Neuropsychological testing for add
Understanding Neuropsychological Testing for ADHD, Learning Disability Diagnosis & More
Understanding Neuropsychological Testing for ADHD, Learning Disability Diagnosis & More
February 5, 2019|ADHD
What is neuropsychological testing?
A useful tool for accurately diagnosing ADHD, learning disabilities, a neuropsychological evaluation is a comprehensive assessment of cognitive and behavioral functions using a set of standardized tests and procedures, utilizing paper and pencil, question and answer, and computer-based tests. Neuropsychological testing is also used to assess other cognitive problems that can result from brain injury, neurological, medical, or emotional conditions. We offer testing for adolescents (16+) and adults in Boston and Newton, MA.
On This Page
- What is neuropsychological testing?
- How long do I have to wait for an appointment?
- What’s the difference between a neuropsychologist and a psychologist?
During testing, a broad range of functions may be assessed, such as intelligence, problem-solving, language, organizational skills, memory, learning, attention, emotion regulation, and more.
Based on the findings, treatment plans and recommendations can be created to help improve functioning in daily life.
How long do I have to wait for an appointment?
Because we are a private practice with a large neuropsychology team, we can generally see new neuropsychological testing clients within 2-3 weeks in our Newton and Boston, MA offices. This is a vastly different wait time than at major hospitals in the Boston area, which often have wait times of 6-8 months. Request an appointment.
What’s the difference between a neuropsychologist and a psychologist?
Neuropsychologists and psychologists have different training. Psychologists are trained to evaluate, diagnose, and treat psychological diagnoses. Neuropsychologists are specially trained to evaluate brain functioning. Neuropsychologists are trained in specific knowledge of clinical neuropsychology, neuroanatomy, and brain-behavior relationships. Our neuropsychologists have all completed an APA-approved internship in neuropsychology and have completed a specialty post-doctoral residency in clinical neuropsychology.
To request an appointment, click here or call us at (781) 551-0999.
Related Posts
Child & Adolescent Therapy Available in Boston
October 30, 2019|ADHD
Commonwealth Psychology Associates® (CPA) has recently expanded child & adolescent behavioral health services into our North Station office, located…
Read More
Part Two: Managing ADHD in Children
July 10, 2018|ADHD
By Riikka Melartin, Psy.D. In part two, I will detail some basic strategies that can be helpful at home if…
Read More
Welcoming New Clinicians, Continued!
August 9, 2016|ADHD
Last week we welcomed Drs. Crowe, Tecce, and Khaira to the clinical team at CPA. This week we are thrilled to introduce two more clinicians who are providing services at our new Newton-Wellesley office.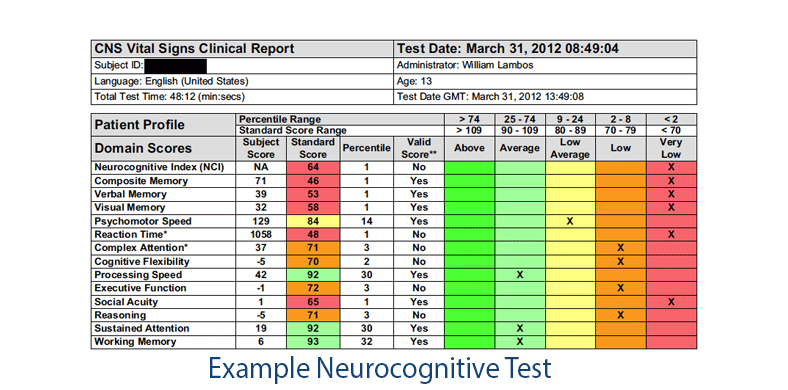
Read More
All contents © 2023 Commonwealth Psychology Associates®, LLC. All rights reserved. • Sitemap • Website Design by Jackrabbit Privacy Policy
How do neuropsychologists diagnose ADHD?
Written by Dr. Nicole M. Vienna
December 23, 2021
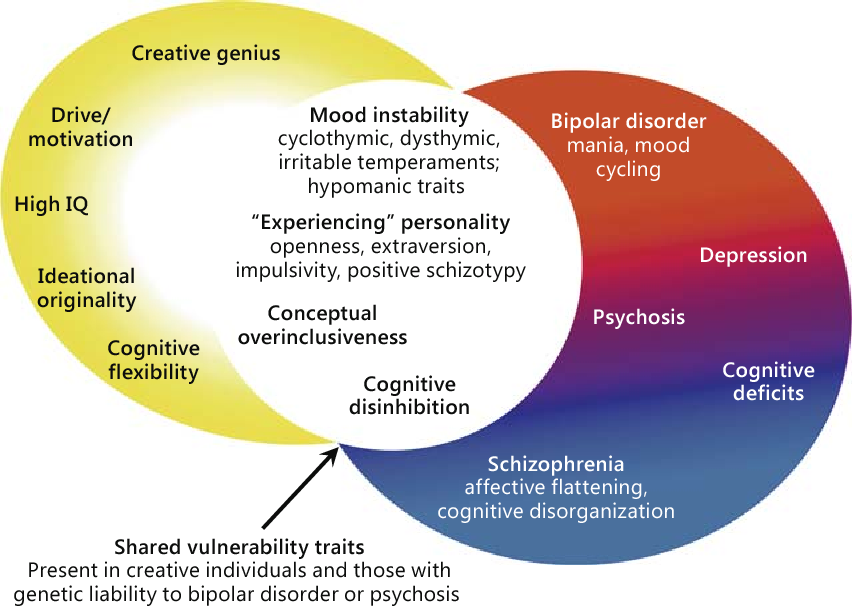
Contrary to popular belief, there is no single test or checklist for diagnosing ADHD. Indeed, it is a complex neurobehavioral diagnosis and often misdiagnosed. To that end, ADHD shares many symptoms with other disorders, such as PTSD, personality disorders, anxiety, bipolar disorder, and depression. This article will give you a brief overview of the ADHD criteria, adults and ADHD, a neuropsychological approach to ADHD, and ADHD’s interaction in juvenile delinquency.
According to the DSM-5, ADHD is considered a neurodevelopmental disorder because symptoms begin in the developmental period. Individuals with ADHD have a persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with life functioning. Inattentive symptoms can include:
Inattentive symptoms can include:
- Difficulty sustaining attention on tasks or play activities
- Does not seem to listen when spoken to directly
- Trouble organizing tasks and activities
- Easily distracted
- Forgetful in daily activities
- Fails to give close attention to details.
Hyperactivity-impulsivity symptoms can include:
- fidgets with hands, arms, or legs, or squirms in place
- leaves the seat when expected to remain seated
- talks excessively
- often on the go or acts as if they are driven by a motor
- interrupts or intrudes in conversations or games
- blurts out the answers
- unable to turn, take or play games quietly.
In addition, symptoms must have been present prior to age 12, present in two or more settings, and cause clinically significant distress or interfere with daily life functioning (work, school, relationships, etc.). Last, the symptoms cannot be better described by another disorder such as depression, anxiety, or a personality disorder.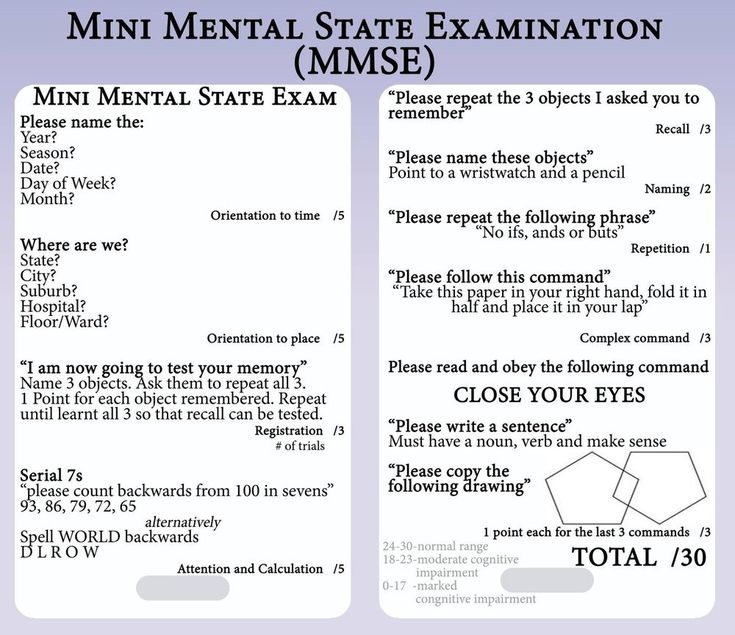
These symptoms can result in three different types of presentations:
- Predominately Inattentive Type– a qualifying number of inattentive symptoms are present for the last six months
- Predominately Hyperactive Type– a qualifying number of hyperactive symptoms are present for the last six months
- Combined Type– a qualifying number of both inattentive and hyperactive symptoms are present for the last six months
Brain Structure and ADHD
Numerous neuroimaging studies have found several morphological abnormalities in children’s brains with ADHD. Specifically, regional abnormalities include the reduced grey matter in the regions making up the frontostriatal circuits, atypical white matter volume in neural tracts (related to impaired communication between circuits), and cortical thinning. Still, over studies have found that ADHD is associated with reduced global brain volume. As such, ADHD is the result of complex abnormalities predominantly affecting the frontal lobes and other regions of the brain. In addition, it is important to note that genetic and adverse rearing association has been associated with reduced cortical volume in ADHD children. Thus, shining light on the role of parenting style and environmental influences on brain development.
In addition, it is important to note that genetic and adverse rearing association has been associated with reduced cortical volume in ADHD children. Thus, shining light on the role of parenting style and environmental influences on brain development.
Adults and ADHD
While it has been thought to only exist in childhood, ADHD symptoms and impairments can persist into adulthood. Adult prevalence rates are estimated at 2.5% (Simon, et al. 2009). Still, other studies have found that over 10 million adults have ADHD.
Neuropsychological Approach to ADHD
Neuropsychologists are specifically trained in brain functioning, neuroanatomy, and brain-behavior relationships. Therefore, when assessing for ADHD, a neuropsychologist may use a variety of standardized cognitive tests and behavioral questionnaires. Depending on potential co-occurring issues, an ADHD evaluation can be very narrow-focused or broadly assessed to rule out or confirm cofounding problems. The tested cognitive domains can include intelligence, memory, learning, attention, problem-solving, organizational skills, and emotional regulation. Once the data is analyzed, the clinician will write a succinct report, including treatment recommendations to help improve daily life functioning.
Once the data is analyzed, the clinician will write a succinct report, including treatment recommendations to help improve daily life functioning.
ADHD and Juvenile Delinquency
Children with ADHD have impairments that can result in various problematic behaviors that can get them mixed into the juvenile justice system. For example, their difficulties paying attention in class, excessive talking and disruption, inability to sit still, being unable to not be distracted (inattention problems), not being able to stop internal thoughts (impulsivity), or being unable to stop acting upon distractions and/or thoughts (hyperactivity) can get them into trouble with their parents or school officials which then can lead them into truancy and eventually dropping out altogether. And if these symptoms continue to go untreated, these children may turn to drugs/alcohol to self-medicate unremitted symptoms, thereby increasing their risk of poor decision making and asocial behavior and coming in contact with the legal system.
Also, children with ADHD may have problems with self-talk (our ability to talk to ourselves), sense of time (in that time can seem to go by very slow or very fast), and shifting from plan A to Plan B. Lastly, they are more likely than their peers to struggle with separating emotion from fact, again, increasing their risk of asocial behavior and engaging in behavior that is not well thought out.
Final Thoughts
ADHD is a complex neurobehavioral diagnosis that shares overlapping symptoms with bipolar disorder, PTSD, anxiety, depression, and even some personality disorders. While most thought to exist in children, some studies have shown upwards of 10 million adults have ADHD. A neuropsychological evaluation can help assess executive functioning systems among other cognitive domains implicated in ADHD. This includes standardized cognitive paper-pencil testing as well as behavioral and symptom questionnaires. Untreated or mismanaged symptoms can lead to self-medicating with drugs or alcohol, thereby increasing their risk of asocial behavior, which is not well thought out.
If you would like to learn more about ADHD, contact our office to speak with Dr. Vienna. Call us at (626) 709-3494.
NEUROPSYCHOLOGICAL TESTING of adults: to whom and why?
It must be admitted that people often take care of their health (especially mental health) or, even worse, keep silent about the violations that have appeared, for example, memory, for fear of getting a “diagnosis-sentence” that entails professional and social restrictions. Only when the memory begins to let down noticeably, the patient actively complains, as it is already impossible not to notice. But at the stage of pronounced disorders to the degree of dementia (dementia), these complaints come from the patient's family, while his criticism of his condition is noticeably reduced.
Timely consultation with a specialist will help to change or prevent this unpleasant scenario. Comprehensive diagnosis and analysis of the characteristics of the disease play a huge role in subsequent treatment. To do this, a doctor who deals with memory problems conducts neuropsychological testing - an objective assessment of the state of cognitive functions. This method allows you to monitor the patient in dynamics and see the effectiveness of the prescribed therapy.
To do this, a doctor who deals with memory problems conducts neuropsychological testing - an objective assessment of the state of cognitive functions. This method allows you to monitor the patient in dynamics and see the effectiveness of the prescribed therapy.
Who is eligible for neuropsychological testing?
People complaining about:
- worse memory than in the past;
- decrease in mental performance;
- problems with the choice of words in a conversation or with the formulation of one's thoughts;
- difficulty concentrating and concentrating;
- high fatigue during mental work;
- heaviness or feeling of "emptiness" in the head, strange sensations in the head;
- clumsiness or retardation in performing normal activities;
- deterioration of vision or hearing with a slight manifestation of diseases of the eye and organ of hearing or their absence;
- complications in interpersonal relationships, professional sphere, difficulties with everyday life and self-service.

Any of the above complaints, especially if it has appeared in recent years, is a good reason for an objective study of cognitive functions using neuropsychological testing.
How neuropsychological testing is done:
Tests consist of various tasks and exercises related to the memorization and pronunciation of words, recognition of drawn objects, the implementation of certain motor programs, tests for focusing and concentration. A comprehensive study provides the most accurate understanding of the type and degree of cognitive impairment, if any.
There are standard test kits (with a quantitative assessment of the results) that allow you to quickly see the picture of the disease in a limited time. Most often, the Mini-Cog technique is used, which includes the task of memorizing and reproducing three words and the clock drawing test. Its main advantage is in significant diagnostic informativeness with simultaneous ease and speed of implementation (up to 5 minutes).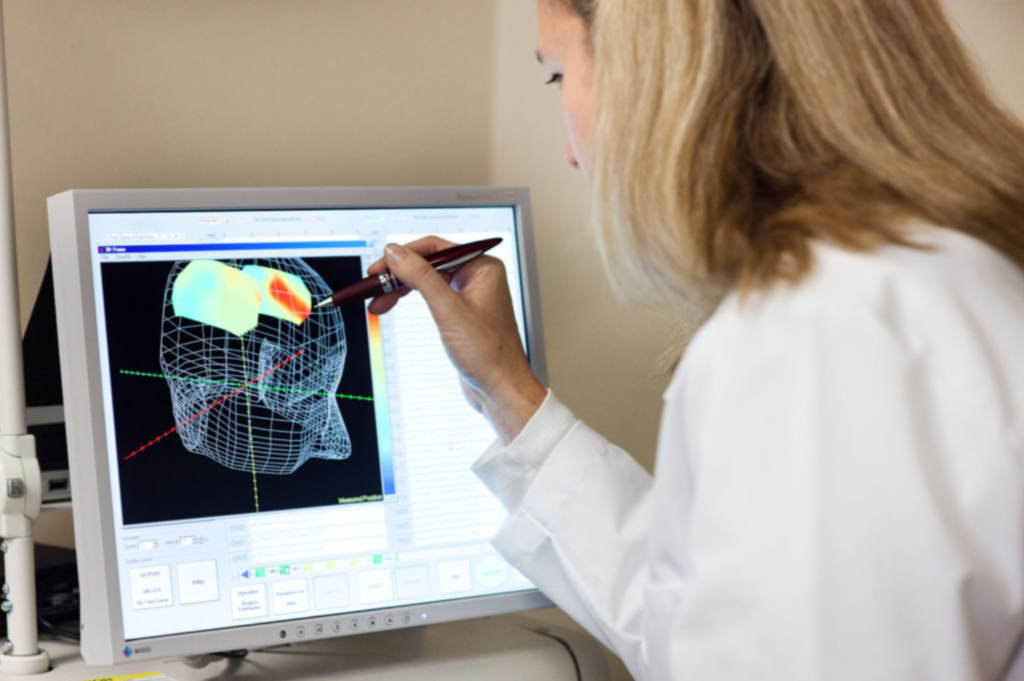
A longer (10-15 minutes) but more meaningful series of tests, the Montreal Cognitive Assessment Scale (MOCA test), assesses in detail each of the cognitive areas: memory, attention span, language, numeracy, executive function, abstract thinking , visual-spatial skills. There are a lot of tests that are diverse in their sensitivity and specificity (a short scale for assessing cognitive functions - MMSE, a battery of frontal dysfunction, etc.). The optimal test is selected by the doctor.
Analysis of the results of neuropsychological testing
Neuropsychological testing is the most accurate diagnostic method, but sometimes (rarely enough) it still gives distorted data. False-positive results occur when the patient scores low on tests, below normal for the appropriate age, in the absence of true cognitive impairment. There may be several reasons for this:
- illiteracy, low level of education and culture, long isolation from society;
- severe situational anxiety at the time of the test, situational lack of concentration and inattention;
- state of intoxication during the study or the day before,
- patient fatigue throughout testing or lack of night sleep before testing;
- indifferent, skeptical or hostile attitude towards testing.
There are also false negative results. Individuals with incipient symptoms of cognitive impairment or who choose a very difficult testing method show age-appropriate test scores despite cognitive decline in subject status. These patients should be monitored and neuropsychologically tested over time, as some of them will soon develop more severe symptoms.
In young people with active complaints of memory impairment, these sensations are a consequence of emotional disorders of an anxiety-depressive nature. Therefore, with negative results of neuropsychological testing, an in-depth study of the psychological state using special questionnaires is required.
Sometimes the cause of cognitive decline is severe weakness, fatigue, and “failure”. To identify asthenic syndrome, the specialist will also offer the necessary scales and questionnaires.
In addition to testing, a conversation with relatives is necessary. It allows you to determine the emotional background of the patient and his natural behavior. For example, how often can he not remember something from the past or from the planned, the content of the conversations; is there any forgetfulness of faces and names; whether there are difficulties with understanding addressed speech, errors in the selection of words or the construction of phrases; whether there are sudden difficulties with performing activities (cooking, cleaning, small household tasks, etc.). Relatives and friends can also provide information about how a person navigates in space and time, whether he has problems traveling, whether he remains sane, as before
For example, how often can he not remember something from the past or from the planned, the content of the conversations; is there any forgetfulness of faces and names; whether there are difficulties with understanding addressed speech, errors in the selection of words or the construction of phrases; whether there are sudden difficulties with performing activities (cooking, cleaning, small household tasks, etc.). Relatives and friends can also provide information about how a person navigates in space and time, whether he has problems traveling, whether he remains sane, as before
What does a neuropsychological test do?
After analyzing the patient's worries, talking with his relatives and obligatory objectifying them using neuropsychological testing methods, it is possible to draw a conclusion about one of the three degrees of severity of cognitive impairment, each of which has its own treatment algorithm, its own prognosis.
A mild form of cognitive impairment is characterized by rare and mild symptoms without functional limitations and invisible to others.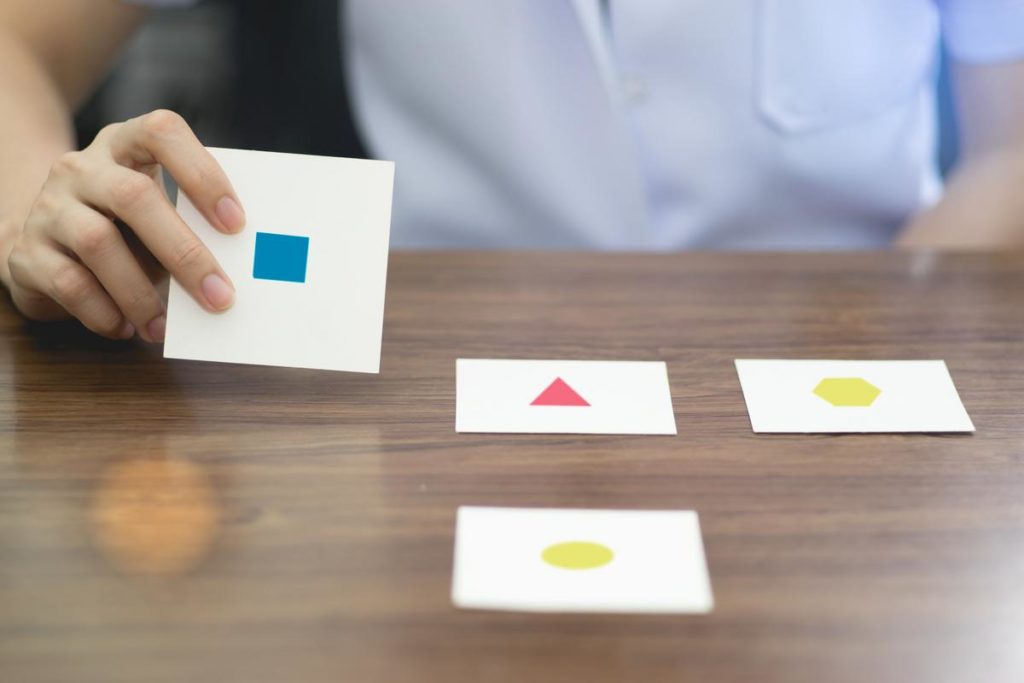 These are periodic forgetfulness, isolated cases of reduced concentration, fatigue during intense mental work, etc.
These are periodic forgetfulness, isolated cases of reduced concentration, fatigue during intense mental work, etc.
The moderate form is manifested by systematic or incessant symptoms, more noticeable, but with no or minimal severity of functional limitation. There is a slight but almost constant forgetfulness, regular difficulty with concentration, and fatigue occurs more often with daily mental activity. These changes are visible to both the patient and the environment. At the same time, a person remains independent and independent, fulfills his professional and social tasks, family responsibilities, etc. However, it will be quite difficult to figure out new or unusual areas of activity for him.
A severe form of cognitive impairment leads to various limitations in functioning, partial or complete loss of independence and autonomy. Such a patient requires specialized anti-dementia therapy, the tasks of which include slowing down the progression of the disease, improving the quality of life of the patient and those caring for him, and alleviating the burden of this disease on his relatives.
It is better not to delay a visit to a dementologist if you or your relatives have the slightest manifestation of cognitive impairment. Age is not to blame! Remember that the earlier the diagnosis is made, the more pronounced and lasting will be the effect of the recommended therapy.
Knyazkina Yuliya Alexandrovna – neurologist of the Health Center “Private Practitioner”, specialist in memory disorders (dementologist), headaches, sleep disorders and extrapyramidal pathology (parkinsonologist).
Epilepsy examination. Diagnosis of epilepsy in children and adults.
Without a full diagnosis of epilepsy in children and adults, it is impossible to correctly determine the characteristics of the nature of the disease and choose the optimal treatment tactics. In addition, it is important to exclude other problems. Since attacks of impaired consciousness can be caused not only by epilepsy, but also by other causes - for example, a traumatic brain injury or a brain tumor.
How to start diagnosing epilepsy in children and adults
According to the recommendation of ILAE (International League against Epilepsy), it is customary to start an examination for epilepsy with non-invasive methods - those that do not involve any surgical interventions in the body, injections, etc. .d.
First of all, it is obligatory to perform:
- Scalp video-EEG monitoring with registration of seizures. Electrodes are placed on the patient's head, which record the electrical activity of the brain. Provoking tests are used to identify brain dysfunctions - opening and closing the eyes, increasing the intensity of breathing, sound and light stimulation, etc.
Examination of epilepsy is carried out in an equipped ward under medical supervision and usually lasts from 2 to 10 days. The more frequent the attacks, the shorter the monitoring period. - MRI of the brain according to the epileptic protocol. The patient lies on a special movable table and is placed inside the tomograph, a device in the form of a cylindrical tube.
 It is important to detect even small structural changes in the brain. Therefore, the study takes from 1 to 1.5 hours. The patient is required not to move and breathe calmly.
It is important to detect even small structural changes in the brain. Therefore, the study takes from 1 to 1.5 hours. The patient is required not to move and breathe calmly.
In difficult situations, MRI is performed under anesthesia.
These types of diagnostics of epilepsy in adults and children show structural or electrophysiological changes - neuronal activity, anomalies in the development of the cerebral cortex, and others. However, it is not always possible to fully diagnose epilepsy only on the basis of MRI and video-EEG monitoring. Then an extended survey is required.
What do you do if the diagnosis of epilepsy using EEG and MRI does not reveal abnormalities?
Additional tests for epilepsy:
- Single photon emission computed tomography. At the first symptoms of an attack, a person is given a radiopharmaceutical. After some time, a tomography is performed. A similar procedure is repeated at rest. The results of the epilepsy examination are combined in a computer program - this allows you to determine the zone of the onset of an attack.

- Positron emission tomography with fluorodeoxyglucose (18F). The patient is injected intravenously with a radiopharmaceutical - it spreads through the tissues of the body and marks biologically active compounds. The study will allow assessing changes at the cellular level and identifying the disease at an early stage.
- Magnetoencephalography. The patient is placed in a scanner with sensors - they measure the magnetic field of the brain and its changes. The information obtained is close to the EEG data, but has a greater sensitivity.
- Neuropsychological testing. Meeting with a neuropsychologist, during which thinking and higher nervous functions of a person (memory, logic, etc.) are assessed. With this disease, long-term memory suffers the most.
Is there always enough information from non-invasive epilepsy tests?
Sometimes tomography, video-EGG monitoring, neuropsychological testing and additional diagnostic methods (PET, SPECT, MEG) cannot determine the epileptogenic zone.