How does ptsd affect daily life
Post-traumatic stress disorder (PTSD) - Symptoms and causes
Overview
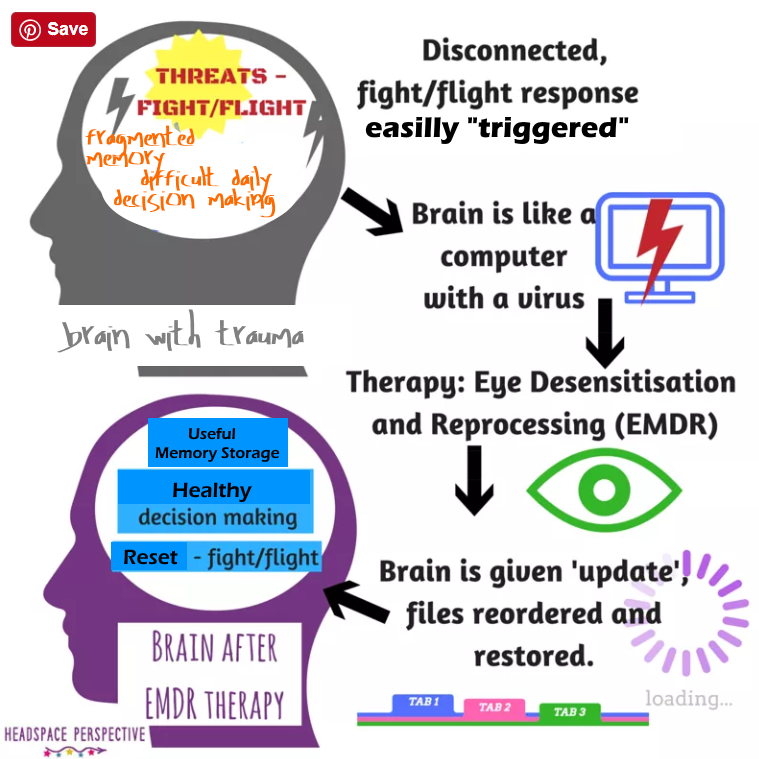
Post-traumatic stress disorder (PTSD) is a mental health condition that's triggered by a terrifying event — either experiencing it or witnessing it. Symptoms may include flashbacks, nightmares and severe anxiety, as well as uncontrollable thoughts about the event.
Most people who go through traumatic events may have temporary difficulty adjusting and coping, but with time and good self-care, they usually get better. If the symptoms get worse, last for months or even years, and interfere with your day-to-day functioning, you may have PTSD.
Getting effective treatment after PTSD symptoms develop can be critical to reduce symptoms and improve function.
Products & Services
- Book: Mayo Clinic Family Health Book, 5th Edition
- Newsletter: Mayo Clinic Health Letter — Digital Edition
Symptoms
Post-traumatic stress disorder symptoms may start within one month of a traumatic event, but sometimes symptoms may not appear until years after the event. These symptoms cause significant problems in social or work situations and in relationships. They can also interfere with your ability to go about your normal daily tasks.
PTSD symptoms are generally grouped into four types: intrusive memories, avoidance, negative changes in thinking and mood, and changes in physical and emotional reactions. Symptoms can vary over time or vary from person to person.
Intrusive memories
Symptoms of intrusive memories may include:
- Recurrent, unwanted distressing memories of the traumatic event
- Reliving the traumatic event as if it were happening again (flashbacks)
- Upsetting dreams or nightmares about the traumatic event
- Severe emotional distress or physical reactions to something that reminds you of the traumatic event
Avoidance
Symptoms of avoidance may include:
- Trying to avoid thinking or talking about the traumatic event
- Avoiding places, activities or people that remind you of the traumatic event
Negative changes in thinking and mood
Symptoms of negative changes in thinking and mood may include:
- Negative thoughts about yourself, other people or the world
- Hopelessness about the future
- Memory problems, including not remembering important aspects of the traumatic event
- Difficulty maintaining close relationships
- Feeling detached from family and friends
- Lack of interest in activities you once enjoyed
- Difficulty experiencing positive emotions
- Feeling emotionally numb
Changes in physical and emotional reactions
Symptoms of changes in physical and emotional reactions (also called arousal symptoms) may include:
- Being easily startled or frightened
- Always being on guard for danger
- Self-destructive behavior, such as drinking too much or driving too fast
- Trouble sleeping
- Trouble concentrating
- Irritability, angry outbursts or aggressive behavior
- Overwhelming guilt or shame
For children 6 years old and younger, signs and symptoms may also include:
- Re-enacting the traumatic event or aspects of the traumatic event through play
- Frightening dreams that may or may not include aspects of the traumatic event
Intensity of symptoms
PTSD symptoms can vary in intensity over time.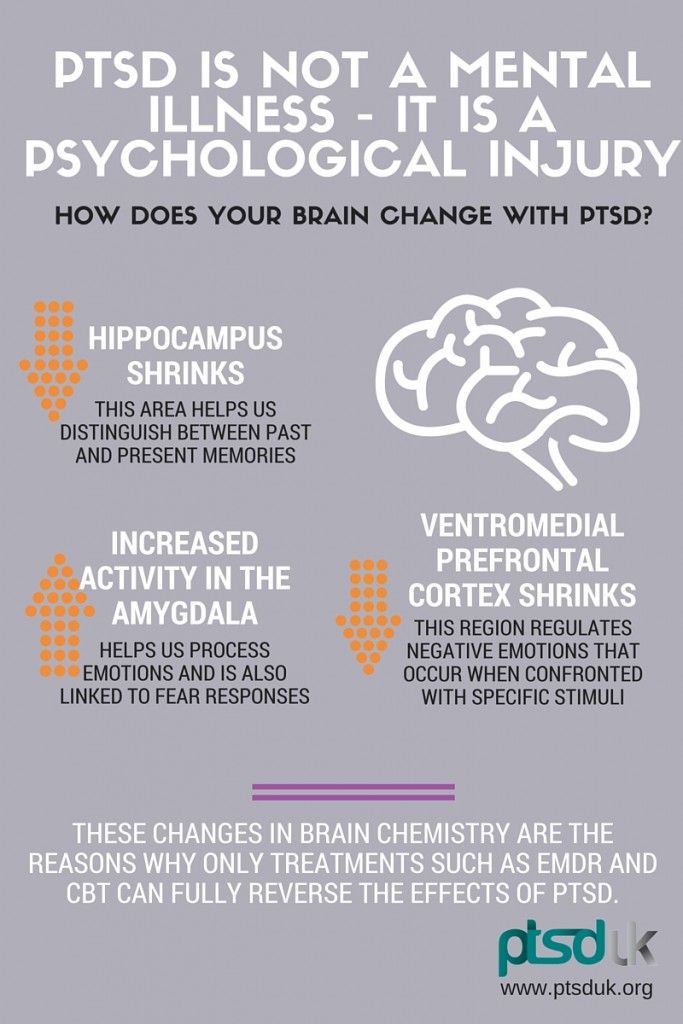 You may have more PTSD symptoms when you're stressed in general, or when you come across reminders of what you went through. For example, you may hear a car backfire and relive combat experiences. Or you may see a report on the news about a sexual assault and feel overcome by memories of your own assault.
You may have more PTSD symptoms when you're stressed in general, or when you come across reminders of what you went through. For example, you may hear a car backfire and relive combat experiences. Or you may see a report on the news about a sexual assault and feel overcome by memories of your own assault.
When to see a doctor
If you have disturbing thoughts and feelings about a traumatic event for more than a month, if they're severe, or if you feel you're having trouble getting your life back under control, talk to your doctor or a mental health professional. Getting treatment as soon as possible can help prevent PTSD symptoms from getting worse.
If you have suicidal thoughts
If you or someone you know has suicidal thoughts, get help right away through one or more of these resources:
- Reach out to a close friend or loved one.
- Contact a minister, a spiritual leader or someone in your faith community.
- Call a suicide hotline number — in the United States, call the National Suicide Prevention Lifeline at 1-800-273-TALK (1-800-273-8255) to reach a trained counselor.
 Use that same number and press 1 to reach the Veterans Crisis Line.
Use that same number and press 1 to reach the Veterans Crisis Line. - Make an appointment with your doctor or a mental health professional.
When to get emergency help
If you think you may hurt yourself or attempt suicide, call 911 or your local emergency number immediately.
If you know someone who's in danger of attempting suicide or has made a suicide attempt, make sure someone stays with that person to keep him or her safe. Call 911 or your local emergency number immediately. Or, if you can do so safely, take the person to the nearest hospital emergency room.
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.
To provide you with the most relevant and helpful information, and understand which
information is beneficial, we may combine your email and website usage information with
other information we have about you. If you are a Mayo Clinic patient, this could
include protected health information. If we combine this information with your protected
health information, we will treat all of that information as protected health
information and will only use or disclose that information as set forth in our notice of
privacy practices. You may opt-out of email communications at any time by clicking on
the unsubscribe link in the e-mail.
If you are a Mayo Clinic patient, this could
include protected health information. If we combine this information with your protected
health information, we will treat all of that information as protected health
information and will only use or disclose that information as set forth in our notice of
privacy practices. You may opt-out of email communications at any time by clicking on
the unsubscribe link in the e-mail.
Causes
You can develop post-traumatic stress disorder when you go through, see or learn about an event involving actual or threatened death, serious injury or sexual violation.
Doctors aren't sure why some people get PTSD. As with most mental health problems, PTSD is probably caused by a complex mix of:
- Stressful experiences, including the amount and severity of trauma you've gone through in your life
- Inherited mental health risks, such as a family history of anxiety and depression
- Inherited features of your personality — often called your temperament
- The way your brain regulates the chemicals and hormones your body releases in response to stress
Risk factors
People of all ages can have post-traumatic stress disorder. However, some factors may make you more likely to develop PTSD after a traumatic event, such as:
However, some factors may make you more likely to develop PTSD after a traumatic event, such as:
- Experiencing intense or long-lasting trauma
- Having experienced other trauma earlier in life, such as childhood abuse
- Having a job that increases your risk of being exposed to traumatic events, such as military personnel and first responders
- Having other mental health problems, such as anxiety or depression
- Having problems with substance misuse, such as excess drinking or drug use
- Lacking a good support system of family and friends
- Having blood relatives with mental health problems, including anxiety or depression
Kinds of traumatic events
The most common events leading to the development of PTSD include:
- Combat exposure
- Childhood physical abuse
- Sexual violence
- Physical assault
- Being threatened with a weapon
- An accident
Many other traumatic events also can lead to PTSD, such as fire, natural disaster, mugging, robbery, plane crash, torture, kidnapping, life-threatening medical diagnosis, terrorist attack, and other extreme or life-threatening events.
Complications
Post-traumatic stress disorder can disrupt your whole life ― your job, your relationships, your health and your enjoyment of everyday activities.
Having PTSD may also increase your risk of other mental health problems, such as:
- Depression and anxiety
- Issues with drugs or alcohol use
- Eating disorders
- Suicidal thoughts and actions
Prevention
After surviving a traumatic event, many people have PTSD-like symptoms at first, such as being unable to stop thinking about what's happened. Fear, anxiety, anger, depression, guilt — all are common reactions to trauma. However, the majority of people exposed to trauma do not develop long-term post-traumatic stress disorder.
Getting timely help and support may prevent normal stress reactions from getting worse and developing into PTSD. This may mean turning to family and friends who will listen and offer comfort. It may mean seeking out a mental health professional for a brief course of therapy. Some people may also find it helpful to turn to their faith community.
Some people may also find it helpful to turn to their faith community.
Support from others also may help prevent you from turning to unhealthy coping methods, such as misuse of alcohol or drugs.
By Mayo Clinic Staff
Related
Associated Procedures
Products & Services
Post-traumatic stress disorder (PTSD) - Better Health Channel
Post-traumatic stress disorder (PTSD) is a set of reactions that can develop in people who have experienced or witnessed a traumatic event that threatens their life or safety (or of others around them). This could be a car or other serious accident, physical or sexual assault, war-related events or torture, or a natural disaster such as bushfire or flood.
In the first days and weeks after a traumatic event, people often experience heightened arousal, alertness, looking for danger and being on guard. These reactions often alternate with numbness and detachment. It also brings constant memories of the event and feelings it may happen again. It also evokes strong feelings of fear, sadness, guilt, anger, or grief. Generally these reactions and feelings will resolve on their own over the next few weeks, however if the reactions and distress continue, it may mean that the person has is at risk for developing PTSD or another mental health condition.
It also evokes strong feelings of fear, sadness, guilt, anger, or grief. Generally these reactions and feelings will resolve on their own over the next few weeks, however if the reactions and distress continue, it may mean that the person has is at risk for developing PTSD or another mental health condition.
Anyone can develop PTSD following a traumatic event, but people are at greater risk if:
- the event involved physical or sexual assault
- they experienced intense helplessness
- the event involved something they never thought would happen to them
- they have had other traumatic experiences involving helplessness or danger including physical or sexual abuse, car accidents, criminal events, natural disasters or conflict
- they have suffered from PTSD in the past.
Symptoms of PTSD
A person with PTSD has four main types of difficulties:
- Re-living the traumatic event through unwanted and recurring memories, flashbacks or vivid nightmares.
 There may be intense emotional or physical reactions when reminded of the event including sweating, heart palpitations, anxiety or panic.
There may be intense emotional or physical reactions when reminded of the event including sweating, heart palpitations, anxiety or panic. - Avoiding reminders of the event, such as thoughts, feelings, people, places, activities or situations that bring back memories of the event. They may feel numb, empty or detached.
- Negative changes in feelings and thoughts, such as feeling angry, afraid, guilty, flat or numb, developing beliefs such as “I’m bad” or “The world’s unsafe”, and feeling cut off from others.
- Being overly alert or ‘wound up’ indicated by sleeping difficulties, irritability, lack of concentration, becoming easily startled and constantly being on the lookout for signs of danger.
A health practitioner may diagnose PTSD if a person has symptoms in each of these four areas for a month or more, which lead to significant distress or impacts on their ability to work and study, their relationships and day-to-day life.
People with PTSD can also have what are termed ‘dissociative experiences’, which are frequently described as:
- “It was as though I wasn’t even there.
 ”
” - “Time was standing still.”
- “I felt like I was watching things happen from above.”
PTSD in children and teenagers
Older children and teenagers experience similar problems to adults when they develop PTSD. Younger children can express distress in a different way. For example, they may re-live the traumatic event through repetitive play rather than having unwanted memories of the event during the day. Many children have frightening dreams without recognisable content rather than nightmares that replay the traumatic event. Children may also lose interest in play, become socially withdrawn, or have extreme temper tantrums.
About one third of children who experience a traumatic event will develop PTSD.
Other problems that can develop alongside PTSD include anxiety or depression, defiant behaviour, attention deficit hyperactivity disorder, and in teenagers and young adults, suicidal thoughts and alcohol or drug use.
Impact of PTSD on relationships and day-to-day life
PTSD can affect a person’s ability to work, perform day-to-day activities or relate to their family and friends. A person with PTSD can often seem uninterested or distant as they try not to think or feel in order to block out painful memories. They may stop them from participating in family life or ignore offers of help. This can lead to loved ones feeling shut out.
A person with PTSD can often seem uninterested or distant as they try not to think or feel in order to block out painful memories. They may stop them from participating in family life or ignore offers of help. This can lead to loved ones feeling shut out.
It is important to remember that these behaviours are part of the problem. People with PTSD need the support of family and friends but may not understand what is happening to them or think that they need help.
When PTSD goes on for some time, it is not unusual for people to experience other mental health problems at the same time. In fact, up to 80 per cent of people who have long-standing PTSD develop additional problems - most commonly depression, anxiety, and alcohol or other substance misuse. These may have developed directly in response to the traumatic event or as a result of the effects of having PTSD.
Risky alcohol and drug use with PTSD
People commonly use alcohol or other drugs to blunt the emotional pain that they are experiencing. Alcohol and drugs may help block out painful memories in the short term, but they can get in the way of a successful recovery and cause other serious problems.
Alcohol and drugs may help block out painful memories in the short term, but they can get in the way of a successful recovery and cause other serious problems.
When to seek help for PTSD
A person who has experienced a traumatic event should seek professional help if they:
- don’t feel any better after two weeks
- feel highly anxious or distressed
- have reactions to the traumatic event that are interfering with home, work and/or relationships
- are thinking of harming themselves or someone else.
Some of the signs that a problem may be developing are:
- being constantly on edge or irritable
- having difficulty performing tasks at home or at work
- being unable to respond emotionally to others
- being unusually busy to avoid issues
- taking risks or not caring what happens to oneself
- using alcohol, drugs or gambling to cope
- having severe sleeping difficulties.
Support is important for recovery
Many people experience some of the symptoms of PTSD in the first two weeks after a traumatic event, but most recover with the help of family and friends. For this reason, for a diagnosis of PTSD is not made until a month after the event. Treatment does not usually start for at least two or more weeks after a traumatic experience. However if the event is very distressing and emotions and reactions are intense, it is advisable to seek help as early as possible to understand what is happening and help recovery to start.
For this reason, for a diagnosis of PTSD is not made until a month after the event. Treatment does not usually start for at least two or more weeks after a traumatic experience. However if the event is very distressing and emotions and reactions are intense, it is advisable to seek help as early as possible to understand what is happening and help recovery to start.
It is important during the first few days and weeks after a traumatic event to get whatever help is needed. This may include accessing information, people and resources that can help you to recover. Support from family and friends may be all that is needed. Otherwise, a doctor is the best place to start to get further help.
Treatment for PTSD
If you are still experiencing problems after two weeks, a doctor or mental health professional may discuss starting treatment. Effective treatments are available. Most involve psychological treatment such as counselling to understand what is happening and to develop ways of managing reactions, but medication can also be helpful. Generally, it’s best to start with psychological treatment rather than use medication as the first and only solution to the problem.
Generally, it’s best to start with psychological treatment rather than use medication as the first and only solution to the problem.
The cornerstone of treatment for PTSD involves confronting the traumatic memory and working through thoughts and beliefs associated with the experience as part of a safe relationship with a trained person.
Trauma-focussed treatments can:
- reduce PTSD symptoms
- lessen anxiety and depression
- improve a person’s quality of life
- be effective for people who have experienced prolonged or repeated traumatic events, though treatment may be required for a longer period.
Treatment for children and teenagers with PTSD
For children and teenagers who are struggling to recover after a traumatic event, the recommended treatment is trauma-focussed cognitive behavioural therapy (CBT). This treatment involves:
- learning about the type of traumatic event experienced (e.g. how common it is) and common reactions to trauma
- teaching how to relax and manage anxiety
- helping to create a coherent story of the traumatic event, and correct any unhelpful beliefs about the event such as self-blame
- gradual exposure to trauma-related objects or situations that are feared or avoided
- helping to get back into everyday activities.

- Çrregullimi i stresit post-traumatik (Post-traumatic stress disorder - Albanian)
- اضطراب ما بعد الصدمة (Post-traumatic stress disorder - Arabic)
- 创伤后应激障碍 (Post-traumatic stress disorder - Chinese Simplified)
- 創傷後壓力症 (Post-traumatic stress disorder - Chinese Traditional)
- اختلال استرس پس از سانحه (Post-traumatic stress disorder - Dari)
- Διαταραχή μετατραυματικού στρες (Post-traumatic stress disorder - Greek)
- पोस्ट-ट्रॉमैटिक स्ट्रेस डिसऑर्डर (अभिघातजन्य तनाव विकार) (Post-traumatic stress disorder - Hindi)
- Disturbo post-traumatico da stress (Post-traumatic stress disorder - Italian)
- ਸਦਮੇ ਤੋਂ ਬਾਅਦ ਦਾ ਤਣਾਅ ਵਿਕਾਰ (Post-traumatic stress disorder - Punjabi)
- Ugonjwa wa mfadhaiko baada ya kiwewe (Post-traumatic stress disorder - Swahili)
- Rối loạn căng thẳng sau chấn thương (Post-traumatic stress disorder - Vietnamese)
Where to get help
- Your GP (doctor)
- Your mental health specialist, such as a psychiatrist, psychologist, counsellor or social worker
- Your local community health centre
- Australian Psychological Society Referral Service Tel.
 1800 333 497
1800 333 497 - Phoenix Australia Centre for Post-traumatic Mental Health Tel. (03) 9035 5599
- Centre for Grief and Bereavement Tel. 1800 642 066
General telephone counselling services can provide advice:
- Lifeline Tel. 13 11 14
- GriefLine Tel. 1300 845 745
- beyondblue Tel. 1300 22 4636
- NURSE-ON-CALL Tel. 1300 60 60 24 – for expert health information and advice (24 hours, 7 days)
PTSD
") end if %>
Variant of Acrobat Samana Gaze | Acrobat Reader Samana Download
PTSD is a normal response
for severe traumatic events.
This booklet deals with signs,
symptoms and treatments for PTSD.
New York State
Department of Mental Health
Have you experienced a terrible and dangerous event? Note please, those cases in which you recognize yourself.
- Sometimes, out of the blue, everything that happened to me is happening again. I never know when to expect it again.
- I have nightmares and memories of the terrible incident which I have experienced.
- I avoid places that remind me of that incident.
- I jump on the spot and feel uneasy at any sudden movement or surprise. I feel alert all the time.
- It's hard for me to trust someone and get close to someone.
- Sometimes I just feel emotionally drained and deaf.
- I get angry very easily.
- I am tormented by guilt that others died, but I survived.
- I sleep poorly and experience muscle tension.
PTSD is a very serious condition that needs to be treated.
Many people who have experienced terrible events suffer from this disease.
It is not your fault that you fell ill, and you should not suffer from it.
Read this booklet to find out how you can be helped.
You can get well and enjoy life again!
What is post-traumatic stress disorder (PTSD/PTSD)?
PTSD is a very serious condition. PTSD symptoms may occur in a person who has experienced a terrible traumatic event. This disease is susceptible medical and therapeutic treatment.
PTSD can occur after you:
- Have been a victim of sexual abuse
- Have been a victim of physical or emotional domestic violence
- Victim of a violent crime
- Been in a car accident or plane crash
- Survived a hurricane, tornado, or fire
- Were at war
- Survived a life-threatening event
- Witnessed any of the above events
If you have post-traumatic stress disorder, you often have nightmares or memories associated with the event. you try to hold on away from anything that might remind you of the experience.
You are bitter and unable to trust or care for others. You are always on your guard and see a hidden threat in everything. You become not by itself, when something happens suddenly and without warning.
You are always on your guard and see a hidden threat in everything. You become not by itself, when something happens suddenly and without warning.
When does PTSD start and how long does it last?
In most cases, post-traumatic stress manifests itself approximately three months after the traumatic event. In some cases, signs Post-traumatic stress symptoms only show up years later. Post-traumatic Stress affects people of all ages. Even children are not immune from it.
Some get better after six months, others may suffer from it illness for much longer.
Am I the only one with this condition?
No, you are not alone. Every year, 5.2 million Americans suffer from PTSD.
Women suffer from this disease two and a half times more often than men. The most common traumatic events that cause PTSD in men are: rape, participation in hostilities, abandonment and abuse in childhood. The most traumatic events in women are rape, sexual molestation, physical assault, threat weapons and childhood abuse.
What other conditions can accompany PTSD?
Common depression, alcoholism and drug addiction, or other anxiety disorders. The likelihood of successful treatment increases if these comorbidities to identify and treat in time.
Frequent headaches, gastroenterological problems, problems with the immune system, dizziness, chest pain or discomfort in other parts of the body. It often happens that a doctor treats physical symptoms, unaware that their cause lies in PTSD.
The National Institute of Mental Health (NIMH) recommends therapists to learn from patients about experiences of violence, recent losses and traumatic events, especially when symptoms persist are returning. After diagnosing PTSD, it is recommended to refer patient to a mental health specialist who has experience in the treatment of patients with PTSD.
What should I do to help myself in this situation?
Talk to your doctor and tell him about your experience, and how you feel. If you are visited by terrible memories, overcomes depression and sadness if you have trouble sleeping and constantly embittered - you should tell your doctor about all this. Tell him Are any of these conditions preventing you from doing your daily activities? lead a normal life. You may want to show this booklet to your doctor. This may help explain to him how you feel. Ask your doctor examine you to make sure there are no physical illnesses.
If you are visited by terrible memories, overcomes depression and sadness if you have trouble sleeping and constantly embittered - you should tell your doctor about all this. Tell him Are any of these conditions preventing you from doing your daily activities? lead a normal life. You may want to show this booklet to your doctor. This may help explain to him how you feel. Ask your doctor examine you to make sure there are no physical illnesses.
Ask your doctor if he has had patients with post-traumatic stress. If your doctor does not have a special preparation, ask him for directions to doctor with relevant experience.
How can a doctor or psychotherapist help me?
Your doctor may prescribe medicine to help reduce your fear or tension. However, it should be borne in mind that usually several weeks before the medicine starts to work.
Many PTSD sufferers benefit from talking with a professional or other people who have experienced traumatic events. This is called "therapy". Therapy will help you get over your nightmare.
This is called "therapy". Therapy will help you get over your nightmare.
One man's story:
"After I was attacked, I He constantly felt fear and depression, became irritable. I couldn't sleep well and lost my appetite. Even when I tried not think about what happened, I was still tormented nightmares and terrible memories.
“I was completely at a loss and didn't know what to do. one buddy advised to see a doctor. My doctor helped me find a specialist in post-traumatic stress."
“I needed a lot of strength, but after medication and a course of therapy, I gradually come to my senses. It’s good that I called my doctor then.”
PTSD and the military
If you are in the military, you have probably been in combat. You, probably got into terrible and life-threatening situations. They shot at you you have seen your friend shot, you have seen death. experienced you events can cause PTSD.
Experts say that PTSD occurs:
- Nearly 30% of Vietnam War veterans
- Nearly 10% of Gulf War veterans (Operation Desert Storm)
- Almost 25% of veterans of the war in Afghanistan (operations "Introducing freedom") and veterans of the war in Iraq (operations "Iraqi Freedom")
Other factors of the military situation can serve as an additional stress to and so stressful situation and can contribute to the development of PTSD and other mental problems. Among these factors are the following: your military specialty, the political aspects of the war, where the battle takes place and who your enemy is.
Another reason that contributes to PTSD in military personnel can be Military Sexual Assault (MST) – any form of sexual harassment or sexual abuse while serving in the military. MST can happen with men and women, and can occur in peacetime, during war training or during the war.
Veterans Affairs (VA) health care approximately:
- 23 out of 100 women (23%) report sexual violence during military service
- 55 out of 100 women (55%) and 38 out of 100 men (38%) were exposed to sexual harassment while serving in the army
Although the trauma of sexual assault is more common in the military among women, more than half of veterans who have experienced sexual trauma violence in the army - it's men.
Remember, you can get the help you need right now:
Tell your doctor about your experience and how you feel. If your doctor does not have special training in the treatment of PTSD, ask him for a referral to a doctor who has relevant experience.
PTSD research
To help those suffering from PTSD, the National Institute of Conservation Mental Health (NIMH) supports research into the study of PTSD, as well as other thematically related to PTSD research on problems anxiety and fear. The challenge for research is to find new ways to help people cope with trauma, as well as find new treatment options and, The main thing is to prevent disease.
Research on possible risk factors for PTSD
Today, the attention of many scientists is focused on genes that play a role in having terrible memories. Understanding the mechanism of "creation" of scary memories can help improve or find new ways to alleviate symptoms of PTSD. For example, PTSD researchers have identified genes that are responsible for:
For example, PTSD researchers have identified genes that are responsible for:
Statmin is a protein involved in the formation of terrible memories. During one experiment, mice were placed in environment designed to instill fear in them. In this situation mice lacking the statmin gene, in contrast to normal mice were less likely to "freeze" - i.e. exercise natural defensive response to danger. Also in the environment designed to evoke innate fear in them, they demonstrated it to a lesser extent than normal mice, more willingly mastering the open "dangerous" space. 1
GRP (gastrin-releasing peptide/GRP) - signal substance brain released during emotional events. At in mice, GWP helps control the fear response, and lack of GWP can lead to a longer memory of fear. 2
Scientists have also discovered a variant of the 5-HTTLPR gene that controls serotonin (a brain substance associated with mood), which, as it turns out, feeds the fear response. 3 It seems that, like in the case of other mental disorders, in the development of PTSD different genes are involved, each of which contributes to the formation of the disease.
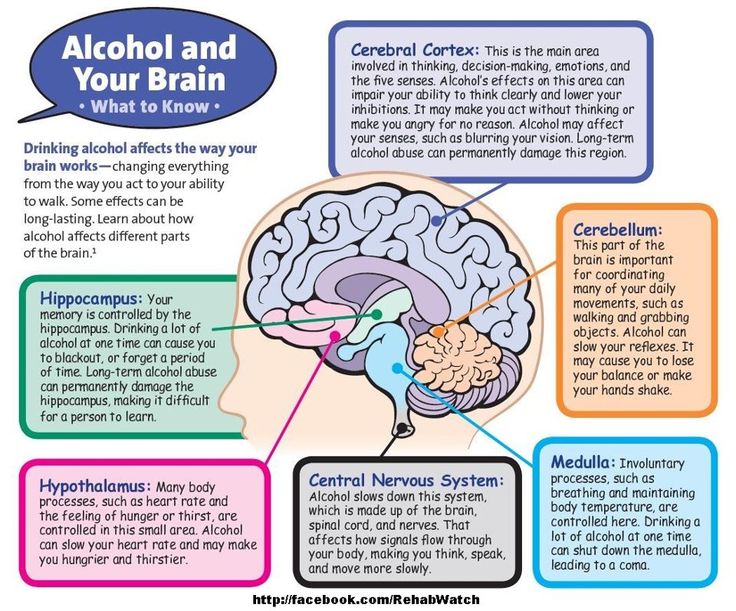
Understanding the causes of PTSD can also be helped by studying different areas brain responsible for fear and stress. One of these areas is cerebellar amygdala, responsible for emotions, learning and memory. It turned out that she plays an active role in the emergence of fear (or other words, "teaches" to be afraid of something, for example, to touch a hot stove), as well as in the early phases of fear repayment (or in other words, "teaches" Do not be scared). 4
The retention of faded memories and the weakening of the initial fear reaction are associated with the prefrontal cortex (PFC / PFC) of the brain, 4 responsible for decision making, problem solving and situation assessment. Each zone PFC has its own role. For example, when the PFC believes that a stressor is amenable to control, the medial prefrontal zone of the PFC suppresses the anxiety center deeply in the brainstem and controls the response to stress. 5 Ventromedial PFC helps maintain long-term fading of fearful memories, and her ability to perform this feature can be affected by its size. 6
Individual differences in genes or characteristics of regions of the brain brain can only set the stage for PTSD, but by themselves do not cause no symptoms. environmental factors such as childhood trauma, head trauma or mental illness in family, favor the development of the disease and increase the risk of disease, affecting the brain in the early stages of its growth. 7 Except In addition, how people adapt to trauma is likely to be influenced by and characteristics of character and behavior, such as optimism and a tendency to consider problems in a positive or negative way, as well as social factors such as availability and use of social support.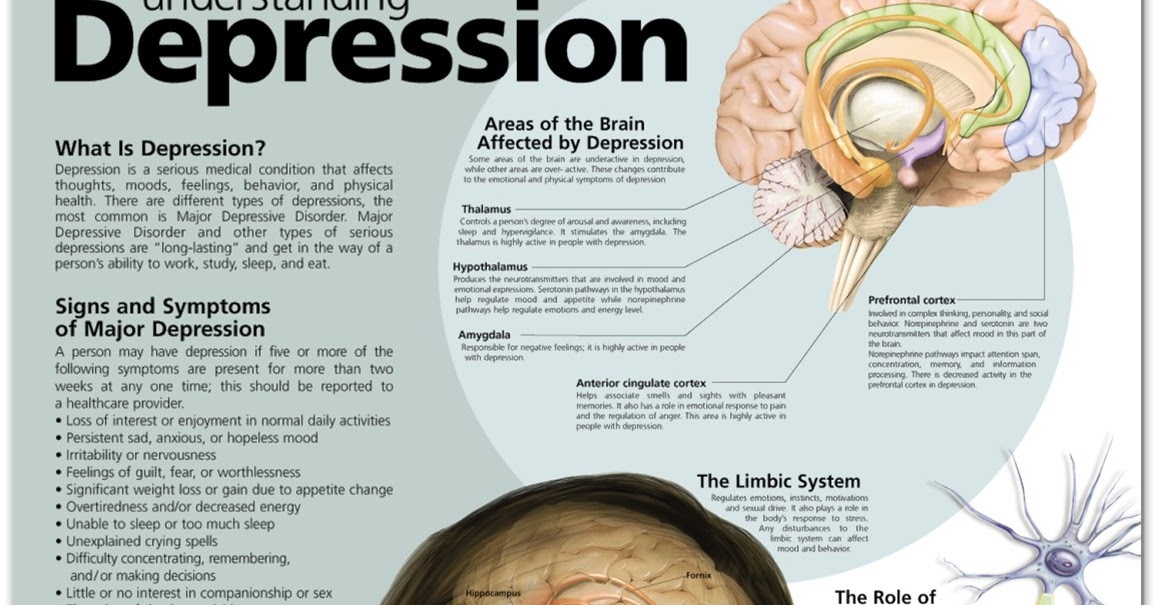 8 Further research may show what combination of these factors or what other factors will allow ever predict who has a traumatic event cause PTSD, and who doesn't.
8 Further research may show what combination of these factors or what other factors will allow ever predict who has a traumatic event cause PTSD, and who doesn't.
PTSD research
Currently, psychotherapy is used in the treatment of PTSD ("talk" therapy), drugs or drug-therapeutic combination.
Psychotherapy
Cognitive behavioral therapy (CBT) helps you learn differently think and react to frightening events that are the impetus for development PTSD, and can help bring the symptoms of the disease under control. There are several types cognitive behavioral therapy, including:
"Push" method - uses mental images, notes or visiting a place experienced trauma to help those affected face the overwhelming their fear and take control of it.
Behavior restructuring (cognitive restructuring) - encourages survivors of a traumatic event express depressing (often erroneous) thoughts about experienced trauma, challenge these thoughts and replace them with more balanced and appropriate.
Implementation in a stressful situation - teaches ways to reduce anxiety and the ability to cope with it, helping to reduce the symptoms of PTSD, and helps to correct the erroneous train of thought associated with the trauma experienced. NIMH is currently conducting research to study the reaction brain response to cognitive behavioral therapy versus response sertraline (Zoloft) - one of two drugs recommended and approved US Food and Drug Administration funds (FDA) for the treatment of post-traumatic stress. This research may help find out why some people respond better to medications, and others for psychotherapy
Drugs
Recently, in a small study, NIMH scientists found that if patients who are already taking a dose of prazosin (Minipress) at bedtime, add a daily dose, then this weakens the general symptoms of PTSD and stress reaction to reminders of the trauma experienced. 9
Another drug of interest is D-cycloserine (Seromycin), which increases the activity of a brain substance called N-methyl-D-aspartate, needed to pay off fear. During the study, which was attended by 28 people suffering from a fear of heights, scientists found that patients who received "push" therapy before a session D-cycloserine, showed lower levels of fear during the session compared to those who did not receive the drug. 10 Currently scientists study the effectiveness of the combined use of D-cycloserine and therapy for the treatment of post-traumatic stress.
During the study, which was attended by 28 people suffering from a fear of heights, scientists found that patients who received "push" therapy before a session D-cycloserine, showed lower levels of fear during the session compared to those who did not receive the drug. 10 Currently scientists study the effectiveness of the combined use of D-cycloserine and therapy for the treatment of post-traumatic stress.
Propranolol (Inderal), a beta-blocker drug, also under study whether it can be used to reduce post-traumatic stress and break the chain of scary memories. First experiments gave consoling results: it was possible to successfully weaken and, it seems, prevent PTSD in a small number of victims of traumatic events. 11
For example, in one preliminary study, scientists created a website self-help, based on the use of a psychotherapeutic method implementation in a stressful situation. First, patients with PTSD meet in person with doctor. After this meeting, participants can go to the site to find more information about PTSD and how to deal with the problem; their doctors may also visit the site to give advice or briefing. In general, scientists believe that therapy in this form - promising treatment for a large number of people suffering from PTSD. 12
First, patients with PTSD meet in person with doctor. After this meeting, participants can go to the site to find more information about PTSD and how to deal with the problem; their doctors may also visit the site to give advice or briefing. In general, scientists believe that therapy in this form - promising treatment for a large number of people suffering from PTSD. 12
Scientists are also working to improve methods for testing early treatment and monitoring of survivors of massive trauma, on developing ways to teach them self-assessment skills and introspection and referral mechanism to psychiatrists (if necessary).
Prospects for PTSD research
In the last decade, rapid progress in the study of mental and biological PTSD has led scientists to conclude that there is a need to focus on prevention, as the most realistic and important goal.
For example, in order to find ways to prevent PTSD, with funding NIMH conducts research to develop new and orphan drugs, aimed at combating the underlying causes of the disease. During another research scientists are looking for ways to enhance behavioral, personality and social protective factors and minimizing risk factors for prevent the development of PTSD after trauma. Another study is studying the question of what factors influence the difference in response to one or another method of treatment, which will help in the development of more individual, effective and productive methods of treatment.
During another research scientists are looking for ways to enhance behavioral, personality and social protective factors and minimizing risk factors for prevent the development of PTSD after trauma. Another study is studying the question of what factors influence the difference in response to one or another method of treatment, which will help in the development of more individual, effective and productive methods of treatment.
Where can I find more information?
MedlinePlus - resource from the American National Library of Medicine (U.S. National Library of Medicine and the National Institutes of Health) - offers the latest information on many health issues. Information about You can find PTSD at: www.nlm.nih.gov/medlineplus/posttraumaticstressdisorder.html.
National Institute of Mental Health
Office of Science Policy, Planning, and Communications
[National Institute of Mental Health
Science Policy Division research, planning and communications]
6001 Executive Boulevard
Room 8184, MSC 9663
Bethesda, MD 20892-9663
Phone: 301-443-4513; Fax: 301-443-4279
fax answering system Free answering machine: 1-866-615-NIMH (6464)
Text phone: 1-866-415-8051 toll-free
Email: nimhinfo@nih. gov
gov
National Center for Post-traumatic Stress Disorder
[National PTSD Center]
VA Medical Center (116D)
215 North Main Street
White River Junction, VT 05009
802-296-6300
www.ncptsd.va.gov
NOTES
- Shumyatsky GP, Malleret G, Shin RM, et al. Stathmin, a Gene Enriched in the Amygdala, Controls Both Learned and Innate Fear. cell. Nov 18 2005;123(4):697-709.
- Shumyatsky GP, Tsvetkov E, Malleret G, et al. Identification of a signal network in lateral nucleus of amygdala important for inhibiting memory specifically related to learned fear. cell. Dec 13 2002;111(6):905-918.
- Hariri AR, Mattay VS, Tessitore A, et al. Serotonin transporter genetic variation and the response of the human amygdala.Science. Jul 192002;297(5580):400-403.
- Milad MR, Quirk GJ. Neurons in medial prefrontal cortex signal memory for fear extinction.
 Nature. Nov 7 2002;420(6911):70-74.
Nature. Nov 7 2002;420(6911):70-74. - 5 Amat J, Baratta MV, Paul E, Bland ST, Watkins LR, Maier SF. Medial prefrontal cortex determines how stressor controllability affects behavior and dorsal raphe nucleus. Nat Neurosci. Mar 2005;8(3):365-371.
- Milad MR, Quinn BT, Pitman RK, Orr SP, Fischl B, Rauch SL. Thickness of ventromedial prefrontal cortex in humans is correlated with extinction memory. Proc Natl Acad Sci USA. Jul 26 2005;102(30):10706-10711.
- Gurvits TV, Gilbertson MW, Lasko NB, et al. Neurological soft signs in chronic posttraumatic stress disorder.Arch Gen Psychiatry. Feb 2000;57(2):181-186.
- Brewin CR. Risk factor effect sizes in PTSD: what this means for intervention. J Trauma Dissociation. 2005;6(2):123-130.
- Taylor FB, Lowe K, Thompson C, et al. Daytime Prazosin Reduces Psychological Distress toTrauma Specific Cues in Civilian Trauma Posttraumatic stress disorder.
 Biol Psychiatry. Feb 3 2006.
Biol Psychiatry. Feb 3 2006. - Ressler KJ, Rothbaum BO, Tannenbaum L, et al. Cognitive enhancers as adjuncts to psychotherapy: use of D-cycloserine in phobic individuals to facilitate extinction of fear. Arch Gen Psychiatry. Nov 2004;61(11):1136-1144.
- Pitman RK, Sanders KM, Zusman RM, et al. Pilot study of secondary prevention of posttraumatic stress disorder with propranolol.Biol Psychiatry. Jan 15 2002;51(2):189-192.
- Litz BTWL, Wang J, Bryant R, Engel CC.A therapist-assisted Internet self-help program for traumatic stress. Prof Psychol Res Pr. December 2004;35(6):628-634.
New York State Department of Mental Health expresses thanks to the National Institute of Mental Health for the information, used in this booklet.
Published by the State Department of Mental Health New York, June 2008.
New York State
Andrew M. Cuomo Governor
Mental Health
Head of Department Michael F. Hogan, PhD
Hogan, PhD
For more information about this edition contact:
New York State Office of Mental Health
Community Outreach and Public Education Office
[New York State Department of Mental Health
Public Relations and Community Education Department]
44 Holland Avenue
Albany, NY 12229
866-270-9857 (toll free)
www.omh.ny.gov
For questions and complaints about mental health services Health in New York contact:
New York State Office of Mental Health
Customer Relations
[New York State Department of Mental Health
Customer Service ]
44 Holland Avenue
Albany, NY 12229
800-597-8481 (toll-free)
For information about mental health services in your neighborhood, contact
nearest New York State Department of Mental Health (NYSOMH) regional office:
Western New York Field Office
[Western New York Regional Office]
737 Delaware Avenue, Suite 200
Buffalo, NY 14209
(716) 885-4219
Central New York Field Office
[Central New York Regional Office]
545 Cedar Street, 2nd Floor
Syracuse, NY 13210-2319
(315) 426-3930
Hudson River Field Office
[Hudson River Regional Office]
4 Jefferson Plaza, 3rd Floor
Poughkeepsie, NY 12601
(845) 454-8229
Long Island Field Office
[Long Island Regional Office]
998 Crooked Hill Road, Building #45-3
West Brentwood, NY 11717-1087
(631) 761-2508
New York City Field Office
[NYC Regional Office]
330 Fifth Avenue, 9th Floor
New York, NY 10001-3101
(212) 330-1671
How to recognize PTSD in everyday life
49,669
Knowing Yourself A Human Among HumansAntistress
Most of us are familiar with the term post-traumatic stress disorder. But not everyone understands that we get traumatic experiences in everyday life. Sometimes it happens completely unnoticed. Psychological trauma can cause anxiety and other problems that differ both in strength and in the way they are expressed.
But not everyone understands that we get traumatic experiences in everyday life. Sometimes it happens completely unnoticed. Psychological trauma can cause anxiety and other problems that differ both in strength and in the way they are expressed.
How does PTSD occur?
The nature of PTSD is quite difficult to comprehend. At a fundamental level, trauma causes shock and fear. The reaction of our mind and body differs depending on the intensity and suddenness of the most traumatic event. When something discouraging or unnerving happens, it throws us off balance.
Usually it only takes time to recover, but sometimes the effects of trauma continue to affect us again and again. Our emotions become out of balance, especially when the arousal and response systems are at work.
Trauma also affects thinking and mood. We try to avoid uncomfortable situations, especially if they somehow resemble a traumatic event.
When all these symptoms are exacerbated to such an extent that a person cannot cope with them independently and normally exist in society, the syndrome becomes a disorder.
Who gets the disorder?
"Classic" cases of PTSD occur in combat veterans who have seen death and destruction, survivors of natural disasters, victims of physical and sexual abuse. But if the injury occurred in less extreme circumstances, it is more difficult to determine that a person is showing symptoms of post-traumatic stress.
It is often possible to get hurt in a relationship with someone. For example, if there was a betrayal, although the marriage seemed strong and happy. This causes shock, a person loses a sense of the reality of what is happening. At first, he may fall into a stupor.
When the shock wears off, a cascade of emotions descends upon him—horror, anger, bitterness, sadness, and even despair. They are exhausting in themselves, but the expectation of the next “trip” from the universe gives rise to constant anxiety.
Case Study
One of my patients came to therapy after learning that her husband (with whom she had been living together for 30 years) was in a long-term relationship with another woman.
They communicated through social networks and never met in person, but for the wife it was still a terrible betrayal and shock.
Despite the emotional coldness that appeared in her relationship with her husband, it seemed to her that everything was fine
The discovery turned her life upside down. She had little idea of what was real and what was not. She could not eat or sleep, did not control her emotions - swings from anger to tears happened all the time. But the most unpleasant moment was the obsessive thoughts and scenes that stood before her eyes: their romantic communication, his face on the day she found out everything. It couldn't be stopped.
Of course the woman received professional help. But her story is one example of trauma that shows up in everyday life. For most of us, the likelihood of getting PTSD under dramatic circumstances, in war or in a disaster, is relatively small. But other types of traumatic events occur at every turn.
Learn more