Atypical antidepressants list
Atypical Antidepressants - MHA Screening
Atypical antidepressants are antidepressants that don’t fall under any of the 4 main classes of antidepressants. They’re most often prescribed if you’ve tried other types of antidepressants, and they didn’t work for you. But they can also be used as a first-line treatment, depending on your symptoms and whether you are experiencing other mental health conditions in addition to depression.
Like other mental health medications, they work by restoring the balance of the chemicals in your brain (neurotransmitters). Each medication works on different chemicals and affects them differently.
Bupropion (brand names: Wellbutrin, Zyban)
Bupropion might be the most “atypical” antidepressant on this list. Unlike most antidepressants, bupropion has no effect on serotonin. Instead, it boosts dopamine and norepinephrine, two other neurotransmitters that affect energy level, motivation, and attention.
Doctors often prescribe bupropion to target specific symptoms, like oversleeping, weight gain, and fatigue [1]. It can also help improve concentration in people with depression and/or ADHD [2]. It also helps people quit smoking [3].
Many antidepressants can decrease a person’s sex drive and lead to drowsiness and weight gain. Bupropion is unlikely to do any of these things—in fact, it is often prescribed alongside another antidepressant to counteract these side effects [1].
However, bupropion can have its own side effects. Common ones include:
- Dry mouth
- Trouble sleeping
- Headache and nausea
- Weight loss
More rarely:
- Restlessness or anxiety
- Constipation
- Congestion
- Dizziness and fatigue
Trazodone
Trazodone is an antidepressant, but it is commonly prescribed for sleep problems, such as trouble sleeping or nightmares due to PTSD [4].
Like many other antidepressants, it works by boosting serotonin levels in the brain. It is less likely than many antidepressants to cause symptoms such as sexual dysfunction, insomnia, or anxiety.
Common side effects include:
- Headaches and fatigue
- Drowsiness and sleepiness
- Dry mouth
- Dizziness or fainting
- Rarely, hallucinations or irregular heartbeat
Some of these side effects go away after the first week or so of taking trazodone.
Mirtazapine (brand name: Remeron)
Mirtazapine works boosting both serotonin and norepinephrine, a neurotransmitter that affects energy levels. It helps with depression but also improves sleep. It may work more quickly than most antidepressants. It’s being studied for potential use in anxiety disorders and other mental health conditions as well [5].
Mirtazapine is unlikely to have any negative sexual side effects. Possible side effects include:
- Increased appetite and weight gain (this may be a positive thing, if you are already underweight or have an eating disorder)
- Dry mouth
- Sleepiness and fatigue
Vortioxetine (brand names: Trintellix, Brintellix)
Vortioxetine is a newer medication (approved by the FDA in 2013). Although it’s considered “atypical,” it has a similar effect to many other antidepressants [6]. It works by boosting serotonin levels in the brain.
Although it’s considered “atypical,” it has a similar effect to many other antidepressants [6]. It works by boosting serotonin levels in the brain.
Common side effects include nausea, constipation, and vomiting. More serious side effects are rare, but may include:
- Serotonin syndrome
- Increased bleeding or bruising when injured
- Hypomania
- Changes in vision, or swelling or pain near the eyes
- Low sodium levels
Show References
- Patel et al. (2016). Bupropion: a systematic review and meta-analysis of effectiveness as an antidepressant. Therapeutic Advances in Psychopharmacology 6(2), pp. 99–144. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4837968/
- Acheson & de Wit. (2008). Bupropion improves attention but does not affect impulsive behavior in healthy young adults. Experimental and Clinical Psychopharmacology, 16(2), 113–123. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4270475/
- Holm & Spencer.
 (2000). Bupropion: A Review of its Use in the Management of Smoking Cessation. Drugs 59, pp. 1007–1024. Retrieved from https://doi.org/10.2165/00003495-200059040-00019
(2000). Bupropion: A Review of its Use in the Management of Smoking Cessation. Drugs 59, pp. 1007–1024. Retrieved from https://doi.org/10.2165/00003495-200059040-00019 - Shin and Saadabadi. (2020). Trazodone. StatPearls Publishing, Treasure Island, Florida. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK470560/
- Croom, et al. (2009). Mirtazapine: A Review of its Use in Major Depression and Other Psychiatric Disorders. CNS Drugs 23, pp. 427-452. Retrieved from https://doi.org/10.2165/00023210-200923050-00006
- D’Agostino, et al. (2015). Vortioxetine (Brintellix): A New Serotonergic Antidepressant. Pharmacy and Therapeutics, 40(1), pp. 36-40. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4296590/
Uses, most common brands and important safety information
Complete a free online enrollment application to find out if you’re eligible to pay only $49 per month for your Atypical Antidepressants medication with our help.
Get started today
Major depressive disorder (MDD) is a chronic mental health condition that is the most common mood disorder in the United States. It is estimated that 14.4% of Americans will have at least 1 episode of major depression in their lifetime.
Depression is thought to be caused by deficiencies in certain neurotransmitters such as dopamine, serotonin, and norepinephrine. Atypical antidepressants work differently than other medications used to treat symptoms of depression and other mental illnesses. The first atypical antidepressant approved for MDD by the U.S Food and Drug Administration (FDA) was Desyrel (trazodone) in 1981. Immediate-release Wellbutrin (bupropion) was approved in 1989 shortly after the introduction of Prozac (fluoxetine).
Atypical antidepressants are not typically first-line treatment for MDD, despite some having similar efficacy and fewer sexual side effects than other antidepressant medications. Treatment for depression is usually treated with selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs).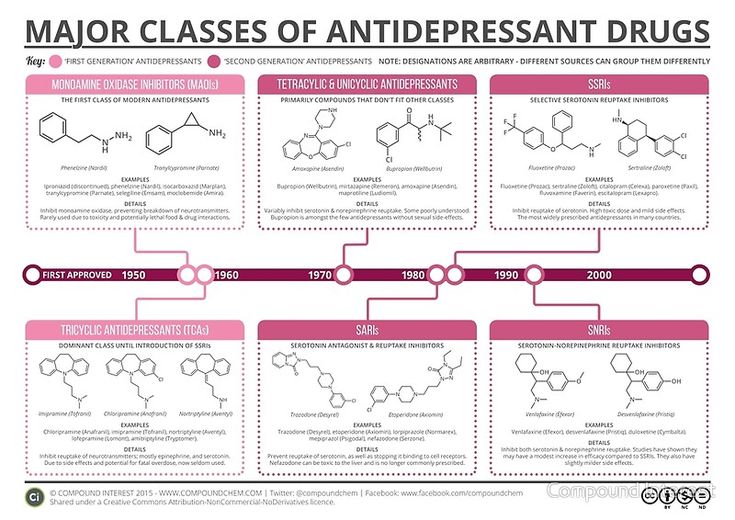
The list below includes the best atypical antidepressants approved by the U.S. Food and Drug Administration (FDA) and their pricing:
List of Atypical Antidepressants
table
Drug name
Learn more
NiceRx pricing
Wellbutrin (bupropion)
Wellbutrin is indicated to treat major depressive disorder, seasonal affective disorder, and as a smoking cessation aid.
Wellbutrin XL (bupropion)
Wellbutrin XL is indicated to treat major depressive disorder, seasonal affective disorder, and as a smoking cessation aid.
Desyrel (trazodone)
Desyrel is indicated to treat depression and insomnia.
Remeron (mirtazapine)
Remeron is indicated to treat depression, PTSD, and insomnia.
Trintellix (vortioxetine)
Trintellix is indicated to treat major depressive disorder.
Viibryd (vilazodone)
Viibryd is indicated to treat major depressive disorder.
Spravato (esketamine)
Spravato is indicated for treatment-resistant depression.
end table
What are atypical antidepressants?
An atypical antidepressant doesn’t fit in with the other 4 major classes of antidepressants, which include SSRIs, SNRIs, tricyclic antidepressants, and monoamine oxidase inhibitors (MAOIs). This class of antidepressants contains drugs that have various mechanisms of action. Atypical antidepressants work like most antidepressants by altering your brain chemistry to treat depression. They are typically used if other medications did not improve your symptoms or if they caused significant side effects.
Atypical antidepressants can also be used to treat other conditions besides depression. For example, Remeron (mirtazapine) is used to treat insomnia and Wellbutrin (bupropion) is used as a smoking cessation aid.
Atypical antidepressants are typically oral medications. The frequency you take it will depend on the condition being treated. How long it takes to work will vary between each atypical antidepressant. You should see some symptom improvement within the first week, but it can take up to 8 weeks to see the full effects.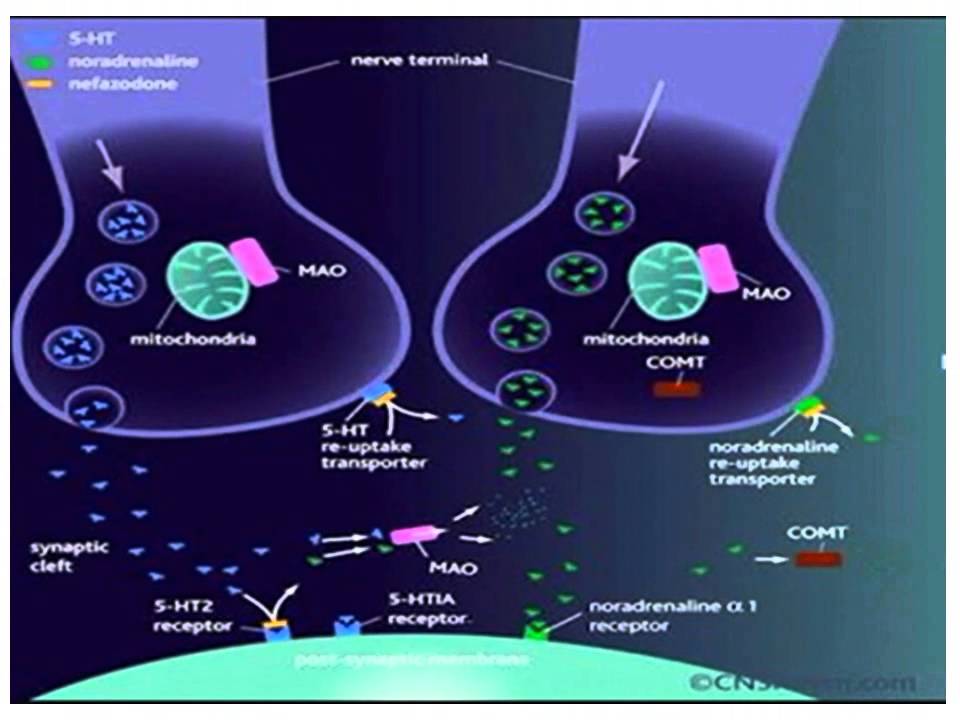
How do atypical antidepressants work?
Each atypical antidepressant has its own unique effect on the neurotransmitters in your brain. They typically all inhibit or alter the reabsorption of dopamine, serotonin, and/or norepinephrine. The combination of these neurotransmitters they act on will determine their therapeutic use and side effect profile.
Wellbutrin (bupropion) increases the amount of norepinephrine and dopamine (NDRI) available in the brain. It is the only antidepressant that doesn’t increase serotonin levels. It is the 3rd most prescribed antidepressant in the U.S.
Remeron (mirtazapine) is considered a noradrenergic and specific serotonergic antidepressant (NaSSA). It blocks the h2 histamine receptor, the alpha-2 adrenergic receptor, and multiple serotonin receptors. Remeron’s antidepressant effect is thought to be due to its antagonism of the 5-HT2C serotonin receptor.
The remaining atypical antidepressants increase serotonin in multiple ways including blocking the reuptake of serotonin and antagonizing serotonin receptors in the brain.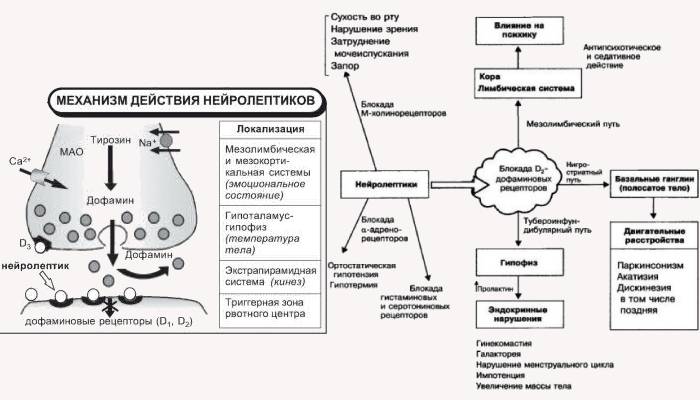
What conditions are atypical antidepressants used to treat?
Atypical antidepressants are a class of medications used in the treatment of depression and other conditions such as:
- Major depressive disorder
- Obsessive-compulsive disorder (OCD)
- Generalized anxiety disorder (GAD)
- Social anxiety disorder (SAD)
- Eating disorders such as bulimia
Are atypical antidepressants safe?
When taken as prescribed, atypical antidepressants are relatively safe and effective. Your prescribing physician should be aware of your medical conditions, including:
- Seizure disorder
- Bipolar disorder
- Heart disease
- Kidney disease
- Liver disease
- Hypertension (high blood pressure)
- Eating disorder
- Are pregnant or plan on becoming pregnant as they may cause fetal harm and/or death
You should also make sure they are aware of all the medications you take, including FDA-approved prescription drugs, over-the-counter medications, and supplements, as they may cause drug interactions:
- SSRIs such as Prozac (fluoxetine), Zoloft (sertraline), Lexapro (escitalopram), Paxil (paroxetine), Luvox (fluvoxamine), and Celexa (citalopram)
- SNRIs such as Cymbalta (duloxetine), Pristiq (desvenlafaxine), and Effexor XR (venlafaxine)
- Monoamine oxidase inhibitors (MAOI) such as Nardil (phenelzine) and Parnate (tranylcypromine).

- Tricyclic antidepressants (TCAs) such as Elavil (amitriptyline), Silenor (doxepin), Tofranil (imipramine), Surmontil (trimipramine), and Pamelor (nortriptyline)
- St. John’s wort, antipsychotics, and any other class of antidepressant that increases serotonin
Can you take atypical antidepressants while you are pregnant or breastfeeding?
There is limited data on whether atypical antidepressant use during pregnancy poses any risk to the fetus. There is a registry that monitors outcomes in women exposed to antidepressants during pregnancy. You can register by calling the National Pregnancy Registry for Antidepressants at 1-844-405-6185 or visiting online at https://womensmentalhealth.org/clinical-and-research-programs/pregnancyregistry/antidepressants/
Most atypical antidepressants are excreted in breast milk. The developmental and health benefits of breastfeeding should be considered as well as the possible adverse events on the breastfed infant.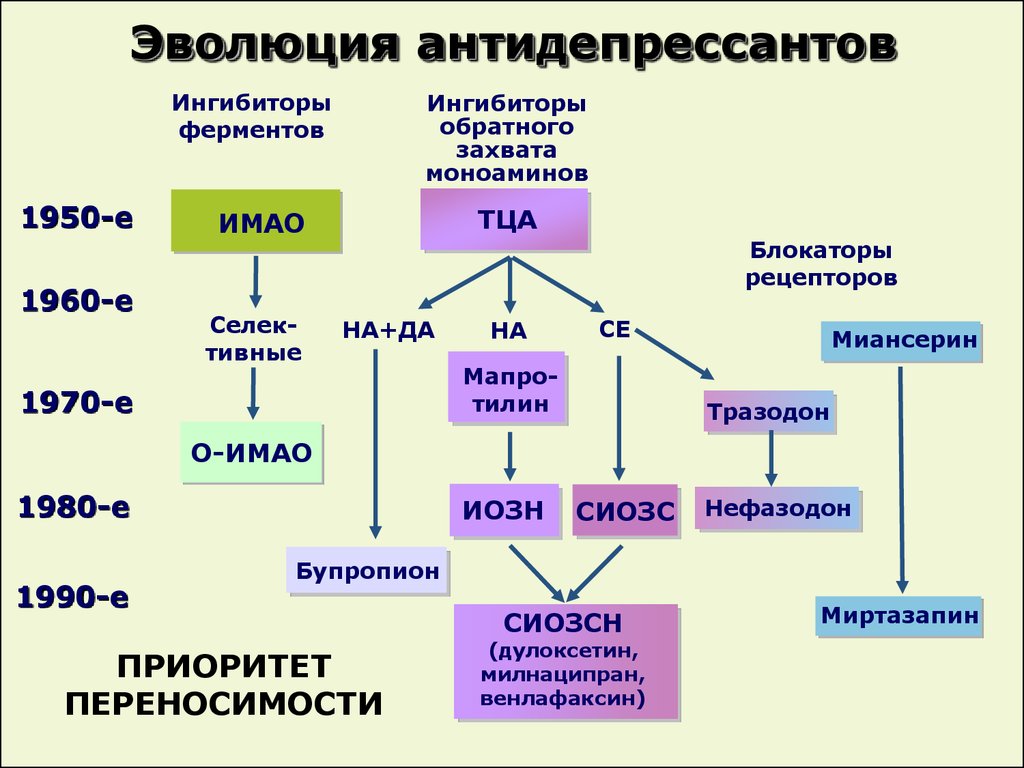
You should always discuss the risks and benefits of any medication you need with your doctor or mental health professional if you are pregnant, plan on becoming pregnant, or are breastfeeding.
What are the common side effects of atypical antidepressants?
Some common adverse effects of atypical antidepressants include:
- Constipation
- Dizziness
- Dry mouth
- Blurred vision
- Confusion
- Urinary retention
- Nausea
- Weight gain
- Drowsiness and sedation
- Sexual dysfunction
- Hyponatremia (low sodium levels)
Atypical antidepressants can sometimes cause rare, severe adverse effects, including:
- Serotonin syndrome
- Seizures
- Increased risk of suicidal thoughts or behavior, especially in adolescents and young adults under the age of 24
- Arrhythmias
- Liver damage
- Manic episodes
- Orthostatic hypotension (low blood pressure upon standing)
- Persistent, painful erection (priapism)
This is not a complete list of side effects and we encourage you to consult with your healthcare professional for medical advice about any possible side effects.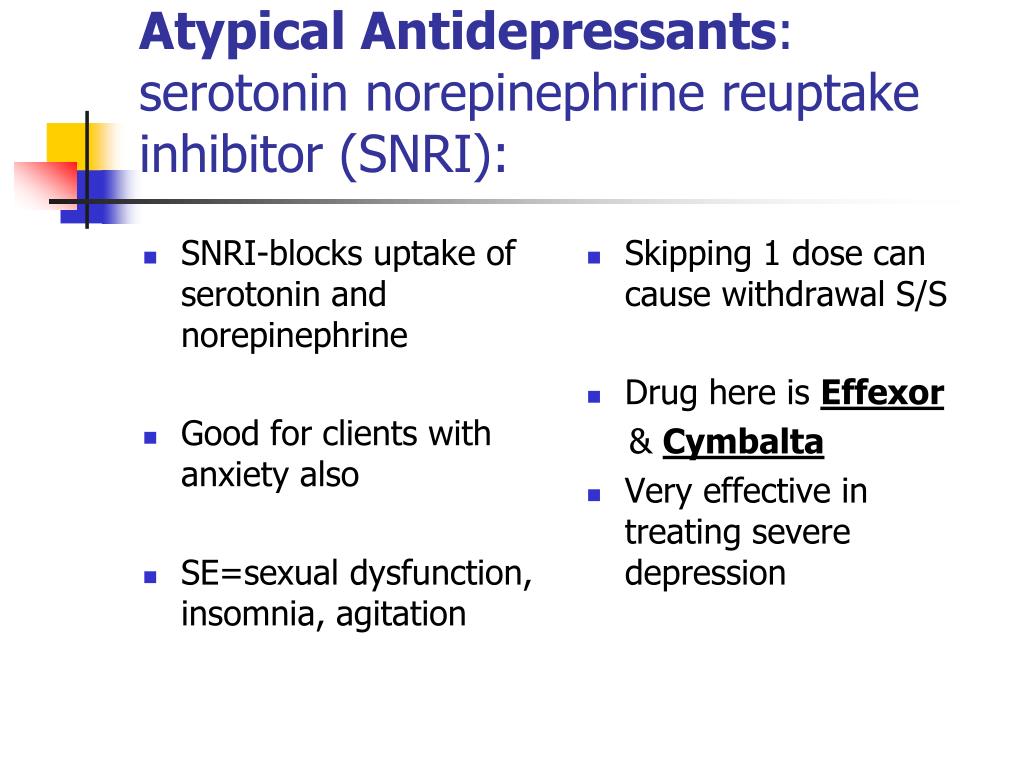
How much do atypical antidepressants cost?
Atypical antidepressants are very expensive with an average cost of around $5,000 per year for brand name medications.
You can purchase atypical antidepressants for $49 per month from NiceRx if eligible for assistance. Prices at the pharmacy vary by location, strength, and quantity, as well as your insurance status.
Related resources for atypical antidepressants
- https://www.ncbi.nlm.nih.gov/books/NBK519059/
- https://www.mayoclinic.org/diseases-conditions/depression/in-depth/atypical-antidepressants/art-20048208
- https://screening.mhanational.org/content/atypical-antidepressants/
- https://middlesexhealth.org/learning-center/articles/atypical-antidepressants
- https://www.rxlist.com/the_comprehensive_list_of_antidepressants/drugs-condition.htm
- https://www.statpearls.com/ArticleLibrary/viewarticle/17687
- https://digital.wpi.edu/downloads/qj72p7427
- https://doi.
 org/10.2174/9781681086071118060003
org/10.2174/9781681086071118060003
What you need to know about antidepressants?
What are the types of antidepressants?
Antidepressants are a heterogeneous group of drugs. There are several varieties:
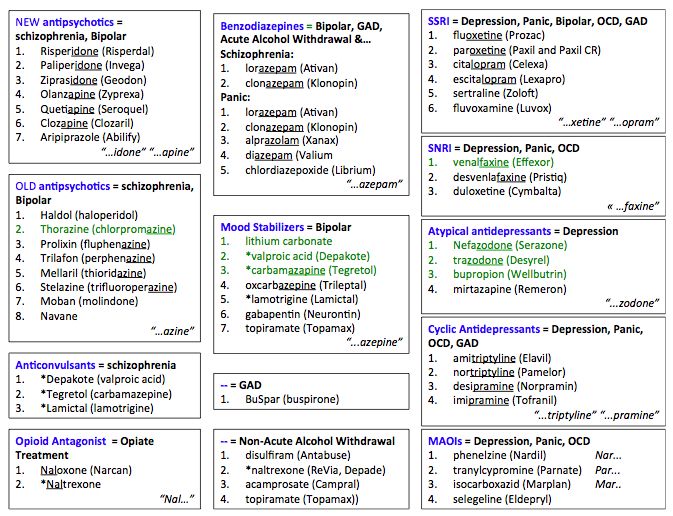
Selective serotonin reuptake inhibitors (SSRIs) . In a sense, this is the most popular type of antidepressant. It is with them that treatment is most often started, since they cause the fewest side effects and are most safe in high doses. This group includes drugs: paroxetine, fluoxetine, sertraline, escitalopram, citalopram. nine0005
Serotonin and norepinephrine reuptake inhibitors : venlafaxine, duloxetine, levomilnacipran, desvenlafaxine.
Tricyclic antidepressants . They are usually prescribed after other drugs have been tried and found to be ineffective, as they have severe side effects. This group includes: amitriptyline, imipramine, nortriptyline, desipramine, doxepin.
Monoamine oxidase inhibitors (MAOIs) have potentially dangerous side effects, so they are also used as backup drugs.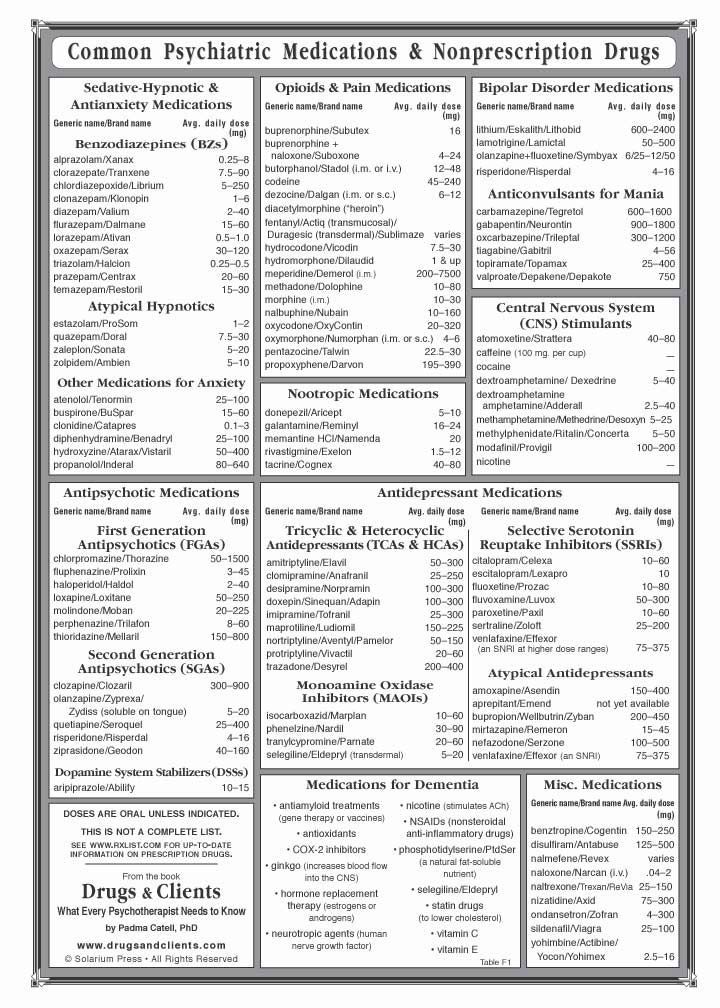 This group includes: nialamide, iproniazid, isocarboxazid, tranylcypromine, phenelzine. nine0005
This group includes: nialamide, iproniazid, isocarboxazid, tranylcypromine, phenelzine. nine0005
Atypical antidepressants include drugs that are not included in other groups: mirtazapine, trazodone, vilazodone, viortoxetine, bupropion.
These are prescription drugs and should only be taken with a doctor's prescription. Not all antidepressants work equally well for all patients. It is important to choose a drug or a combination of them that will be effective in a particular case.
How do you know which antidepressant is best to start with?
Initially, the physician prescribes the drug that he or she thinks is best for the individual patient. It's impossible to know for sure what will work best, but there are some factors to consider: the type and symptoms of depression, the side effects of medications, the general health of the patient, comorbidities. nine0005
If you have a family member who is depressed and some drugs work well for them, chances are that the same drugs will work for you.
Antidepressants may be given during pregnancy and lactation, but with caution. The physician must carefully weigh the possible risks.
What if antidepressants don't help?
First of all, don't panic. Antidepressants begin to help some patients literally from the first days, but this is not always the case. In most cases, improvement occurs within weeks. An antidepressant is not a headache pill that works immediately after taking it. It is important to take them regularly, in the doses prescribed by the doctor. nine0005
Medicines may cause some side effects at first. For example, people who have just started taking SSRIs may experience headaches, nausea, dry mouth, and bowel problems. After a period of adaptation, these symptoms disappear.
If the side effects are very severe, persist for too long, if you have been taking the drug for several weeks and do not feel any improvement, do not do it yourself, consult your doctor .
Can antidepressants cure depression?
Antidepressants are drugs that treat symptoms but do not treat depression. Currently, there is no way to eliminate the cause of the disease and get rid of it completely. However, the manifestations of the disease can be kept under control. A person suffering from depression can live a full life and feel good.
Currently, there is no way to eliminate the cause of the disease and get rid of it completely. However, the manifestations of the disease can be kept under control. A person suffering from depression can live a full life and feel good.
In addition, antidepressants are not the only treatment for depression. Psychotherapy brings good results. nine0005
How dangerous is taking antidepressants? What are the side effects?
Antidepressants cause some side effects. In drugs from different groups, they are expressed to varying degrees. For example, SSRIs are the safest, most patients who take them do not experience any problems. At the same time, MAOIs can cause life-threatening side effects. They are incompatible with certain types of drugs and even with food.
Unfortunately, the safest drugs are not always effective. In such cases, there is nothing left but to resort to "heavy artillery". The doctor should assess the patient's condition well and prescribe the most appropriate drugs in optimal dosages. nine0005
nine0005
Antidepressants sometimes increase suicidal tendencies in patients under 25 years of age, especially in the first weeks of use and when the dosage is changed. However, in the long run, they tend to improve mood and reduce the likelihood of suicide.
“I heard that antidepressants change personality. Will they turn me into a zombie?
Perhaps this is one of the most common and most ridiculous myths about antidepressants. In fact, they will not change your personality. You will remain the same person, you will be able to work normally, communicate with people around you, you will live a full life - just your mood will stabilize, become normal. A far-fetched “side effect” in the form of a change in personality is not at all something to be afraid of. You won't become a zombie. nine0005
The most important thing is to correctly determine whether you have indications for taking antidepressants, choose the appropriate drugs and dosages. Only a specialist can competently solve these problems. Trust an experienced doctor at the Cordia Clinic, contact us:
Trust an experienced doctor at the Cordia Clinic, contact us:
Antidepressants: pharmacological group
Description
Drugs that specifically relieve depression appeared in the late 1950s. In 1957, iproniazid was discovered, which became the ancestor of the group of antidepressants - MAO inhibitors, and imipramine, on the basis of which tricyclic antidepressants were obtained. nine0005
According to modern concepts, depressive states are characterized by a decrease in serotonergic and noradrenergic synaptic transmission. Therefore, the accumulation of serotonin and norepinephrine in the brain caused by them is considered an important link in the mechanism of action of antidepressants. MAO inhibitors block monoamine oxidase, an enzyme that causes oxidative deamination and inactivation of monoamines. Currently, two forms of MAO are known - type A and type B, which differ in the substrates exposed to them. Type A MAO causes mainly the deamination of noradrenaline, adrenaline, dopamine, serotonin, tyramine, and type B MAO causes the deamination of phenylethylamine and some other amines. Allocate inhibition competitive and non-competitive, reversible and irreversible. Substrate specificity can be observed: a predominant effect on the deamination of various monoamines. All this significantly affects the pharmacological and therapeutic properties of various MAO inhibitors. So, iproniazid, nialamide, phenelzine, tranylcypromine irreversibly block MAO type A, and pirlindol, tetrindole, metralindol, eprobemide, moclobemide, etc. have a selective and reversible effect on it. nine0005
Allocate inhibition competitive and non-competitive, reversible and irreversible. Substrate specificity can be observed: a predominant effect on the deamination of various monoamines. All this significantly affects the pharmacological and therapeutic properties of various MAO inhibitors. So, iproniazid, nialamide, phenelzine, tranylcypromine irreversibly block MAO type A, and pirlindol, tetrindole, metralindol, eprobemide, moclobemide, etc. have a selective and reversible effect on it. nine0005
Tricyclic antidepressants are named because of their characteristic tricyclic structure. The mechanism of their action is associated with inhibition of the reuptake of neurotransmitter monoamines by presynaptic nerve endings, resulting in the accumulation of mediators in the synaptic cleft and activation of synaptic transmission. Tricyclic antidepressants, as a rule, simultaneously reduce the capture of various neurotransmitter amines (norepinephrine, serotonin, dopamine). Recently, antidepressants have been created that block predominantly (selectively) the reuptake of serotonin (fluoxetine, sertraline, paroxetine, citalopram, escitalopram, etc. ). nine0005
). nine0005
There are also so-called "atypical" antidepressants that differ from the "typical" ones both in structure and mechanism of action. Preparations of a bi- and four-cyclic structure appeared, in which no pronounced effect was found either on the capture of neurotransmitters or on the activity of MAO (mianserin, etc.).
A common feature of all antidepressants is their thymoleptic effect, that is, a positive effect on the affective sphere of the patient, accompanied by an improvement in mood and general mental state. Different antidepressants differ, however, in the amount of pharmacological properties. So, in imipramine and some other antidepressants, the thymoleptic effect is combined with a stimulating one, and in amitriptyline, pipofezin, fluacizine, clomipramine, trimipramine, doxepin, a sedative component is more pronounced. In maprotiline, the antidepressant effect is combined with anxiolytic and sedative. MAO inhibitors (nialamide, eprobemide) have stimulating properties.