Narcissistic personality disorder vs narcissism
The Narcissist Versus The Narcissistic Personality Disorder
Allan Schwartz, LCSW, Ph.D. was in private practice for more than thirty years. He is a Licensed Clinical Social Worker in the states ...Read More
Judging from email questions I have received, many readers are somewhat confused about the differences between people who are narcissistic versus those who have a narcissistic personality disorder. There is a large difference between the two. Let’s explore those differences:
Narcissistic Personality Disorder:
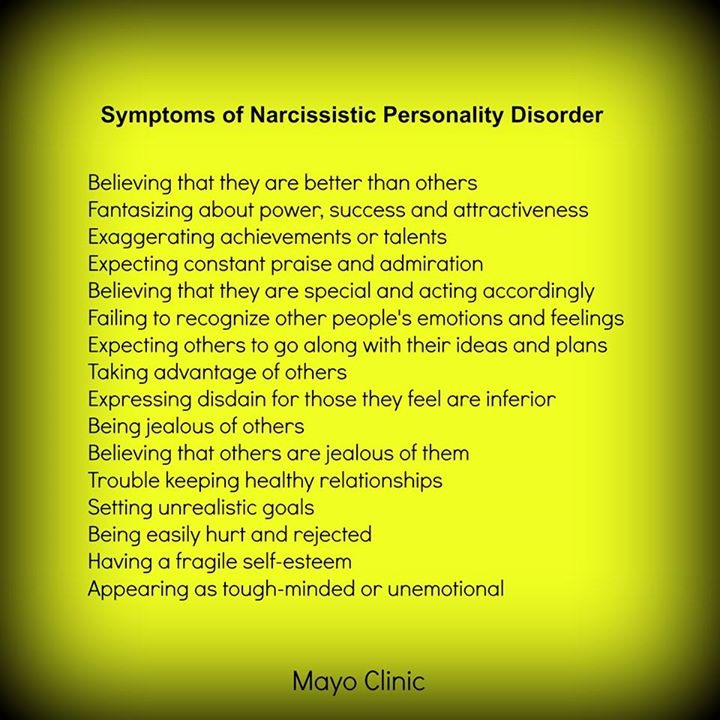
According to the Mayo Clinic “Narcissistic personality disorder is a mental disorder in which people have an inflated sense of their own importance and a deep need for admiration. Those with narcissistic personality disorder believe that they’re superior to others and have little regard for other people’s feelings. But behind this mask of ultra-confidence lies a fragile self-esteem, vulnerable to the slightest criticism.
”
This personality disorder causes people to misunderstand what is really going on with the individual. For example, some one like this will seem to be arrogant and filled with self-confidence. However, just beneath this shallow surface lies a person who feels a deep sense of shame and humiliation and low self-esteen. That is why they are so easily hurt in the face of criticism.
Explore Your Options Today
These are people who do not function well. They alienate friends and family and come to feel socially isolated and depressed. This is very difficult for them because they do not want to think anything is wrong. Narcissistic Personality Disordered people are caught between thinking they are superior and feeling miserable, all at the same time.
Narcissism:
There are people who are narcissistic but who do not have a mental illness. These people are experienced as obnoxious because they feel superior to others and see nothing wrong with that. They have little or no empathy with the feelings, conditions, situations or plight of others. These are people who feel entitled to the best of everything while looking down on those who show admiration for them. They also have no difficult exploiting others in order to get what they want. It’s important to understand that they have no awareness and no insight into what they do. As a result, they feel no shame or remorse.
These are people who feel entitled to the best of everything while looking down on those who show admiration for them. They also have no difficult exploiting others in order to get what they want. It’s important to understand that they have no awareness and no insight into what they do. As a result, they feel no shame or remorse.
It is said that, both in the present and historically, there have been leaders who were narcissists. Narcissists have a knack for getting into positions of power and have no difficulty exercising that power. Some of them exemplify evil in the world. Among these are Adolf Hitler, Joseph Stalin, Pol Pot and others. There are some who are successful in business because they have friends who help guide them. One example is Bill Gates, Larry Ellison and more.
It’s important to remember that the major distinction between the narcissist and the narcissistic personality disorder is that the narcissistic is not mentally ill, does not have a personality disorder and is most interested in gaining power, money and prestige. Too many narcissists succeed in their pursuits. There is no need to worry about the self-esteem of the narcissist, they have an over-abundance of it.
Too many narcissists succeed in their pursuits. There is no need to worry about the self-esteem of the narcissist, they have an over-abundance of it.
Your comments are welcome.
Allan N. Schwartz, PhD
Keep Reading By Author Allan Schwartz, LCSW, Ph.D.
Read In Order Of Posting
How to Tell the Difference
Narcissism exists on a spectrum. If you take accountability, have insight, and establish reciprocal relationships, you may have some narcissistic traits but not a personality disorder.
The concept of narcissism refers to a continuum where you may believe in your superiority and prioritize your needs, sometimes at the expense of others. These tendencies may be mild or situational, or they can become evident across most situations and persistently over time.
When narcissistic traits and behaviors span multiple areas of your life for an extended period of time, a therapist may formally diagnose narcissistic personality disorder (NPD).
Narcissism refers to a sense of self-importance. It can be seen as a personality trait that most people live with to some degree. This trait, as any other trait, exists on a spectrum.
At one end of the spectrum is what some refer to as healthy narcissism. This is considered a positive sense of self often associated with the greater good, says Dr. Kristi K. Phillips, a licensed psychologist in Wayzata, Minnesota.
“Individuals with healthy self-image can balance high self-esteem with prosocial behaviors that nurture reciprocal relational dynamics,” she explains.
At the other end of the spectrum, narcissism may negatively impact how you see and interact with yourself and the world.
Pathological narcissism can lead you to experience friction in relationships and great distress. When this becomes persistent in your life, it may lead you to receive a narcissistic personality disorder diagnosis.
In sum, on the spectrum of self-interest, healthy narcissism appears on one side. In the middle, you’ll have some narcissistic traits that range in severity. On the other side, there’s clinical narcissism, where you might find the most severe narcissistic behaviors that cut across multiple areas of your life.
In the middle, you’ll have some narcissistic traits that range in severity. On the other side, there’s clinical narcissism, where you might find the most severe narcissistic behaviors that cut across multiple areas of your life.
Clinical narcissism protects the ego using maladaptive coping strategies.
“It is characterized by authoritarianism, envy, grandiosity, shallowness, and a deficit of empathy and remorse. It tends to serve the individual with little or no respect for the greater good,” says Phillips.
For example, in a job interview, you may put down previous employers, embellish credentials and accomplishments, take credit for projects that weren’t yours, or make promises you can’t keep.
Narcissistic personality disorder is a formal condition listed in the reference guide that therapists use to make mental health diagnoses, called the Diagnostic and Statistical Manual of Mental Disorders, 5th edition, text revision (DSM-5-TR).
To receive an NPD diagnosis, a health professional will want to determine if you experience at least five of nine formal symptoms across different situations and persistently for more than 6 months.
These symptoms affect your relationships, occupation, sense of identity, and lifestyle. They may cause great distress whether you’re aware of it or not.
The nine formal symptoms of narcissistic personality disorder are:
- grandiosity or a sense of self-importance
- fantasies about power and success
- a sense of entitlement
- limited insight
- a constant need for admiration and praise
- use of manipulation tactics to take advantage of others
- limited or poor empathy
- competitiveness, distrust, and jealousy
- scorn and arrogance toward others
There are at least five types of narcissism, but only one recognized mental health diagnosis.
Personality traits involve patterns of thoughts and behaviors that may manifest in random situations. Narcissistic traits may show up once in a while at work, for example, when you firmly believe and act like you’re the best in your team.
Symptoms of a narcissistic personality, on the other hand, may point to a health challenge that may need professional support. Narcissistic symptoms may impact your quality of life because they appear in most situations.
Narcissistic symptoms may impact your quality of life because they appear in most situations.
Only a trained mental health professional can accurately diagnose narcissistic personality disorder or identify narcissistic traits.
Besides the main list of symptoms, these are other differences between narcissism and narcissistic personality disorder:
Accountability
“A fundamental difference between possessing narcissistic traits versus meeting a full diagnosis is that the person with NPD may not accept responsibility for their behaviors. Someone with narcissistic traits may be able to recognize and take ownership when hurting people they care about,” says Rachel Ann Dine, a licensed professional counselor in Chesapeake, Virginia.
Stability in relationships
Research shows that people with narcissistic personalities may use manipulation tactics and games to get others to do what they want.
“There is typically an exploitative component of the relationship, which can occur in any relational dynamic — romantic, familial, workplace,” says Dine. When someone is no longer considered useful or, perhaps, a threat, a person with NPD may be quick to discard them.
When someone is no longer considered useful or, perhaps, a threat, a person with NPD may be quick to discard them.
On the other hand, “A person who has narcissistic traits may be resistant to admitting faults or receiving constructive criticism, but does have the capacity to do so, albeit limited in some cases,” she explains.
Context and duration
“An additional difference between NPD and narcissistic traits is that for NPD to be present, symptoms must manifest across most areas of a person’s life and remain stable over time,” says Dine. Narcissistic traits, though, may only appear in certain contexts or at times.
The answer is going to be different for everyone.
Your individual narcissistic traits may be nuanced or context-dependent. For example, you may strive to get ahead at work by any means necessary while still being able to accept constructive criticism from your spouse. That’s an example of the gray zone.
In this way, narcissism doesn’t necessarily develop into a diagnosis of narcissistic personality disorder, says Phillips. “NPD is a long-standing diagnosis. Traits can be seen in childhood or adolescence but not confirmed until after that time,” she explains.
“NPD is a long-standing diagnosis. Traits can be seen in childhood or adolescence but not confirmed until after that time,” she explains.
Traits of narcissism can negatively impact a person’s life depending on the severity level, says Dine.
If someone lives with narcissistic personality disorder, the need for help may not be as evident for them.
“Recognizing the need for therapeutic intervention can be difficult, as there is usually a deeply engrained belief they are special,” she explains. “There is a refusal to take responsibility for behavior or accept personal flaws or areas for improvement.”
However, if you or someone you love recognizes the need for treatment, cognitive behavioral therapy (CBT) can be a great place to start, says Dine.
“Seeking a mental health provider who offers a specialization in narcissistic personality disorder is paramount. Empathy-building techniques, such as journaling and identifying emotions, can also be helpful,” she adds.
Narcissism is a personality trait many live with and only becomes evident occasionally. Narcissistic personality disorder is a formal mental health condition with persistent symptoms that significantly impact the quality of life.
You may have some narcissistic traits without meeting the diagnostic criteria for narcissistic personality disorder.
“For a diagnosis of NPD to occur, there must be a pervasive and long-term pattern of grandiosity, lack of empathy for others, inflation of a person’s own abilities, and symptoms generally must be present across most areas of life,” says Dine.
Narcissism - what it is, signs and causes of narcissistic personality disorder
About who people with narcissism are, where it comes from and whether it is always necessary to break off relations with narcissists, says Anna Krymskaya, a clinical psychologist and co-founder of the online psychological help service YouTalk
Surely among your acquaintances there is someone about whom you thought “yes, he is a typical narcissist”. Most likely, the description of this person will look like this: self-confident, ambitious, somewhat selfish. Possibly manipulative.
Most likely, the description of this person will look like this: self-confident, ambitious, somewhat selfish. Possibly manipulative.
Finished reading here
The term "narcissism" sounds everywhere: in psychological blogs, films, "Tiktok". There are articles and studies about him. But often in them this phenomenon is simplified and stigmatized. Who are narcissists, should they be avoided, and when can one speak of a narcissistic disorder?
What is narcissism
Psychologically, narcissism is an exaggerated belief about one's contribution to society or a group, otherwise known as excessive narcissism or even self-centeredness. This is not a monolithic concept, but a whole spectrum. To some extent, its features are present in many of us, this is normal and even useful in some ways. For example, people with a narcissistic temperament are often ambitious, take care of themselves and achieve great success in their careers.
For example, people with a narcissistic temperament are often ambitious, take care of themselves and achieve great success in their careers.
Depending on how pronounced the narcissistic tendencies are and whether they interfere with life, the spectrum of narcissism can be divided into four parts:
Character and accentuation are options for a healthy manifestation of narcissism, and personality disorder is already a psychiatric diagnosis.
Related material
The extreme degree of the norm is the narcissistic accentuation of the personality. This means that the narcissistic qualities of character are so pronounced that in some cases they begin to interfere with a person's life. They can affect his relationships with others or the professional sphere. However, their influence is not so serious as to diagnose a personality disorder. For example, they can lead to conflicts with superiors or prevent a person from sincerely opening up to another, removing the mask of ideality.
However, their influence is not so serious as to diagnose a personality disorder. For example, they can lead to conflicts with superiors or prevent a person from sincerely opening up to another, removing the mask of ideality.
What qualities are considered narcissistic
Based on the Narcissistic Personality Inventory, one of the most popular tools for identifying non-clinical cases of narcissism, the following qualities can be considered narcissistic:
- Demonstration. It is expressed in the idea of one's own unusualness, uniqueness, physical attractiveness and ability to influence others
- Authority. Confidence in possessing leadership qualities, the ability to influence others, power over people, the ability to succeed.
- Chosenness. The feeling of one's own peculiarity, the expectation of an exceptionally good attitude, respect, recognition of one's merits, submission to one's requirements and desires.
- Vanity. The desire to look good in the eyes of others, the need to confirm one's superiority, the desire to hear flattery from other people.
- Self-sufficiency. Confidence in one's independence from people in achieving results, competence, responsibility for making decisions, confidence in the correctness of one's actions, the ability to live in accordance with one's desires, the ability to become a great person.
- Excellence. Conviction in the extraordinary and uniqueness of one's personality, the presence of special achievements and talents, the deserving of appropriate recognition from others.
- Operation. Confidence in one's ability to use other people, the ease of manipulating others to achieve one's own goals, the ability to understand others well, influence their behavior, and convince of something.
Along with these traits, there are often such characteristics as increased sensitivity to shame, perfectionism, a feeling of inner emptiness and loneliness.
People with a narcissistic psychotype are demonized, attributing to them aggressiveness, lack of empathy, a tendency to violence
The traits listed above are manifestations of narcissism as a personality trait, that is, a norm. To be diagnosed with Narcissistic Personality Disorder, according to the American DSM-5 classification of diseases, in early adulthood, a person must exhibit five or more of the following characteristics of narcissism:
In Russia, however, since January 2022 it has become impossible to get a diagnosis of Narcissistic Personality Disorder, because our doctors do not follow the DSM-5, but the International Classification of Diseases from the World Health Organization. In the latest edition, the division into individual personality disorders was removed: now they look at whether a person has general signs of a personality disorder, the degree of their severity and specific manifestations. This will make the approach more comprehensive and personalized.
Is it worth labeling a person "narcissus"
There are two sides to using such labels. They can be a guide, explain individual patterns in their own and others' behavior, feelings and thinking; can help you get the big picture. But they can also become a stigmatizing stigma, if you do not pay attention to the individual characteristics of a person. Unfortunately, in modern culture, this often happens and any people with a narcissistic psychotype are demonized, attributing to them aggressiveness, lack of empathy, a tendency to violence, and offering to avoid any contact with them. But this will not be true for every person with narcissistic traits. Because of such generalizations, even the expression "narcissist" itself has acquired a negative connotation, and its use is considered not entirely ethical.
But they can also become a stigmatizing stigma, if you do not pay attention to the individual characteristics of a person. Unfortunately, in modern culture, this often happens and any people with a narcissistic psychotype are demonized, attributing to them aggressiveness, lack of empathy, a tendency to violence, and offering to avoid any contact with them. But this will not be true for every person with narcissistic traits. Because of such generalizations, even the expression "narcissist" itself has acquired a negative connotation, and its use is considered not entirely ethical.
In addition, in psychology there are many different classifications of narcissism that better convey the shades of this phenomenon than one term.
Related material
What types of narcissism are distinguished by psychologists
Most often they talk about two types:
Grandiose. Such a person wants to be the best. Faster, higher, stronger than all. Career, appearance, relationships - everything should be perfect. This characteristic fits well with the modern philosophy of success and achievement, so often this type achieves a lot in life. Grandiose narcissists can embellish reality to fit their ideal image if reality falls short. The self-esteem of such people is unstable: from the outside it may seem high or even inflated, but inside they often feel empty and dissatisfied.
Such a person wants to be the best. Faster, higher, stronger than all. Career, appearance, relationships - everything should be perfect. This characteristic fits well with the modern philosophy of success and achievement, so often this type achieves a lot in life. Grandiose narcissists can embellish reality to fit their ideal image if reality falls short. The self-esteem of such people is unstable: from the outside it may seem high or even inflated, but inside they often feel empty and dissatisfied.
Vulnerable. He is also hidden or thin-skinned. Clinical psychologist Paul Wink in his work "The Two Faces of Narcissism" described the mental portrait of representatives of this type as prone to introversion, submission, anxiety, vulnerability and always being on the defensive. However, like the grandiose type, they are vain, interested in others, impulsive, and often take risks.
While grandiose narcissists tend to exalt themselves in the eyes of others, vulnerable narcissists may appear to hate themselves. In fact, this is the same idealization, but turned inside out. While grandiose narcissists tend to see themselves as the best, covert narcissists tend to see themselves as the worst, stupidest, most miserable. Keyword: most.
In fact, this is the same idealization, but turned inside out. While grandiose narcissists tend to see themselves as the best, covert narcissists tend to see themselves as the worst, stupidest, most miserable. Keyword: most.
From the grandiose pole, a person with narcissism can fall into the other extreme: feel like a partner unworthy of love in principle
Some researchers believe that these types are not mutually exclusive, but can change depending on the circumstances of a person's life. For example, there was a successful period at work: a person exceeded KPI and received praise from his superiors. At this point, he will be inclined to idealize himself, to feel his own exclusivity and superiority, life will seem beautiful. A week later, the partner shares that some aspect of the relationship does not suit him. From the grandiose pole, a person with narcissism can fall into the other extreme: to feel like a disgusting partner, unworthy of love in principle. And at the same time devalue all previous achievements. In this state, a person may impulsively propose a breakup or show aggression, trying to avoid corrosive shame.
And at the same time devalue all previous achievements. In this state, a person may impulsively propose a breakup or show aggression, trying to avoid corrosive shame.
And if the narcissistic disorder is accompanied by features of sociopathy (indifference, aggressiveness, disregard for social norms), one can speak of perverse narcissism. It is this type that is prone to emotional violence and even crime due to a lack of empathy. Perverted narcissists are people who prove their worth and value through the humiliation of others. It is extremely difficult for them to build a healthy relationship, as they are not able to empathize, lie, manipulate and overly control their partner. This type rarely turns to a psychotherapist, and it is difficult for him to stay in therapy.
Narcissism in Men and Women
Scientists at the Buffalo Institute reviewed studies of narcissistic personality disorder over the past 30 years and found that it is more common in men and manifests somewhat differently than in women.
First, men are more likely to exploit others and feel entitled to enjoy privileges. Secondly, they show more desire for power and leadership. But in the manifestations of vanity and egocentrism, there was no particular difference. Scientists suggest that such results may be the result of a certain gender socialization - that is, the attitudes broadcast by society about what men and women can and cannot be.
Because women are often criticized for being aggressive and authoritarian, they can suppress these narcissistic traits while men do not have to. But the authors note that this topic requires further study.
Causes of narcissism
There are different concepts as to why people develop narcissism. The conducted studies have not proved an unambiguous connection with genetics, so the sociocultural concept remains the main one.
Representatives of psychoanalysis paid particular attention to the nature of narcissism. For example, Sigmund Freud and Heinz Kohut were of the opinion that at a certain stage in the development of a child, the emergence of narcissism is a natural and healthy phenomenon - this is called primary narcissism. In infancy, the child has no other needs than his own, and he does not have to make any effort to satisfy them. In fact, he is the center of his own universe. This is a normal developmental stage that everyone goes through.
However, certain circumstances can lead to secondary narcissism - that is, its unhealthy form. Such a circumstance could be a lack of parental love and acceptance. Moreover, the child did not necessarily encounter excessive severity, cruelty or indifference. It is quite possible that his parents, on the contrary, praised him for any reason and did not forbid anything. Child idealization and permissiveness can also be perceived as dislike and cause secondary narcissism, according to Karen Horney. When only the positive side is seen in a child, ignoring the existence of negative traits, he feels unseen. As if they love not him, but some other person, an image. In both cases, the defensive reaction is the creation of an imaginary ideal "I", designed to deserve the love and attention of others.
Child idealization and permissiveness can also be perceived as dislike and cause secondary narcissism, according to Karen Horney. When only the positive side is seen in a child, ignoring the existence of negative traits, he feels unseen. As if they love not him, but some other person, an image. In both cases, the defensive reaction is the creation of an imaginary ideal "I", designed to deserve the love and attention of others.
Related material
Psychoanalyst Andre Green considers another reason in his article "Dead Mother". He talks about a situation in which the mother was physically alive, but was emotionally unavailable and absent due to depression. For this reason, the child did not receive love, care, support in the proper amount. The researcher believed that the mother's depression becomes a trauma for the child, since the baby, up to a certain age, sees in himself the cause of everything that happens around him and, among other things, blames himself for his mother's condition.
Lack of communication and warmth leads to the fact that the child tries to "bring the mother back to life", changing behavior, attracting attention. Failures give rise to tremendous anxiety and a feeling of a bottomless hole inside. Over time, the baby begins to feel the emptiness, which he will later try to fill: with achievements, attention, other people. In this case, those around him can become his narcissistic extension - like an extension of his personality, an attribute to maintain status and high self-esteem. Other consequences are the replacement of emotions with reasoning, a tendency to depression, aggressiveness, the inability to let someone in, to accept and experience love, to build warm trusting relationships.
Narcissistic trauma
Trauma associated with the narcissistic part of the personality can occur not only in childhood. According to Freud, a narcissistic injury is a situation in which the narcissist feels that his hidden true self has been discovered. Its imperfection is revealed. For example, if he faced failure or his authority was called into question. Narcissistic trauma can lead to depression or what is known as narcissistic rage, an attempt to regain control and avenge the pain.
According to Freud, a narcissistic injury is a situation in which the narcissist feels that his hidden true self has been discovered. Its imperfection is revealed. For example, if he faced failure or his authority was called into question. Narcissistic trauma can lead to depression or what is known as narcissistic rage, an attempt to regain control and avenge the pain.
Treatment of narcissism
Both narcissistic personality disorder and narcissism in the broadest sense are generally amenable to psychotherapy. It's not exactly a "treatment" in the medical sense of the word. Rather, the process of knowing, accepting and adapting to the characteristics of one's personality.
For therapy to be effective, the person must be interested in it. In many cases, the benefits of narcissistic character traits and the difficulty in recognizing one's own imperfection lead to the fact that a person is not too willing to change something in his life and turn to a psychotherapist. And in a situation where we are talking simply about character traits that do not interfere with the person himself and do not harm others, the therapy of narcissism is, in principle, not needed.
And in a situation where we are talking simply about character traits that do not interfere with the person himself and do not harm others, the therapy of narcissism is, in principle, not needed.
If your relationship is bad, then whether the person is a narcissist or not, it makes sense to think about parting. Working with the deep structures of personality requires a lot of effort and time. But at the same time, the very arrival of psychotherapy already has a positive effect. The therapeutic relationship is built on trust, acceptance, and recognition of the person in all of his manifestations, and this is exactly the kind of experience that people with narcissistic disorder or pronounced narcissism practically do not have.Together with the client, the therapist looks for points of support and support. The psychologist is able to endure regular cycles of idealization and devaluation, which allows the relationship to last.
Teaches the client to see himself, not to fall into one of the poles of adoration and hatred, to endure his fears, doubts, vulnerability, envy and a constant sense of shame. See the value of other people in isolation from himself and, if necessary, control his aggression.
Having received the experience of warm acceptance of different aspects of his personality in therapy, a person with narcissism learns to apply this experience in everyday life, to build relationships with the world and himself in a new way.
How to communicate with a person if you suspect narcissism or NPD
There are two main principles to follow: focus on how you feel in contact with this person, and not try to save him. In general, these rules can be applied to any relationship, regardless of the type of person.
It is not so important to recognize how pronounced narcissism is, but to pay attention to the quality of your relationship:
- whether there is disrespect, manipulation, aggression or violence
- Does your self-esteem suffer? No, it makes sense to think about parting.
In the case of an abusive relationship without outside support, this can be very difficult. Psychotherapy can help you find a resource for ending a relationship, as well as understanding the reasons why you ended up and stayed in it so that the scenario does not repeat itself in the future.
If it seems to you that a person has strong narcissistic inclinations, but at the same time the relationships themselves are built on mutual respect, warmth and sincerity, there is no violence in them in any form, then you should not break off contact just because the person is a “narcissist”.
Narcissism and narcissistic disorders | Journal of Practical Psychology and Psychoanalysis
Year of publication and journal number:
2008, No. 4
Recently, I decided to review the psychoanalytic literature on the concept of narcissism and the description of narcissistic disorders to see how they correspond to my clinical experience.
There is probably no area of psychoanalytic literature more abundant than that devoted to to narcissism : it seemed endless when I understood this topic. I will spare you most of this literature, and will only cite what is directly related to my research - however, there is a wide field of work left outside of it. This literature is not only vast, it is full of confusion. There are different patterns of development, which makes any discussion of narcissism difficult - but the confusion is compounded by the fact that the term "narcissism" itself is used in different senses.
Therefore, before moving on, I would like to clarify my use of this term. I decided that the word narcissism is used in three ways in psychoanalytic literature. 1) First, it describes narcissism as a phenomenon : an apparent lack of interest in others, coupled with an obsession with the self. This can be observed in various psychological disorders, as well as in everyday life.
Second, it is used to describe the strength or innate tendency in the personality that prevents relationships outside the self. Thirdly, it is used to refer to a special group of cases of personality dysfunction called narcissistic disorders. In this chapter, I will consider the second and third meanings of the term "narcissism." I will try to answer the following questions: what role does narcissism as a force play in narcissistic disorders, and is there a difference between libidinal and destructive narcissism.
The development of the concept of narcissism
The beginnings of the distinction between libidinal and destructive narcissism can be found in the history of the development of the concept of narcissism. From the very beginning, two themes have been counterpointed in the discourse on clinical narcissism. One is narcissism as a defense against unfavorable object relations ; the other is narcissism as a manifestation of a fundamental hostility to object relations.
Even the original myth of Narcissus exists in two versions: one gives a solipsistic presentation, the other a traumatic explanation. In the famous retelling of Ovid, Narcissus pays the price of considering everyone but himself unworthy of his love; but Pausanias found another version known, in which Narcissus lost his twin sister and mistook his reflection in the pond for this lost sister.
A useful but inaccurate generalization can be made that Freud's train of thought leads us to the concept of libidinal narcissism, while Abraham's ideas, which actually precede Freud's, lead to the concept of destructive narcissism. Freud made it clear that he sees secondary narcissism as a means of maintaining or restoring love when object love seems impossible, while Abraham emphasized hostility to transference objects in narcissistic disorders. Freud described self-love as a substitute for mother-love in narcissistic characters; Abraham, on the other hand, believed that envy promotes narcissism and delays object love.
From the beginning, Abraham associated self-absorption with "negativism." "The negativism of dementia praecox (schizophrenia) is the exact opposite of transference," he wrote in the first psychoanalytic paper on the subject (Abraham, 1908, p. 71). Abraham noted this for the first time in a letter to Freud, with whom he was yet to meet in person. Abraham suggested that, in contrast to hysteria, "dementia praecox destroys a person's capacity for sexual transference, that is, for object love" (Abraham, 1908, p. 69). The term "narcissism" was not yet in use at the time, and Abraham was talking about autoeroticism. He believed that the schizophrenic turns away from all love objects, instead reverting to autoeroticism. Freud was certainly impressed and convinced of the validity of Abraham's theory.
Freud adopted and developed the term narcissism from Paul Nacke and Havelock Ellis, who used it to describe a person who treats his body as a sexual object. Freud's own development of the concept of narcissism began with a footnote he added in 1910th year to Three Essays on the Theory of Sexuality (Freud, 1905d) and describing narcissistic object relations.
Speaking about male homosexuals, Freud wrote:
"in early childhood [they] experienced a brief but very intense fixation on a woman (usually their mother), after overcoming which they identify themselves with a woman and choose themselves in as your sexual object. That is, out of narcissism, they are looking for young men similar to themselves, whom they could love as their mother loved them" (Freud, 1905d, pp. 144–145 fn.).
In the article "On Narcissism", dated 1914 (1914c), Freud further develops the thought of this striving for the ideal of mother-child love. Usually falling in love, in his opinion, drains the ego in favor of the object whose mutual love is the only remedy for this hemorrhagic libido. Those unfortunates whose love is unrequited lose not only the love of another, but also self-love, and therefore suffer from pain and loss of self-respect. However, secondary narcissism, according to Freud, arises only when there is some obstacle to the realization of object love according to internal reasons .
He wrote:
“the satisfaction of love is impossible, and the enrichment of the ego can again be secured only by withdrawing the libido from objects. The return of the object libido to the ego and its transformation into narcissism represents, as it were, happy love again; on the other hand, it is also true that true happy love corresponds to a primordial state in which object libido and ego libido are indistinguishable” (Freud, 1914c, pp. 99–100).
Suddenly, in this last sentence, Freud makes us understand that the accomplished libidinal narcissist is in love with himself just as someone can be "in love" with another person. But is it really another person if "happy love corresponds to the original state in which object libido and ego-libido are indistinguishable"? Here Freud suggests that this "original" - "happy love" - is essentially narcissistic object love, whether it unfolds with another person in the external world or turns out to be a love affair with the self in the internal world.
In both situations, whether the object is external or internal, a positive attitude is conditioned by the elimination of difference.
If this is true, the "narcissistic state" is not just a withdrawal from external objects to an internal object. This is a special type of internal object relation in which the separate existence and proper qualities of the internal object are denied and an internal narcissistic relation is created through projective identification. This sounds like a description of the ideal relationship between the self and the ego-ideal, replacing the relationship between the ego and the super-ego: twin inner souls united by a narcissistic love that may make the ego's need for the super-ego love that Freud considered redundant a necessary condition for life. Isn't the narcissistic state an escape from the superego? Do narcissistic object relations serve as an alternative to the superego's desire for love? And in this case, is it not fear of a hostile Super-Ego or envy of a powerful, impeccable Super-Ego that prompts them? I was convinced of the validity of this assumption by a number of cases, one of which I will describe later in this chapter.
Following Abraham's discussion of narcissism, we find ourselves exploring a topic that will reach its logical conclusion in Rosenfeld's concept of destructive narcissism. In his 1908 paper, Abraham relates the shift from object love to autoeroticism in dementia praecox to the negativism of the patients. In a further approach to the subject, he suggests that the excessive self-esteem of some patients is accompanied by contempt and hostility towards their love objects. In his article on premature ejaculation (Abraham, 1917) Abraham describes narcissism as a source of sexual resistance : “Their object love is very imperfect. Their true love object is themselves. In accordance with Freud's opinion, we find /.../ a particularly high and abnormally emotional evaluation of the penis. Abraham goes further and connects this phallic narcissism with a hostile contempt for women: “he takes revenge on every woman for the disappointments of love that his mother subjected him to in childhood” (ibid.
, p. 297). In his work on the psychogenesis of melancholia, he describes clinical narcissism , existing in both positive and negative forms: positive when manifested as self-admiration, and negative when manifested as self-denigration (Abraham, 1924).
Two years after he described phallic narcissism, Abraham writes the first paper describing narcissistic disorder as a concept that has psychoanalytic meaning and is supported by clinical practice (Abraham, 1919). In this article, he discusses a small group of patients who are unable to comply with the rules of the psychoanalytic method, although they seem to succeed, and notes that "among my patients, these were those in whom narcissism was most pronounced" (Abraham, 1919, pp. 304–305).
This 1919 paper by Abraham was the starting point for Rosenfeld's first major paper on narcissistic disorders (Rosenfeld, 1964). She also influenced two important papers, published in 1936, linking Abraham's description of narcissistic character disorder with negative therapeutic reactions.
One of them belonged to Joan Riviere and the other to Karen Horney. Article by Riviere (Riviere, 1936) brings Klein's new theory of the depressive position and manic defense to the previous understanding of negative reactions in analysis, and adds to it the author's concept of "defensive organizations". Horney (1936) emphasizes the compulsive rivalry of such patients with the analyst, as well as their demand for unconditional love. This love is necessary for them to withstand a double anxiety: the anxiety associated with the awareness and expression of their own hostility, and the anxiety associated with retribution from outside.
Rosenfeld took up and developed Horney's description of the patient's response to the work of the analyst and Riviere's (1936) concept of defense organizations. He developed his own theory of "narcissistic organization" in the personality, which is opposed to true object relations and achieves patient loyalty through seduction, control and tyranny.
Rosenfeld thought it important to distinguish between narcissistic states in which the libidinal aspects predominate and those in which the destructive aspects of narcissism predominate.
Although in the first, libidinal case, when the narcissistic belief system is damaged, envy, resentment and revenge do flare up, analysis improves understanding and reduces negativism. However, in predominantly destructive narcissism, envy is more powerful and less acknowledged, and there is an overwhelming desire to destroy the analyst or the self. In this destructive case, as Rosenfeld notes, "death is idealized as the solution to all problems" (Rosenfeld, 1987, pp. 106-107).
Hanna Segal notes that she disagrees with Rosenfeld on the distinction between destructive and libidinal narcissism: in her opinion, there is only destructive narcissism. However, she limits the scope of the term narcissism to a force in narcissistic organizations that is fundamentally hostile to object relations: “Under narcissism, life-giving relationships and healthy self-love are equally attacked,” she writes. “Envy and narcissism are like two sides of the same coin” (Segal, 1997, pp. 75, 85). Self-love - and, by implication, Freud's description of the "happy love" of narcissistic relationships - Segal categorizes life instincts, which he considers to be object-love-based rather than narcissistic.
As part of her definition of narcissism as a force directed against object relations in the individual - I completely agree with Segal. But if we talk about narcissistic disorders - I believe that they include a whole range of phenomena - both destructive, and libidinal, and protective.
John Steiner covers them with his broader concept of "pathological organizations": in his view, the defenses in them are combined with destructive and libidinal narcissistic forces (Steiner, 1987). Realizing that narcissistic systems are inevitably driven by mixed motives, he does not consider it necessary to separate them (personal communication with J. Steiner). Nevertheless, in my opinion, whatever the set of motives may be and however varied, at any given moment the main motive is either libidinal/protective or hostile/destructive. The formation of narcissistic object relations may be motivated by the desire to retain the capacity for love, giving the object of love a semblance of self, or it may be aimed at the annihilation of the object as a representative of otherness.
Aggression can be generated either by predominantly defensive or predominantly destructive narcissism. But there is a difference between the struggle to retain love and the unbridled violence of hostility towards objects. In the public sphere, war may be defensive, and patriotic aggression may be love misdirected, but genocide is never: it is caused by the xenocidal impulse to annihilate otherness.
To illustrate my understanding of this distinction, I will briefly describe two patients. The first I would call suffering from a predominantly destructive narcissistic disorder, the second from a predominantly libidinal narcissistic disorder. What they have in common is the generation through projective identification of a narcissistic relationship with the Ego-ideal in order to avoid a relationship with the destructive, parental Super-Ego. Moreover, in the first case, destructiveness is translated into a relationship between twins, which then becomes a deadly alliance; on the other hand, in the second case, destructiveness becomes a mental refuge, where the original “happy love” is sought in mutual understanding.
Mrs. L.: twin self vs. old woman
I would like to give a short example from the supervision analysis of Mrs. L., a narcissistic patient. Dr. A was particularly eager for this supervision, for although the analysis had just begun, she already felt considerable difficulty. Dr. A. is a conscientious and skillful analyst with experience in analyzing disturbed and difficult patients; she could not understand her inability to establish and maintain an analytic setting with this patient.
Dr. A. described a series of uncharacteristic blunders that led her to confess to a patient something she had not intended to confess, which she immediately regretted. Therefore, she felt that the analysis was out of her control. Mrs. L., an attractive young woman, came to the analyst after the upsetting end of her relationship with a certain man. She also had teenage disorders and episodes of anorexia in her history. She left the city where she lived with her ex-man and returned to another, where her rich father lived with his second wife and where she was to undergo analysis.
Everything was agreed, but when the workers came on the day of her departure to arrange the move, she refused their services and missed her plane.
Arriving at her new home and arranging the start of the analysis, she missed the first session. She called and explained that she had lost the analyst's office number. Dr. A, feeling the need to establish her analytic stance and method of work from the outset, "firmly decided" to discuss the issue of paying for the missed session. An alarming signal for the analyst was the inexplicable loss of "firm determination" and some other points. When Mrs. L., who was due to pay by check at the end of the month for her missed session, did not do so, Dr. A., to her annoyance, was unable to draw attention to it. Following this session, the patient, very wealthy by any measure, called Dr. A. to say that she could not continue the analysis because she could not afford it. Dr. A suggested that the patient come to the next session on time and they could discuss the matter.
The patient agreed, and then in the session, Dr. A., to her horror and despair, found herself drawn into further fruitless conversation with the patient. For the next session, the patient arrived twenty minutes early, which caused some confusion in the process.
During this session, Mrs. L. lay restlessly on the couch, constantly crawling and getting up several times for sweets and napkins. What disturbed the analyst the most, however, was her own behavior. In this session, she surprised herself by agreeing to reduce the payment for this patient. The feeling that her countertransference was out of control was further heightened when, instead of considering the problem in self-analysis in preparation for the next session, she inadvertently prolonged the current session - which rarely happened to her. However, it was in this session that the patient reported a dream that shed some light on these events.
“I had a very strange dream,” said Ms. L. - I was in a house - this strange house - in every series of dreams I have recurring dreams about a new house.
This one was new - but the sensory experience tells me I was here a hundred years ago. Next to me is another person who was my lover - or sister - or brother, not sure what gender this person was. I was neither a man nor a woman - or was both a man and a woman. I was protecting this other person - we lived with an old lady - we conspired to kill her. It somehow involved ladders and something written, something like a letter. Apparently, we gave her the letter without her seeing it, which led to her death. For our own sake, we had to do it. But six or seven years later we were arrested. I know it was me in the dream - usually I don't lie (she lies all the time, the analyst added) - I remember thinking this is the first time - they won't expose me, they won't find out that we committed murder. If she, the old woman, knew, she would take revenge. She was a kind of vicious old woman - a destructive force. It was not a malice killing, but a matter of life and death for me. The reason was this internal struggle.
I felt in my mouth such a taste as from a huge piece of chewing gum - it was cannibalism - like chewing tasteless meat.
“When I woke up this morning, I felt sick,” the patient continued. “Finally I threw up.” The patient herself recognized the vicious old woman as her mother.
Undoubtedly, there is much condensed in this dream, and it is tempting to explore topics such as cannibalism and oral sadism. But I think the best way to use this dream is to explain what was really going on in the analysis and what light it might shed on the problem of repeated enactments. I suggested that Dr. A. is represented in the dream by and as "twin soul/lover", and as an evil old woman - then the last events make sense. Dr. A's unconscious countertransference identification with the patient is represented in the dream by the patient's "twin soul". Then the plot of the twin souls to kill the "evil old lady" can be seen as an unconscious conspiracy between the patient and the analyst to destroy Dr.
A's professional self. under the threat of being fed poisoned meat through the mysterious practices of psychoanalysis.
The analyst regained her habitual analytic position and lost it only from time to time when the patient dramatically introduced some unexpected complications into the analysis. A stereotypical pattern emerged in which negative therapeutic responses followed forward movement. As the analysis progressed, the full extent of the patient's impairment became more apparent. She had problems with drugs, and episodes of bulimia and vomiting had been repeated for a long time. The unfolding history and transference of the patient indicated that she was bisexual. In particular, there were periods of oscillation between homosexual erotic transference and negative, paranoid transference.
I would like to emphasize my point - that the narcissistic object relationship developed by this patient, the "soul-twin" relationship, was a conspiracy formed to counter the deadly super-ego represented by the "old woman".
However, the destructiveness turned into a narcissistic relationship. The purpose of the libidinal connection, expressed in erotic transference, was to create an alliance whose goal was murder. A dream that the patient had a year and a half after the events described shed more light on this complex narcissistic organization.
Ms. L. is spoon-feeding her baby - her mother is in the room - Ms. L. is not sure whose baby it is. During feeding, the spoon becomes a fork, which tears off pieces of skin from the baby's lips, and he then ate these pieces. The patient turns to her mother for help. The mother says: “do it like this,” and tears off a larger piece from the child’s mouth, while saying: “this is what he eats.”
Ms. L. objects that there must be another way for the child not to eat itself. The lips of the child are very red and tightly clenched, in appearance they resemble the genitals. Then the patient realizes that this is not her mother, but X, her former lover, and they are not feeding the child, but having sex.
“In real life,” the patient noted, “I had a homosexual sexual relationship with X.” “X,” she continued, “had a perfect body, I adored him. When I say “perfect”, this is what I mean: my father, in my opinion, would like a woman to have such a body.”
“We were together in college,” added Ms. L. “It reminded me that at that time I often had one masturbatory fantasy: of watching a man in boots with steel-studded socks kicking in the genitals woman until her clitoris falls off.
“When I was little, I thought that a woman gets pregnant because she swallows something big and round.”
“Food comes in good and comes out crap. I had another dream, she said, in which shit covered everything, nothing was visible behind the shit; it was impossible to get anywhere, everything was covered in shit.”
What goes in can be good, but when it comes out again, it's shit that covers everything. A better description of how the analyst experienced the sessions I cannot imagine.
Again and again I see here a model in which the session begins clearly and clearly, which leads to straightforward interpretations and a positive response from the patient. Then all this is lost in the confusion of confusing and confused information from the patient.
This analysis and the dream have many aspects. But for now I would like to focus on the patient's sexual relationship with her ideal Ego, represented by X, which was constructed from the patient's own Ego-ideal—that is, a woman with exactly the body her father would have wanted. Thus X usurps the place of the mother in the primal scene, and the patient takes the place of the father with X. Thus the idyllic, illusory, narcissistically based homosexual primal scene is built and played out. However, this is due to a sadistic masturbatory fantasy of intercourse resurfacing, which is similar to the scene of feeding a child in a dream with the same substitution of mutilation for satisfaction. So in this case, the ostensibly defensive withdrawal from the terrifying relationship with the lethal nursing figure into an autoerotic genital fantasy entails the same destructive elements.
The cannibal breast-fork that feeds the child itself becomes a steel-studded penis that castrates the female genitals.
Mrs. D.: predominantly libidinal narcissism
My second case is Mrs. D., professor and head of a successful university department, a woman of early middle age. She entered analysis a year after her lengthy course of psychotherapy had been terminated by mutual agreement with her therapist. By the time of this completion, she felt in good shape. Now she came to the analyst because she was afraid, in her words, of "completely breaking down." According to her description, she constantly suffered, being obsessed with a relationship with a young man - a relationship not of sexual, but of intellectual intimacy. She considered her feelings completely irrational and told me that this had happened before to another young man during her previous course of treatment. Both young men were her junior colleagues in her department. Both cases were deployed according to the same scheme.
At first, the patient felt that she and her friend had a complete understanding, a spiritual unity. Then, when this mutual understanding could not be maintained, she began to suffer.
The patient considered her marriage a happy one; children were central to her life. But as soon as a relationship with a young man arose in her soul, they completely absorbed her attention. She was plagued by fears that the children would no longer appreciate her and what she had given them. Whenever something happened that confirmed this idea, she began to consider herself a bad and worthless person. Love, admiration, respect and approval from her husband, children and friends calmed her, but in no way softened the power of the attitude of young people over her self-esteem.
The configuration that determines obsessive relationships with young people became more understandable. The patient was the only child of parents who lived separately. Her mother suffered from a severe narcissistic disorder, and her father was legendary for his egocentrism and vanity.
In the course of her analysis, she was taken aback by dreams in which her brother appeared. In these dreams, she was not surprised by the presence of her brother. She had never seen this man before, but she knew it was her brother. As a child, she had an imaginary companion, and as a teenager, she said, she developed a close but platonic friendship with a young man.
This deep emotional dependence on young people's perceptions contrasted with her relationships with those she truly depended on, such as her husband. Her relationship with him was mutually warm. However, they were guarded by the limitedness of her expectations regarding understanding from her husband - and thus regarding the painfulness of disappointment and the expression of displeasure. Her transference to me followed the same pattern. Although my understanding obviously benefited her, she did not seek it, but she did not resist it either - she simply avoided expecting it. The analytic transference, like her relationship in marriage, followed the pattern of her relationship with her parents.
Relations with them were maintained by Mrs D's severe limitation of expectations and by her search for a kindred spirit somewhere on the side. Turning the expectation of understanding to the parent object, from her point of view, had no chance of success and would lead to the denial of her own subjective existence.
The twin soul mate Mrs. D. hoped for in return had an additional aspect - she served as the ideal of her self. The patient believed that the ideal young man should be the primary love object of the ideal mother, the like of whom she did not know. Therefore, in the relationship of twins, the patient could play both roles - to play the ideal mother and through projective identification to experience (for the other) love that she had never received.
***
I believe that both patients had catastrophic ego-relationships - but with some difference. In Mrs. L., the first patient, the super-ego figure was a deadly woman; in Mrs. D., this place was usually occupied by the inner parent, which seemed to be a void—not merely an absence, but a negating presence.
They both shied away from the relationship with the super-ego by forming an attachment to the ego-ideal - which created a narcissistic organization. This was realized externally in relations with an idealized double. In the first patient, a perverse, sadomasochistic relationship arose; in the second, the authority of superego judgments was invested in the narcissistic object, whose approval thus became a matter of life and death. I think that narcissistic object relations in the first case led to something like the infamous Bonnie and Clyde couple, and in the second to something like the Romeo and Juliet couple. Death lurks in both scenarios, but in one the partnership is based on a shared love of murder, and in the other, death is preferred over life without the love of the other.
The backgrounds of both patients are similar. Both parents divorced; both mothers found it difficult to perform maternal function; both had successful fathers, distinguished by merciless egocentrism.
However, these unfavorable parental traits were much more pronounced in the parents of the predominantly libidinal patient, Mrs. D. Her own disturbances were significantly less and less narcissistic than in either of her parents. Mrs. L., who suffered from predominantly destructive narcissistic disorder, was, on the contrary, significantly more severe than either of her parents. In her case, one can note an aggravation of the situation in the next generation, and in the case of Ms. D., on the contrary, an improvement in the situation.
Conclusion
So, I believe that narcissistic disorders arise from the failure of containment in infancy and childhood, which gives rise to an ego-destructive super-ego. A narcissistic organization develops, using narcissistic object relations—internal, external, or both—in order to evade the hostile superego. This may lead to a predominantly libidinal organization or a predominantly destructive narcissistic organization. Further, I believe that libidinal, defensive organization occurs when the main factor in the initial failure of containment is on the side of the parents; and destructive organization - when the main factor is the excessive hostility to objects in the infant.
Learn more