Can i take antidepressants while pregnant
Antidepressants and Pregnancy: Tips from an Expert
Most pregnant women want to do everything right for their baby, including eating right, exercising regularly and getting good prenatal care. But if you’re one of the many women who have a mood disorder, you might also be trying to manage your psychiatric symptoms as you prepare to welcome your new baby.
It’s common for doctors to tell women with mood disorders to stop taking drugs like antidepressants during pregnancy, leaving many moms-to-be conflicted about giving up the medications that help keep them healthy.
Lauren Osborne, M.D., assistant director of the Johns Hopkins Women’s Mood Disorders Center, talks about why stopping your medication may not be the right approach. She explains how women can — and should — balance their mental health needs with a healthy pregnancy.
Antidepressants and Pregnancy
Women who take antidepressants, such as selective serotonin reuptake inhibitors (SSRIs), during pregnancy may worry about whether the medications can cause birth defects.
There is good news on this front. Osborne says that there is generally no need to taper off medications during pregnancy. “We can say with strong confidence that antidepressants don’t cause birth defects,” says Osborne. She adds that most studies finding a physical effect on babies from antidepressants taken during pregnancy fail to account for the effects of the mother’s psychiatric illness.
In fact, untreated mental illness itself poses risks to a developing fetus. A woman who is depressed is less likely to get good prenatal care and more likely to engage in unhealthy or dangerous behaviors, like smoking and substance abuse. Osborne also says mental illness has direct effects on newborn babies.
“Untreated depression may increase preterm birth or cause low birth weight,” she says. “Babies of depressed moms have higher levels of a hormone called cortisol. This raises a baby’s risk of developing depression, anxiety and behavioral disorders later in life.”
Weighing the Risks
While doctors don’t believe antidepressants cause birth defects, it’s still possible for them to affect the baby. It’s important for a mother and her doctor to know the risks.
It’s important for a mother and her doctor to know the risks.
About 30 percent of babies whose mothers take SSRIs will experience neonatal adaptation syndrome, which can cause increased jitteriness, irritability and respiratory distress (difficulty breathing), among other symptoms. Doctors aren’t sure whether this effect is due to the baby’s withdrawal from the SSRI after birth or exposure to the drug itself before birth.
“It may be distressing and cause pediatricians to run tests, but it will go away,” says Osborne, pointing out that these symptoms also sometimes occur in babies whose mothers don’t take SSRIs.
Common medications women frequently ask about include:
- SSRIs: Some studies link SSRI use with a very rare defect called persistent pulmonary hypertension, which is a condition where babies’ lungs don’t inflate well. “The most recent study looked at 3.8 million women and showed there was no increase in risk to their babies,” says Osborne.

- Paroxetine: Early studies on a small number of patients connected the SSRI paroxetine with cardiac defects in babies. However, these studies didn’t account for smoking, obesity and other risk factors that are more common in women who have depression. Osborne says larger, more recent studies show no such link with cardiac defects. She doesn’t recommend switching medications if paroxetine is the only one that works for you.
- Benzodiazepines: Women should avoid using tranquilizers, such as diazepam, alprazolam and clonazepam, in high doses during pregnancy because they can lead to sedation and respiratory distress in the newborn. You can still use them in small doses for short periods of time. However, Osborne will typically try to get mothers on intermediate-acting options like lorazepam. These medications don’t linger in the baby’s bloodstream like longer-acting forms and aren’t associated with high rates of abuse like shorter-acting forms.
- Valproic acid: This medication treats seizures and bipolar disorder, and does carry significant risk to a developing fetus. Taking valproic acid during pregnancy carries a 10 percent risk of neural tube defects — birth defects that affect the brain or spinal cord, such as spina bifida — as well as risks to the baby’s cognitive development, such as lower IQ. “Valproic acid is the only one I’d never prescribe for pregnant women unless all other treatment had failed,” says Osborne .
Seeing a Reproductive Psychiatrist
If you have a mood disorder, you may benefit from speaking with a reproductive psychiatrist when you are pregnant or thinking about becoming pregnant. Ideally, this should happen when you are planning for pregnancy, although this isn’t always possible. Meeting with a doctor after you become pregnant is not too late.
Osborne says her approach with patients is to limit the number of potentially harmful exposures to the baby. This means considering the number of medications a mother is on, as well as her psychiatric illness.
This means considering the number of medications a mother is on, as well as her psychiatric illness.
“If a woman takes a low dose of many medications and we have time to plan, we’ll try to get that down to a higher dose of fewer medications,” she says. “If a woman is on a low dose and it’s not controlling her illness, then her baby is exposed to both the medication and the illness. In that case, I would increase the medication dosage so her baby isn’t exposed to the illness.”
If your illness is mild, your doctor might recommend getting off medication and replacing it with treatments such as psychotherapy, prenatal yoga or acupuncture to improve your mood.
Ultimately, Osborne says women should weigh the risks of medication against the risk of untreated illness.
“If a particular side effect is extremely rare, it’s still a very rare event even if you double the risk,” she says. Medication risks are typically not greater than those of untreated mental illness. “Switching a woman’s medication is something I do very carefully and reluctantly. ”
”
Pregnancy and Antidepressants
Written by Hedy Marks
In this Article
- Depression and Pregnancy
- Pregnancy and Antidepressants: What the Experts Say
- Pregnancy and Untreated Depression
- Pregnancy and Antidepressants: Understanding the Risks
- Antidepressants and Pregnancy: Keeping Risks in Perspective
- Pregnancy and Antidepressants: Medication Options
- Pregnancy and Antidepressants: What to Do?
Deciding to continue or stop using antidepressants during pregnancy is one of the hardest decisions a woman must make. Untreated depression can have harmful effects on both the mother and the baby. But, taking antidepressants while pregnant may increase the risk of problems for the baby.
When making the decision, it’s important to consider your health, the health of your unborn child, and the well-being of your family, including your other children. It’s also important to not make the decision before discussing it with your doctors.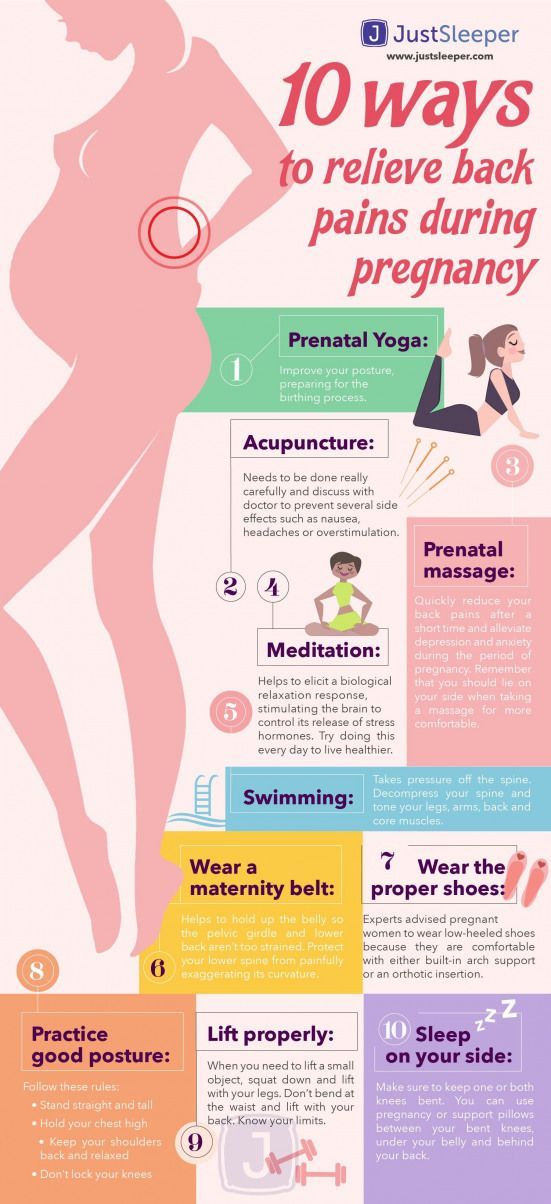 That includes the ob-gyn and the psychiatrist. Together, you can weigh the pros and cons of continuing or stopping your medication and make the right decision for you.
That includes the ob-gyn and the psychiatrist. Together, you can weigh the pros and cons of continuing or stopping your medication and make the right decision for you.
Depression and Pregnancy
Many women battle depression and need antidepressants to manage their symptoms. In the past, it was thought that pregnancy protected against depression. But scientists now realize this is not the case. More and more women are taking antidepressants while pregnant to keep their symptoms in check. One study found that between 1998 and 2005, nearly one out of every 20 women reported using an antidepressant three months before becoming pregnant or during the pregnancy.
There are questions about the safety of taking antidepressants when you are pregnant. But research is showing that most antidepressants, especially the selective serotonin reuptake inhibitors (SSRIs) and older medications, are generally considered safe. Birth defects and other problems are possible. But the risk is very low.
Pregnancy and Antidepressants: What the Experts Say
Both psychiatric experts and ob-gyn experts agree that if you have mild depression and have been symptom-free for at least six months, you may be able to stop using antidepressants under a doctor’s supervision before getting pregnant or while you are pregnant. Psychotherapy, along with lifestyle measures, may be all that you need to manage your depression. You may be able to get through your pregnancy without antidepressants if you:
- Talk with a therapist on a regular basis
- Exercise more
- Spend time outside
- Practice yoga and meditation
- Minimize your stress
But, the experts point out, it will be better for both you and your baby to stay on antidepressants while pregnant if any of the following is true:
- You have a history of severe or recurrent depression
- You have a history of other mental illnesses, such as bipolar disorder
- You have ever been suicidal
Pregnancy and Untreated Depression
Left untreated, depression can have far reaching effects on both your and your baby’s health. Women who are depressed are less likely to take proper care of themselves. For instance, they may not eat a healthy diet or may skip doctors’ appointments. Plus, women who are depressed may be more likely to take part in risky behaviors, such as drinking alcohol, smoking, or taking drugs during pregnancy. All of these actions can lead to potentially serious health problems for the baby, including miscarriage, preterm birth, and low birth weight.
Women who are depressed are less likely to take proper care of themselves. For instance, they may not eat a healthy diet or may skip doctors’ appointments. Plus, women who are depressed may be more likely to take part in risky behaviors, such as drinking alcohol, smoking, or taking drugs during pregnancy. All of these actions can lead to potentially serious health problems for the baby, including miscarriage, preterm birth, and low birth weight.
Untreated depression can also take a toll on family dynamics. That includes your relationship with your spouse and other children. If you have older kids, they need you to care for them. For some pregnant women, regardless of their mental state, it can take all the energy they have to care for themselves. Add depression to the mix, and the suffering can become intolerable for everyone. If depression is preventing you from caring for your family, you may need to stay on your antidepressants during this vulnerable time.
Pregnancy and Antidepressants: Understanding the Risks
Few, if any, medications are considered absolutely safe during pregnancy. Research findings on the effects of antidepressants on the growing baby are mixed and inconclusive. One study may find a particular antidepressant causes one type of risk. Another one, though, may find that it doesn’t. Also, the risks to the baby may be different depending on the type of antidepressant and when in the pregnancy it is taken. Regardless, most risks found by researchers have been low.
Research findings on the effects of antidepressants on the growing baby are mixed and inconclusive. One study may find a particular antidepressant causes one type of risk. Another one, though, may find that it doesn’t. Also, the risks to the baby may be different depending on the type of antidepressant and when in the pregnancy it is taken. Regardless, most risks found by researchers have been low.
Reported risks for the baby include:
- Persistent pulmonary hypertension in the newborn (PPHN), a serious condition of the blood vessels of the lungs.
- Miscarriage
- Heart defects
- Birth defects, including anencephaly (affecting the spinal cord and brain), craniosynostosis (affecting the skull), omphalocele (affecting the abdominal organs), and limb malformation
- Preterm birth (being born before 37 weeks gestation)
- Low birth weight (being born less than 5 pounds, 8 ounces)
- Low Apgar scores
In addition, babies exposed to antidepressants in the womb may experience withdrawal symptoms, such as:
- Breathing problems
- Jitteriness
- Irritability
- Trouble feeding
- Low blood sugar (hypoglycemia)
- Poor tone
Some required a short stay (one to four days) in the neonatal intensive care unit. None of these symptoms is thought to cause any long-term harm to the baby.
None of these symptoms is thought to cause any long-term harm to the baby.
The long-term impact of antidepressant exposure on development and behavior is still unclear. But, studies have not found a significant difference in IQ, behavior, mood, attention, or activity level in children who were exposed to antidepressants in the womb.
Antidepressants and Pregnancy: Keeping Risks in Perspective
It‘s important to keep the reported risks associated with antidepressant use in pregnancy in perspective. All pregnant women have an average 3% risk of having a baby with any type of birth defect in most cases. When researchers say antidepressants may increase the risk of certain birth defects, they are talking about just a slight increase. For example, one study showed that antidepressants increased the risk that the baby would be born with PPHN by 1%. So, even if you take an antidepressant during pregnancy, the overall risk of your baby having a problem is still very low. Other studies showed different levels of risk associated with antidepressants and PPHN, and 1% is on the high end.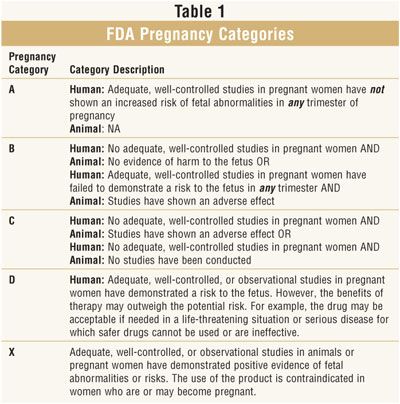 So the risk may be even lower.
So the risk may be even lower.
Pregnancy and Antidepressants: Medication Options
Some antidepressants are considered safer for pregnant women than others. Antidepressants that are considered safer include:
- Amitriptyline (Elavil)
- Bupropion (Wellbutrin)
- Citalopram (Celexa)
- Desipramine (Norpramin)
- Fluoxetine (Prozac, Sarafem)
- Nortriptyline (Pamelor)
- Sertraline (Zoloft)
But if you are pregnant and taking an antidepressant that is not on this list, do not worry. Even the more controversial ones, including paroxetine (Paxil), have relatively low risk. Changing medications mid-pregnancy poses its own set of problems. Talk to your doctor and see what they think would be best for you.
If you are not pregnant but planning on becoming pregnant, it may be worth trying a different medication if you are concerned about the safety of your current antidepressant. Again, talk to your doctor to see if this is a good option for you.
Pregnancy and Antidepressants: What to Do?
No matter how small the risk, no mother wants to unnecessarily expose their baby to medicine. Making the decision to take or stop taking antidepressants in pregnancy is not easy. There is no right answer. You must look at your own set of circumstances and make the decision based on the risks and benefits unique to you. If you and your doctor think you may be able to stop your medication during pregnancy, it is certainly worth a try. But, never stop taking your medication without talking to your doctor first. Most antidepressants require weaning to safely stop the drug. If you need to stay on an antidepressant while you are pregnant, don't panic. Remember, the risks associated with most of the antidepressants in pregnancy are extremely low. Untreated depression could pose a greater risk.
Whatever you finally decide to do, do not second-guess yourself. Once you make the decision, accept it and move on. Trust yourself and your doctors. Like you, your doctors want the very best possible outcome -- a healthy mom and baby.
Like you, your doctors want the very best possible outcome -- a healthy mom and baby.
FGBNU NTsPZ. ‹‹Depression in General Medicine: A Guide for Physicians››
The choice between the need for pharmacotherapy, on the one hand, and the prevention of risks to the health of the fetus or newborn (the risk of congenital malformations, pre- and neonatal complications, etc.) on the other, is required from the doctor in case of depression that manifests or worsens during the period pregnancy.
When deciding on such an alternative (the proportion of benefit to the mother and the potential risk to the child), a number of circumstances are taken into account, including the possibility of a negative impact on the development of the fetus by the mother's severe mental state during pregnancy. nine0003
Psychotropic drugs for pregnant women are prescribed if absolutely necessary according to strict clinical indications:
- with pronounced affective manifestations with anxiety, agitation, sleep and appetite disorders, aggravating the somatic condition of pregnant women and women in childbirth;
- with suicidal thoughts and tendencies.
However, in some cases, such as unplanned pregnancy, antidepressants are taken out of ignorance - a depressed woman, not yet aware of the pregnancy, may continue to take psychotropic drugs and be exposed to them. nine0003
Penetrating through the placenta or with mother's milk, psychotropic drugs can have an adverse effect on the fetus or newborn. Microsomal enzymes of the fetal liver are less active and are in a lower concentration compared to the liver of adults, which prolongs and enhances the effect of drugs. In the prenatal period, the blood-brain barrier is not yet fully formed and the immature CNS is generally more sensitive to the action of drugs. At the stage of embryogenesis, as well as in the early postnatal (neonatal) period of ontogenesis, the development of these vital structures is not completed, which can enhance the toxic effect of psychotropic drugs on both the fetus and the newborn. Such effects include potentially reversible, dose-dependent effects that may be exacerbated by the fact that metabolic systems have not yet fully formed. The constant use of drugs by a pregnant woman can lead to drug dependence of the fetus and, ultimately, to a withdrawal syndrome in the newborn [Vybornykh D. E., 1996].
The constant use of drugs by a pregnant woman can lead to drug dependence of the fetus and, ultimately, to a withdrawal syndrome in the newborn [Vybornykh D. E., 1996].
During lactation, taking antidepressants due to the possibility of the neonatal complications listed above is also highly undesirable. The mother should be convinced that in this situation it is more appropriate to feed with donor milk or artificial mixtures.
Differentiation of antidepressants in accordance with the degree of risk of developing toxic effects for infants fed by a mother taking psychotropic drugs of this class is shown in Table. 16. nine0003
Table 16 Risk of developing toxic effects in infants breastfed by mothers taking antidepressants
| Level of risk | ||
| short | average | tall |
| Mianserin | SSRI | Doxepin |
| TCAs (majority) | ||
When deciding on the use of antidepressants during pregnancy, it is necessary to take into account data on the risk of teratogenic effects of antidepressants. A teratogenic effect of antidepressants cannot be completely ruled out from data obtained from laboratory animals and from some very limited clinical observations. nine0003
A teratogenic effect of antidepressants cannot be completely ruled out from data obtained from laboratory animals and from some very limited clinical observations. nine0003
There are 3 classes of teratogenicity of psychotropic drugs: class A - no teratogenicity in animals, no studies of the risk of teratogenicity in humans, or teratogenicity in animals has been established, but not in humans;
class B - known to be teratogenic in animals, no risk of teratogenicity in humans, or no risk of teratogenicity in animals or humans;
class B - teratogenicity has been proven, but the benefits associated with prescribing drugs sometimes outweigh the risks (eg, in a life-threatening situation). nine0003
The distribution of drugs by teratogenicity classes is presented in Table. 17. Data are given for the first trimester of pregnancy.
Table 17. Distribution of psychotropic drugs by teratogenicity class Psychotropic Drug Directory, 1997]
| Teratogenic class | ||
| AND nine0003 | B | AT |
| SSRIs: fluoxetine (Prozac), paroxetine (Paxil), sertraline (Zoloft) | TCAs: imipramine (melipramine), clomipramine (anafranil), desipramine (petylyl), doxepin (sinequan) | TCAs: amitriptyline, nortriptyline |
| Tranquilizers: chlordiazepoxide (Elenium), alprazolam (Xanax), diazepam (Relanium), lorazepam (Ativan), oxazepam (Nozepam) nine0003 | ||
| Antipsychotics: butyrophenone and phenothiazine derivatives, risperidone | ||
| SSOZS: tianeptine (coaxil)* | Normotimics: lithium preparations | |
| Tranquilizers: clonazepam (antelepsin) | ||
| Antipsychotics: clozapine (azaleptin) | ||
 N., 1995; Winn, 1995; Stowe Z. N., Nemeroff S. V., 1996; Yoshida K. et al., 1997; Piontek C. M., 2001].
N., 1995; Winn, 1995; Stowe Z. N., Nemeroff S. V., 1996; Yoshida K. et al., 1997; Piontek C. M., 2001].  The use of psychotropic drugs in such cases is also the prevention of postpartum depression. nine0003
The use of psychotropic drugs in such cases is also the prevention of postpartum depression. nine0003 | Share
There have been two independent studies showing that a woman taking antidepressants during pregnancy does not significantly affect her child's risk of developing autism. Other risk factors were also taken into account. nine0003 The authors of the studies believe that if a woman is indicated for appropriate medications to support her mental health, she should take them. Depression in a woman during pregnancy can be dangerous for both the mother and the baby. Initial studies in this area have linked antidepressant use in the first trimester of pregnancy with the development of autism spectrum disorder in children, thereby calling into question the prescription of these drugs to pregnant women. Two independent teams of researchers from Canada and Sweden questioned the data from the original studies because of the possible lack of work to exclude other factors that influence the development of autism in children. The Canadian study included 36,000 children, more than 2,800 of whom were exposed in utero to antidepressants taken by their mothers. At the same time, 2% of these children were diagnosed with autism. A comparative analysis was conducted on the basis of 500 different indicators of life and health between those who took antidepressants during pregnancy and those who did not take them. Another group of researchers from Sweden conducted a similar study on 1.5 million Swedish children. Additionally, work was carried out to analyze the fact of taking antidepressants by the fathers of children during their prenatal development. Both groups of researchers came to the same conclusion - an increased risk of developing autism in children when mothers take antidepressants during pregnancy is not confirmed by in-depth detailed analysis and taking into account other risk factors for developing autism. Swedish scientists also found no evidence for the assumption of an increased risk of attention deficit hyperactivity disorder (ADHD) in children. Concerns about the use of antidepressants initially arose in the medical community due to the fact that the drugs could cross the placenta and enter the brain of the fetus, potentially affecting future development. However, genetic predisposition also very likely plays a large role in the risk of developing autism. It is known that diseases such as autism, depression, nervousness and some other mental conditions are associated with the same groups of genes. It is likely that the high risk of developing autism in children whose mothers took antidepressants during pregnancy is due to a genetic predisposition, and not in connection with the use of antidepressants. It should also be taken into account that depressive states are often accompanied by bad habits, lack of sleep and unhealthy diet. nine0003 The scientists also confirmed that the studies carried out are not the last in this area, and additional work is required for the evidence base. According to the website https://www.    Copyright © · The Wright Initiative · Articles · Site Map 
|
 Depression during pregnancy without proper treatment can result in more severe postpartum depression for a woman, and also increases the likelihood of premature birth and / or low birth weight babies.
Depression during pregnancy without proper treatment can result in more severe postpartum depression for a woman, and also increases the likelihood of premature birth and / or low birth weight babies.  The researchers also analyzed data on siblings whose mothers took antidepressants during each pregnancy, or during individual pregnancies. Additionally, work was carried out to analyze the health status of those women who stopped taking previously prescribed antidepressants with the onset of pregnancy, those who continued taking them, and those who never took these drugs. nine0003
The researchers also analyzed data on siblings whose mothers took antidepressants during each pregnancy, or during individual pregnancies. Additionally, work was carried out to analyze the health status of those women who stopped taking previously prescribed antidepressants with the onset of pregnancy, those who continued taking them, and those who never took these drugs. nine0003  nine0003
nine0003