Purpose of mmpi 2
The Minnesota Multiphasic Personality Inventory
The Minnesota Multiphasic Personality Inventory (MMPI) is one of the most commonly used psychological tests in the world.
The test was developed by clinical psychologist Starke Hathaway and neuropsychiatrist J.C. McKinley, two faculty members at the University of Minnesota. It was created to be a tool for mental health professionals to help diagnose mental health disorders.
Since its publication in 1943, the test has been updated several times in an attempt to eliminate racial and gender bias and to make it more accurate. The updated test, known as the MMPI-2, has been adapted for use in over 40 countries.
This article will take a closer look at the MMPI-2 test, what it’s used for, and what it can help diagnose.
The MMPI-2 is a self-report inventory with 567 true-false questions about yourself. Your answers help mental health professionals determine whether you have symptoms of a mental illness or personality disorder.
Some questions are designed to reveal how you feel about taking the test. Other questions are intended to reveal whether you’re being genuine or are under- or over-reporting in an effort to influence the test results.
For most people, the MMPI-2 test takes 60 to 90 minutes to complete.
A shorter version of the test, the MMPI-2 Restructured Form (RF), has 338 questions. This shortened version takes less time to complete — between 35 and 50 minutes for most people.
Researchers have also designed a version of the test for adolescents ages 14 to 18. This test, known as the MMPI-A, has 478 questions and can be completed in about an hour.
There is also a shorter version of the test for teenagers called the MMPI-A-RF. Made available in 2016, the MMPI-A-RF has 241 questions and can be finished in 25 to 45 minutes.
Although the shorter tests are less time consuming, many clinicians opt for the longer assessment because it has been researched over the years.
MMPI tests are used to help diagnose mental health disorders, but many mental health professionals don’t rely on a single test to make a diagnosis. They usually prefer to gather information from many sources, including their own interactions with the person being tested.
The MMPI should only be administered by a trained test administrator, but the test results are sometimes used in other settings.
MMPI evaluations are sometimes used in child custody disputes, substance abuse programs, educational settings, and even employment screenings.
It’s important to note that using the MMPI as part of a job qualification process has caused some controversy. Some advocates argue that it violates the provisions of the Americans with Disabilities Act (ADA).
The test items on the MMPI are designed to find out where you are on ten different mental health scales.
Each scale relates to a different psychological pattern or condition, but there’s a lot of overlap between the scales.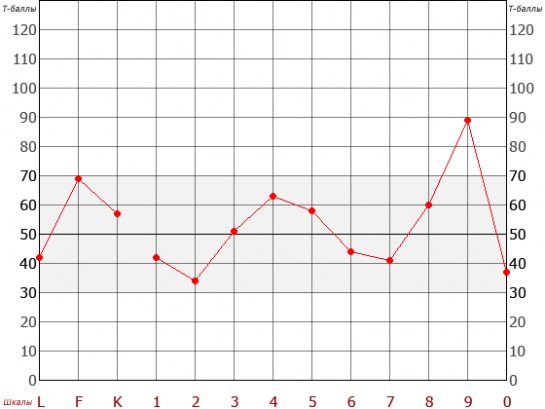 Generally speaking, very high scores may indicate a mental health disorder.
Generally speaking, very high scores may indicate a mental health disorder.
Here’s a brief explanation of what each scale evaluates.
Scale 1: Hypochondriasis
This scale contains 32 items and is designed to measure whether you have an unhealthy concern for your own health.
A high score on this scale could mean that worrying about your health is interfering with your life and causing problems in your relationships.
For example, a person with a high Scale 1 score might be prone to developing physical symptoms that don’t have an underlying cause, especially during periods of high stress.
Scale 2: Depression
This scale, which has 57 items, measures satisfaction with your own life.
A person with a very high Scale 2 score could be dealing with clinical depression or having frequent suicidal thoughts.
A slightly elevated score on this scale could be an indication that you’re withdrawn or unhappy with your circumstances.
Scale 3: Hysteria
This 60-item scale evaluates your response to stress, including both your physical symptoms and emotional response to being under pressure.
Studies have shown that people with chronic pain may score higher on the first three scales because of prolonged, heightened health concerns.
Scale 4: Psychopathic deviate
This scale was originally intended to reveal whether you are experiencing psychopathology.
Its 50 items measure antisocial behaviors and attitudes, in addition to compliance or resistance to authority.
If you score very high on this scale, you might receive a diagnosis with a personality disorder.
Scale 5: Masculinity/femininity
The original purpose of this 56-question test section was to elicit information about people’s sexuality. It stems from a time in which some mental health professionals viewed same-sex attraction as a disorder.
Today, this scale is used to evaluate how consistently you seem to identify with gender norms.
Scale 6: Paranoia
This scale, which has 40 questions, evaluates symptoms associated with psychosis, particularly:
- extreme suspicion of other people
- grandiose thinking
- rigid black-and-white thinking
- feelings of being persecuted by society
High scores on this scale could indicate that you are dealing with either a psychosis disorder or a paranoid personality disorder.
Scale 7: Psychasthenia
This 48-item scale measures:
- anxiety
- depression
- compulsive behaviors
- symptoms of obsessive-compulsive disorder (OCD)
The term “psychasthenia” is no longer used as a diagnosis, but mental health professionals still use this scale as a way of evaluating unhealthy compulsions and the disruptive feelings they cause.
Scale 8: Schizophrenia
This 78-item scale is intended to show whether you have, or are likely to develop, a schizophrenia disorder.
It considers whether you’re experiencing hallucinations, delusions, or bouts of extremely disorganized thinking. It also determines to what degree you may feel alienated from the rest of society.
Scale 9: Hypomania
The purpose of this 46-item scale is to evaluate the symptoms associated with hypomania, including:
- excessive undirected energy
- rapid speech
- racing thoughts
- hallucinations
- impulsivity
- delusions of grandeur
If you have a high Scale 9 score, you may be having symptoms associated with bipolar disorder.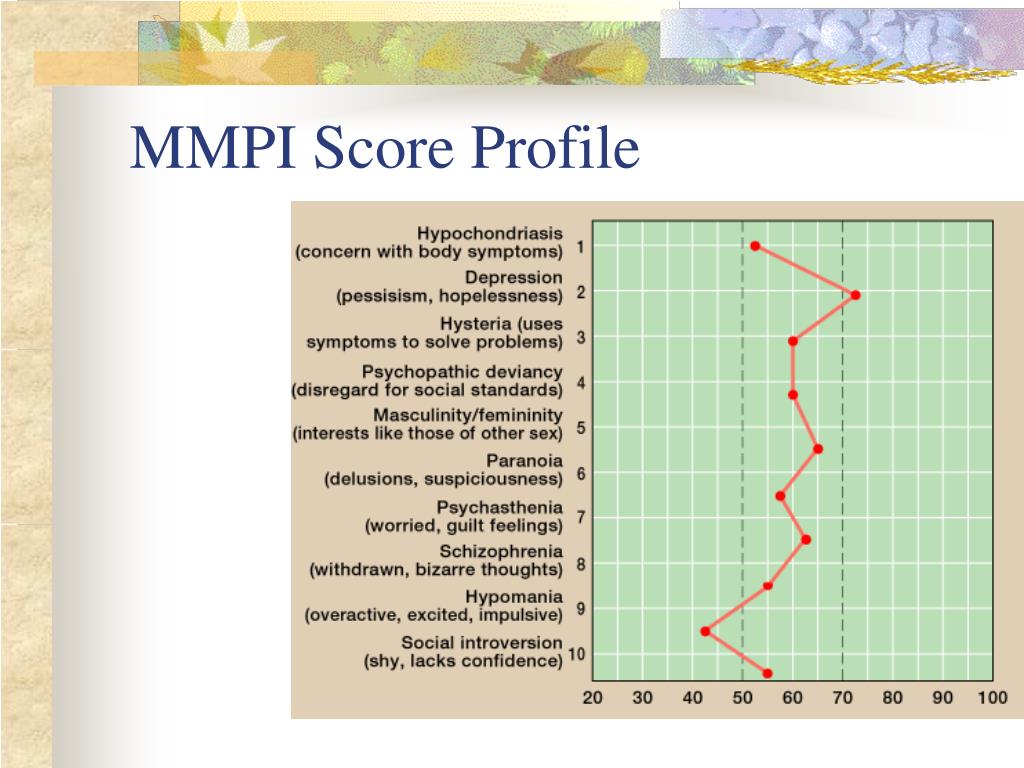
Scale 10: Social introversion
One of the later additions to the MMPI, this 69-item scale measures extroversion or introversion. This is the degree to which you seek out or withdraw from social interactions.
This scale considers, among other things, your:
- competitiveness
- compliance
- timidity
- dependability
Validity scales help test administrators understand how genuine a test taker’s answers are.
In situations where test results could impact a person’s life, such as employment or child custody, people might be motivated to over-report, under-report, or be dishonest. These scales help reveal inaccurate answers.
The “L” or lie scale
People who score high on the “L” scale may be trying to present themselves in a glowing, positive light by refusing to acknowledge traits or responses they fear could make them look bad.
The “F” scale
Unless they’re choosing random answers, people who score high on this scale may be trying to seem in worse condition than they actually are.
These test items aim to reveal inconsistencies in answer patterns. It’s important to note that a high score on the “F” scale could also indicate severe distress or psychopathology.
The “K” scale
These 30 test items focus on self-control and relationships. They’re intended to reveal a person’s defensiveness around certain questions and traits.
Like the “L” scale, items on the “K” scale are designed to highlight a person’s need to be seen positively.
The CNS scale
Sometimes called the “Cannot Say” scale, this evaluation of the entire test measures how often a person doesn’t answer a test item.
Tests with more than 30 unanswered questions may be invalidated.
The TRIN and VRIN scales
These two scales detect answer patterns that indicate the person taking the test chose answers without actually considering the question.
In a TRIN (True Response Inconsistency) pattern, someone uses a fixed answer pattern, such as five “true” followed by five “false” answers.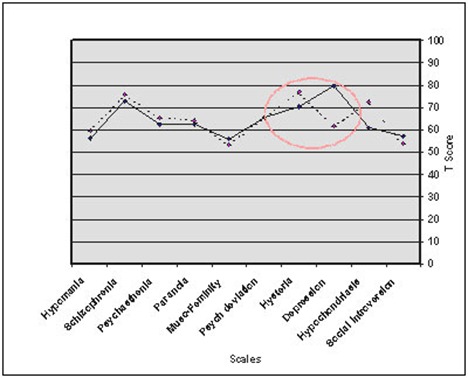
In a VRIN (Varied Response Inconsistency) pattern, a person responds with random “trues” and “falses.”
The Fb scale
To catch a significant change in answers between the first and second halves of the test, test administrators look at 40 questions in the second half of the test that aren’t usually endorsed.
If you answer “true” to these questions 20 more times than you answer “false,” the test administrator may conclude that something is distorting your answers.
It could be that you’ve become fatigued, distressed, or distracted, or that you have begun to over-report for another reason.
The Fp scale
These 27 test items are intended to reveal whether you’re intentionally or unintentionally over-reporting, which can indicate a mental health disorder or extreme distress.
The FBS scale
These 43 test items, which are sometimes called the “symptom validity” scale, are designed to detect intentional over-reporting of symptoms. This can sometimes happen when people are pursuing personal injury or disability claims.
The “S” scale
The Superlative Self-Presentation scale takes a look at how you answer 50 questions about serenity, contentment, morality, human goodness, and virtues like patience. This is to see if you could be intentionally distorting answers to look better.
If you under-report in 44 of the 50 questions, the scale indicates that you may be feeling a need to be defensive.
The MMPI-2 has a total of 567 test items, and it will take you between 60 and 90 minutes to finish. If you’re taking the MMPI2-RF, you should expect to spend between 35 and 50 minutes answering 338 questions.
There are booklets available, but you can also take the test online, either by yourself or in a group setting.
The test is copyrighted by the University of Minnesota. It’s important that your test is administered and scored according to the official guidelines.
To be sure that your test results are interpreted and explained to you accurately, it’s a good idea to work with a clinical psychologist or psychiatrist specially trained in this kind of testing.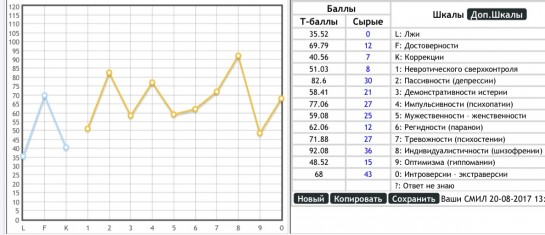
The MMPI is a well-researched and respected test designed to help mental health professionals diagnose mental health disorders and conditions.
It’s a self-reporting inventory that evaluates where you fall on 10 scales related to different mental health disorders. The test also uses validity scales to help test administrators understand how you feel about taking the test and whether you’ve answered the questions accurately and honestly.
Depending on which version of the test you take, you can expect to spend between 35 and 90 minutes answering the questions.
The MMPI is a reliable and widely used test, but a good mental health professional won’t make a diagnosis based solely on this one assessment tool.
Minnesota Multiphasic Personality Inventory - StatPearls
Augustus E. Floyd; Vikas Gupta.
Author Information
Last Update: April 28, 2022.
Definition/Introduction
The Minnesota Multiphasic Personality Inventory (MMPI) is the most common psychometric test devised to assess personality traits and psychopathology.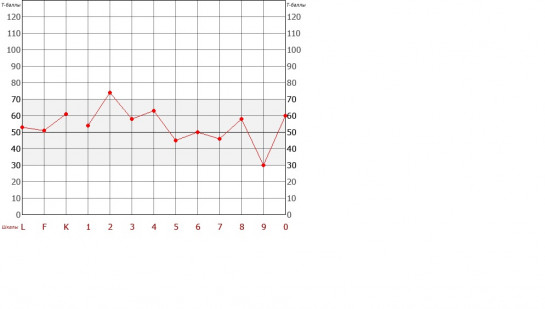 This data can be used to draw conclusions about the test taker’s psychopathy or to interpret psychological characteristics compared to the norm.[1] The most common treatment application of the test by providers is establishing or reevaluating care for an ambiguous clinical picture.[2] For psychiatric management, this aids in creating generalizable data relevant to a plethora of possible conditions.[1][2]
This data can be used to draw conclusions about the test taker’s psychopathy or to interpret psychological characteristics compared to the norm.[1] The most common treatment application of the test by providers is establishing or reevaluating care for an ambiguous clinical picture.[2] For psychiatric management, this aids in creating generalizable data relevant to a plethora of possible conditions.[1][2]
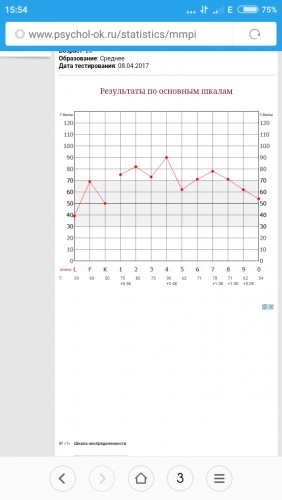
The MMPI was developed in the 1930s and published through the University of Minnesota in 1942 by Stuart Hathaway and Charley McKinley using visitors of patients at the University of Minnesota hospital as a base sample in both theorizing constructs of psychiatric illness and fielding the instrument. Testing is administered through 567 true or false items using a booklet with an accompanying answer sheet. The responses are then hand-scored and plotted on an X-Y graph; a separate version is used for male and female respondents.[3]
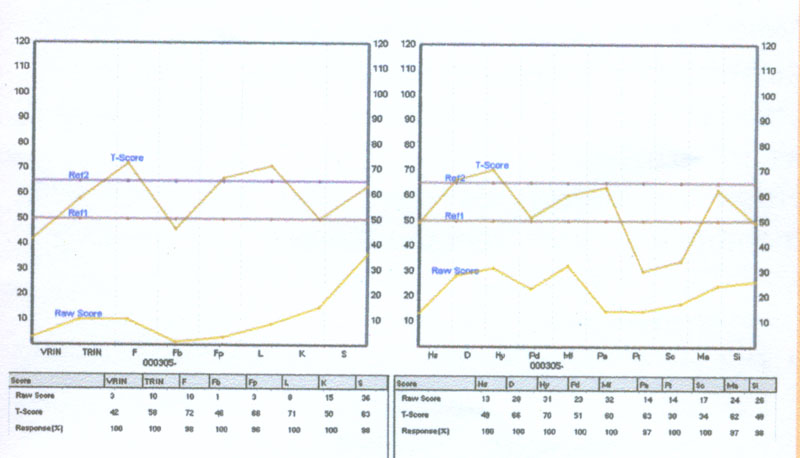
The X-axis is comprised of 14 scales. The first four ‘content scales’ judge the validity of the test attempt and include:
? to represent the number of questions completed incorrectly, either with no attempt or both ‘true’ and ‘false’ selected
L for ‘Lie’ to represent an attempt by the respondent to misrepresent themselves in a more positive light
F or ‘frequency’ to gauge random response as well as the respondent’s exaggeration or downplaying of symptoms
K to gauge ‘defensiveness,’ or evasion of stressful content
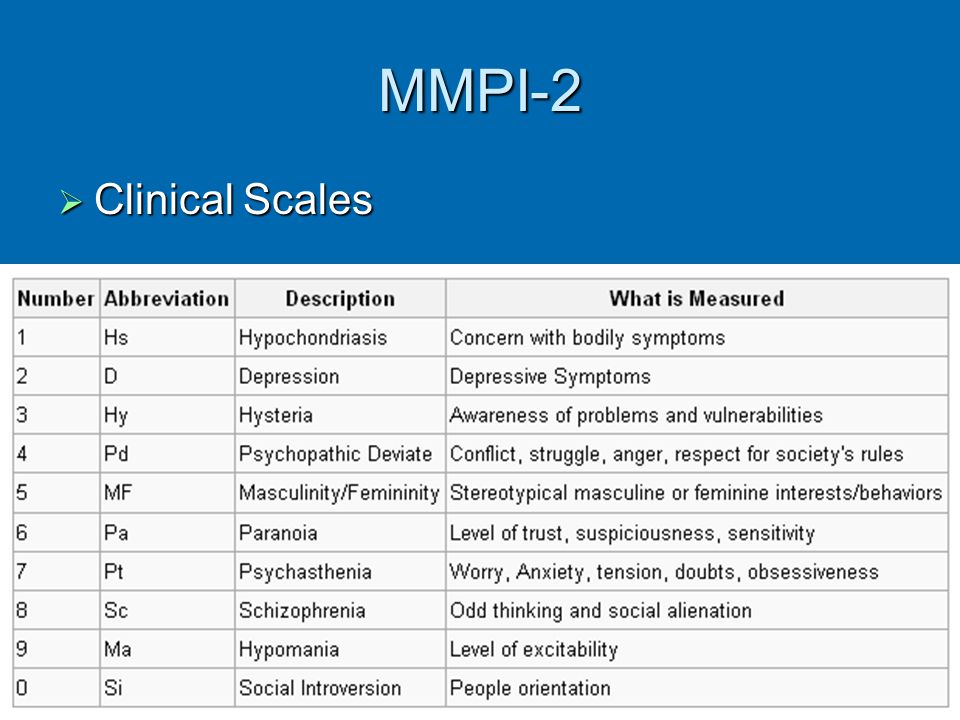
The 10 remaining scales known as ‘clinical scales’ are designed to measure for the presence of psychiatric syndromes, including:
1 or ‘Hs’ for hypochondriasis
2 or ‘D’ for depression
3 or ‘Hy’ for hysteria
4 or ‘Pd’ for psychopathic deviate
5 or ‘Mf’ for the continuum of masculinity-femininity
6 or ‘Pa’ for paranoia
7 or ‘Pt’ for psychasthenia or obsessive-compulsive tendency
8 or ‘Sc’ for schizophrenia
9 or ‘Ma’ for mania
0 or ‘Si’ for social introversion.
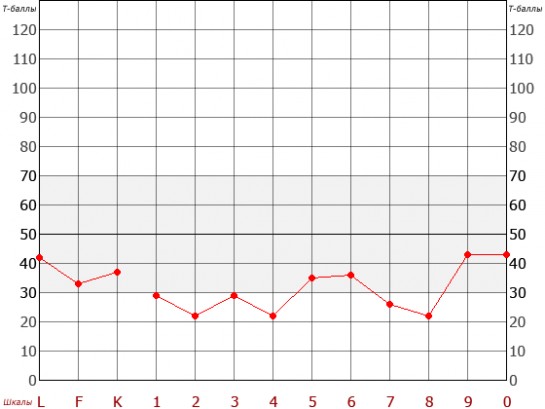
The Y-axis statistically standardizes the grading received on each scale in a range of T-scores from 0 to 120. A mean score is 50, and 82% of respondents are considered the normal population falling between 30 and 70. A T-score greater than 70 indicates psychopathy in that category.
Issues of Concern
The existence of the MMPI has been concurrent with vast reforms in societal convention and increased understanding of behavioral health.[3] Likewise, the instrument has been adapted to reflect such changes. Overarching criticisms to the original test center on its disparity in addressing psychopathy in social and ethnic minorities.[1] This has been attributed to the original sample being a small group, mainly consisting of young rural Caucasian subjects from the Midwestern United States.[4] Studies have established biases in which misunderstanding or failure to identify with the content of questions culturally has led to underreporting or overreporting mental illness.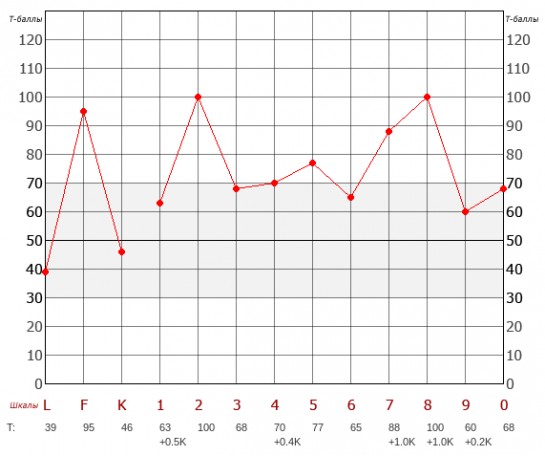 [5][1]
[5][1]
These shortcomings led to the release of the MMPI-2 by James N. Butcher, W. Grant Dahlstrom, John R. Graham, Auke Tellegen, and Beverly Kaemme in 1989.[6] This assessment retains the original total of 567 items with the same corresponding 14 scales with the original number of questions from the test.[6] Test items were revised based upon a larger and more diverse sample size of 2600 attuned to a 6th-grade reading level.[6] Gendered differences were replaced with a nongendered standardized scoring.[6] Despite further advancements, the MMPI-2 is still the most commonly administered version and has been translated into over 40 languages.[1]
In 2003, 9 restructured clinical or ‘RC’ scales were introduced as a prospective replacement for the original clinical scales.[1] These include:
RCd, or ‘demoralization’ – misery or depression
RC1 or ‘somatic complaints, – the fixation on bodily symptoms of illness or somatization
RC2 or ‘low positive emotions’ – weakened positivity, lack of enjoyment
RC3 or ‘cynicism’ – low regard for the merit of others and their actions
RC4 or ‘antisocial behavior’ – selfish and sociopathic conduct
RC6 or ‘ideas of persecution’ – belief in the malintent of others toward oneself
RC7 or ‘dysfunctional negative emotions’ – experiences on a spectrum of anxiety and irritability
RC8 or ‘aberrant experiences’ – uncommon beliefs or interpretation of experiences
RC9 or ‘hypomanic activation’ – energetic drive and desire for exertion
The RC scales were devised to provide a streamlined interpretation and less overlap with an increased focus on the growth in understanding within psychiatry over the past 70 years.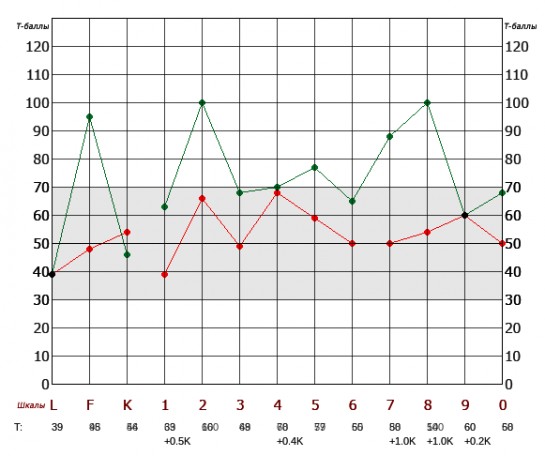 Combinations of high-scoring categories represent distinct psychiatric constructs rather than the nebulous findings of the original clinical scales tying the patient to a specific diagnosis. Arguments also exist that this information is limited in that it categorizes the responder rather than providing data on an individual patient within a personalized spectrum of behavior.[1]
Combinations of high-scoring categories represent distinct psychiatric constructs rather than the nebulous findings of the original clinical scales tying the patient to a specific diagnosis. Arguments also exist that this information is limited in that it categorizes the responder rather than providing data on an individual patient within a personalized spectrum of behavior.[1]
The RC scales were incorporated into the most current form of the MMPI, known as the Minnesota Multiphasic Personality Inventory-2 Revised Form, or the MMPI-2-RF, which was released in 2008 by Yossef Ben-Porath and Auke Telleger of the University of Minnesota. The MMPI-2-RF is composed of 338 items measured by 51 scales broken into 9 validity scales, 3 higher-order scales, the 9 RC scales, 23 specific problem scales, 2 interest scales, and 5 revised personality psychopathy scales.[1]
The 9 validity scales assess incongruent answering or deceptive test-taking and include:
VRIN-r or ‘variable response inconsistency’ – inconsistent reporting of items
TRIN-r or ‘true response inconsistency’ careless reporting of items
F-r or ‘infrequent responses,’ – overreporting of infrequent responses compared to the norm
Fp-r or ‘infrequent psychopathology responses’ – overreporting of infrequent responses compared to those with psychopathy
Fs or ‘infrequent somatic responses’ – overreporting of infrequent responses compared to medical patients
FBS-r or ‘symptom validity’ – overreporting of nonvalid symptoms compared to both physical and mental standard symptomology
RBS or ‘response bias’ – overreporting associated with a statistically invalidated presentation of the disease
L-r or ‘uncommon virtues’ – underreporting through infrequently declared values or actions
K-r or ‘adjustment validity’ – underreporting by tailoring answers to give the impression of healthy psychological adjustment
The 3 higher-order scales broadly categorize psychopathic presentation and include:
EID or ‘emotional/internalizing dysfunction’ – problems concerning mood and affect
THD or ‘thought dysfunction’ – problems concerning disorganization of thought
BXD or ‘behavioral/external dysfunction’ – problems concerning impulsive or inappropriate behavior
The problem scales highlight responses consistent with the presence of specific psychopathic and psychosomatic presentations and include:
MLS or ‘malaise’
GIC or ‘gastrointestinal complaints’
HPC or ‘head pain complaints'
NUC or ‘neurological complaints’
COG or ‘cognitive complaints’
SUI or ‘suicidal/death ideation’
HLP or ‘helplessness/hopelessness’
SFD or ‘self-doubt’
NFC or ‘inefficacy’
STW or ‘stress/worry’
AXY or ‘anxiety’
ANP or ‘anger proneness’
BRF or ‘behavior-restricting fears’
MSF or ‘multiple specific fears’
JCP or ‘juvenile conduct problems’
SUB or ‘substance abuse’
AGG or ‘aggression’
ACT or ‘activation’
FML or ‘family problems’
IPP or ‘interpersonal passivity’
SAV or ‘social avoidance’
SHY or ‘shyness’
DSF or ‘disaffiliativeness’
The interest scales are designed to assess cognitive skills, aptitude, and learning preferences which include:
AES or aesthetic-literary interests – pursuits related to fine art
MEC or mechanical-physical interests – pursuits related to kinesthetic activities
The revised personality/psychopathology five scales are based on 107 distinct items and include:
AGG-r or ‘aggressiveness-revised’ – preference for excess and antagonism
PSYCH-r or ‘psychoticism-revised’ – preference for disconnection from reality
DISC-r or ‘disconstraint-revised’ – preference for impulsion and compulsion
NEGE-r or ‘negative emotionality/neuroticism-revised’ – preference for anxiety
INTR-r or ‘introversion/low positive emotional-revised’ – flat affect and timidity
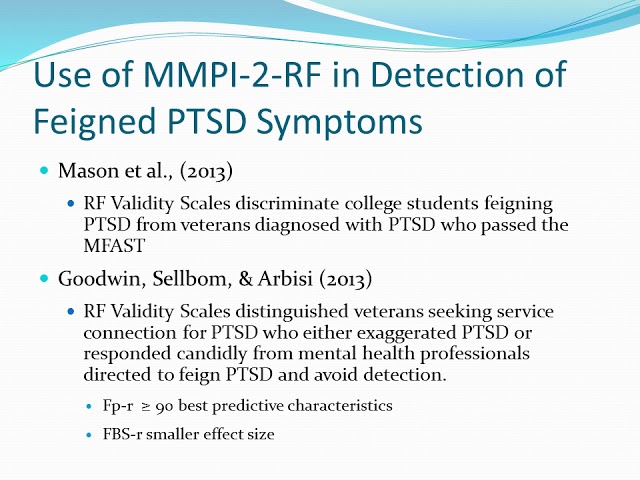
It has been suggested that while the MMPI-2-RF has many additional metrics, the reduction in question number limits the amount of information about psychiatric diseases to about 60% of the original test. There has also been considerable debate over whether the new metrics are inaccurate in detecting psychopathy.[1] In separating genuine psychopathy from attempts to feign a diagnosis for personal incentive, some studies have noted the new validity scales to be overly sensitive to overreporting symptoms to achieve a specific result. It has conversely been found that the L-r and K-r scales are particularly reliable at detecting underreporting of mental illness.[7][8] Overall, literature has supported the MMPI-2-RF in identifying the accuracy of reporting psychiatric information in those who complete it.[1]
There has also been considerable debate over whether the new metrics are inaccurate in detecting psychopathy.[1] In separating genuine psychopathy from attempts to feign a diagnosis for personal incentive, some studies have noted the new validity scales to be overly sensitive to overreporting symptoms to achieve a specific result. It has conversely been found that the L-r and K-r scales are particularly reliable at detecting underreporting of mental illness.[7][8] Overall, literature has supported the MMPI-2-RF in identifying the accuracy of reporting psychiatric information in those who complete it.[1]
Clinical Significance
The MMPI maintains an enduring presence in the field of mental health, and its current adaption has been widely evaluated by the standard of modern behavioral health practices.[1] It continues to receive widespread application as a threshold of determining the presence of psychopathy, as a means of constructing a differential diagnosis for mental health problems, and as a versatile test to achieve transferrable psychological data.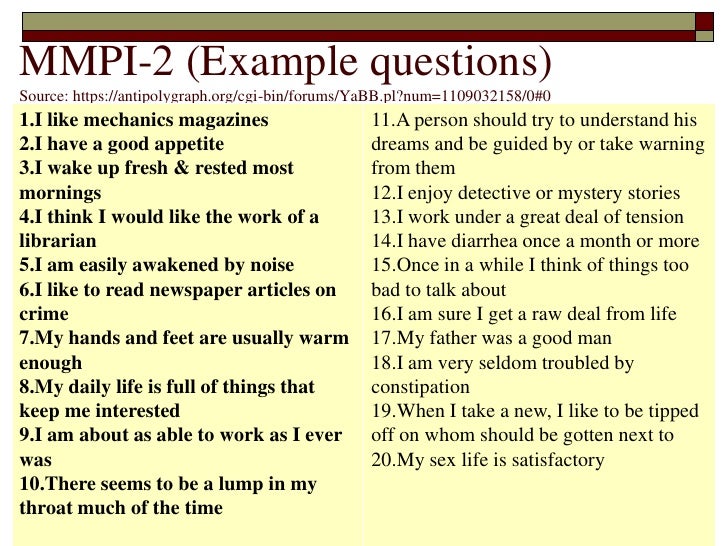 These data points indicate a category, which gives behavioral health professionals a starting point to explore plausible diagnoses and initiate appropriate treatment. Completion may also offer therapeutic benefits to patients in reflecting upon their issues and improving personal understanding of their psychology.[3]
These data points indicate a category, which gives behavioral health professionals a starting point to explore plausible diagnoses and initiate appropriate treatment. Completion may also offer therapeutic benefits to patients in reflecting upon their issues and improving personal understanding of their psychology.[3]
In addition to its predominant clinical application, an extensive body of research exists to assess the MMPI in all its versions for the use in criminology, population studies, and prediction of aptitude in a particular role. Several studies on the MMPI-2-RF have compared those with a criminal history to those who have undergone rehabilitation and found that high scores on externalizing scales were predictive of violent behavior.[9] The MMPI-2-RF has also been used to prescreen applicants for law enforcement to obtain baseline mental health or flagging for aggressive tendencies.[1][10] There has also been usage evaluating parenting suitability in custody battles over children and in predicting the course of domestic disputes in couples. [11][12] Interpretations of the test have also been used to establish criminal intent in defendants.[1][9]
[11][12] Interpretations of the test have also been used to establish criminal intent in defendants.[1][9]
A major consensus of the MMPI in its current form is that increased accessibility for being tested improves retention without compromising outcomes. Prevailing criticisms of the original format were the extensive span of questioning and difficulty of paper administration for both completion and grading, with efforts to provide a more efficient medium well-documented since the 1980s.[13] When evaluating the use of tablet devices compared to conventional forms of electronic administration using a home computer or laptop for taking the MMPI-RF-2, the difference in reliability of results between the two mediums was insignificant.[14] There have also been motions to use the MMPI-2-RF to assess psychopathy utilizing an algorithm using a high score on a higher-order scale and then tailoring the remaining assessment to similar questions to the indicated higher order.[15] To aid in administration to pediatric patients, an adolescent form exists known as the Minnesota Multiphasic Personality Inventory-Adolescent-Restructured Form (MMPI-A-RF). [16]
[16]
Clinical Pearls
The MMPI provides broad information about aspects of personality and the existence of components of psychopathology.
The MMPI is completed by indicating true/false to a series of declarative statements that identify personal beliefs or symptomology.
Interpretation is based upon scoring reasonably truthfully and consistently within the outlined scales of the test.
Scales in older versions represented clinical syndromes, while more recently developed scales are based on identifying symptoms that can be applied to appropriate conditions or disorders.
The MMPI is effective at distinguishing psychopathy from malingering or purposeful test-taking as well as from medical conditions.
The MMPI has been revised to make the test more efficient, reproducible to test-takers in a broader societal demographic, and more grounded in current theory.
The MMPI can be taken by an individual patient to provide evidence of their symptoms but can also be fielded to a population fitting a known category to observe trends within their scoring.
The MMPI has been applied to a variety of non-clinical settings, including legal evidence in criminal and civil cases and screening for employment.
The completion of the MMPI holds value in determining care throughout a variety of treatment considerations. The test should be administered by a licensed psychotherapist, usually a psychiatrist or clinical psychologist, with informed consent obtained by discussing the risks and benefits of completion. Analysis of the results by the psychotherapist interpreting scoring should be attached with a working diagnosis to assess for treatment response. The presence of conditions associated with high-scoring categories will ultimately guide the necessity for pharmacological or non-pharmacological treatment options. This will, in turn, outline the need for referral to appropriate mental healthcare, from continuing outpatient follow-up to institutionalization with fully-staffed nursing and rehabilitative care. Transfer of care should involve appropriate discussion of MMPI data correlated with a summary of interventions.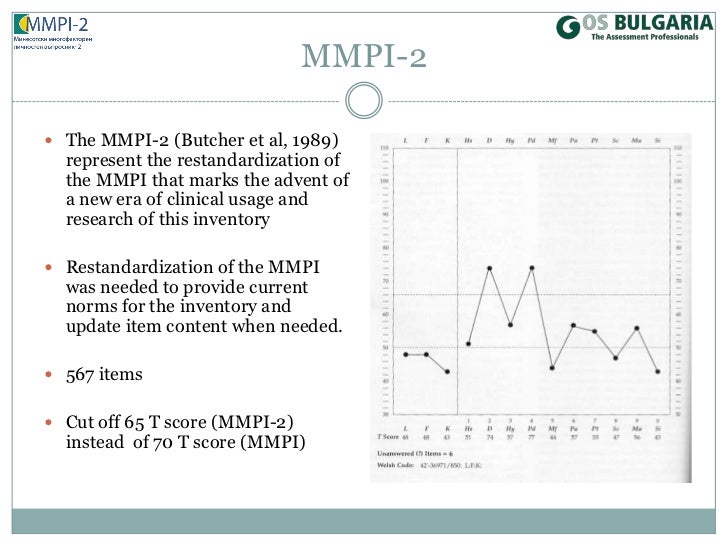 High-scoring in concerning scales such as suicidality highlights an existing need for acute observation or placement. The validity of symptoms should also be corroborated to demonstrate whether a patient is malingering or suffering from organic disorders requiring medical management by a treatment team. The bio-ethical implications of the MMPI should also be identified if the patient is completing the test in concurrence or stipulation with legal charges, and they should be counseled on what findings might hold concerning criminality. The basis for the use of test data in determining adherence has also been documented in a sample consisting of 471 psychiatric patients, with externalizing scales predictive of whether a patient will be more likely to terminate treatment.[1] [Level 3] This illustrates the need for multi-level involvement in facilitating outreach and patient compliance.
High-scoring in concerning scales such as suicidality highlights an existing need for acute observation or placement. The validity of symptoms should also be corroborated to demonstrate whether a patient is malingering or suffering from organic disorders requiring medical management by a treatment team. The bio-ethical implications of the MMPI should also be identified if the patient is completing the test in concurrence or stipulation with legal charges, and they should be counseled on what findings might hold concerning criminality. The basis for the use of test data in determining adherence has also been documented in a sample consisting of 471 psychiatric patients, with externalizing scales predictive of whether a patient will be more likely to terminate treatment.[1] [Level 3] This illustrates the need for multi-level involvement in facilitating outreach and patient compliance.
Nursing, Allied Health, and Interprofessional Team Interventions
The MMPI can be a valuable tool in assessing the psychological status of a patient.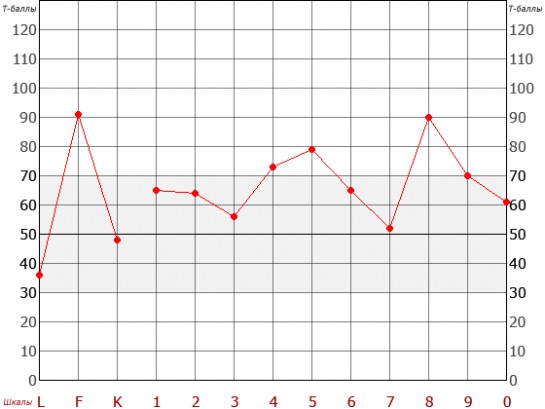 It will be ordered by a psychologically trained clinician but can provide crucial information to many members of the interprofessional healthcare team, including family clinicians, psychologically trained nursing staff, social workers, and counselors. Specifics regarding its use will vary depending on the clinical situation, and it needs to be part of a more complete evaluation to help direct therapeutic interventions and drive optimal patient outcomes. [Level 5]
It will be ordered by a psychologically trained clinician but can provide crucial information to many members of the interprofessional healthcare team, including family clinicians, psychologically trained nursing staff, social workers, and counselors. Specifics regarding its use will vary depending on the clinical situation, and it needs to be part of a more complete evaluation to help direct therapeutic interventions and drive optimal patient outcomes. [Level 5]
Review Questions
Access free multiple choice questions on this topic.
Comment on this article.
References
- 1.
Sellbom M. The MMPI-2-Restructured Form (MMPI-2-RF): Assessment of Personality and Psychopathology in the Twenty-First Century. Annu Rev Clin Psychol. 2019 May 07;15:149-177. [PubMed: 30601687]
- 2.
Butcher JN. Personality assessment from the nineteenth to the early twenty-first century: past achievements and contemporary challenges.
 Annu Rev Clin Psychol. 2010;6:1-20. [PubMed: 20192801]
Annu Rev Clin Psychol. 2010;6:1-20. [PubMed: 20192801]- 3.
Schilling R, Casper ST. Of psychometric means: Starke R. Hathaway and the popularization of the Minnesota Multiphasic Personality Inventory. Sci Context. 2015 Mar;28(1):77-98. [PubMed: 25832571]
- 4.
Carter JH. Racism's impact on mental health. J Natl Med Assoc. 1994 Jul;86(7):543-7. [PMC free article: PMC2607595] [PubMed: 8064907]
- 5.
Dennis PH. A comparative study of Minnesota Multiphasic Personality Inventory (MMPI) scores of four apparently different black populations. J Natl Med Assoc. 1974 May;66(3):244-7 passim. [PMC free article: PMC2609171] [PubMed: 4151276]
- 6.
Drayton M. The Minnesota Multiphasic Personality Inventory-2 (MMPI-2). Occup Med (Lond). 2009 Mar;59(2):135-6. [PubMed: 19233834]
- 7.
Ingram PB, Ternes MS. The detection of content-based invalid responding: a meta-analysis of the MMPI-2-Restructured Form's (MMPI-2-RF) over-reporting validity scales.
 Clin Neuropsychol. 2016 May;30(4):473-96. [PubMed: 27214667]
Clin Neuropsychol. 2016 May;30(4):473-96. [PubMed: 27214667]- 8.
Tarescavage AM, Scheman J, Ben-Porath YS. Reliability and validity of the Minnesota Multiphasic Personality Inventory-2-Restructured Form (MMPI-2-RF) in evaluations of chronic low back pain patients. Psychol Assess. 2015 Jun;27(2):433-446. [PubMed: 25436662]
- 9.
Whitman MR, Tarescavage AM, Glassmire DM, Burchett D, Sellbom M. Examination of differential validity of MMPI-2-RF scores by gender and ethnicity in predicting future suicidal and violent behaviors in a forensic sample. Psychol Assess. 2019 Mar;31(3):404-409. [PubMed: 30520653]
- 10.
Marshall RE, Milligan-Saville JS, Steel Z, Bryant RA, Mitchell PB, Harvey SB. A prospective study of pre-employment psychological testing amongst police recruits. Occup Med (Lond). 2020 May 27;70(3):162-168. [PubMed: 32040153]
- 11.
Lee TTC, Taylor AM, Holbert AM, Graham JR. MMPI-2-RF predictors of interpersonal relationship characteristics in committed couples.
 Psychol Assess. 2019 Sep;31(9):1118-1124. [PubMed: 31192629]
Psychol Assess. 2019 Sep;31(9):1118-1124. [PubMed: 31192629]- 12.
Fariña F, Redondo L, Seijo D, Novo M, Arce R. A meta-analytic review of the MMPI validity scales and indexes to detect defensiveness in custody evaluations. Int J Clin Health Psychol. 2017 May-Aug;17(2):128-138. [PMC free article: PMC6220924] [PubMed: 30487888]
- 13.
Deskovitz MA, Weed NC, McLaughlan JK, Williams JE. Interpretive Reliability of Six Computer-Based Test Interpretation Programs for the Minnesota Multiphasic Personality Inventory-2. Assessment. 2016 Apr;23(2):250-61. [PubMed: 25944798]
- 14.
Menton WH, Crighton AH, Tarescavage AM, Marek RJ, Hicks AD, Ben-Porath YS. Equivalence of Laptop and Tablet Administrations of the Minnesota Multiphasic Personality Inventory-2 Restructured Form. Assessment. 2019 Jun;26(4):661-669. [PubMed: 28618858]
- 15.
Tarescavage AM, Ben-Porath YS. Examination of the feasibility and utility of flexible and conditional administration of the Minnesota Multiphasic Personality Inventory-2-Restructured Form.
 Psychol Assess. 2017 Nov;29(11):1337-1348. [PubMed: 28165271]
Psychol Assess. 2017 Nov;29(11):1337-1348. [PubMed: 28165271]- 16.
Handel RW. An Introduction to the Minnesota Multiphasic Personality Inventory-Adolescent-Restructured Form (MMPI-A-RF). J Clin Psychol Med Settings. 2016 Dec;23(4):361-373. [PubMed: 27752979]
MMPI-2 - Minnesota Multidisciplinary Personality Inventory. Version 2
Copyright holder:
The University of Minnesota Press, USA
Pearson Assessments (USA)
Authors: James N. Butcher, Ph.D., John R. Graham, Ph.D., Yossef S. Ben- Porath, Ph.D., Auke Tellegen, Ph.D., W. Grant Dahlstrom, Ph.D.
Adaptation of the Russian version: Giunti Psychometrics (Russia), E. I. Rasskazova, D. A. Leontiev, S. A. Bogomaz, V. I. Brutman, L. Ya. Dorfman, S. N. Enikolopov, O. V. Mitina, Yu. Yu. Neyaskina, S. Yu. Palatov, E. V. Chetoshnikova
Format: Online - 567 questions
Passing time: 1.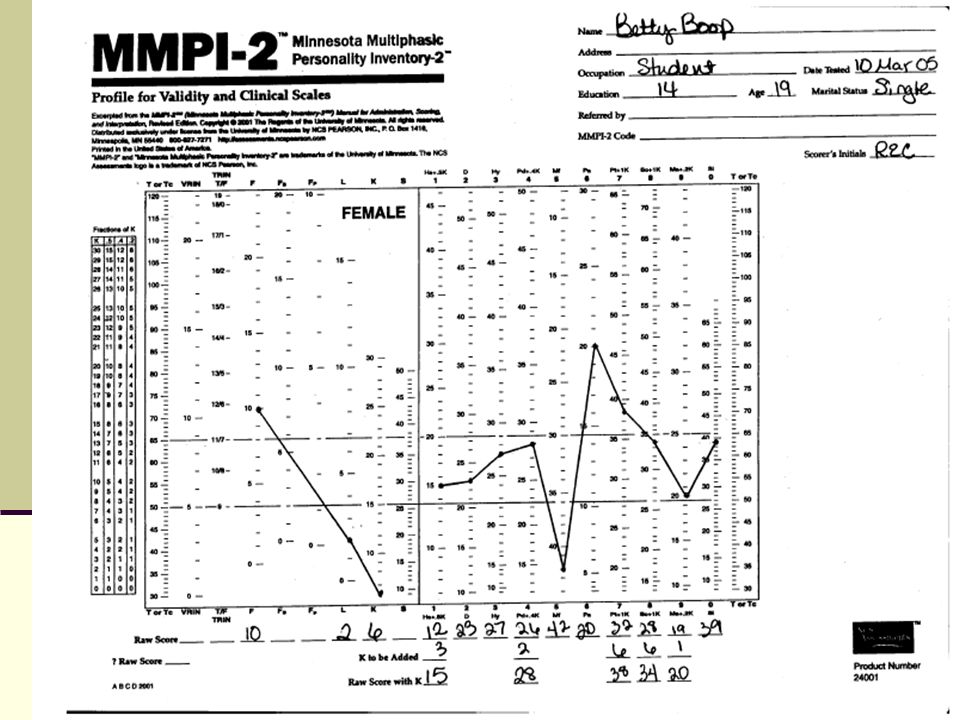 5 - 2 hours
5 - 2 hours
Respondents: from 18 years old
Selection: 1645 residents of six regions of Russia and 262 patients with mental illness
Buy
MMPI - 2 (Minnesota Multidisciplinary Personality Inventory. Version 2) is a multiscale test designed for in-depth diagnostics of the psychological characteristics of the personality of adults. This version of the test is based on the MMPI questionnaire (1941), which for fifty years has been considered the best clinically oriented test. Significant changes have been made in the MMPI-2 version, new indicators and scales have been added, and the way in which raw scores are converted to a standard indicator has been revised. The MMPI-2 has been significantly improved to eliminate ambiguous diagnostic scores and the impact of gender differences.
MMPI-2 is one of the most widely used questionnaires in clinical and forensic psychiatry. It is designed for use by psychiatrists, psychologists, forensic scientists, counseling lawyers, prosecutors and judges.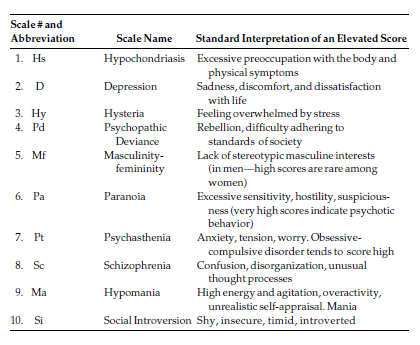 This is due to the fact that MMPI-2 is able to verify the perpetrators of a crime, serial killers, pedophiles, drug addicts, etc. nine0007
This is due to the fact that MMPI-2 is able to verify the perpetrators of a crime, serial killers, pedophiles, drug addicts, etc. nine0007
The questionnaire can be freely used both individually and in a group. The technique allows to identify traits and types of character with a high degree of reliability, to determine the style of behavior and communication, to diagnose the ability to adapt and hidden mental deviations, to assess professional suitability, to study the emotional state and severity of stress, to predict the likelihood and content of difficulties in various types of labor activity.
Structure
The questionnaire consists of 567 questions with dichotomous answers (yes/no). The questions are: eight validity scales, ten basic scales, sixteen additional scales, fifteen content scales, five PSY-5 scales, 27 subscales related to content scales, 28 scales, 3 subscales of SI (social introversion), Harris-Lingoes subscales.
Application
- individual and family counseling;
- mass studies of certain groups of the population; nine0048
- career guidance, personnel recruiting, correction of industrial relations;
- examination of psychological status and monitoring of the state of mental processes;
- psychological assessment of various types of correction and treatment;
- scientific research.
Requirements for specialists
To use this technique, you must meet the following qualification requirements: a diploma (specialty; master's degree; scientific degree) in one of the following specialties: psychology, clinical psychology, medicine (neurology, psychiatry). nine0007
What do the clinical scales of the MMPI questionnaire (MMPI) assess?
Alex B. Caldwell
Caldwell Report, Los Angeles, Department of Psychology and Psychiatry, University of California
Lecture delivered at the Personality Assessment Society Conference March 24, 2000, Albuquerque, New Mexico. (abridged) // JOURNAL OF PERSONALITY ASSESSMENT, - 2001. - 76(1), 1-17
©2021. A. Demkin, translated from English (abridged)
About the Author
Alex B. Caldwell, Ph.D. is a world-renowned leader in the interpretation of the MMPI-2 test. His analysis of the MMPI-2 test results presented in Caldwell Reports is unique in its sensitivity to a wide range of questions and in the specificity of the behaviors described.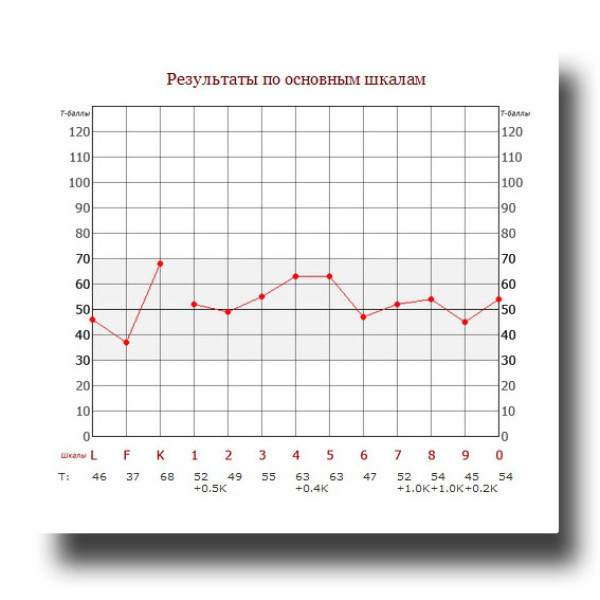 Dr. Caldwell has always considered it a privilege to study at the University of Minnesota. Dr. Stark R. Hathaway was Dr. Caldwell's advisor, mentor, and friend. nine0007
Dr. Caldwell has always considered it a privilege to study at the University of Minnesota. Dr. Stark R. Hathaway was Dr. Caldwell's advisor, mentor, and friend. nine0007
Dr. Caldwell completed his PhD in 1958. In 1959, he joined the faculty of the University of California at Los Angeles in the department of psychiatry, and subsequently received an appointment to the department of psychology. He retired as clinical professor from both UCLA departments in 1997.
Dr. Caldwell began developing one of the first computerized MMPI interpretation programs in the late 1960s. With over 40,000 lines of code and associated algorithms, this expertly crafted program is based on countless case studies and research literature, as well as Dr. Caldwell's extensive clinical experience. It is constantly being improved and updated. nine0007
The resulting program determines personality characteristics and predictions based on MMPI-2 profiles, far beyond the predictive ability of the most experienced clinician.
Recognized by fellow psychologists for his contributions to MMPI and MMPI-2 interpretation and scholarship, Dr. Caldwell was awarded the California Psychological Association's 1991 Distinguished Scientific Achievement Award. He received the "Outstanding Contribution to the Profession of Clinical Psychology" award from the Society of Clinical Psychologists at 1999 year. In 1999, he was recognized by the Wisconsin Foundation for Psychology with his first Wisconsin Psychology Improvement Award. In 2003, the Personality Assessment Society honored Dr. Caldwell with the Bruno Klopfer Award for his "outstanding long-term professional contribution to the field of personality assessment".
Dr. Caldwell is the author of MMPI/MMPI-2 Forensic Questions and Answers. Created for use by lawyers and forensic psychologists, the question and answer format has been especially well received for its direct practical application in forensic science. nine0007
What do the MMPI clinical scores measure?
Some hypotheses.
 Lecture.
Lecture. I am considering whether all psychopathological behavior can be considered on an evolutionary basis as a positive adaptation. I suggested that the higher functions could be differentiated from their associated emotional modulations at the simultaneous subjective, behavioral, and neural levels, and that organizing the analysis in this way would allow us to add to the understanding of both the consequences and the relief of traumatic experiences. I represent each of the 8 clinical MMPI scales (Hathaway & McKinley, 1943) as a measure of positive adaptation with simultaneous cognitive-emotional, operant-classical and neocortical-limbic elements. Various life experience paradigms are then proposed to explain the factors that influence increases in MMPI scores (MMPI in Russian), as well as countermeasures that may help reduce such score rises. Understanding all such behavior as adaptive leads to a marked increase in empathy for clients and patients. nine0094
I'd like to start with what seemed to be the only question Stark Hathaway asked from time to time 50 years ago. His question was: "Can all behavior be considered adaptive?" By now, the concept of evolutionary adaptation has almost completely embraced all areas of biology, especially as structure and function maximize an organism's ability to survive. Psychology has only recently begun to pay much attention to the application of evolutionary logic, and this has often been little more than a lip service to the idea that we should think more in evolutionary terms than before. nine0007
His question was: "Can all behavior be considered adaptive?" By now, the concept of evolutionary adaptation has almost completely embraced all areas of biology, especially as structure and function maximize an organism's ability to survive. Psychology has only recently begun to pay much attention to the application of evolutionary logic, and this has often been little more than a lip service to the idea that we should think more in evolutionary terms than before. nine0007
Intuitively, the evolutionary answer to Stark's question, of course, can only be yes. Everything in us has evolved to adapt to something. In biology, the theory of evolution constantly leads to questions about how the particular organism under study has changed to adapt to changing circumstances: its behavior, its ability to reproduce, its genetics, its physiological responses to extreme circumstances. Evolution is both an explanatory frame of reference and a guide to several lines of biological research. nine0007
nine0007
But when and where were questions asked about "adapting to what in psychopathology? The word 'evolution' is rarely more than an oblique allusion in the Journal of Abnormal Psychology or any clinical or psychopathologically oriented journal I can find.
I think that our fixation on terms like "maladaptation" got in the way. , a less pejorative term, but still with a distinctly "maladaptive" connotation. I would like to consider what might follow if we finally accept the relentlessness of evolutionary logic and insist on finding positive answers to Stark's question in the dimensions of psychopathology.
SUBJECTIVE / LEARNING / NEURAL BASIS
Before setting out my main set of hypotheses, I need to digress for a moment from what I consider to be a long-term and vital limitation in our attempts to apply learning theory to psychopathology, a task so wonderfully begun by Dollard and Miller in 1950, but which lacks diagnostic specificity in many respects (for example, all have ambivalent approach-avoidance conflicts).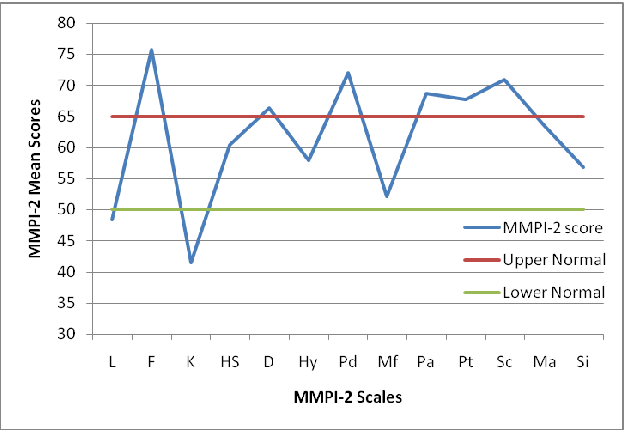 The key problem, in my opinion, is the overwhelming emphasis of our "Western" thinking on operant learning. Although emotional concepts continue to intrude into the formulations of cognitive therapy—for example, rational-emotional therapy—it so often seems that greater cognitive control over our emotional responses, or at least the reduction and management of problematic maladaptive emotions, is a central goal for many therapeutic interventions. . That is, a person needs help in making better operant decisions. nine0007
The key problem, in my opinion, is the overwhelming emphasis of our "Western" thinking on operant learning. Although emotional concepts continue to intrude into the formulations of cognitive therapy—for example, rational-emotional therapy—it so often seems that greater cognitive control over our emotional responses, or at least the reduction and management of problematic maladaptive emotions, is a central goal for many therapeutic interventions. . That is, a person needs help in making better operant decisions. nine0007
An important part of my argument, which I set out in an article almost never read in the comments section of The American Psychologist (Caldwell, A., 1994), is that all psychological responses simultaneously include both operant and classical ( or reflexively) conditioned components. In fact, I think that this is how the structure of the central nervous system works: that is, cortical neural networks are organized to reproduce complex images, to develop chains of verbal meaning, to represent sequences of possible options, and so on.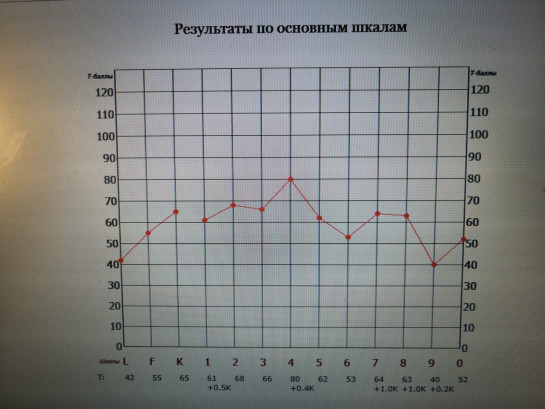 Often the columnar organization of parts of the limbic system is coordinated to simultaneously provide emotional coloring and its regulated intensity associated with any images processed cortically. nine0007
Often the columnar organization of parts of the limbic system is coordinated to simultaneously provide emotional coloring and its regulated intensity associated with any images processed cortically. nine0007
The point of all this is that we have too easily dismissed classical or Pavlovian conditioning as merely reflexive and therefore secondary; we saw it as less interesting, if not almost trivial - a kind of baroque bass continuo repeating very simple melodies. In fact, each individual reaction of the central nervous system simultaneously includes both complex images and emotional coloring, both cortical and limbic excitation, as well as both operant and classically conditioned components. Cortical and subcortical structures are closely interconnected; neither can ever be significantly activated in the absence of excitation in the other. Operant-classical differentiation is very important in our research projects (for example, the application of one or the other paradigm is used in almost every study in the Journal of Behavioral Neuroscience), but despite the special focus of research, one or the other is never one or the other.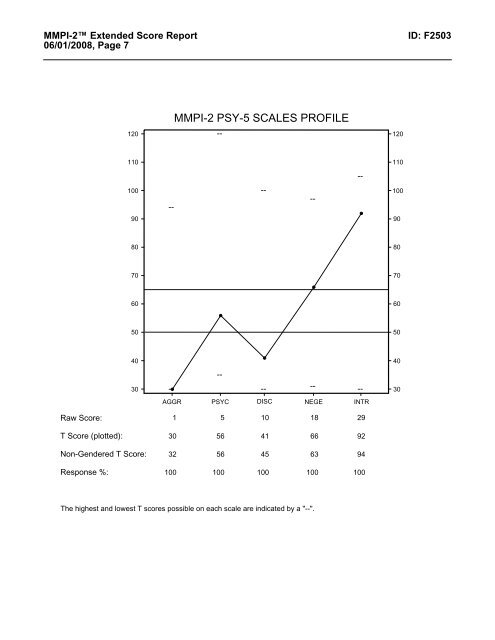 how our brain works. nine0007
how our brain works. nine0007
Within the Ladder of Development concept, each level largely explains the next higher level. What is particularly lacking, and what is central to this lecture, are the limitations of our current understanding of emotion conditioning and especially the formation of psychopathology on both operant and classically conditioned grounds. Our understanding of how subjective awareness is coordinated with simultaneous operant and classical influences is in great need of development. The conditioning of emotional arousal is essentially carried out by continuous association, and it is not voluntary, even if our cerebral cortex functions effectively under operant restrictions. Our emotional feelings are the subjective, limbic component of every response, but we do not control our emotional states. We can consciously arouse or suppress our emotions only to a limited extent through biofeedback, and then only when the emotional stimuli are not overwhelming. The point here is that learning and arousal decay effectively follow the classical constraints of conditioning, even if the cerebral cortex is simultaneously subject to operant learning and voluntary decision making.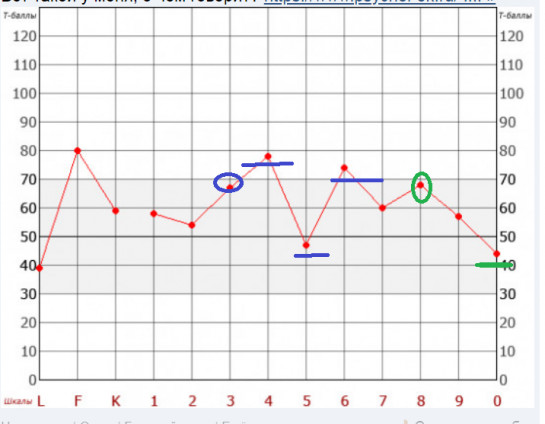 Sometimes it may well be necessary to repeat in therapy an accurate and already clarified cognition in order to attenuate or significantly extinguish the related component of emotional reactive limbic arousal. The most powerful and fear-inducing images must be identified and expressed explicitly or otherwise suppressed. Perhaps disturbances in affective/reactive/limbic arousal during voluntary focusing on maximally repulsive images would help explain the effect of eye movement desensitization (EMDR). nine0007
Sometimes it may well be necessary to repeat in therapy an accurate and already clarified cognition in order to attenuate or significantly extinguish the related component of emotional reactive limbic arousal. The most powerful and fear-inducing images must be identified and expressed explicitly or otherwise suppressed. Perhaps disturbances in affective/reactive/limbic arousal during voluntary focusing on maximally repulsive images would help explain the effect of eye movement desensitization (EMDR). nine0007
Now, with these seemingly distracting but, I believe, vital concepts in mind, let's consider the formation of psychopathological manifestations as an adaptive response.
I am well aware that my thinking has been greatly influenced by my almost 50 years of dedication to the Minnesota Multiphasic Personality Inventory MMPI (Hathaway & McKinley, 1943). Therefore, I am sure that, to everyone's surprise, I am starting from the model of personality described by MMPI as a starting point.