Extreme anxiety test
Anxiety test | Quick, free and clinically-validated
0203 326 9160
0203 761 7026
0203 761 7027
0203 761 7029
0203 326 91600203 761 70260203 761 70270203 761 7029
Fees & Payment Options
FAQs
Share this page
Question 1
I find it very hard to unwind, relax or sit still
- Never
- Rarely
- Sometimes
- Often
- Very often
Question 2
I have had stomach problems, such as feeling sick or stomach cramps
- Never
- Rarely
- Sometimes
- Often
- Very often
Question 3
I have been irritable and easily become annoyed
- Never
- Rarely
- Sometimes
- Often
- Very often
Question 4
I have experienced shortness of breath
- Never
- Rarely
- Sometimes
- Often
- Very often
Question 5
I have felt dizzy and unsteady at times
- Never
- Rarely
- Sometimes
- Often
- Very often
Question 6
I have had difficulties with sleep (including waking early, finding it hard to go to sleep)
- Never
- Rarely
- Sometimes
- Often
- Very often
Question 7
I have felt panicked and overwhelmed by things in my life
- Never
- Rarely
- Sometimes
- Often
- Very often
Question 8
I have felt nervous and on edge
- Never
- Rarely
- Sometimes
- Often
- Very often
Question 9
I have had trembling hands
- Never
- Rarely
- Sometimes
- Often
- Very often
Question 10
I seem to be constantly worrying about things
- Never
- Rarely
- Sometimes
- Often
- Very often
1
Question 1 of 10
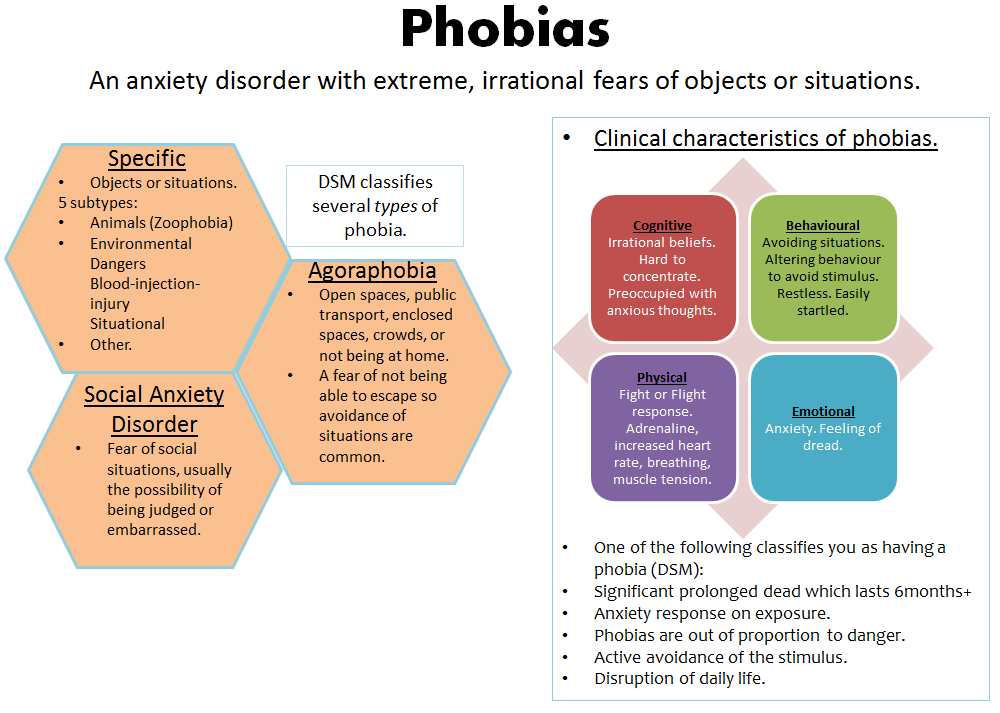
When answering the above questions please consider how they have applied to you in the last month or so.
This test will give an indication as to whether you are experiencing the most common symptoms of an anxiety disorder, but it cannot replace a full assessment nor should be used to self diagnose or decide upon a treatment plan.
This test was adapted from: Generalised Anxiety Disorder GAD-7
Need to talk?
0203 326 9160 0203 326 9160
A free, confidential call could quickly help you get the support you need. Your call will be answered by an assistant psychologist who will listen to your concerns before explaining your options and suggesting the most appropriate treatment.
Take another test
View all tests
We have online mental health quizzes for many conditions including ADHD, autism, anxiety, depression, PTSD, and more. Each one should take no longer than five minutes.
No Internet Connection
Anxiety test | Depression and Anxiety
1.
 How often have you been bothered by feeling nervous, anxious or on edge over the last two weeks?
How often have you been bothered by feeling nervous, anxious or on edge over the last two weeks? - NOT AT ALL
- SEVERAL DAYS
- MORE THAN HALF THE DAYS
- NEARLY EVERY DAY
2. How often have you been bothered by not being able to stop or control worrying over the last two weeks?
- NOT AT ALL
- SEVERAL DAYS
- MORE THAN HALF THE DAYS
- NEARLY EVERY DAY
3.
 How often have you been bothered by worrying too much about different things over the last two weeks?
How often have you been bothered by worrying too much about different things over the last two weeks? - NOT AT ALL
- SEVERAL DAYS
- MORE THAN HALF THE DAYS
- NEARLY EVERY DAY
4. How often have you been bothered by having trouble relaxing over the last two weeks?
- NOT AT ALL
- SEVERAL DAYS
- MORE THAN HALF THE DAYS
- NEARLY EVERY DAY
5.
 How often have you been bothered by being so restless that it is hard to sit still over the last two weeks?
How often have you been bothered by being so restless that it is hard to sit still over the last two weeks? - NOT AT ALL
- SEVERAL DAYS
- MORE THAN HALF THE DAYS
- NEARLY EVERY DAY
6. How often have you been bothered by becoming easily annoyed or irritable over the last two weeks?
- NOT AT ALL
- SEVERAL DAYS
- MORE THAN HALF THE DAYS
- NEARLY EVERY DAY
7.
 How often have you been bothered by feeling afraid as if something awful might happen over the last two weeks?
How often have you been bothered by feeling afraid as if something awful might happen over the last two weeks? - NOT AT ALL
- SEVERAL DAYS
- MORE THAN HALF THE DAYS
- NEARLY EVERY DAY
If you want to change any of your answers, use the progress bar below.
Professional claustrophobia test online
Skip to content
Search for:
Instructions: Assess your level of anxiety in various situations to determine your exposure to fear of enclosed spaces. The test consists of 2 parts (scales) Suffocation Fear Scale (SS) and Freedom of Action Fear Scale (RS) .
The test consists of 2 parts (scales) Suffocation Fear Scale (SS) and Freedom of Action Fear Scale (RS) .
Contents
- Suffocation Fear Scale (SS):
- Freedom of Action Fear Scale (RS):
- Interpretation of results
- Who is this test suitable for
- How long will the test take
- How to respond to a high anxiety score
- Is it possible to cure claustrophobia on your own? 1. Swim with nose clip (or mask)
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
2. Work in the kitchen under the sink for 15 minutes
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
3. Be in the elevator on the 1st floor with the door closed
No alarm
Minor alarm
Medium alarm
High alarm
Extreme alarm
4.
 Inability to breathe through nose due to nasal congestion with a cold
Inability to breathe through nose due to nasal congestion with a cold No anxiety
Slight anxiety
Medium anxiety
High anxiety
Extreme anxiety
5. Try to hold your breath during vigorous exercise
No anxiety
Slight anxiety
Moderate anxiety
High alarm
Extreme alarm
6. Snorkeling in a safe bathyscaphe for 15 minutes
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
7. Oxygen mask use
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
8. Lying on the bottom floor of a bunk bed
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
9. Be in the middle of the 3rd row of a full concert hall, which cannot be left until the end of the concert
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
10.
 to be in the center of a crowded theater row
to be in the center of a crowded theater row No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
11. Work under the vehicle for 15 minutes
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
12. Be in the farthest place from the exit during the tour of cave
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
13. Lie in the sauna for 15 minutes
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
14. Being on the ground with the doors closed for 15 minutes
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
Next
Scale of fear of restriction of freedom of action (RS):
To start the test, click "Next".

1. Stay in a closed room WITHOUT LIGHT for 15 minutes
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
2. Being locked in a small, WELL-LIGHTED, windowless room for 15 minutes
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
3. Be handcuffed for 15 minutes
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
4. Stay with your hands tied behind your back for 15 minutes
No alarm
Slight alarm
Medium alarm
High alarm
Extreme alarm
5. Wear tight clothing that is difficult to remove
No anxiety
Low anxiety
Medium anxiety
High anxiety
Extreme anxiety
6.
 Wear a straitjacket for 15 minutes
Wear a straitjacket for 15 minutes No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
7. Lie in a sleeping bag with arms and legs tightly wrapped around the neck for 15 minutes
No alarm
Low anxiety
Medium anxiety
High anxiety
Extreme anxiety
8. Climb head first into a zippered sleeping bag, with the ability to get out at any time
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
9. Stay in the trunk of a car with free air circulation for 15 minutes
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
10. Being foot-tied to a chair attached to the floor
No alarm
Minor alarm
Medium alarm
High alarm
Extreme alarm
11.
 Being in a public toilet with barred windows
Being in a public toilet with barred windows No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
12. Sitting in an overcrowded train that has stopped between stations
No alarm
Low alarm
Medium alarm
High alarm
Extreme alarm
Next
Claustrophobia is a common fear of closed spaces and the inability to breathe. It can develop in childhood or manifest itself in adulthood as a result of a strong emotional shock. In the most difficult cases, it causes panic and loss of control over oneself. Test yourself with the CLQ online claustrophobia test. The test can be taken for free and without registration.
The CLQ has only recently appeared. Before him, it was impossible to identify the symptoms of claustrophobia on your own. This screening technique has gained wide popularity due to its simplicity and accessibility.
 nine0003
nine0003 The test consists of 2 scales that characterize the main types of fears in claustrophobia: SS (Suffocation Subscale) - fear of suffocation, and RS (Restriction Subscale) - fear of restriction of actions.
Interpretation of results
Questions focus on hypothetical situations and the person's feelings in them to assess the degree of discomfort the respondent feels.
The sum of both scales will show the overall level of development of the disease:
- less than 10 points - no symptoms; nine0018
- 11-28 points - the level of disorder is below average;
- 29-48 points - the level of fear with a tendency to increase;
- More than 49 points - a high degree of development of the disorder.
A score over 18 is considered to indicate a significant risk of deterioration. If your final score exceeds the indicated limit, we recommend that you immediately consult a doctor.
Deciphering the component scales will clarify the nature and specifics of the manifestation of fear.
 For the scale of fear of suffocation, a result of more than 10 is dangerous, for a scale of fear of immobilization - more than 21 points. nine0003
For the scale of fear of suffocation, a result of more than 10 is dangerous, for a scale of fear of immobilization - more than 21 points. nine0003 Based on the analysis of this information, the therapist will select the most appropriate treatment protocol for your needs.
Who is this test for?
The CLQ is designed for an adult audience. It is universal for men and women.
How long will the test take?
The method contains 26 questions, for which 5 response options are expected from “no anxiety” to “severe anxiety”.
The total points will be calculated automatically, so allow only 10-15 minutes to go through the items of the questionnaire and familiarize yourself with its conclusion. nine0003
How to respond to a high level of anxiety
It is important to remember that the test cannot replace a full examination by a specialist. Its result reflects only the primary diagnosis, which requires clarification. We recommend that you do not ignore the alarming symptoms and seek medical advice.

Is it possible to cure claustrophobia on your own
A phobia of any kind is a kind of mental clamp. It is possible to remove it through thoughtful psychological therapy. In advanced cases, medications are used to sedate and reduce nervous tension. nine0003
Tests, questionnaires and work materials - Mental Health Center
1. Which of the following substances have you ever tried in your life? (not prescribed by a doctor)
Nicotine (tobacco, electronic cigarettes)(0) No(1) Yes
Alcoholic products (beer, wine, alcohol)(0) No(1) Yes
Cannabis (marijuana, hashish)(0) No(1 ) Yes
Cocaine (coca, crack)(0) No(1) Yes
Amphetamine-type stimulants (diet pills, speed, ecstasy, etc.)(0) No(1) Yes
Inhalants (glue, gasoline, thinner)(0) No(1) Yes
Sedatives and hypnotics (Corvalol, Xanax, Relanium phenazepam, etc.)(0) No(1) Yes
Hallucinogens (LSD, acid , mushrooms, ketamine, etc.)(0) No(1) Yes
Opioids (heroin, morphine, methadone, codeine, etc.
 )(0) No(1) Yes
)(0) No(1) Yes Other psychoactive substances(0) No(1 ) Yes
2. In the past three months, how often have you used the following types of substances?
Nicotine (tobacco, electronic cigarettes)(0) Never(2) 1-2 times(3) Monthly(4) Weekly(6) Nearly every day
Alcoholic products (beer, wine, alcohol)(0) Never(2) 1-2 times(3) Every month(4) Every week(6) Almost every day
Cannabis (marijuana, hashish)(0) Never(2) 1-2 times(3) Monthly(4) Weekly(6) Almost every day
Cocaine (coca, crack)(0) Never(2) 1-2 times(3) Monthly (4) Every week(6) Almost every day
Amphetamine-type stimulants (speed, diet pills, ecstasy, etc.)(0) Never(2) 1-2 times(3) Every month(4) Every week (6) Almost every day
Inhalants (glue, gasoline, thinner)(0) Never(2) 1-2 times(3) Monthly(4) Weekly(6) Almost every day
Sedatives and hypnotics (Corvalol, Xanax, Relanium phenazepam, etc.)(0) Never(2) 1-2 times(3) Every month(4) Every week(6) Almost every day
Hallucinogens (LSD, acid, mushrooms, ketamine, etc.
 )(0 ) Never(2) 1-2 times(3) Monthly(4) Weekly(6) Almost every day
)(0 ) Never(2) 1-2 times(3) Monthly(4) Weekly(6) Almost every day Opioids (heroin, morphine, methadone, codeine, etc.)(0) Never(2) 1 -2 times(3) Every month(4) Every week(6) Almost every day
Other psychoactive substances(0) Never(2) 1-2 times(3) Monthly(4) Weekly(6) Almost every day
3. In the past three months, how often have you had a strong desire or craving for the following substances?
Nicotine (tobacco, electronic cigarettes)(0) Never(3) 1-2 times(4) Monthly(5) Weekly(6) Almost every day
Alcoholic products (beer, wine, alcohol)(0 ) Never(3) 1-2 times(4) Every month(5) Every week(6) Almost every day
Cannabis (marijuana, hashish)(0) Never(3) 1-2 times(4) Every month(5) Every week(6) Almost every day
Cocaine (coca, crack)(0) Never( 3) 1-2 times(4) Monthly(5) Weekly(6) Nearly every day
Amphetamine-type stimulants (speed, diet pills, ecstasy, etc.)(0) Never(3) 1-2 times(4) Monthly(5) Weekly(6) Almost every day
Inhalants (glue, gasoline, thinner)(0) Never(3) 1-2 times(4) Monthly(5) Weekly( 6) Almost every day
Sedatives and hypnotics (Corvalol, Xanax, Relanium phenazepam, etc.
 )(0) Never(3) 1-2 times(4) Monthly(5) Weekly(6) Almost every day
)(0) Never(3) 1-2 times(4) Monthly(5) Weekly(6) Almost every day Hallucinogens (LSD , acid, mushrooms, ketamine, etc.)(0) Never(3) 1-2 times(4) Monthly(5) Weekly(6) Almost every day
Opioids (heroin, morphine, methadone, codeine and etc.)(0) Never(3) 1-2 times(4) Every month(5) Every week(6) Almost every day
Other psychoactive substances(0) Never(3) 1-2 times(4 ) Every month(5) Every week(6) Almost every day
4. During the past three months, how often did the use of the following substances lead to problems with the law, finances, health, or relationships with others?
Nicotine (tobacco, electronic cigarettes)(0) Never(4) 1-2 times(5) Monthly(6) Weekly(7) Almost every day
Alcoholic products (beer, wine, alcohol)(0 ) Never(4) 1-2 times(5) Every month(6) Every week(7) Almost every day
Cannabis (marijuana, hashish)(0) Never(4) 1-2 times(5) Every Monthly(6) Weekly(7) Almost every day
Cocaine (coca, crack)(0) Never(4) 1-2 times(5) Monthly(6) Weekly(7) Almost every day
Amphetamine-type stimulants (speed, diet pills, ecstasy and etc.
 )(0) Never(4) 1-2 times(5) Every month(6) Every week(7) Almost every day
)(0) Never(4) 1-2 times(5) Every month(6) Every week(7) Almost every day Inhalants (glue, gasoline, thinner)(0) Never(4) 1 -2 times(5) Every month(6) Every week(7) Almost every day
Sedatives and hypnotics (Corvalol, Xanax, Relanium phenazepam, etc.)(0) Never(4) 1-2 times(5 ) Every month(6) Every week(7) Almost every day
Hallucinogens (LSD, acid, mushrooms, ketamine, etc.)(0) Never(4) 1-2 times(5) Monthly(6) Weekly(7) Almost every day
Opioids (heroin, morphine , methadone, codeine, etc.)(0) Never(4) 1-2 times(5) Every month(6) Every week(7) Almost every day
Other psychoactive substances(0) Never(4) 1 -2 times(5) Every month(6) Every week(7) Almost every day
5. In the past three months, how often have you missed planned or regular activities because of your use? nine0404
Nicotine (tobacco, electronic cigarettes)(0) Never(5) 1-2 times(6) Monthly(7) Weekly(8) Almost every day
Alcoholic products (beer, wine, alcohol)(0 ) Never(5) 1-2 times(6) Monthly(7) Weekly(8) Almost every day
Cannabis (marijuana, hashish)(0) Never(5) 1-2 times(6) Every Monthly(7) Weekly(8) Almost every day
Cocaine (coca, crack)(0) Never(5) 1-2 times(6) Monthly(7) Weekly(8) Almost every day
Amphetamine-type stimulants (speed, diet pills, ecstasy, etc.
 )(0) Never(5) 1-2 times(6) Monthly(7) Weekly(8) Nearly every day
)(0) Never(5) 1-2 times(6) Monthly(7) Weekly(8) Nearly every day Inhalants (glue, gasoline, thinner)(0) Never(5) 1-2 times(6) Monthly(7) Weekly(8) Almost every day
0) Never(5) 1-2 times(6) Monthly(7) Weekly(8) Almost every day
Hallucinogens (LSD, acid, mushrooms, ketamine, etc.)(0) Never(5) 1-2 times(6) Every month(7) Every week(8) Almost every day
Opioids (heroin, morphine, methadone, codeine, etc.)(0) Never(5) 1-2 times(6) Monthly(7) Weekly(8) Almost every day
Other psychoactive substances(0 ) Never(5) 1-2 times(6) Monthly(7) Weekly(8) Almost every day
6. Has anyone expressed concern to you about what you used?
Nicotine (tobacco products, electronic cigarettes)(0) Never(6) Yes, in the last 3 months(3) Yes, but not in the last 3 months
Alcoholic products (beer, wine, spirits)(0) Never(6) Yes, within the last 3 months(3) Yes, but not within the last 3 months
Cannabis (marijuana, hashish)(0) Never( 6) Yes, within the past 3 months(3) Yes, but not within the past 3 months
Cocaine (coca, crack)(0) Never(6) Yes, within the past 3 months(3) Yes, but not within the past 3 months
Amphetamine-type stimulants (speed, diet pills, ecstasy, etc.
 )(0) Never(6) Yes, within the past 3 months(3) Yes, but not within the past 3 months
)(0) Never(6) Yes, within the past 3 months(3) Yes, but not within the past 3 months Inhalants (glue, petrol, thinner)(0) Never(6) Yes, within the last 3 months(3) Yes, but not within the last 3 months
Sedatives and hypnotics (Corvalol, Xanax, Relanium etc.)(0) Never(6) Yes, in the last 3 months(3) Yes, but not in the last 3 months
Hallucinogens (LSD, acid, mushrooms, ketamine, etc.)(0) Never(6 ) Yes, within the last 3 months(3) Yes, but not within the last 3 months
Opioids (heroin, morphine, methadone, codeine, etc.)(0) Never(6) Yes, within the last 3 months(3) Yes, but not within the last 3 months
Other psychoactive substances(0) Never( 6) Yes, within the last 3 months(3) Yes, but not within the last 3 months
7. Have you ever tried to control your use and failed?
Nicotine (tobacco products, electronic cigarettes)(0) Never(6) Yes, in the last 3 months(3) Yes, but not in the last 3 months
Alcoholic products (beer, wine, spirits)(0) Never(6) Yes, within the last 3 months(3) Yes, but not within the last 3 months
Cannabis (marijuana, hashish)(0) Never( 6) Yes, within the past 3 months(3) Yes, but not within the past 3 months
Cocaine (coca, crack)(0) Never(6) Yes, within the past 3 months(3) Yes, but not within the past 3 months
Amphetamine-type stimulants (speed, diet pills, ecstasy, etc.