Adhd neuropsychological test battery
Neuropsychological Testing for ADD/ADHD - Fifth Avenue Psychiatry
Fifth Avenue Psychiatry specializes in the accurate diagnosis of ADD/ADHD which often includes Neuropsychological Testing. Unfortunately, many adolescents, teenagers and adults go misdiagnosed. Psychological Testing can help distinguish an underlying anxiety disorder – or even normal energetic adolescents – from what is truly ADD or ADHD.
Depending on the presenting complaint, age and other factors a battery of psychological tests will be recommended. The specific group of tests can range from a small treatment focused battery to guide treatment to a thorough educational assessment that can uncover potential learning disabilities.
What tests are used to diagnose ADD/ADHD?
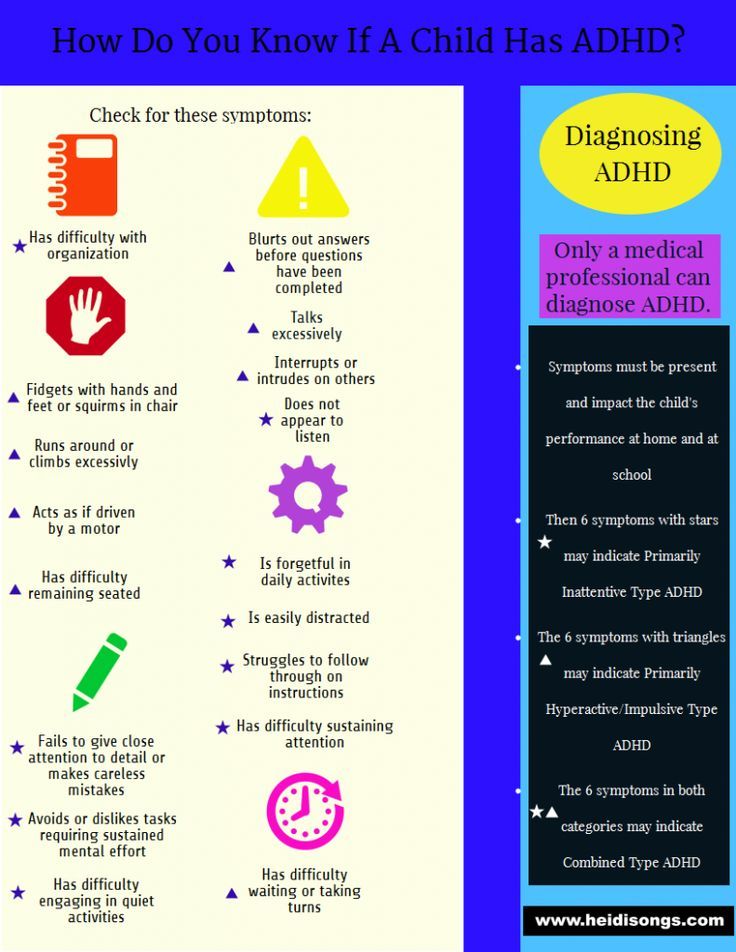
Neuropsychological testing involves a battery of objective and standardized tests. Usually, the doctor gets ADD/ADHD assessments from the parents, teacher or supervisor. Some common rating scales include:
- The Vanderbilt Assessment Scale – reviews symptoms of ADHD according to the DSM-IV criteria.
It also screens for co-existing conditions such as behavioral disorder, oppositional-defiant disorder, anxiety, and depression.
- Behavior Assessment System for Adolescents – assesses hyperactivity, aggression and behavioral problems. It also addresses anxiety, depression, attention and learning problems and lack of certain essential skills.
- Adolescent Behavior Checklist/Teacher Report Form – assesses physical complaints, aggressive or delinquent behavior and withdrawal.
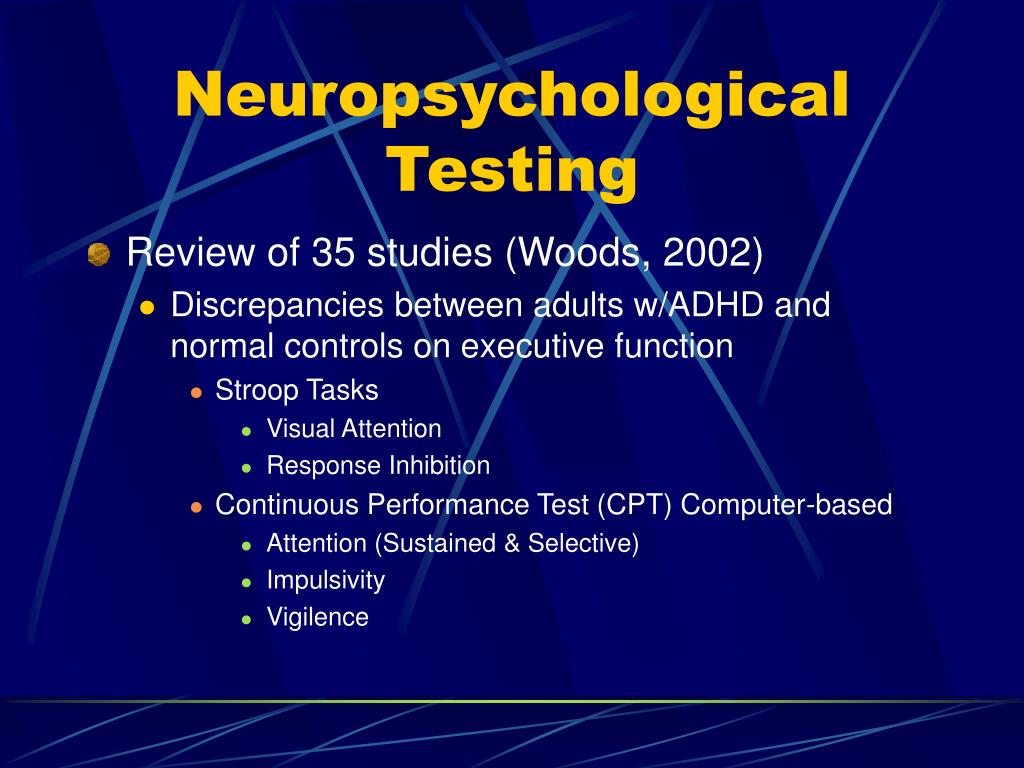
Other important diagnostic tools include computer-based “continuous performance tests” where the adolescent or teen gives very simple responses (i.e., click a button) to a simple stimulus (numbers, letters, etc.) on a computer screen.
These tests are designed to be long and tedious so if an adolescent has ADD/ADHD they will be challenged. The attention they display in this test, and any subsequent mistakes or mistake patterns, are analyzed to help understand the individual weaknesses. Adolescents with ADD/ADHD will make specific errors on this test; some of which also measure hyperactivity.
Adolescents with ADD/ADHD will make specific errors on this test; some of which also measure hyperactivity.
These tests include Continuous Performance tests such as:
- Individual Variables of Attention
- Test of Variables of Attention
- Connors Continuous Performance Test
Simpler Continuous Performance tests, which are shorter in duration and provide less sophisticated data, include:
- Rapidly Recurring Target Figures Test
- Digit Cancellation Tasks
Once there is an ADD/ADHD diagnosis, the doctor may request other tests in order to rule out other causes, such as:
- Blood diseases, i.e., thyroid disease
- Blood lead levels
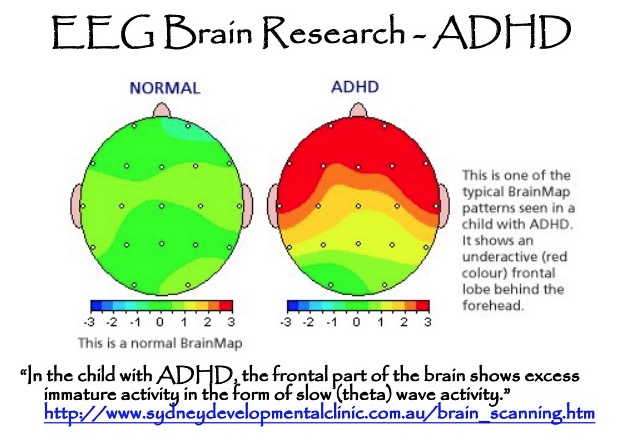
- CT scan or MRI for brain abnormalities
- Encephalograph test brain waves to measure electrical activity in the brain
- Hearing and vision
Neuropsychological assessment of adults with ADHD: A Delphi consensus study
. 2019 Jul-Aug;26(4):340-354.
2019 Jul-Aug;26(4):340-354.
doi: 10.1080/23279095.2018.1429441. Epub 2018 Feb 9.
Anselm B M Fuermaier 1 , Jan A Fricke 1 , Stefanie M de Vries 1 , Lara Tucha 1 , Oliver Tucha 1
Affiliations
Affiliation
- 1 a Department of Clinical and Developmental Neuropsychology, Faculty of Behavioral and Social Sciences , University of Groningen , Groningen , The Netherlands.
- PMID: 29424567
- DOI: 10.
 1080/23279095.2018.1429441
1080/23279095.2018.1429441
Anselm B M Fuermaier et al. Appl Neuropsychol Adult. 2019 Jul-Aug.
. 2019 Jul-Aug;26(4):340-354.
doi: 10.1080/23279095.2018.1429441. Epub 2018 Feb 9.
Authors
Anselm B M Fuermaier 1 , Jan A Fricke 1 , Stefanie M de Vries 1 , Lara Tucha 1 , Oliver Tucha 1
Affiliation
- 1 a Department of Clinical and Developmental Neuropsychology, Faculty of Behavioral and Social Sciences , University of Groningen , Groningen , The Netherlands.
- PMID: 29424567
- DOI: 10.1080/23279095.2018.1429441
Abstract
Within the clinical evaluation of adults with attention deficit hyperactivity disorder (ADHD), cognitive functions are often assessed to characterize individual cognitive problems and guide treatment planning. However, the composition of an adequate neuropsychological assessment battery remains difficult given the large number of cognitive functions that can be distinguished, the variety of available tools to assess these functions, as well as the cognitive heterogeneity that has been observed between individuals with ADHD. Twenty-seven clinicians and researchers experienced in working with adults with ADHD took part in the present study. This study employed the Delphi methodology in order to compose an assessment battery for the measurement of the most important neuropsychological functions by employing the most suitable measures to assess these functions. Consensus between experts was achieved on a ranking of 16 neuropsychological functions that are important for the neuropsychological assessment of adults with ADHD. Furthermore, measures were suggested to assess each of the neuropsychological functions. The assessment battery as composed in the present study may support research and clinical practice in the selection of appropriate functions and measures for the determination of the individual level of cognitive functioning and treatment planning of adults with ADHD.
This study employed the Delphi methodology in order to compose an assessment battery for the measurement of the most important neuropsychological functions by employing the most suitable measures to assess these functions. Consensus between experts was achieved on a ranking of 16 neuropsychological functions that are important for the neuropsychological assessment of adults with ADHD. Furthermore, measures were suggested to assess each of the neuropsychological functions. The assessment battery as composed in the present study may support research and clinical practice in the selection of appropriate functions and measures for the determination of the individual level of cognitive functioning and treatment planning of adults with ADHD.
Keywords: Adult ADHD; Delphi; cognition; neuropsychological assessment.
Similar articles
-
Is motor activity during cognitive assessment an indicator for feigned attention-deficit/hyperactivity disorder (ADHD) in adults?
Fuermaier ABM, Tucha O, Koerts J, Send TS, Weisbrod M, Aschenbrenner S, Tucha L.
 Fuermaier ABM, et al. J Clin Exp Neuropsychol. 2018 Dec;40(10):971-986. doi: 10.1080/13803395.2018.1457139. Epub 2018 Apr 25. J Clin Exp Neuropsychol. 2018. PMID: 29690816
Fuermaier ABM, et al. J Clin Exp Neuropsychol. 2018 Dec;40(10):971-986. doi: 10.1080/13803395.2018.1457139. Epub 2018 Apr 25. J Clin Exp Neuropsychol. 2018. PMID: 29690816 -
Cognitive impairment in adult ADHD--perspective matters!
Fuermaier ABM, Tucha L, Koerts J, Aschenbrenner S, Kaunzinger I, Hauser J, Weisbrod M, Lange KW, Tucha O. Fuermaier ABM, et al. Neuropsychology. 2015 Jan;29(1):45-58. doi: 10.1037/neu0000108. Epub 2014 Jun 16. Neuropsychology. 2015. PMID: 24933488
-
Cognitive heterogeneity in adult attention deficit/hyperactivity disorder: A systematic analysis of neuropsychological measurements.
Mostert JC, Onnink AMH, Klein M, Dammers J, Harneit A, Schulten T, van Hulzen KJE, Kan CC, Slaats-Willemse D, Buitelaar JK, Franke B, Hoogman M.
 Mostert JC, et al. Eur Neuropsychopharmacol. 2015 Nov;25(11):2062-2074. doi: 10.1016/j.euroneuro.2015.08.010. Epub 2015 Aug 21. Eur Neuropsychopharmacol. 2015. PMID: 26336867 Free PMC article.
Mostert JC, et al. Eur Neuropsychopharmacol. 2015 Nov;25(11):2062-2074. doi: 10.1016/j.euroneuro.2015.08.010. Epub 2015 Aug 21. Eur Neuropsychopharmacol. 2015. PMID: 26336867 Free PMC article. -
Utility of cognitive neuropsychological assessment in attention-deficit/hyperactivity disorder.
Lange KW, Hauser J, Lange KM, Makulska-Gertruda E, Takano T, Takeuchi Y, Tucha L, Tucha O. Lange KW, et al. Atten Defic Hyperact Disord. 2014 Dec;6(4):241-8. doi: 10.1007/s12402-014-0132-3. Epub 2014 Mar 18. Atten Defic Hyperact Disord. 2014. PMID: 24639037 Review.
-
[Neuropsychological impairments in adult attention deficit hyperactivity disorder: a literature review].
Bálint S, Czobor P, Mészáros A, Simon V, Bitter I.
 Bálint S, et al. Psychiatr Hung. 2008;23(5):324-35. Psychiatr Hung. 2008. PMID: 19129549 Review. Hungarian.
Bálint S, et al. Psychiatr Hung. 2008;23(5):324-35. Psychiatr Hung. 2008. PMID: 19129549 Review. Hungarian.
See all similar articles
Cited by
-
Stability of Attention Performance of Adults with ADHD over Time: Evidence from Repeated Neuropsychological Assessments in One-Month Intervals.
Guo N, Koerts J, Tucha L, Fetter I, Biela C, König M, Bossert M, Diener C, Aschenbrenner S, Weisbrod M, Tucha O, Fuermaier ABM. Guo N, et al. Int J Environ Res Public Health. 2022 Nov 18;19(22):15234. doi: 10.3390/ijerph292215234. Int J Environ Res Public Health. 2022. PMID: 36429952 Free PMC article.
-
What adults with ADHD want to know: A Delphi consensus study on the psychoeducational needs of experts by experience.
Seery C, Wrigley M, O'Riordan F, Kilbride K, Bramham J. Seery C, et al. Health Expect. 2022 Oct;25(5):2593-2602. doi: 10.1111/hex.13592. Epub 2022 Aug 23. Health Expect. 2022. PMID: 35999687 Free PMC article.
-
Deriving Public Innovation Capacity: Evidence From the Korean Public Sector.
Kim MY, Kim SW. Kim MY, et al. Front Psychol. 2022 Jun 2;13:898399. doi: 10.3389/fpsyg.2022.898399. eCollection 2022. Front Psychol. 2022. PMID: 35719502 Free PMC article.
-
It Takes Time: Vigilance and Sustained Attention Assessment in Adults with ADHD.
Fuermaier ABM, Tucha L, Guo N, Mette C, Müller BW, Scherbaum N, Tucha O. Fuermaier ABM, et al. Int J Environ Res Public Health. 2022 Apr 25;19(9):5216.
 doi: 10.3390/ijerph29095216. Int J Environ Res Public Health. 2022. PMID: 35564612 Free PMC article.
doi: 10.3390/ijerph29095216. Int J Environ Res Public Health. 2022. PMID: 35564612 Free PMC article. -
Primary School Children's Self-Reports of Attention Deficit Hyperactivity Disorder-Related Symptoms and Their Associations With Subjective and Objective Measures of Attention Deficit Hyperactivity Disorder.
Slobodin O, Davidovitch M. Slobodin O, et al. Front Hum Neurosci. 2022 Feb 16;16:806047. doi: 10.3389/fnhum.2022.806047. eCollection 2022. Front Hum Neurosci. 2022. PMID: 35250516 Free PMC article.
See all "Cited by" articles
MeSH terms
Possibilities of neuropsychological correction in overcoming educational difficulties in a younger adolescent with attention deficit hyperactivity disorder
The article describes the main learning difficulties in a younger adolescent with ADHD, with a special emphasis on the neuropsychological causes of such manifestations.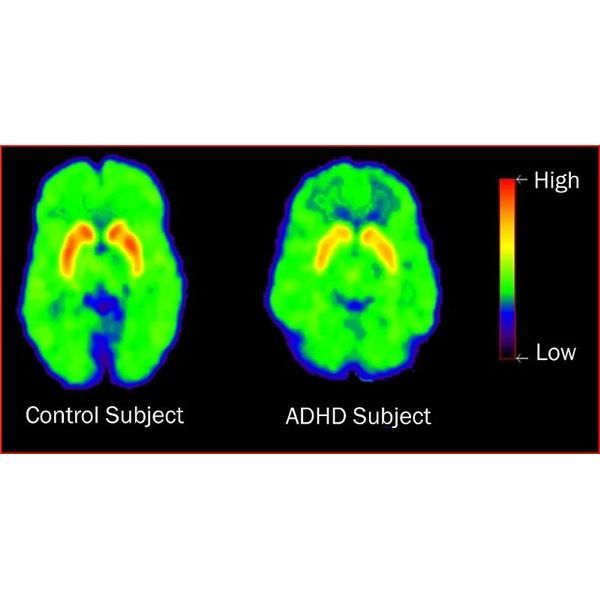 The results before and after neuropsychological correction are presented.
The results before and after neuropsychological correction are presented.
Keywords: nine0012 attention deficit hyperactivity disorder, ADHD, learning difficulties, learning difficulties, younger teenager, neuropsychology, neuropsychological correction.
At present, the search for and elimination of the causes of difficulties that some children have in mastering the school curriculum is one of the main problems. This study focuses on the possibility of correcting learning difficulties in younger adolescents with attention deficit hyperactivity disorder (ADHD), which has recently become more common. To overcome emerging learning difficulties, each child needs an individual approach that takes into account precisely his strengths and weaknesses, this was pointed out, among others, by N. M. Pylaeva and T. V. Akhutina [1;3]. This approach is most developed in neuropsychology, including domestic neuropsychology, based on the ideas of L. S. Vygotsky and built A. R. Luria. Thus, the purpose of this work is to describe the possibilities of neuropsychological correction in overcoming the learning difficulties of a younger adolescent with ADHD. nine0003
S. Vygotsky and built A. R. Luria. Thus, the purpose of this work is to describe the possibilities of neuropsychological correction in overcoming the learning difficulties of a younger adolescent with ADHD. nine0003
Overcoming learning difficulties younger teenager with attention deficit disorder and hyperactivity
The main learning skills that younger teenagers should have at a high level are writing, reading and counting. At the same time, the ability to apply effective mnemonic strategies, the ability to give abstract definitions of words, analyze language metaphors should be formed, and in oral, written stories and retellings of children, much more attention is paid to describing the thoughts and feelings of the characters. It is also necessary to be able to solve mathematical problems in several steps, use different units of measurement and translate them, while younger teenagers must make the transition from arithmetic calculations to simple algebraic ones: solve simple equations, problems with formulas, etc. The development of conceptual thinking contributes to the emergence by the end of primary school age, reflection, which, being a neoplasm of adolescence, transforms not only the cognitive activity of students, but also the nature of their relationship to other people and to themselves. nine0003
The development of conceptual thinking contributes to the emergence by the end of primary school age, reflection, which, being a neoplasm of adolescence, transforms not only the cognitive activity of students, but also the nature of their relationship to other people and to themselves. nine0003
Attention deficit hyperactivity disorder (ADHD) occurs in approximately 1 in 20 children and adolescents today [2]. ADHD in children mainly manifests itself in the form of attention disorders, hyperactivity and impulsivity, which are permanent, non-situational and age-inappropriate. The impulsiveness of a teenager with ADHD is manifested in inaccurate performance of tasks with numerous errors, despite high motivation when performing a task, in restraint in words, deeds and actions [6]. The hyperactivity of such children is manifested in the following features: a reduced level of a sense of security, a tendency to aggressive behavior, increased anxiety, instability to stress, the desire to satisfy their emotions in a fantasy world. In general, they are characterized by a lower level of social maturity than happens at their age [7]. nine0003
In general, they are characterized by a lower level of social maturity than happens at their age [7]. nine0003
In the younger adolescence, cognitive impairments come to the fore: lack of formation of control functions, disorders of attention and working memory. As a result, children with ADHD experience clear learning difficulties.
Domestic neuropsychology of childhood understands learning difficulties as a partial lag in the development of higher mental functions in children who are both students in a correctional class or an adapted educational program in a regular class, and children without a clinical diagnosis, but who experience persistent difficulties in one or more subjects. [eight]. nine0003
A teenager with ADHD can concentrate his attention for up to 10-15 minutes, then the child loses his ability to work and, in general, the ability to calmly wait for the end of a standardized lesson. With a low ability to concentrate their attention for a long time, the adolescent also has low scores on such attentional characteristics as switchability, distribution and stability. At the same time, attention is associated with cognitive and sensory processes, as well as the ability to qualitatively organize one's activities. In this regard, such a teenager shows a deficit of attention in the following types: sensory, intellectual, motor, voluntary and involuntary attention. These manifestations are a catalyst for learning difficulties. nine0003
At the same time, attention is associated with cognitive and sensory processes, as well as the ability to qualitatively organize one's activities. In this regard, such a teenager shows a deficit of attention in the following types: sensory, intellectual, motor, voluntary and involuntary attention. These manifestations are a catalyst for learning difficulties. nine0003
Due to dysfunction of the frontal lobes, it is difficult for a teenager with ADHD to follow the rules or instructions established in the group, while such a student is unable to rationally organize his activities and, as a result, is unable to work efficiently without outside help. It is generally difficult for a teenager with ADHD to engage in types of work that require prolonged mental stress or perseverance [4]. Against the background of these problems, low self-esteem is formed.
An analysis of neuropsychological studies [5;7] indicates a tendency towards increased fatigue and exhaustion of nervous processes, and insufficient control in younger adolescents with ADHD. nine0003
nine0003
General awareness and the amount of simple knowledge in such adolescents do not differ from healthy peers, in contrast to the ability to build inferences. There are also difficulties in spatial and quasi-spatial (understanding logical-grammatical structures) perception. There are low rates in visual-objective and long-term auditory-speech memory. In the field of visual-figurative thinking in children with ADHD, difficulties are noticeable in identifying the essential features of an object, in distinguishing objects within a group of the same semantic field, in updating the image by word-name and in the nominative function of speech. In voluntary movements in adolescents with ADHD, there are often violations of fine motor skills, perseveration [8]. nine0003
Among children with ADHD, there are often cases of mental retardation, which in most cases are the result of problems with attention, as well as features characteristic of ADHD: restlessness, lack of focus and impulsiveness of actions, increased excitability. As a result, ADHD is often accompanied by negative manifestations in such basic learning skills as reading, counting, writing. Thus, in younger adolescents with ADHD, there is a persistent maladaptation in schooling. nine0003
As a result, ADHD is often accompanied by negative manifestations in such basic learning skills as reading, counting, writing. Thus, in younger adolescents with ADHD, there is a persistent maladaptation in schooling. nine0003
An example of the application of the technique of neuropsychological correction of a younger adolescent with attention deficit disorder and hyperactivity
Anamnestic information: Alice M., age 11 years. The family is complete, guardian. There are two brothers: older and younger. At the time of the study, 4 people live in the family: mom, dad, younger brother (7 years old) and the girl herself. The older brother is in another city, periodically visits his family. The girl was taken under guardianship at the age of 4 years, then ADHD was diagnosed. Living conditions are good, the family has its own house. The child has a private space for sleep, play activities and activities. The level of material security of the family is above average. The psychological climate in the family is favorable. nine0003
The psychological climate in the family is favorable. nine0003
Complaints from the mother: high distractibility in the classroom, low concentration of attention, difficulties in understanding tasks in mathematics (tasks can be performed by analogy). With parental control, it makes fewer mistakes. When reading the text, he does not understand the meaning of what he read, he cannot highlight the main idea. There is a decreased sense of fear. The girl is impulsive, emotionally excitable, there are difficulties with self-control.
The study was conducted on the basis of the Psychological Center of the Pedagogical Institute of the Federal State Budgetary Educational Institution of Higher Education "Pacific State University" in Khabarovsk in three stages: nine0003
- History taking and primary neuropsychological diagnostics;
- Drawing up and carrying out corrective work based on the neuropsychological approach;
- Repeated neuropsychological diagnosis and analysis of results.

The choice of diagnostic methods was made on the basis of a battery of neuropsychological tests by A.R. Luria, which determines the accuracy of the neuropsychological study. Methods were selected taking into account age. nine0003
In the course of diagnostics, the girl showed difficulties in independently solving problems with several actions, and in general, difficulties were manifested in retaining instructions. Difficulties were also observed in understanding the hidden and figurative meaning. Were noted: emotional lability, impulsiveness in statements and actions.
The result of the primary diagnostic examination revealed moderate regulatory difficulties: serial organization, programming and control. Also, the lack of energy support for activities against the background of weakness in the processing of visual-spatial information and unexpressed manifestations of the type of verbal paraphasia. This picture was interpreted in favor of functional weakness of the reticulofrontal complex and insufficient formation of the frontal lobes, insufficient formation of the upper parietal-occipital areas of the brain, as well as functional immaturity of the right hemisphere and interhemispheric interaction. At the same time, the study showed a high level of mechanical memory, including auditory-speech and long-term, which is usually not typical for children with ADHD and, as a result, was used as a support during corrective work. nine0003
Based on the diagnostics, an individual neuropsychological correctional program was compiled based on the method of "Replacing ontogenesis" by A. V. Semenovich, as well as the methods of T. V. Akhutina, N. M. Pylaeva, aimed at the development and correction of cognitive functions, as well as those included in them components. Corrective work was carried out for 10 months 4 times a week. The duration of the lessons is 35-40 minutes. It included: motor correction; cognitive and educational. nine0003
Results
Comparison of the results of the primary and final diagnostics showed: an increase in the level of self-control; increase in volume, increase in concentration, stability, level of distribution of voluntary attention; removal of manifestations of impulsivity; development of interhemispheric interaction; development of intellectual abilities; the formation of abstract thinking, the ability to generalize and categorize.
In educational activities, the girl began to show perseverance, independence. Multi-action tasks are no longer difficult. The number of such errors in works on the Russian language has significantly decreased: repetitions and omissions of words and letters, omissions of punctuation marks, writing the beginning of a sentence with a small letter. Improved ability to understand hidden and figurative meaning. nine0003
Conclusion
As the results of the study show, the analysis of the strengths and weaknesses of the mental functions of the child allows you to create the most effective program for correcting the learning difficulties of a younger teenager with attention deficit hyperactivity disorder. This study will be of interest to defectologists, psychologists, neuropsychologists, as well as parents of children with ADHD.
Literature:
- Akhutina T. V. Neuropsychologist at school: a guide for teachers, school psychologists and parents / T.
 V. Akhutina, I. O. Kamardina, N. M. Pylaeva; T. V. Akhutina, I. O. Kamardina, N. M. Pylaeva. - Moscow: Sekachev V. Yu., 2012. - 46 p. nine0062
V. Akhutina, I. O. Kamardina, N. M. Pylaeva; T. V. Akhutina, I. O. Kamardina, N. M. Pylaeva. - Moscow: Sekachev V. Yu., 2012. - 46 p. nine0062 - Zavadenko N. N. Attention deficit hyperactivity disorder: modern principles of diagnosis and treatment / N. N. Zavadenko // Problems of modern pediatrics. - 2014. - No. 4. - S. 48–53.
- Pylaeva N. M. Neuropsychology and school / N. M. Pylaeva, T. V. Akhutina // Moscow University Bulletin. Series 14: Psychology. - 2012. - No. 2. - S. 116–122.
- Semina M. V. Problems of school education for children with attention deficit hyperactivity disorder. / M. V. Semina, A. I. Chinchikova // International scientific journal "Symbol of Science". - 2015. - No. 11. S. - 224–226. nine0062
- Tereshchenko EE Principles of correction of the cognitive sphere of younger adolescents with learning difficulties. / E. E. Tereshchenko // Psychology and pedagogy: methodology and problems of practical application. - 2012. - No.
 7. S. - 86–89.
7. S. - 86–89. - Fotekova T. A. Dynamics of higher mental functions in younger adolescence. / T. A. Fotekova, K. A. Bogomolova // Eurasian Union of Scientists. - 2020. - No. 5. P. 10–12.
- Tsvetkov AV Methods of neuropsychological correction of attention deficit hyperactivity disorder. / A. V. Tsvetkov // Moscow Psychological and Social Institute. - 2010. - No. 4. S. 33-40. nine0062
- Shumakova N. B. Peculiarities of creativity in younger adolescence. / N. B. Shumakova // Electronic journal "Psychological and pedagogical research". - 2017. - No. 4. S. 108-117.
Basic terms (automatically generated) : younger teenager, attention deficit disorder, difficulty, neuropsychological correction, teenager, child, correctional work, high level, domestic neuropsychology, figurative meaning.
Attention deficit hyperactivity disorder in children
1. Avdeenko TV. Metallol and ganandy homeostasis in children with minimal brain dysfunctions: Dis.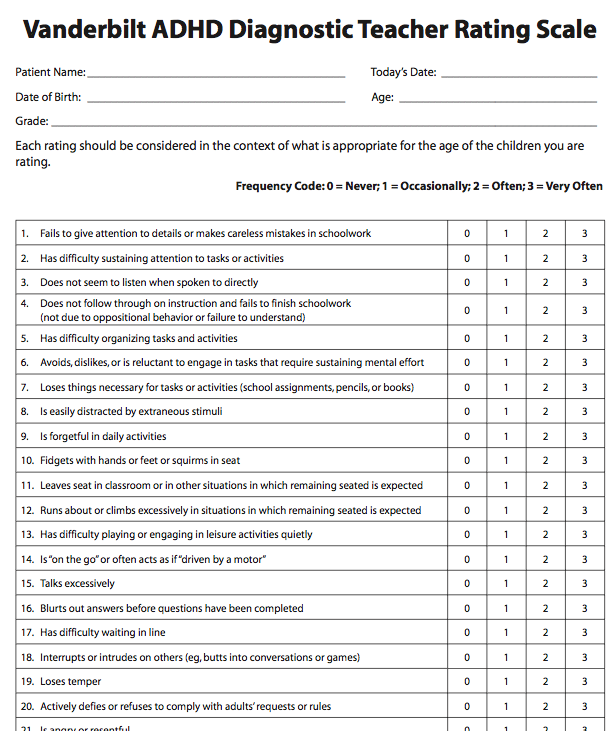 Candidate of Medical Sciences Ivanovo, 1998138 p.
Candidate of Medical Sciences Ivanovo, 1998138 p.
2. Antonov I.P., Shanko G.G. Hyperkinesis in children. Issues of etiology, pathogenesis, treatment. Minsk: Science. -1975. - P.159-160.
3. Badalyan L.O., Zavadenko H.N., Uspenskaya T.Yu. Attention deficit disorder in children. // Review of psychiatrist. and honey. psychol. them. V.M. Bekhterev. SPb., 1993. - No. 3. - P.74-90.
4. Baru A.M. Some indicators of the catecholaminergic system // Proceedings of the V All-Union Congress of neuropathologists and psychiatrists. -nineteen69.-T.1.-S. 268-288.
5. Begaidarova R.Kh., Korshunov M.F. Excretion of catecholamines in healthy children // Healthcare of Kazakhstan. 1979. - No. 5. - P.42-44.
6. Belousova E.D. The system for assessing neuropsychological and neurological disorders in children with minimal brain dysfunctions, taking into account the data of computed tomography of the brain: Dis. Candidate of Medical Sciences M., 1994. - 156 p.
7. Bolshakova T.D. Some indicators of catecholamine metabolism in physiological and pathological conditions in children: Dis. d.med.sci. M., 1973. - 466 p.
Bolshakova T.D. Some indicators of catecholamine metabolism in physiological and pathological conditions in children: Dis. d.med.sci. M., 1973. - 466 p.
8. Budantsev A.Yu. Monoaminergic systems of the brain. M: Higher school, 1976. - 187 p.
9. Glezerman T.B. Brain dysfunction in children. M.: Nauka, 1983.-97 p.
10. Gorbachevskaya N.L., Zavadenko N.N., Yakupova L.P. Electroencephalographic study of childhood hyperactivity // Human Physiology. 1996. - V.22, No. 5. - P.49-55.
11. Gorbachevskaya N.L., Yakupova L.P., Kozhushko L.F. Neurobiological causes of school maladaptation // Human Physiology. nineteen91. -T.17, No. 5. - P.72-80.
12. Gubler E.B. Computational methods for the analysis and recognition of pathological processes. L .: Medicine, 1978. - 294 p.
13. Gurevich M.L., Ozeretsky N. I. Psychomotor. M.: Medgiz, 1930. -S. 328-336.
14. Gurskaya I.K., Kuvshinnikov V.D., Igurko H.H. Daily excretion of catecholamines in healthy children // Lab. 1976. - No. 11. - P.667-669.
1976. - No. 11. - P.667-669.
15. Dadali E.L. Changes in the excretion of catecholamines in various forms and stages of muscular dystonia. The medicine. nineteen80.-#7. - P.41-45.
16. Zavadenko H.H. Clinical and psychological study of school maladaptation: its main causes and approaches to diagnosis // Neurological journal. 1998. - Volume 3, No. 6 - S. 13-17.
17. Zavadenko H.N., Petrukhin A.S., Solovyov O.I. Minimal brain dysfunction in children. Cerebrolysin in the treatment of minimal brain dysfunctions. M. EBEVE, 1997. - 73 p.
18. Ivashkin B.C. Psychological study of schoolchildren. Vladimir: VGPI, 1990. - S.22-23.
9994.-470 p.20. Kovalev VV Psychiatry of childhood. M.: Medicine, 1995. - 256 p.
21. Kolesnichenko L.S., Kul and a certain V.I., Gorina A.S. Amino acids and their metabolites in the blood and urine of children with minimal brain dysfunction II Questions org. and honey. wedge, chemistry 1999. - T.45, No. 1. -p.58-64.
22. Kornev A.N. Reading and writing disorders in children: diagnosis, correction. SPb., 1997. - 78 p.
23. Kornev A.N. On the influence of the gender factor on the prevalence and clinical symptoms of residual organic brain lesions in children // Psyche and gender in children and adolescents in normal and pathological conditions / Edited by D.N. Isaeva, 1986. P.69-73.
24. Korsakova NK, Mikadze Yu.V., Balashova Ye Yu. Underachieving children: neuropsychological diagnosis of learning difficulties in younger schoolchildren. M.: Ros.Ped.Agency, 1997. 124 p.
25. Kosheleva A.D., Alekseeva L.S. Diagnosis and correction of hyperactivity in a child. M .: Research Institute of the Family, 1997. - 62 p.
26. Kryzhanovsky G.N. General pathophysiology of the nervous system. M: Medicine, 1997. - 350 p.
27. Kulinsky V.I., Rapoport Zh.Zh. The daily rhythm of excretion of catecholamines in the urine in children is normal // Pediatrics. nineteen81. - No. 3. - P.40-43.
3. - P.40-43.
28. Kuchma V.R., Bryazgunov I.P. Attention deficit hyperactivity disorder in children (issues of epidemiology, etiology, diagnosis, treatment, prevention and prognosis). Moscow: Oleg and Pavel, 1994. -44 p.
29. Kuchma V.R., Platonova A.G. Attention deficit hyperactivity disorder in Russian children. Prevalence, risk factors and prevention. -M.: RAROG, 1997.-200 p.
30. Laakmann G., Erentraut 3. Endocrinology of psychotropic drugs // Social and Clinical Psychiatry -1998 No. 2 - S.123-152.
31. Luria AR Higher human cortical functions and their disorders in local brain lesions. M: Publishing House of Moscow State University, 1969. - 504 p.
32. Luria A.R. Fundamentals of neuropsychology. M: Enlightenment, 1973. -289 p.
33. Machinskaya R.I., Lukashevich I.P., Fishman M.N. Dynamics of the electrical activity of the brain in children aged 5-8 years in the norm and with learning difficulties I Human Physiology. 1997. - T23, No. 5. - S. 5-11.
5. - S. 5-11.
34. Menshikov VV Methods of clinical biochemistry of hormones and mediators. M: Higher school. - nineteen74. - S. 13-27.
35. Mileikovsky Yu.A. Excretion of catecholamines and tryptophan derivatives in schizophrenia. II Journal of Neurology and Psychiatry named after Korsakov. 1976. - V.76, No. 5. - S. 710-714.
36. Mosunova T.G. The exchange of catecholamines in extrapyramidal disorders in children. II Zh. Neurology and Psychiatry named after Korsakov. 1977. -T.77, No. 10.-S. 1466-1469.
37. Nebolsina L I., Petrosyan K.Yu., Markov Kh.M. Influence of emotional stress on the excretion of catecholamines in children with normal and high blood pressure // Pediatrics. nineteen82. - No. 4. -p.35-38.
38. Nemov R.C. Psychology / T.Z. M .: Education, Vlados, 1994. -S.205-245.
39. Nikonova O.E., Solovieva N.I., Vinokurova L.N. Vegetative provision of schoolchildren with different loads // Actual problems of prevention of non-communicable diseases: scientific and practical. conference, Moscow, November 15-18, 1995. M., 1995. -p.116.
conference, Moscow, November 15-18, 1995. M., 1995. -p.116.
40. Olds J. Reward neurons and brain self-stimulation // Functional significance of the electrical processes of the brain. Moscow: Higher school, 1977. - S. 329-346.
41. Osipchik SI. Clinical and biological typology of hyperactivity syndrome in children: Dis. Candidate of Medical Sciences Minsk, 1995 - 103 p.
42. Peresleni LI, Rozhkova LA Psychophysiological mechanisms of attention deficit in children of different ages with learning difficulties // Human Physiology. -1993. T. 19, No. 4. - P.5-13.
43. Platonova AG Prevalence and physiological and hygienic correction of attention deficit hyperactivity disorder in schoolchildren aged 6-8: Dis. Candidate of Medical Sciences Moscow, 1996. -144 p.
44. Psychodiagnostic complex of methods for determining the level of development of cognitive activity of younger students: teaching aid. M.: KOGITO-center, 1996. - 98 p.
45. Rogov E.I. Handbook of practical psychologist in education. M.: VLADOS, 1995. - 527p.
Handbook of practical psychologist in education. M.: VLADOS, 1995. - 527p.
46. Sidorenko EV Methods of mathematical processing in psychology. -M.: Higher School, 1996. P.59, 220-223, 316.
47. Simernitskaya E.G. Neuropsychological method of express diagnostics "Luria-90". M: Knowledge. -1991.-48 p.
48. Simernitskaya E.G., Matyugin I.Yu. Neuropsychological diagnostics and correction of school failure. M.: Knowledge, 1996.-13 p.
49. Handbook of childhood neurology. / Ed. B.V. Lebedeva. M: Medicine, 1995. - S. 193-194.
50. Structural and functional organization of the developing brain. / Ed. Farber YES and others -L .: Nauka, 1990. S.87-120.
51. Suvorinova N.Yu. Treatment of children with minimal brain dysfunctions with nootropic drugs: Dis. Candidate of Medical Sciences M., 1998.-116 p.
52. Timofeev H.N., Prokop'eva L.P. Neurochemistry of hypobiosis and the limits of cryoresistance of the body. M.: Nauka - 1997. - 87 p.
53. Trzhesoglav 3. Mild brain dysfunction in childhood. M.: Medicine, 1986. - 256 p.
Trzhesoglav 3. Mild brain dysfunction in childhood. M.: Medicine, 1986. - 256 p.
54. Troshin V.M., Radaev A.M., Khaletskaya O.V., Radaeva G.M. Clinical variants of minimal brain dysfunctions in preschool children // Pediatrics. 1994. - No. 2. - P.72-75.
55. Uzbekov M.G., Misionzhik E.Yu., Marincheva G.S., Krasov V.A. Issues of biogenic amine metabolism in children with hyperkinetic syndrome // Russian Psychiatric Journal. nineteen98. - No. 6. - S. 39-43.
56. Farber D.A., Dubrovinekaya N.V. Functional organization of the developing brain // Human Physiology. 1991. - V. 17, No. 5. -p.17-27.
57. Filimonenko Yu., Timofeev V. D. Veksler's guide to the methodology for studying intelligence in children. SPb., 1993. - 57 p.
58. Khaletskaya O.V., Troshin V.M. Minimal brain dysfunction in childhood // Journal of Neurology and Psychiatry named after Korsakov 1998. -T. 98, No. 9 - S. 4-9.
59. Khaletskaya O.V., Troshin V.M. Minimal brain dysfunction in childhood. Nizhny Novgorod, 1995. - 36 p.
Nizhny Novgorod, 1995. - 36 p.
60. Khomskaya E.D. Neuropsychology. M.: Moscow State University, 1987. - 288 p.
61. Khomulo D.P., Smorodina I.P. Catecholamines of blood and brain in conditions of emotional stress // Influence of environmental factors. Proceedings of Leningrad. sanitary and hygienic Medical Institute. - L., 1982. -t. 145. - S.77-79.
62. Tsvetkova L.S. Methods of diagnostic neuropsychological examination of children. M.: Knowledge, 1998. - 67 p.
63. Explicit anxiety scale for children 8-12 years old. // Diagnostic bank of the school psychologist. Moscow: Center for Psychological Services. Laboratory of Scientific Foundations of Child Practical Psychology. Research Institute of Psychology of the Russian Academy of Education, 1994. - Issue 9. - 22 p.
64. Yudaev AD, Titov VN. Determination of free catecholamines in urine by high-performance liquid chromatography with an electrochemical detector.// Laboratory work. 1990. - No. 3. -p. 34-38.
34-38.
65. Yasyukova L A Optimization of learning and development of children with minimal brain dysfunctions. St. Fri.: IMATON, 1997. - 78 p.
66. Albin R.L., Young A.B., Penney J.B. Basal ganglia // Trends of Neuro-sci. 1989.-Vol.12. - P. 366-375.
67. Alexander G. E., Crutcher M. D. Functional architecture of basal ganglia circuits: neural substrates of parallel processing // Trends of Neurosci. -nineteen90.-Vol.13, No.7. P. 266-271.
68. Aylward E.H., Reiss A.L., Reader M.Y., et al. Basal ganglia volumes in children with attention-deficit hyperactivity disorder il J. Child. Neurol. -1996.-Vol.11.-P. 112-115.
69. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders (DSM-II), 2th ed. Washington, DC: American Psychiatric Association; 1968.
70. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders (DSM-HI), 3th ed. Washington, DC: American Psychiatric Association; nineteen80.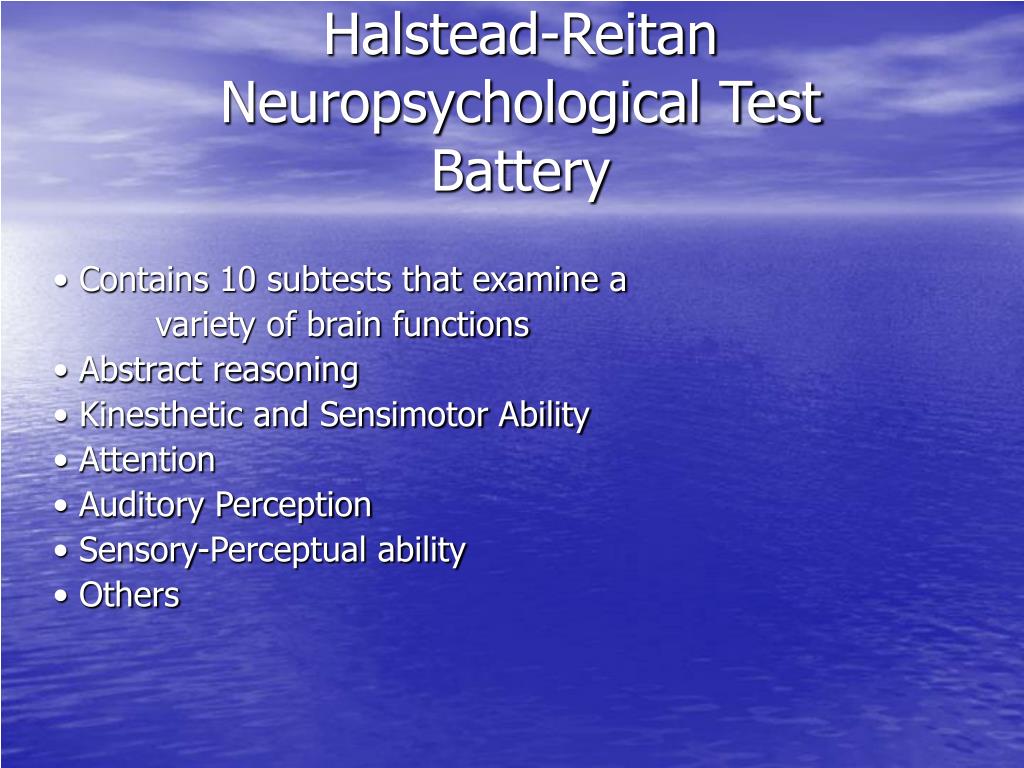
71. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), 4th ed. Washington, DC: American Psychiatric Association; 1994.
72. Anders T.F., Eiben L.A. Pediatric sleep disorders: a review of the past 10 years // J.Am.Acad.Child Adolesc.Psychiatry. 1997. - Vol. 36, no. 1. -P. 9-20.
73. Arnsten A.F.T., Steere J.C., Hunt R.D. The contribution of a2-noradrenergic mechanisms to prefrontal cortical cognitive function // Archives of Gen. Psych. nineteen96. - Vol. 53.-P.448-455.
74. August G.J., Realmuto G.M. Prevalence of attention deficit hyperactivity disorder and comorbid disorders among elementary school childrenscreened for disruptive behavior // J.Abnorm.Child Psychol. 1996.-Vol.24-P.571-595.
75. Background I. NIMH collaborative multisite multimodal treatment study of children with attention deficit hyperactivity disorder // J Am .Acad. Child Adolesc. Psychiatry. 1995. - Vol. 34, no. 8. - P. 987-997.
76. Barkley R A., Fischer M., Edelbrock C.S., Smallish L. The adolescent outcome of hyperactive children diagnosed by research criteria. I. An 8-year prospective follow-up study. J.Am.Acad. Child Adolesc. Psychiatry. -nineteen90. - Vol. 29. - P. 546-557.
Barkley R A., Fischer M., Edelbrock C.S., Smallish L. The adolescent outcome of hyperactive children diagnosed by research criteria. I. An 8-year prospective follow-up study. J.Am.Acad. Child Adolesc. Psychiatry. -nineteen90. - Vol. 29. - P. 546-557.
77. Barkley R A. Age dependent decline in attention deficit hyperactivity disorder: true recovery or statistical illusion // The ADHD Report. 1997. -№5. - P. 1-5.
78. Barkley R A. Attention Deficit Hyperactivity Disorder: a handbook for diagnostic and treatment. New York: Guilfred Press. -1990. - $688
79. Barkley R A. Behavioral ingibition, sustained attention and executive functions: constructing a unifying theory of attention deficit hyperactivity disorder // Psychopharm. Bull. nineteen97. - Vol.121, No. 1. - P.65-94.
80. Baumgaertel A., Wolraich MX., Dietrich M. Comparison of diagnostic criteria for attention deficit disorders in a German elementary school sample II J.Am.Acad.Child Adolesc.Psychiatry. 1995. - Vol.34. - P. 629-638.
1995. - Vol.34. - P. 629-638.
81. Biederman J. Attention deficit I hyperactivity disorder: A life-span perspective // J.Clin.Psychiatry. 1998. - Vol.59/suppl. - P.71-82.
82. Biederman J. Attention deficit hyperactivity disorder and juvenile mania: an overlooked comorbidity? II J.Am Acad. Child Adolesc. Psychiatry. -nineteen96.-Vol. 35, no. 8. P. 997-1008.
83. Biederman J. Is childhood oppositional defiant disorder a precursor to adolescent conduct disorder? Findings from a four-year follow-up study of children with ADHD II J Am.Acad. Child Adolesc. Psychiatry. 1996. - Vol. 35, no. 9. - P. 1193-1204.
84. Biederman J., Faraone S.V. Family genetic and psychosocial risk factors in DSM-III attention deficit disorder” // J .Am.Acad. Child Adolesc. Psychiatry. 1990.-Vol. 29. - P. 526-533.
85. Biederman J., Faraone S.V., Milberger S., et al. A prospective four-year follow-up study of attention deficit hyperactivity and related disorders // Arch.Gen. Psychiatry. nineteen96. - Vol.53. - P.437-446.
Psychiatry. nineteen96. - Vol.53. - P.437-446.
86. Biederman J., Faraone S.V., Spencer T., et al. Gender differences in a sample of adults with attention deficit hyperactivity disorder // Psychiatry Res. 1994.-Vol. 53.-P. 13-29.
87. Biederman J., Mick E., Faraone S.V. Depression in attention deficit hyperactivity disorder children: "True" depression or demoralization? // J. of Affective Disorders 1998-Vol.47-P.113-122.
88. Biederman J., Spencer T. Attention-deficit/hyperactivity disorder as a noradrenergic disorder // Biol. Psychiatry 1999. - Vol.46, No. 9. - P. 12341242.
89. Campbell L.R., Cohen M. J. Management of attention deficit hyperactivity disorder. A continuing dilemma for physicians and educators // Clin.Pediatrics. 1990.-Vol.29, No.3. - P. 191-193
90. Cantwell D P. Attention deficit disorder in adolescent // Clinical Psychology Review.-1986.-Vol.6.-P.237-247.
91. Cantwell D P. Attention deficit disorder: a review of the past 10 years // J . Am.Acad. Child Adolesc. Psychiatry. 1996. - Vol. 35, no. 8. - P. 978987.
Am.Acad. Child Adolesc. Psychiatry. 1996. - Vol. 35, no. 8. - P. 978987.
92. Cardon L.R. Quantative trait locus for reading disability // Science. -1994. Vol. 266. - P. 276-279.
93. Castellanos F X. Toward a pathophysiology of attention deficit/hyperactivity disorder // Clinical Pediatrics. -1997. Vol.36, No.7. - P.381-393.
94. Castellanos F X., Elia J., Kruesi M. J. P., et al. Cerebrospinal homova-nilic acid predicts behavioral response to stumulants in 45 boys with attention deficit hyperactivity disorder // Neuropsychopharmacology. nineteen96.-Vol.14.-P. 125-137.
95. Castellanos F X., Giedd J.N., Marsh W.L. Quantative brain magnetic resonance imaging in attention deficit/hyperactivity disorder // Arch. Gen. Psychiatry. 1996. - Vol.53. - P.607-616.
96. Castellanos F. X., Lau E., Tayebi N. Lack of an association between a dopamine-4 receptor polymorphism and attention-deficit/hyperactivity disorder: genetic and brain morphometric analyses. // Mol Psychiatry. -1998.-Vol. 3, #5. P. 431-434.
-1998.-Vol. 3, #5. P. 431-434.
97. Chase T.N. Biochemical and pharmacological studies of dystonia // Neurology. nineteen70.-Vol.20. - P.122-130.
98. Cohen P., Cohen J., Kasen S., et al. An epidemiological study of disorders in late childhood and adolescence. I. Age- and gender-specific prevalence // J.Child Psychol.Psychiatry. 1993. - Vol.34. - P.851-867.
99. Conners C.K. Rating scales for use in drug studies with children // Psychopharm. Bull, (special edition). 1973. - Vol. 97. - P. 24-84.
100. Cook E.H., Stein M. A., Krasowski M. D. Association of attention deficit disorder and dopamine transporter gene // Am.J.Human Genetics. nineteen95.-Vol.56, No.4. - P.993-998.
101. Corkum P., Tannock R., Moldofsky H. Sleep disturbances in children with attention deficit / hyperactivity disorder // J .Am.Acad. Child Ado-lesc.Psychiatry. 1998. - Vol. 37, no.6. - P.637-646.
102. Delong M.R. Primate models of movement disorders of basal ganglia origin // Trends of Neurosciences 1990. - Vol. 13, no. 7. - P. 281-285.
- Vol. 13, no. 7. - P. 281-285.
103. Denckla M. Revised neurological examination for subtle signs // Psychopharm. Bull. -1985.-Vol. 21. P. 773-789.
104. Denckla MB. A theory and model of executive function. A neuropsychological perspective. In: Lyon G.R. Attention, memory and executive function. Baltimore: Paul H., 1996. - P.263-278.
105. Dienstbier RA. Arousal and physiological toughness: implications for mental and physical health II Psychol. Rev. 1989. - Vol. 96.-P.84-100.
106. Diller H.D. Etiology of attention deficit hyperactivity disorder: nature or nurture? // Am. J. of Psychiatry. 1996.-Vol. 153, no. 3. - P. 451-452. nine0003
107. Douglas V.l. Attentional and cognitive problems. // In developmental neuropsychiatry / M.Rutter, 1983. P.280-329.
108. Elia J., Ambrosini P.J., Rapoport J.L. Treatment of attention deficit hyperactivity disorder // New England J. Medicine. 1999. - Vol. 340, no. 10. - P. 780-788.
109. Faraone S. V., Biederman J. Attention deficit hyperactivity disorder with bipolar disorder: a familial subtype? // J.AmAcad. Child Ado-lesc.Psychiatry. 1997. - Vol. 36, no. 10. - P. 1378-1387. nine0003
V., Biederman J. Attention deficit hyperactivity disorder with bipolar disorder: a familial subtype? // J.AmAcad. Child Ado-lesc.Psychiatry. 1997. - Vol. 36, no. 10. - P. 1378-1387. nine0003
110. Faraone S.V., Biederman J. Is comorbidity with attention deficit hyperactivity disorder a marker for juvenile-onset mania? // J.Am.Acad. Child Adolesc. Psychiatry. 1997.-Vol. 36, no. 8. - P. 1046-1055.
111. Faraone S.V., Biederman J. Neurobiology of attention-deficit hyperactivity disorder // Biol. Psychiatry. 1998. - Vol. 44, no. 10. - P. 951-958.
112. Feingold B.F. Hyperkinesis and learning disabilities linked to artificial food flavors and colors//Am.J.Nurs. nineteen75b. - Vol. 65.-P.793-803.
113. Food man A. Attention deficit disorder and soft signs letter. // J.Am.Acad.Child Adolesc. Psychiatry. 1996. - Vol. 35, no. 7. - P. 841-842
114. Gallicci F. Symptoms of attention deficit hyperactivity disorder in an Italian school sample: findings of a pilot study // J. Am.Acad. Child Adolesc. Psychiatry. 1993.-Vol. 32, no. 5. - P. 1051-1058.
Am.Acad. Child Adolesc. Psychiatry. 1993.-Vol. 32, no. 5. - P. 1051-1058.
115. Gaub M., Carlson C.L. Gender differences in attention deficit hyperactivity disorder: a meta-analysis and critical review // J .Am Acad.Child Adolesc.Psychiatry. nineteen97. - Vol. 36, no. 8. - P. 1036-1045.
116. Gill M., Daly G., et al. Confirmation of association between attention deficit hyperactivity disorder and a dopamine transporter polymorphism. // Mol. Psychiatry. 1997. - Vol 2, No. 4. - P. 464-468.
117. Gittelman R. Diagnosing attention deficit hyperactivity disorder in adolescents. // Psychopharm. BuiI.-1985.-Vol.21. -P. 237-242.
118. Gjone H. Genetic influence on parent-reported attention related problems in a Norwegian general population twin sample // J Am.Acad. Child Adolesc. Psychiatry. nineteen96. - Vol.35, No. 5. - P. 588-596.
119. Goyette C., Conners C.K., Ulrich R. Normative data on the Revised Conners Parent and Teacher Rating Scales // J. Abnorm. child psychology. -1978.-Vol. 6.-P. 221-236.
child psychology. -1978.-Vol. 6.-P. 221-236.
120. Gray J.A. The neuropsychology of anxiety: an enquiry into the functions of the septo-hippocampal system // New York: Oxford University Press, 1982-P. 34-45.
121. Greenhill L., Puig-Antich J., Goetz R., et al. Sleep architecture and REM sleep measures in prepubertal children with attention deficit disorder with hyperactivity // Sleep. nineteen83.-Vol. 6. - P. 91-101.
122. Halperin J.M., Newcorn J H., Koda V.H., McCay K.E. Noradrenergic mechanisms in attention deficit hyperactivity disorder children with and without reading disabilities: a replication and extension. // J.Am. Acad. -1997. -Vol. 36, no. 12. P. 1688-1697.
123. Hanna G.L., Ornitz M., Hariharan M. Urinary epinephrine excretion during intelligence testing in attention deficit hyperactivity disorder and normal boys // Biol. Psychiatry. -1996. Vol. 40. - P. 553-555
124. Hart E.L., Lahey B.B., Loeber R. Developmental change in attention deficit hyperactivity disorder in boys: a four year longitudinal study // J. Abnorm.Child Psychol. 1995.-Vol.23. - P.729-749.
Abnorm.Child Psychol. 1995.-Vol.23. - P.729-749.
125. Hoffman H. Der Struwwelpeter: Older lustige Geschichten und drollige Bilder. Leizig: Insel Verlag. 1845.
126. Howell D C., Huessy H R, Hassuk B. Fifteen-year follow-up of a behavioral history of attention deficit disorder // Pediatrics. 1985. - Vol. 76, no. 2. - P. 185-190.
127. Hynd G.W., Hern K.L, Novey ES, et al. Attention deficit hyperactivity disorder and asymmetry of the caudate nucleus // J. Child. Neurol. 1993.-Vol.8. - P. 339-347.
128. Jacobvitz D. Treatment of attentional and hyperactivity problems in children with sympathonmimetic drugs: a comprehensive review // J.Am.Acad.Child Adolesc.Psychiatry. 1990. - Vol. 29, no. 5. - P. 677-688
129. Kahn C A. Lead screening in children with attention deficit hyperactivity disorder and developmental delay I! Clinical Pediatrics. nineteen95. - Vol. 34, No. 9. - P. 498-501.
130. Kelly D P., Aylward G.P. Attention deficits in school-aged children and adolescents // Pediatrics Clinics of North America. 1992. - Vol. 39, no. 3. -P. 487-513.
1992. - Vol. 39, no. 3. -P. 487-513.
131. LaHoste G.J, Swanson J.M, Wigal S.B., et.al. Dopamine D4 receptor gene polymorphism is associated with attention deficit hyperactivity disorder // Mol. Psychiatry. 1996. - Vol.1. - P.121-124.
132. Levy F. The dopamine theory of attention deficit hyperactivity disorder // Auct. N.-Z. J. Psychiatry. nineteen91.-Vol. 25. - P. 277-283.
133. Licinio J. The dopamine D4 receptor and attention deficit hyperactivity disorder // Mol. Psychiatry. 1996. - Vol. 1. - P. 83-84.
134. Maher B.S., Marazita M.L, Moss H.B., Vanyukov M M. Segregation analysis of attention deficit hyperactivity disorder // Am. J. Med. Genet. -1999. -Vol. 88, no. 1. P. 71-78.
135. Mannuzza S., Klein R.G. Educational and occupational outcome of hyperactive boys grown up // J .Am.Acad. Child Adolesc. Psychiatry. -nineteen97 Vol. 36, No. 9. - P. 1222-1227.
136. Mannuzza S., Klein R.G., Bessler A. Adult psychiatric status of hyperactive boys grown up // Am.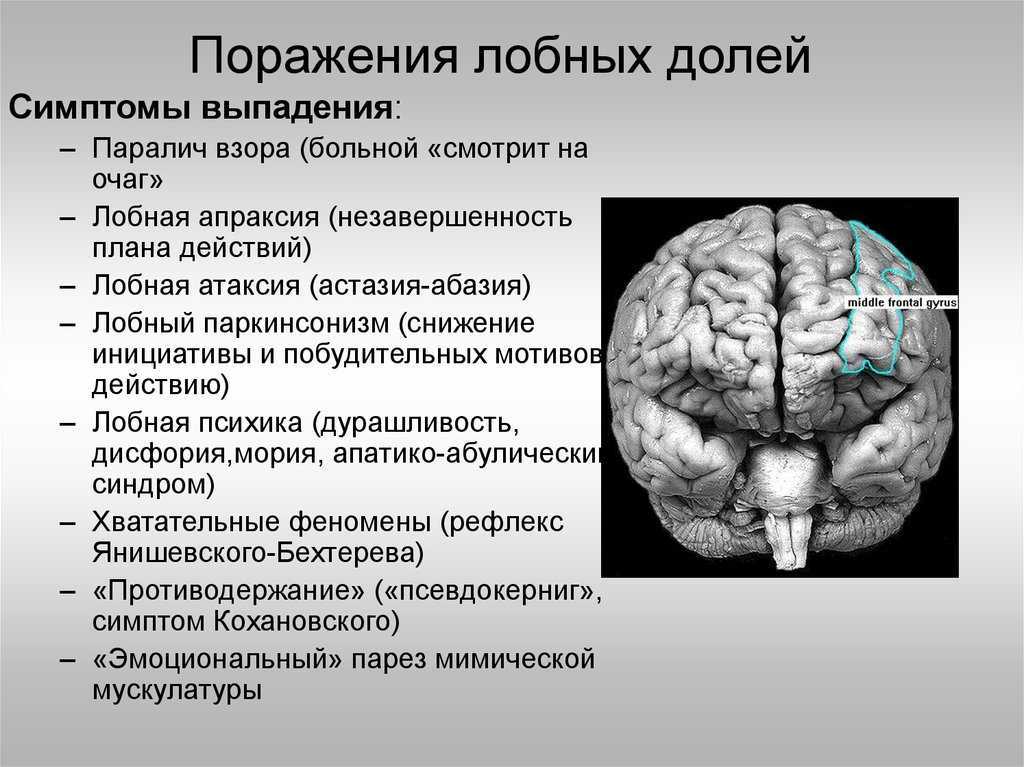 J. Psychiatry. 1998. - Vol. 155, no. 4. -P.493-498.
J. Psychiatry. 1998. - Vol. 155, no. 4. -P.493-498.
137. McConaughy S.H., Achenbach T.M. Comorbidity of empirically based syndromes in matched general population and clinic samples // J. Child Psychol. Psychiatry. 1994.-Vol. 35. - P. 1141-1157.
138. McCracken J.T. A two-part model of stimulant action on attention deficit hyperactivity disorder in children // J.Neuropsychiatry Clin. neurosci. -nineteen91.-Vol. 3.-P. 201-209.
139. Mefford I.N., Potter W.Z. A neuroanatomical and beochemical basis of attention deficit hyperactivity disorder in children: a defect in tonic adrenaline mediated inhibition of locus coeruleus stimulation. // Med. Hypotheses 1989. - Vol. 29 - P.33-42.
140. Milberger S., Biederman J., Faraone S.V. Attention deficit hyperactivity disorder is associated with early initiation of cigarette smoking in children and adolescents II J .Am.Acad. Child Adolesc. Psychiatry. nineteen97. - Vol. 36, no. 1. - P. 37-44.
141. Moskowitz M. A., Wurtman R.J. Catecholamines and neurological diseases II New England J. Medicine. 1975. - Vol. 293. - P. 274-280.
A., Wurtman R.J. Catecholamines and neurological diseases II New England J. Medicine. 1975. - Vol. 293. - P. 274-280.
142. Oades R.D., Daniels R., Rascher W. Plasma neuropeptide-Y levels, monoamine metabolism, electrolyte excretion and drinking behavior in children with attention-deficit hyperactivity disorder // Psychiatry Res. -1998. -Vol. 80, #2. P. 177-186.
143. O'Callaghan M.J., Harvey J.M. Biological predictors and co-morbidity of attention deficit hyperactivity disorder in extremely low birth weight infants at school // J.Paediatr.Child Health. nineteen97. Vol. 33, no. 6. - P. 491-496.
144. Oesterheld J.R., Wilson A. Attention deficit hyperactivity disorder and fetal alcohol syndrome // J.Am.Acad. Child Adolesc. Psychiatry. 1997. -Vol.36, No.9.-P.1163-1165.
145. Ornitz E.M., Gabikian P., Rüssel A.T. Affective valence and arousal in attention deficit hyperactivity disorder and normal boys during a startle habituation experiment // J.Am.Acad.Child Adolesc. Psychiatry. 1997-Vol. 36, no. 12. - P. 1698-1705.
Psychiatry. 1997-Vol. 36, no. 12. - P. 1698-1705.
146. Pliszka S R., Maas J.W. Urinary catecholamines in attention deficit hyperactivity disorder with and without comorbid anxiety. // J.Am.Acad. Child Adolesc. Psychiatry. nineteen94.-Vol. 33. - P. 1165-1173.
147. Pliszka S R., Maas J.W., McCracken J.T. Catecholamins in attention deficit hyperactivity disorder: current perspectives II J .Am .Acad. Child Adolesc. Psychiatry. 1996. - Vol. 35, no. 3. - P. 264-272.
148. Pliszka S R., Maas J.W., McCracken J.T. Catecholamins in attention deficit hyperactivity disorder; current perspectives. // J.Am.Acad. Child Adolesc. Psychiatry. 1996. Vol. 35, no. 3. - P. 264-272.
149. Posner M., Petersen S.E. The attention system of the brain // Annu. Rev. neurosci. nineteen90. - Vol. 13.-P.25-42.
150. Ramos Piaton M.J., Velo Buena A., Espinar Sierra J., et al. Hypnopoly-graphic alterations in attention deficit disorder children // Int. J. Neurosci. -1990. Vol. 53. - P. 87-101.
- P. 87-101.
151. Rapoport J.L., Mikkelsen E.J., Ebert M.H., et al. Urinary catecholamine and amphetamine excretion in hyperactive and normal boys // J. Nerv. Ment. Dis. 1978. - Vol.66. - P. 731-737.
152. Reid J.L., Kopin I.J. Significance of plasma dopamine-beta-hydroxylase as an index of sympathetic neuronal function // Proc. Nat. Acad. Sei. USA. nineteen74. - Vol.71. - P.4392-4394.
153. Richters J E., Arnold L. E., Jengen P. S. NIMH collaborative multisite multimodal treatment study of children with attention deficit hyperactivity disorder // J.Am.Acad.Child Adolesc.Psychiatry. 1995. - Vol.34, No. 8. - P. 987-1000.
154. Rowe DC, Stever C, Giedinghagen LN, et al. Dopamine DRD4 receptor polymorphism and attention deficit hyperactivity disorder // Mol. Psychiatry. -1998.-Vol. 3, #5. P. 419-426.
155. Rutter M L., et al. A guide to multiaxial classification scheme for psychiatric disorders in childhood and adolescence // London Institute of Psychiatry. -nineteen79.387 p.
-nineteen79.387 p.
156. Sandber S. Hyperkinetic or attention deficit disorder // British J. Psychiatry. 1996.-Vol.169, No.7. - P.10-17.
157. Satterfield J.H., Hoppe C.M., Schell A.M. The Satterfield Teacher Rating Scale //Am. J. Psychiatry. 1982. - Vol. 139, no.6. - P.795-798.
158. Satterfield J H., Schell A. A prospective study of hyperactive boys with conduct problems and normal boys: adolescent and adult criminality // J.Am.Acad. Child Adolesc. Psychiatry. 1997. - Vol. 36, no. 12. - P. 17261735.
159. Shaywitz B.A, Fletcher J.M, Shaywitz S.E. Attention-deficiency/hyperactivity disorder//Adv. Pediatr. 1997. - Vol. 44. - P. 331-367.
160. Spencer T.J., Biederman J. Pharmacotherapy of attention deficit hyperactivity disorder across the life cycle // J.Am.Acad. Child Ado-lesc.Psychiatry. 1996. Vol. 35, no. 4. - P. 409-432
161. Strayhorn J.M., Weidman C.S. Reduction of attention deficit and internalizing symptoms in preschoolers through parent-child interaction training // J. Am.Acad. Child Adolesc. Psychiatry. nineteen89.-Vol. 28, no. 6. - P. 888896.
Am.Acad. Child Adolesc. Psychiatry. nineteen89.-Vol. 28, no. 6. - P. 888896.
162. Szatmari P. The epidemiology of attention-deficit hyperactivity disorders. In G. Weiss (Ed.), Child and adolescent psychiatry clinics of North America: Attention deficit disorder (pp. 361-372). Philadelphia: W.B. Saunders - 1992.
163. Szatmari P., Boyle M., Offord D R. Attention deficit hyperactivity and conduct disorder: degree of diagnostic overlap and differences among correlates. // J.Am.Acad. Child Adolesc. Psychiatry. 1989. - Vol. 28. - P. 865-872. nine0003
164. Tao K-T. Hyperactivity and attention deficit disorder syndromes in China // J .Am.Acad. Child Adolesc. Psychiatry. 1992. - Vol.31. - P. 1165-1166.
165. Taylor E.A., Sandberg S., Thorley G., Giles S. The epidemiology of childhood hyperactivity. Maudsley monographs no.33. Oxford, England: Oxford University Press, 1991 P. 93-113.
166. Tennes K., Kreye M. Behavioral correlates of excreted catecholamines and Cortisol in second-grade children // J. Am.Acad. Child Adolesc. Psychiatry. nineteen86.-Vol.25, No.6. - P.764-770.
Am.Acad. Child Adolesc. Psychiatry. nineteen86.-Vol.25, No.6. - P.764-770.
167. Thapar A. Attention deficit hyperactivity disorder: unraveling the molecular genetics // Mol. Psychiatry. 1998. - Vol. 3. - P. 370-372.
168. Trommer B.L., Hoeppner J B., Rosenberg R.S., et al. Sleep disturbance in children with attention deficit disorder // Ann. Neurol. 1988. - Vol. 24. - P. 322.
169. Tryphonas H. Factors possibly implicated in hyperactivity // Hyperactivity in children: etiology, measurement and treatment implications. Baltimore 1979. P. 93-102.
170. Warren R.P. Reading disability, attention deficit hyperactivity disorder and the immune system. // Science. -1995. Vol. 268.-P. 786-787.
171. Wender E.H., Solanto M.V. Effects of sugar on aggressive and inattentive behavior in children with and normal children // Pediatrics. 1991.-Vol. 88.-P.960-966.
172. Wilson J.M. Psychosocial adjustment and educational outcome in adolescents with a childhood diagnosis of attention deficit disorder // J.![]() Am.Acad. Child Adolesc. Psychiatry. nineteen96. - Vol. 35, No. 5. - P. 579587.
Am.Acad. Child Adolesc. Psychiatry. nineteen96. - Vol. 35, No. 5. - P. 579587.
173. Wolraich M.L. Influence sugar on child's behavior // Medical market. -1997.-Vol.25.-P.14.
174. Wolraich M.L., Baumgaertel A. The practical aspects of diagnosing and managing children with attention deficit hyperactivity disorder // Clinical Pediatrics. 1997. - Vol.36, No. 9. - P.497-504.
175. Woolf A.D. Adolescence and its discontens: attentional disorders among teenagers and young adults it Pediatrician. 1986. - Vol.13. - P. 119-127.
176. World Health Organization. The Tenth Revision of the International Classification of Diseases and Related Health Problems. Geneva, 1992.150
177. Zametkin A.J., Rapoport J.L. Neurobiology of attention deficit hyperactivity disorder: where have we come in 50 years? // J.Am.Acad.Child Adolesc. Psychiatry. 1987. - Vol. 26.-P.676-687.
178. Medical Academy. I. M. Sechenova QUESTIONNAIRE FOR PARENTS
179. Name of the child age school (daycare center)
180. Think about your child before he or she came to school. What he was like at the age of 6-7 years, and what he has become over the past six months. Did
Think about your child before he or she came to school. What he was like at the age of 6-7 years, and what he has become over the past six months. Did
181. Have any of the following features observed in your child?
182. When answering the questions, please circle the appropriate number).
183. Behavioral features of a child under 7 years of age for the last six months
184. Fussy movements of arms and legs, or squirming while sitting on a chair (adolescents may have a subjective feeling of impatience). 1-yes, 0-no 1-yes, 0-no
185. Remains in a chair with difficulty when performing any tasks. 1-yes 0 no 1-yes, 0-no
186. Z. Easily distracted by extraneous stimuli. 1-yes, 0-no 1-yes, 0-no
187. Has difficulty waiting in line to join the game. 1-yes, 0-no 1-yes, 0-no
188. Answers questions without thinking and before the question is finished. 1-yes, 0-no 1-yes, 0-no
189. Has difficulty following instructions from others. 1-yes, 0-no 1-yes, 0-no
1-yes, 0-no 1-yes, 0-no
190. With difficulty keeps attention when performing tasks or in game situations. 1-yes, 0-no 1-yes, 0-no
191. Often switches from one unfinished business to another. 1-yes, 0-no 1-yes, 0-no
192. Restless during play. 1-yes, 0-no 1-yes, 0-no
193. Y. Often overly talkative. 1-yes, 0-no 1-yes, 0-no11. In a conversation, he often interrupts, imposes his opinion, in games he is often a "target". 1-yes, 0-no 1-yes, 0-no
194. Often the chr does not seem to hear what is said to HIM or HER. 1-yes, 0-no 1-yes, 0-no
195. Often loses items and things necessary for work at home or in the classroom (toys, pencils, books, etc.) 1-yes, 0-no 1- yes, 0-no
196. Ignores physical danger and possible consequences (eg, running down the street without looking back). 1-yes, 0-no 1-yes, 0-no
197. Information will not be disclosed.
198. Medical Academy. IM Sechenova QUESTIONNAIRE for the teacher's assessment of the characteristics of the child's behavior at school school class
199.