How long to take antidepressants
Overview - Antidepressants - NHS
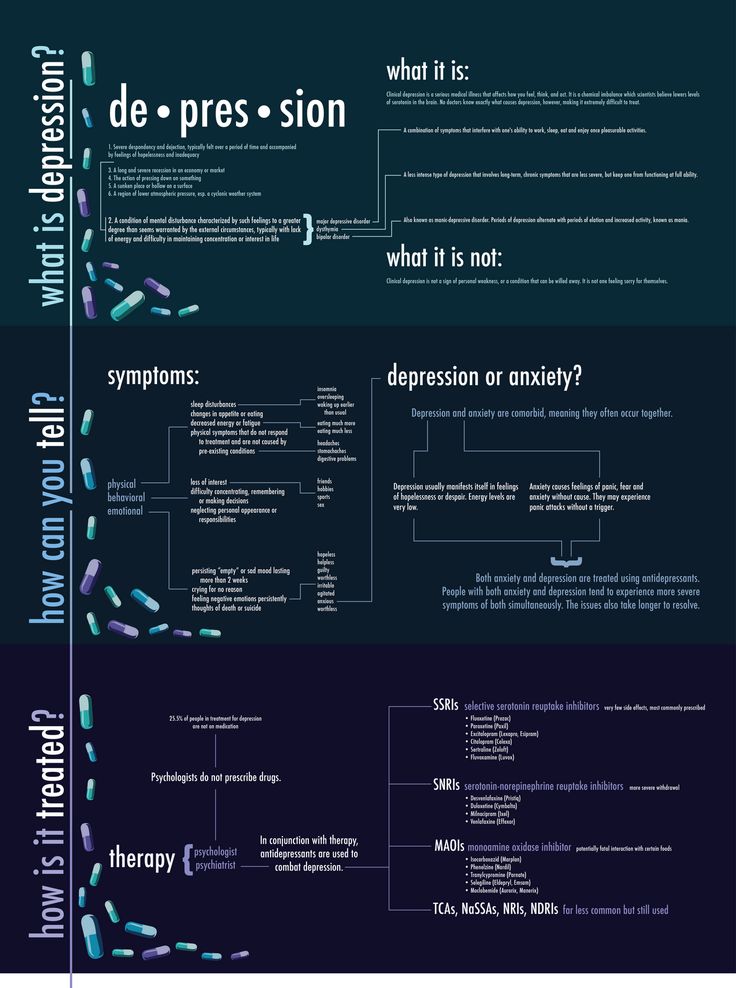
Antidepressants are a type of medicine used to treat clinical depression.
They can also be used to treat a number of other conditions, including:
- obsessive compulsive disorder (OCD)
- generalised anxiety disorder
- post-traumatic stress disorder (PTSD)
Antidepressants are also sometimes used to treat people with long-term (chronic) pain.
Read more about when antidepressants are used.
How antidepressants work
It's not known exactly how antidepressants work.
It's thought they work by increasing levels of chemicals in the brain called neurotransmitters. Certain neurotransmitters, such as serotonin and noradrenaline, are linked to mood and emotion.
Neurotransmitters may also affect pain signals sent by nerves, which may explain why some antidepressants can help relieve long-term pain.
While antidepressants can treat the symptoms of depression, they do not always address its causes. This is why they're usually used in combination with therapy to treat more severe depression or other mental health conditions.
How effective are antidepressants?
Research suggests that antidepressants can be helpful for people with moderate or severe depression.
They're not usually recommended for mild depression, unless other treatments like talking therapy have not helped.
Doses and duration of treatment
Antidepressants are usually taken in tablet form. When they're prescribed, you'll start on the lowest possible dose thought necessary to improve your symptoms.
Antidepressants usually need to be taken for 1 or 2 weeks (without missing a dose) before the benefit starts to be felt. It's important not to stop taking them if you get some mild side effects early on, as these effects usually wear off quickly.
If you take an antidepressant for 4 weeks without feeling any benefit, speak to your GP or mental health specialist. They may recommend increasing your dose or trying a different medicine.
A course of treatment usually lasts for at least 6 months after you start to feel better. Some people with recurrent depression may be advised to take them indefinitely.
Read more about antidepressant dosages.
Side effects
Different antidepressants can have a range of different side effects. Always check the information leaflet that comes with your medicine to see what the possible side effects are.
The most common side effects of antidepressants are usually mild. Side effects should improve within a few days or weeks of treatment, as the body gets used to the medicine.
Read more about:
- possible side effects of antidepressants
- cautions and interactions of antidepressants
Coming off antidepressants
Talk to your doctor before you stop taking antidepressants. It's important that you do not stop taking antidepressants suddenly.
Once you're ready to come off antidepressants, your doctor will probably recommend reducing your dose gradually over several weeks – or longer, if you have been taking them for a long time.
This is to help prevent any withdrawal symptoms you might get as a reaction to coming off the medicine.
Read more about stopping or coming off antidepressants.
Types of antidepressants
There are several different types of antidepressants.
Selective serotonin reuptake inhibitors (SSRIs)
SSRIs are the most widely prescribed type of antidepressants. They're usually preferred over other antidepressants, as they cause fewer side effects. An overdose is also less likely to be serious.
Fluoxetine is probably the best known SSRI (sold under the brand name Prozac). Other SSRIs include citalopram (Cipramil), escitalopram (Cipralex), paroxetine (Seroxat) and sertraline (Lustral).
Serotonin-noradrenaline reuptake inhibitors (SNRIs)
SNRIs are similar to SSRIs. They were designed to be a more effective antidepressant than SSRIs. However, the evidence that SNRIs are more effective in treating depression is uncertain. It seems that some people respond better to SSRIs, while others respond better to SNRIs.
It seems that some people respond better to SSRIs, while others respond better to SNRIs.
Examples of SNRIs include duloxetine (Cymbalta and Yentreve) and venlafaxine (Efexor).
Noradrenaline and specific serotonergic antidepressants (NASSAs)
NASSAs may be effective for some people who are unable to take SSRIs. The side effects of NASSAs are similar to those of SSRIs, but they're thought to cause fewer sexual problems. However, they may also cause more drowsiness at first.
The main NASSA prescribed in the UK is mirtazapine (Zispin).
Tricyclic antidepressants (TCAs)
TCAs are an older type of antidepressant. They're no longer usually recommended as the first treatment for depression because they can be more dangerous if an overdose is taken. They also cause more unpleasant side effects than SSRIs and SNRIs.
Exceptions are sometimes made for people with severe depression that fail to respond to other treatments. TCAs may also be recommended for other mental health conditions, such as OCD and bipolar disorder.
TCAs may also be recommended for other mental health conditions, such as OCD and bipolar disorder.
Examples of TCAs include amitriptyline, clomipramine, dosulepin, imipramine, lofepramine and nortriptyline.
Some types of TCAs, such as amitriptyline, can also be used to treat chronic nerve pain.
Serotonin antagonists and reuptake inhibitors (SARIs)
SARIs are not usually the first choice of antidepressant, but they may be prescribed if other antidepressants have not worked or have caused side effects.
The main SARI prescribed in the UK is trazodone (Molipaxin).
Monoamine oxidase inhibitors (MAOIs)
MAOIs are an older type of antidepressant that are rarely used nowadays.
They can cause potentially serious side effects so should only be prescribed by a specialist doctor.
Examples of MAOIs include tranylcypromine, phenelzine and isocarboxazid.
Other treatments for depression
Other treatments for depression include talking therapies such as cognitive behavioural therapy (CBT).
People with moderate to severe depression are usually treated using a combination of antidepressants and CBT. Antidepressants work quickly in reducing symptoms, whereas CBT takes time to deal with causes of depression and ways of overcoming it.
Regular exercise has also been shown to be useful for those with mild depression.
Read more about alternatives to antidepressants.
Yellow Card Scheme
The Yellow Card Scheme allows you to report suspected side effects from any type of medicine you're taking. It's run by a medicines safety watchdog called the Medicines and Healthcare products Regulatory Agency (MHRA).
It's run by a medicines safety watchdog called the Medicines and Healthcare products Regulatory Agency (MHRA).
See the Yellow Card Scheme website for more information.
Community content from HealthUnlockedHow Long Should You Take Antidepressants?
Written by Carolyn Crist
If you start to feel better while taking antidepressants, you may wonder how long you should take this medication or whether you can stop.
Expert guidelines about antidepressants can be confusing. They depend on a variety of factors, including:
- The type of prescription you take
- Your dosage
- The number of depressive episodes you’ve had
- Your risk of relapse
Whether it’s a good idea to stop depends on you.
“We know that taking antidepressants for too short a time might pose real risks for some people, but for others, taking them for longer could be more than you need,” says David Baron, a psychiatrist and provost of the Western University of Health Sciences in California.
“This decision needs to be made with a professional, just as a patient who takes insulin or chemotherapy would have specific discussions with their specialist,” he says. “Antidepressants can and do work, but they should be used like any other medication.”
If you and your doctor decide it’s time to stop, you’ll need to know the best way to do it and how to avoid possible side effects.
When to Stop
Under American Psychiatric Association guidelines, if you are taking an antidepressant for your first depressive episode, you should stay on it for at least 4 or 5 months after your symptoms of depression stop. Keep in mind that you may need to try several different antidepressants to find the right option for you, and even then, it can take 2 or 3 weeks to see an initial improvement. After that, it can take 3 to 6 months for symptoms to improve to the point that you are no longer depressed. Altogether, this could mean taking a prescription for about a year to get the full benefits.
If you have ongoing major depressive disorder, or you have had three or more depressive episodes, the APA recommends treatment for at least a few years. Doctors may also recommend longer treatment when the risk of relapse is high.
This can depend on a few factors including your:
- Family history of mental illness
- Other long-term medical or mental health problems
- Ongoing symptoms while you’re on medication
- Ongoing stressors, such as trouble sleeping or work or relationship problems
“Decide with your doctor what you expect to gain and improve from taking medication,” Baron says. “Poor sleep, low energy and low self-esteem symptoms might respond to medication, but antidepressants don’t take care of relationship problems.”
How to Stop
If you decide to stop taking antidepressants, don’t quit taking them on your own. And don’t stop all at once. A major drop in medication levels can trigger a relapse or other harmful symptoms, such as suicidal thoughts.
Work with your doctor to create a plan to gradually reduce your medication dose over time. Every antidepressant enters and exits the body at a different speed. It may take several weeks to decrease medication levels safely. During this process, you should schedule regular follow-ups so your doctor can closely monitor you for any side effects or signs of relapse.
You may also want to schedule sessions with a therapist to deal with other life issues, such as grief, low self-esteem, or negative thinking that may control your mood.
“Cognitive therapy can help people reexamine the accuracy of their negative beliefs, which can relieve their distress,” says Steven Hollon, a professor of psychiatry who researches the prevention and treatment of depression at Vanderbilt University in Nashville.
Consider your daily routine, too. Healthy lifestyle habits, such as proper sleep, good nutrition, regular physical activity, and stress reduction techniques, can help your body adjust to the changing medication levels.
What to Expect
Some people report side effects or noticeable changes when they lower their antidepressant dose. Common complaints include:
- Dizziness
- Fatigue
- Flu-like symptoms, such as chills and aches
Keep track of any symptoms you have and discuss them with your doctor. They may be able to further tweak your dose to reduce the discomfort or prescribe something else to relieve the symptoms.
If you quit taking antidepressants suddenly, you may get “antidepressant discontinuation syndrome,” especially if you’ve been taking medication for more than a month or two. Symptoms can include:
- Anxiety
- Insomnia
- Headaches
- Irritability
- Electric shock sensations
It’s important to talk to your doctor about these symptoms to avoid a relapse and to find the right solution to ease symptoms as your body adjusts.
Long-term use of antidepressants is associated with an increased risk of coronary artery disease, cerebrovascular disease, cardiovascular and overall mortality, but a reduced risk of hypertension and diabetes mellitus: a large observational study
is 6 months, with a continuing risk of recurrence - 2 years. Very often, patients continue to take drugs for years.
Very often, patients continue to take drugs for years. It is known that depression is associated with an increase in the incidence of CVD risk factors (smoking, obesity, physical inactivity) and so on. In this situation, it is very difficult to evaluate the safety profile of antidepressants in terms of cardiovascular complications and overall mortality in an observational study: it is not entirely clear which will have an adverse effect - antidepressants or depression itself. Therefore, the bulk of research on this topic, as a rule, causes a lot of comments.
The British Journal of Psychiatry Open published the results of an analysis of the UK Biobank registry, the design of which claims to account for the maximum number of associated risk factors, including behavioral and socioeconomic. This is supposed to help separate the effects of antidepressants and depression itself. The study included patients who initially did not suffer from CVD, did not take cardiometabolic drugs, and did not use antidepressants during the last 12 months before inclusion. Of the 222,121 participants included, 8% were taking antidepressants at 5 years and 6% at 10 years. Serotonin reuptake inhibitors and other antidepressants were analyzed separately (amitriptyline was excluded from the analysis as low doses are often prescribed in older patients for insomnia).
Of the 222,121 participants included, 8% were taking antidepressants at 5 years and 6% at 10 years. Serotonin reuptake inhibitors and other antidepressants were analyzed separately (amitriptyline was excluded from the analysis as low doses are often prescribed in older patients for insomnia).
Multivariate analysis taking into account a large number of risk factors showed that long-term use of serotonin reuptake inhibitors is associated with an increased risk of cerebrovascular disease (OR 1.34, 95% CI 1.02–1.77), cardiovascular mortality (OR 1.87, 95% CI 1.38–2.53) and death from all causes (OR 1.73, 1.48–2.03) after 10 years. For other antidepressants, similar patterns are revealed, but the odds ratios are higher: the OR for CHD is 1.99 (1.31–3.01), for cardiovascular death - 1.86 (1.10–3.15), for death from all causes - 2.2 (1.71–2.84). A relationship was found between doses of drugs and the risk of complications. Whether there is a causal relationship between antidepressants and increased mortality remains unclear. Of particular concern is the fact that the use of serotonin reuptake inhibitors is associated with a reduced risk of developing the main risk factors for CVD - diabetes (OR 0.68.95% CI 0.53–0.87) and hypertension (OR 0.77, 95% CI 0.66–0.89) at 10 years of follow-up. However, such a relationship is potentially possible, therefore, antidepressants should not be taken longer than necessary, it is advisable to use the minimum effective doses, and also actively engage in screening and correction of other CV risk factors in such patients.
Of particular concern is the fact that the use of serotonin reuptake inhibitors is associated with a reduced risk of developing the main risk factors for CVD - diabetes (OR 0.68.95% CI 0.53–0.87) and hypertension (OR 0.77, 95% CI 0.66–0.89) at 10 years of follow-up. However, such a relationship is potentially possible, therefore, antidepressants should not be taken longer than necessary, it is advisable to use the minimum effective doses, and also actively engage in screening and correction of other CV risk factors in such patients.
Adapted from:
Bansal, N., Hudda, M., Payne, R., Smith, D., Kessler, D., & Wiles, N. (2022). Antidepressant use and risk of adverse outcomes: Population-based cohort study. BJPsych Open, 8(5), E164. doi:10.1192/bjo.2022.563
https://www.cambridge.org/
Text: Shakhmatova O.O.
what are the side effects of antidepressants and how long can they be taken?
Among the diseases in which doctors do not recommend driving is depression.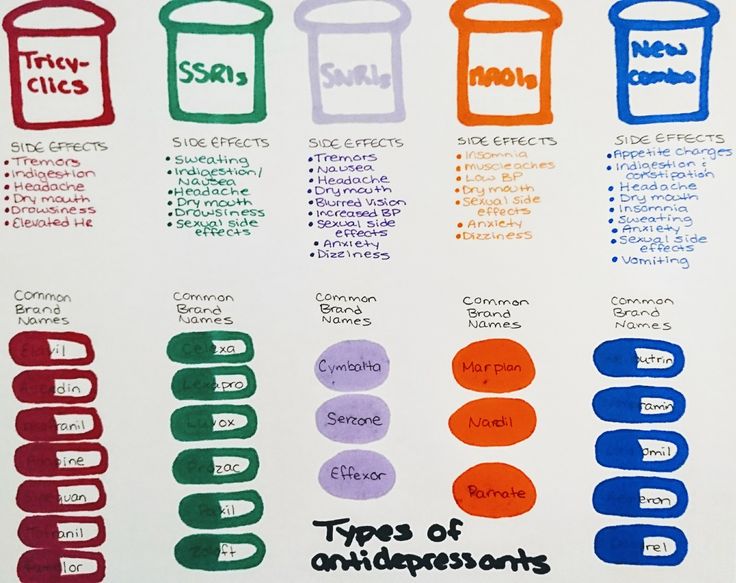 Mir24.tv previously wrote about this, referring to the general practitioner Rustem Osmanov. According to him, along with people suffering from epilepsy, schizophrenia and hallucinations, it is strongly recommended not to drive a car for those diagnosed with a depressive disorder. In addition, it is better not to drive for those who take antidepressants.
Mir24.tv previously wrote about this, referring to the general practitioner Rustem Osmanov. According to him, along with people suffering from epilepsy, schizophrenia and hallucinations, it is strongly recommended not to drive a car for those diagnosed with a depressive disorder. In addition, it is better not to drive for those who take antidepressants.
At the same time, there are more and more people around who are prone to such an ailment as depression. So, at the beginning of 2022, the demand for antidepressants and antipsychotics in Russia increased by 43% and 35%, respectively. Doctors warn: you can take such serious drugs only as directed by a psychotherapist or psychiatrist. Thoughtlessly taking antidepressants can lead to tragic consequences.
Unfortunately, there are more and more people with depression every year. This is especially true for large cities: for example, most recently Moscow was named the most depressing city in Russia. According to a sociological study, every eighth resident of the capital takes antidepressants, in St. Petersburg and the Moscow region - every ninth. The five "depressed regions" also included the Kaluga and Rostov regions.
Petersburg and the Moscow region - every ninth. The five "depressed regions" also included the Kaluga and Rostov regions.
How antidepressants work, who can take them and for how long, and most importantly, how safe they are - Mir24.tv learned the answers to these and other questions from doctors.
Antidepressants are a group of psychopharmacological drugs whose main task is to influence a person's emotions. As the psychiatrist, psychotherapist Mikhail Valuysky notes , antidepressants are not only chemically synthesized, but also natural.
To understand how antidepressants affect a person, let's first understand what depression is.
“There are substances in the brain that are located between nerve cells and help transmit information. These substances are called neurotransmitters. At the moment, the theory of the formation of depression is based on ideas about the lack of these substances, - explains psychotherapist Anton Kavetsky . – The mechanism involves serotonin, norepinephrine or dopamine. Antidepressants aim to increase these substances in a variety of ways.
Antidepressants aim to increase these substances in a variety of ways.
In addition, due to their effect on the neurotransmitter system, antidepressants are also used for other conditions. Often they are prescribed for anxiety spectrum disorders (generalized anxiety disorder, panic disorder, obsessive-compulsive disorder, etc.). Some antidepressants have a sedative effect and are often prescribed for sleep disorders.
Antidepressants are divided into several large groups. Mikhail Valuysky tells more about them.
There are other types of antidepressants, such as relatively new selective serotonin and norepinephrine reuptake inhibitors, atypical antidepressants, and the like.
“The history of the invention of antidepressants is quite interesting,” says Mikhail Valuysky. “A new remedy for tuberculosis was being studied. And in the studies they noticed: the patients taking it noted an improvement in mood, a decrease in the level of anxiety and a sense of doom, the disappearance of insomnia. That is, completely unplanned effects for an anti-tuberculosis drug. And with further research, tricyclic antidepressants were discovered.”
That is, completely unplanned effects for an anti-tuberculosis drug. And with further research, tricyclic antidepressants were discovered.”
Thus, there are many antidepressants, they are all different, each has its own niche, its own type of depression or anxiety disorder, its own type of enzyme activity and human constitution, etc.
Antidepressants affect a person's mood, the emotions that he experiences, indirectly, and not directly, explains Mikhail Valuysky.
“They affect the subcortical structures of the brain, the limbic system, normalizing their work. They do not strengthen them, do not stimulate them, but normalize work. The structures responsible for human emotions begin to work normally - as they should. With joyful stimuli - rejoice, with sad stimuli - be sad. In this way, antidepressants differ from drugs: by themselves, they do not cause an improvement in mood, euphoria. And drugs directly affect the pleasure centers. Therefore, you can’t get hooked on an antidepressant, you shouldn’t be afraid of it - just like taking it without a prescription, however, ”recalls the doctor.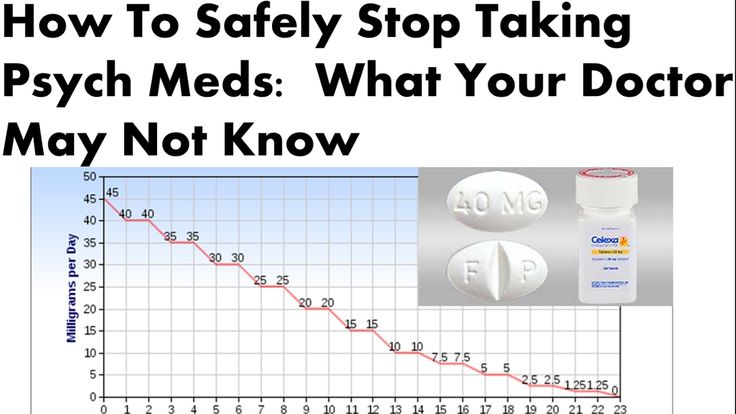
Antidepressants are used for a fairly wide range of disorders. These are not only depressions, but also anxiety disorders, obsessive-compulsive disorders (obsessive-compulsive disorder syndrome), panic attacks, sleep disturbances and the so-called somatophoric disorders - when mental problems manifest themselves in disruption of the internal organs. Antidepressants are also used to treat chronic pain syndrome, fibromyalgia, phantom pain, and post-traumatic stress disorder. “That is, antidepressants have a fairly wide range of indications. Preparations in practice for several decades, are well studied. Therefore, this is not magic, but the normal practice of any neurologist, psychiatrist and psychotherapist, ”says Mikhail Valuysky.
And yet, you should not write off the extensive list of side effects that trails behind each such drug. We will talk about how antidepressants affect the body below.
Nausea, the feeling of "electric shock" and the inability to complete sexual intercourse: what "surprises" to expect when taking antidepressants?
As mentioned above, antidepressants normalize the work of subcortical structures responsible for the emotions experienced by a person. And the duration of the course of treatment depends on which condition is required to be affected.
“If there is, for example, hyperproduction of anxiety, antidepressants act on the structures that generate it, and they stop doing it in such quantities. If it is a structure responsible for generating, for example, sadness, they affect it. If we are talking about depression, then according to the duration of taking the WHO recommendations are as follows: an antidepressant is used until the end of a depressive episode, when, according to tests, scales responsible for recognizing the severity of depression, a person gains the amount of a normal state. And another six months after that, in order to avoid a relapse, to teach a person to live and think without depression, so that the remaining negative thinking habits do not start again the “wrong” work of the subcortical structures.
As for all other conditions, you need to understand that antidepressants (with rare exceptions) are long-term medications.
Because they don't work directly. Until the work of the subcortical systems is rebuilt, until a person learns to feel, think, move, live differently, quite a long time passes. You should not be afraid of this - the drugs were invented for long-term use. Briefly, antidepressants are used in rather narrow, niche cases. For example, rarely, in a short course (no more than a month) - with severe depressive states of bipolar affective disorder. In all other cases, the dose, the regimen should be discussed with the attending physician, because the same drug can be taken differently for different diseases, ”says Mikhail Valuysky.
In general, the entry into therapy on antidepressants is always smooth: they usually start with a half or a quarter of the dose, gradually increasing it to the working one.
“Another important thing to know about antidepressants is that their anti-anxiety effect comes on immediately. In drugs with an analgesic effect, it also occurs immediately (“effect of the first dose”). But the antidepressant effect, that is, reducing melancholy, weakness, most often develops on the 21-40th day of admission. Therefore, you need to take them for a long time, do not despair, wait until they accumulate and start working. Cancellation goes just as smoothly: the dose is gradually reduced, in about 2-3 weeks. If you stop taking the drug abruptly, a withdrawal syndrome may occur - deterioration, fever, a feeling of melancholy and everything that a person was treated for, ”Mikhail Valuysky lists.
But the antidepressant effect, that is, reducing melancholy, weakness, most often develops on the 21-40th day of admission. Therefore, you need to take them for a long time, do not despair, wait until they accumulate and start working. Cancellation goes just as smoothly: the dose is gradually reduced, in about 2-3 weeks. If you stop taking the drug abruptly, a withdrawal syndrome may occur - deterioration, fever, a feeling of melancholy and everything that a person was treated for, ”Mikhail Valuysky lists.
“Antidepressants are most often prescribed for a course of at least 6 months,” says psychotherapist Anton Kavetsky. - Can be appointed for a longer period, even for life. When they need to be canceled, it is done gently and slowly: cutting the dose by half every week, and sometimes even more slowly.
As you know, the stronger the drug, the more side effects it has. And antidepressants in this sense are no exception.
“The most common side effect of taking antidepressants is in the gastrointestinal tract, because our intestines generally run on serotonin. And most often these side effects appear at the moment of entry into therapy, explains psychiatrist Mikhail Valuysky. - Somewhere on the 10-15th day, the brain gets used to it, and the “side effect” passes. It can be nausea, constipation or, conversely, diarrhea, heartburn, belching, etc. The second most common side effect of taking antidepressants is related to the cardiovascular system: a decrease / increase in pressure, an effect on heart rate. The third group - neurological symptoms: a feeling of "electric shock", dizziness, impaired vision or concentration. But side effects are quite rare and, I repeat, at the time of entry into therapy - then the body gets used to it.
And most often these side effects appear at the moment of entry into therapy, explains psychiatrist Mikhail Valuysky. - Somewhere on the 10-15th day, the brain gets used to it, and the “side effect” passes. It can be nausea, constipation or, conversely, diarrhea, heartburn, belching, etc. The second most common side effect of taking antidepressants is related to the cardiovascular system: a decrease / increase in pressure, an effect on heart rate. The third group - neurological symptoms: a feeling of "electric shock", dizziness, impaired vision or concentration. But side effects are quite rare and, I repeat, at the time of entry into therapy - then the body gets used to it.
Interestingly, in some cases, the side effects of antidepressants can, on the contrary, be used to treat certain ailments, such as: rapid ejaculation, eating disorders, menopausal changes and other problems, adds Anton Kavetsky.
“In terms of side effects, it's very common for anxiety symptoms to get worse at the start of treatment, but we're talking about this as an expected side effect and it goes away within a few days, weeks at most,” the doctor says. - In addition, antidepressants can affect the duration of sexual intercourse (to lengthen it too much, up to the inability to complete it), on weight (they can cause both its increase and decrease). Most antidepressants don't work right away. It may take a whole month to achieve the desired effect, and a person needs to function now. Therefore, it is sometimes necessary to prescribe other drugs, such as benzodiazepine tranquilizers, to quickly stop anxiety; antipsychotics to improve appetite or sleep.
- In addition, antidepressants can affect the duration of sexual intercourse (to lengthen it too much, up to the inability to complete it), on weight (they can cause both its increase and decrease). Most antidepressants don't work right away. It may take a whole month to achieve the desired effect, and a person needs to function now. Therefore, it is sometimes necessary to prescribe other drugs, such as benzodiazepine tranquilizers, to quickly stop anxiety; antipsychotics to improve appetite or sleep.
In addition, it is important to understand that depression varies and mood stabilizers are sometimes required. Antidepressants may increase the risk of suicide. This is due to the fact that a depressed person can think about it, but he has no strength at all. And when taking antidepressants, strength can appear before the world takes on colors and the desire to live appears, so sometimes other drugs are prescribed along with antidepressants to reduce risks.
To whom are antidepressants contraindicated?
Like any drug, antidepressants have a number of contraindications. For some, they should not be taken categorically, for others, it is recommended with caution. So, doctors advise taking them with caution for arrhythmias, kidney problems and many severe chronic diseases.
For some, they should not be taken categorically, for others, it is recommended with caution. So, doctors advise taking them with caution for arrhythmias, kidney problems and many severe chronic diseases.
It is also important to keep track of what medications you combine antidepressants with, notes Anton Kavetsky.
“Like all drugs, antidepressants pass through the liver and kidneys. But it is important to remember that some of them have a cardiotoxic effect. In addition, there are a lot of difficulties with prescribing when the patient has angle-closure glaucoma (there is a risk of increased intraocular pressure), prostate adenoma, and heart disorders (not for all antidepressants). It is also not recommended to prescribe with many drugs that affect the cardiovascular system and affect blood coagulation. Also, some antidepressants are not compatible with each other,” says the psychotherapist.
A separate category that should definitely be mentioned here is children and pregnant women.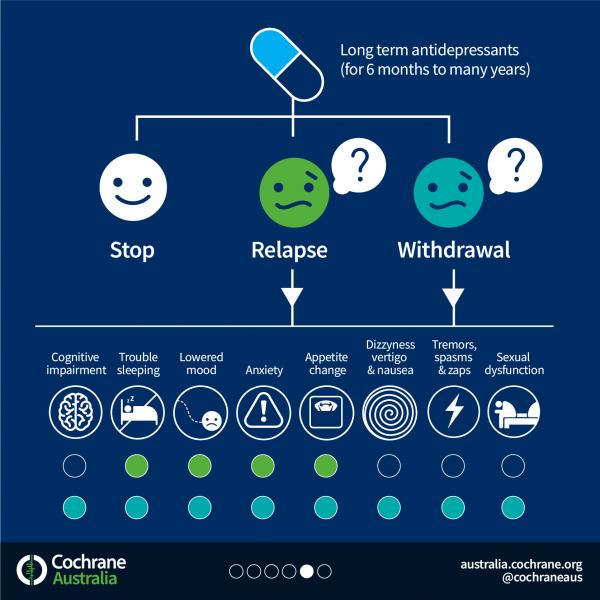 Of course, it cannot be said that taking antidepressants will add health to them, but sometimes you still have to resort to them.
Of course, it cannot be said that taking antidepressants will add health to them, but sometimes you still have to resort to them.
“There are antidepressants for children,” says doctor Mikhail Valuysky. - There are drugs that have passed clinical trials, they can be taken by children. Again, only the doctor knows which ones. Parents who are worried about the safety of the drug can be advised to look at the instructions, which say at what age the drug can be used and in what dosages.
“There are some antidepressants that are legal for children, but there are very few of them. But it is important to understand that it is always a risk. It is difficult to predict how the intake of a psychotropic drug will affect the developing nervous system of a growing organism, ”admits psychotherapist Anton Kavetsky.
Approximately the same situation with pregnant women. There is no single antidepressant recommended by the medical community for them.
“There is a drug that can be used during pregnancy (it is quite often used for perinatal hepatotoxicity, liver damage during pregnancy).
It has a mild antidepressant effect. But most often it is dripped in hospitals. Therefore, if a person has some kind of chronic affective mental disorder (depressive, anxiety, obsessive-compulsive), then it is advisable to finish the course of taking the drugs before pregnancy. And before pregnancy, complete a course of psychotherapy in order to have the skills and techniques to cope with your emotional state during pregnancy and breastfeeding, ”advises Mikhail Valuysky.
What if I get pregnant while taking antidepressants? Most likely, they will have to be canceled, and immediately and without gradual cancellation, says Valuysky. “But in any case, all this should be discussed with the attending physicians - an obstetrician-gynecologist, a psychotherapist. And, of course, it’s better for them to work in tandem, because many drugs say so: taking during pregnancy should be only after carefully weighing the harm to the fetus and the benefit to the mother, ”he says. Anton Kavetsky also advises immediately canceling any psychotropic drugs in the event of pregnancy - of course, under the supervision of specialists.
Many people are also interested in the question: do antidepressants affect reproductive function? Doctors assure: everything is ambiguous here. “There are a few studies that show that antidepressants can affect sperm. A great difficulty can be a delay in ejaculation in men. Separately, a decrease in libido can become a problem, ”says Anton Kavetsky.
Mikhail Valuysky also notes that when taking antidepressants, erectile dysfunction and difficulty achieving orgasm can be observed. This does not affect the actual fertilization in any way, but it can affect the course and quality of sexual intercourse.
“In general, antidepressants are a very important and good group of drugs,” concludes Dr. Valuysky. – They breathed hope and give a new quality of life to a huge number of people, not being drugs and substitutes for something in life. As a psychotherapist, I can say that psychotherapy and antidepressants are things created for each other, not contradictory, but mutually helping.
Learn more