Buspirone weight gain or loss
Buspar Weight Gain: Is It a Side Effect?
If you frequently experience anxiety, you’re not alone. Roughly 19.1% of U.S. adults have an anxiety disorder.
Based on clinical studies that have been conducted on the anti-anxiety medication – Buspar, weight gain is one side effect that can occur. Very few people experience this effect, however.
This article will cover Buspar’s impact on weight gain and weight loss, side effects, and when to see a medical professional about issues relating to this drug.
What is Buspar (Buspirone)?
Buspar, also called buspirone hydrochloride (HCL), is a generic drug people take to combat anxiety.
It also helps people relax, worry less, and think more clearly.
What Does it Treat?
Buspar is a commonly-prescribed anxiolytic medication used to treat anxiety disorders such as generalized anxiety disorder (GAD).
More than 10 million Americans use Buspar to treat their anxiety, as well as physical symptoms of anxiety such as fear, tension, irritability, and dizziness.
Those with an anxiety disorder or who experience anxiety can have any of the following symptoms:
- Nervousness
- Restlessness
- Tenseness
- Rapid breathing
- Sweating
- A feeling of impending doom or danger
- Trembling
- Weakness or tiredness
- Difficulty with concentration and sleeping
- Stomachaches and headaches
- An urge to avoid activities that trigger anxiety
Buspar is a daily, commonly prescribed in addition to other drugs you may already be taking, such as selective serotonin reuptake inhibitors (SSRIs), which are frequently prescribed to treat depression.
While benzodiazepines like Xanax have sedative and muscle-relaxing effects in treating anxiety, Buspar doesn’t.
Feeling Down?
Take our free assessment and learn about your options.
Get Started
Can Buspar Cause Weight Gain?
Just between 0.1 and 1% of the people who use Buspar medication experience weight gain.
Most people who take the drug won’t experience a clinically relevant gain or loss in weight, which is defined as a 7% weight change from their baseline weight.
During an anxiety attack, there are a number of symptoms that you may experience, which can lead to weight gain. These include:
- Increased cortisol levels
- Fat deposit in the stomach
- More fat depositions, resulting in adiposity (being overweight)
- Recovery from loss of appetite during anxiety
Can Buspar Cause Weight Loss?
Just as anxiety can cause you to eat more, it can also cause you to eat less.
Anxiety symptoms such as low appetite and decreased metabolism can result in weight loss.
A change in weight is more likely to be due to the anxiety you’re experiencing, rather than as a side effect of Buspar.
If you’re already overweight, weight loss may be an indirect side effect of using Buspar to treat anxiety.
If you’ve been turning to food as a coping mechanism for anxiety and using Buspar has proven to be effective in treating it, the need to overeat would lessen. Subsequently, weight loss may occur.
Subsequently, weight loss may occur.
Additionally, adverse effects of Buspar, such as nausea and mild stomach aches, could result in weight loss.
Vomiting and diarrhea from the use of the medication could result in water loss and, consequently, weight loss.
Other Factors That Can Cause Weight Gain
Although Buspar is unlikely to contribute directly to weight gain, other effects of improving anxiety may explain why you see a change in weight. These include:
- Mood changes
- Improvement of cognitive function
- Hormonal changes affecting prolactin and growth hormone
- Change in resting metabolic rate
Side Effects
Side effects of taking Buspar include:
- Nervousness or restlessness
- Drowsiness
- Lightheadedness
- Hives
- Swelling of your face, lips, tongue, or throat
- Chest pain
- Shortness of breath or difficulty breathing
1-10% of people who take Buspar also experience side effects such as:
- Central nervous system effects (such as headache, nervousness, excitement, confusion, dizziness, drowsiness, and disturbed sleep)
- Gastrointestinal effects (such as nausea, diarrhea, or upset stomach)
- Chest pain
- Skin rashes
- Blurred vision
- Ringing in the ears
If you have a condition that affects the functioning of your liver, your liver may not be able to break down Buspar effectively, and this will lead to unwanted side effects.
If you have kidney problems, your body may not be able to excrete the drug properly.
To avoid preventable, unwanted side effects, tell your doctor about any medications or supplements that you’re taking to make sure that they won’t interact with Buspar.
Feeling Down?
Take our free assessment and learn about your options.
Get Started
When to See a Medical Professional
Before you take Buspar, a doctor will need to review your medical history to ensure that you don’t have any contraindications to taking Buspar, such as an allergy or hypersensitivity to the drug.
If you have diabetes, your doctor may choose not to prescribe Buspar since the drug can affect blood glucose levels.
Speak with your doctor immediately if you’re experiencing chest pain, shortness of breath, lightheadedness, or faintness after taking the medication.
Similarly, talk with a doctor if you’ve experienced an anxiety attack with any of these symptoms:
- Feelings of danger, panic, or dread
- Rapid heart rate
- Sweating
- Trembling or severe chills
- Nervousness or restlessness
- Tiredness or weakness
- Difficulty with focusing and concentration
- Hyperventilation
If you overdose and experience any of the following symptoms, call the Poison Helpline at 1-800-222-1222.
Buspar overdoses have not resulted in any reported deaths, but symptoms may include:
- Nausea
- Vomiting
- Drowsiness or sleepiness
- Dizziness
- Upset stomach
If you’re having a mental health emergency, call 911 or go to the nearest emergency room. You can also get free 24/7 support from a suicide and crisis expert by calling or texting 988. If you’d prefer to chat online, you can chat with a suicide and crisis expert by visiting the Lifeline Chat.
How K Health Can Help
Think you might need a prescription for buspar (buspirone)?
K Health has clinicians standing by 24/7 to evaluate your symptoms and determine if citalopram is right for you.
Get started with our free assessment, which will tell you in minutes if treatment could be a good fit. If yes, we’ll connect you right to a clinician who can prescribe medication and have it shipped right to your door.
Frequently Asked Questions
Does Buspar Affect Your Appetite?
Buspar can indirectly lead to weight gain through changes to your eating habits as your anxiety improves. An increased appetite is a noted side effect of Busparin in less than 1% of cases, but when it does occur, it can lead to more frequent or larger meals, thus contributing to weight gain.
Clinical trials on the use of Buspar in people with Autism to reduce irritability demonstrated that increased appetite was actually one of the more common side effects in that population.
To lower the chances of losing or gaining while taking Buspar, be conscious of your eating habits while on the medication. Track the number of calories you consume each day to help determine if you’re eating the right amount of food to achieve the appropriate body mass.
An increased appetite is a noted side effect of Busparin in less than 1% of cases, but when it does occur, it can lead to more frequent or larger meals, thus contributing to weight gain.
Clinical trials on the use of Buspar in people with Autism to reduce irritability demonstrated that increased appetite was actually one of the more common side effects in that population.
To lower the chances of losing or gaining while taking Buspar, be conscious of your eating habits while on the medication. Track the number of calories you consume each day to help determine if you’re eating the right amount of food to achieve the appropriate body mass.
Does Buspar Affect Metabolism?
Stress and anxiety can lead to weight loss by changing your appetite and metabolism.
Your body’s cortisol levels rise in response to stress, potentially increasing your appetite and increasing fat (adipose) buildup in the stomach. This can ultimately lead to weight gain (adiposity).
This can ultimately lead to weight gain (adiposity).
K Health articles are all written and reviewed by MDs, PhDs, NPs, or PharmDs and are for informational purposes only. This information does not constitute and should not be relied on for professional medical advice. Always talk to your doctor about the risks and benefits of any treatment.
K Health has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical associations. We avoid using tertiary references.
-
A Review of the Neuropharmacology of Bupropion, a Dual Norepinephrine and Dopamine Reuptake Inhibitor. (2004).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC514842/ -
Any Anxiety Disorder.
 (n.d.).
(n.d.).
https://www.nimh.nih.gov/health/statistics/any-anxiety-disorder -
Bupropion: a systematic review and meta-analysis of effectiveness as an antidepressant. (2016).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4837968/ -
Buspirone.
 (2022).
(2022).
https://www.ncbi.nlm.nih.gov/books/NBK531477/ -
Generalized Anxiety Disorder (n.d.).
https://www.nimh.nih.gov/health/statistics/generalized-anxiety-disorder -
Which anti-anxiety medication is right for me? (2019).
https://vitalrecord.tamhsc.edu/which-anti-anxiety-medication-is-right-for-me/
Does BuSpar® Cause Weight Gain?
Medically reviewed by Kristin Hall, FNP
Written by Our Editorial Team
Last updated 6/30/2022
More than 23 percent of all US adult women experience an anxiety disorder on an annual basis, making anxiety one of the most common mental health issues.
If you’ve been diagnosed with an anxiety disorder, your healthcare provider may suggest taking the medication BuSpar® to control your symptoms.
Many medications for anxiety and depression are associated with changes in your body weight, including weight gain and weight loss.
Does BuSpar cause weight gain? The good news is that there isn’t much of a link between the use of BuSpar and changes in body composition. In fact, in clinical trials of BuSpar, weight gain and weight loss were both extremely infrequent side effects.
In fact, in clinical trials of BuSpar, weight gain and weight loss were both extremely infrequent side effects.
Below, we’ve explained what BuSpar is, as well as how it’s used as a treatment for generalized anxiety disorder (GAD) and other forms of anxiety.
We’ve also talked about why you shouldn’t feel overly concerned about weight gain while you’re using BuSpar to treat anxiety, as well as what you can do to maintain a healthy weight while you take part in treatment.
What Is BuSpar?
BuSpar is an anti-anxiety medication. It’s used to manage anxiety disorders and as a short-term treatment for anxiety symptoms that develop from time to time. BuSpar is also sometimes used as an augmentation agent (meaning a second medication) for treating depression.
The active ingredient in BuSpar is buspirone, which belongs to a class of medications known as azapirones. Experts believe that buspirone reduces feelings of anxiety by targeting receptors in your brain and body, including serotonin 5HT1a and 5HT2 and dopamine D2 autoreceptors.
BuSpar offers several advantages over other medications for anxiety, such as benzodiazepines and selective serotonin reuptake inhibitors (SSRIs).
The first of these advantages is that BuSpar isn’t associated with physical dependence, allowing it to be used with a lower risk of forming habits.
The second is that BuSpar doesn’t cause the withdrawal symptoms that are typically associated with benzodiazepines and SSRIs.
Because of these advantages, BuSpar is often used as a second-line treatment when SSRIs and other medications aren’t effective at controlling the symptoms of anxiety.
BuSpar is currently available as a generic medication and comes as an oral tablet. It’s generally used at a dosage of 15 to 60mg per day to treat generalized anxiety disorder, divided into two to three doses.
Does BuSpar Cause Weight Gain?
Many medications for anxiety and depression are associated with some level of weight gain. For example, changes in appetite and body weight are common side effects of some SSRIs, as well as many tricyclic antidepressants (TCAs).
Unlike other medications for anxiety and depression, BuSpar generally isn’t associated with any significant degree of drug-induced weight gain.
In clinical trials of BuSpar, researchers found that changes in body weight, including weight gain and weight loss, were infrequent side effects, meaning they occurred in less than one percent of study participants.
Because of this, BuSpar is often referred to as a “weight neutral” medication for managing the symptoms of anxiety.
online mental health assessment
your mental health journey starts here
Side Effects of BuSpar
Although BuSpar isn’t associated with an increased risk of weight gain, it can cause other side effects. Many of these are mild side effects that improve over time, although some side effects of BuSpar may be persistent or bothersome.
The most common side effect associated with BuSpar is dizziness, which affects more than 10 percent of people prescribed this medication.
Other common adverse effects of BuSpar include:
Abnormal dreams
Confusion
Drowsiness
Ataxia (lack of coordination)
Excitement
Headaches
Nervousness
Burning or prickling sensations
Outbursts of anger
Numbness
Sore throat
Blurred vision
Chest pain
Tinnitus
Skin rash
Sweating
Nasal congestion
Nausea
Diarrhea
Muscle pain and/or joint pain
Physical weakness
Tremor
Elevated liver enzymes
Unlike many other medications used to treat anxiety and depression, BuSpar usually isn’t linked to sexual dysfunction or other sexual side effects.
Many side effects of BuSpar may improve over time. Inform your healthcare provider if you have any persistent or severe side effects while using BuSpar.
Although BuSpar is typically a safe and effective medication when it’s used as prescribed, it can interact with other medications and potentially cause safety issues.
Medications and substances that can interact with BuSpar and generic buspirone include:
Anticonvulsants such as carbamazepine, phenobarbital and phenytoin
Other medications for treating anxiety, such as benzodiazepines
Selective serotonin reuptake inhibitors (SSRIs)
Serotonin-norepinephrine reuptake inhibitors (SNRIs)
Monoamine oxidase inhibitors (MAOIs)
Tricyclic and tetracyclic antidepressants (TCAs and TeCAs)
Other medications for treating depression
Antibiotics such as erythromycin
Pain medications and narcotics
Sleeping pills and tranquilizers
Muscle relaxant medications
Other over-the-counter and prescription medications may also interact with BuSpar.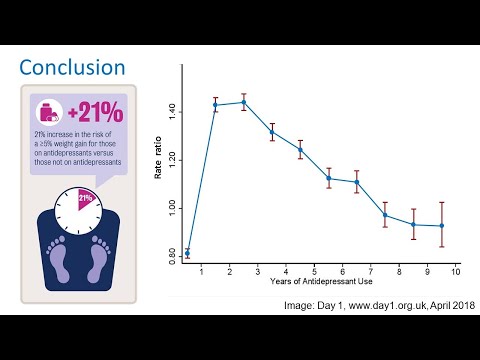 To limit your risk of drug interactions, make sure to inform your healthcare provider about all medications you currently use or have recently used before starting treatment with BuSpar.
To limit your risk of drug interactions, make sure to inform your healthcare provider about all medications you currently use or have recently used before starting treatment with BuSpar.
It’s especially important to inform your healthcare provider if you’ve used an MAOI within the last 14 days, as medications of this type may remain in your system for several weeks after the most recent dose, creating a risk of drug interactions.
BuSpar can interact with medications and substances that affect the enzyme CYP3A4, including grapefruit juice. Make sure to avoid consuming grapefruit juice or grapefruit while taking BuSpar or generic buspirone.
How to Maintain a Healthy Weight While Using BuSpar
If you’re concerned about gaining weight while using BuSpar, making a few simple changes to your habits can help you to maintain your normal body weight and lower your risk of putting on weight during treatment.
Use the following tips to maintain a healthy, stable weight while you use BuSpar:
Check your initial body weight before you start taking medication.
 If you’re worried about gaining weight while using BuSpar, make a note of your original weight before you start using medication.
If you’re worried about gaining weight while using BuSpar, make a note of your original weight before you start using medication.
This way, you’ll be able to accurately track any changes in your body weight that happen during treatment.Calculate your basal metabolic rate (BMR). Your basal metabolic rate is the number of calories your body burns as paper of basic functions. Understanding your BMR can help you to avoid overeating and gaining weight (or undereating and losing weight).
To avoid any unwanted changes in your body weight, try to eat roughly the same amount of calories that your body needs on a daily basis.Eat a healthy diet. Try to eat a healthy, balanced diet. The CDC recommends designing your diet around ingredients such as fruits, vegetables, legumes, nuts, seeds, lean meat, poultry, eggs, seafood, whole grains and low-fat dairy products.
To minimize the impact on comfort foods and junk foods, stick to small portions and try to enjoy these foods in moderation.
Keep yourself physically active. Physical activity not only helps to burn fat — it’s also a great way to prevent feelings of anxiety. Exercise can help to distract you from the things that make you feel anxious while changing your brain chemistry to improve your mood.
Try to get at least 150 minutes of physical activity every week, even if it’s just going for a walk around your neighborhood or doing a quick daily workout.Don’t worry about small weight changes. It’s normal for your weight to fluctuate by a few pounds over the course of each day, often due to changes in your fluid levels or the amount of food in your digestive system.
Try to avoid worrying about small increases or decreases in your weight. Instead, weigh yourself infrequently and focus on the long-term trend before changing your habits and diet to increase or decrease your body weight.
psych meds online
psychiatrist-backed care, all from your couch
The Final Word on BuSpar and Weight Gain
Does BuSpar cause weight gain? Unlike many antidepressant medications, BuSpar and generic buspirone aren’t associated with an increased risk of weight gain.
If you’re prescribed BuSpar and have concerns about your weight, try using the habits above to maintain a healthy weight while you use your medication. Reach out to your healthcare provider if you notice any sudden changes in your appetite, eating habits or body weight.
If you think that you might have an anxiety disorder, you can get help by talking to your primary care provider or contacting a mental health professional in your area.
You can also get help from home with our range of online mental health services, including our online psychiatry service. If appropriate, you’ll receive ongoing care and medication to help you gain control over your anxiety symptoms.
Finally, you can find out more about dealing with anxiety, depression and other common mental health issues using our free online mental health resources and content.
7 Sources
Hims & Hers has strict sourcing guidelines to ensure our content is accurate and current. We rely on peer-reviewed studies, academic research institutions, and medical associations. We strive to use primary sources and refrain from using tertiary references.
We strive to use primary sources and refrain from using tertiary references.
- Any Anxiety Disorder. (n.d.). Retrieved from https://www.nimh.nih.gov/health/statistics/any-anxiety-disorder
- Buspirone Hydrochloride Tablets, USP. (2020, November). Retrieved from https://www.accessdata.fda.gov/spl/data/5bad7053-8f63-45fc-adb0-88c628fa039b/5bad7053-8f63-45fc-adb0-88c628fa039b.xml
- LABEL: BUSPAR- buspirone hydrochloride tablet. (2016, May 25). Retrieved from https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=33accd6b-10a6-5bd3-e054-00144ff88e88
- Wilson, T.K. & Tripp, J. (2022, March 16). Buspirone. StatPearls. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK531477/
- Healthy Eating for a Healthy Weight. (2021, April 19). Retrieved from https://www.cdc.gov/healthyweight/healthy_eating/index.html
- Can exercise help treat anxiety? (2019, October 24). Retrieved from https://www.
 health.harvard.edu/blog/can-exercise-help-treat-anxiety-2019102418096
health.harvard.edu/blog/can-exercise-help-treat-anxiety-2019102418096 - How much physical activity do adults need? (2022, March 17). Retrieved from https://www.cdc.gov/physicalactivity/basics/adults/index.htm
This article is for informational purposes only and does not constitute medical advice. The information contained herein is not a substitute for and should never be relied upon for professional medical advice. Always talk to your doctor about the risks and benefits of any treatment. Learn more about our editorial standards here.
Use of buspirone in clinical practice
Buspirone (spitomin) is a non-benzodiazepine anxiolytic, which is a derivative of azapirone. Azapirones are a class of drugs with high affinity for serotonin 5-HT1A receptors located on the body and in the endings of serotonergic neurons, as well as in the dendrites of postsynaptic neurons with which serotonergic endings contact. The anti-anxiety effect of buspirone is not associated with an effect on GABA-benzodiazepine receptors. However, in terms of anxiolytic activity, buspirone is comparable to such benzodiazepines as diazepam, lorazepam or alprazolam, but unlike them, it does not cause drug dependence, cognitive and psychomotor impairment, pronounced sedative and muscle relaxant effects [1].
However, in terms of anxiolytic activity, buspirone is comparable to such benzodiazepines as diazepam, lorazepam or alprazolam, but unlike them, it does not cause drug dependence, cognitive and psychomotor impairment, pronounced sedative and muscle relaxant effects [1].
Mechanism of action of buspirone
The mechanism of the anxilytic action of buspirone, which predetermines its features, is mainly due to the effect on serotonin receptors. Buspirone has a high affinity for presynaptic serotonin (5-HT1A) receptors, of which it is an agonist, as well as for postsynaptic serotonin receptors, for which it can be considered as a partial (partial) agonist [1].
Partial agonists are ligands that bind to receptors but are only able to cause their partial activation. If a partial agonist interacts with free receptors, it causes incomplete (50%) cell activation. If a partial agonist acts on a tissue whose receptors are already activated by a full agonist, then due to the displacement of the latter from their connection with the receptor, the cell response decreases and, therefore, it has a blocking effect.
Thus, due to its receptor action, buspirone reduces the synthesis and release of serotonin, reduces the activity of serotonergic neurons in the raphe nuclei ("serotonin stabilizer"). Buspirone is also able to interact with postsynaptic 5-HT2 receptors, but has a low affinity for them. Being a partial agonist, due to its postsynaptic action, it can theoretically reduce serotonergic activity and cause an anxiolytic effect, and due to its action on somatodendritic serotonin presynaptic autoreceptors, it can theoretically increase serotonergic activity and cause an antidepressant effect.
To a lesser extent, the drug selectively blocks pre- and postsynaptic D2-dopamine receptors. Moreover, it was originally developed as an antipsychotic, but later it turned out that it has a low affinity for dopamine receptors, and its presynaptic action prevails over the postsynaptic one, which prevents the neuroleptic effect.
Experimental studies have indicated a decrease in serotonin turnover with the introduction of low doses of buspirone, which reflects the stimulation of presynaptic autoreceptors.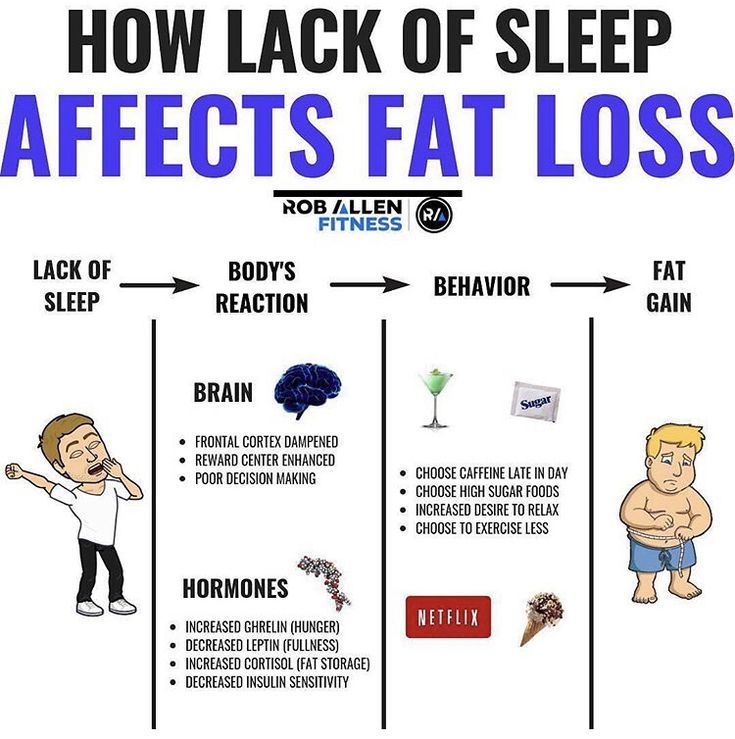 However, repeated administration of buspirone reduces the response of somatodendritic 5-HT1A receptors, since the decrease in 5-HT metabolism was less pronounced.
However, repeated administration of buspirone reduces the response of somatodendritic 5-HT1A receptors, since the decrease in 5-HT metabolism was less pronounced.
Buspirone can act as a partial agonist at postsynaptic serotonin 5-HT1A receptors in the hippocampus and prefrontal cortex, as well as presynaptic autoreceptors on the bodies of serotonergic neurons. Since the effect of azapirones develops over several days, it does not appear to be related to their direct action on receptors. Animal studies suggest that the anxiolytic effect of these drugs is due to their action on presynaptic receptors, and the antidepressant effect is due to the action on postsynaptic receptors.
Decreased serotonin circulation also occurs in the striatum, which may be accompanied by an inhibitory effect on dopaminergic transmission. This effect is manifested in the fact that the co-administration of buspirone can attenuate apomorphine sensitization. Thus, buspirone at a relatively low dose can counteract the side effect of apomorphine. However, the introduction of buspirone at a higher dose caused sensitization of motor behavior [2].
However, the introduction of buspirone at a higher dose caused sensitization of motor behavior [2].
This effect may be due to blockade of presynaptic dopamine autoreceptors. The introduction of a relatively high dose of buspirone in the experiment caused a sharp increase in the synthesis and metabolism of dopamine in the striatum.
The experiment has shown that the administration of buspirone in the brain dialysate reduces the level of serotonin by 50%, but increases the level of dopamine by 100% and norepinephrine by 140%, which indicates a complex effect of buspirone on monoaminergic neurotransmission [3].
However, in addition to acting on autoreceptors, buspirone also has another point of application, since the administration of haloperidol, which blocks D1- and D2-postsynaptic mesolimbic and striatal receptors, did not block the dopaminomimetic effect of buspirone. It has been shown that the antagonistic effect of the drug on D2 receptors is 15 times weaker than the effect on 5-HT1A receptors. Buspirone is a relatively weak blocker of postsynaptic dopamine receptors, even at high doses. It binds with higher affinity to D3 and D4 receptors than to D2 receptors. The action on presynaptic dopamine receptors is stronger than the blockade of postsynaptic receptors. Only in super-high doses, postsynaptic striatal D1- and D2-receptors are blocked quite actively. However, weak postsynaptic dopaminergic antagonism weakens the presynaptic dopaminomimetic effect of the drug, avoiding stereotypy [2, 3].
Buspirone is a relatively weak blocker of postsynaptic dopamine receptors, even at high doses. It binds with higher affinity to D3 and D4 receptors than to D2 receptors. The action on presynaptic dopamine receptors is stronger than the blockade of postsynaptic receptors. Only in super-high doses, postsynaptic striatal D1- and D2-receptors are blocked quite actively. However, weak postsynaptic dopaminergic antagonism weakens the presynaptic dopaminomimetic effect of the drug, avoiding stereotypy [2, 3].
Use of buspirone in generalized anxiety and other affective disorders
The greatest experience with the use of buspirone has been accumulated in generalized anxiety disorder (GAD). Clinical studies of the last 30 years have been accompanied by constant improvement in the nosological structure of anxiety disorders. At the beginning of the 20th century, the understanding of anxiety disorders was rather vague, but over time their place among other mental disorders has been more clearly defined, partly under the influence of pharmacological research.
Symptoms of GAD are chronic and often observed in patients who visit general practitioners. Typically, such patients present vague somatic complaints of fatigue, muscle pain or tension, and sleep disturbances.
Buspirone is the first FDA-approved non-benzodiazepine anxiolytic for the treatment of GAD, based on studies showing that it is comparable in efficacy to benzodiazepines.
In accordance with DSM-V [4] criteria, GAD is characterized by:
A. Excessive anxiety and worry (anxious expectations) that occurs most of the days for at least 6 months and manifests itself in a variety of events or activities (for example, in the performance of professional duties or while studying at school).
B. Difficulty in controlling anxiety.
C. Presence most of the days for 6 months at least 3 of the following symptoms: restlessness or restlessness; fast fatiguability; difficulty concentrating and being distracted; irritability; muscle tension; sleep disturbance.
D. Clinically significant distress or impairment of social, occupational, or other activities caused by anxiety, restlessness, or physical (psychomotor) symptoms.
E. These disorders that cannot be explained by a physiological effect of a psychoactive substance or medical illness.
E. These disorders that cannot be explained by another mental illness.
Buspirone has also been successfully used for the prophylactic treatment of migraine and alcoholism in individuals with comorbid anxiety disorder, as well as for the treatment of anxious depression, anxiety and agitation in patients with traumatic brain injury [5, 6].
The direct antidepressant effect of buspirone, independent of its anxiolytic action, has also been demonstrated. It may be due to the fact that the sensitivity of 5-HT1A autoreceptors in depression is increased, while the properties of postsynaptic 5-HT1A and 5-HT2A receptors do not change in untreated patients with depression.
Data on the effectiveness of buspirone in obsessive-compulsive disorder are contradictory, but some studies show a positive effect of the drug, especially when combined with other psychopharmacological drugs, primarily antidepressants. An open study showed that the addition of buspirone (at a dose of 30-90 mg/day) to selective serotonin reuptake inhibitors (SSRIs) increases the effectiveness of the treatment of body dysmorphic disorder in almost half of patients, mainly in those who had a partial effect on serotonergic antidepressants [7, 8].
Buspirone can be considered as an alternative to antidepressants in the treatment of social phobia. The effect of buspirone on social phobia has been shown in a placebo-controlled study. When added to SSRIs, buspirone may correct some of their side effects. For example, it has been shown that at a dose of 15-60 mg/day it can reduce sexual dysfunction and bruxism [8].
Antiaggressive effect of buspirone
Separate mention should be made of the anti-aggressive effect of buspirone in agitation and aggressive actions in patients with dementia, attention deficit hyperactivity disorder, and traumatic brain injury [8]. At the same time, the effect of buspirone at a dose of 15–60 mg/day was noted both in relation to verbal (60%) and physical (90%) aggression [9–12].
At the same time, the effect of buspirone at a dose of 15–60 mg/day was noted both in relation to verbal (60%) and physical (90%) aggression [9–12].
Effect of buspirone on cognitive functions
Data on the effect of buspirone on cognitive functions are contradictory, some studies show a moderate positive effect on regulatory functions, while others show no clear effect [13]. In any case, unlike benzodiazepines and sedatives, buspirone does not have a negative effect on cognitive functions, which distinguishes it from other drugs used to correct anxiety disorders [14].
Use of buspirone for the treatment of dependence syndrome
Due to its dopaminergic action, buspirone can be used to treat dependence syndrome. Initially, this quality was found in relation to addiction to cocaine. It has been experimentally shown that intramuscular administration of buspirone blocks D2 and D3 receptors, while oral administration of buspirone blocks D3 receptors more selectively, occupying more than 80% of the receptors. Thus, for the treatment of addiction, higher doses may be required - 2-3 times higher than for the treatment of anxiety (up to a maximum of 60 mg). As shown by previous studies, these doses are safe and well tolerated [15]. Correction of withdrawal anxiety under the influence of buspirone may also contribute to the treatment of alcohol and tobacco dependence [16-18].
Thus, for the treatment of addiction, higher doses may be required - 2-3 times higher than for the treatment of anxiety (up to a maximum of 60 mg). As shown by previous studies, these doses are safe and well tolerated [15]. Correction of withdrawal anxiety under the influence of buspirone may also contribute to the treatment of alcohol and tobacco dependence [16-18].
Use of buspirone in extrapyramidal disorders
Experimental and clinical studies indicate that buspirone may be effective in the treatment of tardive dyskinesia. Tardive dyskinesia is characterized by involuntary movements involving the muscles of the head, limbs, or trunk. It usually occurs against the background of long-term therapy with antipsychotics, often manifesting itself or intensifying after their cancellation. Tardive dyskinesia is usually resistant to various treatments. Although the evidence base for buspirone in tardive dyskinesia is low, it may be an alternative to others (particularly dopaminergic drugs) with dangerous side effects. The mechanism of action of buspirone in tardive dyskinesia is unclear [19, twenty].
The mechanism of action of buspirone in tardive dyskinesia is unclear [19, twenty].
Buspirone may also be effective in patients with Parkinson's disease suffering from dyskinesias on the background of long-term levodopa therapy. The mechanism of action of the drug is not clear enough in this case either, but the therapeutic effect depends on the dose. In recent years, using pathomorphological and imaging methods, it has been shown that the serotonergic system is involved in the pathological process in Parkinson's disease, in particular, in the pathogenesis of a number of non-motor symptoms, as well as medicinal dyskinesias. Because of this, drugs that act on the serotonergic system can be effective against dyskinesias and non-motor symptoms such as depression, chronic fatigue, and psychotic disorders [21].
It has already been mentioned that 5-HT1A receptor agonists regulate striatal concentrations of dopamine formed from exogenous levodopa, whereby buspirone can reduce drug-induced dyskinesias ("peak dose") in Parkinson's disease.
In a clinical study [22], it was shown that consecutive administration of the drug for 3 days (at a dose of 15-30 mg / day), but not a single dose of the drug at a dose of 10 and 20 mg, led to a 20% reduction in dyskinesias (without an increase in symptoms parkinsonism). In another study, a 3-week dose of buspirone at a dose of 20 mg/day reduced the severity of drug-induced dyskinesias by 71% without any negative effect on the symptoms of parkinsonism. Thus, buspirone can be considered as a potentially effective strategy in the correction of drug-induced dyskinesias.
These clinical data are experimentally confirmed - at a dose of 2 mg / kg, buspirone attenuated violent movements by 45% in mice with an experimental model of dopaminergic dyskinesias. Administration of buspirone to rats at a dose of 0.25-2.5 mg/kg 30 min before levodopa reduced dyskinesias and improved locomotor activity. In the experiment, buspirone reduced catalepsy in rats induced by 6-OHDA and haloperidol.
The effectiveness of buspirone was also shown in dyskinesias that occurred after transplantation of fetal midbrain tissue. It is believed that transplantation dyskinesias are associated with serotonergic neurotransmission [23]. Correction of dyskinesias is more effective with a high dose of 5-HT1A agonist, which more completely blocks mediator release. Dopaminergic reinnervation after transplantation causes persistent dyskinesias due to the uncontrolled release of dopamine induced by serotonin. The release of dopamine occurs in this case with a lower intensity than with "peak dose" dyskinesia. Accordingly, the effect in this situation is more pronounced with systemic administration of lower doses of 5-HT1A agonists [22, 23].
Buspirone can be effective in hereditary spinocerebellar ataxia, which is explained by the pronounced serotonergic innervation of the cerebellum [24]. It is suggested that this effect may also be associated with an effect on the noradrenergic pathways. This assumption has been confirmed in several studies showing that buspirone reduces mild to moderate cerebellar ataxia by 37%. The positive effect of buspirone on the severity of ataxia was confirmed in a small placebo-controlled study [25, 26].
This assumption has been confirmed in several studies showing that buspirone reduces mild to moderate cerebellar ataxia by 37%. The positive effect of buspirone on the severity of ataxia was confirmed in a small placebo-controlled study [25, 26].
Practical aspects of the use of buspirone (Spitomin)
The main indications for the use of buspirone (spitomin) registered in the Russian Federation are generalized anxiety disorder (GAD), panic disorder, autonomic dysfunction syndrome, alcohol withdrawal syndrome (as adjuvant therapy), depressive disorders (as adjuvant therapy, but not prescribed for monotherapy depression). The literature describes the use of buspirone for various anxiety conditions, tobacco withdrawal, depression, as well as autism, obsessive-compulsive and premenstrual syndromes (in which the drug acts as an adjuvant). The mechanism of action makes it possible to use it for the treatment of resistant depression (in combination with an antidepressant) [27].
The therapeutic (anxiolytic) effect develops gradually, manifests itself after 7-14 days and reaches a maximum after 4 weeks.
The goal of treatment for mood disorders may be to achieve complete remission or at least symptomatic relief, and to prevent possible relapses if possible. In chronic anxiety disorders, long-term maintenance therapy with buspirone may be required for long-term symptom control.
An important advantage of buspirone is that, unlike classical anxiolytics such as benzodiazepines, it does not adversely affect psychomotor functions, does not cause tolerance, drug dependence and withdrawal symptoms, and does not potentiate the effect of alcohol. However, during the period of treatment with buspirone, alcohol should be excluded [28].
The absence of a therapeutic effect within 6-8 weeks requires an increase in the dose, but in some cases indicates resistance to the drug. In the absence of an effect, the drug is usually replaced with another agent (benzodiazepine or antidepressant). With a partial effect, an antidepressant, sedative or hypnotic (with insomnia) can be added to enhance its action. Especially often, buspirone is used in combination with an SSRI or a selective serotonin and norepinephrine reuptake inhibitor (SNRI) [29].
With a partial effect, an antidepressant, sedative or hypnotic (with insomnia) can be added to enhance its action. Especially often, buspirone is used in combination with an SSRI or a selective serotonin and norepinephrine reuptake inhibitor (SNRI) [29].
Use in persons under 18 years of age is contraindicated, according to the current instructions in the Russian Federation for buspirone. In children and adolescents from 6 to 18 years of age, no efficacy studies have been conducted in relation to anxiety disorder. Pregnancy and breastfeeding are also contraindications, although there is no direct evidence of danger.
Buspirone is generally well tolerated. Side effects, if they are observed, usually occur at the beginning of the course of treatment and then disappear, despite the continuation of the drug. In some cases, a dose reduction is necessary. As a side effect, the drug can cause dizziness, headache, weakness, sleep disturbance, decreased attention, extrapyramidal disorders (very rarely), confusion, nausea, dry mouth, diarrhea, vomiting, constipation, weight loss, weight gain, myalgia, muscle spasms, rash, sweating, paresthesia. In case of an overdose, vomiting, dizziness, miosis, depression of consciousness are possible. The drug is carefully combined with antipsychotics, cardiac glycosides, antihypertensive and antidiabetic agents, oral contraceptives. Interaction with MAO inhibitors can lead to serotonin syndrome or hypertensive crisis with more limited symptoms, therefore, the simultaneous use of buspirone and MAO inhibitors is contraindicated in the instructions for medical use.
In case of an overdose, vomiting, dizziness, miosis, depression of consciousness are possible. The drug is carefully combined with antipsychotics, cardiac glycosides, antihypertensive and antidiabetic agents, oral contraceptives. Interaction with MAO inhibitors can lead to serotonin syndrome or hypertensive crisis with more limited symptoms, therefore, the simultaneous use of buspirone and MAO inhibitors is contraindicated in the instructions for medical use.
In the Russian Federation, the drug is presented in the form of 10 mg divided tablets. The initial dose is 5 mg / day, if necessary, it is increased by 5 mg every 5 days. The average daily dose is 15 mg. The maximum single dose is 30 mg, the maximum daily dose is 60 mg. The daily dose is usually divided into 2-3 doses. The advantages of the drug include safety, lack of dependence and withdrawal syndrome, sexual dysfunction and weight gain. Moreover, buspirone is able to reduce sexual dysfunction caused by generalized anxiety and serotonergic antidepressants [28, 30].
The peculiarities of the drug include the gradual onset of the full clinical effect (within 4 weeks), while benzodiazepines act more quickly.
Buspirone is metabolized primarily by the microsomal enzyme CYP450 3A4. T½ is approximately 2-3 hours. Particular care should be taken when combined with CYP450 3A4 inhibitors (for example, diltiazem, verapamil, itraconazole, erythromycin), which can reduce the clearance of buspirone and increase its level in the blood. You should also avoid drinking large amounts of grapefruit and grapefruit juice at the same time. The dose of buspirone should also be reduced when using HIV protease inhibitors or ketoconazole. Conversely, CYP450 3A4 inducers (eg carbamazepine and rifampicin) may increase the clearance of buspirone. Buspirone increases blood levels of nordiazepam, the active metabolite of diazepam, which can cause dizziness, headache, and nausea.
In mild to moderate renal and hepatic insufficiency, liver cirrhosis, heart failure, in the elderly, the drug is prescribed in smaller doses. When discontinuing the drug, a gradual dose reduction is usually not necessary. In severe renal, hepatic insufficiency, uncontrolled epilepsy, glaucoma, myasthenia gravis, the drug is contraindicated.
When discontinuing the drug, a gradual dose reduction is usually not necessary. In severe renal, hepatic insufficiency, uncontrolled epilepsy, glaucoma, myasthenia gravis, the drug is contraindicated.
Thus, buspirone, with its unique neurotransmitter effects, significantly expands the possibilities of treatment for a wide range of mental and neurological disorders - from anxiety disorders to dyskinesia in Parkinson's disease and ataxia. The relative safety of the drug makes its use in clinical practice very promising.
Buspiron instructions, price in pharmacies of Ukraine
Dosage
- Buspirone: 5 mg/tablet (1)
- Buspirone: 10 mg/tablet (1)
Who can
- Older (2)
- Vagi (2)
- Allergic (2)
- Diabetic (2) 9015 (2)
Mutual relations
- Last (1)
- No value (1)
- Product list
- Prices in pharmacies
- Analogues
Product: 2
Sorting: Behind the ratingVid cheapVid expensive
Go to box
Go to box
Analogs Show all
Go to bowl
Go to bowl
Buying goods
-
Type 245.
 20 UAH
20 UAH -
Type 213.80 UAH
-
Type 465.10 UAH
-
Type 479.90 UAH
-
Type 832.
 00 UAH
00 UAH -
Type 559.70 UAH
Editorial team
Creation date: 04/27/2021 Date updated: 01.12.2022
Warehouse and release form
- tab. 5 mg blister, № 20
- Buspirone 5 mg
- tab. 10 mg blister, № 20
- Buspirone 10 mg
Pharmacological activity
Buspiron - an anxiolytic drug zasib, zastosovyatsya for exaltation of anxious states of various walks, especially neuroses, which are accompanied by feelings of anxiety, restlessness, tension, drama. The mechanism of action of buspirone has not been established, but it is known that it is responsible for the mechanism of action of benzodiazepines and other anxiolytic effects.

Buspirone is highly potent as presynaptic 5HT1A receptors and as a frequent agonist of postsynaptic 5HT1A receptors in the CNS. In preclinical studies, experimental models showed that buspiron had powers characteristic of anxiolytics and antidepressants. In the presence of benzodiazepines, buspirone does not show anticonvulsant and muscle relaxant effects, does not cause a chirp, and after completion of the course of treatment, no symptoms develop. Diya buspironu develop step by step. The therapeutic effect begins to appear between the 7th and 14th days of therapy, and the maximum effect is reached only after about 4 days after the cob of treatment.
Pharmacokinetics. After ingestion, the drug is dry and may be more absorbed from the intestinal tract. Equally important plasma concentrations may be reached after approximately 2 doses after the cob of regular ingestion of the drug.
Buspirone is subject to intensive first pass metabolism through the liver.
 Systemic bioavailability to become 4%. Cmax of drug metabolism in blood plasma is also reached after 60-90 minutes.
Systemic bioavailability to become 4%. Cmax of drug metabolism in blood plasma is also reached after 60-90 minutes. close 9Buspirone 5% binds to plasma proteins. T½ of blood plasma becomes 2-3 years. Pharmacological parameters of the drug do not change when taking the drug without interruption (cumulative daily).
The main pharmacologically active metabolite of buspiron is (1-[2-pyrimidinyl]-piperazine (1-PP). 2 times dow, lower for buspiron.0003
Indications
symptomatic relief of anxiety states with dominant symptoms: anxiety, internal restlessness, stress state.
Dosing
doses are determined by the drug individually for the skin patient in case of illness. On the cob of therapy, 5 mg of buspiron hydrochloride is prescribed 2-3 times a day. To achieve the maximum therapeutic effect, the additional dose should be incrementally increased to 15-30 mg of buspirone, subdivided into five doses.
The maximum single dose should not exceed 30 mg.

The maximum supplementary dose should not exceed 45 mg.
Tablets should be taken at the same time, do not drink, drink a small amount of rind, directly from the patient.
If necessary, place the tablet half-and-half in two halves on a hard surface, risking burning and pressing lightly with your thumb.
Special patient groups. With a decrease in the function of the liver, one / the user should stop the minimum possible dose.
Trivality of glee. Tranquilizers cannot be stopped without control over a prolonged period. If it is necessary to administer the drug (≤6 mіs), then further medical monitoring should be carried out. Next memory about the conduct of psychotherapeutic and sociotherapeutic visits in parallel with the treatment of buspirone.
Contraindications
increased sensitivity to Buspirone or to one of the components of the drug; gostra congestive glaucoma; malignant mastonia; important dysfunction of the liver; heavy nirkov deficiency; epilepsy; period of breastfeeding; century to 18 years.

Side effects
from the side of the cardiovascular system: often - non-specific pain in the chest; inodі - timchasova vtrata svіdomosti, arterial hypotension and/or hypertension, tachycardia / apparently heartbeat; rarely - damage to cerebral circulation, heart failure, myocardial infarction, cardiomyopathy, bradycardia.
From the side of the blood system: rarely - changes in blood tests (eosinophilia, leukopenia, thrombocytopenia).
On the side of the psyche: often - nightmares, drowsiness, sleeplessness, confusion, nervousness, decreased concentration of respect, emotional arousal, drativity, fortune-telling, confusion, depression; rarely - depersonalization, discomfort, pathological spontaneity of loud sounds, euphoria, hyperkinesia, restlessness, impaired associative spontaneity, hallucinations, suicidal thoughts, epileptic attacks; rіdko - sharp change in mood, claustrophobia, stupor, unrecognizable language, psychosis, problems to go through memory, serotonin syndrome.

From the side of the central nervous system: sometimes - names, paresthesia (for example, tingling, feeling pain), impaired coordination, tremor; Rarely, spontaneous collapse, galvanism, extrapyramidal symptoms, including early and late dyskinesia, impaired tone, parkinsonism, akathisia.
On the side of the organ: often - cloudy eyes; inodі - chervonіnnya i sverbіzh in the region of eyes, conjunctivitis; rіdko - photophobia, vіdchuttya vnutrіshnoochnogo vice, bіl in the eyes, the field of dawn sounded.
To the side of the organ of hearing: often - noise in the ears.
On the side of the dichal system: often - sore throat, stuffy nose; inodi - sooner dihannya, zadishka, bіl in the region of the heart; rarely - nose bleeding.
From the side of the intestinal tract: often - nudity, xerostomia, epigastric dilatation, diarrhea; sometimes - flatulence, loss of appetite, increased appetite, hypersalivation, colon teasing syndrome, bleeding from the rectum, constipation, vomiting.
On the side of the slitting system: sometimes - often slashing, cutting slitting; rarely - enuresis, no sechoviprosy.
To the side of the coats: sometimes - swelling, croup, hyperemia, hematomas, obliquity, dryness of the coats, eczema, swelling, swelling; rarely - allergic reactions, ecchymosis, acne, thinning of the nails.
To the side of the musculoskeletal apparatus: sometimes - spasm and stiffness of the tongue, myalgia, arthralgia; rarely - myasthenia.
On the side of the endocrine system: rarely - galactorrhea, gynecomastia, dysfunction of the thyroid gland.
Head injuries: often - headache, asthenia; inodі - zbіlshennya masi tіla, fever, zvіn na golovі, zmenshennya masi tіla, unsickness, increased stomlyuvanіst, impaired scent and gustatory smells, increased sweating, hot flushes, cold hyperesthesia; rarely - skhilnist to malice with alcohol, blood coagulation disorder, loss of voice, hooting, glossalgia.
From the side of the hepatobiliary system: rarely - an increase in liver enzymes.
On the side of the reproductive system: sometimes - disruption of the menstrual cycle, change or increase in libido; rarely - amenorrhea, inflammation of the secretory organs, decreased ejaculation, impotence.
Specific indications
Clinical and preclinical studies did not show a sign that could indicate a risk of causation or exposure to Buspirone, however, the indication of the drug is due to primer.
Buspirone is not indicated for the treatment of withdrawal symptoms, benzodiazepine congestion, or other sedative/sedative drug conditions. That is why it is necessary to step-by-step administer the injection of these preparations to the cob with buspirone. This is especially important for patients, for example, they take medications that detract from the central nervous system. Do not prescribe buspirone to patients with a history of epilepsy attacks.
We are ill with impaired functions of the liver and liver in history.
Buspiron Sandoz is lactose-resistant, which has not been reported in patients with mild galactose intolerance, lactase deficiency, or glucose-galactose malabsorption syndrome.

Congestion during pregnancy and breastfeeding. Given the ingestion of buspirone during the period of pregnancy during the day, the drug can only be considered in that period, if the measles for the mother is overwhelmed by the potential risk for the fetus. Buspirone penetrates into breast milk;
Children. Do not prescribe buspirone to children due to the lack of safety and efficacy.
The ability to increase the speed of the reaction when caring for vehicles or robots with other mechanisms. The hour of leniency should be minimized by transport means or by robots with other mechanisms, shards can lead to side reactions from the side of the central nervous system and psyche.
Oxils of buspirone are primarily metabolized by cytochrome P450, inhibition of the inhibitory enzyme may increase the bioavailability of buspirone.
Nefazodon. One-hour ingestion of buspirone and nefazodone to increase Cmax of buspirone in blood plasma by 20 times and AUC by 50 times.

Erythromycin. One-hour ingestion of buspirone and erythromycin can lead to an increase in Cmax of buspirone by 5 times and AUC by 6 times.
Itraconazole. Overnight administration of buspirone and itraconazole resulted in a 13-fold increase in buspirone Cmax and 19-fold increase in AUCrazіv.
Diltiazem. One-hour infusion of buspirone and diltiazem leads to an increase in Cmax of buspirone by 4 times and AUC by 5.3 times.
Verapamil. An overnight dose of buspirone and verapamil should result in a 3.4-fold increase in Cmax and AUC for buspirone.
Cimetidine. Odnochasno zastosuvanya buspirone and cimetidine lead to an increase in the Cmax of buspirone by 40%, Tmax - 2 times, but the AUC practically does not change.
If buspirone is ingested at the same time due to medical considerations, the therapeutic effect and toxicity of buspirone increase, it is recommended that the dose of buspirone be reduced (for example, 2.5 mg 2 times per dose).
Rifampicin.
 An overnight dose of buspirone and rifampicin should result in a change in Cmax for buspirone by 83.9% and AUC by 89.6%.
An overnight dose of buspirone and rifampicin should result in a change in Cmax for buspirone by 83.9% and AUC by 89.6%. Inhibitor and inducer of CYP 3A4. Ketoconazole and ritonavir inhibit the metabolism of buspiron and increase blood plasma levels. If buspirone is administered concomitantly with a CYP 3A4 inhibitor, a lower dose is recommended. CYP 3A4 inducers, such as dexamethasone, phenytoin, phenobarbital, or carbamazepine, may increase the metabolic rate of buspiron. In this case, it is necessary to increase the dose of buspirone to preserve its anxiolytic efficacy.
Serotonin ingestion inhibitor. In clinical studies, there was no relapse of unsafe ingestion of buspirone concomitantly with antidepressants, selective serotonin ingestion inhibitors. Boulli okremі vodomlennya pro viniknennya podadіv ї їkh trivalno zastosuvanni podednanny z buspironom.
Haloperidol. Overnight exposure to buspirone and haloperidol led to an increase in the concentration of haloperidol in the blood serum.

Trazodone. It was reported that in some patients with one-hour ingestion of trazodone with buspirone, AST activity increased by 3 times. However, such an increase in hepatic transaminases has not been confirmed by clinical evidence.
Diazepam. With one-hour instillation of diazepam and buspiron, rhubarb in the blood plasma rises, and can also cause side effects: confusion, headache, boredom.
The first hour of drinking with buspirone will soon disappear from the introduction of alcoholic drinks.
It is not recommended for patients to drink grapefruit juice in significant quantities, but it can lead to an increase in the level of buspiron in the blood plasma to an increase in the frequency or severity of side effects.
Overdose
Symptoms: nausea, vomiting, constipation, exhaustion, miosis and dysfunction of the mucosal-intestinal tract. More important complications in humans have not been reported with daily doses up to 2400 mg.