Light that helps with depression
SAMHSA’s National Helpline | SAMHSA
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Main page content
-
SAMHSA’s National Helpline is a free, confidential, 24/7, 365-day-a-year treatment referral and information service (in English and Spanish) for individuals and families facing mental and/or substance use disorders.
Also visit the online treatment locator.
SAMHSA’s National Helpline, 1-800-662-HELP (4357) (also known as the Treatment Referral Routing Service), or TTY: 1-800-487-4889 is a confidential, free, 24-hour-a-day, 365-day-a-year, information service, in English and Spanish, for individuals and family members facing mental and/or substance use disorders.
This service provides referrals to local treatment facilities, support groups, and community-based organizations.
Also visit the online treatment locator, or send your zip code via text message: 435748 (HELP4U) to find help near you. Read more about the HELP4U text messaging service.
The service is open 24/7, 365 days a year.
English and Spanish are available if you select the option to speak with a national representative. Currently, the 435748 (HELP4U) text messaging service is only available in English.
In 2020, the Helpline received 833,598 calls. This is a 27 percent increase from 2019, when the Helpline received a total of 656,953 calls for the year.
The referral service is free of charge. If you have no insurance or are underinsured, we will refer you to your state office, which is responsible for state-funded treatment programs. In addition, we can often refer you to facilities that charge on a sliding fee scale or accept Medicare or Medicaid. If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
The service is confidential. We will not ask you for any personal information. We may ask for your zip code or other pertinent geographic information in order to track calls being routed to other offices or to accurately identify the local resources appropriate to your needs.
No, we do not provide counseling. Trained information specialists answer calls, transfer callers to state services or other appropriate intake centers in their states, and connect them with local assistance and support.
-
Suggested Resources
What Is Substance Abuse Treatment? A Booklet for Families
Created for family members of people with alcohol abuse or drug abuse problems. Answers questions about substance abuse, its symptoms, different types of treatment, and recovery. Addresses concerns of children of parents with substance use/abuse problems.
Addresses concerns of children of parents with substance use/abuse problems.It's Not Your Fault (NACoA) (PDF | 12 KB)
Assures teens with parents who abuse alcohol or drugs that, "It's not your fault!" and that they are not alone. Encourages teens to seek emotional support from other adults, school counselors, and youth support groups such as Alateen, and provides a resource list.After an Attempt: A Guide for Taking Care of Your Family Member After Treatment in the Emergency Department
Aids family members in coping with the aftermath of a relative's suicide attempt. Describes the emergency department treatment process, lists questions to ask about follow-up treatment, and describes how to reduce risk and ensure safety at home.Family Therapy Can Help: For People in Recovery From Mental Illness or Addiction
Explores the role of family therapy in recovery from mental illness or substance abuse. Explains how family therapy sessions are run and who conducts them, describes a typical session, and provides information on its effectiveness in recovery.
For additional resources, please visit the SAMHSA Store.
Last Updated: 08/30/2022
SAMHSA Behavioral Health Treatment Services Locator
HomeWelcome to the Behavioral Health Treatment Services Locator, a confidential and anonymous source of information for persons seeking treatment facilities in the United States or U.S. Territories for substance use/addiction and/or mental health problems.
PLEASE NOTE: Your personal information and the search criteria you enter into the Locator is secure and anonymous. SAMHSA does not collect or maintain any information you provide.
Please enter a valid location.
please type your address
-
FindTreatment.
 gov
gov Millions of Americans have a substance use disorder. Find a treatment facility near you.
-
988 Suicide & Crisis Lifeline
Call or text 988
Free and confidential support for people in distress, 24/7.
-
National Helpline
1-800-662-HELP (4357)
Treatment referral and information, 24/7.

-
Disaster Distress Helpline
1-800-985-5990
Immediate crisis counseling related to disasters, 24/7.
- Overview
- Locator OverviewLocator Overview
- Locator OverviewLocator Overview
- Finding Treatment
- Find Facilities for VeteransFind Facilities for Veterans
- Find Facilities for VeteransFind Facilities for Veterans
- Facility Directors
- Register a New FacilityRegister a New Facility
- Register a New FacilityRegister a New Facility
- Other Locator Functionalities
- Download Search ResultsDownload Search Results
- Use Google MapsUse Google Maps
- Print Search ResultsPrint Search Results
- Use Google MapsUse Google Maps
- Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
 Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). - Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). Find programs providing methadone for the treatment of opioid addiction (heroin or pain relievers).
The Locator is authorized by the 21st Century Cures Act (Public Law 114-255, Section 9006; 42 U.S.C. 290bb-36d). SAMHSA endeavors to keep the Locator current. All information in the Locator is updated annually from facility responses to SAMHSA’s National Substance Use and Mental Health Services Survey (N-SUMHSS). New facilities that have completed an abbreviated survey and met all the qualifications are added monthly. Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Light therapy against depression - Bipolar.su
Ordinary sunlight or a special lamp can improve depression. This is called light therapy. A member of our community has prepared a review of publications on what light therapy is and how it helps with bipolar disorder and seasonal affective disorder.
Personal experience prompted me to write this article. For as long as I can remember, summer has been the best time of my life. As a child, as a student, this could be attributed to the holidays, which everyone enjoys without exception. Then somehow it became more difficult to tie to the holidays - the holidays were no longer with me, but the habit of rejoicing remained. In summer, everything is easy, everything is simple, everything is fast, there is no time to even sleep, and you don’t feel like it. Then comes the golden autumn, then not very golden, and then not golden at all, but slushy, dreary and dark. Everything around becomes dull and gray, meaningless and useless, and you feel that your life is meaningless, useless, so the best thing is to go to the kitchen, have a big snack on buns and go to sleep. Preferably until spring, so as not to hear those idiots who offer you to cheer up. nine0003
In summer, everything is easy, everything is simple, everything is fast, there is no time to even sleep, and you don’t feel like it. Then comes the golden autumn, then not very golden, and then not golden at all, but slushy, dreary and dark. Everything around becomes dull and gray, meaningless and useless, and you feel that your life is meaningless, useless, so the best thing is to go to the kitchen, have a big snack on buns and go to sleep. Preferably until spring, so as not to hear those idiots who offer you to cheer up. nine0003
It is impossible to force yourself to get up in the morning and start some kind of meaningful activity, everything and everyone around you infuriates. The only good news is the opportunity to go to bed early and try to fall asleep. Then once - and a snowball falls, then another, then everything turns white, and somehow life gets a little better. But soon the snow turns gray, fades, and there, and again, everything acquires a yellow-blue hue, like a boiled yolk. And so on until the summer. And then the cycle repeats. And only many years later I learned that seasonal affective disorder combined with bipolar disorder is not only what I saw in others, but also what I myself have. nine0003
And so on until the summer. And then the cycle repeats. And only many years later I learned that seasonal affective disorder combined with bipolar disorder is not only what I saw in others, but also what I myself have. nine0003
If you recognize yourself in winter, take my word for it - this is not the norm. It's time for you to go to the doctor. You very likely have seasonal affective disorder, as detailed by Dr. Rosenthal in 1984(1). And if in the summer everything is just as wonderful for you as it is for me, then go all the more so, bipolar affective disorder combined with seasonal is no better.
The fact that the length of the daylight hours affects our activity has been known since ancient times(2). The Chinese physician Wong Tei wrote 4700 years ago that a person's mood is connected with the season. Hippocrates associated melancholy with winter and mania with summer, and many other physicians, ancient and not so, drew attention to the connection of mood with the seasons. nine0003
nine0003
There are many hypotheses for SAD (Seasonal Affective Disorder), but the exact cause is unknown. It is believed that the less sun a person sees, the worse a part of the brain called the hypothalamus works for him. It is responsible for many brain functions, including our emotions. Melatonin is overproduced, causing drowsiness, and serotonin, on the contrary, is produced in smaller amounts, which causes a decrease in mood, and these are just some of the possible mechanisms for the development of SAD. The main reason is the lack of sunlight. nine0003
By the way, not only people suffer from SAD. If animals leading a predominantly diurnal lifestyle (humans, for example, or grass rats) are deprived of bright light for a long time, they will somehow develop a depressive state (3). In grass mice, which were placed in an environment with a dim, “winter” light, memory, learning ability worsened, signs of anxiety and depression appeared. Even mice with a lack of sunlight become depressed. What can we say about a person ... At the same time, in mice, no connection was found with circadian rhythm disorders, on which seasonal depression depends, in this study. nine0003
What can we say about a person ... At the same time, in mice, no connection was found with circadian rhythm disorders, on which seasonal depression depends, in this study. nine0003
According to one theory, depression can develop when the circadian rhythm (that is, the change of day and night) and periods of sleep and wakefulness do not match. In other words, a person is forced to go to bed and wake up not in accordance with his biological rhythm, but at an imposed time (not a word about an alarm clock!). This idea is based on the theory of light therapy, which aims to restore the circadian rhythm and thus bring a person out of depression. But the level of illumination, which is necessary for this, turned out to be much higher than in natural conditions. So it's not just about circadian rhythms. But whatever it is, light therapy works well for SAD (4). nine0003
But depression is not limited to SAD. Depression may not be related to the length of daylight hours, and then the question remains: will additional light help such people? And if a person has not just SAD, but bipolar affective disorder?
If he has periods of autumn depression followed by periods of hypo- or manic state in summer? Will he then switch from depression to mania, that is, will the light harm him? In search of answers to these questions, scientists have come to the conclusion that there is no damage due to bright light, but there is a benefit for people with depression. Several studies have recently been published that studied the effect of bright light on depression in bipolar disorder. nine0003
Several studies have recently been published that studied the effect of bright light on depression in bipolar disorder. nine0003
A study was conducted at Chicago Northwestern University where light was used not in the morning but in the afternoon (5). The original plan was to compare morning bright white light with soft red light, but three of the first four patients treated with bright light developed hypomania. The researchers decided that light therapy in the morning might be to blame, and moved the treatment time to the afternoon hours.
They assumed that it would be ineffective, because a person sees the light during the day, unless he lives underground or in the conditions of the polar night. nine0003
It turned out that a bright white lamp significantly alleviated depression in 68% of patients, and a red one only in 22%, which was consistent with the results of other studies with morning light therapy. It is noteworthy that no one developed hypomania during treatment.
Very similar results were obtained in Turkey (6) and China (7), where it was confirmed that bright light in patients with depression increased the effect of antidepressants in both unipolar depression and bipolar disorder, including in patients without seasonality (8) The table below compares the illuminance with different light sources
Although people have known since ancient times that sunlight affects mood, this type of treatment is not fully understood. In Holland, a group of scientists decided to find out whether the effect of light on mood depends on the spectrum of this light (10).
A cloudy day is bad not only because it has little light as such, but also because there is practically no ultraviolet in the radiation. Of course, it is not good for the eyes at all. But was it worth testing the hypothesis of whether dim blue light of just 100 lux is useful for people with depression? nine0003
It turned out that yes, in the study it turned out to be as effective as bright. Unfortunately, there are no definitive recommendations on how and when to properly use a bright lamp. Some people, including psychiatrists and psychotherapists, still have questions about the safety of bright light treatment for the eyes.
A team from the Free University of Amsterdam reviewed 43 scientific articles reporting various adverse events in patients treated with light therapy for various reasons, including depression and bipolar disorder (11). nine0003
In theory, light therapy can be dangerous to the eyes because it can damage the retina with HEV radiation (HEV radiation, or blue light, high-energy visible light) - this is high-frequency high-energy light in the visible spectrum in the range from 400 to 500 nm. No other parts of the eye (lens, cornea, etc.) are affected. During light therapy, some patients (up to 45%) complained of discomfort and visual disturbances, regardless of the dose of light therapy.
No other parts of the eye (lens, cornea, etc.) are affected. During light therapy, some patients (up to 45%) complained of discomfort and visual disturbances, regardless of the dose of light therapy.
However, in part of the studies, there were more complaints in patients treated with dim red light than in those treated with bright white light. In other experiments, on the contrary, bright light was tolerated worse. In some studies, bright light at 10,000 lux did not cause any discomfort, and in others, people complained of discomfort at an intensity of only 400 lux. nine0003
Researchers evaluated the effect of light therapy on the eye's light sensitivity and found that exposure to brighter white light temporarily reduced sensitivity to red light, while exposure to less intense red light increased red light sensitivity.
Both are normal. There are practically no complications from light therapy in people who do not have eye diseases. An exception is complications when taking photosensitizing drugs (photosensitization is an increase in the sensitivity of the body, more often the skin and mucous membranes, to the action of light radiation when taking certain drugs, such as antibiotics). nine0003
nine0003
The only reliable case of damage to the retina during light therapy was recorded in a patient who took the antidepressant clomipramine (anafranil), among the side effects of which is photosensitivity.
It is safe to say that bright light treatment is safe for the eyes. Dr. Carl Aiken, director of the Center for Mood Disorders at Wake Forest University (USA), recommends the use of large lamps with a brightness of at least 2,000 lux with a UV filter to protect the eyes 12. The session is best done during the day, from 12 to 14 hours. It is better to sit half a meter from the lamp, but not directly opposite it, but obliquely, at an angle of 45 degrees. At the same time, you can do the usual things (eat, work, watch TV). The lamp should be changed every three years. nine0003
In any case, you should only start light therapy after consulting your doctor. Although sunlight is beneficial for health, light therapy for bipolar disorder is not fully understood and should be approached with caution. 1. Rosenthal, N. E. et al. Seasonal affective disorder. A description of the syndrome and preliminary findings with light therapy. nine0129 Arch. Gen. Psychiatry 41, 72–80 (1984).
1. Rosenthal, N. E. et al. Seasonal affective disorder. A description of the syndrome and preliminary findings with light therapy. nine0129 Arch. Gen. Psychiatry 41, 72–80 (1984).
2. Geoffroy, P. A., Schroder, C. M. & Bourgin, P. Light treatment in depression: An antique treatment with new insights. Sleep Med. Rev. 40, 218–219 (2018).
3. Yan, L., Lonstein, J. S. & Nunez, A. A. Light as a modulator of emotion and cognition: Lessons learned from studying a diurnal rodent. Horm. behavior. (2018). doi:10.1016/j.yhbeh.2018.09.003
4. Nussbaumer, B. et al. nine0130 Light therapy for preventing seasonal affective disorder. Cochrane Database Syst. Rev. (2015). doi:10.1002/14651858.CD011269.pub2
5. Sit, D.K. et al. Adjunctive Bright Light Therapy for Bipolar Depression: A Randomized Double-Blind Placebo-Controlled Trial. Am. J. Psychiatry 175, 131–139 (2018).
6. Yorguner Kupeli, N., Bulut, N. S., Carkaxhiu Bulut, G., Kurt, E. & Kora, K. Efficacy of bright light therapy in bipolar depression. nine0129 Psychiatry Res. 260, 432–438 (2018).
7. Zhou, T. et al. Clinical efficacy, onset time and safety of bright light therapy in acute bipolar depression as an adjunctive therapy: A randomized controlled trial. J. Affect. Discord. 227, 90–96 (2018).
8. Penders, T. M. et al. Bright Light Therapy as Augmentation of Pharmacotherapy for Treatment of Depression: A Systematic Review and Meta-Analysis. Prim. Care Companion CNS Disord. nine0130 18, (2016).
9. Leahy, L. G. Overcoming Seasonal Affective Disorder. J. Psychosoc. Nurs. Ment. Health Service 55, 10–14 (2017).
10. Meesters, Y., Duijzer, W. B. & Hommes, V. The effects of low-intensity narrow-band blue-light treatment compared to bright white-light treatment in seasonal affective disorder. J. Affect. Discord. 232, 48–51 (2018).
11. Brouwer, A. et al. Light therapy: is it safe for the eyes? Acta Psychiatr. Scand. 136, 534–548 (2017).
et al. Light therapy: is it safe for the eyes? Acta Psychiatr. Scand. 136, 534–548 (2017).
12. Aiken, C. How to Use Light Therapy in Bipolar Disorder | Psychiatric Times. Available at: http://www.psychiatrictimes.com/. (Accessed: 17th December 2018)
Bright light helps with depression
Summary. New study finds evidence that bright light therapy is even more effective than antidepressants
Major depressive disorder is a fairly common problem affecting about 5% of the world's population. Approximately 14% of people from the entire population experience depression at least once during their lives. At the same time, according to the report of the World Health Organization, according to the burden of common diseases in the world, depression is one of the main causes of disability. nine0003
Treatment for major depressive disorder includes antidepressants and psychotherapy, but these are often not sufficient to achieve remission.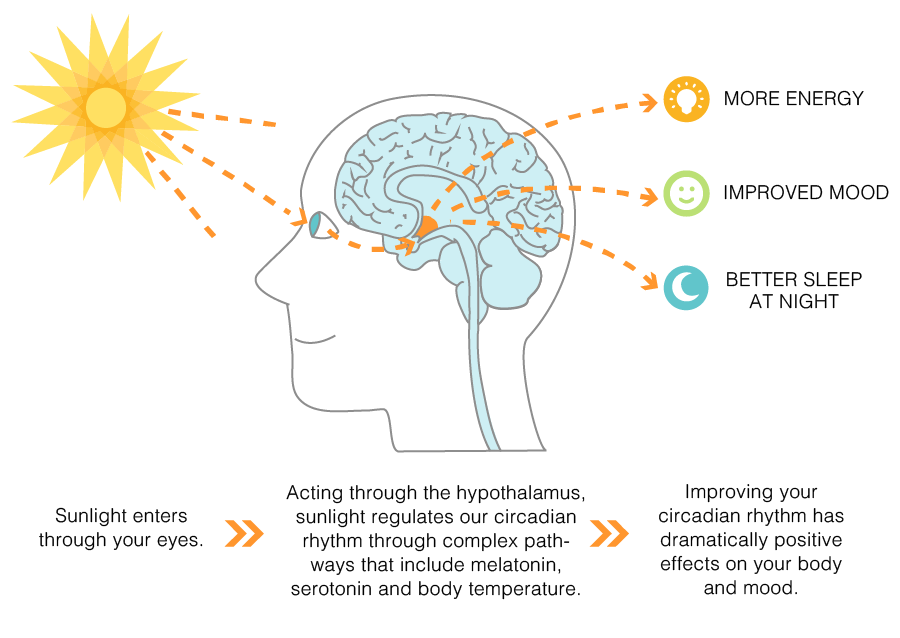
Bright light may be an effective treatment option for depression, according to a new study by a team of researchers from the University of British Columbia, Canada. As you know, such treatment is already used for the so-called seasonal affective disorder. The principle of its action is to correct the circadian rhythm, which is disturbed in this pathology. nine0003
The study itself was a randomized, placebo-controlled clinical trial design with 122 patients. The subjects were randomly divided into 4 groups with the appointment of light therapy, fluoxetine, their combination or placebo. Experimental treatment was carried out by exposing patients to fluorescent light emitted by a special box-shaped apparatus for 30 minutes immediately after waking up. Usually such a procedure was carried out between 7 and 8 o'clock in the morning. nine0003
Fluoxetine (a drug from the group of selective serotonin reuptake inhibitors) at a dose of 20 mg once in the morning was used as pharmacotherapy.
Patients were assessed using valid scales: the Montgomery-Asberg Depression Rating Scale (MADRS), the Hamilton Depression Rating Scale (HAM-D), and the Short Depression Symptom Inventory (Quick Inventory of Depressive Symptomatology - Self Report - QIDS-SR). nine0003
Over 8 weeks of treatment, patients showed an improvement: a decrease in MADRS scores of 16.9 points in the combination therapy group, 13.4 points in the light therapy group, 6.5 points in the placebo group and 8.8 points in the in the fluoxetine group. Differences were statistically significant between light therapy and placebo (p=0.006), combination therapy and placebo (p<0.001), but not between light therapy and fluoxetine (p=0.32). A clinically significant response to therapy (a decrease in the number of MADRS scores by ≥50% compared with baseline values) was observed in 33.3; 29.0; 50% and 75.9% of patients in the placebo, fluoxetine, light therapy, and combination therapy groups, respectively.
As the researchers note, this antidepressant effect of bright light may be due to the fact that circadian rhythm disturbance plays an important role in the pathogenesis of major depressive disorder, as well as seasonal affective disorder.







![]()
Copyright © · The Wright Initiative · Articles · Site Map
