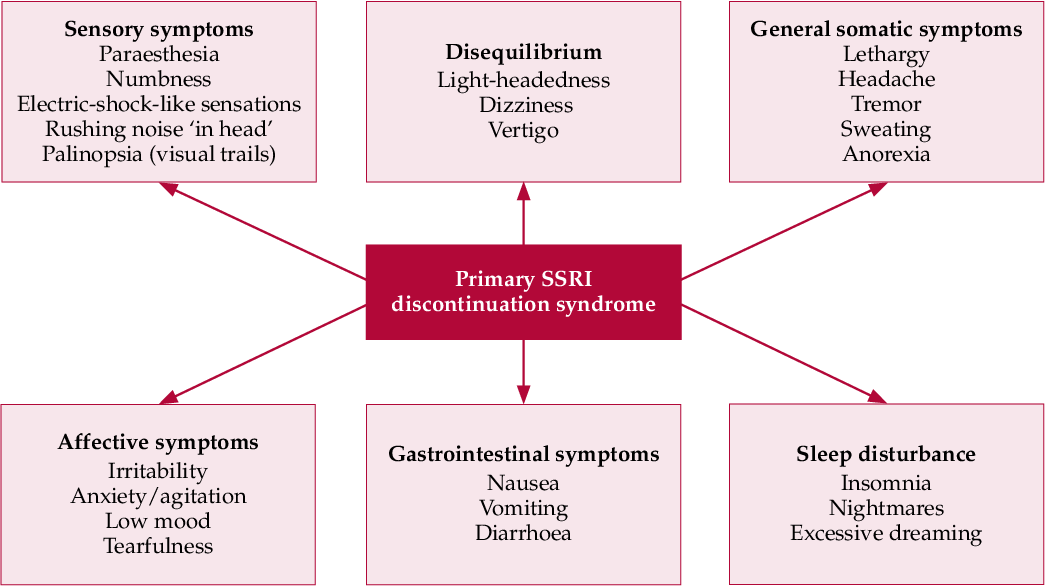
Antidepressants should not be stopped abruptly Antidepressants do not develop dependence. However, if you abruptly stop drinking them, there will be a withdrawal syndrome. This is felt as electric current discharges while moving or turning the head, headaches, dizziness, insomnia. Many people experience symptoms similar to the flu or an intestinal virus: low fever, diarrhea, general malaise, chills. Often there is anxiety, there are intrusive images. nine0003
Often there is anxiety, there are intrusive images. nine0003
Withdrawal symptoms after taking serotonin reuptake inhibitors - Journal of Clinical Psychiatry
How difficult it is to stop taking antidepressants - American Psychological Association
Stopping antidepressants in adults - UpToDate
treatment, they should be canceled only under the supervision of a doctor.
Antidepressant withdrawal occurs as gradually as the start of treatment. The dosage is slowly reduced, usually at this time again a cover-up drug is prescribed to alleviate side effects. As a rule, this is the same medicine that was at the beginning of the intake. nine0003
Withdrawal is usually harmless and resolves within the first weeks of stopping the drug. Sometimes even within a few days - it still depends on which medicine was prescribed. If severely disturbing symptoms appear during the withdrawal period, you should consult a doctor.
Fact No. 7
If you need to change the drug, everything will start over It is far from always possible to immediately find the right antidepressant - sometimes the side effects do not go away and you need to take a new one. nine0003
nine0003
Changing antidepressants in adults - UpToDate
Serotonin syndrome - MSD
Most often, it is started again with a small dosage, this delays the process of obtaining the effect of treatment. The new drug may also have side effects - the same or different. We will have to wait again until they pass.
You won't be able to change the drug on your own, since all antidepressants are sold only by prescription - and that's good. Switching from one drug to another can be dangerous if you do not know the characteristics of different groups of drugs. nine0003
For example, taking SSRIs is possible only some time after the withdrawal of antidepressants from the group of monoamine oxidase inhibitors - due to the risk of developing serotonin syndrome. This is a potentially fatal condition, accompanied by a change in mental state, high fever, increased muscle tone and other symptoms.
If the drug is changed correctly, there will be no dangerous negative effects, so consultation with a doctor is required.
/psychotherapy-search/
How to choose a psychotherapist
Fact No. 8
Among antidepressants there are original drugs and genericsPreparations may be original or generic. Originals are medicines first released by some pharmaceutical company that have passed all clinical trials and checks. Generics are drugs with the same active ingredient from another pharmaceutical company, that is, copied from the original drug.
Theoretically, the action of generics should not differ from the action of original drugs. However, this is possible, since generics may contain other additional substances or the manufacturer may use other raw materials. nine0003
Due to my anxiety, I did not read anything in detail about specific drugs before I bought my first antidepressant in a pharmacy so as not to be scared and not think about taking it. I also didn’t think to ask the doctor about this question.
/list/covid-depression/
Psychoneurological complications after covid: memory problems and depression
As a result, I first bought a generic because it was in stock. Then it turned out that, after all, according to the experience of my psychiatrist, the original drug often gives fewer side effects and is better tolerated. As a result, I changed the generic to the original drug - and, indeed, the side effects softened. nine0003
Then it turned out that, after all, according to the experience of my psychiatrist, the original drug often gives fewer side effects and is better tolerated. As a result, I changed the generic to the original drug - and, indeed, the side effects softened. nine0003
In my subjective opinion, which is supported by some data, in the case of antidepressants and other psychotropic drugs, you should always choose the original medicine. Moreover, the cost of originals and generics does not always differ greatly.
Originals and generics of some SSRIs
| Active ingredient | Original | Original cost | Generics | Cost of generics |
|---|---|---|---|---|
| Sertraline | Zoloft | About 700 R, 100 mg tablets | Serenata, Sirlift | 500-600 R 100mg tablets |
| Escitalopram | Cipralex | 3000 R, tablets 10 mg | "Selektra", "Elycea" | 500-1300 R 10 mg tablets |
| Fluoxetine | Prozac | About 350 R, 20 mg tablets | Profluzak, Fluoxetine | 100-200 R, tablets 20 mg |
CERTRALIN
Original
"Zoloft"
Original cost of the original
about 700 r, tablets 100 mg
Generies
"Serenata", "Cerelift"
The cost of Jeeneriki
9000 500-600 r. , tablets 100 mg
, tablets 100 mg Escitalopram
Original
Cipralex
Original cost
3000 r, tablets 10 mg
generics
“Chektra”, “Elice”
The cost of generics
500-1300 r, tablets 10 mg
Fluoxetine
“Przak”
cost
cost cost
Cost cost cost original
About 350 R, tablets 20 mg
Generics
Profluzak, Fluoxetine
Cost of generics
100—200 R, tablets 20 mg
one remained unclaimedFact No. 9
Do not take alcohol along with antidepressantsDrinking alcohol while taking antidepressants may exacerbate unpleasant side effects. Also, alcohol is a depressant, that is, it has the opposite effect, and its intake can adversely affect the results of treatment.
Why you shouldn't mix antidepressants and alcohol - Mayo Clinic
Alcohol is strictly forbidden to drink with some groups of antidepressants, for example, tricyclic antidepressants and monoamine oxidase inhibitors: combination with the latter, for example, can lead to an uncontrolled increase in pressure.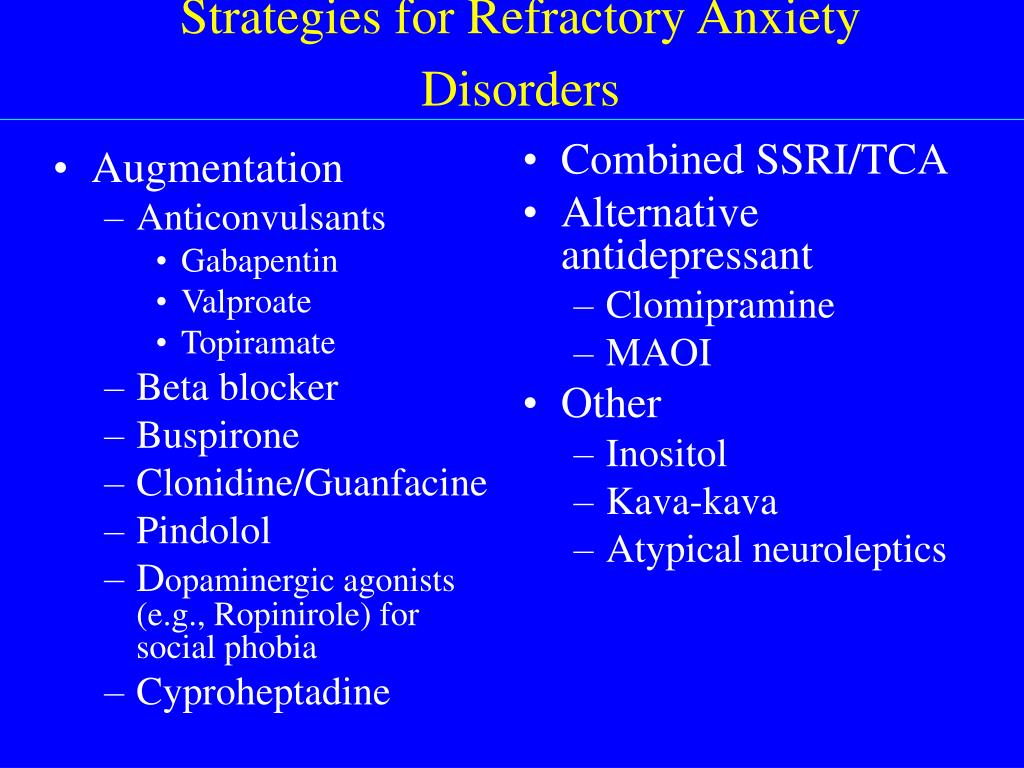 MAO inhibitors in general require a special diet - it is unlikely that a doctor will prescribe such drugs as the first antidepressants, but if necessary, he will issue a list of what is allowed and prohibited. nine0003
MAO inhibitors in general require a special diet - it is unlikely that a doctor will prescribe such drugs as the first antidepressants, but if necessary, he will issue a list of what is allowed and prohibited. nine0003
With other antidepressants, moderate use may not be dangerous and may even pass without consequences, but doctors still recommend abstaining so as not to increase side effects and improve treatment outcome.
The main thing is not to temporarily stop taking the drug in order to drink. This can lead to the development of a withdrawal syndrome.
/trevoga/
How I Treated Generalized Anxiety Disorder under CHI
Fact No. 10
Antidepressants are incompatible with certain drugs and have contraindications nine0017 It is important to tell your doctor what medications you are taking and what chronic illnesses you have. For example, SSRIs may not be suitable for epilepsy and bleeding disorders, and tricyclic antidepressants are usually not prescribed to those who have recently had a heart attack, suffer from glaucoma or porphyria.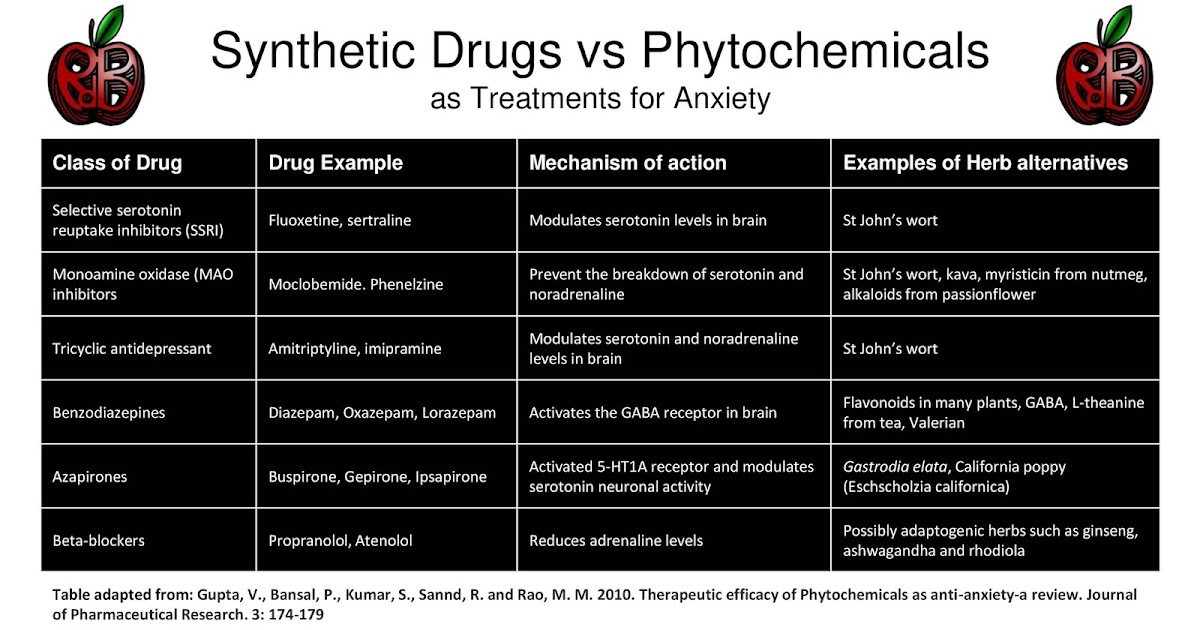
Antidepressant Warnings - NHS
Drug Compatibility Test - Drugs.com
It is also important to be careful if you are about to take any over-the-counter medicine. For example, ibuprofen, which people often take on their own to relieve pain and reduce fever. It should not be taken with SSRIs as it increases the risk of gastrointestinal side effects.
If it is not possible to consult a doctor before taking any medication, carefully read the instructions for it and your antidepressant. It is also worth informing all doctors who prescribe something to you during the therapy period about taking antidepressants. nine0003
Initial anxiety syndrome - practical recommendations
Summary. When prescribing antidepressant drugs, approaches should be used that minimize the increase in anxiety symptoms
An increase in the severity of symptoms of anxiety, agitation and irritability during the initial period of taking antidepressants is considered quite common, especially in the treatment of anxiety disorders. Often this phenomenon is presented as an explanation for the ineffectiveness of the early period of therapy, as well as a subject of particular concern when using antidepressants of the class of selective serotonin reuptake inhibitors (SSRIs). At the same time, there is clearly not enough convincing data for such conclusions. nine0003
Often this phenomenon is presented as an explanation for the ineffectiveness of the early period of therapy, as well as a subject of particular concern when using antidepressants of the class of selective serotonin reuptake inhibitors (SSRIs). At the same time, there is clearly not enough convincing data for such conclusions. nine0003
A systematic review of 107 scientific publications in 2009 by scientists from the Department of Psychopharmacology at the University of Bristol, UK found that there is no reliable information on the stable incidence of this phenomenon when using SSRIs compared with tricyclic antidepressants, as well as the greater frequency of increased anxiety symptoms in the treatment of anxiety disorders specifically. The frequency of this phenomenon, according to publications, varied within 4–65%. Common management of this syndrome, according to the review, included slower titration of antidepressant doses and additional use of drugs of the benzodiazepine class. Convincing data on the effectiveness of this therapeutic tactic has not been identified. Conflicting results have been obtained regarding the assessment of this syndrome as a predictor of response to therapy and the effectiveness of further treatment. Thus, the syndrome of increased anxiety in the initial period of antidepressant therapy remains not fully understood. nine0003
Conflicting results have been obtained regarding the assessment of this syndrome as a predictor of response to therapy and the effectiveness of further treatment. Thus, the syndrome of increased anxiety in the initial period of antidepressant therapy remains not fully understood. nine0003
A 2011 retrospective cohort study by scientists at Duke University Medical Center, North Carolina, Durham, USA found that only about 3% of patients exhibit symptoms of clinically significant anxiety during the 12-week initial period antidepressant therapy. It was also revealed that women, as well as patients aged <65 years, are more prone to the manifestation of these symptoms.
Recommendations to clinicians on the best therapeutic approach to address this problem are provided by Dr. Sarah T. Melton, Associate Professor of Pharmacy Practice, Gatton College of Pharmacy, East Tennessee State University, Tennessee, USA ). nine0003
SSRIs or serotonin and norepinephrine reuptake inhibitors are most often used as first-line drugs in the treatment of depressive and anxiety disorders. Treatment with the use of drugs of these classes can take up to 4 weeks before clinical improvement occurs in the patient's condition. In the period preceding the achievement of a therapeutic effect, symptoms of increased anxiety may appear. This increase in anxiety symptoms is called the initial anxiety syndrome and is often cited as a reason for early discontinuation of therapy. As indicated above, there are no standardized approaches to the treatment of this syndrome, as a result of which there is an insufficient amount of reliable data regarding the effectiveness of a particular therapeutic strategy. nine0003
Treatment with the use of drugs of these classes can take up to 4 weeks before clinical improvement occurs in the patient's condition. In the period preceding the achievement of a therapeutic effect, symptoms of increased anxiety may appear. This increase in anxiety symptoms is called the initial anxiety syndrome and is often cited as a reason for early discontinuation of therapy. As indicated above, there are no standardized approaches to the treatment of this syndrome, as a result of which there is an insufficient amount of reliable data regarding the effectiveness of a particular therapeutic strategy. nine0003
An increase in anxiety levels and a deterioration in general mental state can contribute to an increase in suicidal thoughts and behavior. In a study in which the level of anxiety was studied in patients after a single use of citalopram, it was found that the use of the drug can increase the severity of an existing anxiety disorder, but does not have an anxiogenic effect in patients with an initial absence of anxiety disorders.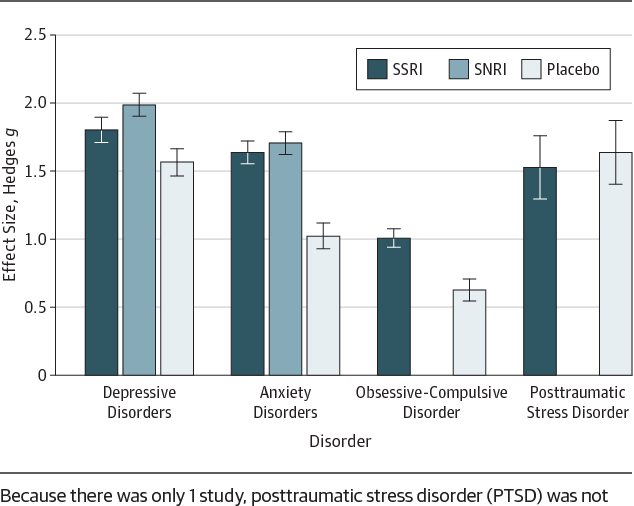 In a study involving patients with depressive disorders treated with SSRIs, it was found that an increase in anxiety during the initial period of therapy was recorded in 15% of cases. nine0003
In a study involving patients with depressive disorders treated with SSRIs, it was found that an increase in anxiety during the initial period of therapy was recorded in 15% of cases. nine0003
Therapy of initial anxiety syndrome can cause certain difficulties, however, there are certain approaches that make it easier for the doctor to prevent its development or minimize the clinical severity of this unwanted symptomatology.
In patients with anxiety disorders, especially those with panic attacks, treatment should be started with low doses of antidepressants, increasing doses according to the patient's clinical tolerance. Patients with panic attacks are very sensitive to the anxiogenic effects of antidepressant drugs, but the severity of the initial anxiety syndrome can be minimized by using initial doses of drugs that are 25-50% of the normal starting dose for treatment of depression. This approach is acceptable for most patients. Daily doses used in the treatment of anxiety disorders are often slightly higher than those used in the treatment of depression, especially in the case of obsessive-compulsive disorders. Doses should be titrated slowly over several weeks until a therapeutic effect is achieved. nine0003
Doses should be titrated slowly over several weeks until a therapeutic effect is achieved. nine0003
Benzodiazepine drugs, such as clonazepam or lorazepam, can be used concomitantly to relieve anxiety symptoms. The rapid onset of the anxiolytic effect makes it possible to consider drugs of this class as the best option for minimizing the severity of the initial anxiety syndrome. Limitations regarding their use include a minimal positive effect on the depressive state of patients, a negative effect on cognitive functions, and a high risk of developing drug dependence. Patients with a history of alcohol dependence should not be given benzodiazepines. nine0003
Benzodiazepines should be used during the first 2-3 weeks of antidepressant therapy in patients who require rapid resolution of anxiety symptoms before antidepressant therapeutic effect occurs. Patients who are prescribed benzodiazepines should be informed about the limited course of treatment with these drugs and the need to stop it after the first 2-3 weeks of treatment.
The use of β-adrenergic blockers may provide some reduction in the severity of anxiety symptoms induced by antidepressants. There is evidence of a decrease in the level of anxiety and anxiety with the additional use of propranolol in patients receiving fluoxetine. nine0003
In symptomatic therapy for anxiety symptoms, the drug hydroxyzine, a blocker of H 1 histamine receptors, can also be used. This drug does not have a risk of developing drug dependence, but its sedative effect is much more pronounced compared to benzodiazepine drugs. Due to anticholinergic side effects, hydroxyzine should not be used in elderly patients. The evidence base for its effectiveness when used in patients with initial anxiety syndrome on the background of antidepressant treatment is insufficient, this drug is indicated for the treatment of generalized anxiety disorders, however, it is often prescribed at the primary level of medical care for the relief of acute symptoms of anxiety. nine0003
Titration of antidepressant doses and the use of adjuvant drugs are acceptable and effective methods of preventing the development and/or relief of initial anxiety syndrome associated with the initiation of antidepressant therapy.