Magnesium attention deficit disorder
Kids, ADHD, and Magnesium: Everything You Should Know
Even if your kids are the most adventurous eaters, beans, dark, leafy greens, and fish can often be a hard sell to kids, meaning it’s even more difficult for them to get the magnesium they need, whether or not they have ADHD.
Studies dating back to the 1920’s show that magnesium plays a significant role in mental health and psychiatric care of all kinds, which is why it comes as no surprise that magnesium is often prescribed to children who struggle with certain symptoms of Attention Deficit Hyperactivity Disorder (ADHD).
Magnesium deficiency leads to trouble concentrating, sleep problems, and muscle twitches even for those without ADHD, so the added factor of having such a condition complicates life in many ways for kids. Because of its little known effects on the brain and nervous system, magnesium is thought to be a multifaceted approach to treating ADHD in children.
What Does ADHD in Children Look Like?
There are some misconceptions about how ADHD presents itself in children. It’s important to note that ADHD is a condition that must be diagnosed, and not an adjective for an energetic little munchkin!
An active child ≠ a child with ADHD.
On average, ADHD will affect about 5% of school-aged children. The primary symptoms are related to difficulty controlling attention, and regulating behaviour and activity levels (impulsivity/hyperactivity).
ADHD is caused by a unique blend of genetics and environmental conditions. It tends to run in families, so it’s not uncommon for parents of children with ADHD to have some form of the condition themselves.
Different Symptoms for Different People
Historically, ADHD has been more common in boys, or at least, more readily diagnosed in boys. This is suspected to be because of the difference in the way the condition presents itself in boys compared to their female counterparts. ADHD symptoms in girls and women are more subtle, and thus harder to identify. In boys they tend to be very obvious and external, e. g impulsivity, lack of focus, etc.
g impulsivity, lack of focus, etc.
Research has shown this parallel difference in symptoms, concluding that where boys show externalized symptoms, girls show internalized symptoms such as low self esteem and inattentiveness. Additionally, girls tend to lean towards being more verbally aggressive, instead of being physically aggressive, which is common for boys. It is these subtle differences that make it harder for girls and women to be diagnosed and treated, and can lead to more behaviour complications and other symptoms.
Trademark ADHD Symptoms in Boys:
- Inability to focus, sit still, and be attentive
- Impulsivity, “acting out”
- Regularly interrupting the conversations and activities of others
- Hyperactivity, e.g running and hitting
- Talking excessively
ADHD Symptoms in Girls
- Anxiety and seeming withdrawn
- Inability to focus, tendency to daydream
- Difficulty with academic achievement
- Low self-esteem
- Verbal aggression, e.
 g teasing or name-calling
g teasing or name-calling
Hyperactive symptoms (more often characteristic of boys) are much easier to identify than inattentive symptoms (more often characteristic of girls).
Girls or others who don’t exhibit the best known symptoms are often misdiagnosed with a learning disability; or the issue is passed off as one of low motivation or work ethic because these lesser-known signs of ADHD aren’t recognized.
Treatment of the condition, no matter what your child’s symptoms are, is imperative in order to prevent or lessen difficulty in the future with work, school, and relationships. Additionally, people with ADHD are at a higher risk of developing other disorders such as anxiety, depression, or a learning disability, and a combination of treatments can help lessen that possibility.
How Magnesium Helps
Magnesium could be helpful for children with ADHD because it plays a role in brain health. This essential mineral regulates numerous hormones that can influence mood and neurological health.
For ADHD patients in particular, magnesium helps by acting as a gatekeeper between certain neurotransmitters and their receptors. Glutamate is the best example of this.
Glutamate is an excitatory neurotransmitter whose primary job is to get other cells in the brain excited and ready to perform important tasks like learning new things or forming memories.
However, excess glutamate can over-excite neurons and lead to cell death. Too much glutamate even in those who don’t have ADHD can result in restlessness, insomnia, and anxiety, not to mention ADHD-like symptoms such as trouble focusing. Excess glutamate could exacerbate these symptoms for children with ADHD.
That’s where magnesium comes in.
In order to apply its effects to the body, glutamate must bind with its receptor, called NMDA. Because too much activation can happen easily, the brain needs a tool to regulate the interaction between glutamate and the NMDA receptor. Magnesium is that tool. Magnesium regulates glutamate activation by inhibiting the NMDA receptor, so that the amount of glutamate available is limited. This helps us stay calm and collected.
Magnesium regulates glutamate activation by inhibiting the NMDA receptor, so that the amount of glutamate available is limited. This helps us stay calm and collected.
Studies have found that supplementing magnesium in conjunction with vitamin B6 (both of which are included in Calm Balance) leads to significantly improved anxiety, attention, and hyperactivity, as well as increased attention, work productivity, and task performance.
Natural supplements like magnesium and B vitamins are often used to treat ADHD as part of a combination that may also include therapy or other medications. If you think you or your child may need ADHD treatment, consult a healthcare professional in order to get a diagnosis and begin the best treatment method for you.
Sources:
Magnesium: The Missing Link in Mental Health? – James Greenblatt, MD
Magnesium supplementation in children with attention deficit hyperactivity disorder
07/16/13: Magnesium: The mind mineral
Attention deficit hyperactivity disorder (ADHD)
ADHD Symptoms Differ in Boys and Girls
Finally Focused: Mineral Imbalances & ADHD (Part 2: Magnesium Deficiency)
https://www. verywellhealth.com/gaba-glutamate-fibromyalgia-chronic-fatigue-716010
verywellhealth.com/gaba-glutamate-fibromyalgia-chronic-fatigue-716010
Effect of Vitamin D and Magnesium Supplementation on Behavior Problems in Children with Attention-Deficit Hyperactivity Disorder
1. Sadock BJ, Sadock VA. Kaplan & Sadock's Comprehensive Textbook of Psychiatry. 9th ed. London: Williams & Wilkins; 2009. pp. 3561–72. [Google Scholar]
2. Thomas R, Sanders S, Doust J, Beller E, Glasziou P. Prevalence of attention-deficit/hyperactivity disorder: A systematic review and meta-analysis. Pediatrics. 2015;135:e994–1001. [PubMed] [Google Scholar]
3. Polanczyk GV, Willcutt EG, Salum GA, Kieling C, Rohde LA. ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. Int J Epidemiol. 2014;43:434–42. [PMC free article] [PubMed] [Google Scholar]
4. Mohammadi MR, Ahmadi N, Salmanian M, Asadian-Koohestani F, Ghanizadeh A, Alavi A, et al. Psychiatric disorders in Iranian children and adolescents. Iran J Psychiatry. 2016;11:87–98. [PMC free article] [PubMed] [Google Scholar]
2016;11:87–98. [PMC free article] [PubMed] [Google Scholar]
5. Klassen AF, Miller A, Fine S. Health-related quality of life in children and adolescents who have a diagnosis of attention-deficit/hyperactivity disorder. Pediatrics. 2004;114:e541–7. [PubMed] [Google Scholar]
6. Frazier TW, Youngstrom EA, Glutting JJ, Watkins MW. ADHD and achievement: Meta-analysis of the child, adolescent, and adult literatures and a concomitant study with college students. J Learn Disabil. 2007;40:49–65. [PubMed] [Google Scholar]
7. Biederman J, Fried R, Petty C, Mahoney L, Faraone SV. An examination of the impact of attention-deficit hyperactivity disorder on IQ: A large controlled family-based analysis. Can J Psychiatry. 2012;57:608–16. [PubMed] [Google Scholar]
8. Hinshaw SP. Externalizing behavior problems and academic underachievement in childhood and adolescence: Causal relationships and underlying mechanisms. Psychol Bull. 1992;111:127–55. [PubMed] [Google Scholar]
9. Biederman J, Faraone SV. The effects of attention-deficit/hyperactivity disorder on employment and household income. MedGenMed. 2006;8:12. [PMC free article] [PubMed] [Google Scholar]
Biederman J, Faraone SV. The effects of attention-deficit/hyperactivity disorder on employment and household income. MedGenMed. 2006;8:12. [PMC free article] [PubMed] [Google Scholar]
10. Thapar A, Langley K, Asherson P, Gill M. Gene-environment interplay in attention-deficit hyperactivity disorder and the importance of a developmental perspective. Br J Psychiatry. 2007;190:1–3. [PubMed] [Google Scholar]
11. Mash EJ, Barkley RA. Assessment of Childhood Disorders. 4th ed. New York: Guilford Publications; 2012. [Google Scholar]
12. Milte CM, Parletta N, Buckley JD, Coates AM, Young RM, Howe PR, et al. Eicosapentaenoic and docosahexaenoic acids, cognition, and behavior in children with attention-deficit/hyperactivity disorder: A randomized controlled trial. Nutrition. 2012;28:670–7. [PubMed] [Google Scholar]
13. Nigg JT, Lewis K, Edinger T, Falk M. Meta-analysis of attention-deficit/hyperactivity disorder or attention-deficit/hyperactivity disorder symptoms, restriction diet, and synthetic food color additives. J Am Acad Child Adolesc Psychiatry. 2012;51:86–97. [PMC free article] [PubMed] [Google Scholar]
J Am Acad Child Adolesc Psychiatry. 2012;51:86–97. [PMC free article] [PubMed] [Google Scholar]
14. Arnold LE, Bozzolo H, Hollway J, Cook A, DiSilvestro RA, Bozzolo DR, et al. Serum zinc correlates with parent- and teacher – Rated inattention in children with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2005;15:628–36. [PubMed] [Google Scholar]
15. Ghanizadeh A. A systematic review of magnesium therapy for treating attention deficit hyperactivity disorder. Arch Iran Med. 2013;16:412–7. [PubMed] [Google Scholar]
16. Goksugur SB, Tufan AE, Semiz M, Gunes C, Bekdas M, Tosun M, et al. Vitamin D status in children with attention-deficit-hyperactivity disorder. Pediatr Int. 2014;56:515–9. [PubMed] [Google Scholar]
17. Kamal M, Bener A, Ehlayel MS. Is high prevalence of Vitamin D deficiency a correlate for attention deficit hyperactivity disorder? Atten Defic Hyperact Disord. 2014;6:73–8. [PubMed] [Google Scholar]
18. Gröber U, Schmidt J, Kisters K. Magnesium in prevention and therapy. Nutrients. 2015;7:8199–226. [PMC free article] [PubMed] [Google Scholar]
Magnesium in prevention and therapy. Nutrients. 2015;7:8199–226. [PMC free article] [PubMed] [Google Scholar]
19. Archana E, Pai P, Prabhu BK, Shenoy RP, Prabhu K, Rao A, et al. Altered biochemical parameters in saliva of pediatric attention deficit hyperactivity disorder. Neurochem Res. 2012;37:330–4. [PubMed] [Google Scholar]
20. Mahmoud MM, El-Mazary AA, Maher RM, Saber MM. Zinc, ferritin, magnesium and copper in a group of Egyptian children with attention deficit hyperactivity disorder. Ital J Pediatr. 2011;37:60. [PMC free article] [PubMed] [Google Scholar]
21. Nogovitsina OR, Levitina EV. Neurological aspect of clinical symptoms, pathophysiology and correction in attention deficit hyperactivity disorder. Zh Nevrol Psikhiatr Im S S Korsakova. 2006;106:17–20. [PubMed] [Google Scholar]
22. Mousain-Bosc M, Roche M, Polge A, Pradal-Prat D, Rapin J, Bali JP, et al. Improvement of neurobehavioral disorders in children supplemented with magnesium-Vitamin B6. I. Attention deficit hyperactivity disorders. Magnes Res. 2006;19:46–52. [PubMed] [Google Scholar]
Magnes Res. 2006;19:46–52. [PubMed] [Google Scholar]
23. Mousain-Bosc M, Roche M, Rapin J, Bali JP. Magnesium VitB6 intake reduces central nervous system hyperexcitability in children. J Am Coll Nutr. 2004;23:545S–8S. [PubMed] [Google Scholar]
24. Nogovitsina OR, Levitina EV. Effect of MAGNE-B6 on the clinical and biochemical manifestations of the syndrome of attention deficit and hyperactivity in children. Eksp Klin Farmakol. 2006;69:74–7. [PubMed] [Google Scholar]
25. Huss M, Völp A, Stauss-Grabo M. Supplementation of polyunsaturated fatty acids, magnesium and zinc in children seeking medical advice for attention-deficit/hyperactivity problems – An observational cohort study. Lipids Health Dis. 2010;9:105. [PMC free article] [PubMed] [Google Scholar]
26. Starobrat-Hermelin B. The effect of deficiency of selected bioelements on hyperactivity in children with certain specified mental disorders. Ann Acad Med Stetin. 1998;44:297–314. [PubMed] [Google Scholar]
27. El Baza F, AlShahawi HA, Zahra S, AbdelHakim RA. Magnesium supplementation in children with attention deficit hyperactivity disorder. Egypt J Med Hum Genet. 2016;17:63–70. [Google Scholar]
El Baza F, AlShahawi HA, Zahra S, AbdelHakim RA. Magnesium supplementation in children with attention deficit hyperactivity disorder. Egypt J Med Hum Genet. 2016;17:63–70. [Google Scholar]
28. Holick MF. Sunlight and Vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr. 2004;80:1678S–88S. [PubMed] [Google Scholar]
29. Mohammadpour N, Jazayeri S, Tehrani-Doost M, Djalali M, Hosseini M, Effatpanah M, et al. Effect of Vitamin D supplementation as adjunctive therapy to methylphenidate on ADHD symptoms: A randomized, double-blind, placebo-controlled trial. Nutr Neurosci. 2018;21:202–9. [PubMed] [Google Scholar]
30. Al-Daghri NM, Alkharfy KM, Khan N, Alfawaz HA, Al-Ajlan AS, Yakout SM, et al. Vitamin D supplementation and serum levels of magnesium and selenium in type 2 diabetes mellitus patients: Gender dimorphic changes. Int J Vitam Nutr Res. 2014;84:27–34. [PubMed] [Google Scholar]
31. Farhanghi MA, Mahboob S, Ostadrahimi A. Obesity-induced magnesium deficiency can be treated by Vitamin D supplementation. J Pak Med Assoc. 2009;59:258–61. [PubMed] [Google Scholar]
Obesity-induced magnesium deficiency can be treated by Vitamin D supplementation. J Pak Med Assoc. 2009;59:258–61. [PubMed] [Google Scholar]
32. Deng X, Song Y, Manson JE, Signorello LB, Zhang SM, Shrubsole MJ, et al. Magnesium, Vitamin D status and mortality: Results from US National Health and Nutrition Examination Survey (NHANES) 2001 to 2006 and NHANES III. BMC Med. 2013;11:187. [PMC free article] [PubMed] [Google Scholar]
33. Risco F, Traba ML. Influence of magnesium on the in vitro synthesis of 24,25-dihydroxyvitamin D3 and 1 alpha, 25-dihydroxyvitamin D3. Magnes Res. 1992;5:5–14. [PubMed] [Google Scholar]
34. Risco F, Traba ML, de la Piedra C. Possible alterations of the in vivo 1,25(OH) 2D3 synthesis and its tissue distribution in magnesium-deficient rats. Magnes Res. 1995;8:27–35. [PubMed] [Google Scholar]
35. Holick MF. Vitamin D and health: evolution, biologic functions, and recommended dietary intakes for Vitamin D. Clin Rev Bone Miner Metab. 2009;7:2–19. [Google Scholar]
2009;7:2–19. [Google Scholar]
36. Drueke TB, Lacour B. Magnesium homeostasis and disorders of magnesium metabolism. In: Feehally J, Floege J, Johnson RJ, editors. Comprehensive Clinical Nephrology. Philadelphia: Mosby; 2007. pp. 136–8. [Google Scholar]
37. Zhang Z, Peluso MJ, Gross CP, Viscoli CM, Kernan WN. Adherence reporting in randomized controlled trials. Clin Trials. 2014;11:195–204. [PubMed] [Google Scholar]
38. Gianarris WJ, Golden CJ, Greene L. The conners’ parent rating scales: A critical review of the literature. Clin Psychol Rev. 2001;21:1061–93. [PubMed] [Google Scholar]
39. Shahaeian A, Shahim S, Bashash L, Yousefi F. Standardisation, factor analysis and reliability of the conners’ parent rating scales for 6- to 11-years-old children in shiraz. Q J Psychol Stud. 2007;3:97–120. [Google Scholar]
40. Heilskov Rytter MJ, Andersen LB, Houmann T, Bilenberg N, Hvolby A, Mølgaard C, et al. Diet in the treatment of ADHD in children – A systematic review of the literature. Nord J Psychiatry. 2015;69:1–8. [PubMed] [Google Scholar]
Nord J Psychiatry. 2015;69:1–8. [PubMed] [Google Scholar]
41. Peacock G, Amendah D, Ouyang L, Grosse SD. Autism spectrum disorders and health care expenditures: The effects of co-occurring conditions. J Dev Behav Pediatr. 2012;33:2–8. [PubMed] [Google Scholar]
42. Doshi JA, Hodgkins P, Kahle J, Sikirica V, Cangelosi MJ, Setyawan J, et al. Economic impact of childhood and adult attention-deficit/hyperactivity disorder in the United States. J Am Acad Child Adolesc Psychiatry. 2012;51:990–100200. [PubMed] [Google Scholar]
43. Annweiler C, Schott AM, Berrut G, Chauviré V, Le Gall D, Inzitari M, et al. Vitamin D and ageing: Neurological issues. Neuropsychobiology. 2010;62:139–50. [PubMed] [Google Scholar]
44. Armstrong DJ, Meenagh GK, Bickle I, Lee AS, Curran ES, Finch MB, et al. Vitamin D deficiency is associated with anxiety and depression in fibromyalgia. Clin Rheumatol. 2007;26:551–4. [PubMed] [Google Scholar]
45. Kelishadi R, Ataei E, Ardalan G, Nazemian M, Tajadini M, Heshmat R, et al. Relationship of serum magnesium and Vitamin D levels in a nationally-representative sample of Iranian adolescents: The CASPIAN-III study. Int J Prev Med. 2014;5:99–103. [PMC free article] [PubMed] [Google Scholar]
Relationship of serum magnesium and Vitamin D levels in a nationally-representative sample of Iranian adolescents: The CASPIAN-III study. Int J Prev Med. 2014;5:99–103. [PMC free article] [PubMed] [Google Scholar]
Attention deficit hyperactivity disorder: diagnosis, pathogenesis, principles of treatment
00:00
Oksana Mikhailovna Drapkina , professor, doctor of medical sciences:
– The next lecture will be devoted to attention deficit hyperactivity disorder. Professor Zavadenko Nikolai Nikolaevich.
Nikolai Nikolaevich Zavadenko , professor, doctor of medical sciences:
– Good afternoon, dear colleagues. nine0003
I will talk about the pathogenesis, diagnosis and treatment of attention deficit hyperactivity disorder.
(Slide show).
Attention Deficit Hyperactivity Disorder (or ADHD for short) is the most common neuropsychiatric disorder in childhood. It occurs in school years in 3-7% of children.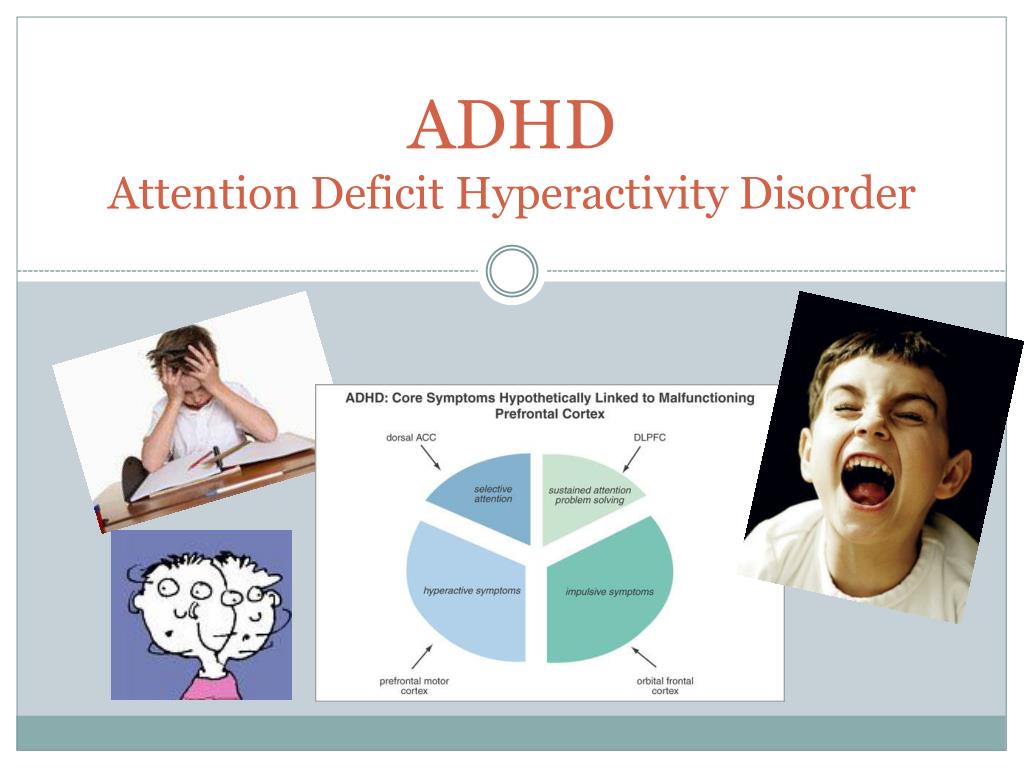 It is known (this is evidenced by the data of longitudinal studies) that the symptoms weaken as they grow older, but continue to manifest themselves in adolescence and even in adulthood in a fairly large number of patients. nine0003
It is known (this is evidenced by the data of longitudinal studies) that the symptoms weaken as they grow older, but continue to manifest themselves in adolescence and even in adulthood in a fairly large number of patients. nine0003
(Slide show).
Traditionally, ADHD is considered in our country within the framework of minimal brain dysfunctions. These include two groups of conditions according to the ICD-10 classification. Attention deficit hyperactivity disorder (or hyperkinetic disorder) is presented in section F9: Behavioral and emotional disorders of childhood and adolescence.
The same group of minimal brain dysfunctions includes psychological developmental disorders (section F8), speech developmental disorders, learning disorders (dysgraphia, dyslexia, dyscalculia) and developmental dyspraxia or static-locomotor insufficiency. nine0003
(Slide show).
This slide presents the results of our surveys of elementary school students in ordinary Moscow general education schools. There were 537 children aged 7 to 11 years old. The aim of the study was to identify those children who have manifestations of school maladaptation (difficulties with learning, behavior, emotional control at school).
There were 537 children aged 7 to 11 years old. The aim of the study was to identify those children who have manifestations of school maladaptation (difficulties with learning, behavior, emotional control at school).
Among the examined children, 31.6% had school maladaptation. A significant part of the cases (about half) was determined by just minimal brain dysfunctions. Including ADHD was diagnosed in 7.6% of children. Other forms of minimal brain dysfunction in about 9%.
02:19
(Slide show).
Pathogenesis of ADHD. To date, there is no doubt about the neurobiological nature of this disorder. The condition is due to the delayed development of interconnected brain structures that provide the processes of behavioral inhibition and self-control. They are defined today as the control functions of the brain.
The key symptoms of ADHD are inattention, hyperactivity and impulsivity. The most characteristic symptoms of the disorder are formulated as its diagnostic criteria. ninesigns of manifestation of hyperactivity and impulsivity, 9 signs of impaired attention.
ninesigns of manifestation of hyperactivity and impulsivity, 9 signs of impaired attention.
Let's start with a list of manifestations of hyperactivity, since they are already pronounced at preschool age.
• The child is constantly spinning and turning.
• Cannot sit still when necessary.
• He is characterized by excessive and aimless motor activity.
• He cannot play quietly and calmly.
• In constant motion. nine0003
• Loquacious.
Hyperactivity is always combined with impulsivity.
• Answers questions without thinking.
• Cannot wait in line.
• Interferes with other people, interrupts them.
I must say that ADHD is characterized by a certain age dynamics. It is the manifestations of hyperactivity that decrease with age, the signs of impulsivity persist.
(Slide show).
As far as attention deficits are concerned, they will become most obvious when the child is being prepared for school or schooling begins. Literally from the first grade of school, the following signs will be very pronounced. nine0003
Literally from the first grade of school, the following signs will be very pronounced. nine0003
• Does not pay attention to details, makes many mistakes.
• Difficulty paying attention to school and other tasks.
• Does not listen to spoken language.
• Unable to follow instructions, follow through.
• Unable to independently plan and organize tasks.
• Avoids activities that require prolonged mental effort.
• Often loses his belongings.
• Easily distracted. nine0003
• Shows forgetfulness.
04:28
(Slide show).
In order for the diagnosis to be substantiated according to ICD-10, which we use in our country, we need to confirm at least 6 symptoms of inattention, 3 signs of hyperactivity and 1 impulsivity.
But there is another internationally recognized DSM-4 classification in the world, the American classification. According to it, the presence of 6 or more symptoms in at least one of two groups will be enough to make a diagnosis: impaired attention or hyperactivity / impulsivity.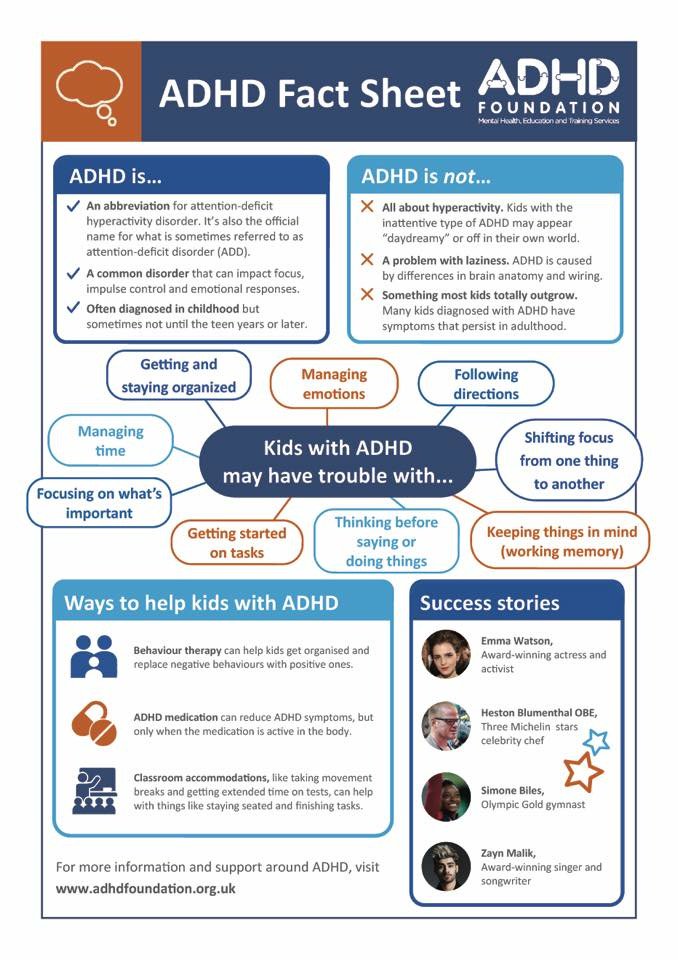 nine0003
nine0003
There are additional criteria for ADHD. In particular, the symptoms must be of sufficient duration to occur continuously for at least 6 months.
Age of onset: they first appear before 7 years of age. Characterized by constancy, distribution to all spheres of life. Accordingly, they lead to significant signs of maladaptation in at least two types of environment: at school, at home. It can be public places, sports, leisure time. The violation is quite pronounced. Another important criterion (this is a matter of differential diagnosis) is that other disorders must be excluded. nine0003
05:44
(Slide show).
According to the DSM-4 classification, depending on the presence and prevalence of symptoms, 3 forms of ADHD are distinguished:
• combined form. Both groups of symptoms are present. It accounts for 50 to 75% of cases.
• ADHD with predominant attention deficits. 20-30%. This group will mainly be represented by teenagers. And it also often happens that in girls the manifestation of hyperactivity is less pronounced.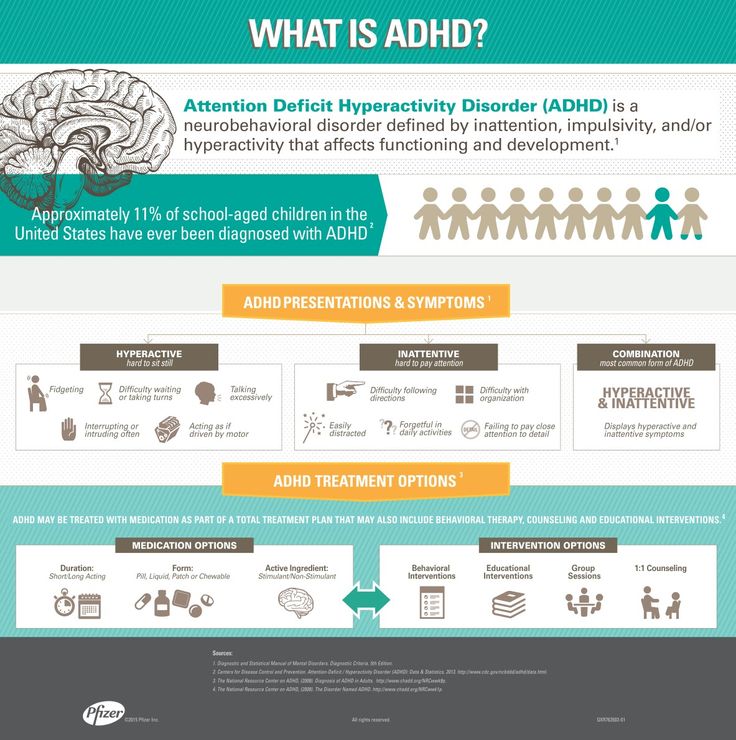
• ADHD with a predominance of hyperactivity and impulsivity. This form (15% of cases), on the contrary, is more common in preschool age. nine0003
According to the ICD classification, we make a diagnosis - we determine the combined form of ADHD. The ICD-10 classification criteria that we use are more stringent.
(Slide show).
Often there are conditions that mimic ADHD. This is 15-20% of school-age children. They may experience similar phenomena, but their cause is not ADHD at all, but some other violations or even a variant of the norm - individual characteristics of temperament. Including:
• impaired attention, periodic hyperactivity may be present in anxiety disorders - what used to be called neuroses, neurotic reactions in children; nine0003
• in case of asthenic syndrome in case of somatic diseases;
• in case of consequences of traumatic brain injury, neuroinfection, intoxication;
• in a number of endocrine diseases, including thyroid pathology;
• for sensorineural hearing loss;
• in a number of forms of epilepsy;
• Tourette's syndrome;
• for a wide range of mental disorders.![]()
All of these conditions require a differential diagnosis. nine0003
(Slide show).
Pathogenesis of ADHD. As I said, this condition is based on neurobiological factors. These are genetic mechanisms and early organic damage to the central nervous system associated with the pathological course of pregnancy and childbirth.
Genetic mechanisms, early organic damage to the CNS, lead to neurotransmitter disorders. First of all, this concerns two neurotransmitter systems: dopaminergic and noradrenergic. But the production, synthesis of neurotransmitters does not decrease directly, the processes of synaptic transmission suffer. nine0003
Social and psychological factors can play an additional negative role. First of all, these are negative intra-family factors. As a result, the child will suffer from the formation of higher mental functions, behavioral deviations and all the clinical symptoms that we have just considered will be noted.
08:29
(Slide show).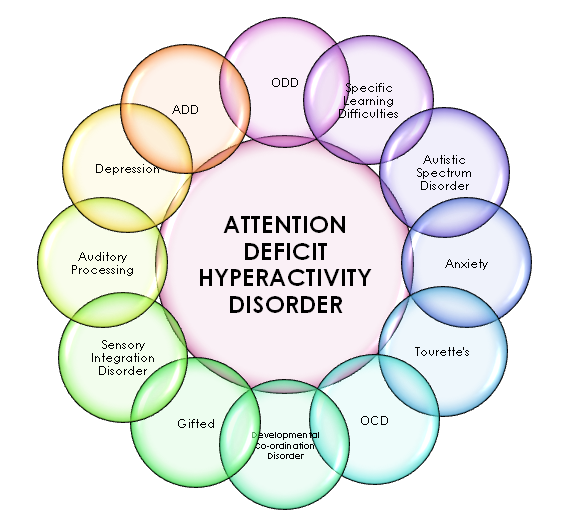
Mechanisms of development of ADHD. If we talk about higher mental functions that suffer in this state and are not sufficiently formed, these are control functions. They are provided by the frontal lobes, primarily their anterior sections, prefrontal structures of the brain. nine0003
Prefrontal structures are responsible for control functions and behavioral inhibition. Accordingly, patients with ADHD exhibit executive dysfunction.
Control functions components. It is these aspects of behavior that are affected by Attention Deficit Hyperactivity Disorder.
• Control of attention.
• Braking, containment, impulse control.
• Planning and organization.
• Inner speech.
• Working or random access memory. nine0003
• Foresight, forecasting, foresight, which, of course, should be based on a look into the past, a retrospective assessment of past events and miscalculations.
• Choice of priorities.
• Time management also suffers in patients with ADHD.
• Change, revision of plans.
• Separation of emotions from real facts.
09:44
(Slide show).
As a result of the influence of these neurobiological factors, the functions of the entire brain system for controlling attention and organizing behavior suffer. This system includes a number of areas of the brain: the associative cortex, basal ganglia, thalamus, cerebellum, prefrontal cortex. nine0003
As I said, failures in the functioning of this system, this complex of brain structures result from certain genetic mechanisms and early organic damage to the central nervous system. An additional negative role is played by socio-psychological factors.
Recently, attention has also been drawn to the influence of adverse environmental factors in terms of the pathogenesis of ADHD. This includes the effect of neurotoxicants on the developing brain. The most common of these is such a heavy metal as lead. nine0003
The role of nutritional factors is being studied, including the role of unbalanced nutrition and nutritional deficiencies of micronutrients: vitamins, macro- and microelements. Including attention is paid to the lack of magnesium in food.
Including attention is paid to the lack of magnesium in food.
What is the physiological role of magnesium in the central nervous system. This is maintaining the balance of the processes of excitation and inhibition. It affects the activity of neurons and the metabolism of neurotransmitters, is a cofactor for a number of enzymes that regulate neurotransmitter metabolism. In addition, magnesium prevents the accumulation of neurotoxic metals in the brain (in particular, lead, aluminum, nickel, and a number of others) and acts as their antagonist. nine0003
(Slide show).
Magnesium deficiency leads to an imbalance in the processes of excitation and inhibition in the brain towards excitation. Accordingly, it can intensify, further exacerbate the manifestation of ADHD symptoms. Magnesium deficiency causes additional disorders of neurotransmitter metabolism that are present in this condition.
Magnesium deficiency in ADHD can be formed due to insufficient intake of this element with food, with an increased need for magnesium during critical periods of growth and development, when exposed to severe physical and neuropsychic stress, and stress. Also, under conditions of environmental stress, lead, nickel and cadmium act as magnesium displacing metals. These mechanisms are currently being actively studied. nine0003
Also, under conditions of environmental stress, lead, nickel and cadmium act as magnesium displacing metals. These mechanisms are currently being actively studied. nine0003
I must say that in addition to a lack of magnesium in the body, the manifestation of ADHD symptoms can also be affected by zinc, iodine and iron deficiencies.
(Slide show).
Manifestations of magnesium deficiency in the body are:
• increased neuro-reflex excitability with corresponding neurological symptoms;
• asthenia, physical and mental fatigue;
• attention deficit;
• cerebral angiodystonia, which manifests itself in the form of headaches, dizziness, fainting; nine0003
• muscle pain and spasms;
• sleep disturbance.
In order to confirm the presence of magnesium deficiency, we must rely on laboratory values. For example, on the content of magnesium in blood serum. Here are indicators that correspond to moderate and severe magnesium deficiency.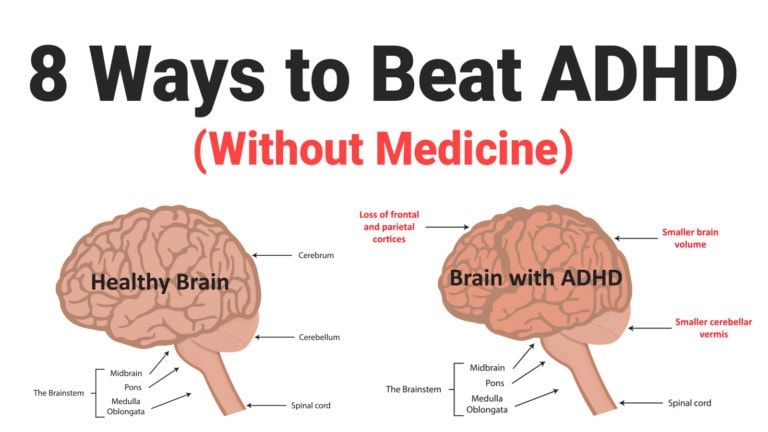
13:16
ADHD therapy must be comprehensive. First of all, it should begin with educational work with parents and teachers. Of great importance, of course, is pharmacotherapy. Specialists work with parents to develop skills for raising children with ADHD, and here we also mean parent education and training programs, specially designed programs. nine0003
(Slide show).
Good internet resources are available. Here are the names of two Internet sites. Parent organization (meaning parents of patients with ADHD, children and adolescents with ADHD). This organization is called Impulse. A lot of useful information can be found on these sites.
Psychotherapeutic methods are aimed at overcoming difficulties and developing communication skills in children and adolescents with ADHD.
(Slide show).
This book was recently released (last year) by Thera-Wind. It describes the methodology of parent training. Undoubtedly, this technique should be widely adopted in our country.
14:29
Complex therapy for ADHD also includes (if possible) control of negative nutritional and environmental factors, limiting the intake of neurotoxic xenobiotics into the child's body. These are lead and other heavy metals, pesticides, food colorings and preservatives. nine0003
Therapy should include micronutrients that help reduce symptoms of ADHD. These are vitamins, macro- and microelements and a whole range of well-known drugs.
(Slide show).
cases where a child's cognitive and behavioral problems cannot be overcome with non-pharmacological methods alone.
Traditionally in our country we use nootropic drugs. There is a wide range of them. In particular, they are very well studied in childhood. nine0003
A fairly new and effective drug that has been specifically developed for the treatment of ADHD is Atomoxetine Hydrochloride or Strattera. The drug was registered in Russia in 2005 and is widely used today.
(Slide show).
Nootropic drugs have a pathogenic effect in ADHD. They have a beneficial effect on the insufficiently formed higher mental functions in these patients. Nootropics have a positive effect on metabolic processes in the brain, contribute to the maturation of inhibitory and regulatory systems. nine0003
They have a beneficial effect on the insufficiently formed higher mental functions in these patients. Nootropics have a positive effect on metabolic processes in the brain, contribute to the maturation of inhibitory and regulatory systems. nine0003
Efficiency in their application we can achieve in 50 - 70% of cases. This efficiency is manifested in the improvement of behavioral characteristics, indicators of motor skills, attention, memory, and other higher mental functions. And also in a certain improvement in the indicators of bioelectrical activity of the brain. For example, according to the EEG.
(Slide show).
Here is a list of nootropics. They are well known/ Include, for example, drugs of the neuropeptide series. Pyrrolidone derivatives, Nootropil (Piracetam). It is considered the ancestor of this group of nootropics. GABA derivatives: domestic drugs Pantogam and Phenibut ) As well as a number of other drugs.
I would like to draw your attention to the last line.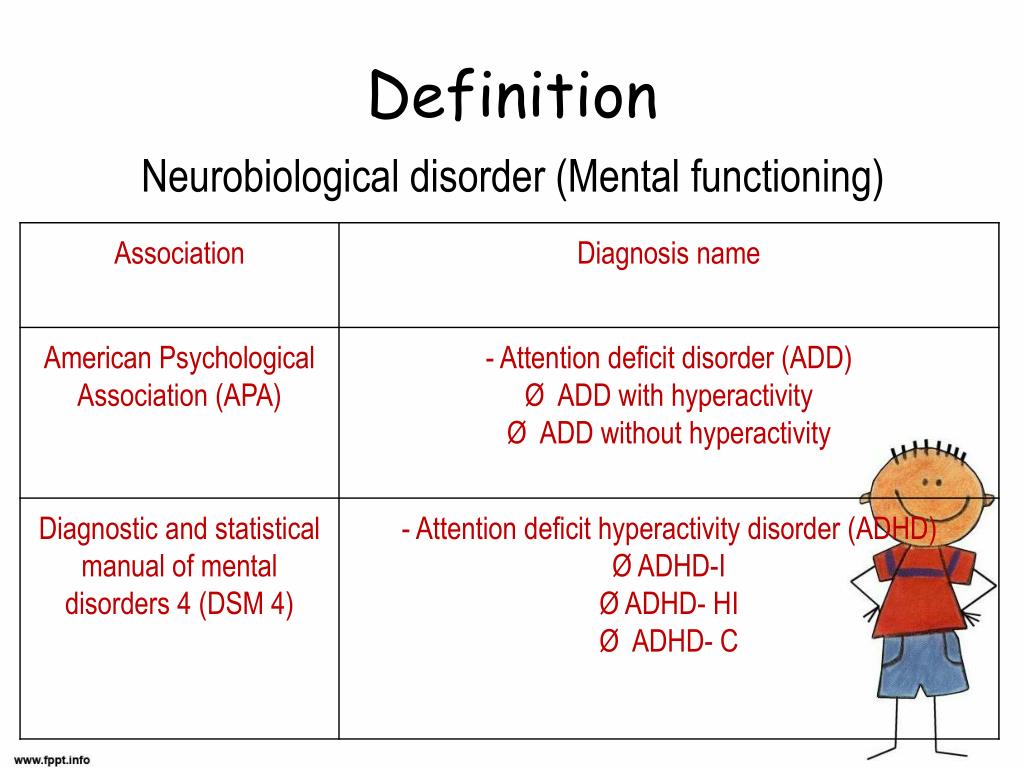 The group of nootropic agents also includes neurometabolic agents with nootropic properties. Among them is such a drug as "Magne B6" ("Magne B6"). I would like to dwell on it in more detail.
The group of nootropic agents also includes neurometabolic agents with nootropic properties. Among them is such a drug as "Magne B6" ("Magne B6"). I would like to dwell on it in more detail.
16:58
It is an optimal combination of magnesium salts and vitamin B6. Magnesium makes up for the lack of a macronutrient in the body, and vitamin B6, pyridoxine, helps the absorption and fixation of magnesium by the cell.
Magnesium is an essential trace element involved in many metabolic processes. On the other hand, pyridoxine is necessary for the normal functioning of the nervous system, is a coenzyme of the most important enzymes that act in the nervous tissue, and is involved in the biosynthesis of neurotransmitters. We talked about the fact that magnesium is the same coenzyme, that is, the action of the two components is synergistic. nine0003
(Slide show).
These are dosage forms of Magne-B6. From the age of 1 year, an oral solution can be used. It comes in ampoules and contains magnesium lactate. The solution contains mainly magnesium pidolate and magnesium lactate.
The solution contains mainly magnesium pidolate and magnesium lactate.
The traditional tablet form contains magnesium lactate. A fairly new form of Forte tablet contains magnesium citrate. Tablet forms can be used from the age of 6 years.
(Slide show). nine0003
The effectiveness of the drug in ADHD is due to the synergism of the action of its components. Pyridoxine increases the concentration of magnesium in plasma and erythrocytes, reduces the amount of magnesium excreted from the body, improves the absorption of magnesium in the gastrointestinal tract, its penetration and fixation in cells.
There has been evidence of a positive clinical effect of Magne-B6 in the treatment of those children with ADHD who have been confirmed to have a laboratory magnesium deficiency. These works were published abroad in 1998th year and 2004th.
These investigators administered a combination of magnesium and pyridoxine for several months to patients with ADHD. As a result, regression of symptoms was achieved.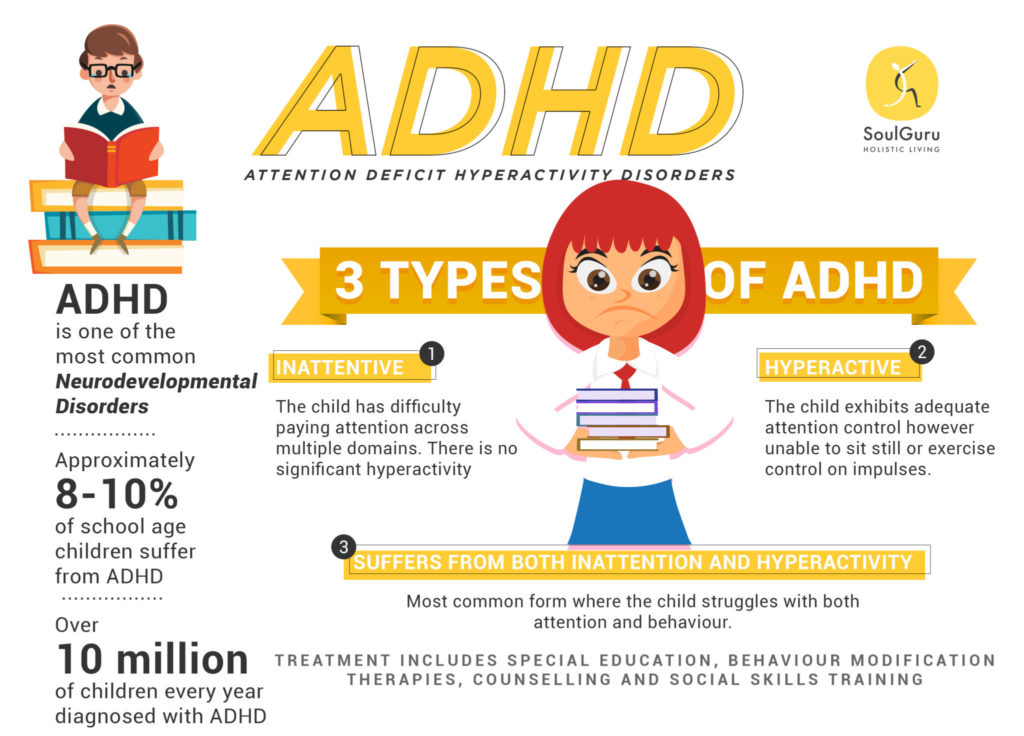 Magnesium levels in erythrocytes were monitored and restored to normal values.
Magnesium levels in erythrocytes were monitored and restored to normal values.
19:22
(Slide show).
Russian researchers (in particular, the data of the works of Olga Alekseevna Gromova are presented here) studied the imbalance of macro- and microelements in children with ADHD. Here in the diagram, the red columns show us the percentage of patients with concentrations of certain macro- and microelements above the upper limit of normal. And the blue columns, on the contrary, are the content below the lower limit of the norm. nine0003
(Slide show).
The main part of the deviations was accounted for by deficits - this is 70% of cases. Excessive accumulation of elements was determined only in 11% of cases. The core of the deficits were 6 metals: magnesium, zinc, copper, calcium, manganese and cobalt.
I must say that an excess of lead has always correlated with a low level of magnesium. It is very important.
Magnesium deficiency occupied the leading position in the structure of elemental status deviations in patients with ADHD. Its level was below normal in 72% of patients. The level of magnesium in the hair was determined - this approach is also possible. More than 65% of patients had magnesium levels 2 or more times lower than normal. nine0003
Its level was below normal in 72% of patients. The level of magnesium in the hair was determined - this approach is also possible. More than 65% of patients had magnesium levels 2 or more times lower than normal. nine0003
(Slide show).
The results of therapy with Magne-B6 in patients with ADHD were also published by Russian researchers Nogovitsina and Levitina. Therapy was carried out in 31 patients with ADHD (age from 6 to 12 years) and 20 children of the control group were examined at the same time.
Questioning of parents showed a significant decrease in scores on the scales "anxiety", "impaired attention" and "hyperactivity". Improvement in concentration, accuracy and speed of tasks, a decrease in the number of errors were confirmed during psychological testing. nine0003
Positive dynamics on the encephalogram was registered. It was found that the concentration of magnesium in erythrocytes and blood plasma returned to normal after this therapy.
(Slide show).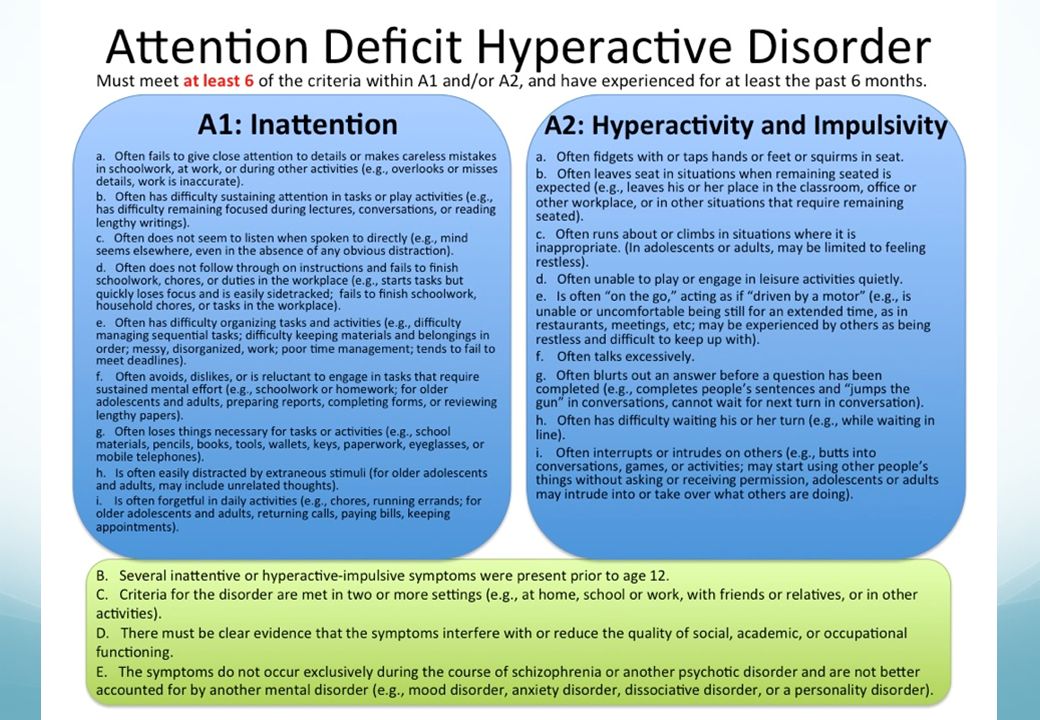
But in general, replenishment of magnesium deficiency, if the child already has it, should last at least two months. Considering that alimentary deficiency of magnesium occurs most often, when drawing up nutritional recommendations, one should take into account not only the quantitative content of magnesium in foods, but also its bioavailability. nine0003
Fresh vegetables, fruits, herbs and nuts are known to be richest in magnesium. When harvesting products for storage, the concentration of magnesium does not decrease so significantly, but its bioavailability drops sharply. This also needs to be taken into account.
It must be taken into account that the deepening of magnesium deficiency in children with ADHD coincides with the period of schooling, that is, from September to May. This refers to the magnesium content in foods. The use of "Magne-B6" is advisable just during the school year. nine0003
Thus, the efforts of specialists should be aimed at early detection of ADHD in children.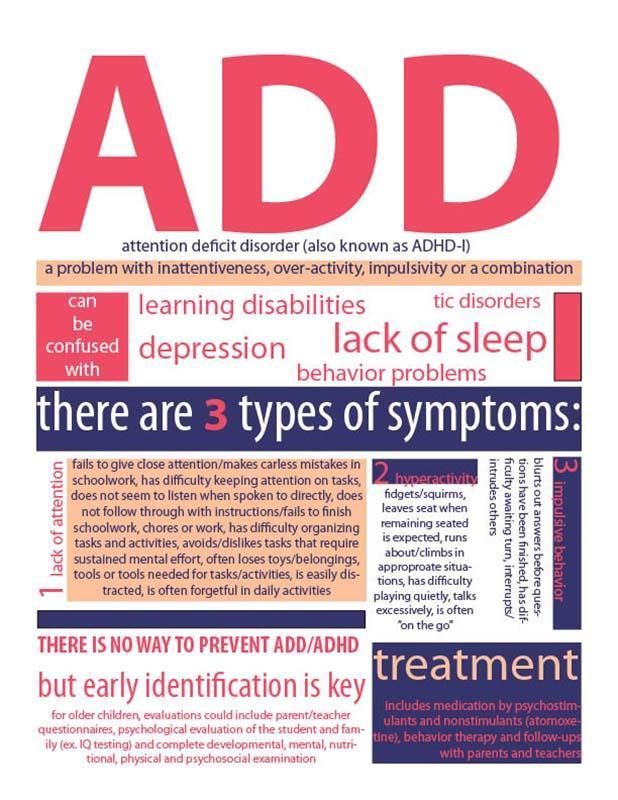 The development and application of complex correction should be carried out in a timely manner, be of an individual nature. Correction, including drug therapy, should have sufficient duration.
The development and application of complex correction should be carried out in a timely manner, be of an individual nature. Correction, including drug therapy, should have sufficient duration.
Thank you for your attention.
Attention Deficit Disorder and Magnesium B6 in the treatment of ADHD
The combination of Magnesium B 6 and Ginkgo Biloba in the treatment of children with ADHD, in our opinion, is a major discovery of Israeli medicine in 2010. nine0006
Clinical value of magnesium:
Magnesium (Mg) is an extremely important universal element for the regulation of human health. Magnesium is the second most abundant intracellular cation and has been identified as a metabolic cofactor in more than 300 important enzymatic reactions in energy metabolism, protein metabolism, and nucleic acid synthesis. In addition, magnesium has its own channel for the passage of calcium through cell membranes, and this is a necessary component for maintaining the integrity of the cell membrane of the heart, lungs, brain and other important organs and systems. nine0003
nine0003
Approximately half of the total body magnesium has been shown to be found in soft tissues and the other half in bone. Less than 1% of the total magnesium level is present in the blood, and only about 0.3% in the serum. Therefore, the assessment of the level of magnesium in the fluid through a blood test is inaccurate and approximate.
Nutritional malnutrition
It is estimated that 90% of the population of the Western world use diets in which magnesium intake is below the daily requirement . Magnesium deficiency is more common than commonly thought and can lead to cardiovascular disease leading to disease at all stages of life.
"Magnesium B 6 " - the patient receives magnesium in the form of magnesium lactate dihydrate - the most easily digestible and close to exchange formula.
"Magnesium B 6 " contains magnesium in the most concentrated form, this leads to a significantly better result.
Designed for optimal suction
"Magnesium B 6 " dissolves in gastric juice, where it forms magnesium chloride (MgCl 2 ), which is especially well absorbed and brings such an unusual result.
Best results are 1 capsule before bed.
Thus, "Magnesium B 6 " easily provides the daily intake of the daily requirement of magnesium in 1 capsule. This may be helpful for those on a diet.
Research shows that magnesium is a fundamental element of good health. nine0003
"Magnesium B 6 " has been shown to play a beneficial role in the following diseases:
- Quite quickly normalizes high blood pressure (especially high "lower" pressure). Against the background of general treatment improves the condition after a stroke. Approximately on the 3-6th day of admission, patients feel lightness in the whole body and higher endurance during physical exertion.
 nine0387
nine0387 - Endocrine system
Confidently reduces high levels of lipids in blood serum, balances sugar levels in diabetes.- Women's health
Indicated even for pregnant women in case of nocturnal calf cramps. Provides the daily requirement of magnesium for a pregnant woman and her fetus. Prevention of preeclampsia, prevention of preterm birth.
ATTENTION: "MAGNE B 6 " is also the prevention of osteoporosis in pregnant women (tooth decay, increased bone fragility, malnutrition of hair and nails). nine0387- Children with Attention Disorders and Hyperactivity ADD/ADHD
In combination with Ginkgo Biloba, which improves cerebral circulation, magnesium balances nerve processes, normalizes the permeability of brain cell membranes, and from about the 3rd month of intake contributes to noticeable for teachers and educators to stabilize the attention and social behavior of the child.- Pain.
- Endocrine system