Adhd and impulse control disorder
Here’s What ADHD Impulsivity Is Like
Everyone has a story about That Kid in School from their childhood, right?
Whether it was eating paste, arguing with the teacher, or some manner of a Lovecraftian bathroom nightmare scenario, That Kid in School had scene-stealing outbursts on lock. Sometimes, we all wonder what happened to them, what they’re doing now.
Unless, like me, *you* were That Kid in School because you had impulse control issues from untreated ADHD.
Impulsivity, in the clinical sense, can be neatly defined as “action without foresight.”
I would speak without raising my hand, interrupt the class with emotional outbursts, and get out of my desk so often I’m surprised the use of duct tape was never bandied around the teacher’s lounge.
I would get asked why I was doing any of it and I never had a clear answer — even to myself. I didn’t like drawing that bad sort of attention to myself. It was humiliating.
It’s funny how often suffering in children gets them labelled as merely troublemakers. Part of this is shame-based masking in kids because they’ll do anything to deny they’re different, and part of it is how our school systems aren’t adequately equipped to recognize or act on these circumstances that are ultimately health issues.
But this is a column on ADHD and not on how we’re systemically failing our young people, so let’s keep it pushing!
Let’s go ahead and do our inventory of “jerk-type” behavior.
I was an impulsive child and I am a slightly less impulsive adult. We all have our moments of it, but for me it can feel like a dozen controllers are all in charge of my brain at once and nobody is checking in with each other before they’re pushing buttons.
Especially in stressful conditions, I find I tend to move first and then process and deal with my actions second.
It’s not the most efficient or effective process!
I’m not going to lie, impulse control is one of the trickiest parts of ADHD. Even the first step of admitting we’re someone who flies off the handle is tricky because it’s a real struggle session of the ego.
Fortunately, we’ve got a checklist for that — do you do any of the following?
- Interrupt conversations (even when you have nothing of substance to add). Why is it hard to not just shut up and let someone have a word in edgewise?
- Have distractions for your distractions? Often, the most straight-forward tasks can become arduous because the impulsive brain shifts our perception of priority like a spinning slot machine. You never know where your attention span is gonna land!
- Spend like you make money moves even when you’re broke as hell? We all know about those juicy brain chemicals that get released with the instant gratification of impulsive purchasing, and those with ADHD often find themselves in the trickiest of rabbit holes regarding what is a want and what is a need. I’ve even caught myself trying to justify buying ADHD management tools like planners and calendars and then realized the ones I have work fine.
 Late stage capitalism, baby!
Late stage capitalism, baby! - Find it hard to resist risky, self-destructive behavior like fighting or unsafe sex? I have a guy in my contacts that has about eight different emojis that all convey “DANGER! DO NOT TEXT HIM!” Anyone else?
- Want to Hulk out at the very thought of standing in a line that takes more than 5 minutes? It’s not (necessarily) that we feel our time is worth more than others, sometimes just the challenge of remaining relatively still and not fidgeting makes standing in a line for a long time positively exhausting! Too bad it’s one of those “part of being in society” things?
If any or all of these resonate, your impatient ass might need some professional intervention to deal with this symptom of ADHD.
So what can we do about it?
Some of us treat our ADHD with medications, but the jury still seems to be out on how effective they are alone for this issue in particular.
Therapy, like cognitive behavioral therapy, may be useful if you’re going proactive on impulsivity issues.
Active mindfulness is like working out a muscle. You might start working out after a scenario of feeling particularly weak, and progress might feel impossibly slow at the start. Just like with getting physically active, I want to remind you to literally be patient with yourself as you try to be patient with others.
The more you flex that self-restraint and compassion, the easier it will come to you. And the better your results will be long-term!
Now if you’ll excuse me, this former Weird Kid in School is going to resist the impulse to look up Natalie from sixth grade who TOTALLY framed me for the bathroom horror story. That was your IBS, Natalie, YOUR IBS!
Reed Brice is a writer and comedian based in Los Angeles. Brice is an alum of UC Irvine’s Claire Trevor School of the Arts and was the first transgender person to ever be cast in a professional revue with The Second City. When not talking the tea of mental illness, Brice also pens our love & sex column, “U Up?”
5 Tips to Tame Impulsive Behavior
We include products we think are useful for our readers. If you buy through links on this page, we may earn a small commission Here’s our process.
If you buy through links on this page, we may earn a small commission Here’s our process.
Psych Central only shows you brands and products that we stand behind.
Our team thoroughly researches and evaluates the recommendations we make on our site. To establish that the product manufacturers addressed safety and efficacy standards, we:
- Evaluate ingredients and composition: Do they have the potential to cause harm?
- Fact-check all health claims: Do they align with the current body of scientific evidence?
- Assess the brand: Does it operate with integrity and adhere to industry best practices?
We do the research so you can find trusted products for your health and wellness.
Read more about our vetting process.If you have difficulty paying attention, often feel restless, and give in to urges easily, you may be living with the hyperactive-impulsive presentation of ADHD.
Managing impulsivity is possible, even if it might feel really challenging at times.
The first step to control your impulses is to seek the support of a mental health professional who can help you create and maintain a treatment plan for adult attention deficit hyperactivity disorder (ADHD).
But there’s a lot you can also do on your own to manage and improve impulse control. By being an active player in your treatment, you can further improve your quality of life.
What does impulsive behavior look like in ADHD?
Every adult is unique, so it depends on your personality and circumstances.
In general, impulsive behavior often looks like an improvised or unpredicted course of action that’s not based on logic. It’s your emotions driving your behavior.
These impulsive actions may sometimes go against your own plans and habits, and on some occasions, they might become harmful to you or others.
Examples of impulsive behavior include:
- Constantly interrupting conversations or say things you later regret.
- Hopping from one activity to the next one or try to handle three simultaneously.
- Go shopping for one item and return home with endless bags.
- While driving, you get impatient and begin cutting in front of everyone.
- Go out to have one drink and end up coming home with someone you don’t know.
Most people act impulsively from time to time. The difference is that ADHD — particularly the hyperactive-impulsive subtype — affects impulse control to the point that these behaviors become persistent over time and across situations.
The following impulse control techniques may help.
How does your impulsivity manifest? What are the common negative consequences? When and where are you the most impulsive?
“No two ADHD adults look the same,” says Terry Matlen, ACSW, a psychotherapist and author of “Survival Tips for Women with AD/HD.” “That’s why it’s vital to understand how your particular ‘flavor’ of ADHD affects your life.”
To become aware and identify the particulars of impulse control challenges, you can begin by taking notes and keeping an inventory.
Eventually, you’ll find a system that works best for you. To start, you could:
- list recent behaviors that you consider impulsive
- list recent behaviors that other people consider impulsive in you
- identify negative consequences of recent impulsive behaviors
- identify positive consequences of recent impulsive behaviors
- pinpoint the places where you most often become impulsive
- select some impulsive behaviors that might be the most harmful to you or others
Matlen also suggests reading about ADHD in adults and attending support groups and conferences that can provide further resources.
To control your impulses, you can sharpen your self-awareness by practicing mindfulness.
“[B]ring attention to the present moment and observe what is happening without judging it,” says Lidia Zylowska, MD, a board-certified psychiatrist who specializes in adult ADHD and penned the book “The Mindfulness Prescription for Adult ADHD. ”
”
For instance, focus on your thoughts, emotions, and urges along with how your body feels when you’re about to be impulsive, says Zylowska.
This may not be easy at first. You might pick up on your impulsivity only after being impulsive. But with practice, you can start identifying what precipitates your impulsive behavior.
Mindfulness may also help you gain some distance from your urges. This way, you aren’t driven by your impulses but simply observing them. Then, you can decide on your actions, adds Zylowska.
Here’s how it could work:
- Practice how to recognize an urge before you act impulsively.
- Put a name on that urge. For example, “This is anger I feel.”
- Identify the action that emotion is leading you to. For example, “I want to criticize my spouse (because I’m angry).”
- Identify what you need to do to stop the impulsive behavior. For example, “I need to express my frustration without making it personal.” Or, “I need to step away, take a moment, and come back later.
 ”
” - Approach the situation once your urge has decreased.
- Document your emotion, what you felt like doing, and what you ended up doing.
Use a supportive, compassionate, and encouraging voice, says Zylowska. For instance, if you want to manage your impatience, you might say: “Waiting is hard for you, but see if you can be a bit more patient right now.”
Checking in refers to taking inventory of how you feel and what your predominant thoughts are right before acting impulsively.
The goal is to pinpoint the inner dialogue underlying your impulsive behaviors. Once you do, you can challenge them.
For instance, let’s say you had to complete a job task but ended up browsing Facebook for an hour.
Carol Perlman, PhD, a psychologist who developed a cognitive behavioral therapy for adult ADHD, suggests asking yourself a series of questions.
For example:
- What was going on when you started the task?
- Did it feel doable?
- Was it interesting?
- Was any resistance in you regarding the task itself?
Maybe you started looking at Facebook because the thought of sitting at your desk for two hours straight seemed utterly unbearable, she says.
Once you’ve identified the challenges or emotions underlying your impulses, you can implement correctives.
There are many ways you can go about this. Here are some examples Perlman, also co-author of the therapist guide and workbook “Mastering Your Adult ADHD,” suggests:
- Break out your tasks into bite-sized steps. For example, work on your task for 30 minutes and then take a five-minute break in a different environment.
- When taking a break, plan for short and relaxing activities. Also, set up an alarm. If you stay on break too long, you may get distracted and move to other tasks.
- Keep asking questions about the task you’re having difficulty completing. For example, “How bad can this really be?” or “Can I coach myself through the less enjoyable parts?” or “How good will it feel once I finish?”
Once you improve your self-awareness and mindfulness, you’ll be able to know where and when you typically act impulsively. The following step is to sabotage those instances, says Matlen.
For example, if you usually overspend when you go out shopping, leave your credit card and checkbook at home. Take cash instead, and take only what you need to purchase what you’ll be shopping for.
If you need to curb impulsive speech, Perlman suggests taking a notepad with you to important meetings. Instead of blurting out your comments, jot them down as soon as they come to you. Read them later and mention them at the appropriate time.
To plan for this, go back to your initial list. Next to the impulsive behaviors you have identified, write the possible impulse control solutions.
Sometimes ADHD impulsivity might be the result of being stressed or on edge, says Perlman.
Relaxing can increase your impulse control.
Perlman suggests the following:
- Practice guided imagery.
- Listen to calming music at all times, particularly when you need to get busy.
- Implement deep breathing techniques throughout your day.
- Exercise as often as possible.
- Learn progressive muscle relaxation.
Managing ADHD impulsivity might be challenging at times, but it’s possible.
Self-awareness is the first step to impulse control, besides seeking the guidance of a mental health professional.
You can begin taming your impulsive behaviors by checking in with yourself, making it more difficult to act on impulse, and improving your mental and physical relaxation.
Publications for the keyword "impulsivity"
Medicine
Publication date: 06/14/2019
Rate the material Average rating: 5 (Total: 1)
Dubatova Iandovna 5 honey. Sciences, Associate ProfessorRostov State Medical University of the Ministry of Health of Russia , Rostov Region
Antsyborov Andrey Viktorovich , chief physician, psychiatrist, addictive medicine specialist, psychotherapist
LLC KMZ "Psyche" Rostov region
"The role of impulsivity and impulse control disorders in the formation of addictive disorders"
Currently, a large number of studies have been published on the study of the relationship between impulse control disorders and addictive pathology. Attempts to single out behavioral addictions as a separate group of addictive disorders force us to re-evaluate the role of impulsivity and impulse control disorders at various stages of the formation of both behavioral and substantive addictions. This review is based on the results of research and analysis of existing models of addictive disorders, where the dominant position is given to impulsivity and impulse control disorders as predictors of addictive pathology. Impulsivity plays an important role in most forms of aberrant behavior and other disorders included in current classifications (DSM-V, MBC-10). In our opinion, in most existing models of addictive pathology, impulsivity and impulse control disorders are given undeservedly little attention, which ultimately leads to an incorrect assessment of substantive and behavioral addictions. A model of the development of disorders of the addictive register is proposed, where the disorder of impulse control is given a decisive place in the question of "to be or not to be" addictive pathology.
Attempts to single out behavioral addictions as a separate group of addictive disorders force us to re-evaluate the role of impulsivity and impulse control disorders at various stages of the formation of both behavioral and substantive addictions. This review is based on the results of research and analysis of existing models of addictive disorders, where the dominant position is given to impulsivity and impulse control disorders as predictors of addictive pathology. Impulsivity plays an important role in most forms of aberrant behavior and other disorders included in current classifications (DSM-V, MBC-10). In our opinion, in most existing models of addictive pathology, impulsivity and impulse control disorders are given undeservedly little attention, which ultimately leads to an incorrect assessment of substantive and behavioral addictions. A model of the development of disorders of the addictive register is proposed, where the disorder of impulse control is given a decisive place in the question of "to be or not to be" addictive pathology.
Psychological aspects of pedagogical activity
Date of publication: 09/25/2019.
Assess the material Average rating: 0 (total: 0)
Dinmukhametova Rushania Farazievna , teacher
MBOU “Kukmorskaya School No. 4” , Tatarstan Republic
"Attention deficit hyperactivity disorder in primary school students"
The article considers the relevance of the problem of teaching children with ADHD in the context of the Federal State Educational Standard, highlights the essence of attention deficit hyperactivity disorder: signs and causes. The psychological characteristics of these children are given. Psychological assistance to the child is considered, recommendations are given to the teacher and parents on organizing assistance to children with behavioral problems, recommendations for eliminating the problems of attention disorders in children of primary school age. The work will be of interest to those who have children with attention deficit hyperactivity disorder in their class, parents, psychologists. The main goal of the work is to provide assistance in organizing psychological and pedagogical support for children with ADHD studying in a mass school.
The work will be of interest to those who have children with attention deficit hyperactivity disorder in their class, parents, psychologists. The main goal of the work is to provide assistance in organizing psychological and pedagogical support for children with ADHD studying in a mass school.
Psychology
Date of publication: 04/03/2019.
Assess the Material Average rating: 0 (total: 0)
Chuprikova Elizaveta Valerievna , student
FSBEI State University , Voronezhskaya, Voronezhskaya obl
"Relationship of the main personality traits with the propensity to take risks"
The article analyzes the main personality traits associated with the propensity to take risks. The results of studies confirming the relationship of risk appetite with impulsiveness, aggressiveness, achievement motivation, independence, etc. are given.
Psychological and pedagogical aspects of education
Date of publication: 02/28/2017.
Assess the Material Average Assessment: 0 (total: 0)
Antonova Antonova Angelina Sergeevna , student
Togapou “Pedagogical College” , Tambovskaya obl. Particular attention is drawn to the fact that the presence of ADHD leads to the formation of various consequences, such as the complexity of the psychological readiness of children for schooling. The relevance of this topic is proved both in the field of psychology and in the field of pedagogy.
Psychological and pedagogical foundations of preschool education
Date of publication: 05/18/2016
Assess the material Average rating: 0 (total: 0)
Malovitskaya Nadezhda Ruslanovna , student
Smoleva Tatyana Oktyabrinovna , candy . ped. Sciences, Associate Professor, Lecturer
Irkutsk State University , Irkutsk Region
“Manifestation and overcoming of impulsiveness of a preschool child”
The article is devoted to the problem of increased impulsivity of a child at the stage of senior preschool age. Particular attention is paid to the picture of the manifestation of impulsivity in the cognitive, affective and behavioral spheres. The stages and content of the organization of game training are presented. These training methods can be used by students, psychologists and teachers.
Particular attention is paid to the picture of the manifestation of impulsivity in the cognitive, affective and behavioral spheres. The stages and content of the organization of game training are presented. These training methods can be used by students, psychologists and teachers.
Correctional pedagogy, defectology
Publication date: 05/06/2016
Rate the material Average rating: 5 (Total: 59)
Burachevskaya Olga Vladimirovna Head of Department
Moscow State University Center for Innovative Learning and Development Logos Belarus the main concepts and concepts of attention deficit hyperactivity disorder (ADHD) are considered. The author analyzes the main models of pedagogical support for children with ADHD. The paper provides guidelines for organizing work with children of preschool and primary school age.
ABIZOL IZITAB instructions UA/18410/01/01 (44896) NOBEL ILAC SANAJ VE TIJARET A.
 Sh.
Sh. Back to instruction list
| International nonproprietary name | Aripiprazole |
| ATC code | N05AX12 |
| Type MNN | Mono |
| Release form | tablets, dispersible in the mouth empty, 10 mg, 7 tablets in a blister, 4 blisters in a carton pack |
| Wash your permit | for prescription |
| Warehouse | 1 tablet to replace aripiprazole 10 mg |
| Pharmacological group | Psycholeptic problems. Antipsychotic treatments. Other neuroleptics. Antipsychotic treatments. Other neuroleptics. |
| Applicant | NOBEL ILACH SANAI VE TIJARET A.Sh. Turechchina |
| Virobnik | NOBEL ILACH SANAI VE TIJARET A.Sh. Turkey |
| Registration number | UA/18410/01/01 |
| Cob date | 11/11/2020 |
| Line end date | 11/11/2025 |
| Dostrokove | Hi |
| Type LZ | Zvichayny |
| LZ biological care | Hi |
| Hi | |
| LZ-orphan | Hi |
| Homeopathic LZ | Hi |
| Applicability term | 3 rocks |
| Pharmaceutical form | tablets that are dispersed in the mouth empty |
| Manual | Get instructions |
Stock:
oral speech: aripiprazole;
1 tablet to replace aripiprazole 10 mg or 15 mg;
additional speech: calcium silicate, manite (E 421), manite DC (E 421), crospovidone XL-10, crospovidone CL, anhydrous silica, aspartame (E 951), potassium acesulfame, tartaric acid yellow (E 172) (for a dose of 15 mg), chervonium oxide (E 172) (for a dose of 10 mg), magnesium stearate, cherry flavor additive, microcrystalline cellulose.
Pharmaceutical form. Tablets to be dispersed in the empty mouth.
Basic physical and chemical powers:
tablets 10 mg: round tablets in erysipelas color with "10" embossed on one side;
tablets 15 mg: yellow color round tablets with "15" embossed on one side.
Pharmacotherapeutic group.
Psycholeptic problems. Antipsychotic treatments. Other neuroleptics.
ATX code N05A X12.
Pharmacological authorities.
Pharmacodynamics.
Mechanism diy. Therapeutic use of aripiprazole in the treatment of schizophrenia and bipolar disorder type I has been associated with partial agonism of the alpha dopamine D2 receptors and serotonin 5-HT1a, as well as antagonism of the alpha receptors of serotonin 5-HT2a. It has been observed that aripiprazole exhibited antagonistic power in creature models of dopaminergic hyperactivity and agonistic power in animal models of dopaminergic hypoactivity. Aripiprazole may have a high affinity for linking in vitro receptors for dopamine D2 and D3, serotonin receptors 5-HT1a and 5-HT2a, as well as a decrease in affinity for receptors for dopamine D4, serotonin 5-HT2c and 5-HT7, and adrenergic receptors for h2 receptors Aripiprazole also has a significant affinity for serotonin receptors and no significant affinity for muscarinic receptors. Interactions with other receptors, krim subtypes of dopamine and serotonin, may explain other clinical effects of aripiprazole.
Aripiprazole may have a high affinity for linking in vitro receptors for dopamine D2 and D3, serotonin receptors 5-HT1a and 5-HT2a, as well as a decrease in affinity for receptors for dopamine D4, serotonin 5-HT2c and 5-HT7, and adrenergic receptors for h2 receptors Aripiprazole also has a significant affinity for serotonin receptors and no significant affinity for muscarinic receptors. Interactions with other receptors, krim subtypes of dopamine and serotonin, may explain other clinical effects of aripiprazole.
Pharmacokinetics.
Wetting. Aripiprazole is well absorbed, and its maximum plasma concentration (Cmax) is reached in 3-5 years after ingestion. Aripiprazole is known to have minimal first pass metabolism. The absolute bioavailability of the drug when taken orally is 87%. Livening with high fat content does not affect the pharmacokinetics of aripiprazole.
Rozpodil. Aripiprazole is widely distributed in body tissues. The volume of the subdivision becomes 4. 9l / kg, which indicates a great extravascular rozpodіl. When administered at therapeutic doses, aripiprazole and dehydroaripiprazole are more than 99% less bound to blood serum proteins, more importantly to albumin.
9l / kg, which indicates a great extravascular rozpodіl. When administered at therapeutic doses, aripiprazole and dehydroaripiprazole are more than 99% less bound to blood serum proteins, more importantly to albumin.
Biotransformation. Aripiprazole is extensively metabolized in the liver, mainly via dehydrogenation, hydroxide and N-dealkylation. in vitro enzymes CYP3A4 and CYP2D6 seem to be responsible for the dehydrogenation and hydroxylation of aripiprazole, and N-dealkylation catalyzes CYP3A4. Aripiprazole is the main drug in the systemic bloodstream. At an equally important level, dehydroaripiprazole, its most active metabolite, should be close to 40% of the AUC value of aripiprazole in plasma.
Visit. The median period of administration of aripiprazole is approximately 75 years in case of active CYP2D6 metabolism and approximately 146 years in case of poor CYP2D6 metabolism.
Global clearance of aripiprazole is up to 0.7 ml/min/kg, mainly due to hepatic clearance. Following a single oral dose of 14 C-labeled aripiprazole, approximately 27% was excreted in the section and approximately 60% was excreted in the feces. Less than 1% of unchanged aripiprazole was excreted in the stool, approximately 18% of unchanged aripiprazole was excreted in the feces.
Pharmacokinetics in special groups of patients.
Patients of the summer age. Review of pharmacokinetics of aripiprazole in healthy volunteers during the summer and more young patients during the day.
Article. Review of pharmacokinetics of aripiprazole in healthy men and women during the day.
Chicken and race. Pharmacokinetic assessment of the population did not reveal clinically significant, race-specific or smoking influences on the pharmacokinetics of aripiprazole.
Troubleshooting. It has been shown that the pharmacokinetic characteristics of aripiprazole and dehydroaripiprazole are the same both in patients with severe ailments and in healthy volunteers.
Impaired liver function. There is no sufficient data on the metabolic properties of aripiprazole in patients with impaired liver function.
Clinical characteristics.
Indications for treatment of schizophrenia in adults.
The drug is indicated for the treatment of mild and severe manic episodes in bipolar disorder type I, as well as for the prevention of new maniacal episodes in adults who had earlier suffered maniacal episodes and were treated with aripprazole.
Contraindication.
Hypersensitivity to aripiprazole or to any other component of the drug.
Interaction with other medical procedures and other types of interaction.
As a result of α1-adrenergic receptor antagonism, aripiprazole may potentiate the effect of other antihypertensive drugs.
In view of the main injection of aripiprazole into the central nervous system (CNS), care should be taken when aripiprazole is ingested with alcohol or other medical problems that are injected into the CNS, in connection with possible cross-effects, such as adverse effects.
Consideration should be given to conserve aripiprazole in other medical cases, as it may extend the QT interval or disrupt the electrical balance.
Potential injection of other drugs for aripiprazole.
Hydrochloric acid secretion inhibitor, h3-histamine receptor antagonist famotidine, reduces the absorption rate of aripiprazole, but the effect is not considered clinically significant. Aripiprazole is metabolized by dekilcom pathways through the participation of CYP2D6 and CYP3A4 enzymes, but not CYP1A enzymes. In this rank, it is not necessary for chickens to correct the dose.
Quinidine and other CYP2D6 inhibitors.
In the first hour of clinical follow-up, it was reported that in healthy volunteers, the CYP2D6 inhibitor (quinidine) increased the AUC of aripiprazole by 107%, while the indicator Cmax remained unchanged. The AUC and Cmax of dehydroaripiprazole, the active metabolite, decreased by 32% and 47% significantly.
The dose of aripiprazole needs to be reduced by about half at every one-hour dose with quinidine. Other inhibitors of CYP2D6, such as fluoxetine and paroxetine, also show a similar effect, so dose reductions in different situations may be the same.
Ketoconazole and other CYP3A4 inhibitors.
In those with reduced CYP2D6 metabolism, one-hour administration of CYP3A4 anti-anxiety inhibitors may produce higher plasma concentrations of aripiprazole compared to those in patients with active CYP2D6 metabolism. In times of need for one-hour infusion of ketoconazole or other CYP3A4 inhibitory inhibitors with aripiprazole, the potential for overestimation of possible risks for the patient. In cases of one-hour administration of aripiprazole and ketoconazole, the dose of aripiprazole should be reduced by approximately half. Other inhibitors of CYP3A4, such as itraconazole and inhibitors of the VIL protease, could theoretically have the same effect, but should similarly reduce doses.
After taking the CYP2D6 or CYP3A4 inhibitor, the dose of aripiprazole should be increased up to the level, after which it stopped until the cob of suputny lykuvannya.
Possible non-significant increase in the concentration of aripiprazole during one-hour exposure to weak CYP3A4 inhibitors (for example, diltiazem or escitalopram) or CYP2D6.
Carbamazepine and other CYP3A4 inhibitors.
After one-hour treatment with carbamazepine, a CYP3A4 strain inducer, aripiprazole Cmax and AUC were 68% and 73% lower, similar to those with aripiprazole (30 mg) monotherapy. Similarly, Cmax and AUC values after one-hour ingestion of dehydroaripiprazole with carbamazepine were 69% and 71% lower, lower with aripiprazole monotherapy.
The dose of aripiprazole needs to be adjusted at different one-hour doses with carbamazepine. Other CYP3A4 inducers (such as rifampicin, rifabutin, phenytoin, phenobarbital, primidone, efavirenz, nevirapine, and animal savage) theoretically may have a similar effect, so a dose shift is needed. If a CYP3A4 strain inducer is prescribed, the dose of aripiprazole should be reduced to the recommended dose.
Valproate and lithium.
No clinically significant changes in aripiprazole concentrations were observed when taking valproate or lithium one-hourly with aripiprazole.
Serotonin syndrome.
In patients treated with aripiprazole, serotonin syndrome depression was suspected; especially in the case of one-hour congestion with other serotonergic drugs, such as SIS3C (selective serotonin serum inhibitor/selective serotonin/norepinephrine serum inhibitor), or drugs that increase the concentration of aripiprazole. vitro . In this manner, it is unlikely that aripiprazole causes a clinically significant infusion in the speech, which is metabolized by the enzyme.
No clinically significant changes in the concentrations of valproate, lithium or lamotrigine were observed in the case of one-hour administration of aripiprazole with valproate, lithium or lamotrigine.
When treated with antipsychotics, the clinic can take a patient from a decade to a decade. During this period, we should keep a close look at the camp of patients.
Lower QT interval. Clinical trials of aripiprazole equivocal with placebo showed a decrease in QT interval depression. Aripiprazole, as well as other antipsychotics, should be taken with care in patients with a history of a prolonged QT interval.
Life of dyskinesia. In the event of the appearance of symptoms of chronic dyskinesia in the presence of a medical condition, the dose of the drug should be changed or yogo administered. After the introduction of therapy and symptoms, the symptoms may timchasovo possilititsya or navіt z'avіtisya after the application of zastosuvannya.
Other extrapyramidal symptoms. Akathisia and parkinsonism have been reported in pediatric patients with aripiprazole. If the symptoms of other extrapyramidal disorders in patients are to be blamed for taking aripiprazole, then changing the dose of the drug should be carefully monitored for the clinical setting of patients.
Malicious neuroleptic syndrome (NMS). NMS is a complex of symptoms associated with drug addictions-neuroleptics, which can potentially lead to a lethal outcome.
Clinical manifestations of NMS - hyperpyrexia (even high body temperature), malignancy, changes in mental status and signs of disorder of the autonomic nervous system (irregular pulse or arterial pressure, tachycardia, increased sweating). Additional signs may include an increase in creatine kinase levels, myoglobinuria (rhabdomyolysis), and hostile deficiency. Prote posterigalis and okremі vypadki p_dvishchennya equal creatine kinase and rhabdomіolіzu, not ob'yazkovo po'yazanі z MNS. If a patient develops symptoms of NMS or an undiagnosed high body temperature without additional clinical manifestations of NMS, in the presence of neuroleptic drugs, including aripiprazole, it is necessary to inject.
Sudomi. In clinical trials, aripiprazole has been infrequently reported with court cases. In this manner, aripiprazole should be taken with caution in patients with a history of court proceedings in the countries that were convicted by the court.
Patients of the summer age with psychosis on aphids dementia.
Increased mortality. In clinical studies with aripiprazole in patients with Alzheimer's disease in the summer (middle century - 82 years), there was an increase in the risk of fatality compared with placebo. Mortality rates were equal with aripiprazole 3.5% compared to 1.7% with placebo, although there were different causes of death: cerebrovascular disease (eg, heart failure, rapt death), infections (eg, pneumonia).
Uncommon reactions of a cerebrovascular nature. In some clinical cases, it was reported about the cardiovascular side effects (for example, stroke, transient ischemic attacks), including fatal episodes (middle age - 84 years, years 78 to 88 years). Zagalom in 1.3% of patients, yakі took off aripiprazole, it was reported about the heart-vascular side reactions equally with 0. 6% of patients, ykі took off placebo.
These features are not statistically significant. In addition, in one of them, there was an association with the use of aripiprazole and cerebrovascular side effects due to fixed doses.
Hypersensitivity. As with other drug exposures, hypersensitivity reactions may develop with aripiprazole exposure.
Increased body oil.
at Patziyntiv Isophrenia -Mauchayu abyazodes of the bipolar outlet often get the zbizhnnya of Masi Tila, sopetologii, the heaviness of the neuroleptic, the way of the Zbizhnnya, the method of life, the way
Patients treated with aripiprazole during post-exposure period showed increased body weight. In these patients, there is a significant risk factor, such as a history of circulatory diabetes, disease of the thyroid gland and adenoma of the pituitary gland. In clinical studies of aripiprazole in mature adults, there was no clinically significant increase in body mass. In clinical studies of aripiprazole in the course of manic episodes of bipolar disorder after 4 days of treatment, an increase in the body mass associated with the use of aripiprazole was observed. In patients with manic episodes of bipolar disorder, it is necessary to control body weight. With a significant increase in body mass, it is necessary to change the diet as much as possible to change the dose (div. section "Adverse reactions").
Dysphagia. Antipsychotics, including aripiprazole, can cause dysmotility of the stravokhod and aspiration, so aripiprazole has been shown to be safe in patients with acute aspiration pneumonia.
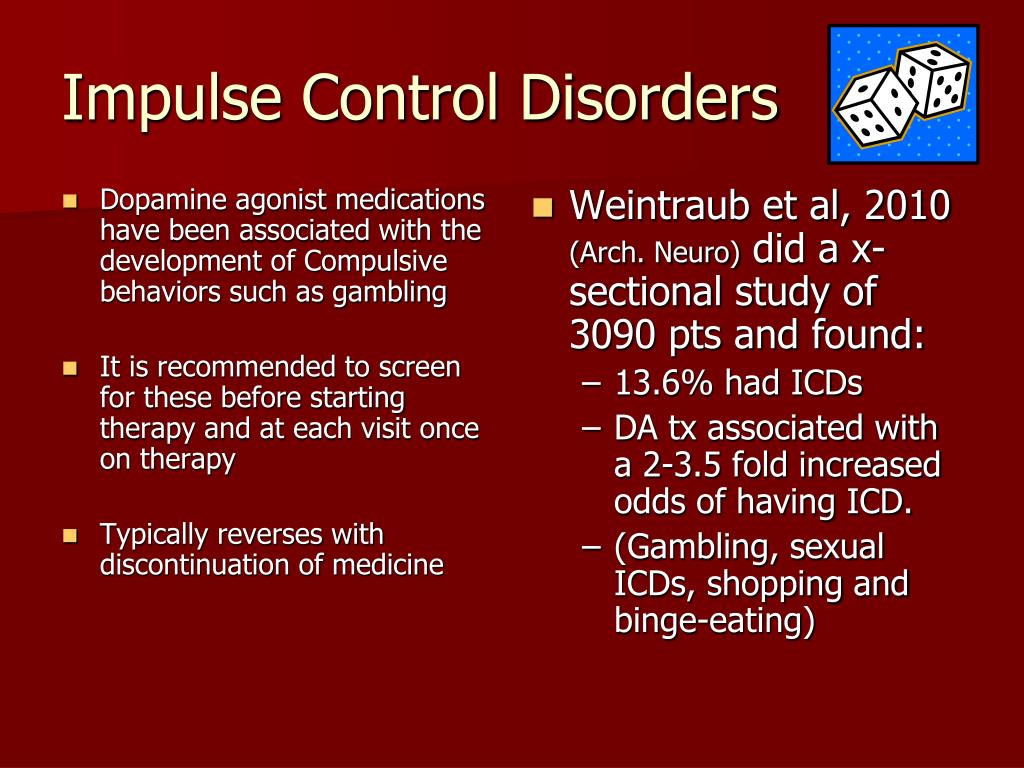
Pathological susceptibility to gambling and other disorders of impulse control.
Patients may experience worsening of their pathological weakness, especially gambling, and lack of control of attacks under the hour of taking aripiprazole. Also, it was said about hypersexuality, non-pereborny cravings before shopping, overdoing or non-controlling cravings before getting used to and other disorders of impulsive and compulsive behavior. It is important that the doctors informed the patients about the development of new or more important disorders when treated with aripiprazole. It has been noted that the symptoms of impulse control may be associated with the main disorder, however, it has sometimes been said about taking a sip when the dose of the drug is changed, or when taking a drug. Disorders of impulse control can cause harm to the patient and other people, as the stench is not intended. If a patient develops such stubbornness for an hour taking aripiprazole, it is necessary to check the nutrition about the dose change, or else to take it.
Patients with concomitant ailments of ADHD (syndrome of deficiency of respect and hyperactivity). Regardless of the high frequency of such concomitant illnesses, such as bipolar disorder type I and ADHD, given the safety of an one-hour intake of aripiprazole and a stimulant in the same place, in case of an one-hour recognition of these diseases, supervised care is necessary.
Congestion during pregnancy and breastfeeding.
Vagity.
Adequate follow-up of aripiprazole for the participation of pregnant women has not been conducted. Congenital anomalies were reported, and no causal link with aripiprazole was identified. Based on the data obtained on animals, it is impossible to exclude the possibility of embryo-fetotoxicity. Patients should be told to tell the doctor about the current vagity, or we should take care of the pregnancy under the hour of treatment with aripiprazole. In connection with the lack of information about the safety of aripiprazole ingestion in the period of pregnancy, it can be recognized only once, if the measles for the vagitum is estimated, the potential risk for the fetus is overestimated.
Newborns whose mothers have taken neuroleptics (including aripiprazole) during the third trimester of pregnancy, may experience adverse reactions, including extrapyramidal symptoms and/or withdrawal syndrome, which may be reduced due to severity and trivalence. Vіdomo pro vpadki zbudzhennya, pіdvishchennya or decrease m'yazovogo tone, tremors, drowsiness, derangement of the breath or problems with years. Otzhe, it is necessary to carefully watch the camp of such new people.
Breastfeeding period.
Aripiprazole is seen in breast milk. It is necessary to make a decision about whether to apply the breastfeeding or to the treatment with aripiprazole with the improvement of the cortex of the chest for the child and the transfer of the therapy for the woman.
Fertility.
Data on reproductive toxicity of aripiprazole does not affect fertility.
Healthiness to add to the speed of the reaction when caring for vehicles or other mechanisms.
Arip Prisol Ma, the insignificant abstract, having fed to the building of Keruvati by the vehicle by the mechanisms of the Zv'yazka, the potatoes on the nervous system of the same organ of the Victory reacts, such yak sedasia, dreaming, inconsistency, Razmithicity of Rye. "Side reactions").
Dosing method.
Adults
Schizophrenia . It is recommended that the initial dose of the drug be 10 or 15 mg/dobu, and the lower dose is 15 mg/dobu. The qiu dose is taken 1 time for doba independently in the course of living.
The drug is effective in the dose range of 10 to 30 mg/dose. There has been no evidence of an increase in efficacy with doses that could be increased to an additional dose of 15 mg, although sane patients may be able to increase the dose.
The maximum additional dose is not to be exceeded 30 mg.
Manic episodes in bipolar disorder type I. The recommended dose of the drug is 15 mg. The qiu dose is taken 1 time for doba independently in the course of living. The drug can be used as monotherapy or at the warehouse of combined treatment. For a small number of patients, dose adjustments may be effective. The maximum additional dose is not guilty of overdosing 30 mg.
Prevention of new manic episodes in bipolar I type . To prevent relapses of manic episodes in patients, if they took aripiprazole as monotherapy, or at the warehouse of combined treatment, they should continue taking the drug at the same dose. Looking back at the clinical situation of the patient, a correction of the additional dose is possible, including a reduction.
Special groups of patients
Patients with impaired liver function. Patients with weak or moderate stages of liver failure do not need dose adjustment. There are not enough obvious data to provide recommendations to patients with severely impaired liver function. The dose for these patients should be taken carefully. For patients with severely impaired liver function, the maximum additional dose of 30 mg should be reserved.
Patients with impaired neurological function. Patients with impaired function do not require dose adjustment.
Patients of the summer age. The efficacy of the drug in treating schizophrenia and type I bipolar disorder in patients of 65 years of age has not been established. Taking into account the greater sensitivity of the population of patients, the next thing to look at is the increase in low cob doses of the drug, which allows other clinical factors.
Article. Dose adjustment is not necessary according to patient status.
Chicken. In view of the pathways to aripiprazole metabolism, chickens do not require dose adjustment.
Dose adjustment in conjunction with interactions. In case of one-hour administration of CYP3A4 or CYP2D6 anti-anxiety inhibitors with aripiprazole, the dose of aripiprazole should be reduced. In addition, combination regimens include the CYP3A4 or CYP2D6 inhibitor, the dose of aripiprazole should be adjusted.
At times of one-hour administration of CYP3A4 strain inducers with aripiprazole, the dose of aripiprazole was slightly increased. If the combination regimens include the CYP3A4 inducer, the dose of aripiprazole should be reduced to the recommended dose.
Method of ingestion
Prescription drug for oral ingestion.
Place the tablet in the mouth on the tongue, it will be easily dispersed in the line. The tablet can be taken with or without the mother. It is important to see a tablet from the mouth empty of a non-shocked one. Oskіlki tablet є krikhkoy, її slud take it negligently after taking the blister As an alternative, the tablet can be dispersed in water and drink the suspension.
Tablets that are dispersed in the mouth emptying can be vicarious as an alternative to other pharmaceutical forms of the drug for patients, as they may be difficult to work with.
Children.
The drug is not suitable for children, but it is impossible to provide a cob dose according to the dosage regimen.
Overdose.
Signs and symptoms
Sudden or acute acute overdose of aripiprazole at doses up to 1260 mg has been described in adult patients without a fatal case. Potentially important from a medical point of view, the symptoms that were suspected were bully lethargy, arterial pressure, drowsiness, tachycardia, nausea, vomiting, and diarrhea.
Ok, let's take a look at the data on the incidence of overdose, including aripiprazole (at doses up to 195 mg) in children, which is not a little lethal. Potentially important from a medical point of view, the symptoms that were suspected were drowsiness, short-term loss of symptoms and extrapyramidal symptoms.
Treatment for overdose
Treatment for overdose should include supportive therapy, airway clearance, oxygen therapy, mechanical ventilation, and symptom control. Take care of the possibility of overdosing with numerous medical problems. Through tse necessitate negligent control of the heart-vascular system, it is my responsibility to turn on the constant monitoring of the ECG for the detection of possible arrhythmias. After an confirmed or immediate overdose of aripiprazole, a further medical review and monitoring of the patient's state of health is necessary until the end of his recovery.
Activated Vugill (50 g), which stopped 1 year after taking aripiprazole, reduced the Cmax of aripiprazole by approximately 41% and the AUC by approximately 51%, suggesting the possibility of effective redundancy in activated Vugillum.