Haltlose type personality disorder
Personality disorder classification - wikidoc
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Ayesha Anwar, M.B.B.S[2]
Overview
There are two approaches used to classify personality disorders; categorical and dimensional. Categorical classification is based on distinct operational criteria depending on behavioral characteristics. DSM-5 and ICD-10 both uses this approach. As compared to this, dimensional classification is based on the personality traits and using a quantitative distinction. It places normality at one end and disorder at other. DSM-5 classifies 10 personality disorders into three clusters due to similar characteristics: CLUSTER A is defined as odd and eccentric and include Paranoid, Schizoid, and Schizotypal. CLUSTER B is defined by erratic and emotional behavior and includes Antisocial, Borderline, Histrionic and Narcissist. CLUSTER C PDs patients are anxious and fearful and incorporate Avoidant, Dependent and Obsessive-Compulsive.
ICD-10 classifies into 3 clusters as well, which are A, Odd/eccentric and includesParanoid and Schizoid, B, Dramatic and includes Dissocial, Emotionally unstable borderline type, Emotionally unstable impulsive type and Histrionic, and C, Anxious/fearful that include Anxious, Dependent and Anankastic.
Classification
List of Personality Disorders Defined in the DSM
- DSM-5 classifies 10 personality disorders into three clusters due to similar characteristics:
- CLUSTER A: odd and eccentric
- Paranoid-distrust and suspiciousness
- Schizoid-detachment from social relationships
- Schizotypal-distortion in interpersonal relationships and cognition, and behavioural eccentrism
- CLUSTER B: erratic and emotional
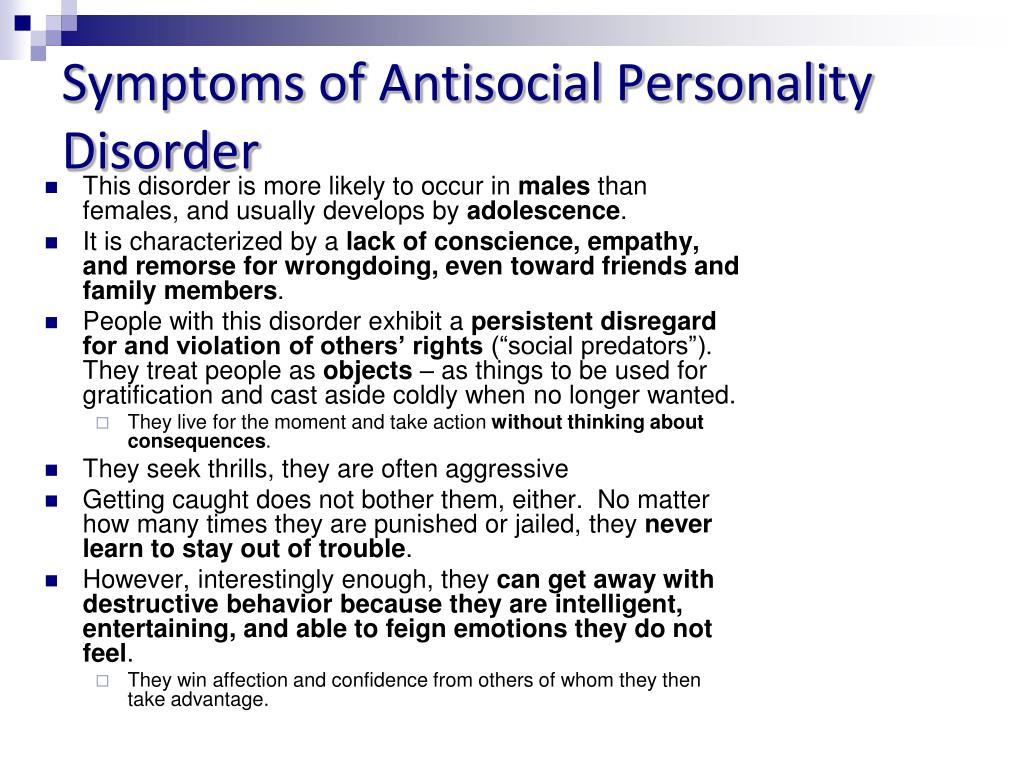
- Antisocial-disregard and violation of rights of others
- Borderline-instability in interpersonal relationships, and impulsivity
- Histrionic-eccessive emotionality and attention-seeking behaviour
- Narcissist-grandiosity and lack of empathy
- CLUSTER C: anxious and fearful
- Avoidant-social inhibition and fear of criticism
- Dependent-submissive and excessive need for reassurance
- Obsessive-Compulsive-preoccupation with perfectionism and orderliness
- CLUSTER A: odd and eccentric
- ICD-10 classifies into 3 clusters as well, which are as follows:
- A: Odd/eccentric
- Paranoid
- Schizoid
- B: Dramatic
- Dissocial
- Emotionally unstable borderline type
- Emotionally unstable impulsive type
- Histrionic
- C: Anxious/fearful
- Anxious
- Dependent
- Anankastic
- A: Odd/eccentric
The DSM-IV lists ten personality disorders, grouped into three clusters. The DSM also contains a category for behavioral patterns that do not match these ten disorders, but nevertheless exhibit characteristics of a personality disorder. This category is labeled Personality Disorder NOS (Not Otherwise Specified).
The DSM also contains a category for behavioral patterns that do not match these ten disorders, but nevertheless exhibit characteristics of a personality disorder. This category is labeled Personality Disorder NOS (Not Otherwise Specified).
Cluster A (odd or eccentric disorders)
- Paranoid personality disorder
- Schizoid personality disorder
- Schizotypal personality disorder
Cluster B (dramatic, emotional, or erratic disorders)
- Antisocial personality disorder
- Borderline personality disorder
- Histrionic personality disorder
- Narcissistic personality disorder
Cluster C (anxious or fearful disorders)
- Avoidant personality disorder
- Dependent personality disorder (not the same as Dysthymia)
- Obsessive-compulsive personality disorder (not the same as Obsessive-compulsive disorder)
Revisions and Exclusions from Past DSM Editions
The revision of the previous edition of the DSM, DSM-III-R, also contained the Passive-aggressive Personality Disorder, the Self-defeating Personality Disorder, and the Sadistic Personality Disorder.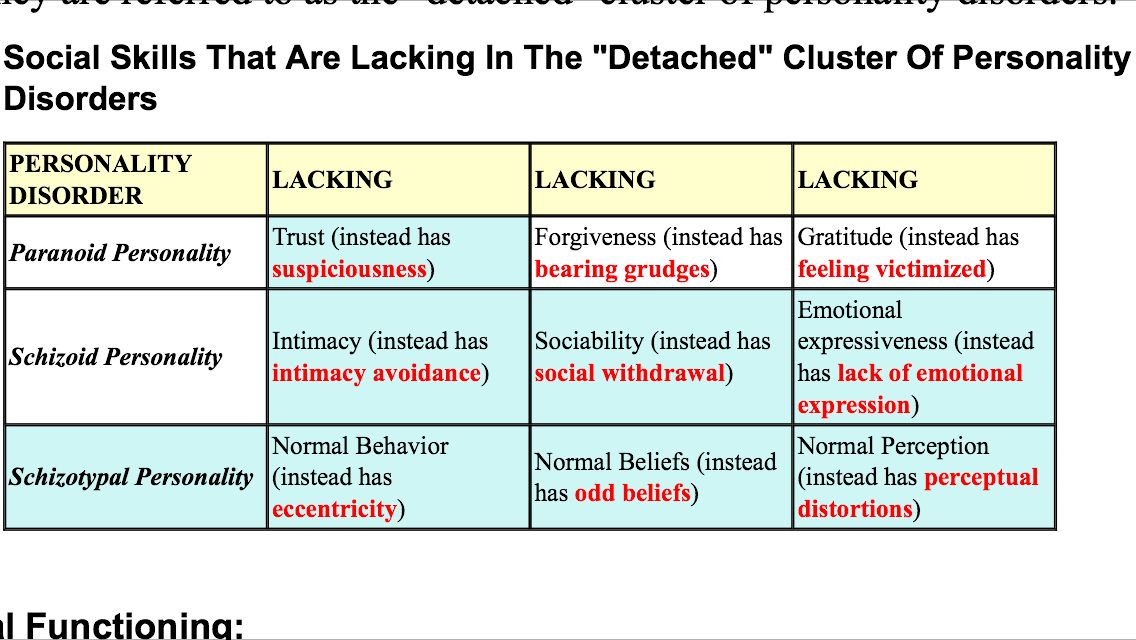 Passive-Aggressive Personality Disorder is a pattern of negative attitudes and passive resistance in interpersonal situations. Self-defeating personality disorder is characterised by behaviour that consequently undermines the person's pleasure and goals. Sadistic Personality Disorder is a pervasive pattern of cruel, demeaning, and aggressive behavior. These categories were removed in the current version of the DSM, because it is questionable whether these are separate disorders. Passive-aggressive Personality Disorder and Depressive personality disorder were placed in an appendix of DSM-IV for research purposes.
Passive-Aggressive Personality Disorder is a pattern of negative attitudes and passive resistance in interpersonal situations. Self-defeating personality disorder is characterised by behaviour that consequently undermines the person's pleasure and goals. Sadistic Personality Disorder is a pervasive pattern of cruel, demeaning, and aggressive behavior. These categories were removed in the current version of the DSM, because it is questionable whether these are separate disorders. Passive-aggressive Personality Disorder and Depressive personality disorder were placed in an appendix of DSM-IV for research purposes.
World Health Organization
The ICD-10 section on mental and behavioral disorders includes categories of personality disorder and enduring personality changes. They are defined as ingrained patterns indicated by inflexible and disabling responses that significantly differ from how the average person in the culture perceives, thinks and feels, particularly in relating to others. [1]
[1]
The specific personality disorders are: paranoid, schizoid, dissocial, emotionally unstable (borderline type and impulsive type), histrionic, anankastic, anxious (avoidant) and dependent.[2]
There is also an 'Other' category involving conditions characterized as eccentric, haltlose (derived from "haltlos" (German) = drifting, aimless and irresponsible),[3]immature, narcissistic, passive-aggressive or psychoneurotic. An additional category is for unspecified personality disorder, including character neurosis and pathological personality.
There is also a category for Mixed and other personality disorders, defined as conditions that are often troublesome but do not demonstrate the specific pattern of symptoms in the named disorders. Finally there is a category of Enduring personality changes, not attributable to brain damage and disease. This is for conditions that seem to arise in adults without a diagnosis of personality disorder, following catastrophic or prolonged stress or other psychiatric illness.
Other
Some types of personality disorder were in previous versions of the diagnostic manuals but have been deleted. This includes two types that were in the DSM-III-R appendix as "proposed diagnostic categories needing further study" without specific criteria, namely sadistic personality disorder (a pervasive pattern of cruel, demeaning and aggressive behavior) and Self-defeating personality disorder (masochistic personality disorder) (characterised by behaviour consequently undermining the person's pleasure and goals).[4] The psychologist Theodore Millon and others consider some relegated diagnoses to be equally valid disorders, and may also propose other personality disorders or subtypes, including mixtures of aspects of different categories of the officially accepted diagnoses.[5]
| Personality disorder diagnoses in each edition of American Psychiatric Association's Diagnostic Manual[6] | |||||
|---|---|---|---|---|---|
| DSM-I | DSM-II | DSM-III | DSM-III-R | DSM-IV(-TR) | DSM-V Proposals |
| Personality | |||||
| Pattern disturbance: | |||||
| Inadequate | Inadequate | ||||
| Schizoid | Schizoid | Schizoid | Schizoid | Schizoid | |
| Cyclothymic | Cyclothymic | ||||
| Paranoid | Paranoid | Paranoid | Paranoid | Paranoid | |
| Schizotypal | Schizotypal | Schizotypal | Schizotypal* | ||
| Personality | |||||
| Trait disturbance: | |||||
| Emotionally unstable | Hysterical | Histrionic | Histrionic | Histrionic | |
| Borderline | Borderline | Borderline | Borderline | ||
| Compulsive | Obsessive-compulsive | Compulsive | Obsessive-compulsive | Obsessive-compulsive | Obsessive-compulsive |
| Passive-aggressive: | |||||
| Passive-depressive subtype | Dependent | Dependent | Dependent | ||
| Passive-aggressive subtype | Passive-aggressive | Passive-aggressive | Passive-aggressive | ||
| Aggressive subtype | |||||
| Explosive | |||||
| Asthenic | |||||
| Avoidant | Avoidant | Avoidant | Avoidant | ||
| Narcissistic | Narcissistic | Narcissistic | Narcissistic** | ||
| Sociopathic personality | |||||
| Disturbance: | |||||
| Antisocial reaction | Antisocial | Antisocial | Antisocial | Antisocial | Antisocial-psychopathic |
| Dyssocial reaction | |||||
| Sexual deviation | |||||
| Addiction | |||||
| Appendix: | Appendix: | Appendix: | |||
| Self-defeating | Negativistic | Dependent | |||
| Sadistic | Depressive | Histrionic | |||
| Paranoid | |||||
| Schizoid | |||||
| Negativistic | |||||
| Depressive | |||||
* – Not actually to be classified as a personality disorder; classified instead as a form of schizophrenia-spectrum disorder.
** – Originally proposed for deletion; status remains unclear for DSM-5.
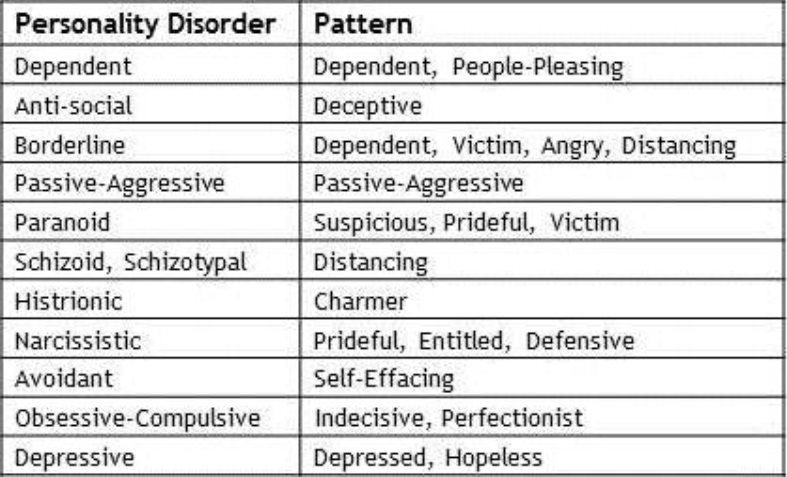
Millon's Description of Personality Disorders
Psychologist Theodore Millon, who has written numerous popular works on personality, proposed the following description of personality disorders:
| Millon's brief description of personality disorders[7] | |
|---|---|
| Type of personality disorder | Description |
| Paranoid | Guarded, defensive, distrustful and suspiciousness. Hypervigilant to the motives of others to undermine or do harm. Always seeking confirmatory evidence of hidden schemes. Feels righteous, but persecuted. |
| Schizoid | Apathetic, indifferent, remote, solitary, distant, humorless. Neither desires nor need human attachments. Withdrawal from relationships and prefer to be alone. Little interest in others, often seen as a loner. Minimal awareness of feelings of self or others. Few drives or ambitions, if any. Few drives or ambitions, if any. |
| Schizotypal | Eccentric, self-estranged, bizarre, absent. Exhibits peculiar mannerisms and behaviors. Thinks can read thoughts of others. Preoccupied with odd daydreams and beliefs. Blurs line between reality and fantasy. Magical thinking and strange beliefs. |
| Antisocial | Impulsive, irresponsible, deviant, unruly. Acts without due consideration. Meets social obligations only when self-serving. Disrespects societal customs, rules, and standards. Sees self as free and independent. |
| Borderline | Unpredictable, manipulative, unstable. Frantically fears abandonment and isolation. Experiences rapidly fluctuating moods. Shifts rapidly between loving and hating. Sees self and others alternatively as all-good and all-bad. Unstable and frequently changing moods. |
| Histrionic | Dramatic, seductive, shallow, stimulus-seeking, vain. Overreacts to minor events. Exhibitionistic as a means of securing attention and favors. Sees self as attractive and charming. Constant seeking for others' attention. Exhibitionistic as a means of securing attention and favors. Sees self as attractive and charming. Constant seeking for others' attention. |
| Narcissistic | Egotistical, arrogant, grandiose, insouciant. Preoccupied with fantasies of success, beauty, or achievement. Sees self as admirable and superior, and therefore entitled to special treatment. |
| Avoidant | Hesitant, self-conscious, embarrassed, anxious. Tense in social situations due to fear of rejection. Plagued by constant performance anxiety. Sees self as inept, inferior, or unappealing. Feels alone and empty. |
| Dependent | Helpless, incompetent, submissive, immature. Withdraws from adult responsibilities. Sees self as weak or fragile. Seeks constant reassurance from stronger figures. |
| Obsessive–compulsive | Restrained, conscientious, respectful, rigid. Maintains a rule-bound lifestyle. Adheres closely to social conventions. Sees the world in terms of regulations and hierarchies. Sees self as devoted, reliable, efficient, and productive. Sees the world in terms of regulations and hierarchies. Sees self as devoted, reliable, efficient, and productive. |
| Depressive | Somber, discouraged, pessimistic, brooding, fatalistic. Presents self as vulnerable and abandoned. Feels valueless, guilty, and impotent. Judges self as worthy only of criticism and contempt. |
| Passive–aggressive (Negativistic) | Resentful, contrary, skeptical, discontented. Resist fulfilling others’ expectations. Deliberately inefficient. Vents anger indirectly by undermining others’ goals. Alternately moody and irritable, then sullen and withdrawn. |
| Sadistic | Explosively hostile, abrasive, cruel, dogmatic. Liable to sudden outbursts of rage. Feels selfsatisfied through dominating, intimidating and humiliating others. Is opinionated and closeminded. |
| Self-defeating (Masochistic) | Deferential, pleasure-phobic, servile, blameful, self-effacing. Encourages others to take advantage. Deliberately defeats own achievements. Seeks condemning or mistreatful partners. Encourages others to take advantage. Deliberately defeats own achievements. Seeks condemning or mistreatful partners. |
Additional Classification Factors
Except for classifying by category and cluster, it is possible to classify personality disorders using such additional factors as severity, impact on social functioning, and attribution.[8]
References
- ↑ WHO (2010) ICD-10: Specific Personality Disorders
- ↑ "International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) Version for 2010 (Online Version)". Apps.who.int. Retrieved on 2013-04-16.
- ↑ Langmaack, C. (2000). "'Haltlose' type personality disorder (ICD-10 F60.8)". The Psychiatrist. 24 (6): 235–236. doi:10.1192/pb.24.6.235-b.
- ↑ Fuller, AK, Blashfield, RK, Miller, M, Hester, T (1992). "Sadistic and self-defeating personality disorder criteria in a rural clinic sample".
 Journal of Clinical Psychology. 48 (6): 827–31. doi:10.1002/1097-4679(199211)48:6<827::AID-JCLP2270480618>3.0.CO;2–1 Check
Journal of Clinical Psychology. 48 (6): 827–31. doi:10.1002/1097-4679(199211)48:6<827::AID-JCLP2270480618>3.0.CO;2–1 Check |doi=value (help). PMID 1452772.CS1 maint: Multiple names: authors list (link) - ↑ Millon, Theodore (2004) Personality Disorders in Modern Life, John Wiley & Sons, ISBN 0471668508.
- ↑ Widiger, Thomas (2012). The Oxford Handbook of Personality Disorders. Oxford University Press. ISBN 978-0199735013.
- ↑ Millon, Theodore (2004). Personality Disorders in Modern Life, p. 4. John Wiley & Sons, Inc., Hoboken, New Jersey. ISBN 0-471-23734-5.
- ↑ Murray, Robin M. et al (2008). Psychiatry. Fourth Edition. Cambridge University Press. ISBN 978-0-521-60408-6.
Template:WS Template:WH
What Was a Constitutional Psychopath?
Source: Gwendolyn Murray, used with permission
A student recently shared that in 1911, her relative was institutionally discharged with a diagnosis of Constitutional Psychopath.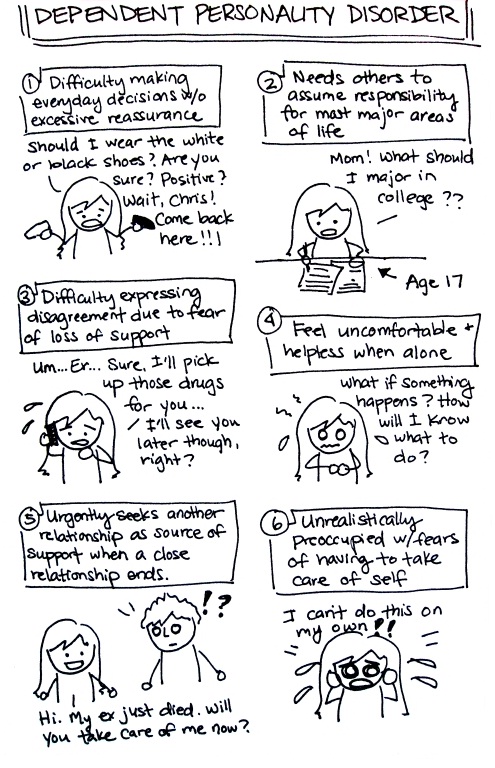 She wondered if it meant her ancestor was a socially corrupt, morally depraved individual, like what we call psychopaths today.
She wondered if it meant her ancestor was a socially corrupt, morally depraved individual, like what we call psychopaths today.
Not likely.
The usual definitions
To the uninitiated, "psychopath" is likely not reserved for someone with a debased relationship to society, as those in the psychology field know it.
Many readers have likely encountered "psychopath" or "psycho" being used as a catch-all for people acting in some psychologically-puzzling manner. This could range from the vexing behaviors of someone with severe OCD to Cluster B personality disorders. It's as if the prefix "psycho" is simply pop-culture shorthand indicating the observance of something psychologically askew.
In my classes and trainings, students often wonder how psychopath differs from sociopathy, the latter tending to be associated with antisocial personality disorder (APD). A raised hand often leads to, "Aren't they all the same?" Ostensibly, yes, but let's look at the nuance as it's accepted in the field.
APD, sociopath, and psychopath are a matter of synonym and degree. Antisocial personality disorder is just a modern term for sociopath (e.g., Millon, 2011; Shannon, 2019) in that it was thought to be more descriptive of the interactive style. In short, "antisocial" has nothing to do with social inhibitions like in social anxiety disorder; it means they do things in a fashion grossly against societal norms, usually in a marked morally bereft fashion, in order to meet their needs.
Psychopaths, on the other hand, don't just disregard and violate the rules of society and the rights of others. What they do is egregious and beyond disregard, it is entirely without conscience. "Without conscience" so aptly describes the condition that Robert Hare, Ph.D. (1999), used this as the title of his comprehensive book on the subject.
Johnson (2019) nicely discusses the psychopathic nuances by painting a picture of psychopaths as more predatory, emotionally desensitized, calculating, and conniving; there is a marked effrontery to the "normal" antisocial activity.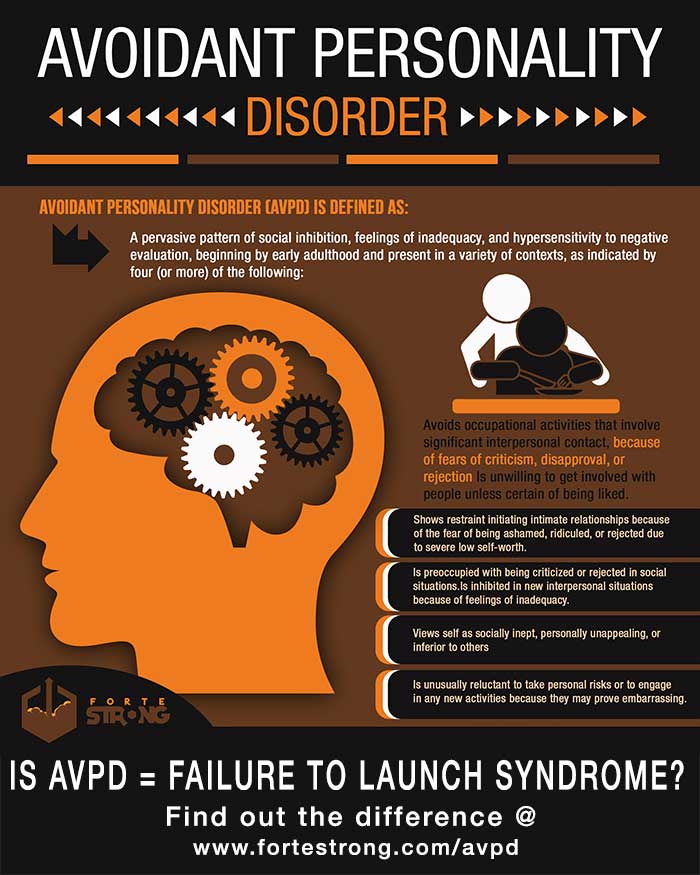 He explained that those on the psychopathic end of the spectrum are thought to be born with abnormal brain development, influencing the severity of their personality problems.
He explained that those on the psychopathic end of the spectrum are thought to be born with abnormal brain development, influencing the severity of their personality problems.
It may help to illustrate that your garden variety thug or murderer would more likely be in the APD realm; Saddam Hussein, Jeffrey Dahmer, Eileen Wournos, and BTK would easily meet APD criteria, but in a much more malicious manner, earning them the category of psychopath.
Before psychopathy as we know it
APD/psychopaths as we now understand them have existed since time immemorial. From the biblical Cain to Vlad the Impaler, the latter impaling people and then putting them on display outside his castle to watch them suffer (Markarian, 2020), society has dealt with severely morally-defunct characters.
In their respective eras, such people were probably most frequently referred to as some derivative of "evil," though an ancient Greek, Theophrastus, categorized them as "the unscrupulous" in recognition of the pathological lack of empathy (Kiehl & Hoffman, 2011). Closer to our times, Pinel, in 1801, wrote that some patients had "insanity without delirium" (Millon, et al., 1998). By this, he meant they were impulsive and self-damaging with intact reasoning abilities; in short, this illustrates the calculated, negative behaviors without regard for consequence that psychopaths exhibit. Millon furthered that this conceptualization went on to be termed "moral insanity" given the value-laden bent of psychiatry at the time.
Closer to our times, Pinel, in 1801, wrote that some patients had "insanity without delirium" (Millon, et al., 1998). By this, he meant they were impulsive and self-damaging with intact reasoning abilities; in short, this illustrates the calculated, negative behaviors without regard for consequence that psychopaths exhibit. Millon furthered that this conceptualization went on to be termed "moral insanity" given the value-laden bent of psychiatry at the time.
"Psychopath" wasn't always synonymous with social scourge
According to Kiehl & Hoffman (2011), the word psychopath didn't enter the scene until 1888 when the German psychiatrist J.L.A. Koch used the term psychopastiche, literally meaning "suffering of the soul." Surely, this was the root of "psychopathology" as in the examination of psychological sufferings/diagnoses, like the course some readers took in graduate school.
Soon, as pointed out by Millon (2011), a shorter version, "psychopath," became popular. It was a generalized term of the era for any "persistent styles of abnormal functioning ... of an ostensive organic nature." Essentially, it was a catch-all term for psychological pathology/behaviors so omnipresent they were assumed to have genetic/congenital roots. "Psychopath" had yet to be considered synonymous with unconscionable activity.
It was a generalized term of the era for any "persistent styles of abnormal functioning ... of an ostensive organic nature." Essentially, it was a catch-all term for psychological pathology/behaviors so omnipresent they were assumed to have genetic/congenital roots. "Psychopath" had yet to be considered synonymous with unconscionable activity.
This was, however, the dawn of the study of psychopathology as we know it. Koch soon began to recognize nuances amongst the psychopastiche, and it could be argued that this led to opening the gates of personality disorder study.
Taking a step closer to our modern understanding of the term, in 1891 Koch, beginning to expand from the general "psychopath," suggested that "moral insanity" be replaced with "psychopathic inferiority." Koch preferred "inferior" as it indicated the personalities deviated unfavorably from the norm (Millon, 2011).
Source: Stux/Pixabay
Have we come full circle in understanding the causes of psychopathy?
Given the proximity of Koch's use of the terms "constitutional" and "inferiority," one could also hypothesize that though he didn't write it, "inferior" to Koch indicated some arrested component of brain development that encouraged those afflicted to never expand from the pure id state they were born with. Thus, they weren't able to assimilate to acceptable social mores and behaviors and, though he couldn't prove it at the time, Koch was perhaps precocious in his belief that there were significant neurodevelopmental components contributing to this morally depraved state, much as Johnson discussed evidence for in 2019.
Thus, they weren't able to assimilate to acceptable social mores and behaviors and, though he couldn't prove it at the time, Koch was perhaps precocious in his belief that there were significant neurodevelopmental components contributing to this morally depraved state, much as Johnson discussed evidence for in 2019.
Researchers (e.g., DeBrito et al., 2021; Tully et al., 2021) continue to inform us of the increasing evidence of significant neurodevelopmental underpinnings of psychopathy. DeBrito (2021) documented that structural and functional brain abnormalities in, for example, the prefrontal cortex and amygdala contribute heavily to "disruption in emotional responsiveness, reinforcement-based decision-making and attention," which are characteristic of psychopathy.
Modern conceptualization of "psychopathy" and importance of subtypes
Though our modern idea of APD/psychopathy was included in the term psychopathic inferior, Millon (2011) was quick to note that, upon closer look, this was only a small portion of what Koch had in mind. He included numerous subtypes, some marked less by significant moral depravity than by high sensitivity, eccentricities, and impulsive fury.
He included numerous subtypes, some marked less by significant moral depravity than by high sensitivity, eccentricities, and impulsive fury.
It's interesting to consider that these composite states Koch noticed were primitive recognitions of what we now call mixed personality disorders, as written about in "Can a Person Have More than One Personality Disorder?" It is not unheard of, for example, that the eccentric paranoid or schizotypal personalities have an antisocial streak, as illustrated, for example, in Yudofsky (2005).
Eventually, the "inferiority" term did not sit well due to its belittling intonation (Millon, 2011), and, in America, "constitutional psychopathic state" and "psychopathic personality" became the preferred term for what we would now pointedly refer to as a psychopath. Provided the fascination with understanding this "insane/non-insane" disposition (Hulbert, 1939), differentiating and dissecting psychopathic (as we know it) presentations persisted.
In the 21st century, Millon (2011) listed seven distinct subtypes, including not only the more traditional malevolent sort but an adventurous type he called the "disaffected aggrandizing subtype. " This would align with what early on was called a Haltlose personality, a morally-devious modus operandi superimposed on a hypomanic personality. In short, a personality in regular need of new stimulation, impulsivity, and drifting in their antisocial pursuits to please themselves.
" This would align with what early on was called a Haltlose personality, a morally-devious modus operandi superimposed on a hypomanic personality. In short, a personality in regular need of new stimulation, impulsivity, and drifting in their antisocial pursuits to please themselves.
Source: Geralt/Pixabay
More recently, much like Koch, researchers continue to express interest in the utility of psychopathy subtypes. For example, Hicks and Drislane (2018) noted, "subtypes can help to inform the understanding of psychopathy and antisocial deviance more generally." This obviously can help with matters such as profiling, public safety, and further research on developing interventions, and, perhaps, eventually, even prevention, of psychopathic behavior.
All things considered
Ironically, it seems that the more it was attempted to neatly compartmentalize personality pathology into super-distinct disorders, the more evidence mounted for understanding them as more multifaceted and nebulous, leading to alternative conceptualization proposals (e. g., APA, 2013; Hopwood et al., 2018).
g., APA, 2013; Hopwood et al., 2018).
At the heart of these alternative proposals is understanding personality pathology in a more dimensional or trait-domain manner. Rather than taking note of defining symptoms of, say, Histrionic personality disorder, and leaving it at that, a dimensional or trait lens could encourage observation for clinically-relevant things that might be missed if a clinician is trying to neatly categorize the patient's diagnosis. A prime example is someone with marked histrionic characteristics who, upon closer examination, has strong dependency needs, as written about in "Why Some Adults May Still Have an Infantile Personality." Clearly, there can be treatment implications to nuance.
Disclaimer: The material provided in this post is for informational purposes only and not intended to diagnose, treat, or prevent any illness in readers. The information should not replace personalized care from an individual's provider or formal supervision if you’re a practitioner or student.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
De Brito S.A., Forth A.E., Baskin-Sommers A.R., Brazil I.A., Kimonis E.R., Pardini D., Frick P.J., Blair R.J.R., & Viding E. (2021). Psychopathy. Nature Reviews Disease Primers, 7 (1), 49. doi: 10.1038/s41572-021-00282-1.
Hare, R. (1999). Without conscience: The disturbing world of the psychopaths among us. Guilford.
Hicks, B. M., & Drislane, L. E. (2018). Variants (“subtypes”) of psychopathy. In C. J. Patrick (Ed.), Handbook of psychopathy (pp. 297–332). The Guilford Press. Abstract retrieved from APA PsycNet.
Hopwood, C. J., Kotov, R., Krueger, R. F., Watson, D., Widiger, T. A., Althoff, R. R., Ansell, E. B., Bach, B., Michael Bagby, R., Blais, M. A., Bornovalova, M. A., Chmielewski, M., Cicero, D. C., Conway, C., De Clercq, B., De Fruyt, F., Docherty, A. R., Eaton, N. R., Edens, J. F.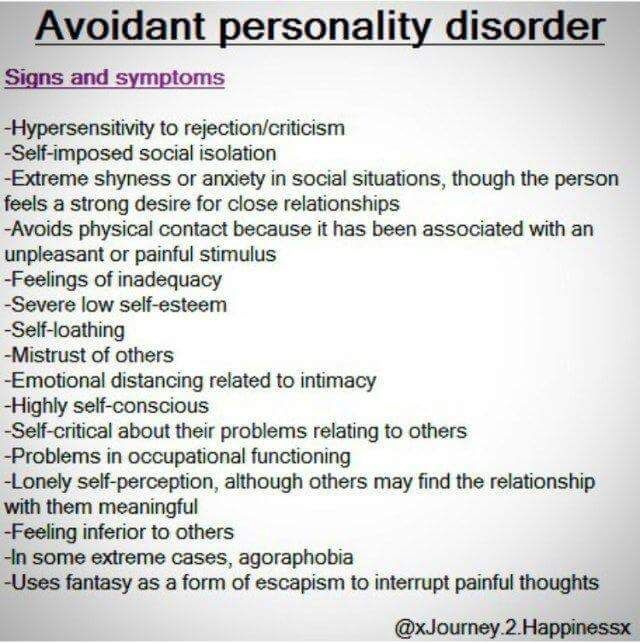 , Forbes, M. K., … Zimmermann, J. (2018). The time has come for dimensional personality disorder diagnosis. Personality and mental health, 12(1), 82–86. https://doi.org/10.1002/pmh.1408
, Forbes, M. K., … Zimmermann, J. (2018). The time has come for dimensional personality disorder diagnosis. Personality and mental health, 12(1), 82–86. https://doi.org/10.1002/pmh.1408
Hulbert, H. (1938). Constitutional psychopathic inferiority in relation to delinquency. Journal of Law and Criminology, 2 (1), 3-21.
Johnson, S. (2019). Understanding the violent personality: Antisocial personality disorder, psychopathy, & sociopathy explored. Forensic Research & Criminology International Journal, 7(2), 76-88.
Kiehl, K. A., & Hoffman, M. B. (2011). The criminal psychopath: History, neuroscience, treatment and economics. Jurimetrics, 51, 355–397.
Markarian, T. (2020, March 28). 15 of the most famous psychopaths in history. Reader's Digest. https://www.rd.com/list/most-famous-psychopaths-in-history/.
Millon T., Simonsen, E., & Burket-Smith, M. (1998). History and viewpoints. In Millon T., Simonsen, E.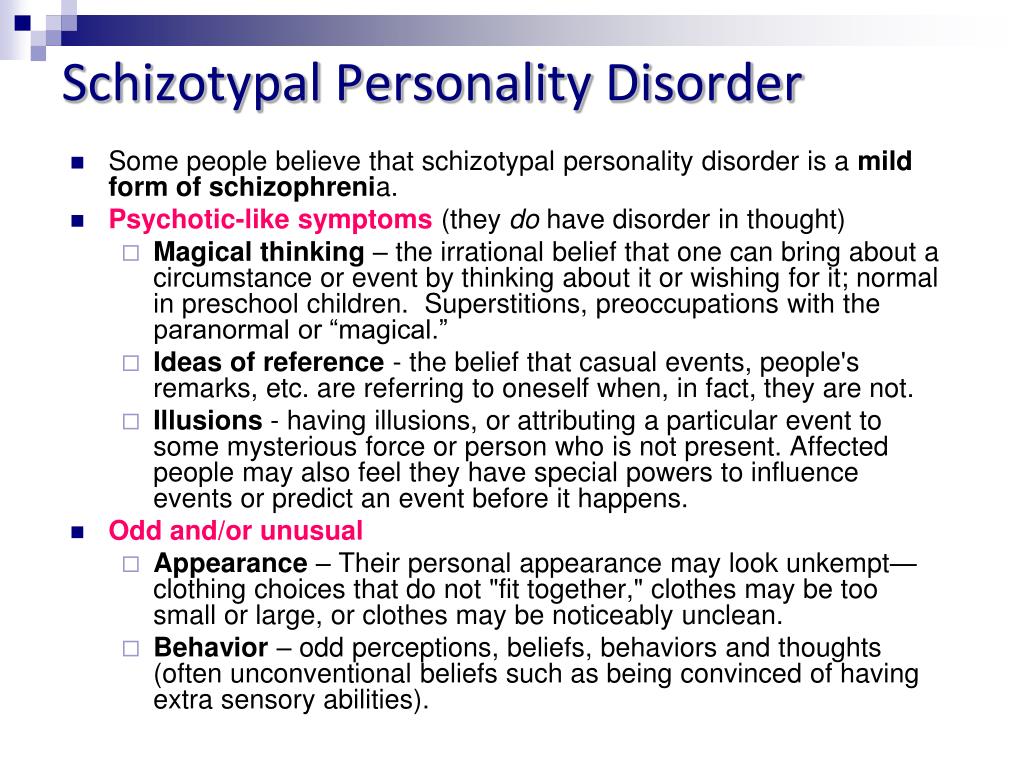 , Burket-Smith, M, & Davis, R. (Eds.). Pychopathy: Antisocial, criminal and violent behavior. Guilford.
, Burket-Smith, M, & Davis, R. (Eds.). Pychopathy: Antisocial, criminal and violent behavior. Guilford.
Shannon, Joseph W. (2019, October 25). Character flaws: How to understand and navigate relationships with high conflict clients. Brattleboro Retreat, Brattleboro, Vermont.
Tully, J., Frey, A., Fotiadou, M., Kolla, N., & Eisenbarth, H. (2021). Psychopathy in women: Insights from neuroscience and ways forward for research. CNS Spectrums, 1-13. doi:10.1017/S1092852921001085
Yudofsky, S. (2005). Fatal flaws: Navigating destructive relationships with people with disorders of personality and character. American Psychiatric Publishing.
Personality disorder - causes, types, types, symptoms, signs, diagnosis (test), treatment
Features
Causes
Symptoms
Diagnosis
Treatment
Personality disorder, the causes of which are not always obvious, used to be called constitutional psychopathy.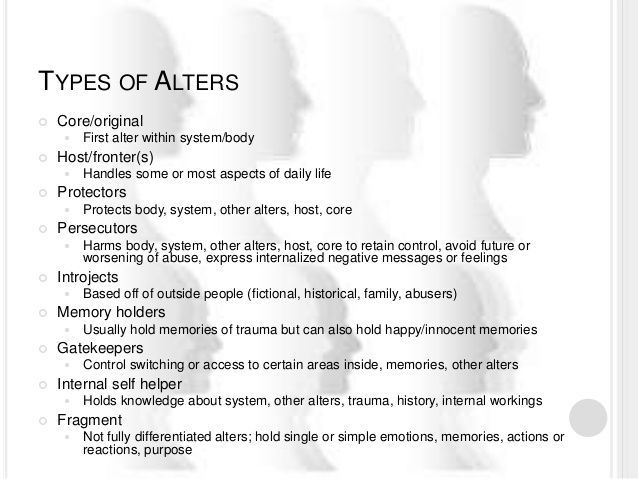 This is a mental disorder that accompanies a person throughout life. The main changes affect the character, thinking and behavior, which causes difficulties in social adaptation. The psychopath breaks the norms and rules accepted in the social environment. The severity of the changes is different - from everyday inconsistency to criminal acts with subsequent restriction of freedom.
This is a mental disorder that accompanies a person throughout life. The main changes affect the character, thinking and behavior, which causes difficulties in social adaptation. The psychopath breaks the norms and rules accepted in the social environment. The severity of the changes is different - from everyday inconsistency to criminal acts with subsequent restriction of freedom.
Features of personality disorder
World statistics of diseases states that about 10% of the world's population suffers from psychopathy. Each type of personality disorder accounts for an average of about 2% of cases. A distinctive feature is that the first manifestations are noticeable already in early childhood, practically unchanged throughout life.
Psychopathy is not quite a disease in the usual sense of the word. The disease has a beginning, progression and consequences in the form of organic (irreversible) disorders of the function and structure of organs. Psychopathy is a special, painful personality structure that does not undergo any changes in the changing conditions of life. This prevents the psychopath from adapting to the environment. Relatively speaking, a person with a personality disorder will behave in the same way with a first grader and a scientist, in a tram and a living room, not realizing that different people and situations require different behavior.
Psychopathy is a special, painful personality structure that does not undergo any changes in the changing conditions of life. This prevents the psychopath from adapting to the environment. Relatively speaking, a person with a personality disorder will behave in the same way with a first grader and a scientist, in a tram and a living room, not realizing that different people and situations require different behavior.
The problem of psychopathic personalities, anomalies of character was thoroughly studied by the Soviet and Russian psychiatrist Pyotr Borisovich Gannushkin, whose definitions of personality disorders have not lost their relevance to this day.
Causes of personality disorders
Experts consider several main reasons:
- genetic factor - practice shows that pathological character traits are found in representatives of different generations of the same family;
- an established vicious system of interpersonal relationships - the child does not have before his eyes an example of a normal, sympathetic and empathetic family;
- a psychopathic pattern (template, model) of behavior that the child unconsciously copies due to the lack of other examples;
- pathological pregnancy, difficult childbirth and diseases of early childhood;
- childhood abuse, physical or psychological;
- difficult childhood, unfavorable developmental conditions.
Researchers believe that genetic factors are of paramount, determining importance. This theory is confirmed by the twin method: identical brothers and sisters, separated in early childhood and raised in different families, behave exactly the same in adulthood. Twins who have never interacted with each other show the same types of personality disorder.
Personality disorder symptoms
Gannushkin identified 7 types of psychopathy. Since the 90s, when the 10th revision of the International Classification of Diseases, Injuries and Causes of Death came out, the condition has been called a personality disorder, but the essence has not changed. Each type of psychopathy has its own distinctive features.
Schizotypal personality disorder is distinguished by the minimization of social contacts, lack of need for communication, coldness, lack of empathy (the ability to empathize). Schizoids are attracted to fantasies, various distant theories, they are unable to perceive life directly, sensually.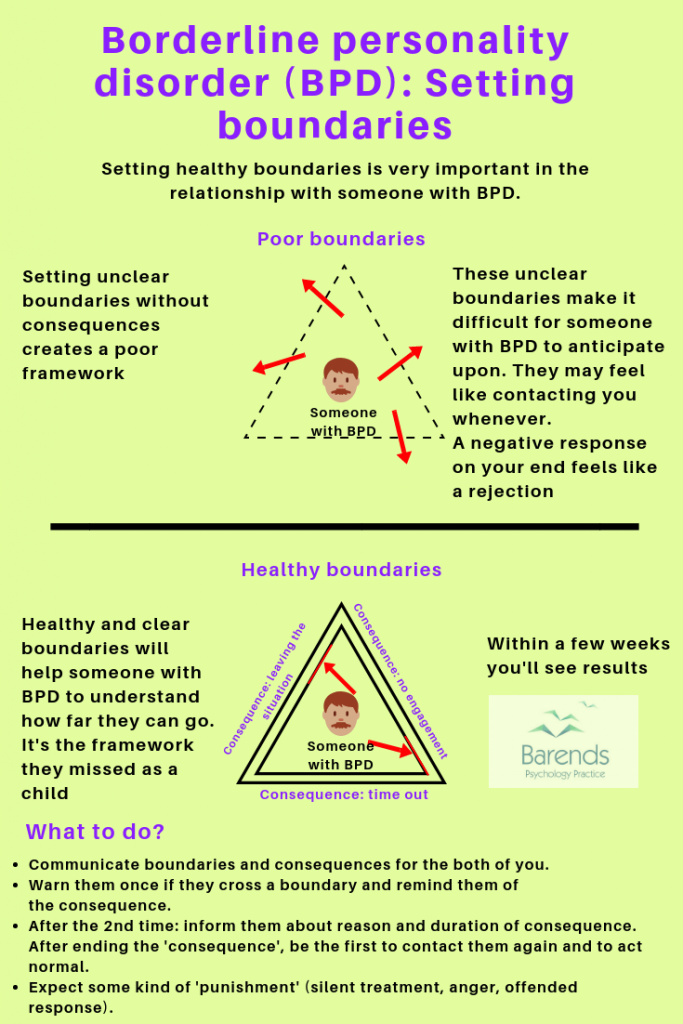 Teamwork is not for them, they can be more or less successful in individual activities. Their main feature is indifference, both to themselves and to others. Such people sincerely do not understand what pleasure and joy are, because they have never experienced them.
Teamwork is not for them, they can be more or less successful in individual activities. Their main feature is indifference, both to themselves and to others. Such people sincerely do not understand what pleasure and joy are, because they have never experienced them.
Bipolar personality disorder according to Gannushkin includes 3 types: depressive, agitated and cyclothymic. Depressives are lifelong pessimists who are able to see only sad, gloomy sides in all the diversity of life. Excited - easy-going, carried away, often unable to foresee the consequences of their actions. The vast majority of gamblers and swindlers are of this type. Cyclothymics combine both of the above features, they are characterized by undulating mood swings, lack of stable attachments, blurring and diversity of interests.
Dissociative identity disorder in Western culture is called a split identity. It is believed that several personalities coexist in one person, which are periodically activated. We have been using this diagnosis since 2000, but it does not take root well. Domestic psychiatrists consider this disorder a kind of psychological defense of a person who has experienced extreme, unbearably painful emotions. At the same time, a person perceives the events of his life as something that happened to others.
We have been using this diagnosis since 2000, but it does not take root well. Domestic psychiatrists consider this disorder a kind of psychological defense of a person who has experienced extreme, unbearably painful emotions. At the same time, a person perceives the events of his life as something that happened to others.
Narcissistic personality disorder refers to the Greek myth of Narcissus, a young man who preferred the love of a real girl to looking at his reflection in the water of a stream. Like the hero of a myth, a narcissist is convinced of his exclusivity and originality, and this applies to everything from appearance to achievements. The narcissist believes that real achievements are hindered by the envy of others who put up all sorts of obstacles. Own uniqueness requires constant confirmation, so the narcissist maintains relationships only with those who admire him.
Organic personality disorder - a consequence of damage to the brain tissue by various hazards: trauma, intoxication, infection. Such a disorder occurs in the clinic in patients who have had a stroke, encephalitis, in alcoholics and drug addicts. In the latter, the condition is aggravated by the consequences of closed craniocerebral injuries, which they receive when falling from a height of their own height in a state of intoxication.
Such a disorder occurs in the clinic in patients who have had a stroke, encephalitis, in alcoholics and drug addicts. In the latter, the condition is aggravated by the consequences of closed craniocerebral injuries, which they receive when falling from a height of their own height in a state of intoxication.
In a mild form of the disorder, the patient is disturbed by frequent headaches, weakness, fatigue, tearfulness, intolerance to stuffiness, meteorological dependence. Over time, thinking is disturbed, thoroughness, viscosity, concentration on minor details joins. Such a patient cannot separate the main from the secondary, speech becomes impoverished, emotions coarsen, periods of an evil-dreary mood (dysphoria) occur. An intellectual decline occurs, the patient cannot cope with the previous work, criminal episodes with fights and bodily injuries to the “offender” are not uncommon.
Borderline personality disorder is manifested by unstable mood, fluctuating from overestimation of oneself to humiliation. Patients are impulsive, commit rash acts, anxious, suicidal. Any little thing causes a feeling of emptiness, fears of being unnecessary, "thrown out of life." This disorder is the basis for the formation of drug addiction and eating disorders.
Patients are impulsive, commit rash acts, anxious, suicidal. Any little thing causes a feeling of emptiness, fears of being unnecessary, "thrown out of life." This disorder is the basis for the formation of drug addiction and eating disorders.
Personality disorder diagnostics
It is desirable to carry out such a diagnosis as early as possible, because the disorder accompanies a person all his life. Problem children should be under the supervision of a child psychiatrist in order to overcome teenage difficulties with minimal losses. Even a single consultation with a specialist will allow parents to correct the behavior of the baby, as they will understand the motives of his actions.
A variety of tests for personality disorder are used in adolescents and adults. Popular tests based on the work of Eysenck, Beck, Freeman. The test is a questionnaire with several standardized answers, a lie scale is provided so that the subject cannot be misled.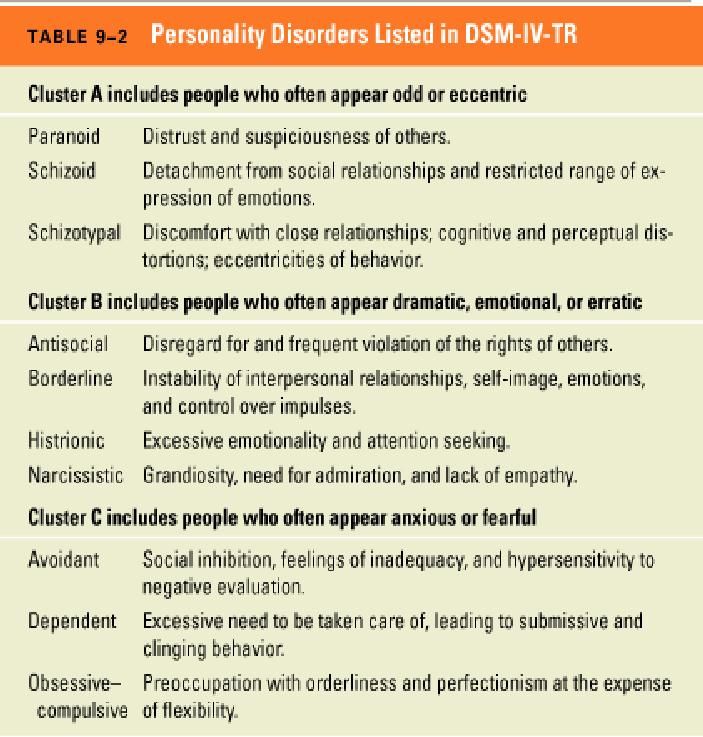 The tests are fairly objective and are widely used in the clinic.
The tests are fairly objective and are widely used in the clinic.
Personality disorder treatment
The basis of treatment is the choice of a life path, profession and occupation suitable for the type of personality. This is where a clinical psychologist can help. An occupation corresponding to a personality type can make a person so successful that no one will notice the disorder.
In severe cases, when the time for professional orientation is missed, medications (antidepressants, tranquilizers, nootropics), psychotherapeutic methods, including psychoanalysis, are used. Treatment options for advanced personality disorders are limited, especially in patients with addiction or irreversible brain damage.
The best solution for suspected psychopathy is timely consultation with an experienced psychiatrist.
Article author:
Novikov Vladimir Sergeevich
psychotherapist, clinical psychologist, kmn, member of the Professional Psychotherapeutic League
reviews leave a review
Clinic m.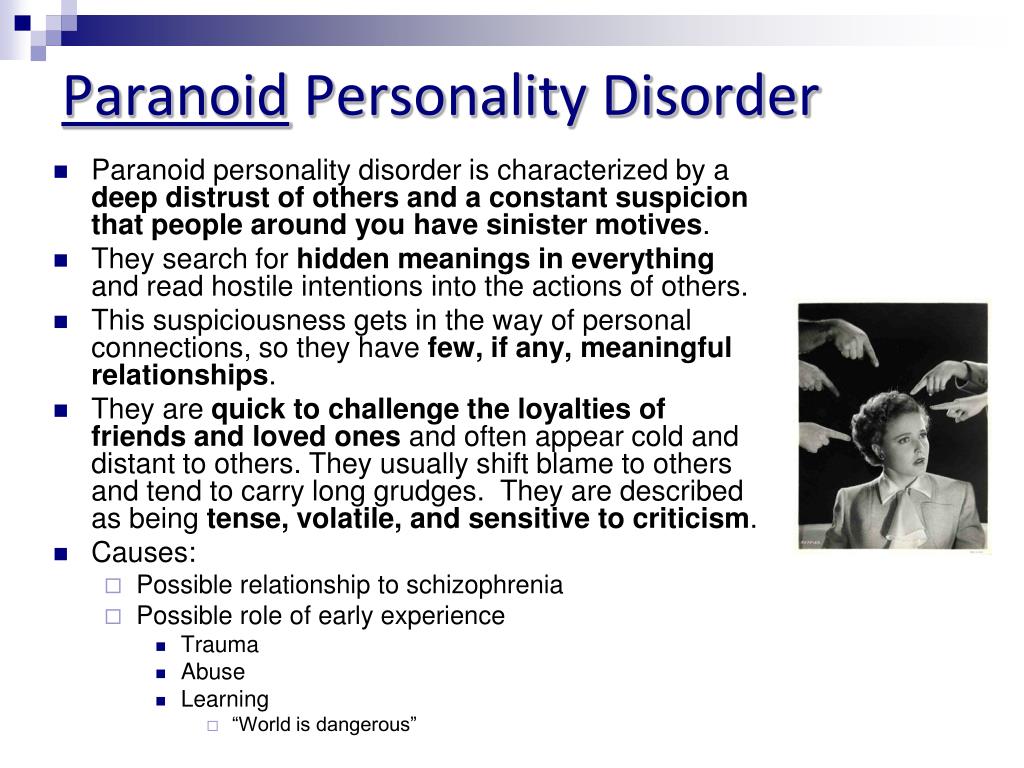 Frunzenskaya
Frunzenskaya
Reviews
Services
- Title
- Initial appointment, consultation with a psychotherapist (up to 1 hour) 4400 905 years. Red Gates. AvtozavodskayaPharmacy. Glades. Sukharevskaya. st. Academician Yangelam. Frunzenskaya Zelenograd
- National Institute of Mental Health. borderline personality disorder. NIH publication number QF 17-4928. Available from: https://www.nimh.nih.gov/health/publications/borderline-personality-disorder/index.shtml [accessed 30 September 2019].
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
 5th ed. Arlington, VA: American Psychiatric Association; 2013.
5th ed. Arlington, VA: American Psychiatric Association; 2013. - Grant BF, Chou SP, Goldstein RB, Huang B, Stinson FS, Saha TD, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: results from the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry. 2008;69(4):533–545.
- National Institute for Health and Clinical Excellence. Borderline personality disorder: recognition and management. 2009. Available from: https://www.nice.org.uk/guidance/cg78/resources/borderline-personality-disorder-recognition-and-management-pdf-975635141317 [accessed 30 September 2019].
- Bailey RC, Grenyer BFS. Burden and support needs of carers of persons with borderline personality disorder: a systematic review. Harv Rev Psychiatry. 2013;21(5):248–258.
- Zanarini MC, Frankenburg FR, Reich DB, Fitzmaurice G. Time to attainment of recovery from borderline personality disorder and stability of recovery: a 10-year prospective follow-up study.
 Am J Psychiatry. 2010;167(6):663–667.
Am J Psychiatry. 2010;167(6):663–667.
Sorokin Maxim Vladimirovich
psychotherapist
reviews Make an appointment
Clinic
metro Frunzenskaya
Borderline personality disorder
Borderline personality disorder is associated with unstable mood and behavior that has a significant impact on a person's daily life
Borderline personality disorder is a type of personality disorder in which a person experiences periods of tension, unstable moods and behaviors, and an altered "feeling of self".1 All of these can result in impulsive actions and relationship problems with friends and family members, impairing the person's ability to cope with everyday life.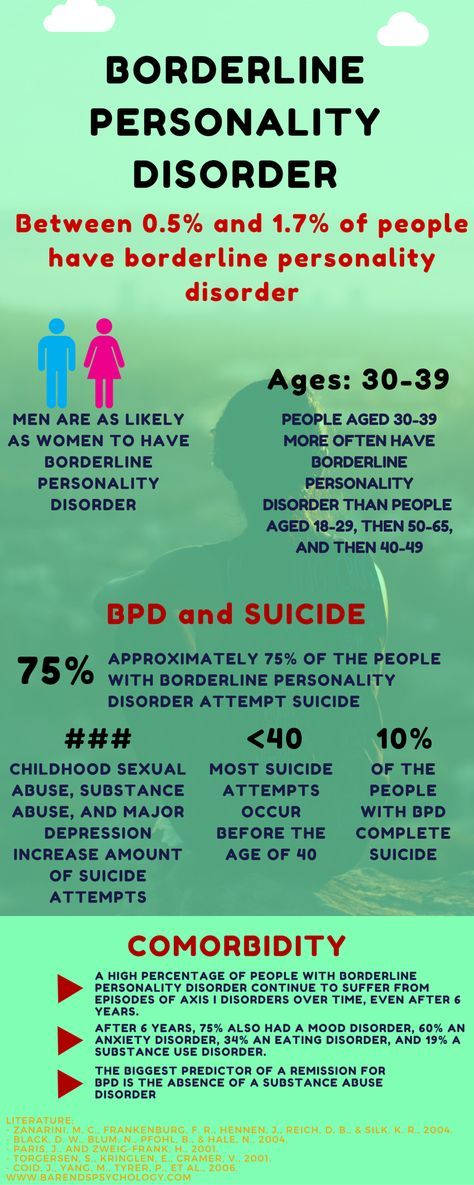 1.2
1.2
Borderline personality disorder is a serious illness associated with self-harm and suicidal attempts. One in ten patients complete suicide. 2
Facts About Borderline Personality Disorder
Borderline personality disorder is a type of personality disorder in which a person experiences periods of tension, unstable mood and behavior, and an altered sense of self. 1
One in ten patients complete suicide. 2
Patients with borderline personality disorder are very sensitive to changes in their environment, and may respond inappropriately and acutely to such changes. They may, for example, be afraid of being abandoned by a loved one.2 If the person whom patient
is expecting arrives late, the patient easily changes the feeling of attachment to dislike or anger.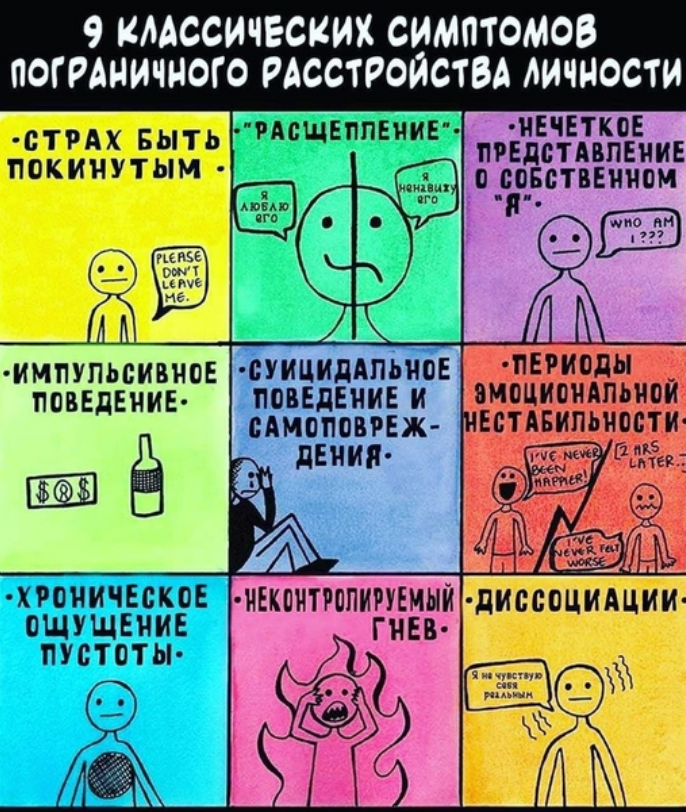 1,2 This reflects the extreme perception of the world by the patient, who sees everything and everyone - including oneself – either good or bad.1,2
1,2 This reflects the extreme perception of the world by the patient, who sees everything and everyone - including oneself – either good or bad.1,2
People with borderline personality disorder are often insecure, may suddenly change their life goals and views on career, life values and friends.2 Such patients have impulsive and dangerous behavior: reckless spending, unsafe driving, addiction to chemicals. 2 They may develop intense unwarranted anger or feelings of emptiness, and are prone to self-harm.2 Patients with borderline personality disorder may also experience depression and anxiety.1,2
Facts about Borderline Personality Disorder
Estimates of the proportion of people who have borderline personality disorder vary from less than 1% to around 6%. 2-4
Borderline personality disorder affects a roughly equal number of men and women, but appears to be more disabling in women the same frequency in men and women, but in women it is more severe.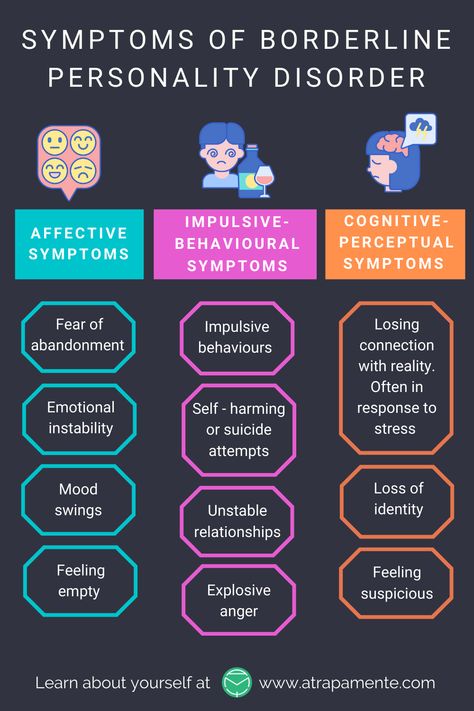 3
3
Symptoms of borderline personality disorder most often first appear during adolescence.4 The disease is most severe and problematic in young adults and tends to improve with age.2 Symptoms may persist throughout life, but most patients with borderline personality disorder by the age of 30-40 have a stable job and a home.2
People with borderline personality disorder are emotionally and functionally unstable, which places a significant burden on their families.5 Mood swings are a source of stress for both the patient and his/her others, which can lead to the development of mental disorders in the latter.1,5
People who are concerned that they – or their loved ones – are experiencing symptoms of borderline personality disorder should see their doctor for help and advice.
Borderline personality disorder is diagnosed by a mental health professional using interviews and discussions about symptoms and medical history. 1
1
Psychotherapy can help people with borderline personality disorder by, for example, teaching them how to interact with others and to express their thoughts and feelings more clearly. 1 It may also be beneficial for caregivers and family members of those affected to receive therapy and guidance on how best to care for a person with borderline personality disorder. 1 There is currently no cure, but one study showed that, after 10 years, 50% of people with borderline personality disorder had recovered, being able to function at work and maintain personal relationships. 6
1. National Institute of Mental Health. borderline personality disorder. NIH publication number QF 17-4928. Available from: https://www.nimh.nih.gov/health/publications/borderline-personality-disorder/index.shtml [accessed 30 September 2019].
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013.
3. Grant BF, Chou SP, Goldstein RB, Huang B, Stinson FS, Saha TD, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: results from the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry. 2008;69(4):533–545.
4. National Institute for Health and Clinical Excellence. Borderline personality disorder: recognition and management. 2009. Available from: https://www.nice.org.uk/guidance/cg78/resources/borderline-personality-disorder-recognition-and-management-pdf-975635141317 [accessed 30 September 2019].