Most effective ssri
The most effective antidepressants for adults revealed in major review
This is a plain English summary of an original research article
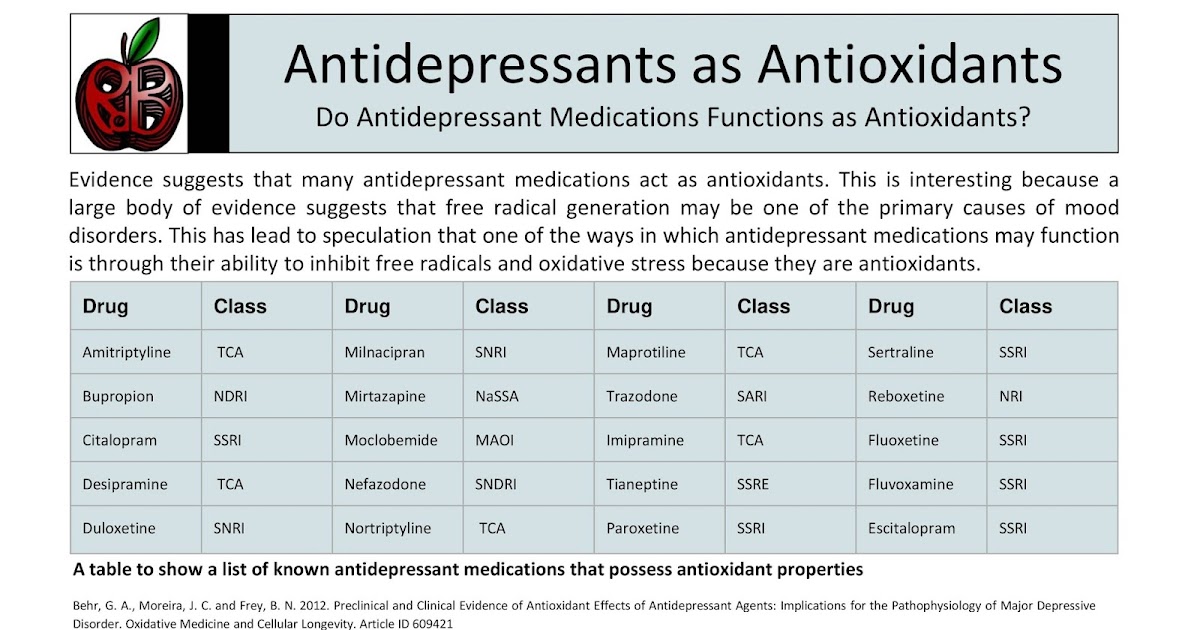
Antidepressants are effective to treat moderate to severe depression in adults. Five antidepressants appear more effective and better tolerated than others.
A major review of 522 antidepressant trials found that all of the 21 drugs studied performed better than placebo, in short-term trials measuring response to treatment. However, effectiveness varied widely.
Researchers ranked drugs by effectiveness and acceptability after eight weeks of treatment. Several drugs were more effective and were stopped by fewer people than others:
- escitalopram
- paroxetine
- sertraline
- agomelatine
- mirtazapine.
The review provides new evidence which may help people decide which antidepressant to choose first-line for moderate to severe depression. However, it did not assess antidepressants compared to other treatments such as cognitive behavioural therapy, or treatments in combination. Though there are some concerns over items not reported by individual trials, this review is likely to be reliable. It is extensive, included only placebo controlled double blind trials and searched successfully for unpublished trials.
Why was this study needed?
Depression is a common condition, affecting an estimated 1 in 10 adults at some point in their lives. Antidepressants are widely prescribed in primary and secondary care, along with psychological interventions such as cognitive behavioural or interpersonal therapy. There is conflicting evidence to guide which antidepressants should be prescribed first-line, although NICE recommends a selective serotonin reuptake inhibitor (SSRI).
There has been uncertainty in recent years about the effectiveness of antidepressants. Their mode of action is poorly understood, and improvement in mood tends to be modest. One 2008 meta-analysis suggested that antidepressants gave little benefit over placebo for mild to moderate depression.
This new analysis went to some lengths to find unpublished studies and additional data from published studies, to give us the best overview of the current state of research.
What did this study do?
This systematic review and network meta-analysis compared 21 antidepressants with placebo or each other, directly within trials and indirectly across trials. They included 522 double-blind randomised controlled trials of 116,477 adults with moderate to severe depression.
More than 100 trials were previously unpublished. As well as publication databases, international trial registers and drug approval websites, the researchers had contacted all pharmaceutical companies marketing antidepressants to ask for unpublished studies.
The antidepressants were compared for effectiveness (at least 50% improvement in symptoms) and acceptability (assessed as drop-out rate). They found 380 trials at possible risk of bias due mainly to lack of reporting of randomisation methods, and 46 at high risk. However, the trials were all placebo controlled.
However, the trials were all placebo controlled.
What did it find?
- All 21 antidepressants were more likely to produce a treatment response after eight weeks treatment than a placebo. The most effective antidepressant compared to placebo was the tricyclic antidepressant amitriptyline, which increased the chances of treatment response more than two-fold (odds ratio [OR] 2.13, 95% credible interval [CrI] 1.89 to 2.41). The least effective was the serotonin and noradrenaline reuptake inhibitor reboxetine, which increased treatment response by 37% (OR 1.37, 95% CrI 1.16 to 1.63).
- Drop-out rates by eight weeks of treatment were similar to placebo for the majority of antidepressants. People were 30% more likely to stop taking the tricyclic clomipramine than placebo (OR 1.30, 95% CrI 1.01 to 1.68) and slightly less likely to stop taking agomelatine (an “atypical” antidepressant) or the SSRI fluoxetine (OR for agomelatine 0.84, 95% CrI 0.72 to 0.97; OR for fluoxetine 0.
 88, 95% CrI 0.8 to 0.96).
88, 95% CrI 0.8 to 0.96). - In head-to-head comparisons between the drugs, five were identified as having a combination of better effectiveness and lower drop-out rates, compared to others: the SSRIs escitalopram, paroxetine and sertraline, and atypicals agomelatine and mirtazapine. Reboxetine (atypical), trazodone (similar to a tricyclic) and fluvoxamine (SSRI) were identified as having lower effectiveness and higher drop-out rates.
- Though absolute effect sizes were not reported in the results, the researchers described the effect sizes as “modest”. However, they also said that “non-response to treatment will occur.”
What does current guidance say on this issue?
The NICE 2009 guideline on depression advises that people with moderate to severe depression should be offered an antidepressant and psychological therapy such as cognitive behavioural therapy or interpersonal therapy. It says the antidepressant prescribed “should normally be an SSRI in a generic form because SSRIs are equally effective as other antidepressants and have a favourable risk-benefit ratio. ”
”
The guideline warns that venlafaxine is more associated with risk of death from overdose than other SSRIs, while “tricyclic antidepressants, except for lofepramine, are associated with the greatest risk in overdose.”
The guideline, last updated in 2016, is under review.
What are the implications?
The findings are of interest to GPs and psychiatrists, who need to decide on the best initial treatment for adults with moderate to severe depression. The comparative data may help doctors select drugs with better efficacy and side-effects.
However, treatment choice will be guided by an individual patient's circumstances and preferences. The meta-analysis was unable to look at the potentially different effects of treatment on subgroups based on age, sex, the severity of symptoms or duration of illness.
The review did not consider combined drug and psychological treatments, as recommended by NICE for moderate to severe depression, or long-term effects which limit its applicability.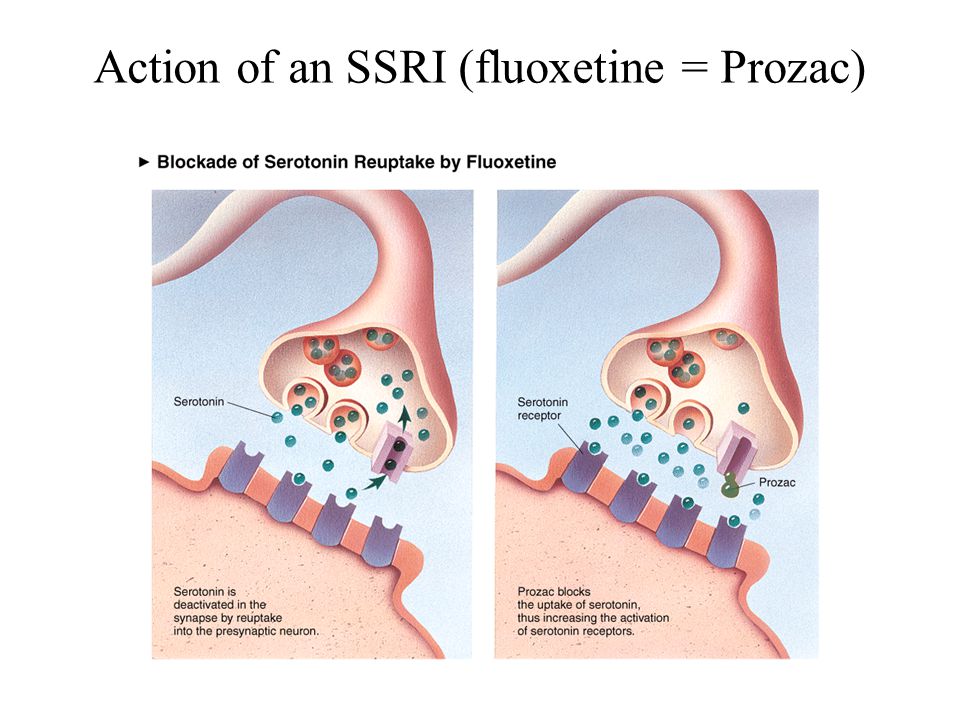
Citation and Funding
Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. 2018. [Epub ahead of print].
This project was funded by the National Institute for Health Research Oxford Health Biomedical Research Centre (BRC-1215-20005) and the Japan Society for the Promotion of Science.
Bibliography
Parikh SV, Kennedy SH. More data, more answers: picking the optimal antidepressant. Lancet 2018.
NICE. Depression in adults: recognition and management. CG90. London: National Institute for Health and Care Excellence; 2009.
Produced by the University of Southampton and Bazian on behalf of NIHR through the NIHR Dissemination Centre
What's the best antidepressant for me?
There are dozens of options. This guide can help you determine which might be the best for your needs.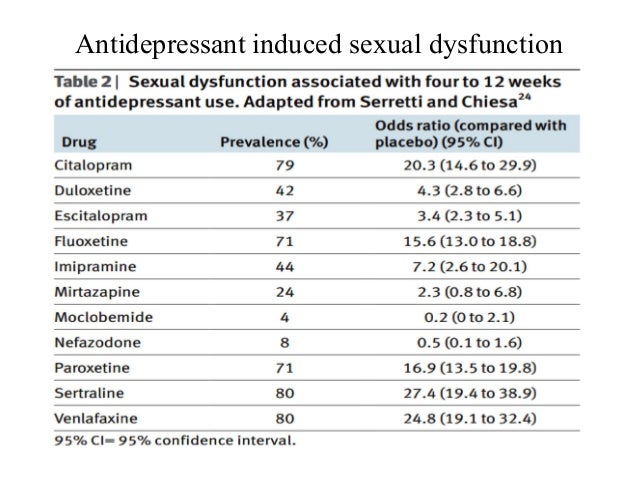
Types of antidepressants | Compare common antidepressants | Most effective antidepressant | Discontinuation syndrome | Side effects | Newest antidepressant | How to find the best antidepressant | Safety tips
The National Institute of Mental Health estimates that in 2019, about 19 million people—or 7.8% of the U.S. population—experienced at least one major depressive episode. There are several types of depression, but major depressive disorder is one of the most common.
A major depressive episode is defined as having persistent feelings of sadness, loss of interest in usual activities, changes to appetite and sleep patterns, loss of energy, difficulty concentrating, and suicidal ideation for at least two weeks, per the American Psychiatric Association.
Despite the fact that so many adults, across all age groups, live with depression each year, there are still many hurdles to receiving proper treatment. One is finding the right antidepressant medication to treat your individualized symptoms: with seven classes of antidepressants and roughly two dozen common medications available, identifying the right drug for you can seem as hard as finding a needle in a haystack.
Thankfully, there are ways to narrow down your options with your healthcare provider to make the search less intimidating. Here are some strategies for honing in on the best antidepressant to meet your needs.
RELATED: Depression statistics
Types of antidepressants
When you hear the word antidepressant, your mind might immediately jump to drugs like Prozac and Zoloft. That makes sense; those drugs are selective serotonin reuptake inhibitors (SSRIs) and are some of the most commonly prescribed antidepressants in the U.S.
But SSRIs aren’t the only type of antidepressant out there—and not everyone with depression needs to increase their levels of serotonin, a neurotransmitter (a.k.a chemical messenger) responsible for feelings of well-being.
“Antidepressants target the neurotransmitters in your brain, increasing or decreasing activity in the brain circuits related to mood regulation,” says adult and geriatric psychiatrist David A. Merrill, MD, Ph. D., director of the Pacific Neuroscience Institute’s Pacific Brain Health Center at Providence Saint John’s Health Center in California.
D., director of the Pacific Neuroscience Institute’s Pacific Brain Health Center at Providence Saint John’s Health Center in California.
The neurotransmitters most commonly affected by antidepressants include serotonin, norepinephrine, and dopamine; different classes of antidepressants work on these different neurotransmitter systems.
There are seven types of antidepressants:
- Selective serotonin reuptake inhibitors (SSRIs), including Prozac (fluoxetine), Paxil (paroxetine), Lexapro (escitalopram), Celexa (citalopram), and Zoloft (sertraline)
- Serotonin-norepinephrine reuptake inhibitors (SNRIs), including Cymbalta (duloxetine), Pristiq (desvenlafaxine), and Effexor XR (venlafaxine)
- Atypical antidepressants, including Wellbutrin (bupropion), Desyrel (trazodone), and Remeron (mirtazapine)
- Tricyclic antidepressants (TCAs), including amitriptyline, Tofranil (imipramine), and Pamelor (nortriptyline)
- Monoamine oxidase inhibitors (MAOIs), including Marplan (isocarboxazid) and Nardil (phenelzine)
- Norepinephrine and dopamine reuptake inhibitors (NDRIs), including dexmethylphenidate, and Wellbutrin (bupropion)
- Serotonin antagonist and reuptake inhibitors (SARIs), including Oleptro (trazodone), and Brintellix (vortioxetine)
Although all of these antidepressants are prescribed by healthcare providers to treat different types of patients and different types of depression, SSRIs are used the most often as a first-line treatment, says Dr. Merrill, with some SSRIs prescribed far more frequently than others.
Merrill, with some SSRIs prescribed far more frequently than others.
“Within the SSRIs, the most commonly used is Prozac because it has a lot of evidence [to support its use],” he explains, adding that Zoloft and Lexapro are also broadly prescribed.
RELATED: SSRIs vs. SNRIs: What’s the difference?
What’s the best antidepressant?
Let’s be clear: The best antidepressant for you is the one that you and your healthcare provider agree provides the most symptom relief with the least amount of side effects. Only you, in conjunction with your healthcare team, can decide what specific drug that is.
However, there are some antidepressants prescribed more often than others to people within certain population groups—and certain factors, like age, gender, pregnancy, and overall health, can determine which group you fall into (and which different antidepressants might be worth trying first).
Here are the most commonly prescribed antidepressants for the following groups of people:
The best antidepressants were chosen through a combination of expert interviews and popular data. SingleCare doesn’t endorse any particular drug over another.
SingleCare doesn’t endorse any particular drug over another.
What’s the most effective antidepressant?
There’s no single best antidepressant. Because everyone has a unique body chemistry, all antidepressants will work differently across the population of users. But some antidepressants have been shown to work more reliably and effectively for large groups of patients.
A 2018 study in The Lancet asserts that, based on extensive reviews of published studies, the antidepressants Lexapro, Paxil, Zoloft, and Remeron performed better than many other antidepressants, including popular drugs like Prozac, Luvox, and Desyrel.
It should be noted, though, that the study wasn’t able to look at how well these antidepressants work alongside other treatments, like therapy, or the side effects they may cause. (In other words, a drug that technically works to treat your depression may still not be feasible for you if it causes disruptive or serious side effects.)
It’s also important to note that most antidepressants take a long time to show their full effectiveness. “Despite brain changes happening quickly, the mood changes can take a couple of months with most of the broadly prescribed antidepressants,” says Dr. Merrill, adding that it can take anywhere from six to eight weeks, or even 12 weeks for older adults.
“Despite brain changes happening quickly, the mood changes can take a couple of months with most of the broadly prescribed antidepressants,” says Dr. Merrill, adding that it can take anywhere from six to eight weeks, or even 12 weeks for older adults.
While two or three months is a long time to wait to see if your antidepressant is truly helping you, it may not be necessary to wait quite so long if you aren’t feeling any improvement at all. “Many times, if patients are going to benefit [from a specific drug], they’ll start feeling improvement within two weeks; if you’re not, it might be worth considering moving on more rapidly, depending on how severe your depression is,” Dr. Merrill says.
Which is the hardest antidepressant to come off of?
Some antidepressants, particularly SSRIs and SNRIs, can cause a condition called “discontinuation syndrome” when therapeutic use is abruptly stopped; Dr. Merrill says this occurs because of the way the brain and body respond to the loss of serotonin support.
Per Harvard Health, typical symptoms of discontinuation syndrome include:
- Gastrointestinal upset
- Difficulty sleeping
- Flu-like symptoms
- Sweating and flushing
- Dizziness
- Hyperarousal
- Anxiety
- Agitation or irritability
While any SSRI or SNRI can cause discontinuation syndrome, the SNRI Effexor (venlafaxine) can be one of the trickiest to wean off, says psychiatrist and sleep medicine specialist Alex Dimitriu, MD, founder of Menlo Park Psychiatry & Sleep Medicine.
“Venlafaxine is an excellent medication, but missed doses can give people ‘brain zaps’ and quick feelings of vertigo, which I’ve called ‘vestibular jitters,’” Dr. Dimitriu explains. “These go away, fortunately, but it can make it hard to stop venlafaxine in particular.”
Dr. Merrill notes that Paxil is similarly difficult to discontinue, to the point where people will often put up with a lot of side effects simply to avoid having to stop its use. There are ways to make this process easier, though, so you don’t have to either suffer from discontinuation syndrome or stay on a drug in spite of your desire to wean off.
There are ways to make this process easier, though, so you don’t have to either suffer from discontinuation syndrome or stay on a drug in spite of your desire to wean off.
“Prozac has a longer half-life [than some of these other drugs], so it can be used as a bridging drug,” Dr. Merrill says. “We can transition off shorter-acting antidepressants into Prozac until your mood remains stable and we can get you off [the short-acting drug completely].”
Which antidepressants have the mildest side effects?
In general, SSRIs are considered the most well-tolerated antidepressants, per the Mayo Clinic; they typically have fewer side effects than other types and can be safely used at higher doses. Common side effects of SSRIs include sexual dysfunction, weight gain, trouble sleeping, drowsiness, dizziness, and nausea. SNRIs are also considered fairly safe, though Dr. Dimitriu says they can sometimes cause insomnia and elevate your blood pressure.
Atypical antidepressants all come with a common side effect profile, which includes dry mouth, headaches, dizziness, nausea, and fatigue. Tricyclic antidepressants are an older class and often carry more side effects: They have what Dr. Merrill calls a strong “cross-reactivity” with other drugs, a high instance of anticholinergic effects like blurred vision, sudden drops in blood pressure, and confusion, and can result more easily in toxicity than other antidepressants.
Tricyclic antidepressants are an older class and often carry more side effects: They have what Dr. Merrill calls a strong “cross-reactivity” with other drugs, a high instance of anticholinergic effects like blurred vision, sudden drops in blood pressure, and confusion, and can result more easily in toxicity than other antidepressants.
MAOIs can be complicated because they inhibit the metabolic response to an enzyme called tyramine, which causes them to potentially interact with a significant number of foods and drugs containing tyramine. As tyramine levels in the body rise, people can experience headaches, heart problems, nausea, and visual disturbances. It can be more challenging to take these drugs safely, but they do work well for some people.
Finally, it’s important to know that starting any new antidepressant can lead to increased suicidal thoughts; while these are considered rare adverse events, they are still possible, especially in children and adolescents taking antidepressants.
It’s difficult for researchers to assess the risk of suicide related to antidepressants since there are so many factors to account for. However, one 2015 study in The BMJ found that MAOIs, atypical antidepressants, and SNRIs were more likely to result in suicide or self harm than SSRIs and tricyclic antidepressants, with the highest risks found with Remeron (mirtazapine), Effexor (venlafaxine), and Desyrel (trazodone).
If you start taking a new antidepressant and notice an increase in thoughts related to suicide or death, reach out to a healthcare professional or trusted friend or family member as soon as possible. You can also contact the National Suicide Prevention Lifeline at 1-800-273-8255 or text GO to 741741 for immediate help.
What’s the newest antidepressant on the market?
SSRIs and SNRIs are newer antidepressants among the five major classes, and
vortioxetine, or Trintellix, is one of the more recent SSRIs to come on the market, says Dr. Dimitriu. Approved by the FDA for treating major depressive disorder in 2013, it works a bit differently than other SSRIs by directly interacting with serotonin receptors.
Dimitriu. Approved by the FDA for treating major depressive disorder in 2013, it works a bit differently than other SSRIs by directly interacting with serotonin receptors.
“It touts lower sexual side effects and possibly improved cognition as its features,” Dr. Dimitriu explains. “These benefits have seen mixed results in clinical practice, [but] for people who have not responded to the older SSRIs, Trintellix may offer hope.”
RELATED: Trintellix side effects
How to find the best antidepressant for you
If you’re ready to start finding the right antidepressant for you, here are four basic steps you should take to ensure the process moves as seamlessly and quickly as possible.
1. Talk to a healthcare professional
It can be your PCP, your gynecologist, your therapist—it doesn’t matter who you talk to, just that you find a healthcare professional you’re comfortable with. If they can’t personally prescribe an antidepressant, most providers will happily refer you to someone who can or work with that healthcare provider to coordinate your care.
2. Identify your target symptoms
As you can see, different symptoms, types of depression, and co-existing factors like age and gender can determine which antidepressant might be the best fit. It’s important to know what areas you, personally, need the most help with or want to see the most improvement in. Dr. Merrill says these are called “target symptoms of depression,” and they include things like energy, appetite, concentration, and sleep.
If you struggle with energy and motivation, for example, Dr. Dimitriu says a combination drug that targets more than just serotonin may be particularly helpful: “Adding the norepinephrine piece to the SSRI helps with energy and motivation, [and] bupropion, which is a dopamine and norepinephrine reuptake inhibitor, is also good.”
RELATED: What to expect from a depression screening
3. Consider pharmacogenomic testing
One of the most fascinating medical advances in recent history is pharmacogenomic testing, which helps you identify how your body will metabolize a drug and how your brain will respond to it, says Dr. Merrill.
Merrill.
Using this testing (which involves a simple blood draw or saliva swab) can make it easier for your healthcare provider to tell which antidepressants you might have a hard time metabolizing. This is important information, because if your body can’t metabolize a drug the way it’s supposed to, it will likely either not work well or cause troublesome side effects. With testing, you might be able to identify more quickly the class of drugs that will benefit you rather than going through months of ineffective drug trials.
“If you’ve failed with one or more antidepressants, it could be reasonable to do a pharmacogenomic test to see which one you’re most likely to tolerate,” advises Dr. Merrill.
4. Discuss all depression treatment options
Unfortunately, the best antidepressant for you won’t completely cure or eliminate your depression—it’s a whole body condition that affects every part of your life, and it’s important to use antidepressants as only part of a comprehensive treatment plan.
“Sleep and exercise are essential to getting better; as a sleep specialist, we have had extraordinary breakthroughs by getting people to sleep better,” says Dr. Dimitriu. “[You have] to meet your medicine halfway…[as the saying goes], you cannot push the gas pedal if there is no gas in the tank.”
It’s also recommended to receive some type of therapy in addition to taking medication, such as psychotherapy. While drugs can alter your neurochemistry, says Dr. Merrill, they can’t change your life circumstances. You will see better results if you can address the origin of your depression and work to heal or resolve the things that contribute to it. A good therapist can assist with that, as can increasing your social support network.
“There are no silver bullets—antidepressants aren’t going to work in isolation even under the best of circumstances,” Dr. Merrill asserts. “They are modulators of the responses to what’s going on in our lives, and it really takes an all-around holistic approach [to feel better]. ”
”
RELATED: How to get therapy without insurance
How to take antidepressants safely
Once you find the right antidepressant for you, it’s important to always take it safely. Remember to:
- Take the medication every day—don’t skip doses.
- Avoid drug interactions (ask your doctor or pharmacist what foods, medications, or supplements you should avoid while taking your antidepressant).
- Don’t stop taking the medication suddenly; talk to your healthcare provider about safely discontinuing use.
- Make note or keep a diary of side effects so you can share them with your provider.
- Avoid excessive alcohol use while taking antidepressant drugs.
Above all else, be patient—it may take several months for the medication to be fully effective, so as long as you’re seeing some improvement after a few weeks, try to stay the course for a bit rather than switching medications too frequently. If you still feel your medication isn’t helping, however, please reach out to a healthcare professional for assistance.
If you still feel your medication isn’t helping, however, please reach out to a healthcare professional for assistance.
The most powerful tank in the world: Why the USSR did not adopt the IS-7
A very modest design engineer Nikolai Fedorovich Shashmurin worked in the tank design bureau of the Kirov Plant in Leningrad. He was a real tank building genius. Everyone knows the names of Joseph Kotin and Nikolai Dukhov. Only their names are associated with the appearance in the USSR of machines such as KV-1, KV-2, IS-1, IS-2, IS-3, T-10. Only meticulous researchers in the history of tank building know about Shashmurin. Although it was these tanks that appeared largely due to the engineering talent of Shashmurin. nine0003
KV-1 and KV-2 - the first heavy tanks in the world, but they had a serious drawback - they had an extremely unreliable transmission. Often the tanks broke down as soon as they left the factory gates.
Nikolai Shashmurin was able to develop a transmission no less unique than a tank, which made it possible for a heavy vehicle to move at the speeds of medium tanks and was distinguished by the highest reliability. In the spring of 1943, the KV-1S (high-speed) began to be produced. It was they, and not the T-34/76, that played a decisive role in the Battle of Kursk. The trouble was that the tankers, knowing about the problematic gearboxes of the classic KV-1, did not fully use the capabilities of the new transmission. On the Kursk Bulge, the KV-1S tanks were often amazed precisely because the drivers were afraid to turn on the high-speed mode and crawled on the battlefield like turtles. nine0003
In the spring of 1943, the KV-1S (high-speed) began to be produced. It was they, and not the T-34/76, that played a decisive role in the Battle of Kursk. The trouble was that the tankers, knowing about the problematic gearboxes of the classic KV-1, did not fully use the capabilities of the new transmission. On the Kursk Bulge, the KV-1S tanks were often amazed precisely because the drivers were afraid to turn on the high-speed mode and crawled on the battlefield like turtles. nine0003
Nevertheless, the Kremlin appreciated what Shashmurin had done, and, as he himself recalled, they gave him complete carte blanche to develop new tanks. Having assessed the technological capabilities of the then domestic production, Nikolai Fedorovich proposed a project for a heavy tank, which went down in history as the IS-2. When Stalin saw this car, brought specially to the territory of the Kremlin, he said: we will end the war on it, this is the tank of our Victory.
Encouraged by the success of the IS-2, Dukhov and Kotin set about creating the truly unique IS-3. The tank was created in record time and formally put into service even before the end of the Great Patriotic War. But he never appeared on the battlefield, even in the war with Japan. The reason is the inherent problem of heavy tanks - an extremely unreliable transmission. For some reason, Shashmurin was not involved in work on the IS-3. nine0003
The tank was created in record time and formally put into service even before the end of the Great Patriotic War. But he never appeared on the battlefield, even in the war with Japan. The reason is the inherent problem of heavy tanks - an extremely unreliable transmission. For some reason, Shashmurin was not involved in work on the IS-3. nine0003
At the end of the Great Patriotic War, engineer Shashmurin formulated the concept of a tank of limiting parameters. As the experience of World War II showed, a tank lives on the battlefield in extreme mode for a day or two. During this time, he is obliged to destroy the maximum number of enemy armored vehicles. Therefore, it must have the maximum possible protection, the maximum possible specific engine power, the maximum possible mobility and the maximum possible weapon power.
Nikolai Fedorovich independently designed and achieved the construction of a prototype tank of precisely the limiting parameters - the IS-7. At 19In 1948, this car was delivered to the Kubinka training ground, where it was tested in all respects. The results of the tests came as a shock to those who participated in them.
The results of the tests came as a shock to those who participated in them.
There are surviving memories of Yevgeny Kulchitsky, the chief tester of armored vehicles of the Ministry of Transport Engineering of the USSR. I will cite them with slight abbreviations.
"I heard a lot about the new post-war tank -" object 260 "(IS-7), I was looking forward to the start of its testing," wrote Kulchitsky. done by the designers and production workers of the Kirov Plant. It is hard to imagine. The Great Patriotic War, which ended quite recently, required a titanic effort of all forces. It seemed that no one in these conditions could switch to other tasks. But a short time passed, as it was designed and built a prototype of a new heavy tank, which, in terms of its characteristics, significantly surpassed all known examples of world tank building.0003
None of the components in the new machine were of the old design. Almost everything was applied for the first time in world practice. I was given a great honor, I was the first to sit at the levers of the new tank. It's hard to put into words my feelings. At speeds of more than 60 km/h, this heavy machine is controlled by little effort on the levers and pedals, and the gears are shifted with literally three fingers. The car handles well in all conditions. I want to sing while sitting in the driver's seat! You can't feel it on any car. A real revolution was caused by the appearance on the new tank of an ejection diesel cooling system with a capacity of more than 1000 hp. With. Wonderful car!"
I was given a great honor, I was the first to sit at the levers of the new tank. It's hard to put into words my feelings. At speeds of more than 60 km/h, this heavy machine is controlled by little effort on the levers and pedals, and the gears are shifted with literally three fingers. The car handles well in all conditions. I want to sing while sitting in the driver's seat! You can't feel it on any car. A real revolution was caused by the appearance on the new tank of an ejection diesel cooling system with a capacity of more than 1000 hp. With. Wonderful car!"
So what was so special about the IS-7? Its power was felt already in dimensions. At the same time, the tank did not look like a clumsy heavyweight. He even looked elegant, as if embodying the martial beauty of the Russian hero - Svyatogor. It was huge and very organic throughout.
Tank weight - 68 tons. Crew - 5 people. Dimensions (length, width, height) in meters: 10 x 3.4 x 2.48. Number of rollers - 7. Armament: 130 mm semi-automatic cannon, 8 machine guns. The total ammunition of cartridges - 7000, shells - 25.
The total ammunition of cartridges - 7000, shells - 25.
Diesel engine power - 1050 hp With. Power reserve - 300 km. The maximum speed is 60 km/h. The thickness of the frontal armor of the hull is 150 mm, the turret is 210 mm.
The Miracle Tank was not accepted into service, despite the rave reviews of the testers. Most likely, it was his breakthrough novelty that scared him. As a result, tank engines with a capacity of 1000 hp. With. appeared only at the end of the twentieth century, and even then gas turbine ones. But the ease with which the heavy IS-7 was controlled has not been achieved to this day.
By some miracle, the only sample of the IS-7 was not melted down, it survived, you can see it in the BTVT Museum in Kubinka.
Reference "RG"
Nikolai Fedorovich Shashmurin was born on June 26, 1910 in St. Petersburg. He worked all his life in Leningrad, at the Kirov plant. Managed to take part in the design of the T-80. He died all alone at his dacha near St. Petersburg near the village of Kuzhenkino in 1996. Eternal memory to him.
He died all alone at his dacha near St. Petersburg near the village of Kuzhenkino in 1996. Eternal memory to him.
Top 10 players from the USSR who did not play in the NHL
When the NHL expanded to 12 clubs in the 1967-68 season, many hockey players from Europe had the opportunity to prove themselves overseas.
However, this was not the case for one European country that is particularly rich in hockey talent. We are talking about the Soviet Union, whose government forbade the best players in the country to leave for the best hockey league in the world. Until 1989, not a single player from the USSR managed to go overseas and try his hand at the highest level. nine0003
The Soviet Union team, which dominated the 60s and 70s of the last century, is perhaps the strongest in history. She won nine world championships in a row from 1963 to 1971. However, attempts by scouts to lure the great Soviet hockey players were unsuccessful. In the 1983 draft, the Montreal Canadiens drafted famed goaltender Vladislav Tretiak in the hope that the best goaltender in hockey history could play for the NHL's most decorated team. However, all these attempts did not lead to anything, and Tretyak, even at the end of his career, could not go overseas. nine0003
However, all these attempts did not lead to anything, and Tretyak, even at the end of his career, could not go overseas. nine0003
NHL.com/Ru offers you the top ten Soviet hockey players who did not play a single match in the National Hockey League team:
1986, 1989, 1990, 1993), as well as a two-time Olympic champion (1988, 1992). In the World Championships and the Olympic Games, Vyacheslav played 99 matches, scoring 46 goals. He is a 1987 Canada Cup finalist. Bykov is the owner of 10 gold medals of the USSR championships as part of CSKA, with whom he also won the European Champions Cup seven times. nine0003
9. Andrey Khomutov
Together with the team of the Soviet Union, Khomutov won three Olympic awards of the highest dignity, standing on a par with the legendary heroes of the past Vitaly Viktor Kuzkin, Alexander Ragulin and Anatoly Firsov. Only six people in the world have the title of three-time Olympic hockey champions.
Andrei played 400 matches for CSKA in the USSR championships, scoring 197 goals. Together with the club he became 9-time champion of the country and won several European Champions Cups. Khomutov is the owner of the Canada Cup in 1981, as well as a 7-time world champion (1981, 1982, 1983, 1986, 1989, 1990, 1993).
8. Valery Vasiliev
One of the best defenders in the history of world hockey. In the national championships, Vasiliev played 619 matches, scoring 71 goals. In the World and European Championships, as well as in the Olympic tournaments, he played 116 meetings, scoring 18 accurate throws.
In 1973, 1977 and 1979, Valery was recognized as the best defender of the world championships and 5 times in 1974-75, 1977, 1979 and 1981 was a member of the symbolic team of the world. In 1981, Vasiliev was elected captain of the USSR national team. Canada Cup Winner 1981. With Dynamo Moscow, Valery's successes were more modest, but even after many years for Dynamo fans, he and Alexander Maltsev remain symbols of Dynamo hockey.
7. Boris Mikhailov
In the national championships, he scored 428 goals in 572 matches - more than anyone else in Soviet hockey. This result alone testifies to the highest skill of a hockey player. He has many achievements. Mikhailov - Honored Master of Sports, two-time Olympic champion, eight-time world champion, seven-time European champion, eleven-time champion of the USSR, four times in the chain of glorious army hockey players made a circle of honor with the USSR Cup and nine times after winning the European Champions Cup. In total, the hockey player scored 109 in the international arenagoals in 120 meetings.
6. Alexander Maltsev
During his brilliant career, Maltsev became world champion 9 times and twice Olympic champion. Alexander in 1970, 1972 and 1981 was named the best forward of the World and European Championships. With any coach of the national team, Maltsev found his place in its composition, he could practically play from the sheet and the right kerine, and in the center, and on the left. Thanks to his great talent, he quickly found a common language with a wide variety of teammates. Alexander (the most unique fact in the history of hockey!) at 1970, 1971, 1978 was included in the symbolic team of the world as a right striker, and in 1972 and 1981 as a center forward.
Thanks to his great talent, he quickly found a common language with a wide variety of teammates. Alexander (the most unique fact in the history of hockey!) at 1970, 1971, 1978 was included in the symbolic team of the world as a right striker, and in 1972 and 1981 as a center forward.
5. Alexander Yakushev
Yakushev was one of the best scorers of the USSR national team, which included world stars of that time and real legends of world hockey. In total, during his career, 517 goals were recorded on Yakushev's account, which allowed him to become the 7th most productive hockey player in the country at the moment in the club of Vsevolod Bobrov. In official international competitions for the SSSS team, Yakushev played in 90 meetings and scored 64 goals in them. The famous Canadian defender Bobby Orr after the 2016 Super Series called the Yak-15 the best left winger in the history of hockey.
Alexander is a two-time Olympic champion (1972, 1976), a 7-time world and European champion (1967, 1969, 1970, 1973-75, 1979), and a 3-time champion of the USSR (1967, 1969, 1976).
4. Vsevolod Bobrov
Bobrov was a unique athlete, a phenomenon that had no analogues in the history of sports. Winter 19At the age of 44, Vsevolod Bobrov began playing for the CDKA hockey team. In the fall of 1945, Bobrov was invited to play for the Moscow Dynamo football team during a tour of Great Britain, where he proved himself to be an excellent striker, hitting the opponents' gates six times. Vsevolod Bobrov is a multiple champion of the USSR in football and hockey. Olympic champion in 1956, two-time world champion and three-time European champion in ice hockey.
Bobrov played 116 matches in the USSR football championships, scoring 97 goals. In 1948 he received the title of Honored Master of Sports. In 1946-1957, he also played hockey, defending the colors of the CSKA and VVS clubs, scoring 254 goals in 130 games. For the USSR national team, he scored 89 goals in 59 games. Bobrov is the only athlete in the history of the Olympic Games who was the captain of the national football (Helsinki, 1952) and hockey (Cortina d'Ampezzo, 1956) teams.
3. Anatoly Firsov
Anatoly Firsov is a legend of Soviet hockey. He is 9-time champion of the USSR (1963-1966, 1968, 1970-1973), 4-time winner of the USSR Cup (1966-1969, 1973) and 6-time winner of the European Champions Cup (1969-1974). In the championships of the USSR, Anatoly played 474 matches, scored 344 goals. In the USSR national team (1962-1972) he played 67 matches and scored 66 goals. Firsov is a 3-time Olympic champion (1964, 1968, 1972), 8-time world champion (1964-1971) and 7-time European champion (1964-1970). He was recognized as the best hockey player of the USSR (1968, 1969, 1971), the best forward of the Olympic Games (1968) and world championships (1967, 1971), as well as the top scorer of the world championships (1967-1969, 1971).
2. Valery Kharlamov
During his 15-year career, Kharlamov played 438 matches for CSKA, scored 293 goals, played 123 matches as a member of the USSR national team at the Olympic Games and World Championships. The legendary forward is a multiple champion of the Soviet Union, a five-time winner of the USSR Cup. Kharlamov - twice Olympic champion, eight-time world champion, top scorer of the USSR Championship 1971 years old and the 1972 Olympic Games, the best hockey player of the USSR in 1972 and 1973, the best striker in the world in 1976.
The legendary forward is a multiple champion of the Soviet Union, a five-time winner of the USSR Cup. Kharlamov - twice Olympic champion, eight-time world champion, top scorer of the USSR Championship 1971 years old and the 1972 Olympic Games, the best hockey player of the USSR in 1972 and 1973, the best striker in the world in 1976.
Kharlamov is a holder of two Orders of the Red Banner of Labor, the Order of the Badge of Honor, and the medal "For Labor Valor". In recognition of Kharlamov's services to the club, he is assigned the 17th number in CSKA, his name is immortalized in the Hockey Hall of Fame in Toronto.
1. Vladislav Tretyak
Being just a 20-year-old kid, Tretyak conquered the hockey world with a great performance in the Super Series-1972. He also had a fantastic performance in the 1981 Canada Cup final, in which the Soviet team defeated the Canadians 8-1. Tretiak was named the best player in Europe three times. He was the best goalkeeper in the world from 1968 to 1984, conceding a career average of less than two goals per game.