How to spot fake ptsd
A Systematic Approach to the Detection of False PTSD
Research ArticleRegular Article
Mikel Matto, Dale E. McNiel and Renée L. Binder
Journal of the American Academy of Psychiatry and the Law Online June 2019, JAAPL.003853-19; DOI: https://doi.org/10.29158/JAAPL.003853-19
- Article
- Figures & Data
- Info & Metrics
Abstract
Posttraumatic stress disorder (PTSD) can occur after a traumatic experience and can cause severe symptoms that interfere with a person's psychological, physical, interpersonal, occupational, and social functioning. It is important to accurately identify genuine cases of PTSD and, as part of the differential diagnosis, to rule out instances of false PTSD. False PTSD diagnoses can adversely affect treatment planning, resource management, and research. The subjective nature of stressors, stereotypic presentation of symptoms, wealth of resources detailing how to malinger PTSD, and the high stakes for individuals involved in criminal, civil, and disability evaluations create challenges for making an accurate diagnosis.
This article presents a systematic approach to help clinicians and forensic evaluators distinguish genuine PTSD from false variants of the disorder. It describes the types of false PTSD to be considered as alternative diagnoses, including malingered PTSD (for external gain, such as receiving a disability pension or evading criminal consequences), factitious PTSD (for internal gain, such as assuming the victim or hero/veteran role), and misattributed PTSD (legitimate psychopathology misdiagnosed as PTSD). The authors describe clinical features and psychological testing that may be leveraged to aid in reaching a more valid diagnosis.
Posttraumatic stress disorder (PTSD) is a serious condition that is associated with high levels of social, occupational, and physical disability, as well as considerable economic costs and high levels of medical utilization.1 Service members are returning to their communities from the wars in Iraq and Afghanistan with symptoms of psychiatric disorders, including PTSD. Survivors of sexual assault on college campuses share their experiences with increasing openness, and some report severe psychological sequelae after their trauma. In short, PTSD is a growing problem that the mental health field continues to study for predisposing factors, mitigation strategies, and the development of more effective treatments. To do so effectively, great care needs to be taken to distinguish between genuine and false cases of PTSD.
Survivors of sexual assault on college campuses share their experiences with increasing openness, and some report severe psychological sequelae after their trauma. In short, PTSD is a growing problem that the mental health field continues to study for predisposing factors, mitigation strategies, and the development of more effective treatments. To do so effectively, great care needs to be taken to distinguish between genuine and false cases of PTSD.
Trauma is used frequently as the basis for civil suits involving mild to severe injuries. It is also used in criminal cases to minimize responsibility or mitigate sentencing. PTSD can also be alleged as the basis for financial incentives such as those related to disability. Forensic evaluators are often called upon to help distinguish between genuine and false PTSD. This article describes a detailed approach designed to help with these evaluations and to assist treating clinicians and PTSD researchers.
Despite its apparent ubiquity, PTSD is not the expected outcome from trauma exposure. The National Comorbidity Survey demonstrated that although 61 percent of men and 51 percent of women were exposed to a traumatic experience at some point in their lives, the lifetime prevalence of PTSD was 8 percent and 20 percent, respectively.2 Experiencing symptoms after a trauma (e.g., intrusive thoughts, nightmares, insomnia, avoidance of reminders of the event, exaggerated negative beliefs, irritability, and hypervigilance that do not spontaneously resolve within months after trauma) is the exception to the norm. Such symptoms become less exceptional, however, as cumulative trauma burden increases.
The National Comorbidity Survey demonstrated that although 61 percent of men and 51 percent of women were exposed to a traumatic experience at some point in their lives, the lifetime prevalence of PTSD was 8 percent and 20 percent, respectively.2 Experiencing symptoms after a trauma (e.g., intrusive thoughts, nightmares, insomnia, avoidance of reminders of the event, exaggerated negative beliefs, irritability, and hypervigilance that do not spontaneously resolve within months after trauma) is the exception to the norm. Such symptoms become less exceptional, however, as cumulative trauma burden increases.
After being described by various terms throughout each of the country's wars, bearing names like “soldier's heart,” “shell shock,” “combat neurosis,” and “battle fatigue,” PTSD formally entered the psychiatric lexicon in 1980 with the publication of the Diagnostic and Statistical Manual of Mental Disorders, Third Edition (DSM-III). Because of the subjective nature of the symptoms in the diagnostic criteria, clinicians have always relied heavily on patient report. This reliance has increased in recent years by the gradual broadening of the definition of what constitutes a traumatic stressor, which changed in 1994 with the publication of Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) from an objective standard (an event that would be distressing to anyone) to a subjective one (an event the individual found distressing).3 In 2013, with the publication of Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), the diagnosis no longer requires a reaction at the time to include “fear, helplessness, or horror.” The PTSD criteria for what constitutes trauma and how a patient reacts to it have become more inclusive over time.
This reliance has increased in recent years by the gradual broadening of the definition of what constitutes a traumatic stressor, which changed in 1994 with the publication of Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) from an objective standard (an event that would be distressing to anyone) to a subjective one (an event the individual found distressing).3 In 2013, with the publication of Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), the diagnosis no longer requires a reaction at the time to include “fear, helplessness, or horror.” The PTSD criteria for what constitutes trauma and how a patient reacts to it have become more inclusive over time.
Patients may have conscious and unconscious motivations to feign a diagnosis of PTSD. These can include legal (e.g., reducing or avoiding criminal liability), personal (e.g., justifying relationship strife and occupational problems), financial (e.g., acquiring money from civil lawsuits, disability, and veteran pensions), shelter (e. g., securing inpatient or ER admission), and social (e.g., gaining sympathy or respect from peers). Clinicians may be reluctant to question the validity of self-reported trauma and related symptoms. They may worry about loss of rapport, stigmatizing patients, and the moral responsibility to veterans or patients as victims deserving additional services.4
g., securing inpatient or ER admission), and social (e.g., gaining sympathy or respect from peers). Clinicians may be reluctant to question the validity of self-reported trauma and related symptoms. They may worry about loss of rapport, stigmatizing patients, and the moral responsibility to veterans or patients as victims deserving additional services.4
The importance of an accurate PTSD diagnosis is critical on both individual and community levels. For the individual, accurate identification of true PTSD is important so that appropriate treatment can be provided. On the other hand, patients may be given inappropriate or even harmful treatment for non-present PTSD, and suspicion of feigning during treatment can have negative impacts on rapport.5 An inaccurate PTSD diagnosis also often obscures a legitimate alternate diagnosis that is left untreated. On a community level, the availability of clinical resources to treat PTSD is limited, and efforts to treat misdiagnosed PTSD deprive others in need of treatment. Inappropriate diagnosis also leads to inaccuracies in medical research because these cases would not be expected to respond to PTSD treatment. Many researchers are emphasizing the importance of ruling out suspected malingered PTSD from clinical trials to more reliably measure the effectiveness of PTSD treatment.5,–,7
Inappropriate diagnosis also leads to inaccuracies in medical research because these cases would not be expected to respond to PTSD treatment. Many researchers are emphasizing the importance of ruling out suspected malingered PTSD from clinical trials to more reliably measure the effectiveness of PTSD treatment.5,–,7
On a national level, the financial need for accurate PTSD diagnosis is critical. Between 1999 and 2004, PTSD disability payments increased 149 percent (up to $4.3 billion) versus an increase of 42 percent for all other disability payments. The number of veterans receiving Veterans Affairs (VA) disability for PTSD rose 80 percent (versus 12% for other disabilities) during that time. By 2010, the number of veterans receiving PTSD disability had risen by 222 percent compared with 1999.8,–,10 By 2013, 6.8 percent of all veterans receiving any VA disability payments were receiving compensation for PTSD, and 34.9 percent of veterans receiving disability payments for mental health reasons, such as PTSD, received compensation at a 70 percent or higher disability rating (compared with 3. 8% receiving ratings at this level for all other conditions).11 Data have also demonstrated that service-connected veterans reported increasingly worsening symptoms of PTSD until reaching 100 percent disability, followed by an 82 percent decrease in their use of VA mental health services (without a change in their use of VA medical services).8,12 PTSD is now the most prevalent service-connected mental disorder and the third most prevalent service-connected disability for veterans receiving pension benefits.13 Whether this rapid rise in the number and severity of PTSD claims is due to the diagnostic criteria changes in DSM, the nature of the combat during Operations Iraqi Freedom and Enduring Freedom (OIF/OEF) (e.g., high comorbidity of traumatic brain injuries, increased rates of multiple amputations, etc.), the trauma burden of recent veterans, or increased rates of feigned PTSD is unclear at this time, but it warrants consideration.
8% receiving ratings at this level for all other conditions).11 Data have also demonstrated that service-connected veterans reported increasingly worsening symptoms of PTSD until reaching 100 percent disability, followed by an 82 percent decrease in their use of VA mental health services (without a change in their use of VA medical services).8,12 PTSD is now the most prevalent service-connected mental disorder and the third most prevalent service-connected disability for veterans receiving pension benefits.13 Whether this rapid rise in the number and severity of PTSD claims is due to the diagnostic criteria changes in DSM, the nature of the combat during Operations Iraqi Freedom and Enduring Freedom (OIF/OEF) (e.g., high comorbidity of traumatic brain injuries, increased rates of multiple amputations, etc.), the trauma burden of recent veterans, or increased rates of feigned PTSD is unclear at this time, but it warrants consideration.
How frequently are cases of PTSD feigned? Prevalence of general malingering is largely a matter of context. Base rates are estimated at 15.7 percent for forensic evaluations versus 7.4 percent for non-forensic evaluations.14 In the criminal justice system, malingering estimates for competency to stand trial evaluations vary between 8 percent and 17.4 percent, and malingering in requests for psychological services in the correctional setting is estimated to be 45 to 56 percent.15 Malingering is estimated to occur in 20 to 30 percent of personal injury claims for PTSD and at least 20 percent of compensation- and pension-seeking combat veterans.9,16,17
Base rates are estimated at 15.7 percent for forensic evaluations versus 7.4 percent for non-forensic evaluations.14 In the criminal justice system, malingering estimates for competency to stand trial evaluations vary between 8 percent and 17.4 percent, and malingering in requests for psychological services in the correctional setting is estimated to be 45 to 56 percent.15 Malingering is estimated to occur in 20 to 30 percent of personal injury claims for PTSD and at least 20 percent of compensation- and pension-seeking combat veterans.9,16,17
Given the level of PTSD awareness in popular culture and the attraction the diagnosis may hold for some patients, it is important that clinicians, researchers, and forensic evaluators consider a methodical approach to facilitate diagnostic accuracy by arriving at a determination of PTSD after considering and ruling out alternatives resembling PTSD (i.e., false PTSD).
Steps to Evaluate False PTSD
The five steps to properly evaluate false PTSD are listed here and discussed in the following sections:
Review collateral information and relevant records.
Conduct the evaluation.
Consider misattributed PTSD.
Consider malingered or factitious PTSD.
Consider performing psychological testing.
Collateral Information and Records
The most accepted way to confirm volitionally produced PTSD is to compare the patient's subjective report with outside evidence. For single-session evaluations, it is desirable to collect and review collateral information prior to the evaluation. This can facilitate consideration of the consistency between information derived from the interview (including signs, symptoms, and described cross-domain functionality) with pertinent documentation in multiple domains, as listed in Table 1.
Table 1
Data Domains to Consider in the Evaluation of False PTSD
The Evaluation
Further relevant information can be gathered from behavioral observations prior to the formal beginning of the evaluation session. Observation of an evaluee's interaction with his or her environment can be useful (e.g., waiting room seating selection, demonstration of irritability with paperwork or delays, eye contact or behavior with patients or staff). Discussion prior to the perceived initiation of the formal evaluation interview can yield information that is helpful for determining potential PTSD symptom clusters. Casual questions about things like traffic, sporting events, or hobbies can help reveal the presence or absence of triggers for road rage, avoidance symptoms, and level and ubiquity of impairment, respectively.
Observation of an evaluee's interaction with his or her environment can be useful (e.g., waiting room seating selection, demonstration of irritability with paperwork or delays, eye contact or behavior with patients or staff). Discussion prior to the perceived initiation of the formal evaluation interview can yield information that is helpful for determining potential PTSD symptom clusters. Casual questions about things like traffic, sporting events, or hobbies can help reveal the presence or absence of triggers for road rage, avoidance symptoms, and level and ubiquity of impairment, respectively.
Interviewing an evaluee in the presence of others can be problematic.4,5 A third party can potentially taint the evaluation through interruptions or unsolicited input and can affect the responses of the evaluee. Given that PTSD often presents in ways similar to portrayals in film and television, particular care needs to be taken to use open-ended and non-leading questions. This gives evaluees the ability to report genuine symptoms in their own words and provides more opportunity for suspected malingerers to contradict themselves. 18,20,21
18,20,21
Whereas a structured interview format is helpful in research settings, it can be problematic in forensic evaluations by suggesting possible symptoms that an evaluee may readily endorse due to demand characteristics of the setting. Instead, eliciting more detail about each symptom and evaluating each of the criteria for the PTSD diagnosis in DSM-5 helps determine whether the PTSD diagnosis is genuine.
Exposure (Criterion A)
As mentioned above, the definition of what constitutes “exposure” and “trauma” in PTSD have changed over the years. The Criterion A specification in DSM-III that characterized the index trauma as “outside the range of usual human experience” (Ref. 22, p 236) and one that would “evoke significant symptoms of distress in almost everyone” (Ref. 22, p 238) was eliminated in DSM-IV after epidemiologic surveys used examples from lists of qualifying traumatic events and determined that clinical judgment about the stress resulting from specific traumatic events for a typical person was not a feasible standard. 3 DSM-IV also included language in Criterion A1 indicating that the event could be “witnessed” or the individual “confronted with” the trauma,23 explicitly incorporating a class of traumatic experiences that, prior to this, had been the subject of debate. One study found that this change increased the number of traumatic events meeting the exposure criteria by 59 percent, with a corresponding 38 percent increase in the number of people meeting PTSD diagnostic criteria.3 DSM-5 criteria serve to limit the indirect exposure described in DSM-IV by requiring “learning that the traumatic event(s) occurred to a close family member or close friend” for an event in which the “actual or threatened death was violent or accidental (Ref. 1, p 271) and specifically excluding witnessing events through media (such as television, movies, or video games) unless the exposure is work related.1,24 The Criterion A2 requirement that individuals respond to the traumatic event with “intense fear, helplessness, or horror” (Ref.
3 DSM-IV also included language in Criterion A1 indicating that the event could be “witnessed” or the individual “confronted with” the trauma,23 explicitly incorporating a class of traumatic experiences that, prior to this, had been the subject of debate. One study found that this change increased the number of traumatic events meeting the exposure criteria by 59 percent, with a corresponding 38 percent increase in the number of people meeting PTSD diagnostic criteria.3 DSM-5 criteria serve to limit the indirect exposure described in DSM-IV by requiring “learning that the traumatic event(s) occurred to a close family member or close friend” for an event in which the “actual or threatened death was violent or accidental (Ref. 1, p 271) and specifically excluding witnessing events through media (such as television, movies, or video games) unless the exposure is work related.1,24 The Criterion A2 requirement that individuals respond to the traumatic event with “intense fear, helplessness, or horror” (Ref. 23, p 467) was removed entirely in DSM-5, making a PTSD diagnosis more applicable to individuals whose background and training might preclude them from expressing such a response in the moment, such as first responders and military service members. The forensic evaluator's determination of a Criterion A-qualifying traumatic event is critical to distinguish PTSD from an adjustment disorder with similar PTSD-like symptoms. With changes that will potentially serve to both increase inclusion (lack of emotional reaction requirement) and decrease inclusion (“learned-about” trauma limited to family or close friend suffering violent or accidental threats or trauma), it is unclear at this time how the changes between DSM-IV and DSM-5 will affect prevalence.
23, p 467) was removed entirely in DSM-5, making a PTSD diagnosis more applicable to individuals whose background and training might preclude them from expressing such a response in the moment, such as first responders and military service members. The forensic evaluator's determination of a Criterion A-qualifying traumatic event is critical to distinguish PTSD from an adjustment disorder with similar PTSD-like symptoms. With changes that will potentially serve to both increase inclusion (lack of emotional reaction requirement) and decrease inclusion (“learned-about” trauma limited to family or close friend suffering violent or accidental threats or trauma), it is unclear at this time how the changes between DSM-IV and DSM-5 will affect prevalence.
Finally, when determining whether an evaluee's described traumatic event satisfies Criterion A, it is important to consider this event in the context of the individual's overall trauma history. While a subject may focus on a single recent event of modest intensity, the literature suggests that there is a cumulative burden of trauma with increased prevalence, symptom complexity, and functional impairment of PTSD and other psychopathologies that correlate to the number of childhood and adult trauma exposures (including combat deployments, sexual assault, and other traumatic experiences). 25,–,27
25,–,27
Intrusion Symptoms (Criterion B)
Dreams and flashbacks are often viewed by the layperson as the hallmark of PTSD, and these symptoms are often predominant in feigned PTSD. The forensically-oriented PTSD literature contains the following descriptions of ways to assist in determining the likelihood that intrusion symptoms are legitimate. It is particularly helpful to validate these symptoms with third parties and collateral, when possible.
Individuals with PTSD related to combat or rape are believed to more likely have repetitive dreams of discrete content from the traumatic event itself, whereas other sufferers of PTSD typically have more thematic types of content during nightmares.9,18,28,–,31 Emotions experienced during nightmares are often representative of emotions experienced at the time of trauma. For example, nightmares related to civilian trauma, such as rape, often consist of feelings of anxiety and helplessness, versus nightmares related to combat trauma, which more frequently have predominant themes of horror, grief, hostility, or rage. 18,28 PTSD nightmares are almost always accompanied by either sudden awakenings or notable body movement while asleep, a fact that should be apparent to bedmates.4,18,30,32
18,28 PTSD nightmares are almost always accompanied by either sudden awakenings or notable body movement while asleep, a fact that should be apparent to bedmates.4,18,30,32
Although individuals experiencing flashbacks re-experience perceptual and emotional details, feigning evaluees may underappreciate that flashbacks are more likely to include auditory and olfactory components (compared with nightmares, which are often purely visual) and not understand that during flashbacks individuals also experience and remember portions or the entirety of their actions.18,33
Avoidance (Criterion C)
Whereas DSM-IV employed one criterion consisting of avoidance (C1–C2) and numbing (C3–C7), DSM-5 separated them into symptoms of “persistent avoidance of stimuli associated with the traumatic event(s)” (Criterion C) and “negative alterations in cognitions and mood associated with the traumatic event(s)” (Criterion D) (Ref. 1, p 271). This change was made in the setting of factor analysis, which suggests that avoidance and numbing symptoms were distinct entities originating from separate mechanisms and having different clinical associations with other psychopathologies. 34,–,37 A study indicated that when avoidance was created as the standalone Criterion C in DSM-5, this change reduced classification of PTSD cases when compared with DSM-IV criteria by 22 percent and 26 percent at 3 months and 12 months after trauma, respectively,34 with many of the re-classified cases instead likely attributable to major depressive disorder.
34,–,37 A study indicated that when avoidance was created as the standalone Criterion C in DSM-5, this change reduced classification of PTSD cases when compared with DSM-IV criteria by 22 percent and 26 percent at 3 months and 12 months after trauma, respectively,34 with many of the re-classified cases instead likely attributable to major depressive disorder.
While intrusion symptoms are often understood and appreciated by individuals feigning PTSD, the importance of avoidance in the diagnosis and presentation of PTSD is often undervalued; this is particularly relevant with avoidance now being a required component of PTSD diagnosis. When evaluees are familiar with the concept of PTSD avoidance, it may be literal (e.g., avoiding movies about the wars in Afghanistan and Iraq) rather than the subtler symbolic associations (e.g., avoiding gas stations due to the smell of oil triggering memories of the patrols in trucks while deployed). As with other aspects of detection of false PTSD, it is important to consider whether underreporting is an overlooked feigned symptom or a component of underreporting of all PTSD and other mental health symptoms due to an emphasis on resiliency stemming from a military background or other elements of an evaluee's culture.
Negative Cognitions and Mood (Criterion D)
Changes to DSM-5 added new symptoms to represent a broad range of disturbances in PTSD, including “persistent and exaggerated negative beliefs or expectations about oneself, others, or the world” (Criterion D2), “persistent, distorted cognitions about the cause or consequences of the traumatic event(s) that lead the individual to blame himself/herself or others” (Criterion D3), and “persistent negative emotional state” (Criterion D4) (Ref. 1, p 272). Studies have demonstrated that these symptom clusters are predictive of later development of PTSD and are well represented in validated civilian and combat PTSD.24,38,–,40 The challenge for evaluators is to distinguish PTSD-related negative alterations in cognitions and mood (such as survivor guilt, a sense of foreshortened future, and feelings of detachment) from the negative alterations in cognition and mood that can result from similar features in depression. Two other symptoms in this PTSD criterion (i. e., inability to recall important aspects of trauma and reckless or self-destructive behavior) may be presented by individuals feigning PTSD due to the potential for these symptoms to reduce or mitigate legal responsibility. These two symptoms, however, represent the least commonly endorsed symptoms seen in individuals with PTSD per DSM-5,24,38 and in a large-scale study of active duty military service members, risky behavior was moderately associated with anxiety and depression but only mildly associated with PTSD.41
e., inability to recall important aspects of trauma and reckless or self-destructive behavior) may be presented by individuals feigning PTSD due to the potential for these symptoms to reduce or mitigate legal responsibility. These two symptoms, however, represent the least commonly endorsed symptoms seen in individuals with PTSD per DSM-5,24,38 and in a large-scale study of active duty military service members, risky behavior was moderately associated with anxiety and depression but only mildly associated with PTSD.41
Arousal and Reactivity (Criterion E)
Similar to intrusion symptoms, hypervigilance and exaggerated startle response are well known to individuals with even a minimal understanding of PTSD. Care needs to be taken to compare collateral sources and third-party reports of observed behavior with the presentation of the evaluee during the interview (e.g., an evaluee sitting with his back to the door of a busy hallway exhibiting discomfort or exaggerated response to unexpected noise that is consistent with claims). As is described in more detail in the testing section below, there is a dearth of instruments to quantitatively detect physiological changes in individuals with PTSD without prohibitive false-positive and false-negative rates that render these tests unsuitable for most forensic evaluations.18
As is described in more detail in the testing section below, there is a dearth of instruments to quantitatively detect physiological changes in individuals with PTSD without prohibitive false-positive and false-negative rates that render these tests unsuitable for most forensic evaluations.18
Duration and Impairment (Criteria F and G)
Two separate studies evaluated cases of emotional reactions to non-traumatic events that met PTSD criteria for intrusion, avoidance/numbing, and arousal symptoms. When the duration and impairment criteria were applied, the PTSD rate decreased from 20 percent to 3 percent.42 The subject needs to demonstrate clinically significant distress or impairment in work, relationships, and other major activities of daily life for more than one month to be accurately characterized as PTSD. This requires attention to whether reduction in function is limited to areas of unpleasant duties or impacts domains of life that would be otherwise pleasurable.
Consider Misattributed PTSD
After a thorough review of symptoms, accurate evaluation of potential PTSD can be facilitated by a consideration of a broad differential diagnosis to rule out non-PTSD psychopathology. Techniques vary, but using a simple acronym (i.e., STAMP) can be helpful in clinical encounters to ensure the consideration of multiple diagnostic possibilities:
Cases in which the suspected PTSD is due to psychopathology from another etiology is a form of misattributed PTSD due to misdiagnosis. Experiences of irritability, insomnia, poor concentration, and stress intolerance may be a result of persistent postconcussive syndrome from a traumatic brain injury. Anxiety disorders may be the cause of hyperarousal and non-trauma–focused avoidance symptoms. Affect dysregulation and impaired behavioral control may be due to underlying personality disorders. Depressive disorders may be responsible for symptoms of negative beliefs, guilt, and persistent negative affect. Given that a traumatic event is a discrete and often life-changing experience for an individual, survivors may be more likely to assign symptoms of psychopathology to the trauma itself rather than to recognize that these symptoms predated it.24 Even in cases in which PTSD is genuine, it is still important to screen for missed diagnoses. PTSD is rarely seen as a standalone disorder. In one large study of outpatients with a principal PTSD diagnosis, 92 percent had another active psychiatric diagnosis,43 and the National Comorbidity Survey showed that 59 percent of men and 44 percent of women diagnosed with PTSD had three or more other psychiatric diagnoses.2 Clinicians may attribute symptoms to PTSD that are instead related to unrecognized comorbidities such as depression, anxiety, or personality disorder. These comorbidities are particularly important to recognize in cases in which PTSD is being utilized for purposes of criminal responsibility, civil liability, or pension or disability.
Given that a traumatic event is a discrete and often life-changing experience for an individual, survivors may be more likely to assign symptoms of psychopathology to the trauma itself rather than to recognize that these symptoms predated it.24 Even in cases in which PTSD is genuine, it is still important to screen for missed diagnoses. PTSD is rarely seen as a standalone disorder. In one large study of outpatients with a principal PTSD diagnosis, 92 percent had another active psychiatric diagnosis,43 and the National Comorbidity Survey showed that 59 percent of men and 44 percent of women diagnosed with PTSD had three or more other psychiatric diagnoses.2 Clinicians may attribute symptoms to PTSD that are instead related to unrecognized comorbidities such as depression, anxiety, or personality disorder. These comorbidities are particularly important to recognize in cases in which PTSD is being utilized for purposes of criminal responsibility, civil liability, or pension or disability. Misattributed PTSD is likely to produce substandard responses to treatment due to non–evidence-based interventions (in the case of misdiagnosis) or incomplete interventions (in the case of missed diagnosis).
Misattributed PTSD is likely to produce substandard responses to treatment due to non–evidence-based interventions (in the case of misdiagnosis) or incomplete interventions (in the case of missed diagnosis).
Consider Malingered or Factitious PTSD
The next step is to determine whether observed PTSD-like symptoms are being volitionally produced. Patients feigning symptoms of PTSD will often give vague or non-specific answers to direct questions and will provide stereotypic or dramatic, heroic, or cinematic symptom depiction. It is important to determine if this is due to symptom avoidance, mistrust of the clinician, or exaggeration compensating for memory impairment.4,5,9,18,28,44 Patients attempting to portray PTSD often underestimate the body movement that typically occurs with PTSD nightmares, overestimate the frequency of flashbacks, and underappreciate the dissociative quality that typically accompanies them.4,18
Although there is a wealth of clinical lore regarding features of volitionally produced symptoms of PTSD, caution is warranted because much of it represents an accumulation of anecdotal evidence rather than the results of formal studies. Further, many such generalizations (e.g., “Real combat veterans are reluctant to talk about their combat.”) are culturally biased and may be out of date. While the generalization of the stoic World War II veterans reluctant to discuss their experiences may have had some validity at a point in time, it is difficult to apply this convincingly (without further study) to an Iraq or Afghanistan veteran who grew up with social media without further study. Rogers and Schuman describe six indications for feigned symptoms: rare symptoms, improbable or absurd responses, indiscriminate symptom endorsement, unlikely symptom combinations, contradictory symptoms, and symptom severity.45,46
Further, many such generalizations (e.g., “Real combat veterans are reluctant to talk about their combat.”) are culturally biased and may be out of date. While the generalization of the stoic World War II veterans reluctant to discuss their experiences may have had some validity at a point in time, it is difficult to apply this convincingly (without further study) to an Iraq or Afghanistan veteran who grew up with social media without further study. Rogers and Schuman describe six indications for feigned symptoms: rare symptoms, improbable or absurd responses, indiscriminate symptom endorsement, unlikely symptom combinations, contradictory symptoms, and symptom severity.45,46
If the symptoms appear to be feigned, clinicians need to consider the type of motivation behind it. Feigned symptoms are often assumed to represent malingering, which is described in DSM-5 as the “intentional production of false or grossly exaggerated physical or psychological symptoms, motivated by external incentives such as avoiding military duty, avoiding work, obtaining financial compensation, evading criminal prosecution, or obtaining drugs” (Ref. 1, p 726). Examples of external motivations that can be present in malingered PTSD include acquiring VA disability pension, military medical retirement, or state disability; obtaining financial rewards through civil damages; securing housing through veteran- or PTSD-specific programming; obtaining drugs or medications such as benzodiazepines, sedatives, or medical marijuana; gaining workplace accommodations; and avoiding criminal responsibility through not guilty by reason of insanity defense, unconscious defense, self-defense, or mitigating circumstances.4,5,44,47
1, p 726). Examples of external motivations that can be present in malingered PTSD include acquiring VA disability pension, military medical retirement, or state disability; obtaining financial rewards through civil damages; securing housing through veteran- or PTSD-specific programming; obtaining drugs or medications such as benzodiazepines, sedatives, or medical marijuana; gaining workplace accommodations; and avoiding criminal responsibility through not guilty by reason of insanity defense, unconscious defense, self-defense, or mitigating circumstances.4,5,44,47
Feigned PTSD is not necessarily a complete manufacturing of symptoms, and it is valuable to consider malingering patterns as described by Resnick: pure malingering is when the person feigns non-existing symptoms, partial malingering is when the person consciously exaggerates existing symptoms, and false imputation is when the individual consciously attributes existing symptoms to a cause not responsible for the symptoms (e. g., an individual with longstanding anxiety disorder intentionally attributese these symptoms to a later accident for the sake of a civil lawsuit).19 The motivation for malingering may be influenced by third parties, such as when patients are encouraged by legal representation to present for treatment for the sake of gaining a diagnostic report to bolster their case or for prolonged care to demonstrate refractory psychopathology to increase a potential financial settlement.9
g., an individual with longstanding anxiety disorder intentionally attributese these symptoms to a later accident for the sake of a civil lawsuit).19 The motivation for malingering may be influenced by third parties, such as when patients are encouraged by legal representation to present for treatment for the sake of gaining a diagnostic report to bolster their case or for prolonged care to demonstrate refractory psychopathology to increase a potential financial settlement.9
When patients appear to consciously produce symptoms in the absence of external gain, a form of “factitious PTSD” is a potential diagnosis. Whereas a diagnostic criterion of factitious disorder in DSM-IV was “the motivation for the behavior is to assume the sick role” (Ref. 23, p 517), DSM-5 does not require this distinction and only requires that the subject's “deceptive behavior is evident even in the absence of obvious external rewards” (Ref. 1, p 325). In this rarely discussed form of feigned PTSD, patients may fabricate symptoms for the sake of the potential benefits that the community and society give to individuals who are in the sick role. 48 This can be further amplified for individuals in the victim role (e.g., motor vehicle accidents, rape, assault) or the hero role (e.g., combat veterans). This phenomenon has been repeatedly observed in veterans presenting with feigned symptoms of PTSD in which a review of collateral information demonstrated that the described traumas did not occur and there is no obvious external gain.49,–,51 Similar cases of factitious PTSD have been described in civilian counterparts in claims of abuse and abductions.52 Explanations have been posed that patients may desire to take on this patient or victim role to transform their identity and cultivate desired relationships.53 PTSD can be used as a way to gain recognition, respect, and appreciation from peers, loved ones, and society at large. It can also be used as an explanation or rationalization for failures in interpersonal relationships, professional obligations, or sobriety. In a large study of VA disability claimants for PTSD in the Midwest over one year, 74 percent agreed both that the service connection for PTSD was important because “it will show the government acknowledges how I was affected by my military experience” and “it will show that there is a reason for my problems” (Ref.
 54, p 2138). With increased destigmatization of PTSD and the cultural cachet of the survivor designation, PTSD is a more attractive diagnosis than substance use disorder, anxiety, or depression. While the Stolen Valor Act of 201355 (a revised version of the 2005 law of the same name56 determined by United States v. Alvarez57 to be an infringement on the First Amendment) made it a crime for individuals to claim to have received valor awards by the military only if done so for the sake of external gain, there are still many websites that detail cases of men and women falsely claiming war veteran and PTSD status only for other reasons. Factitious PTSD and seeking internal gain is a consideration for clinicians noting feigned symptoms when there is no obvious material reward.
54, p 2138). With increased destigmatization of PTSD and the cultural cachet of the survivor designation, PTSD is a more attractive diagnosis than substance use disorder, anxiety, or depression. While the Stolen Valor Act of 201355 (a revised version of the 2005 law of the same name56 determined by United States v. Alvarez57 to be an infringement on the First Amendment) made it a crime for individuals to claim to have received valor awards by the military only if done so for the sake of external gain, there are still many websites that detail cases of men and women falsely claiming war veteran and PTSD status only for other reasons. Factitious PTSD and seeking internal gain is a consideration for clinicians noting feigned symptoms when there is no obvious material reward.
Psychological Testing
Although listed last here, formal psychological testing to distinguish genuine PTSD from the variants of false PTSD may be employed at any point in the forensic evaluation and, in fact, may be a critical part of the evaluation. In one study, 86 percent of college students without specific training and without clinical evidence of PTSD were able to successfully meet criteria for PTSD by using a symptom checklist.58 Although a comprehensive review of psychological tests that can assist in evaluation for false PTSD is beyond the scope of this article, some examples will be described.
In one study, 86 percent of college students without specific training and without clinical evidence of PTSD were able to successfully meet criteria for PTSD by using a symptom checklist.58 Although a comprehensive review of psychological tests that can assist in evaluation for false PTSD is beyond the scope of this article, some examples will be described.
One initial approach is to use a screening test such as the Miller-Forensic Assessment of Symptoms (M-FAST).59 This 25-question instrument requires 5–10 minutes to complete. Studies have demonstrated identification of 78 percent of subjects who have been instructed to malinger.60 It is commonly used to identify individuals who score above a cutoff suggesting malingering and are then referred for more intensive testing. As is true for any forensic determination, the determination of feigned PTSD should not rely on any single measure.61
Self-report symptom checklists such as the PTSD Checklist for DSM-5 or PCL-562 can be problematic due to the potential for over-reported or feigned symptoms but can be helpful if the evaluator uses them cautiously to contrast the results with observed signs or symptoms during the interview or via collateral. The Clinician-Administered PTSD Scale (CAPS)63 is a structured interview developed by the Department of Veterans Affairs that includes 17 items rated on a scale of 0–4 points and takes approximately one hour to complete. While widely used in research settings, the measure has the potential to be exploited by evaluees feigning symptoms. Although the measure permits the evaluator to note items of “questionable validity,” the accuracy of the clinician ratings in detecting exaggerated or invalid symptom endorsement has not been demonstrated empirically.16,64
The Clinician-Administered PTSD Scale (CAPS)63 is a structured interview developed by the Department of Veterans Affairs that includes 17 items rated on a scale of 0–4 points and takes approximately one hour to complete. While widely used in research settings, the measure has the potential to be exploited by evaluees feigning symptoms. Although the measure permits the evaluator to note items of “questionable validity,” the accuracy of the clinician ratings in detecting exaggerated or invalid symptom endorsement has not been demonstrated empirically.16,64
The Structured Interview of Reported Symptoms-2 (SIRS-2)65 requires 30–45 minutes to complete and is widely used to assess malingering in general and in PTSD specifically. It includes a variety of strategies to detect feigning, such as questions about highly unusual symptoms or atypical symptom pairing.9 It has been used in inpatient, correctional, and forensic populations with high accuracy.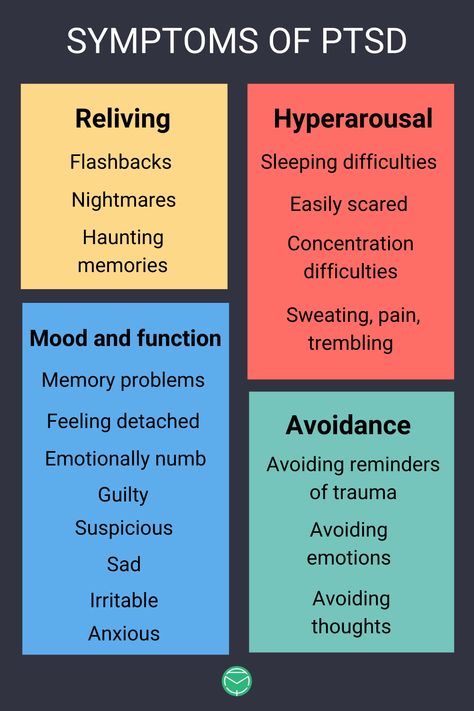 4 The tool uses eight primary and five supplementary scales to detect 13 response styles that have been associated with feigned symptoms.45 One study tested subjects coached with PTSD diagnostic criteria, and the results indicated that the RS, IA, SC, BL, SU, SEL, SEV, and RO scales of the SIRS discriminated legitimate patients from coached subjects.64,66
4 The tool uses eight primary and five supplementary scales to detect 13 response styles that have been associated with feigned symptoms.45 One study tested subjects coached with PTSD diagnostic criteria, and the results indicated that the RS, IA, SC, BL, SU, SEL, SEV, and RO scales of the SIRS discriminated legitimate patients from coached subjects.64,66
The Minnesota Multiphasic Personal Inventory-2 (MMPI-2)67 is a self-report multi-scale personality inventory that is reported by multiple studies to have high sensitivity for identifying malingered PTSD.47 In early studies of the MMPI, more than 90 percent of subjects attempting to malinger PTSD were correctly identified using the F and PK scales, leading to a recommendation that examiners use cutoff scores of T > 88 and T > 30, respectively.47,68,69 More recent studies of the MMPI-2 found that the strongest predictors of malingering in civilian samples were the Fp, F-K, and O-S scales, whereas the strongest predictor in a veteran study was the F-K scale, closely followed by the F, Ds2, F-FB, O-S, and OT fake-bad scales. 47,70,–,72 Although the F scale is the most effective at detecting malingered psychopathology in general, it has not been shown to be one of the best MMPI-2 predictors for malingered PTSD. A specific Infrequency-Posttraumatic Stress Disorder scale (Fptsd) was developed to assist with feigned PTSD detection. Results appear to indicate that the Fptsd scale was more effective at predicting malingering using combat PTSD patients, whereas Fp was most useful with civilian PTSD patients.72,–,74
47,70,–,72 Although the F scale is the most effective at detecting malingered psychopathology in general, it has not been shown to be one of the best MMPI-2 predictors for malingered PTSD. A specific Infrequency-Posttraumatic Stress Disorder scale (Fptsd) was developed to assist with feigned PTSD detection. Results appear to indicate that the Fptsd scale was more effective at predicting malingering using combat PTSD patients, whereas Fp was most useful with civilian PTSD patients.72,–,74
The Personality Assessment Inventory (PAI)75 is a widely used multi-scale inventory that includes validity scales to assess response style and scales that assess symptoms related to PTSD. The Negative Impression (NIM) scale, Negative Distortion Scale (NDS), and Malingering Index (MAL) are validity scales that are reported to be useful in differentiating genuine from feigned PTSD.61,76
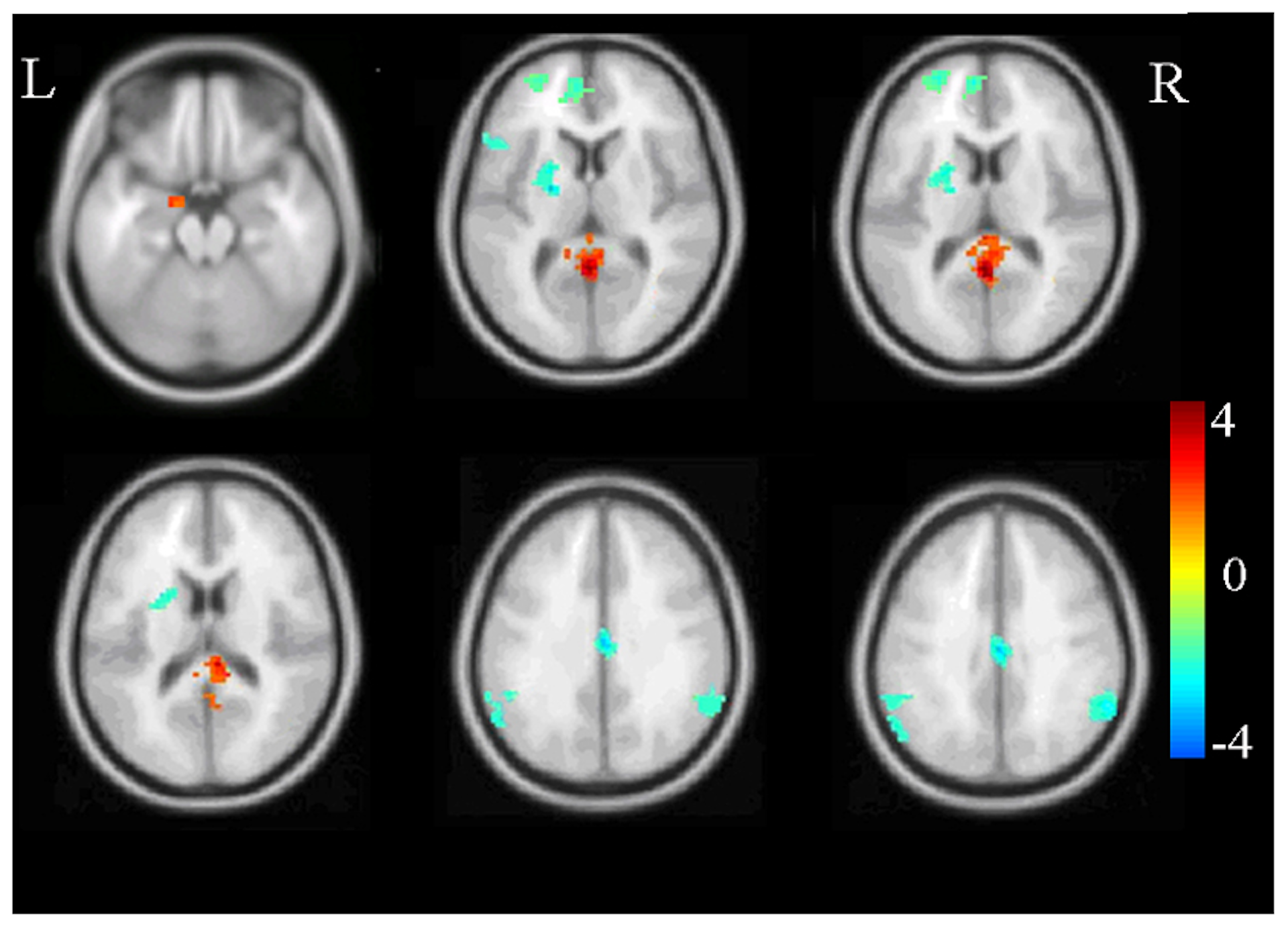
Other domains of testing show promise but have not reached a level of acceptance required for forensic purposes. Psychophysiologic testing is occasionally used and has variable admissibility in court.4 Testing can include measurements such as blood pressure, heart rate, temperature, forehead electromyography, and galvanic skin response after exposure to sudden loud noises or via script-driven imagery. At this time, there is a lack of consistent criteria for identifying feigned PTSD on the basis of psychophysiological testing, although the approach may be promising.18 There has also been growing research in the diagnostic use of hormones and neurotransmitters (including cortisol, cortisol-releasing factor, neuropeptide Y, and norepinephrine), but current findings cannot be used reliably to diagnose PTSD or to rule out feigned PTSD.18,64 Neuroimaging has also been utilized to identify increased or signature brain activity associated with lying, particularly the orbito-frontal/ventrolateral prefrontal cortex, dorsolateral prefrontal cortex, anterior cingulate cortex, and thalamus,77 but these are areas of research and are not used clinically at this time.
Psychophysiologic testing is occasionally used and has variable admissibility in court.4 Testing can include measurements such as blood pressure, heart rate, temperature, forehead electromyography, and galvanic skin response after exposure to sudden loud noises or via script-driven imagery. At this time, there is a lack of consistent criteria for identifying feigned PTSD on the basis of psychophysiological testing, although the approach may be promising.18 There has also been growing research in the diagnostic use of hormones and neurotransmitters (including cortisol, cortisol-releasing factor, neuropeptide Y, and norepinephrine), but current findings cannot be used reliably to diagnose PTSD or to rule out feigned PTSD.18,64 Neuroimaging has also been utilized to identify increased or signature brain activity associated with lying, particularly the orbito-frontal/ventrolateral prefrontal cortex, dorsolateral prefrontal cortex, anterior cingulate cortex, and thalamus,77 but these are areas of research and are not used clinically at this time.
Conclusion
A methodical approach can help clinicians and forensic evaluators rule out several types of false PTSD prior to arriving at an accurate diagnosis of genuine PTSD. Consideration of the data described in this paper can help ensure that more valid research occurs and that clinical and financial resources are allocated to individuals with genuine PTSD, while evaluees presenting with false PTSD can be approached intentionally, compassionately, and tactfully.
References
- 1.↵
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Washington, DC: American Psychiatric Association, 2013
- 2.↵
- Kessler RC,
- Sonnega A,
- Bromet E,
- et al
: Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 52:1048–60, 1995
- 3.↵
- Breslau N,
- Kessler RC
: The stressor criterion in DSM-IV posttraumatic stress disorder: an empirical investigation.
 Biol Psychiatry 50:699–704, 2001
Biol Psychiatry 50:699–704, 2001 - 4.↵
- Knoll J,
- Resnick PJ
: The detection of malingered post-traumatic stress disorder. Psychiatr Clin North Am 29:629–47, 2006
- 5.↵
- Ali S,
- Jabeen S,
- Alam F
: Multimodal approach to identifying malingered posttraumatic stress disorder: a review. Innov Clin Neurosci 12:12–20, 2015
- 6.↵
- Charney DS,
- Davidson JRT,
- Friedman M,
- et al
: A consensus meeting on effective research practice in PTSD. CNS Spectrums 3:6–10, 1998
- 7.↵
- Rosen GM
: DSM's cautionary guideline to rule out malingering can protect the PTSD data base. J Anxiety Disord 20:530–5, 2006
- 8.
 ↵
↵Review of State Variances in VA Disability Compensation Payments (Report #05-00765-137). Washington, DC: Department of Veterans Affairs Office of Inspector General, 2005
- 9.↵
- Taylor S,
- Frueh BC,
- Asmundson GJ
: Detection and management of malingering in people presenting for treatment of posttraumatic stress disorder: methods, obstacles, and recommendations. J Anxiety Disord 21:22–41, 2007
- 10.↵
- Marx BPH,
- Holowka DW
: PTSD disability assessment. PTSD Res Q 22:1–6, 2011
- 11.↵
- McNally RJ,
- Frueh BC
: Why are Iraq and Afghanistan War veterans seeking PTSD disability compensation at unprecedented rates? J Anxiety Disord 27:520–6, 2013
- 12.↵
- Frueh BC,
- Grubaugh AL,
- Elhai JD,
- Buckley TC
: US Department of Veterans Affairs disability policies for posttraumatic stress disorder: administrative trends and implications for treatment, rehabilitation, and research.
 Am J Public Health 97:2143–5, 2007
Am J Public Health 97:2143–5, 2007 - 13.↵
2015 Annual Benefits Report (Compensation). Available at: https://www.benefits.va.gov/REPORTS/abr/ABR-Compensation-FY15-05092016.pdf. Accessed January 22, 2018
- 14.↵
- Rogers R,
- Sewell KW,
- Goldstein A
: Explanatory models of malingering: a prototypical analysis. Law & Hum Behav 18:543–52, 1994
- 15.↵
- McDermott BE,
- Dualan IV,
- Scott CL
: Malingering in the correctional system: does incentive affect prevalence? Int'l J L & Psychiatry 36:287–92, 2013
- 16.↵
- Frueh BC,
- Hamner MB,
- Cahill SP,
- et al
: Apparent symptom overreporting in combat veterans evaluated for PTSD. Clin Psychol Rev 20:853–85, 2000
- 17.
 ↵
↵- Lees-Haley PR
: MMPI-2 base rates for 492 personal injury plaintiffs: implications and challenges for forensic assessment. J Clin Psychol 53:745–55, 1997
- 18.↵
- Hall RC,
- Hall RC
: Malingering of PTSD: forensic and diagnostic considerations, characteristics of malingerers and clinical presentations. Gen Hosp Psychiatry 28:525–35, 2006
- 19.↵
- Rogers R
- Resnick PJ,
- West S,
- Payne JW
: Malingering of posttraumatic disorders, in Clinical Assessment of Malingering and Deception, Third Edition. Edited by Rogers R. New York: Guilford Press, 2008, pp 109–27
- 20.↵
- Resnick PJ
: The detection of malingered psychosis. Psychiatr Clin North Am 22:159–72, 1999
- 21.
 ↵
↵- Wiley SD
: Deception and detection in psychiatric diagnosis. Psychiatr Clin North Am 21:869–93, 1998
- 22.↵
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Third Edition. Washington, DC: American Psychiatric Association, 1980
- 23.↵
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC: American Psychiatric Association, 2000
- 24.↵
- Zoellner LA,
- Bedard-Gilligan MA,
- Jun JJ,
- et al
: The evolving construct of posttraumatic stress disorder (PTSD): DSM-5 criteria changes and legal implications. Psychol Inj Law 6:277–289, 2013
- 25.↵
- Karam EG,
- Friedman MJ,
- Hill ED,
- et al
: Cumulative traumas and risk thresholds: 12-month PTSD in the World Mental Health (WMH) surveys.
 Depress Anxiety 31:130–42, 2014
Depress Anxiety 31:130–42, 2014 - 26.↵
- Cloitre M,
- Stolbach BC,
- Herman JL,
- et al
: A developmental approach to complex PTSD: childhood and adult cumulative trauma as predictors of symptom complexity. J Trauma Stress 22:399–408, 2009
- 27.↵
- Kline A,
- Falca-Dodson M,
- Sussner B,
- et al
: Effects of repeated deployment to Iraq and Afghanistan on the health of New Jersey Army National Guard troops: implications for military readiness. Am J Public Health 100:276–83, 2010
- 28.↵
- Resnick PJ
: Malingering of posttraumatic psychiatric disorders. J Pract Psychiatry Behav Health 4:329–339, 1998
- 29.↵
- Ross RJ,
- Ball WA,
- Sullivan KA,
- Caroff SN
: Sleep disturbance as the hallmark of posttraumatic stress disorder.
 Am J Psychiatry 146:697–707, 1989
Am J Psychiatry 146:697–707, 1989 - 30.↵
- Van der Kolk B,
- Blitz R,
- Burr W,
- et al
: Nightmares and trauma: a comparison of nightmares after combat with lifelong nightmares in veterans. Am J Psychiatry 141:187–90, 1984
- 31.↵
- Schreuder BJ,
- Kleijn WC,
- Rooijmans HG
: Nocturnal re-experiencing more than forty years after war trauma. J Trauma Stress 13:453–63, 2000
- 32.↵
- Zervas IM,
- Soldatos CR
: Nightmares: personality dimensions and psychopathological attributes. Int Rev Psychiatry 17:271–6, 2005
- 33.↵
- Geraerts E,
- Kozarić-Kovačić D,
- Merckelbach H,
- et al
: Traumatic memories of war veterans: not so special after all.
 Conscious Cogn 16:170–7, 2007
Conscious Cogn 16:170–7, 2007 - 34.↵
- Forbes D,
- Fletcher S,
- Lockwood E,
- et al
: Requiring both avoidance and emotional numbing in DSM-V PTSD: will it help? J Affect Disord 130:483–6, 2011
- 35.↵
- Naifeh JA,
- Elhai JD,
- Kashdan TB,
- et al
: The PTSD symptom scale's latent structure: an examination of trauma-exposed medical patients. J Anxiety Disord 22:1355–68, 2008
- 36.↵
- Palmieri PA,
- Weathers FW,
- Difede J,
- et al
: Confirmatory factor analysis of the PTSD Checklist and the Clinician-Administered PTSD Scale in disaster workers exposed to the World Trade Center Ground Zero. J Abnorm Psychol 116:329–41, 2007
- 37.↵
- Simms LJ,
- Watson D,
- Doebbeling BN
: Confirmatory factor analyses of posttraumatic stress symptoms in deployed and nondeployed veterans of the Gulf War.
 J Abnorm Psychol 111:637–47, 2002
J Abnorm Psychol 111:637–47, 2002 - 38.↵
- Miller MW,
- Wolf EJ,
- Kilpatrick D,
- et al
: The prevalence and latent structure of proposed DSM-5 posttraumatic stress disorder symptoms in US national and veteran samples. Psychol Trauma 5:501–12, 2013
- 39.↵
- Foa E,
- Ehlers A,
- Clark DM,
- et al
: The Posttraumatic Cognitions Inventory (PTCI): development and validation. Psychological Assessment 11:303–14, 1999
- 40.↵
- Dunmore E,
- Clark DM,
- Ehlers A
: A prospective investigation of the role of cognitive factors in persistent posttraumatic stress disorder (PTSD) after physical or sexual assault. Behav Res Ther 39:1063–84, 2001
- 41.↵
- Thomsen CJ,
- Stander VA,
- McWhorter SK,
- et al
: Effects of combat deployment on risky and self-destructive behavior among active duty military personnel.
 J Psychiatr Res 45:1321–31, 2011
J Psychiatr Res 45:1321–31, 2011 - 42.↵
- Boals A,
- Hathaway LM
: The importance of the DSM-IV E and F criteria in self-report assessments of PTSD. J Anxiety Disord 24:161–6, 2010
- 43.↵
- Brown TA,
- Campbell LA,
- Lehman CL,
- et al
: Current and lifetime comorbidity of the DSM-IV anxiety and mood disorders in a large clinical sample. J Abnorm Psychol 110:585–99, 2001
- 44.↵
- Berger O,
- McNiel DE,
- Binder RL
: PTSD as a criminal defense: a review of case law. J Am Acad Psychiatry Law 40:509–21, 2012
- 45.↵
- McCullumsmith CB,
- Ford CV
: Simulated illness: the factitious disorders and malingering.
 Psychiatr Clin N Am 34:621–41, 2011
Psychiatr Clin N Am 34:621–41, 2011 - 46.↵
- Rogers R,
- Shuman DW
: The mental state at the time of the offense measure: its validation and admissibility under Daubert. J Am Acad Psychiatry Law 28:23–8, 2000
- 47.↵
- Guriel J,
- Fremouw W
: Assessing malingered posttraumatic stress disorder: a critical review. Clin Psychol Rev 23:881–904, 2003
- 48.↵
- Bass C,
- Halligan P
: Factitious disorders and malingering: challenges for clinical assessment and management. Lancet 383:1422–32, 2014
- 49.↵
- Sparr L,
- Pankratz L
: Factitious posttraumatic stress disorder. Am J Psychiatry 140:1016–19, 1983
- 50.
 ↵
↵- Lynn EJ,
- Belza M
: Factitious posttraumatic stress disorder: the veteran who never got to Vietnam. Hosp. Comm Psychiatry 35:697–701, 1984
- 51.↵
- Hamilton J
: Pseudo-posttraumatic stress disorder. Mil Med 150:353–6, 1985
- 52.↵
- Rosen GM,
- Taylor S
: Pseudo-PTSD. J Anxiety Disord 21:201–10, 2007
- 53.↵
- Baumeister RF,
- Sommer KL
: Patterns in the bizarre: common themes in satanic ritual abuse, sexual masochism, UFO abductions, factitious illness, and extreme love. J Soc Clin Psychol 16:213–23, 1997
- 54.↵
- Sayer NA,
- Spoont M,
- Nelson D
: Veterans seeking disability benefits for post-traumatic stress disorder: who applies and the self-reported meaning of disability compensation.
 Soc Sci Med 58:2133–43, 2004
Soc Sci Med 58:2133–43, 2004 - 55.↵
18 U.S.C. § 704 (2013).
- 56.↵
18 U.S.C. § 704 (2006), invalidated by United States v. Alvarez, 567 U.S. 709 (2012).
- 57.↵
United States v. Alvarez, 567 U.S. 709 (2012).
- 58.↵
- Lees-Haley PR,
- Dunn JT
: The ability of naive subjects to report symptoms of mild brain injury, post-traumatic stress disorder, major depression, and generalized anxiety disorder. J Clin Psychol 50:252–6, 1994
- 59.↵
- Miller HA
: Miller Forensic Assessment of Symptoms Test (M-FAST). Lutz, FL: Psychological Assessment Resources, 2001
- 60.↵
- Messer JM,
- Fremouw WJ
: Detecting malingered posttraumatic stress disorder using the Morel Emotional Numbing Test-Revised (MENT-R) and the Miller Forensic Assessment of Symptoms Test (M-FAST).
 J Forensic Psychol Pract 7:33–57, 2007
J Forensic Psychol Pract 7:33–57, 2007 - 61.↵
- Wooley CN,
- Rogers R
: The effectiveness of the personality assessment inventory with feigned PTSD: an initial investigation of Resnick's model of malingering. Assessment 22:449–58, 2015
- 62.↵
- Weathers FW,
- Litz BT,
- Keane TM,
- et al
: The PTSD Checklist for DSM-5 (PCL-5) – Standard [Measurement instrument]. Available at: http://www.ptsd.va.gov. Accessed November 24, 2018
- 63.↵
- Weathers FW,
- Blake DD,
- Schnurr PP,
- et al
. Clinician-Administered PTSD Scale for DSM-5 (CAPS-5). US Department of Veterans Affairs. PTSD: National Center for PTSD [Measurement instrument]. Available at: http://www.ptsd.va.gov. Accessed November 24, 2018
- 64.
 ↵
↵- Hall RC,
- Hall RC
: Detection of malingered PTSD: an overview of clinical, psychometric, and physiological assessment: where do we stand? J Forensic Sci 52:717–25, 2007
- 65.↵
- Rogers R,
- Bagby RM,
- Dickens SE
: Structured Interview of Reported Symptoms (SIRS) and professional manual. Odessa, FL: Psychological Assessment Resources, 2010
- 66.↵
- Rogers R,
- Kropp PR,
- Bagby RM,
- Dickens SE
: Faking specific disorders: a study of the Structured Interview of Reported Symptoms (SIRS). J Clin Psychol 48:778, 1992
- 67.↵
- Butcher JN,
- Graham JR,
- Ben-Porath YS,
- et al
. MMPI-2: Manual for Administration and Scoring (revised).
 Minneapolis: University of Minnesota Press, 2001
Minneapolis: University of Minnesota Press, 2001 - 68.↵
- Fairbank JA,
- McCaffrey RJ,
- Keane TM
: Psychometric detection of fabricated symptoms of posttraumatic stress disorder. Am J Psychiatry 142:501–3, 1985
- 69.↵
- McCaffrey RJ,
- Bellamy-Campbell R
: Psychometric detection of fabricated symptoms of combat-related post-traumatic stress disorder: a systematic replication. J Clin Psychol 45:76–9, 1989
- 70.↵
- Elhai JD,
- Frueh BC,
- Gold PB,
- et al
: Clinical presentations of posttraumatic stress disorder across trauma populations: a comparison of MMPI-2 profiles of combat veterans and adult survivors of child sexual abuse. J Nerv Ment Dis 188:708–13, 2000
- 71.↵
- Elhai JD,
- Frueh BC
: Subtypes of clinical presentations in malingerers of posttraumatic stress disorder: an MMPI-2 cluster analysis.
 Assessment 8:75–84, 2001
Assessment 8:75–84, 2001 - 72.↵
- Elhai JD,
- Gold SN,
- Sellers AH,
- Dorfman WI
: The detection of malingered posttraumatic stress disorder with MMPI-2 fake bad indices. Assessment 8:221–36, 2001
- 73.↵
- Elhai JD,
- Naifeh JA,
- Zucker IS,
- et al
: Discriminating malingered from genuine civilian posttraumatic stress disorder: a validation of three MMPI-2 infrequency scales (F, Fp, and Fptsd). Assessment 11:139–44, 2004
- 74.↵
- Elhai JD,
- Ruggiero KJ,
- Frueh BC,
- et al
: The Infrequency-Posttraumatic Stress Disorder scale (Fptsd) for the MMPI-2: development and initial validation with veterans presenting with combat-related PTSD. J Pers Assess 79:531–49, 2002
- 75.
 ↵
↵- Morey LC
: The Personality Assessment Inventory (PAI): Professional Manual, 2nd Edition. Lutz, FL: Psychological Assessment Resources, 2007
- 76.↵
- Rogers R,
- Bender SD
- Boccaccini MT,
- Hart JR
: Response style on the Personality Assessment Inventory and other multiscale inventories, in Clinical Assessment of Malingering and Deception, Fourth Edition. Edited by Rogers R, Bender SD. New York: Guilford Press, 2018, pp. 280–300
- 77.↵
- Seron X
: Lying in neuropsychology. Neurophysiol Clin 44:389–403, 2014
Back to top
False PTSD: A Diagnostic Challenge
by Joyce Frieden, News Editor, MedPage Today November 14, 2016
Last Updated November 15, 2016
Distinguishing false post-traumatic stress disorder (PTSD) from the real thing can be very tricky, but it's necessary in order both to help patients and to make sure treatment resources are allocated correctly, according to Mikel Matto, MD, assistant clinical professor of psychiatry at the University of California San Francisco.
"There is a very finite number of psychiatrists who are well-qualified to treat PTSD, and if they're spending time on [false] PTSD cases, they're not able to treat the people who need help the most, " Matto said in a phone interview.
At last month's American Academy of Psychiatry and the Law annual meeting in Portland, Ore., Matto laid out a framework for assessing potential PTSD cases. Matto is a captain in the California Army National Guard and chief mental health officer for the Joint Force Headquarters.
The framework delineates five possible types of PTSD diagnoses:
- Misattributed PTSD: Symptoms that are consistent with PTSD but are actually more attributable to a co-morbidity such as anxiety. Misattributed PTSD is fairly common, since 92% of patients with a primary PTSD diagnosis have at least one other psychiatric diagnosis, according to Matto.
- Malingered PTSD: Symptoms are being deliberately falsified by the patient in order to achieve some sort of external gain, such as pension or disability payments, or dismissal from a lawsuit.

- Factitious PTSD: Symptoms are being deliberately falsified by the patient for intrinsic gain, such as respect from peers or using the "victim" role to justify a poor level of functioning, like failed relationships or legal problems.
- Elevated PTSD: Symptoms are consistent with PTSD but seem exaggerated.
- Genuine PTSD: Symptoms are real and are consistent with a diagnosis of PTSD.
Misattributed PTSD
To spot misattributed PTSD, "The first thing you look to see is whether or not someone who is misidentified as having PTSD when there's a set of symptoms that are better explained by another diagnosis," he said.
For example, "Misattribution is very common in victims of trauma. You have a clinician bias -- 'Oh, they were in a war' -- that leads to an early PTSD diagnosis, when in fact the most common response to trauma is depression or anxiety. If it does [turn out to be] misattributed, you can address the underlying pathology instead of progressing down the PTSD treatment path, which is inappropriate and won't get optimal results. "
"
Once misattributed PTSD is ruled out, the clinician should look at the symptoms and say, 'Are they being volitionally produced or not?'" Matto continued. If they are being intentionally produced, "Physicians in the past have attributed it to malingering PTSD," but clinicians should dig deeper and see whether it's being produced for primary or secondary gain.
Only if it's produced for secondary gain -- external rewards such as getting out of legal responsibility in a criminal case -- is it actual malingering, according to Matto. For example, a patient might decide, "I was assaulted by an employee at WalMart; I'll sue WalMart and claim that I have PTSD as a result of the assault."
This is a common strategy in civil cases as well, he said. "The most accurate data seem to be that in 20%-30% of personal civil injury lawsuits, PTSD is falsely claimed." In the case of the Veterans Affairs health system, PTSD was the third most common disability claim by 2012.
How to Treat Malingering
As for malingering, "I get called in for challenging or diagnostically unclear cases, so probably see more of it than most," said Matto. Although it can be hard to address, "If someone's malingering it's because they want something. [For example] I have folks malingering for the sake of getting a pension, so I will say, 'You do not have PTSD but I can tell you're suffering; if it's because of financial need, let's see what resources I have to help with that.'"
Although it can be hard to address, "If someone's malingering it's because they want something. [For example] I have folks malingering for the sake of getting a pension, so I will say, 'You do not have PTSD but I can tell you're suffering; if it's because of financial need, let's see what resources I have to help with that.'"
If the patient is producing the symptoms for primary gain -- an intrinsic reason like getting to play the role of a sick person -- that's known as factitious PTSD. "This is very common in primary care physician offices -- people want the sort of sympathy that comes from being sick; they want to be pampered. They will inject insulin -- or even inject feces to make themselves septic."
"The main difference between factitious PTSD and malingered PTSD is that malingered PTSD is not a mental illness, while factitious PTSD is a psychopathology. Factitious disorder is recognized in the DSM, whereas malingering is not." The treatment for factitious PTSD is longitudinal psychotherapy, since one of the main motivations is unmet social need, he added.
There is real danger in not recognizing malingered PTSD, Matto noted. "If malingered PTSD isn't caught, then you get the stereotype of it being violent, since people are using it to get out of responsibility for committing crimes. "
"Also, not catching it calls into question legitimacy of the research database," he said. "That's because if you take a look at people's response rates to therapy or pharmaceutical interventions for PTSD, [those who malinger] never claim to get better. That makes the efficacy rates for different treatment modalities look worse than they are and people might be more reluctant to enter treatment."
Then there are the cases of elevated PTSD, in which patients have PTSD but appear to be volitionally producing symptoms. "Sometimes when you do psychological testing, the symptoms can appear amplified; that's something we need to be very cautious about," he said.
"Studies have found that a certain number of veterans seem to be overreporting their claims, but when you look a little deeper, they're not doing so for the sake of malingering; they're doing it as a cry for help . .. One study showed that of the evaluated claims, 23% appeared to be intentionally exaggerating their symptoms but 77% were actually a sign of distress. This requires careful calibration of neuropsychiatric testing to make sure we're not missing folks."
.. One study showed that of the evaluated claims, 23% appeared to be intentionally exaggerating their symptoms but 77% were actually a sign of distress. This requires careful calibration of neuropsychiatric testing to make sure we're not missing folks."
The Devil is in the Details
Matto suggests people depart from the traditional way of thinking about PTSD. "The traditional way has been to look [first] for signs and symptoms of malingered PTSD; I'm saying go the other way around -- look for genuine PTSD and if there's a deviation, see whether it's false PTSD or not."
This involves carefully going through the patient's medical records and look very closely at progress notes, rather than at case summaries, he said. "You really want to look at progress notes because you can get a day-by-day accounting of symptoms and create logs yourself to see how people are doing over time, and compare it with testing that may occur on particular days, or with symptom logs you give the patient. "
"
He also recommended looking at military records, in particular the DD-214 discharge form from the military. "It's a one-pager; it's not hard to fake," Matto said. "I recommend people request it directly from the [military's] National Personnel Records Center."
Also, when you're talking to patients about their about military service, try to get as much detail as possible, he said. "One stereotype physicians have about individuals with PTSD is that they don't want to talk about their military experience. They may not want to talk about traumatic experiences, but they should be able to talk about other details. if they were in the Navy, you can ask, 'What sort of boat were you on and where did you stop?'" Or you can ask about their uniform; if the response is "I wore my greens," the physician can ask what was on their utility belt. "We should ask for a lot of details."
In addition, "I always recommend they take a look for inconsistencies in their story between what they're describing and what they're demonstrating," said Matto. For example,"I'll [position] patients with their back to a door and while I'm talking to them" because a common sign of PTSD is being uncomfortable with having one's back to a door.
For example,"I'll [position] patients with their back to a door and while I'm talking to them" because a common sign of PTSD is being uncomfortable with having one's back to a door.
If the patient genuinely has PTSD, "they'll [immediately] see where the chair is and ask to move it," whereas a patient with false PTSD may seem fine until you start asking about their symptoms, and then they may remember about that being a symptom and will ask to move the chair.
Or they may say that their memory is terrible and they can't remember what happened the day of their trauma, but if you ask what day they filed a lawsuit they'll know the exact day and year. "Look for those inconsistencies," but also give them a chance to explain them because there may be a good reason for it, he said.
Please enable JavaScript to view the comments powered by Disqus.
How to distinguish the original TCP from a fake and not lose a car
Good day, dear readers!
After reading today's material, you will learn how to distinguish the original TCP from a fake on your own, if you do not have the opportunity to involve an expert in this matter.
When buying a car, of course, you check all the documents necessary for the seller to sell the vehicle (TC) in accordance with all the rules.
But unfortunately, this will not be able to completely protect you from fraudulent activities if they relate to the main document of the car - the vehicle passport (PTS). It can be faked by high-class crooks, whose work is sometimes very difficult to distinguish without special knowledge.
But using a fake PTS, they can sell you a stolen car, which is then necessarily confiscated by the traffic police, leaving you without money and a car. In the best case, such vehicles can be sold for spare parts. And if you try, in turn, to deliberately deceive another by reselling a problematic vehicle from a sick head to a healthy one, then you may be threatened with a prison, if the buyer does not believe in your innocence, he will contact the police.
Do you need it? I think no.
Contents
- 1 Fake TCP
- 2 Methods for determining fake TCP
- 2.
 1 Study of TCP using improvised means
1 Study of TCP using improvised means - 2.2 Study of TCP using special tools
- 2.2.1 Pocket microscope
- 2.2.2 Ultraviolet lamp
- 2.2 Infrared Detector
- 2.
- 3 Life Story
- 4 Helpful Tips
- 5 Conclusion
Counterfeit PTS
Many motorists will agree that counterfeiting of TCP is a very common occurrence, unfortunately. Such passports are used to provide a set of new documentation for criminal, auto-designers and simply for some reason not subject to registration of cars.
In the 1990s, a whole business was built on counterfeit titles, and anyone could, if desired, replace their documents with other fake ones for quite a reasonable amount. Maybe you remember those dashing times when there was a lot, as they say, “you can’t, but you can, if you really want to”?
But now, with the development of document security and authentication technologies, everything is much better in this respect, although it has not been possible to completely eliminate the forgery of car passports.
There are four main varieties of fake PTS:
- Simple double-sided printouts by a high-quality color printer, with a fake hologram sticker - such a “passport” can arouse suspicion even among the most inexperienced buyer, but still the method has not yet become obsolete and crooks find people ( mostly inexperienced women), who can be so artlessly deceived. Such fakes are easy to distinguish through the light or even by touch.
- Classic counterfeit PTS - here paper, paint of similar properties are already used, and a wider imitation of security markers is used. The level of forgery directly depends on the experience of the swindlers who make it. Very good imitations can be found. Such forgeries often need more detailed research to identify fraud.
- PTS on original forms is already a serious variant of fraud, sometimes capable of misleading not only drivers, but also some traffic police officers. The forms themselves can be purchased (from the black market of documents) or stolen from the State Sign.
 In the first case, forgery can be caught with the help of expert tools, and in the second, if a swindler competent in his business worked, only rechecking all the TCP data and the car itself in the traffic police can bring the deceit to clean water.
In the first case, forgery can be caught with the help of expert tools, and in the second, if a swindler competent in his business worked, only rechecking all the TCP data and the car itself in the traffic police can bring the deceit to clean water. - Original titles used for criminal purposes - this is the most difficult case to detect, since the package of documents for the car, which includes the passport, is not forged at all. The swindlers legally buy a broken car for nothing, supposedly for restoration, and then steal another vehicle that completely or almost completely corresponds to the parameters in the received TCP. Then segments of the body of a broken car with its marking are welded into the stolen car and legally sold, because according to the law, the vehicle can be sold without re-registration. Only traffic police experts will be able to determine such a fake.
However, the fact that in some cases it is very difficult to distinguish a forgery of the TCP does not at all eliminate the need to know the basic methods of authentication for simpler cases. Do you agree? I'm sure yes! Then let's join.
Do you agree? I'm sure yes! Then let's join.
Methods for detecting counterfeit PTS
Researching PTS using available tools
Well, let's examine the passport for the car and feel like a pro-expert.
If you do not have special equipment, then it does not matter - take these easily accessible tools with you for inspection:
- Ordinary small lantern;
- Powerful loupe with x10 magnification.
Attention! You should know that at a car inspection meeting, all obvious manifestations of haste on the part of the seller should be taken into account as an argument for a more thorough check of both the TCP and all other documentation and the car itself. With artificial excitement, scammers scatter the attention of their victim, remember this.
So, you have picked up the TCP.
Of course, pay attention to whether it is a duplicate or not.
However, if the document turned out to be a duplicate, then this does not mean that the owner has bad intentions. The duplicate of the vehicle passport, which I wrote about here, is just as legal as its original. Just ask about the reason for dubbing and, if the owner's arguments inspire confidence in you, proceed to further inspection:
The duplicate of the vehicle passport, which I wrote about here, is just as legal as its original. Just ask about the reason for dubbing and, if the owner's arguments inspire confidence in you, proceed to further inspection:
- The paper of the TCP blank must visually and to the touch correspond to all similar products from the State Sign.
- Run your thumb over the hologram: it should form a single whole with the main body of the document, without perceptible transition boundaries.
- Place a magnifying glass on the hologram: a car is depicted in its center, and there is a protective inscription on its windshield: “Russia. Russia". This inscription can only be seen with the naked eye (at least a 10X magnifier, and ideally a pocket microscope).
- Tilt the PRT at an angle of 30 (approximately) degrees and shine a flashlight on the upper left corner (the field above the hologram): “PTS” should appear on this field.
- Run your fingers over the main inscription "Vehicle Passport": it is made with three-dimensional embossing and this should be clearly felt when palpated.

- On the last page of the PTS, there is a protective rose pattern in the upper left corner. If you look at it from an acute angle, then it changes from green to gray. Run your finger over it - this pattern is also made with volumetric embossing and this should be felt.
- Unfold the passport and light it to check the watermarks (WZ): the “RUS” WA and asterisks should show through. Also, all fields to be filled in should be checked against the light: to detect possible so-called. rewashing - chemical reduction of original inscriptions and their replacement with fake data.
- There is a dark stripe on the line of the internal bend of the TCP reversal: if you look at it with a magnifying glass, you can see on the original that it consists of a closed microtext, which is very difficult to fake: “passport of a vehicle”.
- Pay attention to the year of manufacture of the form (lower left corner): if it is younger than the year the title was issued, then you have a clear fake.
- Pay attention to the series and number of the title. For imported cars, today only the first two letter identifiers are used: “T” and “U” (for example, 25 TV 684907, or 16 of the Criminal Code 654678). Also look at the first two digits of the series (they mean the regional code) and the place of issue of the passport (at the bottom of the title page) - they must comply with the logic (the Baltic customs cannot issue a PTS with the 25th code of the Far East). By the way, for VAZs, the regional code of the original is always 63.
PTS research using special tools
If you want to independently conduct an examination of an almost professional level, then it is possible to do this, but you will have to get something.
With the help of special tools, you can more reliably and easily determine the authenticity of a document. Such tools are quite affordable and available in wide retail.
These are:
- Pocket microscope;
- UV flashlight;
- Infrared detector.
You may already have some of these. Then great! But even if you decide to purchase these things, they will come in handy more than once in other everyday cases or just for fun: look at a bug under a microscope or take a picture of something at night in the infrared range - interesting? Yes, for me!
Pocket microscope
This is a relatively inexpensive, small and light household instrument for studying various small elements, giving an optical magnification of up to 100x.
With its help, the clarity of the hologram pattern, as well as the number/series of the PTS are examined: they are applied with red-gold paint and corrections made are clearly visible under a pocket microscope in case of washing out of the original inscriptions.
This device is also used to study the background texture pattern (which should not lose clarity at high magnification) and the system of protective fibers embedded in the paper (it is noticeable that multi-colored short threads are embedded in the middle of the paper, and not applied to its surface).
UV flashlight
Under its radiation, the entire protection of the document is clearly visible with the help of markers invisible in normal light, which is very helpful if the transaction is carried out in a dark place and it is difficult to check the TCP through the light.
Expose your passport to UV radiation: in its light, security threads (fibers) will clearly appear throughout the field of the document. They will glow in a three-color spectrum: PTS uses randomly arranged fibers of the three primary colors of the spectrum.
By the way, with this flashlight you can quickly check any banknotes (and not only them) for authenticity. A very useful device in everyday life and not expensive besides.
Infrared Detector
This is a compact device equipped with an infrared CMOS camera that displays a very clear infrared image, which can distinguish even the smallest fragments.
If you point this detector at some PTS inscriptions, then in its light all the corrections made or complete false data replacements will be clearly visible: a trace of washed out characters will appear. Also, if you point the detector at the drawing of the car in the upper right corner of the first spread and the upper left corner of the second, then in infrared light the car will disappear.
Also, if you point the detector at the drawing of the car in the upper right corner of the first spread and the upper left corner of the second, then in infrared light the car will disappear.
Such a tool costs decently (at the level of a mid-budget tablet), but many additional functions are included in its functionality: from games to various multimedia features, so it will not lie dead weight.
If you want to know more details, then watch this video, where a professional expert in automotive documentation reveals his secrets to the respected AvtoLise:
Life story
In conclusion, dear friends, I will tell you one useful story.
One day my friend bought a car, the title of which he did not check for authenticity, although he considered himself an experienced car owner who bought and sold more than one “wheel”. The passport was filled with several resale re-registrations and this misled him. He thought: well, in the MREO this TCP was checked several times for authenticity when the new owners applied, so everything should be OK here.
The passport was filled with several resale re-registrations and this misled him. He thought: well, in the MREO this TCP was checked several times for authenticity when the new owners applied, so everything should be OK here.
Logical, isn't it?
But upon re-registration in Moscow, the falsification of the document was immediately revealed. What is the matter here?
And the fact that scammers sometimes resort to a tricky trick: they find some kind of regional MREO, where they approach the examination carelessly (unfortunately, there are still such) and make a “history” of the car there, making several fictitious sales transactions with valid registrations.
It happens that attackers in this way even manage to get even a genuine duplicate instead of the “lost original”. Therefore, be vigilant, paying attention not only to the number of owners, but also to the frequency of their change in the TCP.
For example, if a car has been visited by several owners in a year, and the technical inspection did not give any particular complaints, then such a car is extremely suspicious of criminality - it could be a theft with false documentation!
Useful tips
- You should keep in mind that before 1996 the traffic police also issued original titles, so the legality of all cars imported before this year may be in doubt, but there is no way to determine this for sure.
- Keep in mind that sometimes in the regional traffic police of small settlements in the state there are temporarily or permanently no expert experts and you may get a car that has already successfully re-registered by authorities with a “successful” examination of a fake title.
- Be wary of suspicious cars somehow connected with the Baltic States, where they traditionally deal with professional forgery of car documents and generally legalization of cars, including criminal ones.
- By the way, some modern smartphones and cameras are prudently equipped by manufacturers with ultraviolet illumination and an infrared filter that can be turned on, which will not only help in identifying fakes, but also allow you to take interesting photos in almost complete darkness.
Conclusion
Now you know that there are four types of TCP forgeries and not all of them can be checked on your own, but forgeries related to the structure of the document, with the help of modern security technologies and its identification, are detected quite easily even at the level of an ordinary motorist.
Have you had any interesting cases related to checking the authenticity of the TCP? Tell us about it in the comments, which will undoubtedly arouse the interest of many motorists.
That's all for today, dear friends, expect new publications and feel free to subscribe to the blog. Share the most interesting through social buttons and bring your own drive to the information space of Runet!
Be vigilant with documents and on the roads!
How to check the vehicle passport for authenticity
Hello! Each driver must have not only a license, but also the necessary documents for the car. Among them, PTS deserves special attention. That is the passport of the vehicle. The only problem is that this document is often forged, and illegal data and signatures are also introduced. It is the signature that is of great importance in this matter. Therefore, you should learn how to distinguish a real signature in the PTS from a fake.
We will separately consider the issue of falsification of the document itself, as well as responsibility for such manipulations with official papers.
Corresponding entries in the PTS are made when buying a car, as well as when registering it with the traffic police.
It is necessary to understand for what purposes signatures and the TCP itself are forged, how to recognize fraud, and what consequences one should be prepared for.
Counterfeit Title
Many motorists will agree that counterfeit Title is a very common occurrence, unfortunately. Such passports are used to provide a set of new documentation for criminal, auto-designers and simply for some reason not subject to registration of cars.
But now, with the development of document security and authentication technologies, everything is much better in this respect, although it has not been possible to completely eliminate the forgery of car passports.
There are four main varieties of counterfeit TCPs:
However, the fact that in some cases it is very difficult to distinguish a fake TCP does not at all eliminate the need to know the basic authentication methods for simpler cases. Do you agree? I'm sure yes! Then let's join.
Do you agree? I'm sure yes! Then let's join.
Visual inspection
Now that it has become clear what papers a person has to deal with, it is possible to study the direct difference between the original and a duplicate of the car's technical passport. This is by no means the most difficult task of all.
Recommended! How many days are given to register the car from the date of purchase
The first thing you need to pay attention to is the appearance of the document. Duplicate documents visually look new. The old TCP does not give the impression of a freshly printed form. This moment may help to understand what is happening.
Suspicion should be raised by the original technical data sheets of old cars, which visually look like they were recently printed. It's most likely a fake.
Methods for detecting counterfeit PTS
Investigation of PTS using improvised means
If you do not have special equipment, then it does not matter - take these easily accessible tools with you for inspection:
Attention! You should know that at a car inspection meeting, all obvious manifestations of haste on the part of the seller should be taken into account as an argument for a more thorough check of both the TCP and all other documentation and the car itself.
With artificial excitement, scammers scatter the attention of their victim, remember this.
So you've picked up the TCP.
Of course, pay attention to whether it is a duplicate or not.
However, if the document turned out to be a duplicate, then this does not mean that the owner has bad intentions. The duplicate of the vehicle passport, which I wrote about here, is just as legal as its original. Just ask about the reason for the dubbing and, if the owner's arguments inspire confidence in you, proceed to further examination:0067
If you want to do your own near-professional due diligence, it's possible to do so, but you'll need to get some supplies.
With the help of special tools, you can more reliably and easily determine the authenticity of a document. Such tools are quite affordable and available in wide retail.
Here's what they are:
You may already have some of these. Then great! But even if you decide to purchase these things, they will come in handy more than once in other everyday cases or just for fun: look at a bug under a microscope or take a picture of something at night in the infrared range - interesting? Yes, for me!
Pocket microscope
This is a relatively inexpensive, small and light household instrument for studying various small elements, giving an optical magnification of up to 100x.
With its help, the clarity of the hologram pattern, as well as the number/series of the PTS are examined: they are applied with red-gold paint and corrections made are clearly visible under a pocket microscope in case of washing out of the original inscriptions.
This device is also used to study the background texture pattern (which should not lose clarity at high magnification) and the system of protective fibers embedded in the paper (it is noticeable that multi-colored short threads are embedded in the middle of the paper, and not applied to its surface).
UV flashlight
Under its radiation, the entire protection of the document is clearly visible with the help of markers invisible in normal light, which is very helpful if the transaction is carried out in a dark place and it is difficult to check the TCP through the light.
By the way, with this flashlight you can quickly check any banknotes (and not only them) for authenticity. A very useful device in everyday life and not expensive besides.
Infrared Detector
This is a compact device equipped with an infrared CMOS camera that displays a very clear infrared image, which can distinguish even the smallest fragments.
If you point this detector at some PTS inscriptions, then in its light all corrections made or complete false data replacements will be clearly visible: a trace of washed out characters will appear. Also, if you point the detector at the drawing of the car in the upper right corner of the first spread and the upper left corner of the second, then in infrared light the car will disappear.
Such a tool costs decently (at the level of a mid-budget tablet), but many additional functions are included in its functionality: from games to various multimedia features, so it will not lie dead weight.
If you want to know more details, then watch this video, where a professional expert in automotive documentation reveals his secrets to the respected AvtoLissa:
How to distinguish a fake
the moment of buying a car fake title is not so easy. Moreover, some of the fake forms are of such high quality that not every MREO of the traffic police is able to identify a fake. However, the purchase of a used car should certainly be accompanied by a thorough study of the document provided.
Moreover, some of the fake forms are of such high quality that not every MREO of the traffic police is able to identify a fake. However, the purchase of a used car should certainly be accompanied by a thorough study of the document provided.
It is quite easy to identify a duplicate TCP, in terms of its differences from the original. In the case of a fake, the matter is complicated - often on a fake duplicate of the TCP there are basic security elements in the form of watermarks and holograms. Therefore, before buying, you should carefully evaluate the TCP for some points.
- Watermarks. A real PTS is characterized by a slight blurring of watermarks, while fakes are distinguished by exceptionally even, clear inscriptions.
- Hologram. If the duplicate TCP is fake, the hologram will be dimmer and will only be reflected at certain angles. A real hologram is always distinguished by exceptional brilliance. In addition, the stars on the original are smaller in size than on the fake.
- Embossed lettering. On a fake, it is very rare to find an inscription that is determined by touch.
- Paper quality. A real PTS is slightly rough, a fake is often made on thicker and smoother paper.
Life story
In conclusion, dear friends, I will tell you one useful story.
Logical, isn't it?
But upon re-registration in Moscow, the falsification of the document was immediately revealed. What is the matter here?
And the fact that scammers sometimes resort to a tricky trick: they find some kind of regional MREO, where they approach the examination carelessly (unfortunately, there are still such) and make a “history” of the car there, making several fictitious sales transactions with valid registrations.
It happens that attackers in this way even manage to get even a genuine duplicate instead of the “lost original”. Therefore, be vigilant, paying attention not only to the number of owners, but also to the frequency of their change in the TCP.
For example, if a car has been visited by several owners in a year, and the technical inspection did not give any particular complaints, then such a car is extremely suspicious of criminality - it could be a theft with false documentation!
Characteristic features of the original
Now to the question of how to distinguish a fake TCP.
PTS is a special document that has a regulated design, is printed only by authorized organizations, and also differs in a number of elements.
If we talk about how to identify a fake TCP, then you need to know the signs of this document. The original consists of:
- series and numbers;
- vehicle VIN;
- full name of the vehicle;
- vehicle category;
- machine production;
- model and engine numbers;
- chassis and body serial number;
- body color;
- motor power;
- environmental class;
- permitted maximum weight;
- organization-manufacturer of the vehicle;
- other data.
In Russia, there is a single standard and format for all TCPs. If you know all its features, this will avoid problems with fakes. That is, you will be able to figure out how to distinguish a fake TCP from the original without any problems.
"Fake PTS and TS" They said in the traffic police
Yesterday there was an unpleasant situation. Bought a Mazda 6 2007 September 16 and went 26 to put on record.
While inspecting the car, the specialist looked at the VIN markings for a long time and announced suspicions of brokenness. In addition, they told me that the TCP looked like a fake one. From the observation deck, together with a representative of the traffic police, we moved to the department, where we drove the car into the box for examination. On another review of the documents, I was informed that the STS was also fake. I was asked to wait half an hour for an examination, my request for my presence was refused, referring to the ban on being there for safety reasons.