Can wellbutrin make you nauseous
A Complete Guide to Bupropion (Wellbutrin, Zyban) Side Effects
Sold under the brand name Wellbutrin®, bupropion is a medication that’s commonly prescribed in the treatment of depression. Sold under the brand name Wellbutrin XL®, it’s also used to treat seasonal affective disorder (SAD) and, when sold as Zyban®, as a medication to help people quit smoking.
Although bupropion is less likely to cause certain side effects than other antidepressants, there are still numerous side effects that you should be aware of if you currently use bupropion or are considering this medication.
Below, we’ve listed the side effects you may experience while using bupropion, with information on how frequently each side effect occurs, what you can do to manage it and your best options if any particular side effect persists.
Common Bupropion (Wellbutrin, Zyban) Side EffectsBupropion is an antidepressant medication used to help treat the symptoms of depression. Its most common side effects are similar to those of many other medications prescribed to treat depression. As with other antidepressants, most side effects that are associated with bupropion occur in the first few weeks of treatment and go away over time.
Common side effects of bupropion include:
Agitation
Dry mouth
Insomnia
Headache or migraine
Nausea and vomiting
Constipation
Tremor
Dizziness
Excessive sweating
Blurred vision
Tachycardia
Confusion
Rash
Hostility
Cardiac arrhythmia (irregular heartbeat)
Weight loss
Auditory disturbance
Of these, the most common side effects reported in clinical trials of bupropion were constipation, dizziness, dry mouth, headaches/migraines, nausea/vomiting, excessive sweating, agitation and tremor, which were all reported by more than 20 percent of users.
AgitationAgitation was the most common side effect reported in clinical trials of Wellbutrin, a medication containing bupropion prescribed to treat major depressive disorder (MDD) and seasonal affective disorder. According to data from the FDA, 31.9 percent of people reported agitation while using bupropion.
According to data from the FDA, 31.9 percent of people reported agitation while using bupropion.
Other side effects associated with agitation include insomnia, which affected about 18 percent of bupropion users in clinical trials.
If you feel agitated after using bupropion and don’t notice this side effect improving in the first few weeks of treatment, talk to your healthcare provider. They may adjust your bupropion dosage or recommend other changes to manage this side effect.
Try to exercise regularly. Other techniques that may help include deep-breathing exercises and yoga. If you continue to feel agitated while using bupropion, you may also want to talk to your healthcare provider about using medication to help you relax or switching to a different antidepressant.
If you find it difficult to sleep after taking bupropion, avoid taking your medication close to your bedtime. Using bupropion earlier in the day will mean that a lower dose of the medication will be in your bloodstream at bedtime, which may make it easier for you to fall asleep.
And vice versa, if you find yourself saying, “Boy, Wellbutrin makes me tired” it may be worth talking to your healthcare provider about taking it at night, closer to bedtime.
Dry MouthBupropion and other antidepressants may cause xerostomia, or dry mouth. This side effect was reported by 27.6 percent of people who were prescribed bupropion in clinical trials, making it the second-most common side effect after agitation.
Dry mouth is a common side effect of many antidepressants, not only bupropion. It may be due to changes in your salivary glands caused by the medication. This side effect is generally more common with older antidepressants, such as tricyclic antidepressants (TCAs).
If you get dry mouth while using bupropion that doesn’t improve over the course of a few weeks, it’s best to talk to your healthcare provider. You can also try chewing sugarless or CPP-ACP gum to stimulate saliva production, which may help to loosen mucus and keep your mouth moist.
online counseling
the best way to try counseling
Headache/MigraineHeadaches and migraines are a fairly common side effect of bupropion, affecting 25.7 percent of people in clinical trials (versus 22.2 percent of people given a non-therapeutic placebo).
Like dry mouth, headaches are a common side effect of antidepressants. Interestingly, a 2012 study found that headaches were less common in bupropion users than in people prescribed SSRIs and other antidepressants.
As with other side effects of bupropion, your headaches may become less severe or go away completely as your body gets used to the medication. If you get persistent headaches, it’s best to talk to your healthcare provider.
Nausea/VomitingNausea and vomiting are common side effects of bupropion, reported by 22.9 percent of people in clinical trials.
As with many other side effects of bupropion, nausea and vomiting are common side effects of many antidepressants. Nausea caused by bupropion may get better or disappear completely over time as you become more used to the effects of the medication.
Nausea caused by bupropion may get better or disappear completely over time as you become more used to the effects of the medication.
If you often feel nauseous after using bupropion, try to take your medication with food, eat small and frequent meals and make sure that you stay hydrated. You can also try an over-the-counter antacid such as Pepto-Bismol® to provide temporary relief.
If you have persistent nausea or vomiting that doesn’t get better over time or with treatment, it’s best to talk to your healthcare provider.
ConstipationAccording to clinical trial data, 26 percent of people who use bupropion experience constipation as a side effect.
Like many other side effects of bupropion, constipation is a common side effect of medications used to treat major depression or the symptoms of depression. It’s particularly common with older antidepressants such as tricyclic antidepressants, as these medications can affect digestive function.
If you feel constipated after using bupropion or are experiencing Wellbutrin stomach pain, try increasing your intake of fiber-rich foods or use an over-the-counter fiber supplement. Other techniques that may help include drinking plenty of water and exercising regularly.
Other techniques that may help include drinking plenty of water and exercising regularly.
If you have severe, persistent or painful constipation after you start using bupropion, talk to your healthcare provider. They may recommend a non-prescription stool softener such as docusate sodium to ease your symptoms and make going to the toilet easier.
DizzinessDizziness is a relatively common side effect of bupropion, reported by 22.3 percent of people in clinical trials.
In addition to bupropion, several other antidepressants can cause dizziness. You may feel dizzy when you first start taking bupropion, or notice occasional dizziness when you stand up from a seated position or make other sudden movements.
To avoid dizziness, try avoiding caffeine, tobacco and alcohol while you use bupropion or other antidepressants. It can also help to avoid driving or operating machinery and practice standing up slowly when you need to get up. If necessary, you can use other items for support.
If you feel dizzy during the daytime, you can also talk to your healthcare provider about taking Wellbutrin at night, which may help to reduce the severity of this side effect.
Excessive SweatingAnother relatively common side effect of bupropion users, 22.3 percent of people in clinical trials experienced excessive sweating — a significantly larger percentage than those given a non-therapeutic placebo.
Sweating is a common side effect of antidepressants. It’s referred to as antidepressant-induced excessive sweating, or ADIES, and is estimated to affect between four and 22 percent of people who use antidepressants overall.
Excessive sweating from antidepressants usually affects the scalp, face, neck and chest areas, with symptoms often developing in bursts.
If you notice yourself sweating excessively or uncomfortably after you start using bupropion, it’s best to talk to your healthcare provider. They may prescribe medication to treat the sweating or switch you to new antidepressant or different dosage of bupropion.
Tremors — involuntary muscle contractions that usually affect your hands, limbs, head, face or eyes — is a common side effect of bupropion, affecting 21.1 percent of people in clinical trials.
Like other bupropion side effects, tremor is a common side effect of antidepressants, including selective serotonin reuptake inhibitors (SSRIs) and tricyclic antidepressants. It’s referred to as drug or medication-induced tremor (MIT) and can also occur with other medications.
If you get tremors after you start using bupropion, talk to your healthcare provider. Medication-induced tremors as usually treated by ending treatment with the medication that causes the tremors. They may also recommend adjusting your dosage or using a different type of antidepressant.
Bupropion and Sexual Side EffectsAntidepressants are often associated with sexual side effects, such as decreased sexual desire, erection problems, reduced sexual excitement and difficulty ejaculating.
These adverse effects are a particularly common occurrence in people who use selective serotonin reuptake inhibitors (SSRIs) and serotonin norepinephrine reuptake inhibitors (SNRIs).
In a 2000 article, researchers found that 30 to 40 percent of patients prescribed antidepressants developed some degree of sexual dysfunction. Other research has found that between 25 and 73 percent of SSRI and SNRI users reported sexual side effects.
Interestingly, although some bupropion users report experiencing a decrease in sexual function, research tends to show that bupropion is less likely to cause sexual side effects than other antidepressants, and may even help to reverse antidepressant-related sexual issues.
In a 2008 review, researchers noted there’s robust evidence that bupropion tends to cause less sexual dysfunction than SSRIs.
A separate study from 2004 also found that a sustained-release version of bupropion increased sexual desire and frequency of sexual activity in people with SSRI-induced sexual dysfunction.
In other words, bupropion may not cause the same sexual side effects as other antidepressants, or at least not cause them as often or severely. Still, if you notice any changes in your interest in sex or sexual performance after starting bupropion, it’s best to talk to your healthcare provider.
Bupropion and Changes in Weight
Antidepressants are commonly associated with weight gain. This association is so strong that many people who are prescribed antidepressants stop using them either due to weight gain or concerns about weight gain during treatment.
Although there’s some evidence that you may gain weight after you start using antidepressants, the link isn’t as strong as many people think.
According to a study published in JAMA Psychiatry, most people who use antidepressants only gain a small amount of weight over 12 months — for most medications, an increase of less than one percent of their original, pre-treatment body mass index (BMI).
Unlike other antidepressants, bupropion typically doesn’t cause weight gain. For example, in the study above, the researchers found that people who used bupropion experienced fluctuations of less than 0.25 percent of their original BMI over the course of 12 months of treatment.
For example, in the study above, the researchers found that people who used bupropion experienced fluctuations of less than 0.25 percent of their original BMI over the course of 12 months of treatment.
Clinical trials of bupropion have also found that it typically doesn’t cause weight loss. In trials for Wellbutrin, a popular brand of bupropion, only 9.4 percent of people gained weight compared to 35 percent of people who received tricyclic antidepressants. Additionally, 28 percent of bupropion users actually lost more than five pounds.
Other studies have also found that bupropion causes mild weight loss when used over the long term.
In short, bupropion doesn’t appear to cause weight gain, at least not to the same extent as other common antidepressants. Most studies show the opposite — that bupropion either produces little change in weight or a small amount of weight loss.
Serious Side Effects of BupropionAlthough uncommon, bupropion may cause a range of more serious adverse effects, including adverse reactions that may require medical attention. We’ve listed these below and provided information on each potential side effect, as well as what you can do if you’re affected.
We’ve listed these below and provided information on each potential side effect, as well as what you can do if you’re affected.
Like other types of antidepressant medication, bupropion carries a “black box” warning from the FDA stating that it, as well as other medications in this category, may produce an increased risk of suicidal thoughts and behavior in children, adolescents and young adults.
Clinical trials of antidepressants do not show this risk in people over the age of twenty-four. Despite this, the FDA recommends monitoring for signs of suicidal thoughts or behavior in anyone prescribed an antidepressant.
This warning is common to antidepressants and also appears on the packaging of most SSRIs, SNRIs and other medications prescribed to treat depression and major depressive disorder. A less severe warning is used on the packaging of Zyban, a form of bupropion prescribed for smoking cessation.
If you experience suicidal thoughts, worsened depression or other abnormal thoughts after you start using bupropion, contact your healthcare provider as soon as you can. Call 911 if you think you are having a medical emergency.
Call 911 if you think you are having a medical emergency.
Bupropion may cause seizures. Use of bupropion is associated with seizures in approximately 0.4 percent of people at typical dosages of 450mg or less per day, making this a rare side effect. Seizures are significantly more common at dosages higher than 450mg per day.
The risk of seizures in people using bupropion is dose-related and is typically higher in people with conditions such as bulimia or anorexia, people who have quit using certain drugs or alcohol recently and people affected by seizure disorders.
Other conditions, such as metabolic disorders, head injury, prescription drug use or illegal drug use, may also increase your risk of seizures while using bupropion.
Hypertension (High Blood Pressure)Bupropion may contribute to an increase in blood pressure and hypertension (overly high blood pressure). Your healthcare provider may ask that you monitor your blood pressure periodically while using bupropion to stay aware of any increases or changes.
If you currently have hypertension, or have a history of cardiovascular health issues, your healthcare provider may adjust your dosage of bupropion, recommend careful monitoring of your blood pressure or prescribe a different medication.
Activation of Mania/HypomaniaTreatment with antidepressants such as bupropion is associated with an increased risk of manic and hypomanic episodes, particularly in people who have risk factors for bipolar disorder or who have been diagnosed with bipolar disorder.
Bupropion is currently not approved by the FDA for treating bipolar depression. If you have bipolar disorder or display risk factors for bipolar disorder, your healthcare provider may recommend using another type of medication to treat your symptoms.
Psychosis and Other Neuropsychiatric SymptomsThere have been several reported cases of psychosis and other neuropsychiatric symptoms in patients treated with bupropion for depression. Several of these involved people who had previously used illicit drugs, while others involved patients diagnosed with bipolar disorder.
If you or a loved one experience any delusions, hallucinations, psychosis, paranoia, confusion or concentration disturbance while using bupropion, contact your healthcare provider.
Hypersensitivity ReactionsAlthough rare, bupropion may cause anaphylactoid/anaphylactic reactions. If you develop any symptoms of an allergic reaction, such as hives, skin rash, shortness of breath, edema, pruritus (itchy skin) or chest pain, contact your healthcare provider.
Drug InteractionsBupropion also may interact with other medications in ways that could cause some potential side effects.
If you’ve used monoamine oxidase inhibitors (MAOIs) within 14 days of starting bupropion, tell your healthcare immediately, as these drug interactions may be severe.
Potential drug interactions with bupropion also include other antidepressants like SSRIs, SNRIs and TCAs, as well as medications like antipsychotics, beta-blockers, blood thinners, corticosteroids and others.
As with other antidepressants, bupropion may cause withdrawal symptoms if you abruptly stop taking it as prescribed. This is known as antidepressant discontinuation syndrome, and is a common issue for people who suddenly end their usage of antidepressants.
Bupropion may be less likely to cause severe withdrawal symptoms than other antidepressants, such as SSRIs and SNRIs. However, if you’re prescribed bupropion and want to stop taking it, it’s still important to talk to your healthcare provider first.
To reduce your risk of experiencing bupropion withdrawal symptoms, your healthcare provider may recommend tapering your dosage gradually over time. We’ve explained this in more detail in our guide to bupropion withdrawal.
online psychiatrist prescriptions
talk to a psychiatry provider. it’s never been easier
Learn More About BupropionBupropion can help in the treatment of depression and make it easier for you to deal with nicotine cravings while quitting smoking. Our full guide to bupropion goes into more detail on how this medication works, common dosages, frequently asked questions and more.
Our full guide to bupropion goes into more detail on how this medication works, common dosages, frequently asked questions and more.
This article is for informational purposes only and does not constitute medical advice. The information contained herein is not a substitute for and should never be relied upon for professional medical advice. Always talk to your doctor about the risks and benefits of any treatment. Learn more about our editorial standards here.
Wellbutrin side effects and how to avoid them
Wellbutrin treats major depressive disorder (MDD), seasonal affective disorder (SAD), and assists with smoking cessation
Wellbutrin side effects | Serious side effects | Suicide | Angle-closure glaucoma | Neuropsychiatric events | Weight loss | How long do side effects last? | Warnings | Interactions | How to avoid side effects
Wellbutrin (bupropion hydrochloride) is a brand-name prescription drug used for the treatment of major depressive disorder (MDD), the prevention of seasonal affective disorder (SAD), and smoking cessation, in addition to several off-label uses. As an antidepressant medication, Wellbutrin works by increasing the amount of norepinephrine and dopamine in the brain. These substances are neurotransmitters that are involved with regulating mood, emotions, memory, and motivation, and by increasing the levels of these neurotransmitters, Wellbutrin can help manage mental health conditions.
As an antidepressant medication, Wellbutrin works by increasing the amount of norepinephrine and dopamine in the brain. These substances are neurotransmitters that are involved with regulating mood, emotions, memory, and motivation, and by increasing the levels of these neurotransmitters, Wellbutrin can help manage mental health conditions.
Brand-name Wellbutrin is available as a sustained-release (Wellbutrin SR) or extended-release (Wellbutrin XL) tablet, and generic Wellbutrin is available as an immediate-release tablet in addition to a sustained- or extended-release tablet. Bupropion might also be sold under other brand names including Forfivo XL and Aplenzin (bupropion hydrobromide), as well as Zyban, which has recently been discontinued. Although Wellbutrin works differently than other antidepressants, it does have side effects and may not be suitable for some people with pre-existing medical conditions.
RELATED: What is Wellbutrin?
Common side effects of Wellbutrin
The most common side effects of Wellbutrin are:
- Trouble sleeping
- Headache
- Agitation
- Dry mouth
- Constipation
- Weight loss or weight gain
- Migraine
- Nausea
- Vomiting
- Excessive sweating
- Tremor
- Dizziness
- Blurred vision
- Fast heartbeat
- Joint aches
- Sore throat
Serious side effects of Wellbutrin
Possible side effects of Wellbutrin that can be serious or even life-threatening include:
- Worsened depression
- Suicidal thoughts and behaviors
- Homicidal thoughts
- Neuropsychiatric events (psychosis, mania, hallucinations, and panic attacks)
- Seizures
- Severe high blood pressure (hypertension)
- Heart problems, including irregular heartbeat
- Angle-closure glaucoma
- Liver problems
- Visual problems, such as changes in vision
- Severe allergic reactions
Wellbutrin and suicide
Wellbutrin has a black box warning that highlights a risk of worsening depression and suicidal thoughts or behaviors in children, teens, and young adults. The incidence of these adverse effects is between 0.1% and 1%, although older adults are at a lower risk of this effect. Patients and caregivers should watch behavior and mood closely and call a healthcare provider at any signs of suicidality, such as:
The incidence of these adverse effects is between 0.1% and 1%, although older adults are at a lower risk of this effect. Patients and caregivers should watch behavior and mood closely and call a healthcare provider at any signs of suicidality, such as:
- Talks of suicide or dying
- Suicide attempts
- New or worsened depression, anxiety, or irritability
- Agitation and restlessness
- Extreme dietary changes
- Irritability
- Trouble sleeping
- Increased use of illicit substances or alcohol
- Unusual, aggressive, or violent behaviors
- Isolation from friends and family
Wellbutrin and angle-closure glaucoma
Angle-closure glaucoma is a medical emergency that comes on suddenly when the opening, or angle, between the iris and the cornea is blocked, causing fluid pressure to build up rapidly in the eye. This opening allows fluid to drain from the eye, but people with uncorrected “narrow angles” between the iris and the cornea are particularly vulnerable to closure. Because angle-closure glaucoma can rapidly develop into permanent vision loss, you should immediately stop taking Wellbutrin and go to an emergency room at any sign of angle-closure glaucoma, such as:
This opening allows fluid to drain from the eye, but people with uncorrected “narrow angles” between the iris and the cornea are particularly vulnerable to closure. Because angle-closure glaucoma can rapidly develop into permanent vision loss, you should immediately stop taking Wellbutrin and go to an emergency room at any sign of angle-closure glaucoma, such as:
- Eye pain
- Changes in vision
- Swelling or redness in or around the eye
Wellbutrin and neuropsychiatric events
When taken for smoking cessation, Wellbutrin has been reported to cause neuropsychiatric events, such as depression, anxiety, panic attacks, hostility, and even psychosis or hallucinations. The risk of experiencing these events can vary, but people with a history of mental health problems may be at a high risk of experiencing these events. Patients and caregivers should monitor behaviors and mood closely and call a healthcare provider at any sign of psychiatric problems.
Wellbutrin and weight loss
Weight loss is a common side effect of Wellbutrin, affecting 14% to 23% of people who take the medication. Anorexia—loss of appetite—is also commonly experienced, with an incidence between 1% and 18%. For this reason, some healthcare professionals may prescribe bupropion off-label for weight loss or weight loss maintenance, while others consider it the antidepressant of choice for patients diagnosed with both depression and obesity. The U.S. Food and Drug Administration (FDA) has approved at least one bupropion drug for weight loss: Contrave, a combination of bupropion and naltrexone, a drug normally used to treat opioid or alcohol abuse.
How long do side effects last?
With a half-life of 14 hours when taken as a single dose and 21 hours when taken on a consistent basis, bupropion and its active metabolites can remain in the body for three or four days. However, side effects are usually mild and temporary. Side effects of bupropion can last a couple of days or weeks as the body gets used to the drug. Consult a healthcare provider if side effects last longer than two to three weeks, or if side effects are particularly bothersome or severe.
Consult a healthcare provider if side effects last longer than two to three weeks, or if side effects are particularly bothersome or severe.
Some side effects may take longer to resolve or require medical attention. Serious adverse effects, such as severe allergic reactions, angle-closure glaucoma, irregular heartbeat, heart attack, seizures, severe high blood pressure, and severely low blood sodium levels will require medical attention. Some of these side effects, such as angle-closure glaucoma or heart attack, may have lifelong complications.
Suicidality, worsening of depression, mood changes, mania, hostility, and other neuropsychiatric events can occur with the use of bupropion. In many cases, Wellbutrin will be discontinued. However, these symptoms may be due to pre-existing mental health problems, so long-term psychiatric treatment for other mental health problems may be recommended.
Wellbutrin contraindications & warnings
Wellbutrin affects the brain and body in different ways, and it can cause problems in people with a variety of pre-existing conditions.
Abuse and dependence
The U.S. Food and Drug Administration (FDA) does not consider Wellbutrin a drug that can cause physical dependence, abuse, or tolerance. However, Wellbutrin can produce a mild amphetamine-like reaction. For this reason, Wellbutrin is commonly abused as a street drug and sometimes referred to as “the poor man’s cocaine.” This medication also carries a risk for psychological dependence, but the most serious problems are side effects, particularly seizures, when people abuse bupropion by snorting the drug, injecting the drug, or taking it in large doses.
Overdose
A Wellbutrin overdose is potentially serious and will often require medical attention. The most common side effect of a Wellbutrin overdose is seizures, but other symptoms include:
- Hallucinations
- Loss of consciousness
- Fast heartbeat
- Irregular heartbeat
- Overactive reflexes
- Convulsions
When taken in excessive amounts in combination with other drugs, Wellbutrin may also cause fever, muscle rigidity, low blood pressure, stupor, coma, and respiratory failure.
Restrictions
Some medical conditions make taking Wellbutrin too hazardous:
- Anyone with allergies to bupropion will not be prescribed Wellbutrin.
- Because of an increased risk of seizures, Wellbutrin is never given to people with a history of seizures, a prior diagnosis of an eating disorder, such as anorexia or bulimia, or anyone undergoing abrupt withdrawal from alcohol, barbiturates, benzodiazepines, or antiepileptic medications.
Other pre-existing conditions may cause problems, so healthcare providers will prescribe Wellbutrin cautiously and watch carefully for side effects.
- Because of the increased risk of suicidal thoughts and behaviors, people younger than the age of 25 should be carefully watched for signs of worsening depression, unusual behaviors, or thoughts about suicide or dying. Any mood changes, depression, or suicidality need to be reported to the prescribing healthcare professional as soon as they’re noticed.
- Because of an increased risk for seizures, people with risk factors for seizures may need to be carefully monitored. These risk factors include head injury, CNS infection, severe stroke, arteriovenous malformation, and drug or alcohol abuse.
- People with a history of mental health problems will be monitored for neuropsychiatric side effects, particularly when taking Wellbutrin for smoking cessation.
- All antidepressants can provoke mania or hypomania in people with bipolar disorder, so people with bipolar disorder should be closely monitored for behavioral changes.
- People with high blood pressure or a recent heart attack may require close monitoring of blood pressure.
- People who have uncorrected narrow angles are at a higher risk of narrow-angle glaucoma when taking Wellbutrin, so they should watch for and report any eye problems.
- People with Tourette’s syndrome or with a tic disorder may be at risk for new or worsening tics when taking Wellbutrin.
- Wellbutrin may require dose modifications and monitoring in people with liver or kidney problems.
Pregnancy and nursing
There is no evidence that bupropion increases the risk of birth defects, miscarriage, or other problems when taken during pregnancy. Because untreated depression does have pregnancy risks, women should get medical advice from a healthcare professional about the safety and benefits of taking Wellbutrin during pregnancy.
Nursing mothers are advised to be cautious about taking Wellbutrin. Bupropion and its active metabolites are present in breast milk, but healthcare providers are uncertain about its effects on the baby. Before taking Wellbutrin, women who are breastfeeding should talk to a healthcare professional about its benefits and risks.
Children
The Food and Drug Administration (FDA) has not approved bupropion for anyone younger than the age of 18. Some healthcare providers, however, may prescribe Wellbutrin off-label to children as young as 11 years of age, but these children are at an increased risk of worsening depression, suicidal thoughts, and suicidal behaviors.
Some healthcare providers, however, may prescribe Wellbutrin off-label to children as young as 11 years of age, but these children are at an increased risk of worsening depression, suicidal thoughts, and suicidal behaviors.
Seniors
People older than 65 can take Wellbutrin in the same doses as younger adults, but doses may be modified in some older adults if the person has liver or kidney problems.
Wellbutrin interactions
Most Wellbutrin drug interactions are minor, but some are serious enough to require monitoring, dosing changes, or avoiding the drug combination altogether.
Wellbutrin is never combined with some drugs because of the potential hazards. These include:
- MAO inhibitors: Because of the risk for high blood pressure or seizures, Wellbutrin is never taken with monoamine oxidase inhibitors (MAOIs), a small family of drugs that includes the antidepressants isocarboxazid, phenelzine, tranylcypromine, and selegiline.
 Other examples of MAOIs include the cancer drug procarbazine, the antibiotic linezolid, and methylene blue injections.
Other examples of MAOIs include the cancer drug procarbazine, the antibiotic linezolid, and methylene blue injections. - Anti-seizure medications, barbiturates, and benzodiazepines: Because of an increased risk of seizures, treatment with Wellbutrin is not started if these medications have been used excessively or discontinued suddenly.
- Other precautions: Because of the increased risk of serious heart rhythm problems, Wellbutrin is not recommended to be taken with the antipsychotic drugs pimozide or thioridazine.
Some drugs that lower the seizure threshold may need to be avoided. These include:
- Antipsychotics
- Tricyclic antidepressants
- Appetite suppressants
- Certain opioids
- Systemic corticosteroids
- Theophylline
- Stimulants
Bupropion raises dopamine levels in the brain. When combined with similar drugs (dopaminergic drugs), dopamine can rise to toxic levels. So both levodopa and amantadine should be used cautiously with bupropion.
When combined with similar drugs (dopaminergic drugs), dopamine can rise to toxic levels. So both levodopa and amantadine should be used cautiously with bupropion.
Bupropion can block the body’s metabolism of other drugs. As a result, the concentration of other drugs in the body can increase, raising the risk of side effects. Either these drugs must be stopped or the doses must be changed. These include:
- Tricyclic antidepressants
- Selective serotonin reuptake inhibitors (SSRIs)
- Antipsychotics
- Beta blockers
- Certain types of heart rhythm medications
Finally, alcohol mixed with bupropion can provoke neuropsychiatric events. The use of alcohol should be avoided or minimized when taking Wellbutrin.
How to avoid Wellbutrin side effects
1. Take Wellbutrin as directed
Take Wellbutrin as instructed. The typical dose is 300 mg a day. Don’t skip a dose, but if you do, don’t make up that dose. Wait until the next scheduled dose and take that dose as planned.
Wait until the next scheduled dose and take that dose as planned.
2. Tell the healthcare provider about all medical conditions
To avoid potentially serious side effects, tell the prescribing healthcare professional about all medical conditions, especially if you’ve had a history of:
- Eating disorders
- Suicide attempts
- Depression or other mental health problems, such as mania, hypomania, or bipolar disorder
- Heart disease, high blood pressure, or recent heart attack
- Liver problems
- Kidney problems
- Head injuries
- Seizures
- Brain or spinal tumors
- Diabetes
- Alcohol or illicit drug use
- Pregnancy or pregnancy plans
- Breastfeeding or plans to breastfeed
3. Tell the healthcare provider about all medications
Drug interactions can also cause side effects, so tell your healthcare provider about all prescription and over-the-counter medications you take, especially:
- MAO inhibitors
- Anti-seizure medications
- Sedatives
- Benzodiazepines
- Opioids
4.
 Do not drink alcohol
Do not drink alcoholDrinking alcohol when being treated with Wellbutrin can cause neuropsychiatric side effects. Avoid alcohol entirely or drink in moderation according to your doctor’s instructions.
5. Be careful about driving and other risky activities at first
Avoid driving cars or operating machinery for a few days until you’re familiar with Wellbutrin and how it affects your body.
6. Eat a healthy diet
To avoid weight loss or weight gain, eat a healthy diet and carefully monitor weight while taking Wellbutrin. A dietitian or nutritionist may be able to help if appetite and weight changes become a problem while taking this medication.
7. Talk to a healthcare provider before discontinuing Wellbutrin
The sudden discontinuation of Wellbutrin can cause unpleasant withdrawal effects. Seek medical advice if Wellbutrin does not seem to be working or the side effects become hard to manage. Upon discontinuing Wellbutrin, a healthcare provider may recommend tapering, or gradually lowering, the dose to help prevent problems when stopping Wellbutrin.
Related resources for Wellbutrin side effects:
- 15 years of clinical experience with bupropion HCl: from bupropion to bupropion SR to bupropion XL, Primary Care Companion to The Journal of Clinical Psychiatry
- Bupropion compound summary, U.S. National Library of Medicine
- Bupropion drug summary, Prescriber’s Digital Reference
- “Narrow angles” a tip-off to eyesight risk, Harvard Health Publishing
- One antidepressant shown to control weight during a 2-year study, Science Daily
- Wellbutrin SR, Epocrates
- Wellbutrin SR prescribing information, U.S. National Library of Medicine
- What is naltrexone?, UAMS Psychiatric Research Center
All the truth and myths about antidepressants | Health
The chances that antidepressants will become “the best treatment for depression” are only about 30%. Studies have shown that only 30% of those who are clinically depressed respond best to regular exercise. For another 30%, cognitive behavioral therapy is the best treatment. And only the remaining 30% are better treated with antidepressants. But for those 30%, antidepressants can really be a godsend. As for their fast action, then everything is different here. Most antidepressants have a noticeable effect in at least 1-2 weeks. But for the onset of the full effect, doctors ask patients to wait 6 weeks.
Studies have shown that only 30% of those who are clinically depressed respond best to regular exercise. For another 30%, cognitive behavioral therapy is the best treatment. And only the remaining 30% are better treated with antidepressants. But for those 30%, antidepressants can really be a godsend. As for their fast action, then everything is different here. Most antidepressants have a noticeable effect in at least 1-2 weeks. But for the onset of the full effect, doctors ask patients to wait 6 weeks.
Antidepressants are not additives. These are very complex drugs that require careful monitoring by an experienced doctor. Scientists have not yet found a way to make or produce brain hormones called neurotransmitters (eg, serotonin, norepinephrine, dopamine), insulin (to treat diabetes), or thyroxine (to treat hypothyroidism). However, they have found a way to make parts of the brain more sensitive to neurotransmitters that are essential for good mental health. But again, the increase in sensitivity takes time, so it may take 2-6 weeks before you really feel the effect of the drug.
The short answer to this question is no. They won't make you outgoing if you've always been shy, or analytical if you've always been intuitive. Your core self will remain completely unscathed.
Antidepressant chemicals are not addictive. According to the American Society of Addiction Medicine, one of the key components of addiction is the inability to control one's behavior. Antidepressants have no such effect on the brain. In fact, many patients on antidepressants report having greater control over their behavior and life. They feel able to communicate again and be more productive. At the same time, your body may become addicted to a particular drug (this will be seen as a physical addiction rather than a mental one), and decreasing the dosage may cause you to experience certain withdrawal side effects. Therefore, it is very important to gradually reduce the dose, sometimes over several weeks. Sudden withdrawal may cause some unpleasant but temporary symptoms such as nausea, diarrhea, headache, and other flu-like symptoms.
People who suffer from multiple bouts of depression but are relieved by antidepressants usually have to stay in treatment indefinitely. So yes, some people choose to take antidepressants for decades. But the vast majority of people continue to take them for only a few months after going into remission.
Many of these drugs affect the sexual function of some people, especially at the beginning of therapy. In certain cases, antidepressants can cause erectile dysfunction and make it harder to experience orgasm, even if you've only been taking them for a short time. Fortunately, the percentage of people who experience this side effect is quite low. If you experience these symptoms, talk to your doctor about it. The solution to the problem can be as simple as, for example, changing the drug.
Certain antidepressants cause changes in appetite in some people. For example, nortriptyline or fluoxetine (Prozac) can increase it, while bupropion (also known as Wellbutrin) often lowers it. Since one side of the influence of moderate and severe cases of depression is weight loss, this may not be so bad. But, as a rule, antidepressants by themselves do not increase weight. However, if you are already overweight or have a medical condition that gets worse with weight gain (such as diabetes, orthopedic problems, or heart disease), it is recommended that you engage in physical activity before taking antidepressants, such as going to the gym, cycling, swimming, or take yoga lessons. Perhaps your case is in the 30% whose depression can be alleviated with exercise. Regular moderate exercise increases brain oxygenation, releasing healthy hormones, improving self-esteem and improving mood.
Since one side of the influence of moderate and severe cases of depression is weight loss, this may not be so bad. But, as a rule, antidepressants by themselves do not increase weight. However, if you are already overweight or have a medical condition that gets worse with weight gain (such as diabetes, orthopedic problems, or heart disease), it is recommended that you engage in physical activity before taking antidepressants, such as going to the gym, cycling, swimming, or take yoga lessons. Perhaps your case is in the 30% whose depression can be alleviated with exercise. Regular moderate exercise increases brain oxygenation, releasing healthy hormones, improving self-esteem and improving mood.
Quite the contrary. Clinical depression can be so painful that emotions disappear, leaving the person in a blunted state. When depression begins to recede (under the influence of any kind of treatment), people often find that they feel alive again and see the world in bright colors, and not as it used to be gray.
Far from it. For example, depression caused by bipolar disorder (formerly known as manic depression) must be treated with a very different class of medications (such as mood stabilizers or antipsychotics) than those used to treat major depression. Antidepressants can actually induce psychotic episodes in patients with bipolar disorder. Loss-related depression (divorce, death of a family member, job loss, etc.) is usually best treated with support groups or individual medication (cognitive behavioral therapy).
Depression is not like an infection, and antidepressants are nothing like antibiotics. This myth probably comes from the tendency of society to take medication instead of putting in some effort to get rid of the problem. Back pain is treated with muscle relaxants instead of strengthening and stretching exercises. Headaches are drowned out by vasoconstrictors and anti-inflammatory drugs instead of meditation and proper diet. Depression is much more difficult than most people think. There is a long list of stressors that can cause depression, and most of the time there is more than one. Medicines can be a good boost, but they are not enough to get a person out of depression.
There is a long list of stressors that can cause depression, and most of the time there is more than one. Medicines can be a good boost, but they are not enough to get a person out of depression.
Most doctors recommend taking antidepressants for at least 6 months to allow the brain to adjust to the higher levels of sensitivity. Also, as mentioned earlier, stopping antidepressants prematurely can lead to recurrence of symptoms.
Yes, antidepressants can cause unpleasant side effects in some people, but according to the patients themselves, they are much easier than depression. For example, in some cases, antidepressants can cause or increase suicidal thoughts, make dreams more vivid, sometimes even very realistic. Side effects of tricyclics (TCAs) are typically associated with dry mouth, nose, dry skin, blurred vision, urinary problems, weight gain, drowsiness, and constipation. Selective serotonin reuptake inhibitors (SSRIs) sometimes cause anxiety, irritability, nervousness, confusion, headache, decreased sexual desire, insomnia, weight changes, diarrhea, and nausea. But it's also true that many people don't have any side effects at all. It is impossible to predict in advance whether you will experience side effects, and if so, what they will be.
But it's also true that many people don't have any side effects at all. It is impossible to predict in advance whether you will experience side effects, and if so, what they will be.
There are 29 different antidepressant formulations on the market that fall under one of seven drug classes: Aminoketones, MAO inhibitors, selective norepinephrine and dopamine reuptake inhibitors, selective serotonin and norepinephrine reuptake inhibitors, selective serotonin reuptake inhibitors, tricyclic antidepressants, tetracyclic antidepressants. Each class of drugs affects the brain differently, and drugs within the same class have chemical differences. For example, citalopram (Celexa) and escitalopram (Lexapro) are both SSRIs and are chemically very similar, yet people react differently to each. Many patients who have tried both find that one is more effective while the other has little to no effect. It is impossible to predict how each person's brain will react to a particular antidepressant.
How to identify and treat a depressive disorder? Diagnosis of depressive disorder
Close people, relatives of patients often confuse depression with a bad mood, laziness - apathy, lethargy, tearfulness, a bleak state of a person is perceived as a temporary disorder, strangeness. Depression is actually a disease that can last for years and develop into psychosis or lead to suicide. Depressive disorder requires increased attention and good treatment.
Submit an application for diagnosis and treatment
I confirm that I accept the terms of consent to the processing of personal data.
Signs of depression can be easily identified by a specialist, but the surrounding patients often mistake them for laziness and bad mood, which will pass by itself. However, in reality, everything is not so simple - in the absence of medical help, depression can easily end in suicide. Women, men, the elderly and even children are susceptible to depression. Diagnosis of the disease is carried out during a conversation between the doctor and the patient, additional diagnostic techniques. Treatment (in severe cases) may consist in prescribing various antidepressants or in the selection of their combinations.
Diagnosis of the disease is carried out during a conversation between the doctor and the patient, additional diagnostic techniques. Treatment (in severe cases) may consist in prescribing various antidepressants or in the selection of their combinations.
How to identify and treat a depressive disorder?
Depression is an illness that involves the body, mood and thoughts. Depression affects how a person eats and sleeps, how a person feels about themselves, and how they think about things. Depression is not the same as going through a bad mood. This is not a sign of personal weakness or a condition that can be willed or brushed aside. People with depression can't just "pull themselves together" and get better. Without treatment for depression, symptoms of depression can last for weeks, months, or years. Appropriate treatment for depression, however, can help most people who suffer from depression.
Depression types
Depression comes in various forms, just as it does with other illnesses such as heart disease. This booklet provides a brief description of the three most common types of depression. However, in these types of depression there are variations in the number of signs of depression, their severity, and persistence. Depression is manifested by a combination of symptoms of depression (see symptom list) that affects the ability to work, study, sleep, eat, and enjoy one day's enjoyable activities. Such a disabling episode of depression may only occur once, but usually occurs several times in a lifetime. A less serious type of depression, dysthymia, includes long-term, chronic symptoms of depression that don't turn off but keep one from functioning well or feeling good. Many people with dysthymia also experience major depressive episodes at some time in their lives. Another depression type is bipolar disorder, also called manic depressive illness. Not quite as acute as other forms of depressive disorders, bipolar disorder is characterized by cycling mood changes: severe highs (mania) and lows (depression).
This booklet provides a brief description of the three most common types of depression. However, in these types of depression there are variations in the number of signs of depression, their severity, and persistence. Depression is manifested by a combination of symptoms of depression (see symptom list) that affects the ability to work, study, sleep, eat, and enjoy one day's enjoyable activities. Such a disabling episode of depression may only occur once, but usually occurs several times in a lifetime. A less serious type of depression, dysthymia, includes long-term, chronic symptoms of depression that don't turn off but keep one from functioning well or feeling good. Many people with dysthymia also experience major depressive episodes at some time in their lives. Another depression type is bipolar disorder, also called manic depressive illness. Not quite as acute as other forms of depressive disorders, bipolar disorder is characterized by cycling mood changes: severe highs (mania) and lows (depression). Sometimes mood switches are dramatic and quick, but more often than not they are gradual. When in a depressed cycle, a person may have any or all of the symptoms of depression. When in a manic cycle, the person may be overactive, overtalkative, and have large amounts of energy. Mania often affects thinking, judgment, and social behavior in ways that cause serious problems and embarrassment. For example, a person in a manic phase may feel elated, full of grand schemes that can range from unwise business decisions to romantic sprees. Mania, left untreated, may worsen into a psychotic state.
Sometimes mood switches are dramatic and quick, but more often than not they are gradual. When in a depressed cycle, a person may have any or all of the symptoms of depression. When in a manic cycle, the person may be overactive, overtalkative, and have large amounts of energy. Mania often affects thinking, judgment, and social behavior in ways that cause serious problems and embarrassment. For example, a person in a manic phase may feel elated, full of grand schemes that can range from unwise business decisions to romantic sprees. Mania, left untreated, may worsen into a psychotic state.
Symptoms of depression
Not everyone who is depressed or manic experiences every single symptom of depression. Some people experience few symptoms of depression, some a lot. The severity of depression symptoms varies with individuals and also changes over time.
Depression
Always sad, anxious, or "empty" moods Feelings of hopelessness, pessimism Feelings of guilt, worthlessness, helplessness Loss of interest or pleasure in hobbies and activities that were once enjoyed, including sex Decreased energy, fatigue, being "slowed down" Difficulty concentrating, remembering, making decisions Insomnia, waking up early in the morning, or oversleeping Appetite and/or weight loss or overeating and weight gain Thoughts of death or suicide; suicide attempts Anxiety, irritability Persistent physical symptoms of depression that do not respond to treatment, such as headaches, indigestion, and chronic pain
Depressed women
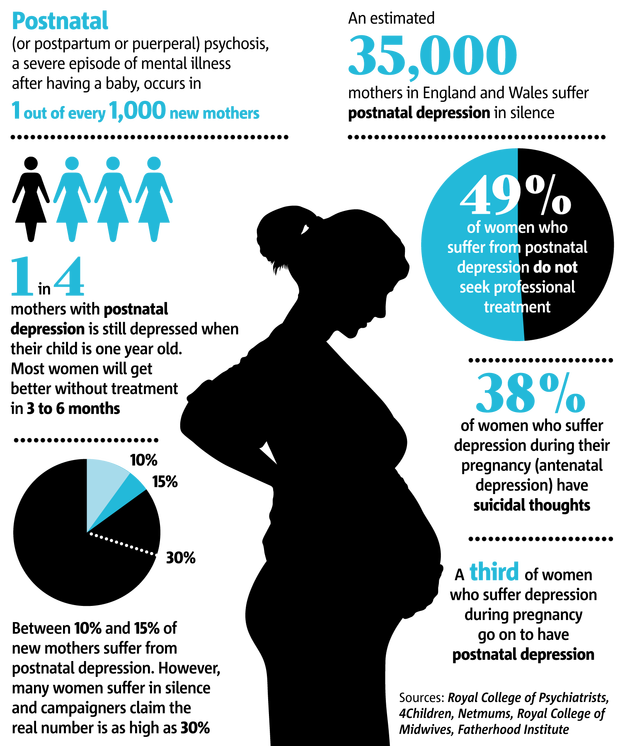
Women experience depression about twice as often as men.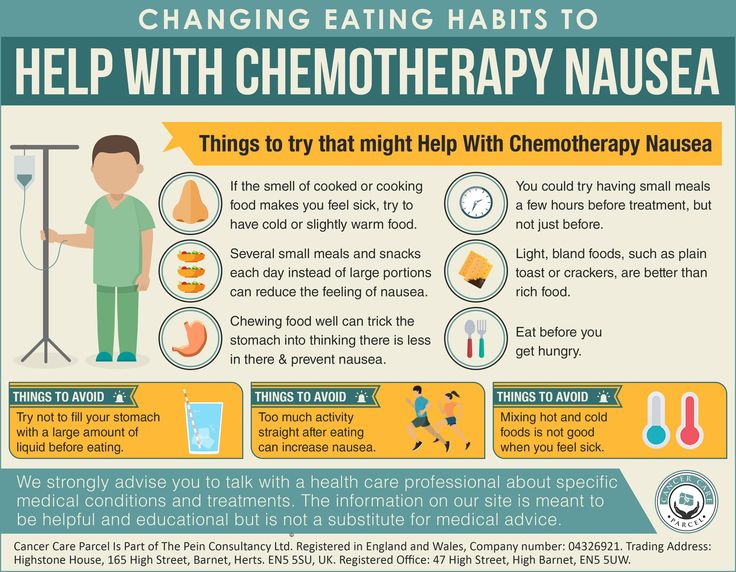 Many hormonal factors can contribute to an increase in women's proportion of depression - in particular, factors such as changes in the menstrual cycle, pregnancy, miscarriage, postpartum, pre-menopause, and menopause. Many women also face additional stresses such as responsibility, both at work and at home, with a single parent, and caring for children and elderly parents. A recent NIMH study showed that in the case of severe premenstrual syndrome (PMS), women with pre-existing vulnerabilities to PMS experienced and experienced relief from physical symptoms of depressed mood when their sex hormones were suppressed. Shortly after the hormones were reintroduced, they reappeared PMS symptoms. Women without a history of PMS reported no effects of hormonal manipulation. Many women are especially vulnerable after having a baby. Hormonal and physical changes, as well as the added responsibility of a new life, may be factors that lead to a woman's postpartum depression. Although transient "blues" are common in new mothers, a full blown depressive episode is not normal and requires active intervention.
Many hormonal factors can contribute to an increase in women's proportion of depression - in particular, factors such as changes in the menstrual cycle, pregnancy, miscarriage, postpartum, pre-menopause, and menopause. Many women also face additional stresses such as responsibility, both at work and at home, with a single parent, and caring for children and elderly parents. A recent NIMH study showed that in the case of severe premenstrual syndrome (PMS), women with pre-existing vulnerabilities to PMS experienced and experienced relief from physical symptoms of depressed mood when their sex hormones were suppressed. Shortly after the hormones were reintroduced, they reappeared PMS symptoms. Women without a history of PMS reported no effects of hormonal manipulation. Many women are especially vulnerable after having a baby. Hormonal and physical changes, as well as the added responsibility of a new life, may be factors that lead to a woman's postpartum depression. Although transient "blues" are common in new mothers, a full blown depressive episode is not normal and requires active intervention. Depression, treatment and family emotional support for a young mother are simple considerations in helping her regain her physical and mental well being and her ability to care for and enjoy her baby.
Depression, treatment and family emotional support for a young mother are simple considerations in helping her regain her physical and mental well being and her ability to care for and enjoy her baby.
Depressed men
Although men are less likely to suffer from depression than women, three to four million men in the US suffer from depression. Men are less likely to admit to depression, and doctors are less likely to suspect it. The suicide rate among men is four times that of women, although more women attempt it. In fact, after the age of 70, the rate of male suicide increases, reaching a maximum after 85 years. Men depression can also affect physical health unlike women. A new study shows that while male depression is associated with an increased risk of coronary heart disease in both men and women, only men suffer the highest mortality rate. Male depression is often masked by alcohol or drugs, or by a socially acceptable habit of working longer hours. Male depression usually manifests itself not as feelings of hopelessness and helplessness, but as irritability, anger, and distress, which means depression can be difficult to recognize as such in men. Even if a man realizes that he has male depression, he may be less willing than women to seek help. Encouragement and support from the right family members can make a difference. In the workplace, worker assistance professionals or workplace mental health programs can help in helping men understand and accept depression as a real illness that needs treatment.
Male depression usually manifests itself not as feelings of hopelessness and helplessness, but as irritability, anger, and distress, which means depression can be difficult to recognize as such in men. Even if a man realizes that he has male depression, he may be less willing than women to seek help. Encouragement and support from the right family members can make a difference. In the workplace, worker assistance professionals or workplace mental health programs can help in helping men understand and accept depression as a real illness that needs treatment.
Depression in old age
Some people have the misconception that it is normal for older people to feel depressed. On the contrary, most older people are satisfied with their lives. Sometimes, however, when depression develops, it can be dismissed as a normal part of aging. Depression in old age, undiagnosed and left untreated, causes unnecessary suffering for the family and for the individual who could live a fruitful life. When he or she goes to the doctor, the symptoms of depression described are usually physical; for an older person it is often reluctant to discuss feelings of hopelessness, sadness, loss of interest in normally pleasurable activities, or very prolonged grief after a loss. Recognizing how symptoms of depression in the elderly are often overlooked, many health care professionals are trained to identify and treat underlying depression. They acknowledge that some symptoms of depression may be side effects of medications the older person is taking for a physical problem, or they may be caused by comorbidities. Once a diagnosis of depression is made, treating the depression with medication and/or psychotherapy will help the depressed person return to a happier, more fulfilling life. Recent studies show that brief psychotherapy (discussing therapies that help a person in a day-to-day relationship or in learning to deal with the distorted negative thinking that usually accompanies depression) is effective in reducing depressive symptoms in short-term depression in older adults who are medically poorly.
When he or she goes to the doctor, the symptoms of depression described are usually physical; for an older person it is often reluctant to discuss feelings of hopelessness, sadness, loss of interest in normally pleasurable activities, or very prolonged grief after a loss. Recognizing how symptoms of depression in the elderly are often overlooked, many health care professionals are trained to identify and treat underlying depression. They acknowledge that some symptoms of depression may be side effects of medications the older person is taking for a physical problem, or they may be caused by comorbidities. Once a diagnosis of depression is made, treating the depression with medication and/or psychotherapy will help the depressed person return to a happier, more fulfilling life. Recent studies show that brief psychotherapy (discussing therapies that help a person in a day-to-day relationship or in learning to deal with the distorted negative thinking that usually accompanies depression) is effective in reducing depressive symptoms in short-term depression in older adults who are medically poorly. Psychotherapy is also helpful in older patients who are unable or unwilling to take medication. Efficacy studies show that late in life depression can be treated with psychotherapy. Improved recognition and treatment of depression at the end of life will make those years even more enjoyable and a fulfillment for depression in the elderly, family, and caregivers.
Psychotherapy is also helpful in older patients who are unable or unwilling to take medication. Efficacy studies show that late in life depression can be treated with psychotherapy. Improved recognition and treatment of depression at the end of life will make those years even more enjoyable and a fulfillment for depression in the elderly, family, and caregivers.
Children of depression
Only in the last two decades, depression in children has been very serious. A depressed child may pretend to be sick, refuse to go to school, cling to a parent, or fear that the parent may die. Older children may sulk, get into trouble at school, be negative, grouchy, and feel misunderstood. Because normal behaviors vary from one childhood stage to the next, it can be hard to tell whether a child is just going through a temporary "phase" or suffering from depression. Sometimes parents become worried about how the child's behavior has changed, or the teacher comments that "your child doesn't seem to be himself. " In such a case, if a visit to the child's pediatrician rules out physical symptoms of depression, the physician may suggest that the child cannot be evaluated, preferably by a psychiatrist who specializes in treating children. If treatment is needed, the doctor may suggest that another therapist, usually a social worker or psychologist, provide the treatment while the psychiatrist will oversee the treatment if necessary. Parents should not be afraid to ask questions: What are the qualifications of a psychotherapist? What treatment will the child have? Will the family as a whole be involved in therapy? Will my child's therapy include antidepressants? If yes, what are the possible side effects? The National Institute of Mental Health (NIMH) has identified the use of treatment for depression in children as an important area of research. NIMH-supported Research Units for Child Psychopharmacology (RUPPs) form a network of seven research sites where clinical research on the effects of drugs to treat psychiatric disorders can be conducted in children and adolescents.
" In such a case, if a visit to the child's pediatrician rules out physical symptoms of depression, the physician may suggest that the child cannot be evaluated, preferably by a psychiatrist who specializes in treating children. If treatment is needed, the doctor may suggest that another therapist, usually a social worker or psychologist, provide the treatment while the psychiatrist will oversee the treatment if necessary. Parents should not be afraid to ask questions: What are the qualifications of a psychotherapist? What treatment will the child have? Will the family as a whole be involved in therapy? Will my child's therapy include antidepressants? If yes, what are the possible side effects? The National Institute of Mental Health (NIMH) has identified the use of treatment for depression in children as an important area of research. NIMH-supported Research Units for Child Psychopharmacology (RUPPs) form a network of seven research sites where clinical research on the effects of drugs to treat psychiatric disorders can be conducted in children and adolescents. Among the medications being studied are antidepressants, some of which have been found to be effective in treating children with depression if properly supervised by the child's physician.
Among the medications being studied are antidepressants, some of which have been found to be effective in treating children with depression if properly supervised by the child's physician.
Depression treatment
The first step to getting the treatment you need for depression is a physical examination by a doctor. Certain medications, as well as certain illnesses such as a viral infection, can cause the same symptoms of depression, and the physician must rule out these possibilities through examination, interviews, and laboratory tests. If a physical cause for depression is ruled out, a psychological evaluation should be done by a physician or referral to a psychiatrist or psychologist. A good diagnostic evaluation will include a complete history of the symptoms of depression, i.e. when they started, how long they lasted, how severe they are, whether you had a patient before and, if so, what the symptoms of depression were treated for and what depression treatment. The doctor should ask about alcohol and drug use and if the patient has thoughts of death or suicide. Next, the history should include questions about whether other family members have had depressive illness and, if treated, what treatments for depression they received and which were effective. Last, the diagnostic evaluation should include a mental status examination to determine if speech or thinking or memory is affected, as is sometimes the case in depressive or manic-depressive psychosis. Depression treatment choices will depend on the results of the evaluation. There are various depression treatments and psychotherapies that can be used to treat depressive disorders. Some people with mild forms can only do well with psychotherapy. People with moderate to severe depression most often benefit from antidepressants. Most of them are even better with combined treatment for depression: treatment to get relatively quick relief from symptoms of depression and psychotherapy to find out better ways to deal with life's problems, including depression.
The doctor should ask about alcohol and drug use and if the patient has thoughts of death or suicide. Next, the history should include questions about whether other family members have had depressive illness and, if treated, what treatments for depression they received and which were effective. Last, the diagnostic evaluation should include a mental status examination to determine if speech or thinking or memory is affected, as is sometimes the case in depressive or manic-depressive psychosis. Depression treatment choices will depend on the results of the evaluation. There are various depression treatments and psychotherapies that can be used to treat depressive disorders. Some people with mild forms can only do well with psychotherapy. People with moderate to severe depression most often benefit from antidepressants. Most of them are even better with combined treatment for depression: treatment to get relatively quick relief from symptoms of depression and psychotherapy to find out better ways to deal with life's problems, including depression. Depending on the patient's diagnosis and the severity of the depression, the doctor may prescribe medication and/or one of several forms of psychotherapy that have been shown to be effective for depression. Electroconvulsive therapy (ECT) is useful, especially for individuals who have severe or life-threatening depression or who cannot take antidepressants. ECT is often effective when depression medications do not provide sufficient relief from depression symptoms. In recent years, the ECT has been greatly improved. Muscle relaxants are given before treatment for depression, which is performed under light anesthesia. Electrodes are attached to specific areas on the head to deliver electrical impulses. The stimulation results in a short (about 30 seconds) seizure in the brain. The person receiving ECT the patient is unaware of being subjected to electrical stimulation. For the full therapeutic effect, at least several sessions of electroshock, usually done at a rate of three per week, are required.
Depending on the patient's diagnosis and the severity of the depression, the doctor may prescribe medication and/or one of several forms of psychotherapy that have been shown to be effective for depression. Electroconvulsive therapy (ECT) is useful, especially for individuals who have severe or life-threatening depression or who cannot take antidepressants. ECT is often effective when depression medications do not provide sufficient relief from depression symptoms. In recent years, the ECT has been greatly improved. Muscle relaxants are given before treatment for depression, which is performed under light anesthesia. Electrodes are attached to specific areas on the head to deliver electrical impulses. The stimulation results in a short (about 30 seconds) seizure in the brain. The person receiving ECT the patient is unaware of being subjected to electrical stimulation. For the full therapeutic effect, at least several sessions of electroshock, usually done at a rate of three per week, are required.
Depression medications
There are several types of depression medications used to treat depressive disorders. These include new drugs, predominantly selective serotonin reuptake inhibitors (SSRIs)-tricyclics and monoamine oxidase inhibitors (MAOIs). SSRIs and other newer drugs that affect neurotransmitters such as dopamine or norepinephrine generally have fewer side effects than tricyclics. Sometimes a doctor will try different antidepressants before finding the most effective drug or combination of drugs. Sometimes the dose must be increased to be effective. Although some improvement can be seen in the first few weeks, antidepressants must be taken regularly for 3 to 4 weeks (in some cases, at least 8 weeks) before the full therapeutic effect occurs. Patients often feel like stopping treatment too soon. They may feel better and think they no longer need depression treatment. Or they may think depression treatment isn't helping at all. It is important to continue taking depression treatment for as long as it has a chance of working, although side effects may occur before antidepressant activity does. Once the person feels better, it is important to continue treatment for at least 4 to 9months to prevent a recurrence of depression. For some types of depression, medications must be stopped gradually to give the body time to adjust. Never stop taking antidepressants without consulting your doctor for instructions on how to safely stop treatment. For people with bipolar disorder or chronic depression, medications may need to be kept indefinitely. Antidepressants are not addictive. However, as is the case with any type of treatment prescribed for more than a few days, antidepressants must be carefully monitored to ensure that the correct dosage is being given. The doctor checks the dosage and its effectiveness on a regular basis. For the small number of people for whom MAO inhibitors are the best treatment for depression, avoid certain foods that contain high levels of tyramine, such as many cheeses, wines, and pickles, as well as medications such as decongestants. The interaction of tyramine with MAOIs can cause a hypertensive crisis, a sharp increase in blood pressure that can lead to a stroke.
Once the person feels better, it is important to continue treatment for at least 4 to 9months to prevent a recurrence of depression. For some types of depression, medications must be stopped gradually to give the body time to adjust. Never stop taking antidepressants without consulting your doctor for instructions on how to safely stop treatment. For people with bipolar disorder or chronic depression, medications may need to be kept indefinitely. Antidepressants are not addictive. However, as is the case with any type of treatment prescribed for more than a few days, antidepressants must be carefully monitored to ensure that the correct dosage is being given. The doctor checks the dosage and its effectiveness on a regular basis. For the small number of people for whom MAO inhibitors are the best treatment for depression, avoid certain foods that contain high levels of tyramine, such as many cheeses, wines, and pickles, as well as medications such as decongestants. The interaction of tyramine with MAOIs can cause a hypertensive crisis, a sharp increase in blood pressure that can lead to a stroke. The doctor must provide a complete list of prohibited products that the patient must wear at all times. Other types of antidepressants do not require any food restrictions. Medicines of any kind - prescribed, over the counter, or borrowed - should never be mixed without the advice of a doctor. Other health care professionals who may prescribe drugs, such as a dentist or other medical professionals, should be told about the medication the patient is taking. Some medications, although safe when taken, can, if taken with others, cause serious and dangerous side effects. Certain medications, such as alcohol or drugs, may reduce the effectiveness of antidepressants and should be avoided. This includes wine, beer and spirits. Some people who have not had a problem with alcohol may be allowed by their doctor to use moderate amounts of alcohol by taking one of the newer antidepressants. Anti-anxiety drugs or sedatives are not antidepressants. They are sometimes prescribed along with antidepressants, however they are not effective when taken only for a depressive disorder.
The doctor must provide a complete list of prohibited products that the patient must wear at all times. Other types of antidepressants do not require any food restrictions. Medicines of any kind - prescribed, over the counter, or borrowed - should never be mixed without the advice of a doctor. Other health care professionals who may prescribe drugs, such as a dentist or other medical professionals, should be told about the medication the patient is taking. Some medications, although safe when taken, can, if taken with others, cause serious and dangerous side effects. Certain medications, such as alcohol or drugs, may reduce the effectiveness of antidepressants and should be avoided. This includes wine, beer and spirits. Some people who have not had a problem with alcohol may be allowed by their doctor to use moderate amounts of alcohol by taking one of the newer antidepressants. Anti-anxiety drugs or sedatives are not antidepressants. They are sometimes prescribed along with antidepressants, however they are not effective when taken only for a depressive disorder. Stimulants, such as amphetamines, are not effective antidepressants, but they are sometimes used under close supervision in medically ill patients with depression. Questions about any antidepressants prescribed, or problems that may be associated with treatment, should be discussed with your doctor.
Stimulants, such as amphetamines, are not effective antidepressants, but they are sometimes used under close supervision in medically ill patients with depression. Questions about any antidepressants prescribed, or problems that may be associated with treatment, should be discussed with your doctor.
Side effects
Antidepressants can cause mild and usually side effects (sometimes referred to as adverse effects) in some people. This is usually annoying, but not serious. However, any unusual reactions and side effects or those that interfere with functioning should be reported to the doctor. The most common side effects of tricyclic antidepressants, and how to deal with them, are: Dry mouth, sipping water, chewing sugar-free gum is helpful; brush your teeth daily. · Constipation bran cereals, prunes, fruits and vegetables should be in the diet. · Bladder Emptying of the bladder may be troublesome, and the flow of urine may not be as strong as usual, the physician should be notified if there is noted difficulty or pain. · Sexual function problems may change, if disturbing, ask your doctor about male enhancement or female enhancement options. · Blurred vision that will soon pass, and not usually the need for new glasses. · Dizziness getting out of bed or chair slowly is helpful. · Drowsiness as a daytime problem that usually goes away soon. A sleepy feeling or sedated person should not drive or operate heavy machinery. More sedating antidepressants are usually taken at bedtime to help sleep and minimize daytime sleepiness. The newer antidepressants have different types of side effects: · Headache, this will usually go away. · Nausea is also temporary, but even when it occurs, it is transient after each dose. Nervousness and insomnia (trouble falling asleep or staying awake often at night) this may occur during the first few weeks; dosage or time reduction is usually their solution. · Agitation (feeling jittery), if this occurs for the first time after the drug is taken and is more than transient, the physician should be notified.
· Sexual function problems may change, if disturbing, ask your doctor about male enhancement or female enhancement options. · Blurred vision that will soon pass, and not usually the need for new glasses. · Dizziness getting out of bed or chair slowly is helpful. · Drowsiness as a daytime problem that usually goes away soon. A sleepy feeling or sedated person should not drive or operate heavy machinery. More sedating antidepressants are usually taken at bedtime to help sleep and minimize daytime sleepiness. The newer antidepressants have different types of side effects: · Headache, this will usually go away. · Nausea is also temporary, but even when it occurs, it is transient after each dose. Nervousness and insomnia (trouble falling asleep or staying awake often at night) this may occur during the first few weeks; dosage or time reduction is usually their solution. · Agitation (feeling jittery), if this occurs for the first time after the drug is taken and is more than transient, the physician should be notified. · Sexual problems A doctor should be consulted if the problem is persistent or distressing.
· Sexual problems A doctor should be consulted if the problem is persistent or distressing.
Herbal Treatments for Depression
In the last few years there has been a significant increase in interest in the use of herbs in the treatment of depression. St. John's wort (Hypericum perforatum), an herb widely used in the treatment of depression in Europe, has recently aroused interest in the United States. St. John's wort, an attractive bushy, low-growing plant covered in yellow summer flowers, has been used for centuries in many folk and herbal remedies. Today in Germany, St. John's wort is used in the treatment of depression more than any other antidepressant. However, the scientific studies that have been conducted on its use have been short term and have used several different doses. Because of the strong interest in John's Wort, the National Institutes of Health (NIH) conducted a 3-year study sponsored by three NIH components—the National Institute of Mental Health, the National Center for Complementary and Alternative Medicine, and the Office of Dietary Supplements. The study was designed to include 336 patients with moderate depression randomly assigned to an 8-week study with one third of patients receiving a uniform dose of St. a third of a placebo (a pill that looks exactly like SSRI and St. John's Wort, but has no active ingredients). Study participants who responded positively were followed up for another 18 weeks. At the end of the first phase of the study, participants were measured on two scales, one for depression and one for general functioning. There was no significant difference in response rate from depression, but the scale for overall functioning was better for antidepressants than for wort or St. John's or placebo. While this study does not support the use of St. John's wort in the treatment of depression, ongoing NIH-supported research is investigating a possible role for St. John's wort in the treatment of milder forms of depression. The Food and Drug Administration issued a Health Advisory on February 10, 2000. She stated that John's Wort St.
The study was designed to include 336 patients with moderate depression randomly assigned to an 8-week study with one third of patients receiving a uniform dose of St. a third of a placebo (a pill that looks exactly like SSRI and St. John's Wort, but has no active ingredients). Study participants who responded positively were followed up for another 18 weeks. At the end of the first phase of the study, participants were measured on two scales, one for depression and one for general functioning. There was no significant difference in response rate from depression, but the scale for overall functioning was better for antidepressants than for wort or St. John's or placebo. While this study does not support the use of St. John's wort in the treatment of depression, ongoing NIH-supported research is investigating a possible role for St. John's wort in the treatment of milder forms of depression. The Food and Drug Administration issued a Health Advisory on February 10, 2000. She stated that John's Wort St. appears to affect an important metabolic pathway that is used in many medications prescribed to treat conditions such as AIDS, cardiovascular disease, depression, seizures, certain cancers, and transplant rejection. Therefore, healthcare professionals should warn their patients about the potential interactions of these drugs. Some other herbal treatments for depression supplements commonly used that have not been evaluated in large scale clinical trials are ephedra, ginkgo biloba, echinacea, and ginseng. Any herbal treatment for depression should only be taken after consultation with a doctor or other health care provider.
appears to affect an important metabolic pathway that is used in many medications prescribed to treat conditions such as AIDS, cardiovascular disease, depression, seizures, certain cancers, and transplant rejection. Therefore, healthcare professionals should warn their patients about the potential interactions of these drugs. Some other herbal treatments for depression supplements commonly used that have not been evaluated in large scale clinical trials are ephedra, ginkgo biloba, echinacea, and ginseng. Any herbal treatment for depression should only be taken after consultation with a doctor or other health care provider.
The best treatment for depression
Relora is a 100% natural product, all that effectively relieves the varied and debilitating symptoms of stress, anxiety and depression. Relora is a non-prescription antidepressant like Prozac, Paxil, Zoloft, Wellbutrin and Effexor. Relora is designed to treat you safely and naturally, without the worries you might find over the counter drugs and their unwanted side effects. Relora also helps you release that stubborn extra weight around your waist caused by high levels of the stress hormone cortisol.
Relora also helps you release that stubborn extra weight around your waist caused by high levels of the stress hormone cortisol.
Depression Treatment
There is no easy cure for depression because your brain is not easy. But science has shown that some natural ingredients can help. It is perfectly normal to feel some depression from time to time. But you don't have to feel them all the time. The active ingredients in Relora can work to help regulate the chemicals that affect your mood without the debilitating side effects of prescription drugs! We recommend "Relora" as the top (92 out of 100 points) Relora's depression and anxiety relief formula ingredients have been extensively researched and documented with over 45 studies currently available. Most areas of research include cancer adjuvant therapy, reducing depression, stress and anxiety, promoting relaxation, improving learning and concentration, etc. It has also proven beneficial in significantly reducing the physical, mental and social symptoms of PMS such as depression, insomnia, muscle stiffness, seizures, anxiety, irritability, etc.