Average time off work with depression
SAMHSA’s National Helpline | SAMHSA
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Main page content
-
SAMHSA’s National Helpline is a free, confidential, 24/7, 365-day-a-year treatment referral and information service (in English and Spanish) for individuals and families facing mental and/or substance use disorders.
Also visit the online treatment locator.
SAMHSA’s National Helpline, 1-800-662-HELP (4357) (also known as the Treatment Referral Routing Service), or TTY: 1-800-487-4889 is a confidential, free, 24-hour-a-day, 365-day-a-year, information service, in English and Spanish, for individuals and family members facing mental and/or substance use disorders.
This service provides referrals to local treatment facilities, support groups, and community-based organizations.
Also visit the online treatment locator, or send your zip code via text message: 435748 (HELP4U) to find help near you. Read more about the HELP4U text messaging service.
The service is open 24/7, 365 days a year.
English and Spanish are available if you select the option to speak with a national representative. Currently, the 435748 (HELP4U) text messaging service is only available in English.
In 2020, the Helpline received 833,598 calls. This is a 27 percent increase from 2019, when the Helpline received a total of 656,953 calls for the year.
The referral service is free of charge. If you have no insurance or are underinsured, we will refer you to your state office, which is responsible for state-funded treatment programs. In addition, we can often refer you to facilities that charge on a sliding fee scale or accept Medicare or Medicaid. If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
The service is confidential. We will not ask you for any personal information. We may ask for your zip code or other pertinent geographic information in order to track calls being routed to other offices or to accurately identify the local resources appropriate to your needs.
No, we do not provide counseling. Trained information specialists answer calls, transfer callers to state services or other appropriate intake centers in their states, and connect them with local assistance and support.
-
Suggested Resources
What Is Substance Abuse Treatment? A Booklet for Families
Created for family members of people with alcohol abuse or drug abuse problems. Answers questions about substance abuse, its symptoms, different types of treatment, and recovery. Addresses concerns of children of parents with substance use/abuse problems.
Addresses concerns of children of parents with substance use/abuse problems.It's Not Your Fault (NACoA) (PDF | 12 KB)
Assures teens with parents who abuse alcohol or drugs that, "It's not your fault!" and that they are not alone. Encourages teens to seek emotional support from other adults, school counselors, and youth support groups such as Alateen, and provides a resource list.After an Attempt: A Guide for Taking Care of Your Family Member After Treatment in the Emergency Department
Aids family members in coping with the aftermath of a relative's suicide attempt. Describes the emergency department treatment process, lists questions to ask about follow-up treatment, and describes how to reduce risk and ensure safety at home.Family Therapy Can Help: For People in Recovery From Mental Illness or Addiction
Explores the role of family therapy in recovery from mental illness or substance abuse. Explains how family therapy sessions are run and who conducts them, describes a typical session, and provides information on its effectiveness in recovery.
For additional resources, please visit the SAMHSA Store.
Last Updated: 08/30/2022
Alcohol, Tobacco, and Other Drugs
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Misusing alcohol, tobacco, and other drugs can have both immediate and long-term health effects.The misuse and abuse of alcohol, tobacco, illicit drugs, and prescription medications affect the health and well-being of millions of Americans. NSDUH estimates allow researchers, clinicians, policymakers, and the general public to better understand and improve the nation’s behavioral health. These reports and detailed tables present estimates from the 2021 National Survey on Drug Use and Health (NSDUH).
Alcohol
Data:
- Among the 133.1 million current alcohol users aged 12 or older in 2021, 60.0 million people (or 45.1%) were past month binge drinkers.
 The percentage of people who were past month binge drinkers was highest among young adults aged 18 to 25 (29.2% or 9.8 million people), followed by adults aged 26 or older (22.4% or 49.3 million people), then by adolescents aged 12 to 17 (3.8% or 995,000 people). (2021 NSDUH)
The percentage of people who were past month binge drinkers was highest among young adults aged 18 to 25 (29.2% or 9.8 million people), followed by adults aged 26 or older (22.4% or 49.3 million people), then by adolescents aged 12 to 17 (3.8% or 995,000 people). (2021 NSDUH) - Among people aged 12 to 20 in 2021, 15.1% (or 5.9 million people) were past month alcohol users. Estimates of binge alcohol use and heavy alcohol use in the past month among underage people were 8.3% (or 3.2 million people) and 1.6% (or 613,000 people), respectively. (2021 NSDUH)
- In 2020, 50.0% of people aged 12 or older (or 138.5 million people) used alcohol in the past month (i.e., current alcohol users) (2020 NSDUH)
- Among the 138.5 million people who were current alcohol users, 61.6 million people (or 44.4%) were classified as binge drinkers and 17.7 million people (28.8% of current binge drinkers and 12.8% of current alcohol users) were classified as heavy drinkers (2020 NSDUH)
- The percentage of people who were past month binge alcohol users was highest among young adults aged 18 to 25 (31.
 4%) compared with 22.9% of adults aged 26 or older and 4.1% of adolescents aged 12 to 17 (2020 NSDUH)
4%) compared with 22.9% of adults aged 26 or older and 4.1% of adolescents aged 12 to 17 (2020 NSDUH) - Excessive alcohol use can increase a person’s risk of stroke, liver cirrhosis, alcoholic hepatitis, cancer, and other serious health conditions
- Excessive alcohol use can also lead to risk-taking behavior, including driving while impaired. The Centers for Disease Control and Prevention reports that 29 people in the United States die in motor vehicle crashes that involve an alcohol-impaired driver daily
Programs/Initiatives:
- STOP Underage Drinking interagency portal - Interagency Coordinating Committee on the Prevention of Underage Drinking
- Interagency Coordinating Committee on the Prevention of Underage Drinking
- Talk. They Hear You.
- Underage Drinking: Myths vs. Facts
- Talking with your College-Bound Young Adult About Alcohol
Relevant links:
- National Association of State Alcohol and Drug Abuse Directors
- Department of Transportation Office of Drug & Alcohol Policy & Compliance
- Alcohol Policy Information Systems Database (APIS)
- National Institute on Alcohol Abuse and Alcoholism
Tobacco
Data:
- In 2020, 20.
 7% of people aged 12 or older (or 57.3 million people) used nicotine products (i.e., used tobacco products or vaped nicotine) in the past month (2020 NSDUH)
7% of people aged 12 or older (or 57.3 million people) used nicotine products (i.e., used tobacco products or vaped nicotine) in the past month (2020 NSDUH) - Among past month users of nicotine products, nearly two thirds of adolescents aged 12 to 17 (63.1%) vaped nicotine but did not use tobacco products. In contrast, 88.9% of past month nicotine product users aged 26 or older used only tobacco products (2020 NSDUH)
- Tobacco use is the leading cause of preventable death, often leading to lung cancer, respiratory disorders, heart disease, stroke, and other serious illnesses. The CDC reports that cigarette smoking causes more than 480,000 deaths each year in the United States
- The CDC’s Office on Smoking and Health reports that more than 16 million Americans are living with a disease caused by smoking cigarettes
Electronic cigarette (e-cigarette) use data:
- In 2021, 13.2 million people aged 12 or older (or 4.7%) used an e-cigarette or other vaping device to vape nicotine in the past month.
 The percentage of people who vaped nicotine was highest among young adults aged 18 to 25 (14.1% or 4.7 million people), followed by adolescents aged 12 to 17 (5.2% or 1.4 million people), then by adults aged 26 or older (3.2% or 7.1 million people).
The percentage of people who vaped nicotine was highest among young adults aged 18 to 25 (14.1% or 4.7 million people), followed by adolescents aged 12 to 17 (5.2% or 1.4 million people), then by adults aged 26 or older (3.2% or 7.1 million people). - Among people aged 12 to 20 in 2021, 11.0% (or 4.3 million people) used tobacco products or used an e-cigarette or other vaping device to vape nicotine in the past month. Among people in this age group, 8.1% (or 3.1 million people) vaped nicotine, 5.4% (or 2.1 million people) used tobacco products, and 3.4% (or 1.3 million people) smoked cigarettes in the past month. (2021 NSDUH)
- Data from the Centers for Disease Control and Prevention’s 2020 National Youth Tobacco Survey. Among both middle and high school students, current use of e-cigarettes declined from 2019 to 2020, reversing previous trends and returning current e-cigarette use to levels similar to those observed in 2018
- E-cigarettes are not safe for youth, young adults, or pregnant women, especially because they contain nicotine and other chemicals
Resources:
- Tips for Teens: Tobacco
- Tips for Teens: E-cigarettes
- Implementing Tobacco Cessation Programs in Substance Use Disorder Treatment Settings
- Synar Amendment Program
Links:
- Truth Initiative
- FDA Center for Tobacco Products
- CDC Office on Smoking and Health
- National Institute on Drug Abuse: Tobacco, Nicotine, and E-Cigarettes
- National Institute on Drug Abuse: E-Cigarettes
Opioids
Data:
- Among people aged 12 or older in 2021, 3.
 3% (or 9.2 million people) misused opioids (heroin or prescription pain relievers) in the past year. Among the 9.2 million people who misused opioids in the past year, 8.7 million people misused prescription pain relievers compared with 1.1 million people who used heroin. These numbers include 574,000 people who both misused prescription pain relievers and used heroin in the past year. (2021 NSDUH)
3% (or 9.2 million people) misused opioids (heroin or prescription pain relievers) in the past year. Among the 9.2 million people who misused opioids in the past year, 8.7 million people misused prescription pain relievers compared with 1.1 million people who used heroin. These numbers include 574,000 people who both misused prescription pain relievers and used heroin in the past year. (2021 NSDUH) - Among people aged 12 or older in 2020, 3.4% (or 9.5 million people) misused opioids in the past year. Among the 9.5 million people who misused opioids in the past year, 9.3 million people misused prescription pain relievers and 902,000 people used heroin (2020 NSDUH)
- According to the Centers for Disease Control and Prevention’s Understanding the Epidemic, an average of 128 Americans die every day from an opioid overdose
Resources:
- Medication-Assisted Treatment
- Opioid Overdose Prevention Toolkit
- TIP 63: Medications for Opioid Use Disorder
- Use of Medication-Assisted Treatment for Opioid Use Disorder in Criminal Justice Settings
- Opioid Use Disorder and Pregnancy
- Clinical Guidance for Treating Pregnant and Parenting Women With Opioid Use Disorder and Their Infants
- The Facts about Buprenorphine for Treatment of Opioid Addiction
- Pregnancy Planning for Women Being Treated for Opioid Use Disorder
- Tips for Teens: Opioids
- Rural Opioid Technical Assistance Grants
- Tribal Opioid Response Grants
- Provider’s Clinical Support System - Medication Assisted Treatment Grant Program
Links:
- National Institute on Drug Abuse: Opioids
- National Institute on Drug Abuse: Heroin
- HHS Prevent Opioid Abuse
- Community Anti-Drug Coalitions of America
- Addiction Technology Transfer Center (ATTC) Network
- Prevention Technology Transfer Center (PTTC) Network
Marijuana
Data:
- In 2021, marijuana was the most commonly used illicit drug, with 18.
 7% of people aged 12 or older (or 52.5 million people) using it in the past year. The percentage was highest among young adults aged 18 to 25 (35.4% or 11.8 million people), followed by adults aged 26 or older (17.2% or 37.9 million people), then by adolescents aged 12 to 17 (10.5% or 2.7 million people).
7% of people aged 12 or older (or 52.5 million people) using it in the past year. The percentage was highest among young adults aged 18 to 25 (35.4% or 11.8 million people), followed by adults aged 26 or older (17.2% or 37.9 million people), then by adolescents aged 12 to 17 (10.5% or 2.7 million people). - The percentage of people who used marijuana in the past year was highest among young adults aged 18 to 25 (34.5%) compared with 16.3% of adults aged 26 or older and 10.1% of adolescents aged 12 to 17 (2020 NSDUH)
- Marijuana can impair judgment and distort perception in the short term and can lead to memory impairment in the long term
- Marijuana can have significant health effects on youth and pregnant women.
Resources:
- Know the Risks of Marijuana
- Marijuana and Pregnancy
- Tips for Teens: Marijuana
Relevant links:
- National Institute on Drug Abuse: Marijuana
- Addiction Technology Transfer Centers on Marijuana
- CDC Marijuana and Public Health
Emerging Trends in Substance Misuse:
- Methamphetamine—In 2019, NSDUH data show that approximately 2 million people used methamphetamine in the past year.
 Approximately 1 million people had a methamphetamine use disorder, which was higher than the percentage in 2016, but similar to the percentages in 2015 and 2018. The National Institute on Drug Abuse Data shows that overdose death rates involving methamphetamine have quadrupled from 2011 to 2017. Frequent meth use is associated with mood disturbances, hallucinations, and paranoia.
Approximately 1 million people had a methamphetamine use disorder, which was higher than the percentage in 2016, but similar to the percentages in 2015 and 2018. The National Institute on Drug Abuse Data shows that overdose death rates involving methamphetamine have quadrupled from 2011 to 2017. Frequent meth use is associated with mood disturbances, hallucinations, and paranoia. - Cocaine—In 2019, NSDUH data show an estimated 5.5 million people aged 12 or older were past users of cocaine, including about 778,000 users of crack. The CDC reports that overdose deaths involving have increased by one-third from 2016 to 2017. In the short term, cocaine use can result in increased blood pressure, restlessness, and irritability. In the long term, severe medical complications of cocaine use include heart attacks, seizures, and abdominal pain.
- Kratom—In 2019, NSDUH data show that about 825,000 people had used Kratom in the past month. Kratom is a tropical plant that grows naturally in Southeast Asia with leaves that can have psychotropic effects by affecting opioid brain receptors.
 It is currently unregulated and has risk of abuse and dependence. The National Institute on Drug Abuse reports that health effects of Kratom can include nausea, itching, seizures, and hallucinations.
It is currently unregulated and has risk of abuse and dependence. The National Institute on Drug Abuse reports that health effects of Kratom can include nausea, itching, seizures, and hallucinations.
Resources:
- Tips for Teens: Methamphetamine
- Tips for Teens: Cocaine
- National Institute on Drug Abuse
More SAMHSA publications on substance use prevention and treatment.
Last Updated: 01/05/2023
No sleep, no rest for the tormented soul
Sleep is one of the basic needs of the human body, and its lack leads to severe psychological and physical stress: not only mood and cognitive abilities suffer, but also the cardiovascular system and metabolism. Nevertheless, for almost 50 years, sleep deprivation has been trying to treat one of the most difficult and terrible conditions for the human psyche - depression. We set out to explore what forced sleep therapy for psychiatric disorders is, why it can be effective, and why it should be used with caution.
Anyone who has not slept for a long time at least once knows perfectly well what this is fraught with: lethargy appears, attention decreases, mood deteriorates and severe physical fatigue occurs. Available stimulants like caffeine stop working (their mechanism of action is rather limited), and the only way out is to take a break and still rest.
In chronic sleep deprivation and insomnia (we talked about it in detail in the material “Your words rock well”, prepared for World Sleep Day last year), deeper and more serious conditions and diseases are added to superficial symptoms.
For example, the consequences of lack of sleep include cardiovascular disease, nutritional and metabolic problems (from overeating to type 2 diabetes), and various mental disorders. Last but not least, lack of sleep is closely associated with depression, which is surprising in its own way, because sleep deprivation is often used to treat it, and at times quite successfully.
At least that's what the meta-analyses suggest. One, conducted in 2017, focuses on 66 studies published since 1974 to 2016: it states that sleep deprivation is effective in 50 percent of patients in randomized control trials and 45 percent in other studies. The effect did not depend on what experimental technique was used, on what preparations the patient was sitting, and also on his gender and age.
The authors of the study call the effect significant, but given the fact that the side variables that would provide the desired effect could not be found, the result can be called random - of course, if we consider the use of sleep deprivation as a binary variable. In other words, when psychiatrists give patients with depression forced sleep therapy, it can either help or not - as luck would have it.
At the same time, sleep deprivation is still considered a fairly effective way to treat depression, and why this is so (even if it is intuitively clear that lack of sleep is more likely to be harmful) should still be understood.
Intervene experimentally
The relationship between sleep quality and mental disorders is complex. First of all, the relationship between them is two-way: insomnia, as well as hypersomnia - excessive sleep duration and daytime sleepiness, are considered both symptoms of depression and factors that largely affect its development.
First of all, therefore, in case of depression, it is necessary to restore normal sleep hygiene: do not eat a few hours before going to bed, go to bed at the same time, sleep the number of hours recommended for age (for an adult - about seven to eight hours a day). day) and do not put off rest for the weekend in anticipation of a cumulative effect.
Obviously this can be quite difficult; in this case, patients with depression are prescribed drugs from the group of neuroleptics or other substances with anti-anxiety (trouble, as you know, does not come alone: with depression, the risk of developing anxiety is higher) or sedative effect.
In the early 1970s, the German psychiatrist Walter Schulte discovered and studied that sleep deprivation could have a therapeutic effect on depression. He observed three patients diagnosed with depressive disorder: two teachers and one doctor. Each of them reported to Schulte that after a sleepless night at work or playing sports, they feel an improvement in their mental state.
Of course, it is impossible to base an entire psychiatric practice on three cases, so after the first statements about the benefits of sleep deprivation (after Schulte, two more of his colleagues managed to achieve a significant effect in 23 out of 34 patients), scientists began to actively conduct research.
First, it was necessary to determine exactly how many hours of sleep deprivation it takes to achieve at least some effect - and at what time to start the experiment. Usually, sleep deprivation therapy involves a whole day (or even more: sometimes up to 36-40 hours) of forced wakefulness: the patient is woken up at about one in the morning, after which he does not sleep the whole next day and sometimes even the whole next night.
With this therapy, the intake of any CNS stimulants (even coffee) is excluded, and it is also recommended to combine forced insomnia with light therapy (however, both are considered branches of chromotherapy - artificial "tuning" of sleep and wake cycles).
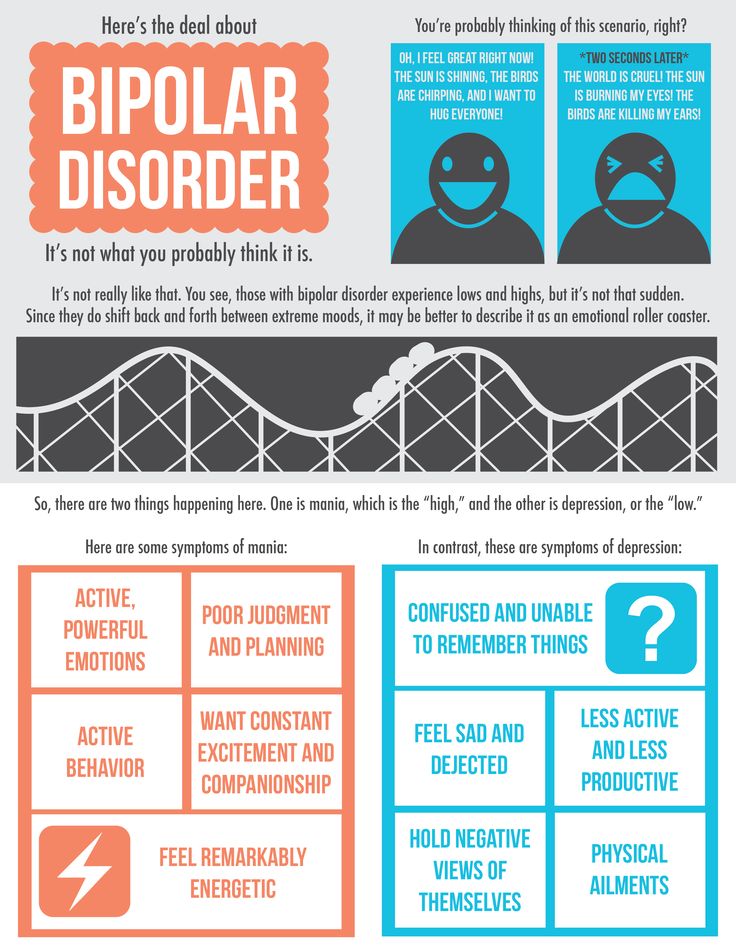
The effect is quite fast: with sleep deprivation in a depressed patient, visible improvements are immediately observed. However, this is a rather deceptive success: studies indicate that in 50-80 percent of patients the state returns to the usual depressive state after they do get some sleep. At the same time, in 10-15 percent of patients, improvements, on the contrary, appear only after sleep following deprivation. In 2-7 percent of patients, the condition may worsen, and symptoms of mania may be added to depression (sleep deprivation, therefore, is not recommended for people with bipolar disorder - even in the depressive phase).
Some vagueness of the effect can be explained by the fact that a day or more without sleep is still quite painful for the body.![]() Therefore, scientists tried to reduce the time of forced wakefulness to a few hours at night. To do this, for example, you can wake up the patient in the middle of the night and keep him awake for a couple of hours. Such a study was conducted in the early 1990s, but forced wakefulness until five in the morning after waking up at three did not give any special effect.
Therefore, scientists tried to reduce the time of forced wakefulness to a few hours at night. To do this, for example, you can wake up the patient in the middle of the night and keep him awake for a couple of hours. Such a study was conducted in the early 1990s, but forced wakefulness until five in the morning after waking up at three did not give any special effect.
Although meta-analyses indicate that there are no precise confounding variables that would provide the desired effect of sleep deprivation, anecdotal studies still state that several conditions must be met for such a method to be effective.
For example, sleep deprivation works best on patients with endogenous depression, rather than depression caused by external factors. In addition, the variation in the patient's mood during the day must also be taken into account: sleep deprivation works most effectively in those who feel better in the evening, rather than during the day.
The mechanism of the therapeutic effect of sleep deprivation has not been fully established. For example, recent research suggests the role of the neurotransmitter adenosine, which accumulates in the brain during the day and is ultimately responsible for making us feel tired and fall asleep.
For example, recent research suggests the role of the neurotransmitter adenosine, which accumulates in the brain during the day and is ultimately responsible for making us feel tired and fall asleep.
Other studies point to the involvement of the serotonergic system, which is central to the pathology of depression, in such therapy. When taking the drug pindolol, which blocks serotonin autoreceptors and improves the effect of antidepressants from the group of selective serotonin reuptake inhibitors, sleep deprivation more effectively improves well-being in depression.
A logical reason for the effectiveness of lack of sleep seems to be its comparison with the use of psychostimulants (eg, amphetamine). Indeed, in the absence of sleep, effects similar to taking psychoactive substances are sometimes observed (you may be familiar with this: sometimes, with a long wakefulness, it seems that there is more strength and energy).
In both cases, the concentration of monoamines in the brain increases (primarily, however, not serotonin, but dopamine), due to which the work of the limbic system stabilizes, and mental well-being improves. Such a theory is consistent with the fact that the effect of sleep deprivation is often unstable and short-lived - like psychostimulants. However, this is still just a theory.
Such a theory is consistent with the fact that the effect of sleep deprivation is often unstable and short-lived - like psychostimulants. However, this is still just a theory.
Use with caution
Despite a fairly long history of study and use in psychiatric practice, sleep deprivation still remains an experimental treatment for depression and is not included in the standard treatment recommendations along with antidepressant drugs and psychotherapy. This is evidenced both by the fact that depression is often treated with sleep deprivation only under controlled conditions (under the supervision of doctors), and by the fact that sleepless nights have many negative consequences.
One of the most serious is the possible increased risk of developing Alzheimer's disease even from one night of sleeplessness. Two proteins play a key role in the development of the disease: beta-amyloid, which forms plaques in the brain, and tau, which contributes to the formation of intracellular neurofibrillary cords.
Studies show that just one sleepless night significantly increases the concentration of beta-amyloid in the brain and tau in the blood. The mechanism of such an action is not fully known in either case, and it is also not clear whether there are actually any negative consequences.
It is also interesting that lack of sleep leads to increased feelings of loneliness and social isolation. Here the effect, however, is more psychological: the lack of sleep makes people look for a variety of ways to escape from the accumulated fatigue, which increases the need for communication. Other people, on the contrary, find a sleepy person more repulsive and do not want to make contact with him.
A rather understandable conflict arises, which makes it difficult to establish communication with others - hence the feeling of loneliness appears. And with depression (unless, of course, it was not there before, since loneliness is one of the common psychological symptoms of a disorder), it is definitely not necessary.
In addition, a recent study showed that a sleepless night reduces the activity of the prefrontal cortex, which is responsible, among other things, for cognitive control. With a decrease in cognitive control, in turn, anxiety increases significantly - and it can significantly worsen the condition of depression.
However, it should be borne in mind that the use of sleep deprivation for the treatment of insomnia and the same technique for behavioral research are two different things. Healthy people without mental disorders take part in the latter; in them, control studies of sleep deprivation therapy show that not getting a night's rest only increases irritability—and doesn't work the way it does for people with depression, even in the short term.
Therefore, it is logical to assume that lack of sleep may not bring negative behavioral and mental aspects to people with depression: review studies also speak about the severity of the presence of mental disorders for the effectiveness of sleep deprivation. But do not forget about the average effectiveness of 50 percent (as well as the fact that the drug treatment of depression has about the same indicators).
But do not forget about the average effectiveness of 50 percent (as well as the fact that the drug treatment of depression has about the same indicators).
So, while sleep deprivation can actually help improve depression, we don't recommend experimenting with your body, brain, and mental state in this way: it's better to have your psychiatrist do it.
Elizaveta Ivtushok
What to do if a loved one is depressed: psychologist explains This time we figure out how to behave if your friend, relative or loved one is depressed: is it worth feeling guilty for what is happening, will support and participation help him, and what to do if you are angry with him.
Writer Ella Derzai, when reading psychological materials on this topic, suggested replacing the word "depression" with the word "leprosy" - simply because many journalists do not try to understand the meaning of this word. It seems to me that this approach well illustrates the difficulties of getting the name of the disease beyond the boundaries of psychiatry (when the word begins to denote a number of things that have nothing to do with the original problem). Imagine materials like "Ten Hot Drinks for Leprosy" or "How to Avoid Winter Leprosy?"
Imagine materials like "Ten Hot Drinks for Leprosy" or "How to Avoid Winter Leprosy?"
So what is depression? Depression is very different.
First, there are three levels of depression—mild, moderate (clinical), and severe (chronic). Mild depression usually goes away on its own in 2-3 months, medium depression can go away on its own or turn into severe depression, if it goes away on its own, then in six months to a year. As a rule, mild and moderate depression can be treated with a psychologist without the use of drugs, but with the use they are faster and easier.
You can no longer confuse severe depression with spleen: a person has a difficult time when he takes great care of himself, including in the sense of hygiene, it is difficult for him to get up, wash dishes, brush his teeth, clean the apartment, leave the house . In very bad situations, he forgets to eat and may die of hunger.
There is a masked depression - this is a depression in which a person is overly cheerful and constantly busy with something so as not to feel how bad he is, how tired and sad he is. This usually leads to a breakdown and the transition of depression to a severe stage.
This usually leads to a breakdown and the transition of depression to a severe stage.
Depressions are also of different types according to sensations. For example, asthenic depression is a severe loss of a resource due to (usually) heavy workloads and stress. It is characterized by an unpleasant feeling of a weight hanging from you, an inability to rejoice (you wake up in the morning - and it feels like you just worked two shifts in the mine).
Anasthenic depression, or depression with derealization, is characterized by a feeling that the world is not real, the walls are cardboard, the view outside the window is drawn, feelings have died out forever, the world has frozen. This type of depression can also accompany more severe mental diagnoses, such as schizophrenia. Also, depression can be with bipolar disorder - and in the other pole, a person is cheerful and full of energy.
Depression can be caused by a hormonal imbalance after childbirth or due to menopause and aging (in a number of modern countries, antidepressants are automatically prescribed for older people). Such depressions include, for example, postpartum depression.
Such depressions include, for example, postpartum depression.
Endogenous depression is caused by internal biochemical processes in the body, usually leads to lifelong medication, because the body is simply not able (or has lost this ability) to produce the necessary substances on its own. Sometimes - very rarely - such depression leads to such severe conditions that it may be the basis for euthanasia in countries where this is possible.
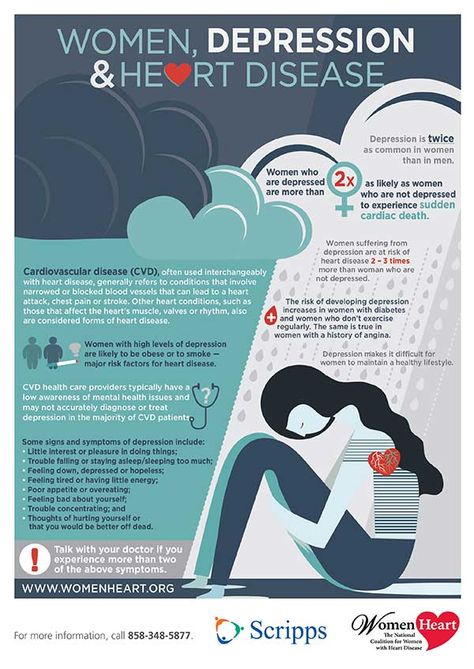
Atypical depression is usually accompanied by a number of other symptoms that are uncharacteristic of ordinary depression, such as severe anxiety, increased appetite (usually in patients before taking antidepressants, their appetite is just reduced), severe somatic pain.
Depression also differs in causes. Psychogenic depression is caused by severe stress, and psychotypical depression is caused by a predisposition of the nervous system and head injuries.
Also, depression can be childish and adolescent (in this category of patients, it usually occurs as a result of severe trauma - a terrible divorce of parents, school bullying, natural or man-made disasters, wars).
This is our set - quite diverse in terms of reasons, ages, statuses and manifestations.
Finding recommendations for relatives of all patients with depression is quite difficult. Therefore, it is probably worth starting with an understanding of what kind of depression your loved one has, how long it lasts and what is needed for it to pass.
For example, with asthenic and psychogenic, as well as with childhood and adolescent depression, rest and recovery, love and support of loved ones, hope - hope is very necessary - and faith in a brighter future. Over time, the body will recover itself. And while he is recovering, in general, the approach is the same as with a severe flu - remind him to take pills, hold his hand, stroke his head and sympathize with what is happening.
In more severe cases, care is very much needed: people in this state really find it difficult to do even household chores, and when taking antidepressants, when the body begins to recover, drowsiness also increases (and, as a rule, libido is depressed). Therefore, such things as many hours of sex, extreme sports, a trip to Burma for a week, snowball fights and long shopping trips will not lead to the fact that Princess Nesmeyana will come to life, but to the fact that she will turn into the shadow of Hamlet's father, which can only cursing indistinctly. He will also get sick for sure with something - from a banal cold to some exotic inflammation of the Achilles tendon and neuralgia.
Therefore, such things as many hours of sex, extreme sports, a trip to Burma for a week, snowball fights and long shopping trips will not lead to the fact that Princess Nesmeyana will come to life, but to the fact that she will turn into the shadow of Hamlet's father, which can only cursing indistinctly. He will also get sick for sure with something - from a banal cold to some exotic inflammation of the Achilles tendon and neuralgia.
If you are not the cause of depression in a person (you have not betrayed, you have not divorced, you have not tried to drown yourself in acid in a Joker costume), do not blame yourself. Depression, like cancer, is caused by a complex combination of different factors, and you are probably not the most important person there.
On the contrary, the ability to stay with a person in depression without depreciation (are you completely lazy?) is a jewelry art that is far from accessible to every person, even if he has a special education.
And it seems to me that an important factor in being around a depressed person is taking care of yourself. Remember that living next to someone who is constantly worried, afraid, or crying is also not easy. Do not lock yourself at home with him, otherwise depression will defeat you too. Look for support in work, friends, trips to nature (if it makes you happy), shopping, skydiving, watching funny comedies - in general, do not forget about yourself. Your life goes on - as does the life of a person with depression.
Remember that living next to someone who is constantly worried, afraid, or crying is also not easy. Do not lock yourself at home with him, otherwise depression will defeat you too. Look for support in work, friends, trips to nature (if it makes you happy), shopping, skydiving, watching funny comedies - in general, do not forget about yourself. Your life goes on - as does the life of a person with depression.
Don't forget about responding to aggression. If you are an ordinary active person who is used to living and enjoying life, then a slow, whiny, tired and weak person, who at the same time has not lost either arms or legs, will cause you a lot of irritation. Find yourself a place where you can swear at such a life and such a sad state of affairs.
Distribute your attention evenly so as not to leave the one who is nearby without support, food and help, and yourself without life and pleasures.
If your loved one is seriously ill for a long time, remember that there are support groups for relatives of patients with psychiatric diagnoses, as well as psychologists and psychotherapists who can support you too.