Interpersonal psychotherapists believe that therapy must address
Interpersonal Psychotherapy | Psychology Today
Reviewed by Psychology Today Staff
Interpersonal psychotherapy (IPT) is a time-limited, focused, evidence-based approach to treat mood disorders. The main goal of IPT is to improve the quality of a client’s interpersonal relationships and social functioning to help reduce their distress. IPT provides strategies to resolve problems within four key areas.
First, it addresses interpersonal deficits, including social isolation or involvement in unfulfilling relationships. Second, it can help patients manage unresolved grief—if the onset of distress is linked to the death of a loved one, either recent or past. Third, IPT can help with difficult life transitions like retirement, divorce, or moving to another city. Fourth, IPT is recommended for dealing with interpersonal disputes that emerge from conflicting expectations between partners, family members, close friends, or coworkers.
When It's Used
IPT was originally developed to treat major depressive disorder. It’s also used effectively to treat eating disorders, perinatal depression, drug and alcohol addiction, dysthymia, and other mood disorders—including bipolar disorder. IPT differs from other traditional psychodynamic approaches in that it examines current rather than past relationships, and recognizes—but does not focus on—internal conflicts.
The practice differs from cognitive and behavioral therapy approaches because it addresses maladaptive thoughts and behaviors only as they apply to interpersonal relationships. IPT aims to change relationship patterns rather than the associated depressive symptoms, as well as target relationship difficulties that exacerbate these symptoms. IPT is less directive than cognitive-behavioral approaches—focusing on the patient’s specified target areas without dwelling on his or her personality traits.
Read More
Treat Depressed Mothers, and Their Children Recover
Social Intelligence, Authentic Relationship and Conscious Communication
What to Expect
IPT treatment typically consists of individual therapy sessions or group work completed within 12 to 16 weeks. Treatment is structured—including homework, continuous assessment, and interviews by the therapist. The first phase of IPT often involves one to three sessions during which the therapist will assess depressive symptoms and examine social history and close relationships, including any changes in relationship patterns and expectations. Then, the therapist works with the patient to implement treatment strategies specific to any identified problem areas. As treatment progresses, a targeted problem area might change.
Treatment is structured—including homework, continuous assessment, and interviews by the therapist. The first phase of IPT often involves one to three sessions during which the therapist will assess depressive symptoms and examine social history and close relationships, including any changes in relationship patterns and expectations. Then, the therapist works with the patient to implement treatment strategies specific to any identified problem areas. As treatment progresses, a targeted problem area might change.
Correspondingly, so might the therapist’s recommended strategies. Group sessions—like individual ones—are time-limited, semi-structured, and focused on interpersonal dynamics. Groups provide more opportunities for patients to practice interpersonal skills in a safe, supportive environment. Group therapy, also often includes pre-treatment, mid-treatment, and post-treatment individual meetings to review goals, strategies, and progress.
How It Works
IPT developed more than 20 years ago as a time-structured treatment for major depression, and it has gained popularity in recent years. Practitioners believe that change in social environment is a key factor in the onset of depression as well as continued depression. Originally developed for adults, IPT has been modified for practice with adolescents and elderly patients. IPT first appeared as part of a study investigating the efficacy of antidepressants, and was found comparable in efficacy to medication.
Practitioners believe that change in social environment is a key factor in the onset of depression as well as continued depression. Originally developed for adults, IPT has been modified for practice with adolescents and elderly patients. IPT first appeared as part of a study investigating the efficacy of antidepressants, and was found comparable in efficacy to medication.
What to Look for in an IPT Therapist
IPT is a relatively young psychotherapy that was developed as a research intervention, and until recently, most practitioners of IPT were researchers. Its research success has led to IPT’s inclusion in clinical treatment guidelines and growing interest among clinicians, but the standards for clinical training for non-researchers are still being defined. The International Society for Interpersonal Psychotherapy (ISIPT), an international umbrella organization, deliberates training issues and allows countries to develop their own credentialing processes for IPT.
A therapist should help the patient identify any interpersonal issues he or she wants to address, and rank them in order of importance. The therapist should also offer support regarding clarification of issues, communication analysis, and supportive listening.
References
Klerman, G. L., & Weissman, M. M. (1994). Interpersonal psychotherapy of depression: A brief, focused, specific strategy. Jason Aronson, Incorporated.
Wilfley, Denise E., & Shore, Allison L. (2015). Interpersonal Psychotherapy. In International Encyclopedia of the Social & Behavioral Sciences (pp. 631-636).
Wurm, C, Robertson, M, & Rushton, P. (2008). Interpersonal psychotherapy: An overview. Psychotherapy in Australia, 14(3), 46-54.
National Institutes of Health
What is interpersonal therapy?
Interpersonal therapy (IPT) is a type of psychotherapy that aims to cultivate strong attachments. Research suggests that it can help improve the symptoms of several mental health conditions.
IPT is a form of psychotherapy that can treat depression and some other mental health issues.
Two psychotherapists developed it in the 1970s to help with depression, and clinicians have since used it to treat a variety of mental health issues. Learn more in this article.
IPT is a short-term form of therapy that usually lasts for fewer than 12–16 weeks. It focuses on cultivating communication and interpersonal effectiveness skills; practitioners believe that many mental health issues stem from relational deficits or role conflicts.
IPT practitioners endorse the notion of depression and other mental health conditions as real illnesses requiring treatment. They focus on this in therapy to prevent clients from blaming themselves for their challenges.
Proponents of IPT also argue that mood and life situations, especially relationships, are closely related. Improving relationships can improve a person’s mental health.
In IPT sessions, a person learns and practices skills that may help heal relationships and prevent the development of additional relationship issues.
IPT is a structured type of therapy, which means that treatment progresses in three distinct phases.
During the first one to three sessions, a therapist will diagnose the issue and help the client identify the interpersonal issues that preceded or maintained the psychological distress.
For example, a person going through a breakup might notice that their depression developed after the breakup. The therapist will also develop an “interpersonal inventory” that reviews the client’s pattern of behavior in relationships and evaluation of current relationships.
IPT therapists believe that four areas of conflict typically trigger relationship and mental health issues. These are:
- relationship conflicts that cause stress
- life changes that alter a person’s role or relationships
- difficulty beginning or maintaining relationships
- grief or loss
Once the therapist and their client identify the area of conflict that causes the latter’s distress, therapy will focus on managing this conflict.
During the middle portion of treatment, the therapist will develop targeted relationship strategies to bolster interpersonal functioning. For example, they might help a client who is going through a breakup mourn the relationship and the role it represents, then help them cultivate new skills and ways of relating to others.
In the final weeks of treatment, the therapist will remind the client that treatment will be ending soon, and they will help them practice their new skills.
Some therapists use a combination of IPT and other therapies. When this is the case, IPT may last longer or be less formulaic.
As with all forms of therapy, the therapist will encourage the client to discuss their emotions, identify patterns in their behavior, and be open about their goals for treatment. The therapist must also keep the client’s information private.
Research consistently suggests that IPT works well for depression — especially depression related to relationship issues.
More recent research has started to test IPT for other psychological issues. For example, a 2020 study of family caregivers of people with schizophrenia found that IPT coupled with psychoeducation could help improve self-efficacy and reduce the family’s care burden.
In the 1970s, psychotherapists Myrna Weissman and Gerald Klerman developed IPT to treat mood disorders such as depression. They drew upon the research of John Bowlby and Mary Ainsworth, who studied the role that attachments, especially in early life, play in relationships.
IPT practitioners highlight research showing that social factors, such as the loss of a relationship, are often major factors in the onset and maintenance of depression.
Drawing on these data, Weissman and Klerman used IPT to treat depression and other mood issues. Since then, researchers have shown that IPT can also treat social phobia, anxiety disorders, post-traumatic stress disorder, and eating disorders.
Most research shows that IPT works about as well as other types of therapy. In some cases, it even seems to provide better results.
In some cases, it even seems to provide better results.
A 2005 meta-analysis of IPT for the treatment of depression looked at studies that compared IPT with a placebo and with cognitive behavioral therapy (CBT). IPT was more effective than CBT and placebo, and it offered similar results to medication.
A much larger 2016 meta-analysis assessed the effectiveness of IPT for various mental health issues. Drawing on data from 90 studies, the researchers found no significant difference between IPT and other clinically evaluated studies.
IPT was effective in treating depression, eating disorders, and similar issues, though the study suggests that CBT is likely more effective in the early stages of eating disorder treatment.
IPT builds upon many theories, including attachment theory. Therefore, its methods are similar to those of some other approaches. For example, emotionally focused therapy also prioritizes attachments and human relationships.
Learn more about different types of therapy here.
Some strengths of IPT include:
- a focus on relationships, communication skills, and life situations rather than viewing mental health issues as things that occur in a vacuum
- a structured, formulaic approach that makes it easier to track progress
- an ability to build a strong relationship with the therapist, which may enable the client to test new skills
Research has consistently shown that IPT works well for depression and relationship transitions and conflict. Although many studies have shown that IPT works well for some other issues, the evidence there is less consistent, and some other therapies may work better.
One potential weakness of IPT is its shorter timeline, which may not offer enough support for people with chronic or relapsing mental health issues. That said, IPT practitioners recognize that maintenance sessions may be necessary for recurring symptoms.
Also, its formulaic approach may mean that therapy does not offer relief if a person drops out early or cannot pay for continued treatment.
Like all forms of psychotherapy, IPT can empower a person to change the way they think about and interact with others.
The focus on relationships may be especially helpful for those grieving lost relationships or struggling to make their relationships work.
For people with depression, IPT is a highly effective treatment option that may be an alternative to medication.
No matter which treatment a person chooses, it is important to work with a licensed mental health counselor with experience in treating the specific issue for which the person seeks care.
what you need to know and who it helps
Interpersonal psychotherapy (IPT - interpersonal psychotherapy) is a type of therapy aimed at cultivating strong attachments. Studies show that it can improve the symptoms of several mental illnesses.
What is interpersonal psychotherapy?
Interpersonal psychotherapy (IPT) is a short-term form of psychotherapy that typically lasts 12-16 weeks. Treatment focuses on developing communication skills and interpersonal effectiveness; practitioners believe that many mental health problems stem from relationship deficits or role conflicts.
Treatment focuses on developing communication skills and interpersonal effectiveness; practitioners believe that many mental health problems stem from relationship deficits or role conflicts.
Practitioners support the notion of depression and other mental health conditions as real illnesses that require treatment. Psychiatrists focus on this in therapy so that patients do not blame themselves for their problems. MLP advocates also argue that mood and life situations, especially relationships, are closely related. Improving relationships can improve a person's mental health.
In MLP sessions, the patient learns and practices skills that can improve relationships and prevent further relationship problems from developing.
Origins
In the 1970s, psychotherapists Myrna Weissman and Gerald Klerman developed the MLP to treat mood disorders such as depression. They drew on the research of John Bowlby and Mary Ainsworth on the role of attachment, especially at an early age, in human relationships. Research shows that social factors, such as the loss of a relationship, are often major contributors to depression.
Research shows that social factors, such as the loss of a relationship, are often major contributors to depression.
Based on these findings, Weissman and Clerman used MLP to treat depression and other mood problems. Since then, MLP has been used to treat social phobias, anxiety disorders, post-traumatic stress disorder, and eating disorders.
How does MLP work?
MLP is a structured type of psychotherapy. Within one to three sessions, the therapist diagnoses the problem and helps the patient overcome the interpersonal problems that preceded the psychological distress. For example, a person going through a breakup may notice that their depression develops after the breakup. The therapist will also develop an "interpersonal inventory" that will analyze the person's behavior pattern in the relationship and evaluate the current relationship.
Psychotherapists believe that four areas of conflict commonly cause relationship and mental health problems. These are:
These are:
- relationship conflicts that cause stress
- life changes that change the person's role or relationship
- difficulty starting or maintaining relationships
- grief or loss
of the latter disorder, therapy will focus on managing this conflict.
Midway through treatment, the therapist will develop purposeful relationship strategies to strengthen interpersonal functioning. For example, help a person going through a breakup to speak up and then help them develop new skills and ways to communicate with others.
During the final weeks of treatment, the therapist will remind you that the treatment will end soon and that new skills should be practiced.
Some psychotherapists use a combination of MLP and other treatments. In this case, the MLP may last longer.
As in all forms of psychotherapy, the therapist encourages the patient to discuss their emotions, identify patterns in their behavior, and be open about their treatment goals. The doctor must also keep the patient's information confidential.
The doctor must also keep the patient's information confidential.
Research shows that MLP works well for depression - especially depression associated with relationship problems.
More recently, studies have begun testing MLT for other psychological problems. For example, a 2020 study of caregivers of people with schizophrenia found that MLP, when combined with psychoeducation, can increase self-efficacy and reduce the burden of caregiving.
MLP versus other types of psychotherapy
Most research shows that MLP works in much the same way as other types of therapy. In some cases, it even gives better results.
In a 2005 meta-analysis, researchers compared MLP with placebo and with cognitive behavioral therapy (CBT). MLP was more effective than CBT and placebo and produced the same results as drug treatment.
A much larger 2016 meta-analysis assessed the effectiveness of MLP for a variety of mental health problems. Based on data 90 studies found no significant difference between MLP and other treatments. MLP was more effective in treating depression, eating disorders, and similar problems, although the authors of this study believe that CBT is more effective in the early stages of treating eating disorders.
MLP was more effective in treating depression, eating disorders, and similar problems, although the authors of this study believe that CBT is more effective in the early stages of treating eating disorders.
MLP is based on many theories, including attachment theory. Therefore, its methods are similar to those of some other approaches. For example, Emotionally Focused Therapy also focuses on attachment and human relationships.
Strengths and weaknesses of MLP
Some of the strengths of MLP include:
- emphasis on relationships, communication skills and life situations instead of viewing mental health problems as things that happen in a vacuum
- structured, formulaic approach that facilitates tracking progress
- the ability to build a strong relationship with the therapist, which may allow the patient to test new skills
Research shows that MLP works well for depression, relationship transitions, and conflict.
One of the potential disadvantages of MLP is its short duration, which may not provide sufficient support for people with chronic or recurrent mental health problems. However, doctors recognize that support sessions are necessary for recurring symptoms.
In addition, his formulaic approach may mean that therapy does not bring relief if the person quits early or cannot pay to continue treatment.
Conclusion
Like all forms of psychotherapy, MLP can enable a person to change the way they think about and interact with other people. Focusing on relationships can be especially helpful for those who are grieving a lost relationship. For people with depression, MLP is a highly effective treatment that can be an alternative to medication. Regardless of which treatment a person chooses, it is important to work with a licensed mental health consultant who is experienced in treating a particular problem.
Research paper on topic: Psychotherapy should be the first line of treatment for depression in young people.
Trusova Valentina Ivanovna
Neurologist JSC "SZTsDM", St. Petersburg
Editor and author of articles.
Contact email - [email protected]
Before using the advice and recommendations set out on the website "Medical Insider" , , be sure to consult your doctor!
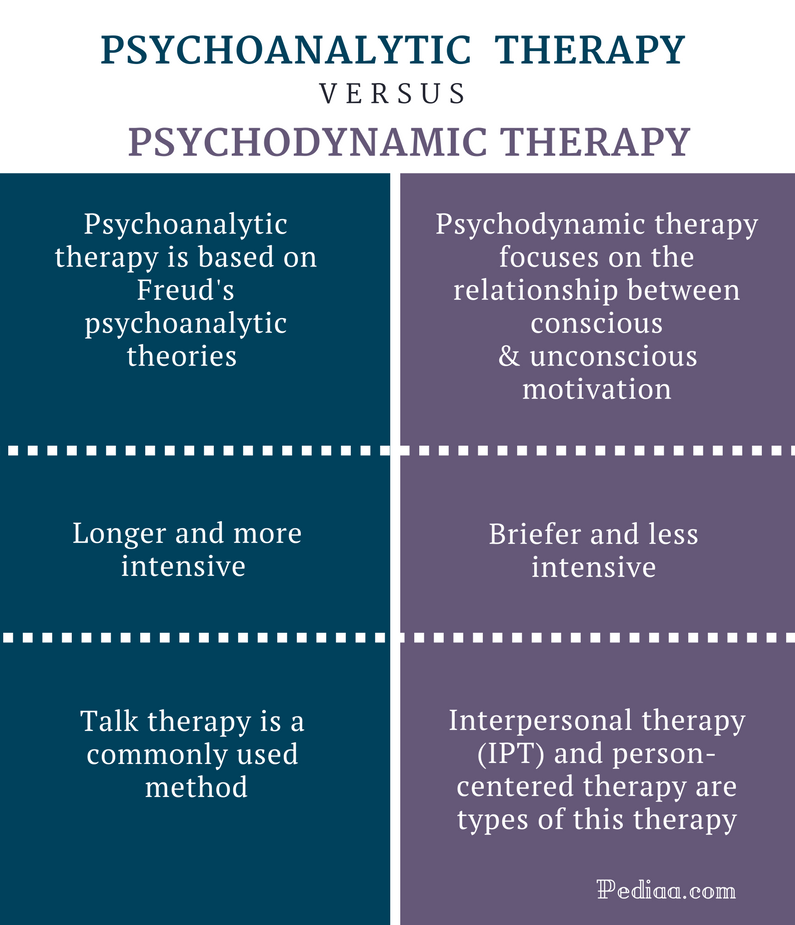
Dynamic psychotherapy
What are the features of dynamic psychotherapy, what are its main directions, how did it originate and develop, what are its main provisions, theoretical justifications and practical goals, we decided to ask the Chief Physician of the Health Harmony Medical Center, a practitioner psychiatrist, psychiatrist-narcologist and psychotherapist Vladislav Sipovich. The topic for discussion is rather complicated, so we asked to cover it in a form that is accessible to readers.
What are the basic principles of dynamic psychotherapy?
Dynamic Psychotherapy (DPT), known as psychodynamic or psychoanalytic psychotherapy, combines several types of psychotherapy based on psychoanalysis and existential psychology. At the head of understanding the mental processes and behavior of the individual, dynamic psychotherapy puts the sphere of the unconscious and the experience of a past life deeply hidden in it, starting from childhood, sometimes even infancy. The main elements of such an impact are the features of thinking (cognitive protection (more about cognitive-behavioral therapy)), interpersonal relationships and the perception of other people through the transfer of experience hidden in the subconscious to the surrounding reality.
Why dynamic? Perhaps many will think that this definition refers to the speed and intensity of this direction of psychotherapy. But no, indeed, from a technical point of view, dynamics means strength, energy and movement, but when applied to mental activity, the term dynamic indicates the development of the mental sphere of the personality, as a struggle between the internal processes of the psyche and a conflict laid down by certain circumstances between instincts and the Ego of a person resisting them. According to Freud, it is this conflict that underlies the development of neuroses. He believed that their cause is of a sexual nature, and the development of neurotic states is subject to such basic principles as dynamism, structure, development and adaptation.
According to Freud, it is this conflict that underlies the development of neuroses. He believed that their cause is of a sexual nature, and the development of neurotic states is subject to such basic principles as dynamism, structure, development and adaptation.
The entire psychoanalytic model is based on the following basic principles:
• The main role in mental processes belongs to the instincts and their transformation as a result of suppression and resistance to their painful manifestations for the psyche.
• Between the physiological instincts and the protective mechanism of the Ego ("I", which mediates the connection with the outside world) there is a constant struggle - the instincts are suppressed by the moral standards and norms of behavior existing in society.
• The suppression of instincts itself has a sexual character, therefore the main etiological factor of neuroses is considered to be an incorrect psychosexual education and a correspondingly distorted libidinal attraction.
• The sources of such pathological development are in the rather distant past, in the psychological traumas received in childhood, associated, for example, with the oedipal complex (unconscious erotic attraction) to the parent of the opposite sex.
• The presence of internal resistance to the identification of this complex.
• Mental determinism, i.e. conditionality of behavioral and mental phenomena by previous events, consciously or unconsciously affecting the characteristics of the psyche and behavior of the individual.
In general, the chain of cause-and-effect relationships in the development of neuroses according to Freud can be represented as follows:
Attraction → Anxiety → Defense mechanism.
Freud's dynamic model expanded the understanding of the human psyche, explaining its individual characteristics by the presence of conflicting thoughts, emotions, behavioral reactions, which can be both adaptive in nature and be the basis for psychopathological disorders. By the way, the conflict of forces can be laid at different levels, both deep in the unconscious and in consciousness.
By the way, the conflict of forces can be laid at different levels, both deep in the unconscious and in consciousness.
How did the history of dynamic psychotherapy develop?
Dynamic psychotherapy is a logical continuation of the classical psychoanalysis of Sigmund Freud. Its most common variants were Jung's analytical psychology, Rank's volitional therapy, Sullivan's interpersonal psychotherapy, Adler's individual psychology, Wahlberg's hypnoanalysis (more about hypnosis), Myasishchev's personality-oriented, otherwise reconstructive psychotherapy, widespread in Russia, and many others. By the way, reconstructive psychotherapy is a purely domestic scientific product and is based on the teachings of V.N. Myasishchev about neuroses and the principles of their psychotherapy as borderline states.
It should be noted that the development of the dynamic approach in psychotherapy proceeded along three fundamentally different directions:
1. Freudian, based on the conflict of innate instincts, which gradually intensifies in the course of psychosexual development. The conflict arises between opposing instincts, between instincts and the environment, as well as between the immediate satisfaction of the child's needs and the world that opposes and delays this process.
The conflict arises between opposing instincts, between instincts and the environment, as well as between the immediate satisfaction of the child's needs and the world that opposes and delays this process.
2. Neo-Freudian presented by G.S. Sullivan, K. Horney and E. Fromm and considering the internal conflict not as programmed by innate instincts, but as formed by interpersonal and social relations. They consider the child's need for security, acceptance and approval of his actions by significant adults to be basic. Children's innate curiosity, energy, innocence of bodily desires, potential for growth and development, as well as unlimited desire for complete possession of a loved adult, do not always meet the requirements of adults nearby. This is the main conflict of children. If parents, for various reasons, are not able to ensure the safety of the child and create conditions for realizing the potential of his growth, then he has a real danger of developing a severe mental conflict, including delayed in time.
3. Existential, in which the conflict arises due to the confrontation of the individual with the givens of his being, the so-called inevitable final factors of the existence of the individual. There are only 4 of them:
• Death is a terrifying and quite conscious ultimate given. Its inevitability is opposed by the strongest desire of man to continue to exist. Even on his deathbed, man strives to live. Confirmation of this is a classic case when an incurable severely suffering patient asked the doctor for euthanasia. He left pills near his bed, explaining what dose could be fatal. In the morning he found the patient in the same condition, but not a single pill had been taken from the package.
• Freedom is a less obvious, but no less significant given. The attitude towards freedom is ambiguous. In general, it is regarded positively if a person tries it on himself, but since we all live in society, the freedoms of different individuals may come into confrontation with each other. Therefore, a structured community, in which rules and standards of behavior operate, opposes the so-called absolute freedom, creating for a person a support and ground for security. The loss of such a support and the realization that instead of it is emptiness, inevitably gives rise to an internal existential conflict.
Therefore, a structured community, in which rules and standards of behavior operate, opposes the so-called absolute freedom, creating for a person a support and ground for security. The loss of such a support and the realization that instead of it is emptiness, inevitably gives rise to an internal existential conflict.
• Isolation is seen not as a feeling of loneliness and isolation from other people, but as a more fundamental given. We come into this world alone and leave it alone. No human intimacy can overcome this barrier. Therefore, a conflict arises between absolute isolation and the need for protection, contacts and a person's feeling of himself as part of a large human world.
• Nonsense that is generated by the first three data. If we all die, we ourselves are responsible for our universe and are alone in this indifferent world, then what is the meaning of our existence, why do we live and how can we live on? This dynamic conflict is due to the search for the meaning of life by a person who finds himself in a world that is meaningless according to his ideas.
The task of an existential psychotherapist is to clarify the nature and causes of deep personality conflicts. It is quite difficult to do this, since most often the symptoms presented by the patient look like a motley mosaic, and the root cause of mental problems is deeply hidden under many layers of repression, replacement, denial and symbolization of painful memories for the psyche. The previous scheme of the dynamic approach proposed by Freud in existential psychodynamics radically changes the content and can be represented as follows:
Awareness of the ultimate reality → Anxiety → Defense mechanism
In both formulas, anxiety plays a key role in the emergence and development of mental disorders, triggering conscious and unconscious processes of mental activity as a defense mechanism. This mental activity is the basis of various psychopathologies.
According to the characteristics of each direction, the methods of dynamic psychotherapy used in psychotherapeutic practice also differ.
How does a dynamic psychotherapist work?
Therapeutic action in dynamic psychotherapy is achieved through awareness of the unconscious, i.e. understanding by the patient that the roots of his problems lie deep in the subconscious. To reveal the causal relationship hidden in it between a neurotic disorder and past psychic trauma, and to interpret it, is the main task of a dynamic psychotherapist.
Of course, to reveal and unravel this connection, and even more so to eliminate the conflict of instincts and the Ego, is a slow and scrupulous process, therefore the result of therapy is quite distant in time, sometimes stretching for months and even years. But it's worth it, because. in the process of dynamic treatment, it is supposed to achieve a complete reorganization of the personality, the dominance of the power of the ego over sexual instincts and the elimination of neurotic disorder.
In dynamic psychotherapy, the most important aspect is the interaction between the therapist and the patient.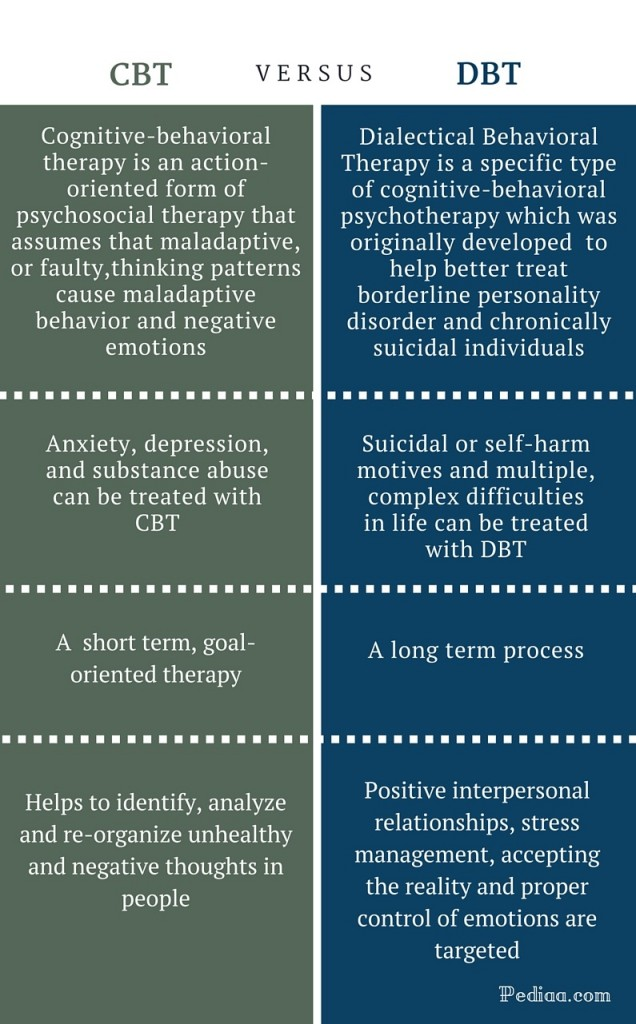 It involves the following two stages in its development:
It involves the following two stages in its development:
• Primary with phenomena of unconscious transfer (transfer) of previously experienced feelings to one person to another, in this case, to a psychotherapist. In this role, it is important for the analyst to reflect only what comes from the patient and not to introduce his own values, feelings, and even more so elements of his personal life into the interaction process. The position of the psychotherapist should be reduced to the role of an abstaining and neutral observer, and the attitudes must necessarily be based on ethical principles and norms.
• Secondary - the formation of a really working healing union on the basis of a rational and practical relationship between the psychotherapist and the patient to identify the causes of his problems.
The dynamic approach in psychotherapy is carried out mainly by verbal (verbal) communication and analysis of the patient's free (uncensored) associations, the study of transference and resistance reactions.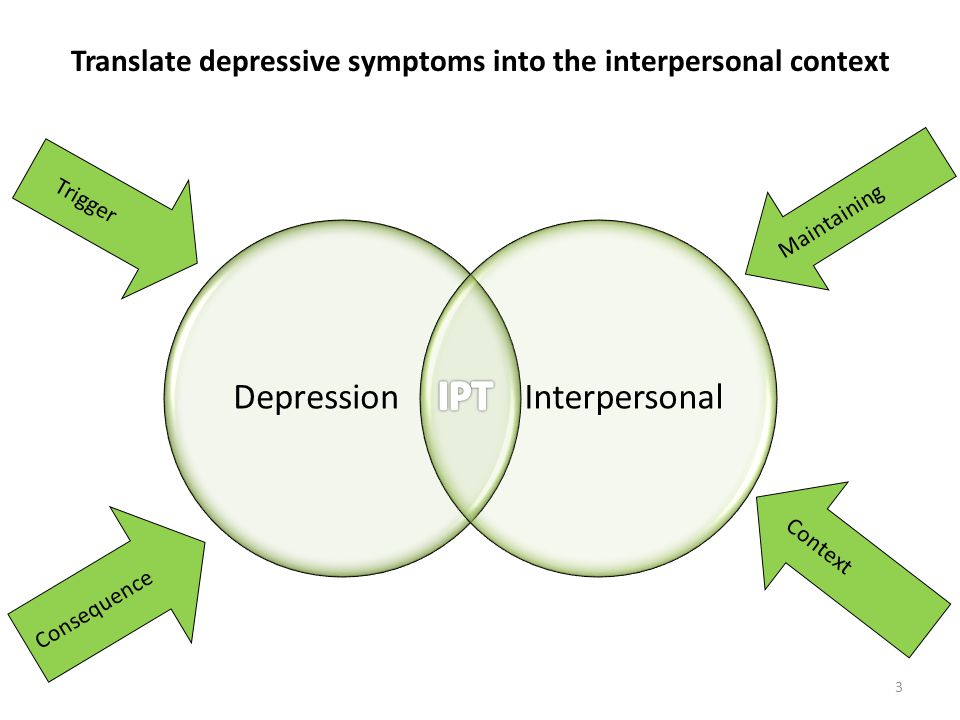 To do this, a psychotherapist practicing within the framework of Freud's classical psychodynamics uses the following tools:
To do this, a psychotherapist practicing within the framework of Freud's classical psychodynamics uses the following tools:
• Confrontation, which consists in the patient's awareness of the need to investigate those specific phenomena that may be the cause of his mental disorder.
• Clarification, as the clarification and separation of important mental phenomena from non-essential ones by their sharp focusing and artificial sharpening.
• Interpretation of the results of the analysis to determine the meaning and establish a causal relationship between the past event and the patient's present problems.
This is the most important tool in dynamic psychotherapy.
• Processing includes constant repetition, consistent adherence to the developed plan for integrating into the patient's consciousness the interpretations of the revealed connections between past and present mental phenomena. This is the longest stage in the work of the psychotherapist, going up to the patient's complete and final understanding of the results of psychoanalysis, which practically means the recovery and victory of the Ego.
• Analysis of dreams, which Freud considered "the royal road to the unconscious."
By the way, when working through, the patient's independent participation in the therapy process is also very important, which provides for work outside of school hours, i.e. outside of sessions.
The work of a psychotherapist practicing in the field of personality-oriented psychotherapy, which is the development of our domestic scientists on the basis of Myasishchev's pathogenetic psychotherapy, looks somewhat different. This concept appeared in the 30s and 40s. of the last century and its fundamental position was the idea of personality as a result of its dynamic relationship with the social environment. Psychotherapy in this case is aimed at restoring (reconstructing) the harmonious interaction of the individual with society. Myasishchev assigned the main role in understanding the personality to the experience of social relations, considering the biological in a person not as a personality or even a part of it, but only as a condition of personality. Otherwise, it can be said that the personality in reconstructive psychotherapy is considered as a system of relations with people, formed in specific social, cultural and economic conditions on the basis of the higher mental activity of the brain. Self-consciousness is an important structural component in this system; man's attitude towards himself. Developing later than all relationships and on their basis, self-consciousness completes the process of personality formation and makes it complete.
Otherwise, it can be said that the personality in reconstructive psychotherapy is considered as a system of relations with people, formed in specific social, cultural and economic conditions on the basis of the higher mental activity of the brain. Self-consciousness is an important structural component in this system; man's attitude towards himself. Developing later than all relationships and on their basis, self-consciousness completes the process of personality formation and makes it complete.
The main goal of personality-oriented psychotherapy is to clarify the life circumstances that led to overstrain and disorganization of the patient's psyche. For a successful therapeutic effect, the relationship between the psychotherapist and the patient is also important, but the role of the doctor, in contrast to the Freudian approach, is somewhat different - it involves his active rather than passive position. The main treatment technique in this case is a psychotherapeutic conversation and the authority of a psychotherapist, who is required to know life, the ability to patiently listen to the patient, a tactful and benevolent attitude towards him, along with the ability to resist, if necessary, the patient’s unacceptable tendencies in communication.
The basic tasks of a psychotherapeutic conversation include clarifying the following aspects:
• Features of life experience gained depending on age.
• Significant traumatic and happy memories.
• Systems of evaluation of oneself and others, likes and dislikes.
• The main motivation of the patient's own behavior.
• Interests, aspirations and needs.
And, finally, the achievement of the main task of the psychotherapist is the establishment and awareness by the patient of the relationship between the manifestations of the disease and inadequate response to current circumstances with the history of his life and the relationships formed by it. This is precisely the cardinal factor that ensures the success of reconstructive psychotherapy.
At the final stage, when the nervous tension subsides, the patient becomes more open, frank and liberated, begins to critically rethink his life positions, the psychotherapist begins to reconstruct the patient's disturbed relationship with society and himself.