Is derealization curable
Depersonalization-Derealization Disorder | Co-Occuring Disorder Treatment
There is no cure for depersonalization derealization disorder, but treatment can reduce distressing symptoms and even lead to full remission of the disorder.
Depersonalization-derealization disorder is a dissociative disorder that was once only vaguely understood. Advances in understanding and treating trauma-related disorders have led to improved insight into depersonalization and other dissociative disorders, which are now known to be trauma-related disorders. Depersonalization disorder treatment typically involves using one or more therapeutic interventions to address different aspects of the disorder. Individual therapy is the primary depersonalization treatment, though medications are sometimes used in conjunction with therapy to treat the disorder. While derealization is considered to be a distinct aspect of this condition, derealization treatment is incorporated fully into interventions for depersonalization.
Article at a Glance:
- Depersonalization-derealization disorder is typically treated with individual therapy and sometimes medication too.
- SSRIs and antipsychotic medications do not cure this condition but can reduce distressing symptoms.
- Therapy options include teletherapy, psychotherapy, cognitive behavioral therapy, dialectical behavioral therapy, and eye movement desensitization and reprocessing.
- Depression and anxiety are the most common co-occurring disorders alongside this condition.
- Alcohol and drug use is common among people with depersonalization-derealization disorder.
Medications for Depersonalization-Derealization Disorder
There is no depersonalization cure, but treatment can reduce distressing symptoms and even lead to full remission of the disorder. It’s important for people experiencing depersonalization or derealization to talk to a professional about their symptoms so they can begin treatment and start feeling like themselves again. Antidepressant and antipsychotic medications may be prescribed to help with symptoms of depersonalization.
Antidepressant and antipsychotic medications may be prescribed to help with symptoms of depersonalization.
Selective Serotonin Reuptake Inhibitors (SSRIs)
Most people with dissociative disorders have co-occurring conditions, and depression is one of the most common. Antidepressants, especially selective serotonin reuptake inhibitors (SSRIs), are frequently prescribed to treat comorbid depression. Popular SSRIs for dissociative disorders include:
- Sertraline (Zoloft)
- Fluoxetine (Prozac)
- Citalopram (Celexa)
These SSRIs can treat several symptoms specific to depersonalization-derealization disorder. The sense of detachment that accompanies depersonalization is often closely linked with flat affect and blunted emotion, all of which can be improved with SSRIs. Antidepressants can also stabilize mood and reduce the intrusive symptoms that trigger dissociative symptoms. Research shows that a combination of an SSRI and lamotrigine, a mood stabilizer, is an effective treatment for dissociative disorders, especially depersonalization-derealization disorder. SSRIs can also be used to treat anxiety, which is another commonly co-occurring condition with depersonalization-derealization disorder. They are often the best medical option for treating dissociative disorders with comorbid anxiety.
SSRIs can also be used to treat anxiety, which is another commonly co-occurring condition with depersonalization-derealization disorder. They are often the best medical option for treating dissociative disorders with comorbid anxiety.
Antipsychotic Medications
One of the defining features of dissociative disorders like depersonalization is that they are not psychotic disorders. People who experience them maintain an intact sense of reality. However, antipsychotic drugs can be an effective option for treating these disorders.
Antipsychotics can provide a number of desirable effects for people with depersonalization-derealization disorder, including mood stabilization, anxiety reduction, and improved range of affect. They may even target and reduce depersonalization and derealization symptoms.
Therapy for Depersonalization-Derealization Disorder
Depersonalization and derealization symptoms can make someone feel unreal. At various times, the self, body, emotions and the external world may all feel like they don’t exist or as if they are distorted or distant. The extent to which any of these symptoms are present can point to a diagnosis of depersonalization-derealization disorder.
The extent to which any of these symptoms are present can point to a diagnosis of depersonalization-derealization disorder.
There is a depersonalization-derealization disorder test a therapist may use to diagnose the disorder. While a specific test like the structured clinical interview for dissociative disorders may be used, the main depersonalization disorder test is the Steinberg Depersonalization Questionnaire. There is a similar derealization test, the Steinberg Derealization Questionnaire.
While philosophical inquiries can lead to questions about what is real, the feeling that the self and the external world aren’t real is usually a dissociative response, often one that was learned to detach from terrifying or painful traumatic experiences. The goal of any therapeutic treatment of depersonalization-derealization disorder is to help individuals regain access to their full emotional range, which often requires establishing both safety and insight.
Teletherapy
Using teletherapy, patients are matched with a licensed therapist. The therapist will work with the patient on a personalized treatment plan, guiding him or her on the path to lifelong recovery. Read more about getting started with teletherapy.
The therapist will work with the patient on a personalized treatment plan, guiding him or her on the path to lifelong recovery. Read more about getting started with teletherapy.
Psychotherapy
Psychotherapy is the general term used to describe any form of talk therapy in which a client explores their thoughts and feelings by speaking to a therapist about them.
While significant advances have been made in the pharmacotherapeutic treatment of mental health conditions, psychotherapy remains the primary and essential psychiatric intervention. This is especially true in the treatment of depersonalization-derealization disorder, which may not be fully treatable with any medication. Psychodynamic psychotherapy is one of the oldest styles of therapy. This form of therapy is now much less popular than it once was, but it still can be effective in particular therapeutic contexts.
Psychodynamic psychotherapy focuses on exploring the past to gain insight into what caused a person to think and feel in certain ways. By making the unconscious sources of emotional reactions conscious, someone with depersonalization-derealization disorder can start to understand the reasons they feel disconnected from reality and take steps to remedy this.
By making the unconscious sources of emotional reactions conscious, someone with depersonalization-derealization disorder can start to understand the reasons they feel disconnected from reality and take steps to remedy this.
Insight may be the most effective tool to treat depersonalization-derealization disorder, opening the door to once-blocked emotions. By unlearning previously unconscious ways of responding to the world, people can start to experience emotions and thoughts that they once found intolerable and that previously triggered their dissociative symptoms.
Cognitive Behavioral Therapy
Cognitive behavioral therapy (CBT) is one of the most well-researched therapeutic modalities and is considered an evidence-based practice for the treatment of many psychiatric disorders. It works by helping people identify cognitive distortions and irrational beliefs. By challenging and reframing these thoughts, people can reduce or eliminate the negative emotions and behaviors caused by them.
Individuals with depersonalization-derealization disorder usually respond well to CBT. Many symptoms of the disorder have a cognitive basis. Obsessive thinking about the self and the world intensifies feelings of unreality. People with depersonalization-derealization disorder can use CBT to examine and question thoughts that exacerbate derealization and learn grounding and breathing techniques that counteract disembodiment and other dissociative symptoms.
Dialectical Behavioral Therapy
Dialectical behavioral therapy (DBT) was developed for the treatment of borderline personality disorder, which is a trauma-related condition. DBT combines cognitive-behavioral tools and techniques with mindfulness practices and a philosophy of acceptance.
By shifting from the CBT approach of labeling certain thoughts or feelings as negative, DBT helps people with histories of abuse and trauma to explore painful emotions without guilt or shame and to feel more comfortable in sharing what they think and feel. Interventions in DBT help people develop distress tolerance and improve emotional regulation.
Interventions in DBT help people develop distress tolerance and improve emotional regulation.
This kind of behavioral therapy yields key insights and benefits for the treatment of depersonalization disorder. People with this dissociative disorder often learned to mistrust their thoughts or feelings and to label them as bad. This mistrust is what makes them feel as if these inner states or even their very selves aren’t real.
By teaching people to accept their inner states, DBT can help people reconnect to them. The mindfulness, breathing, and self-soothing techniques taught in DBT can also help people with depersonalization-derealization disorder to reconnect with their bodies and the sensations of being in the moment.
Eye Movement Desensitization and Reprocessing
Eye movement desensitization and reprocessing (EMDR) is another intervention developed specifically for people with trauma-related disorders. Its goal is to help people who have been repressing or avoiding traumatic memories, thoughts and feelings to gradually and safely process them.
In EMDR, clients talk or think about traumatic memories while tracking a back-and-forth visual or auditory cue designed to help their brains reprocess these events. While people debate the reasons this technique works, research shows that EMDR is an effective approach for people with histories of trauma, including people with depersonalization-derealization disorder.
Like CBT, EMDR can help people change their thought processes, and, like DBT, it can help them do so in a way that is nurturing and grounded in physical experience. Since this form of treatment specifically focuses on exploring trauma, it can help people who have repressed or avoided traumatic memories begin to address them in a safe environment.
Many people with symptoms of depersonalization and derealization have had experiences that caused them to invalidate their emotions and to repress thoughts and memories — traumatic or otherwise. EMDR can help them break through those defenses and feel their emotions more directly again.
Treating Depersonalization-Derealization Disorder and Co-Occurring Conditions
Most people with dissociative disorders have co-occurring conditions, with depression and anxiety being the most common. The symptoms of these disorders are deeply interconnected and are best treated simultaneously.
For example, depressive symptoms, like blunted emotions, naturally arise from the experience of depersonalization and derealization. When symptoms of derealization and depersonalization are caused by emotional abuse and trauma, they function as defenses. Anxiety can arise when repressed material starts becoming conscious.
When people have depersonalization-derealization disorder and co-occurring anxiety or depression, medication can be an especially effective tool in the therapeutic process. Taking medications is not always necessary or the best option, however, depending on the person being treated and the existence of any other comorbid medical or mental health conditions.
You can also check out the Nobu app to learn more about depersonalization-derealization disorder and other mental health topics. It is free and for anyone that is looking to reduce anxiety, work through depression, build self-esteem, get aftercare following treatment, attend teletherapy sessions and so much more. Download the Nobu app today!
Depersonalization-Derealization Disorder and Substance Abuse
Drug and alcohol use is common among people with dissociative disorders. Depersonalization-derealization disorder can drive substance abuse in one of two ways. People may take substances to intensify depersonalization and derealization symptoms as well as to further entrench their protective function. In some cases, they might use alcohol or drugs to break down dissociative defenses and feel emotions they normally can’t feel. These dynamics can quickly lead to the development of substance dependence.
The best and most effective way to treat co-occurring depersonalization-derealization and substance use disorders is to use an integrated approach. This means several interventions should be provided in a coordinated way, ideally by the same organization or treatment team.
This means several interventions should be provided in a coordinated way, ideally by the same organization or treatment team.
Many treatment centers throughout the United States, like The Recovery Village, use an integrated approach to treating drug and alcohol addiction and co-occurring disorders, including those involving depersonalization derealization disorder. To learn more about the benefits of treating co-occurring disorders, contact The Recovery Village today.
Editor – Camille Renzoni
Cami Renzoni is a creative writer and editor for The Recovery Village. As an advocate for behavioral health, Cami is certified in mental health first aid and encourages people who face substance use disorders to ask for the help they deserve. Read more
Medically Reviewed By – Stephanie Hairston, MSW
Stephanie Hairston received her Bachelor of Arts degree in Psychology and English from Pomona College and her Master of Social Work degree from New York University. Read more
Medical Disclaimer
The Recovery Village aims to improve the quality of life for people struggling with substance use or mental health disorder with fact-based content about the nature of behavioral health conditions, treatment options and their related outcomes. We publish material that is researched, cited, edited and reviewed by licensed medical professionals. The information we provide is not intended to be a substitute for professional medical advice, diagnosis or treatment. It should not be used in place of the advice of your physician or other qualified healthcare providers.
We publish material that is researched, cited, edited and reviewed by licensed medical professionals. The information we provide is not intended to be a substitute for professional medical advice, diagnosis or treatment. It should not be used in place of the advice of your physician or other qualified healthcare providers.
Is There A Depersonalization Cure? What You Need To Know (2022)
If you look at the most common Google searches related to Depersonalization Disorder, the term ‘Depersonalization Cure’ is easily the most popular.
I remember when I first developed chronic Depersonalization Disorder, I spent days, weeks, months researching every online forum and website and in every book I could find for just that: A simple, easy Depersonalization cure so that I just recover as quickly as possible.
The condition, and my research of it (which I later learned I should have avoided) took up all my attention and put my life on hold. I didn't look at social media, news, anything else.
I desperately wanted to know how to get rid of Depersonalization.
In fact, was totally consumed by the search for a Depersonalization cure. And if you're suffering from DPDR?
I bet you're already doing the exact same thing.
So in this article I’m going to save you a lot of time and frustration and tell you the answer, once and for all.
Is there a cure for Depersonalization Disorder?
The answer is
YES.And I know a lot of you are also asking - Can you get rid of Derealization too?
Again, the answer is YES! We'll get to that soon.
But first, we need to clarify the initial question.
When we ask, ‘Is Depersonalization curable?’, we need to think about what that question. What do we need cures for?
For example, if you have a cold or a headache, you can ‘cure’ them. The cold can be cured with a decongestant. The headache can be cured with aspirin.
If you have something more serious, like say, appendicitis or laryngitis, then you'll need to seek out medical help. But still -- there are definitive treatments that are guaranteed to fix the problem.
The point is, there are specific medications you can take that will CURE you of the illness. That’s the miracle of modern medicine:
You have an issue, you ask a doctor, you're prescribed a cure, you get better.
It’s a process that we pretty much take for granted!
But that doesn't apply to all medical problems.
For example, is there a cure for smoking? Is there a cure for being overweight?
Of course not. Why? Because the term ‘cure’ doesn’t apply to these things.
These are problems based on behaviours rather than being standalone illnesses. They can absolutely be reduced and stopped with therapies and treatment.
They can absolutely be reduced and stopped with therapies and treatment.
But there's no overnight 'cure' and it can be frustrating, even damaging, to think of them in that way!
A Song Stuck In Your Head
Let's look at a really simple example. If you get a song stuck in your head for a day or two and you can’t seem to get rid of it, what do you do? Well, you don’t do anything!
You go about your life, you listen to other songs and allow the annoying thought to run its course. You know that it will pass.
What you DON'T do is seek out a cure for it. You don’t go to a doctor looking for medication. You don’t spend hours and days on the internet researching the details of that song, other peoples’ experiences with similar songs.
You don’t start blogging about it. You don’t go and start discussing the roots of that song and how and why it got into your head in the first place.
Frustrated and Frightened
Why? Because you know that having a song stuck in your head is NOT a sickness.
It’s a habit, a behaviour. It will run its course naturally as you go about your life. But taking time out of your life to sit around researching it, learning about it, focusing on it intently? Of course that will only prolong it!
Now I know that's a bit of an oversimplification, but Depersonalization has a lot more in common with having a song stuck in your head than you might think. It's an anxiety-driven behaviour of thought, that's all.
It's completely different from organic conditions like schizophrenia, cancer etc. It can't hurt you and it won't turn into anything worse.
But of course, you don't know that when you first experience the bizarre thoughts and feelings of DPDR.
So just like I did, you spend entire days researching how to get rid of Depersonalization. And you want an easy, quick solution, right?
You want to know how to cure Depersonalization as immediately as possible, and find yourself frustrated and frightened when you can't find a quick answer, like you would with a flu or an allergy.
Is Depersonalization Curable?
So asking ‘Is Depersonalization curable?’ is like asking ‘Is there a cure for smoking?’ or ‘Is there a cure for for having a song stuck in your head?’
It's a totally understandable question, but it's simply not relevant to DPDR. There's no pill or medication that will cure Depersonalization overnight. But you know what? THAT'S OK!
There's no pill or medication that makes people quit smoking or get over social anxiety overnight either. But can people do these things? Of course they can, they do it every day!
There are tons of different techniques to deal with them. CBT, cognitive distancing, positive reinforcement etc etc. You probably know people who have done those things -- You may even have done them yourself!
Look -- asking 'Is there a cure for Depersonalization Disorder?' is totally understandable. Everyone asks the same thing at first. But the idea of a single 'cure' is not helpful.
There's no single cure for smoking, for obesity etc. They're behavioural conditions, just like Depersonalization, and all anxiety conditions are. But people still recover from them every single day!
They're behavioural conditions, just like Depersonalization, and all anxiety conditions are. But people still recover from them every single day!
So instead you should ask: “Can I learn how to get rid of Depersonalization? To stop thinking about it for good and recover completely?”
Because the answer to that question is YES.
How To Get Rid Of Derealization?
But what if you're suffering from Derealization more than Depersonalization? Doesn't that make your situation, and the process of recovery, completely different?
Not at all! There's a common misconception that DP and DR are completely different conditions, when in fact they are both essentially normal (and very common!) symptoms of anxiety.
If you've been searching for a Derealization cure and coming up with lots of conflicting information, don't worry. There is no practical difference between how to get rid of Derealization and Depersonalization, and they don't need to be addressed separately.
Treatment of depersonalization and derealization in St. Petersburg
- Main
- Psychiatry
- Treatment of depersonalization and derealization
We treat depersonalization and derealization in our clinic. To start the treatment of the syndrome, a face-to-face consultation with a psychiatrist and a differential examination are necessary to clarify the diagnosis and exclude / confirm diseases that cause a similar condition against the background of the course (for example, OCD, phobic and depressive disorders, delusional and dissociative disorders, early dementia). nine0011
About half of the world's population has experienced a state of depersonalization-derealization at least once in their lives. But only 2% of them fully meet the diagnostic criteria for the syndrome.
But only 2% of them fully meet the diagnostic criteria for the syndrome.
In order to shorten the period of selection of pharmacotherapy in the treatment of depersonalization and derealization, hospitalization is required (4–6 weeks). The conditions of the hospital allow you to monitor the patient's condition in dynamics and promptly adjust drug treatment. Also, in the hospital of the clinic, patients are provided with psychotherapeutic assistance, which precedes individual and / or group sessions after discharge, adapting to a full life in the family and society. nine0011
In particular, if the disease has caused intra-family conflicts, they can be resolved in family therapy sessions. In addition, participation in a group of open problems will allow you to get rid of internal experiences, restore lost communication skills. In parallel with outpatient treatment (taking prescribed drugs), one should not forget about visits to the attending physician, who should be informed of any conditions that cause anxiety or seem unusual. Such an approach to the treatment of depersonalization and derealization will make it possible to correct drug treatment in a timely manner, get rid of addictive attitudes and, as a result, prevent a relapse of the disease. nine0011
Such an approach to the treatment of depersonalization and derealization will make it possible to correct drug treatment in a timely manner, get rid of addictive attitudes and, as a result, prevent a relapse of the disease. nine0011
Doctor's consultation on the treatment of depersonalization:
+7 (812) 407-18-00
Thank you for your trust!
- Assistance in resocialization
- Safe drug therapy
- Psychologists with clinical experience
| Service | Price | |
|---|---|---|
| Psychotherapist appointment | 5 000 ₽ | nine0043|
| Family Therapy | 10 000 ₽ | |
| Hypnotherapy | 8 000 ₽ | |
| Psychiatric consultation | 5 000 ₽ Depersonalization under academic stress — https://pubmed. Update date: 12/28/2020
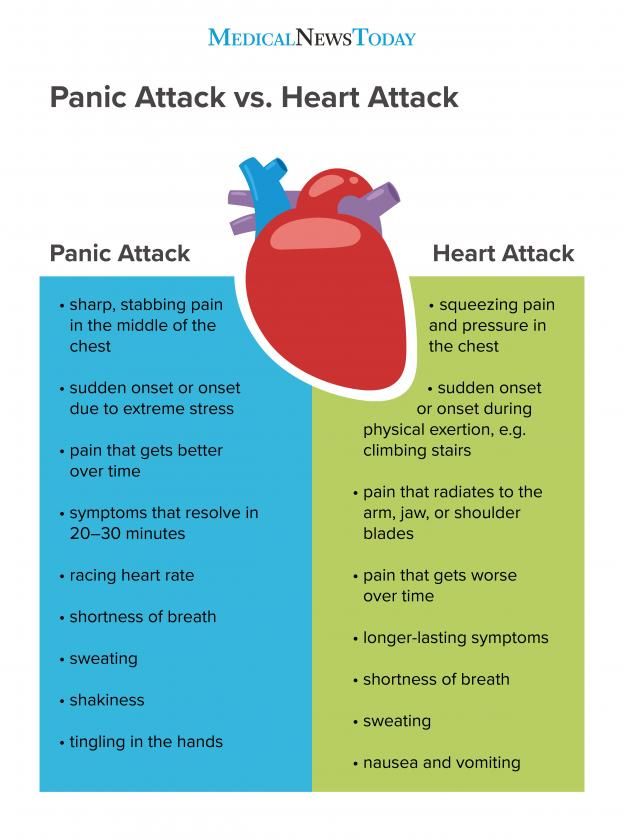
Make an appointment Date and time: (not set) Make an appointment with a psychiatrist nine0010 Make an appointment with a psychiatristSelect the date and time of your appointment Today January 14 Tomorrow January 15 Monday January 16 Tuesday January 17 Wednesday January 18 Thursday January 19 Friday January 20 Saturday January 21 Sunday January 22 Monday January 23 Tuesday January 24 Wednesday January 25 Thursday January 26 Friday January 27 Saturday January 28 Sunday January 29 Monday January 30 Tuesday January 31 Treatment of depersonalization and derealization is carried out Bocharov Alexey Psychiatrist, psychotherapist Psychiatrist, psychotherapist, sexologist, child psychiatrist Work experience 42 years Sinenchenko Andrey Psychiatrist, psychotherapist Psychiatrist, psychotherapist, narcologist Work experience 23 years Zun Sergey Psychiatrist, narcologist Psychiatrist, narcologist, psychotherapist Work experience 34 years Lisitsyna Elena Psychiatrist Psychiatrist Work experience 34 years Buchelnikova Victoria Psychiatrist Psychiatrist Work experience 16 years Voronina Elvira Psychiatrist Psychiatrist Work experience 28 years Efimova Evgenia Psychiatrist Psychiatrist Experience 20 years Gorobets Elena Psychiatrist Psychiatrist Work experience 17 years Travnikova Oksana Psychiatrist Psychiatrist Work experience 22 years nine0010 Kurochkina NadezhdaPavlovna Psychiatrist Psychiatrist Experience 20 years Suslennikova Elena Psychiatrist, psychotherapist Psychiatrist, psychotherapist Work experience 26 years Chuban Olga First category Work experience 14 years Psychiatrist, psychotherapist, psychologist Work experience 14 years Popov Andrey Psychiatrist Psychiatrist Work experience 36 years Stetsiv Lyudmila Psychiatrist, psychotherapist Psychiatrist, psychotherapist Work experience 32 years Prokhorchev Konstantin Psychiatrist, psychotherapist Psychiatrist, psychotherapist Work experience 13 years Gulevsky Roman Psychiatrist, narcologist Psychiatrist, narcologist Work experience 26 years Konoplin Dmitry Narcologist, psychiatrist Narcologist, psychiatrist Work experience 25 years Stavitskaya Svetlana Psychiatrist Psychiatrist Experience 25 years nine0010 Pylskaya AnnaNikolaevna Psychiatrist Psychiatrist Work experience 8 years Trofimova Alexandra Psychiatrist, child psychiatrist Psychiatrist, child psychiatrist Work experience 29 years Zhelobetskaya Maria Psychiatrist, psychotherapist Psychiatrist, psychotherapist Work experience 23 years Endrzheevskaya Diana Second category Work experience 15 years Psychiatrist, child psychiatrist, psychotherapist Work experience 15 years Usov Grigory Psychiatrist, psychotherapist Psychiatrist, psychotherapist Experience 25 years Ivanov Alexander Psychiatrist, narcologist Psychiatrist, narcologist Work experience 21 years Semenov Andrey Psychiatrist, narcologist Psychiatrist, narcologist, transfusiologist Work experience 24 years Leave a request for a call: +7 (812) 407-18-00 What is depersonalization and how to live with it?It happened to me Dima Kozachenko look like symptoms of depersonalization disorder, which is often confused with schizophrenia. Tatyana, 28 years old: “For the first time I encountered a feeling of unreality of what was happening when I was 22 years old. One day, I just stopped feeling any emotions; my relatives suddenly became strangers, I didn’t want to communicate with anyone, go out anywhere. I didn’t feel like myself - the personality was erased, and I became a different person: the feeling that there was no more soul, only one shell. This was accompanied by constant anxiety, soul-searching, headaches, and a sense of hopelessness. This is a terrible state when suicide seems to be the only way to stop everything. nine0011 I was very frightened and urgently called my mother, because I myself could not even go to the doctor. The neurologist at the hospital said that I was depressed and prescribed a cocktail of antidepressants and neuroleptics. Surprisingly, almost from the first days of taking the pills, I returned to life: the symptoms disappeared, my mood improved, my ability to work increased, I became sociable and open. The symptoms returned when a relative offered me a new job. There were rather high requirements for employees - a mandatory driver's license, specialized education in the field of shipping and fluent English. I was given six months to prepare. The relative paid for all the courses, the university - and then the stress began. I felt that it was covering me, so I arbitrarily returned to the pills. It got a little easier for a while. I tried my last strength not to lose face, to get this job, not to let down the person who believed in me and also spent money. But I got worse and worse, and I failed the job interview. It was a very difficult period. nine0011 After that, I began to sit on forums, google articles about mental disorders with similar symptoms. There were thoughts that I had schizophrenia and I was finally going crazy. Once on some website I saw a description of a diagnosis that exactly matched my symptoms. Then my acquaintance with depersonalization-derealization disorder began. I went to doctors, but they basically didn't know what it was and how to treat it. Sometimes they simply did not want to listen to me - they immediately prescribed medicines and sent me home. One professor said that I "read on the Internet." I found my salvation in online consultations with a doctor who dealt with dereal: according to his scheme, I started taking antidepressants and antiepileptic drugs. nine0011 The reason for my depersonalization is neurosis, which is accompanied by anxiety: under stress, the body defends itself and the brain seems to turn off, isolation from the outside world occurs. This happens to impressionable people who worry about anything, take everything to heart. My experience is 2.5 years. I know that there may be deterioration, but there is a way out. Now I have reached the stage when a new job is a joy, I feel like myself again, mental abilities, emotions and feelings are the same as before the illness. And, although I'm still on the pills, it's better than suffering again. I hope someday I can cancel them. It sounds strange, but this illness has changed me for the better. Thanks to her, I truly began to appreciate life and loved ones. Became more patient. I am glad that I can live a normal life again, feel, love, enjoy communication with people and from my favorite activities. nine0011 Our society is very contemptuous of those in need of psychological help. If they find out that a person has been to a psychiatrist, they immediately label him a psycho and avoid him. Nevertheless, you should not be afraid to seek qualified help, the main thing in this matter is to find a really good doctor. And there are very few of them. Nikolai, 27 years old: “I have been neurotic since childhood: stuttering, obsessive-compulsive disorder (obsessive thoughts syndrome). In August 2014, I went to a psychiatrist with depression and impaired perception of reality, I was then 25 years old. It all started with rare panic attacks, which were replaced by bouts of severe derealization. The world turned upside down, and I had to lie down on the floor and close my eyes, this helped to come to my senses. After another such attack, I developed anxiety. nine0011 Exactly 6 months I thrashed around looking for and inventing physical illnesses to justify my condition. Admitting to yourself that you are a little "cuckoo" is difficult, and this is how hypochondria appears. The catalyst for hypochondria is still such an unpleasant reality as unskilled medicine. The inertia coming from the USSR still persists - doctors sculpt a diagnosis of VVD (which has long been absent from the world classification of diseases), say that everything is in order, prescribe vitamins and send them home. Finally, miraculously, I managed to get to a good psychiatrist. Properly selected drugs have built a solid foundation for my recovery. Now pharmacology has reached such a level that drugs work reliably with a minimum of side effects and consequences for the body. Of course, they do not eliminate psychological problems, but they provide a runway for climbing to the height where these problems could be eliminated. The antidepressant began to noticeably act somewhere in 3-4 weeks after the start of the reception. Depersonalization is, in the usual sense, the loss of oneself; when you can't understand what kind of person you are. Recovery after this leads to a rethinking of life attitudes. For example, in the past, I limited myself, tried to conform to the ideas dictated by society. He lived according to the principle “as it should be”, and not “as I want”. During this period, the understanding of one's person is lost: who are you? why are you? who are you supposed to be? You are depersonalizing. At the turning point of frustration, you understand that you need to live for yourself, and not for others, you stop constantly looking for flaws and correcting them in order to become someone. I accepted myself. Anastasia, 20 years old: “At school, I was often bullied because of my excess weight, no one took me seriously at home, there were constant screams and scandals because of my father’s alcohol addiction. At the age of 15, I decided to try drugs and, not knowing the “correct dosages”, I took too much at one time. After that, my health deteriorated sharply: short-term panic attacks began, heart palpitations, unsteadiness of gait, dizziness appeared. At first I thought that I had something with my heart or blood vessels; over time, this developed into a fear of a heart attack, stroke, or sudden death. Then there was an examination of the whole body, but nothing concrete was found out: the doctors either did not find anything, or made a diagnosis of "vegetovascular dystonia". One doctor advised me to get tested for cancer. nine0011 Over time, the situation progressed. There was a terrible feeling inside, like anxiety: I couldn’t sleep normally, it seemed that I would die any minute. I found out that this is not schizophrenia on a website about dissociative disorder. Thus began a new phase. On VKontakte, I found a group about dereal, where there were hundreds of people like me. For about a week I sat in the community, reading information, personal stories and recommendations, until I fully understood that this was it - depersonalization-derealization disorder. In the 11th grade, everything got to the point that I was taken from the exam in an ambulance. When I went to the doctor, he started asking something, and I was silent: I was so tired of this shit that I could not say a word. My parents found out that I have serious mental problems. It seemed to me that my mother did not understand me. I was again taken to the doctors, but we failed to find an intelligent specialist. In Soviet-era hospitals, doctors are not at all familiar with depersonalization: in one of these, I was prescribed 12 dubious pills a day, and glycine was also completely useless for my symptoms. As a result, I found my psychiatrist, with whom we still keep in touch, through my mother's friend. If we talk about treatment, then you can’t do without antidepressants. They help to return to the previous mode and significantly improve the condition. Now I'm 20, and I'm still on pills: I decided that it's better to feel good with them than to think about suicide every day. “The basis of the depersonalization-derealization syndrome is an attempt of the psyche to adapt to stress in conditions of its high intensity, for example, during fear or panic. This syndrome as a separate disorder is included in the international classification of diseases (ICD-10), but often occurs as a secondary syndrome with severe anxiety, depression and other acute conditions. Depersonalization and derealization, although combined into one term due to their similarity and general nature, represent two independent symptoms that can manifest themselves separately from each other. The main cause of DP/DR lies in the activation of opiate receptors - there is an assumption that in this way the human body tries to reduce severe anxiety. Stress can become a reason if it was intense and caused a vegetative crisis (like a panic attack). Feelings during depersonalization-derealization frighten with their unusualness. It seems to the patient that he has lost control of his own body, and this in itself provokes even more intense fear. It differs from schizophrenia primarily in the absence of symptoms of psychosis (hallucinations, delusions, catatonia, etc.). Also, the DP / DR syndrome can be observed in acute psychotic episodes, but then there must be appropriate mandatory symptoms of a severe mental illness.    Copyright © · The Wright Initiative · Articles · Site Map 
|
 ncbi.nlm.nih.gov
ncbi.nlm.nih.gov  branch
branch  Afisha Daily publishes three stories of people with this terrible diagnosis. nine0011
Afisha Daily publishes three stories of people with this terrible diagnosis. nine0011  A month later, I stopped taking these drugs and did not go to the doctor again (although I was warned not to give up the drugs). For four years, I forgot about the problems. nine0011
A month later, I stopped taking these drugs and did not go to the doctor again (although I was warned not to give up the drugs). For four years, I forgot about the problems. nine0011  I started running around psychiatrists, but all of them refuted my suspicions. Depression was re-diagnosed, antidepressants were prescribed - anxiety subsided a little, but emotions and feelings never returned.
I started running around psychiatrists, but all of them refuted my suspicions. Depression was re-diagnosed, antidepressants were prescribed - anxiety subsided a little, but emotions and feelings never returned.  I am one of those.
I am one of those.  "
"  Therefore, I had to engage in self-diagnosis and be terribly afraid of what was really happening to me. Unfortunately, I made the diagnosis of "depersonalization disorder" myself, once again surfing the Internet. Through acquaintances, I managed to go to a psycho-neurological dispensary. There I was pumped with the same Soviet drugs, put on droppers, there was even a massage and a circular shower. At discharge, there were no significant results: it became easier to sleep, but the condition remained the same painful. nine0011
Therefore, I had to engage in self-diagnosis and be terribly afraid of what was really happening to me. Unfortunately, I made the diagnosis of "depersonalization disorder" myself, once again surfing the Internet. Through acquaintances, I managed to go to a psycho-neurological dispensary. There I was pumped with the same Soviet drugs, put on droppers, there was even a massage and a circular shower. At discharge, there were no significant results: it became easier to sleep, but the condition remained the same painful. nine0011  The mood improved, strength appeared, life began to bring pleasure. Then slowly: communication with friends began to recover, I began to go out, my libido and the desire to do something woke up. I recovered at work: when getting to the toilet is a huge test, work becomes something unbearable. nine0011
The mood improved, strength appeared, life began to bring pleasure. Then slowly: communication with friends began to recover, I began to go out, my libido and the desire to do something woke up. I recovered at work: when getting to the toilet is a huge test, work becomes something unbearable. nine0011 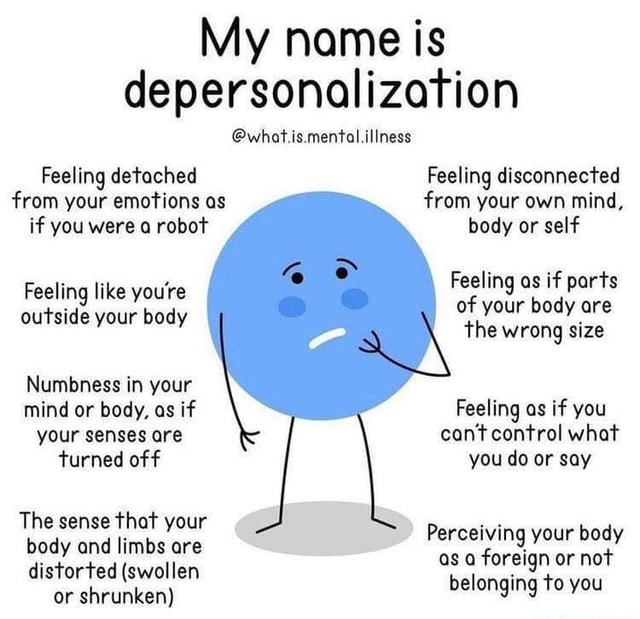 " nine0011
" nine0011  One day I realized that I did not feel my body. There was a feeling of lightness and weightlessness at the same time, and then I began to catch myself thinking that it was as if I were not there. The sensations in my hands became not mine, the reflection in the mirror was not the same. Then I realized that I was in danger not of a heart attack, but of schizophrenia. I completely surrendered to this fear: the physical symptoms disappeared, there was an indescribable horror that now I would lose touch with reality and control over myself. I began to hide the handle from the balcony so that in a fit of unconsciousness the window would not suddenly jump out. The world as I knew it was shattered. Going out into the street, I understood that there was a big barrier between me and reality. The world behind the glass seemed flat, colorless, dead. I couldn't figure out if this was a dream or reality, or maybe I had died altogether. Time just stopped, it didn't exist, it didn't exist for me. And in the soul there is emptiness, silence and no emotions.
One day I realized that I did not feel my body. There was a feeling of lightness and weightlessness at the same time, and then I began to catch myself thinking that it was as if I were not there. The sensations in my hands became not mine, the reflection in the mirror was not the same. Then I realized that I was in danger not of a heart attack, but of schizophrenia. I completely surrendered to this fear: the physical symptoms disappeared, there was an indescribable horror that now I would lose touch with reality and control over myself. I began to hide the handle from the balcony so that in a fit of unconsciousness the window would not suddenly jump out. The world as I knew it was shattered. Going out into the street, I understood that there was a big barrier between me and reality. The world behind the glass seemed flat, colorless, dead. I couldn't figure out if this was a dream or reality, or maybe I had died altogether. Time just stopped, it didn't exist, it didn't exist for me. And in the soul there is emptiness, silence and no emotions. nine0011
nine0011  There were doctors who were more interested in my outlook on life than my health. nine0011
There were doctors who were more interested in my outlook on life than my health. nine0011  During depersonalization, the patient's own face, figure, smile, speech seem unfamiliar, as if you are watching yourself as an outsider. Derealization, on the other hand, concerns the perception of the environment: place, time, circumstances, etc. Sometimes a feeling of “drunkenness”, “unreality” and “floating picture” is added. nine0011
During depersonalization, the patient's own face, figure, smile, speech seem unfamiliar, as if you are watching yourself as an outsider. Derealization, on the other hand, concerns the perception of the environment: place, time, circumstances, etc. Sometimes a feeling of “drunkenness”, “unreality” and “floating picture” is added. nine0011