Where is serotonin produced in the brain
The Expanded Biology of Serotonin
1. Rapport MM, Green AA, Page IH. Serum vasoconstrictor, serotonin; isolation and characterization. J. Biol. Chem. 1948;176:1243–51. [PubMed] [Google Scholar]
2. Roth BL, editor. The Serotonin Receptors: From Molecular Pharmacology to Human Therapeutics. Totowa, NJ: Humana; 2007. [Google Scholar]
3. Roth BL. Multiple serotonin receptors: clinical and experimental aspects. Ann. Clin. Psychiatry. 1994;6:67–78. [PubMed] [Google Scholar]
4. Roth BL, Xia Z. Molecular and cellular mechanisms for the polarized sorting of serotonin receptors: relevance for genesis and treatment of psychosis. Crit. Rev. Neurobiol. 2004;16:229–36. [PubMed] [Google Scholar]
5. Kroeze WK, Kristiansen K, Roth BL. Molecular biology of serotonin receptors: structure and function at the molecular level. Curr. Top. Med. Chem. 2002;2:507–28. [PubMed] [Google Scholar]
6. Kroeze WK, Hufeisen SJ, Popadak BA, et al. h2-histamine receptor affinity predicts short-term weight gain for typical and atypical antipsychotic drugs. Neuropsychopharmacology. 2003;28:519–26. [PubMed] [Google Scholar]
7. Roth BL. Drugs and valvular heart disease. N. Engl. J. Med. 2007;356:6–9. [PubMed] [Google Scholar]
8. Gershon MD, Tack J. The serotonin signaling system: from basic understanding to drug development for functional GI disorders. Gastroenterology. 2007;132:397–414. [PubMed] [Google Scholar]
9. Mengod G, Vilaro MT, Cortes R, et al. Chemical neuroanatomy of 5-HT receptor subtypes in the mammalian brain. In: Roth BL, editor. The Serotonin Receptors: From Molecular Pharmacology to Human Therapeutics. Totowa, NJ: Humana; 2007. pp. 319–64. [Google Scholar]
10. Araneda R, Andrade R. 5-Hydroxytryptamine 2 and 5-hydroxytryptamine 1A receptors mediate opposing responses on membrane excitability in rat association cortex. Neuroscience. 1991;40:399–412. [PubMed] [Google Scholar]
11. Airan RD, Meltzer LA, Roy M, et al. High-speed imaging reveals neurophysiological links to behavior in an animal model of depression.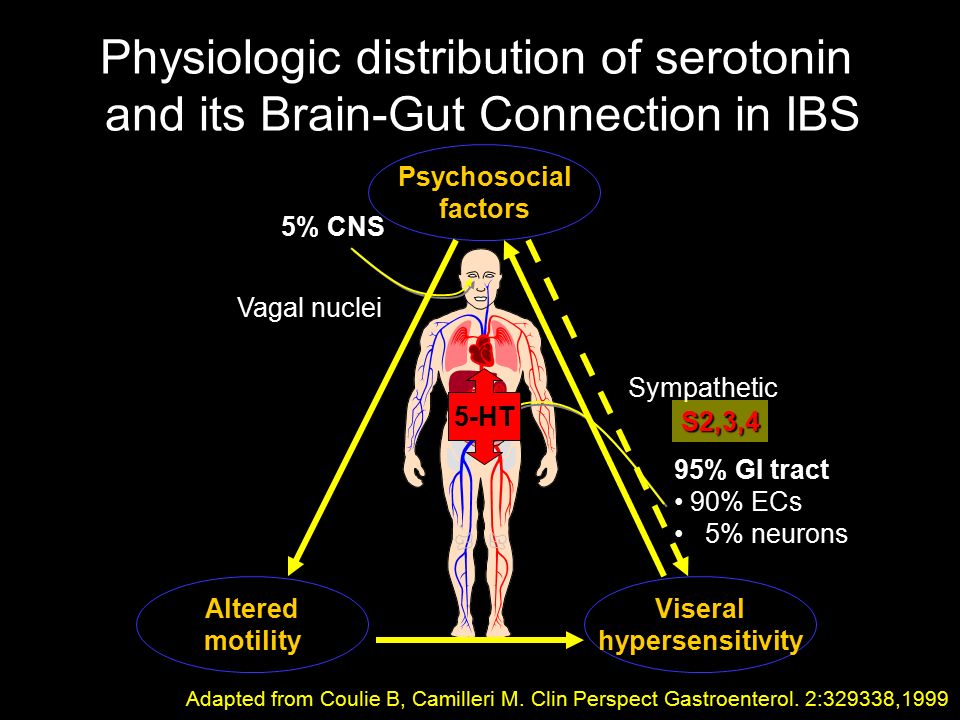 Science. 2007;317:819–23. [PubMed] [Google Scholar]
Science. 2007;317:819–23. [PubMed] [Google Scholar]
12. Canli T, Lesch KP. Long story short: the serotonin transporter in emotion regulation and social cognition. Nat. Neurosci. 2007;10:1103–9. [PubMed] [Google Scholar]
13. Roth BL, Hanizavareh SM, Blum AE. Serotonin receptors represent highly favorable molecular targets for cognitive enhancement in schizophrenia and other disorders. Psychopharmacology (Berl.) 2004;174:17–24. [PubMed] [Google Scholar]
14. Gross C, Hen R. The developmental origins of anxiety. Nat. Rev. Neurosci. 2004;5:545–52. [PubMed] [Google Scholar]
15. Lesch KP. Serotonergic gene inactivation in mice: models for anxiety and aggression? Novartis Found. Symp. 2005;268:111–40. [PubMed] [Google Scholar]
16. Giorgetti M, Tecott LH. Contributions of 5-HT2C receptors to multiple actions of central serotonin systems. Eur. J. Pharmacol. 2004;488:1–9. [PubMed] [Google Scholar]
17. Gray JA, Roth BL. The pipeline and future of drug development in schizophrenia. Mol. Psychiatry. 2007;12:904–22. [PubMed] [Google Scholar]
Mol. Psychiatry. 2007;12:904–22. [PubMed] [Google Scholar]
18. Schechter LE, Ring RH, Beyer CE, et al. Innovative approaches for the development of antidepressant drugs: current and future strategies. NeuroRx. 2005;2:590–611. [PMC free article] [PubMed] [Google Scholar]
19. Kaumann AJ, Levy FO. 5-hydroxytryptamine receptors in the human cardiovascular system. Pharmacol. Ther. 2006;111:674–706. [PubMed] [Google Scholar]
20. Hamel E. Serotonin and migraine: biology and clinical implications. Cephalalgia. 2007;27:1293–300. [PubMed] [Google Scholar]
21. Ni W, Watts SW. 5-hydroxytryptamine in the cardiovascular system: focus on the serotonin transporter (SERT) Clin. Exp. Pharmacol. Physiol. 2006;33:575–83. [PubMed] [Google Scholar]
22. Carneiro AM, Cook EH, Murphy DL, Blakely RD. Interactions between integrin αIIbβ3 and the serotonin transporter regulate serotonin transport and platelet aggregation in mice and humans. J. Clin. Invest. 2008;118:1544–52. [PMC free article] [PubMed] [Google Scholar]
23. Sauer WH, Berlin JA, Kimmel SE. Effect of antidepressants and their relative affinity for the serotonin transporter on the risk of myocardial infarction. Circulation. 2003;108:32–36. [PubMed] [Google Scholar]
Sauer WH, Berlin JA, Kimmel SE. Effect of antidepressants and their relative affinity for the serotonin transporter on the risk of myocardial infarction. Circulation. 2003;108:32–36. [PubMed] [Google Scholar]
24. Taylor CB, Youngblood ME, Catellier D, et al. Effects of antidepressant medication on morbidity and mortality in depressed patients after myocardial infarction. Arch. Gen. Psychiatry. 2005;62:792–98. [PubMed] [Google Scholar]
25. Glassman AH. Does treating postmyocardial infarction depression reduce medical mortality? Arch. Gen. Psychiatry. 2005;62:711–12. [PubMed] [Google Scholar]
26. Somberg TC, Arora RR. Depression and heart disease: therapeutic implications. Cardiology. 2008;111:75–81. [PubMed] [Google Scholar]
27. Walther DJ, Peter JU, Winter S, et al. Serotonylation of small GTPases is a signal transduction pathway that triggers platelet alpha-granule release. Cell. 2003;115:851–62. [PubMed] [Google Scholar]
28. Dale GL. Coated-platelets: an emerging component of the procoagulant response. J. Thromb. Haemost. 2005;3:2185–92. [PubMed] [Google Scholar]
J. Thromb. Haemost. 2005;3:2185–92. [PubMed] [Google Scholar]
29. Langer C, Piper C, Vogt J, et al. Atrial fibrillation in carcinoid heart disease: the role of serotonin. A review of the literature. Clin. Res. Cardiol. 2007;96:114–18. [PubMed] [Google Scholar]
30. Singh S. Trials of new antiarrhythmic drugs for maintenance of sinus rhythm in patients with atrial fibrillation. J. Interv. Cardiol. Electrophysiol. 2004;10(Suppl. 1):71–76. [PubMed] [Google Scholar]
31. Brattelid T, Qvigstad E, Lynham JA, et al. Functional serotonin 5-HT4 receptors in porcine and human ventricular myocardium with increased 5-HT4mRNAin heart failure. Naunyn Schmiedebergs Arch. Pharmacol. 2004;370:157–66. [PubMed] [Google Scholar]
32. Birkeland JA, Sjaastad I, Brattelid T, et al. Effects of treatment with a 5-HT4 receptor antagonist in heart failure. Br. J. Pharmacol. 2007;150:143–52. [PMC free article] [PubMed] [Google Scholar]
33. Doggrell SA. The role of 5-HT on the cardiovascular and renal systems and the clinical potential of 5-HT modulation.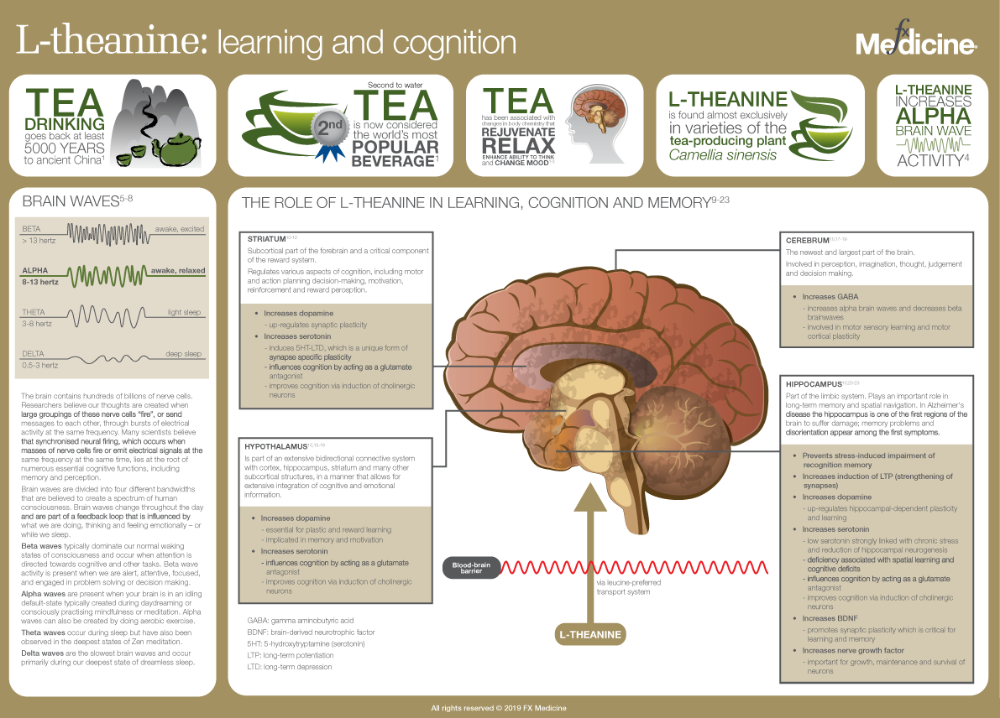 Expert Opin. Investig. Drugs. 2003;12:805–23. [PubMed] [Google Scholar]
Expert Opin. Investig. Drugs. 2003;12:805–23. [PubMed] [Google Scholar]
34. Rothman RB, Baumann MH, Savage JE, et al. Evidence for possible involvement of 5-HT2B receptors in the cardiac valvulopathy associated with fenfluramine and other serotonergic medications. Circulation. 2000;102:2836–41. [PubMed] [Google Scholar]
35. Setola V, Hufeisen SJ, Grande-Allen KJ, et al. 3,4-methylenedioxymethamphetamine (MDMA, “Ecstasy”) induces fenfluramine-like proliferative actions on human cardiac valvular interstitial cells in vitro. Mol. Pharmacol. 2003;63:1223–29. [PubMed] [Google Scholar]
36. Nebigil CG, Maroteaux L. Functional consequence of serotonin/5-HT2B receptor signaling in heart: role of mitochondria in transition between hypertrophy and heart failure? Circulation. 2003;108:902–8. [PubMed] [Google Scholar]
37. Kereveur A, Callebert J, Humbert M, et al. High plasma serotonin levels in primary pulmonary hypertension. Effect of long-term epoprostenol (prostacyclin) therapy.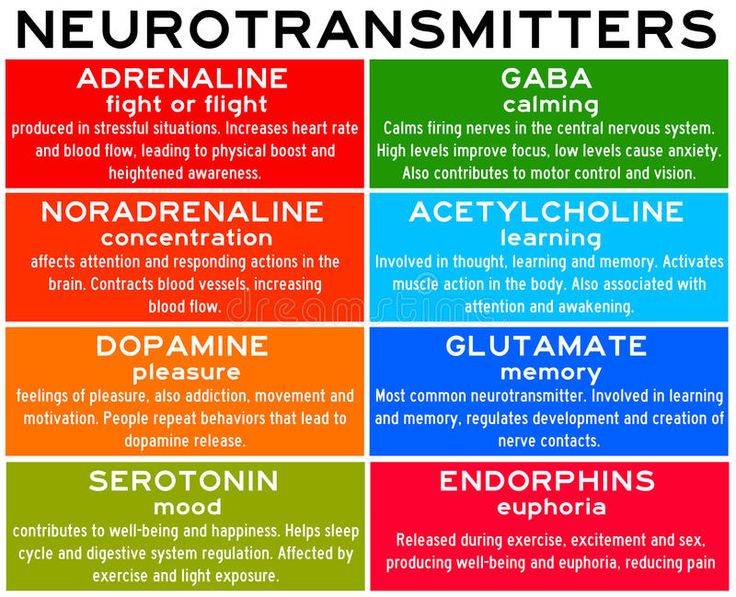 Arterioscler. Thromb. Vasc. Biol. 2000;20:2233–39. [PubMed] [Google Scholar]
Arterioscler. Thromb. Vasc. Biol. 2000;20:2233–39. [PubMed] [Google Scholar]
38. Esteve JM, Launay JM, Kellermann O, Maroteaux L. Functions of serotonin in hypoxic pulmonary vascular remodeling. Cell. Biochem. Biophys. 2007;47:33–44. [PubMed] [Google Scholar]
39. Launay JM, Herve P, Peoc’h K, et al. Function of the serotonin 5-hydroxytryptamine 2B receptor in pulmonary hypertension. Nat. Med. 2002;8:1129–35. [PubMed] [Google Scholar]
40. Deraet M, Manivet P, Janoshazi A, et al. The natural mutation encoding a C terminus–truncated 5-hydroxytryptamine 2B receptor is a gain of proliferative functions. Mol. Pharmacol. 2005;67:983–91. [PubMed] [Google Scholar]
41. Guilluy C, Rolli-Derkinderen M, Tharaux PL, et al. Transglutaminase-dependent RhoA activation and depletion by serotonin in vascular smooth muscle cells. J. Biol. Chem. 2007;282:2918–28. [PubMed] [Google Scholar]
42. Marcos E, Adnot S, Pham MH, et al. Serotonin transporter inhibitors protect against hypoxic pulmonary hypertension.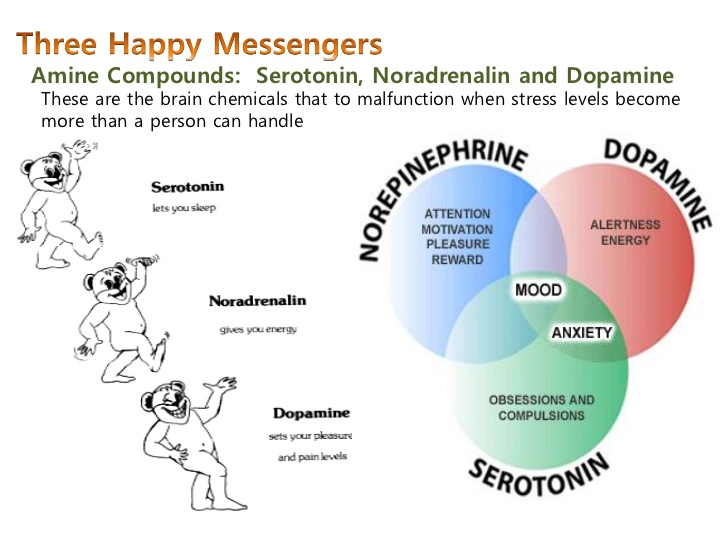 Am. J. Respir. Crit. Care Med. 2003;168:487–93. [PubMed] [Google Scholar]
Am. J. Respir. Crit. Care Med. 2003;168:487–93. [PubMed] [Google Scholar]
43. Eilers H, Schumacher MA. Opioid-induced respiratory depression: Are 5-HT4a receptor agonists the cure? Mol. Interv. 2004;4:197–99. [PubMed] [Google Scholar]
44. Manzke T, Guenther U, Ponimaskin EG, et al. 5-HT4a receptors avert opioid-induced breathing depression without loss of analgesia. Science. 2003;301:226–29. [PubMed] [Google Scholar]
45. Kinney HC, Filiano JJ, White WF. Medullary serotonergic network deficiency in the sudden infant death syndrome: review of a 15-year study of a single dataset. J. Neuropathol. Exp. Neurol. 2001;60:228–47. [PubMed] [Google Scholar]
46. Paterson DS, Trachtenberg FL, Thompson EG, et al. Multiple serotonergic brainstem abnormalities in sudden infant death syndrome. JAMA. 2006;296:2124–32. [PubMed] [Google Scholar]
47. Richerson GB, Wang W, Tiwari J, Bradley SR. Chemosensitivity of serotonergic neurons in the rostral ventral medulla.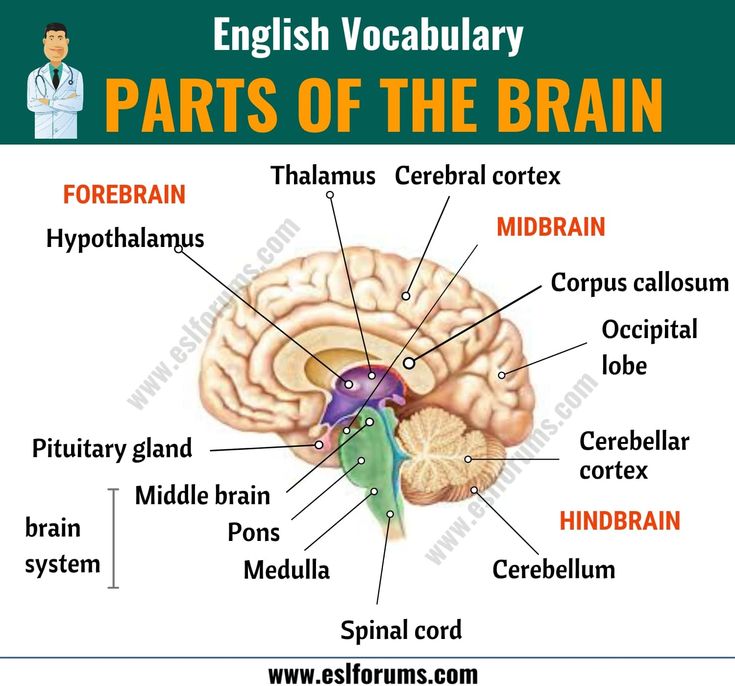 Respir. Physiol. 2001;129:175–89. [PubMed] [Google Scholar]
Respir. Physiol. 2001;129:175–89. [PubMed] [Google Scholar]
48. Erickson JT, Shafer G, Rossetti MD, et al. Arrest of 5HT neuron differentiation delays respiratory maturation and impairs neonatal homeostatic responses to environmental challenges. Respir. Physiol. Neurobiol. 2007;159:85–101. [PMC free article] [PubMed] [Google Scholar]
49. Tecott LH, Abdallah L. Mouse genetic approaches to feeding regulation: serotonin 5-HT2C receptor mutant mice. CNS Spectr. 2003;8:584–88. [PubMed] [Google Scholar]
50. Lam DD, Heisler LK. Serotonin and energy balance: molecular mechanisms and implications for type 2 diabetes. Expert Rev. Mol. Med. 2007;9:1–24. [PubMed] [Google Scholar]
51. Lam DD, Przydzial MJ, Ridley SH, et al. Serotonin 5-HT2C receptor agonist promotes hypophagia via downstream activation of melanocortin 4 receptors. Endocrinology. 2008;149:1323–28. [PMC free article] [PubMed] [Google Scholar]
52. Hodges MR, Tattersall GJ, Harris MB, et al. Defects in breathing and thermoregulation in mice with near-complete absence of central serotonin neurons.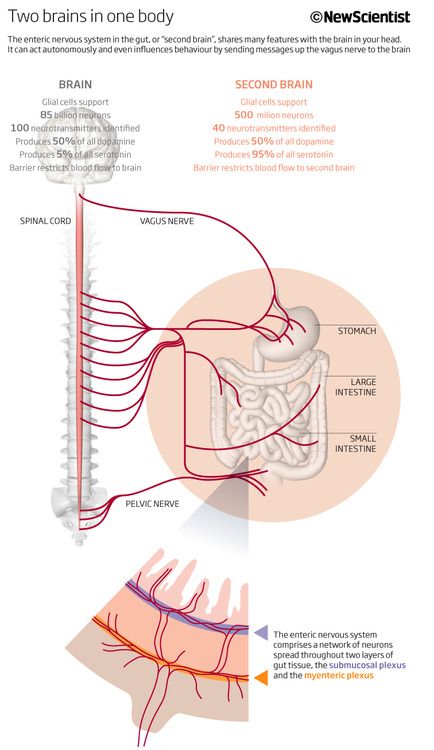 J. Neurosci. 2008;28:2495–505. [PMC free article] [PubMed] [Google Scholar]
J. Neurosci. 2008;28:2495–505. [PMC free article] [PubMed] [Google Scholar]
53. Hedlund PB, Kelly L, Mazur C, et al. 8-OH-DPAT acts on both 5-HT1A and 5-HT7 receptors to induce hypothermia in rodents. Eur. J. Pharmacol. 2004;487:125–32. [PubMed] [Google Scholar]
54. Carrasco GA, Van de Kar LD. Neuroendocrine pharmacology of stress. Eur. J. Pharmacol. 2003;463:235–72. [PubMed] [Google Scholar]
55. Matsuda M, Imaoka T, Vomachka AJ, et al. Serotonin regulates mammary gland development via an autocrine-paracrine loop. Dev. Cell. 2004;6:193–203. [PubMed] [Google Scholar]
56. Stull MA, Pai V, Vomachka AJ, et al. Mammary gland homeostasis employs serotonergic regulation of epithelial tight junctions. Proc. Natl. Acad. Sci. USA. 2007;104:16708–13. [PMC free article] [PubMed] [Google Scholar]
57. Lesurtel M, Graf R, Aleil B, et al. Platelet-derived serotonin mediates liver regeneration. Science. 2006;312:104–7. [PubMed] [Google Scholar]
58. Tecott LH. Serotonin and the orchestration of energy balance.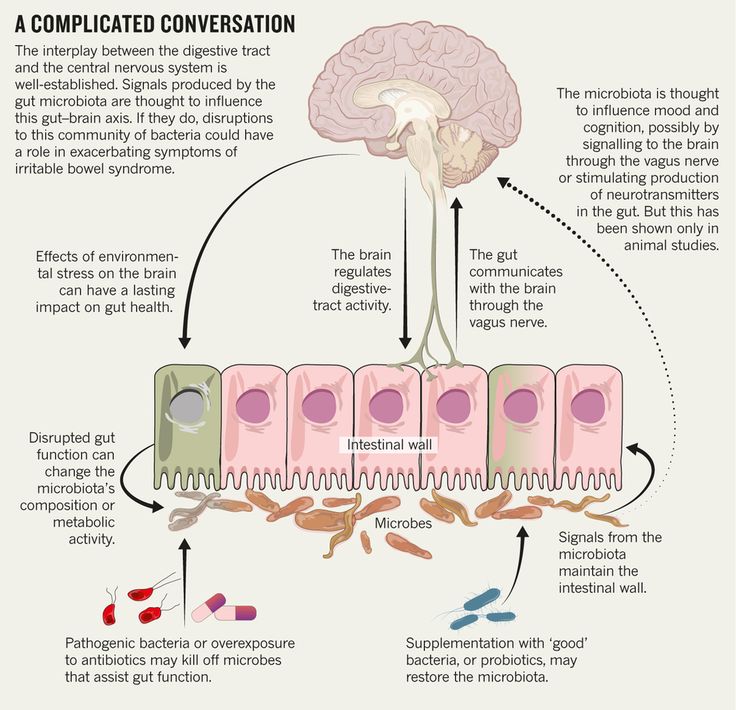 Cell. Metab. 2007;6:352–61. [PubMed] [Google Scholar]
Cell. Metab. 2007;6:352–61. [PubMed] [Google Scholar]
59. Roper SD. Cell communication in taste buds. Cell. Mol. Life Sci. 2006;63:1494–500. [PMC free article] [PubMed] [Google Scholar]
60. Suzuki A, Naruse S, Kitagawa M, et al. 5-hydroxytryptamine strongly inhibits fluid secretion in guinea pig pancreatic duct cells. J. Clin. Invest. 2001;108:749–56. [PMC free article] [PubMed] [Google Scholar]
61. Minami M, Endo T, Hirafuji M, et al. Pharmacological aspects of anticancer drug–induced emesis with emphasis on serotonin release and vagal nerve activity. Pharmacol. Ther. 2003;99:149–65. [PubMed] [Google Scholar]
62. Sommer C. Serotonin in pain and analgesia: actions in the periphery. Mol. Neurobiol. 2004;30:117–25. [PubMed] [Google Scholar]
63. Braz JM, Basbaum AI. Genetically expressed transneuronal tracer reveals direct and indirect serotonergic descending control circuits. J. Comp. Neurol. 2008;507:1990–2003. [PMC free article] [PubMed] [Google Scholar]
64. Jann MW, Slade JH. Antidepressant agents for the treatment of chronic pain and depression. Pharmacotherapy. 2007;27:1571–87. [PubMed] [Google Scholar]
Jann MW, Slade JH. Antidepressant agents for the treatment of chronic pain and depression. Pharmacotherapy. 2007;27:1571–87. [PubMed] [Google Scholar]
65. Mukaida K, Shichino T, Koyanagi S, et al. Activity of the serotonergic system during isoflurane anesthesia. Anesth. Analg. 2007;104:836–39. [PubMed] [Google Scholar]
66. Isbister GK, Buckley NA, Whyte IM. Serotonin toxicity: a practical approach to diagnosis and treatment. Med. J. Aust. 2007;187:361–65. [PubMed] [Google Scholar]
67. de Jong TR, Veening JG, Waldinger MD, et al. Serotonin and the neurobiology of the ejaculatory threshold. Neurosci. Biobehav. Rev. 2006;30:893–907. [PubMed] [Google Scholar]
68. Giuliano F. 5-Hydroxytryptamine in premature ejaculation: opportunities for therapeutic intervention. Trends Neurosci. 2007;30:79–84. [PubMed] [Google Scholar]
69. Ramage AG. The role of central 5-hydroxytryptamine (5-HT, serotonin) receptors in the control of micturition. Br. J. Pharmacol. 2006;147(Suppl. 2):S120–31. [PMC free article] [PubMed] [Google Scholar]
2):S120–31. [PMC free article] [PubMed] [Google Scholar]
70. Basu M, Duckett J. The treatment of urinary incontinence with duloxetine. J. Obstet. Gynaecol. 2008;28:166–69. [PubMed] [Google Scholar]
71. Bolte AC, van Geijn HP, Dekker GA. Pathophysiology of preeclampsia and the role of serotonin. Eur. J. Obstet. Gynecol. Reprod. Biol. 2001;95:12–21. [PubMed] [Google Scholar]
72. Gupta S, Hanff LM, Visser W, et al. Functional reactivity of 5-HT receptors in human umbilical cord and maternal subcutaneous fat arteries after normotensive or pre-eclamptic pregnancy. J. Hypertens. 2006;24:1345–53. [PubMed] [Google Scholar]
73. Dawes SD. Can SSRIs reduce the risk of preeclampsia in pregnant, depressed patients? Med. Hypotheses. 2005;64:33–36. [PubMed] [Google Scholar]
74. Salkeld E, Ferris LE, Juurlink DN. The risk of postpartum hemorrhage with selective serotonin reuptake inhibitors and other antidepressants. J. Clin. Psychopharmacol. 2008;28:230–34. [PubMed] [Google Scholar]
75.![]() Chambers CD, Hernandez-Diaz S, Van Marter LJ, et al. Selective serotonin-reuptake inhibitors and risk of persistent pulmonary hypertension of the newborn. N. Engl. J. Med. 2006;354:579–87. [PubMed] [Google Scholar]
Chambers CD, Hernandez-Diaz S, Van Marter LJ, et al. Selective serotonin-reuptake inhibitors and risk of persistent pulmonary hypertension of the newborn. N. Engl. J. Med. 2006;354:579–87. [PubMed] [Google Scholar]
76. Minosyan TY, Lu R, Eghbali M, et al. Increased 5-HT contractile response in late pregnant rat myometrium is associated with a higher density of 5-HT2A receptors. J. Physiol. 2007;581:91–97. [PMC free article] [PubMed] [Google Scholar]
77. Oropeza MV, Ponce Monter H, Reynoso Isla M, Campos MG. The ovarian and cervical regions of the rat uterus display a different contractile response to serotonin and prostaglandin F2αI. The estrous cycle. Life Sci. 2000;66:PL345–51. [PubMed] [Google Scholar]
78. Jeffrey JJ, Ehlich LS, Roswit WT. Serotonin: an inducer of collagenase in myometrial smooth muscle cells. J. Cell Physiol. 1991;146:399–406. [PubMed] [Google Scholar]
79. Ruhe HG, Mason NS, Schene AH. Mood is indirectly related to serotonin, norepinephrine and dopamine levels in humans: a meta-analysis of monoamine depletion studies. Mol. Psychiatry. 2007;12:331–59. [PubMed] [Google Scholar]
Mol. Psychiatry. 2007;12:331–59. [PubMed] [Google Scholar]
80. Weintraub M, Hasday JD, Mushlin AI, Lockwood DH. A double-blind clinical trial in weight control. Use of fenfluramine and phentermine alone and in combination. Arch. Intern. Med. 1984;144:1143–48. [PubMed] [Google Scholar]
81. Connolly HM, Crary JL, McGoon MD, et al. Valvular heart disease associated with fenfluraminephentermine. N. Engl. J. Med. 1997;337:581–88. [PubMed] [Google Scholar]
82. Fitzgerald LW, Burn TC, Brown BS, et al. Possible role of valvular serotonin 5-HT2B receptors in the cardiopathy associated with fenfluramine. Mol. Pharmacol. 2000;57:75–81. [PubMed] [Google Scholar]
83. O’Connor KA, Roth BL. Finding new tricks for old drugs: an efficient route for public-sector drug discovery. Nat. Rev. Drug Discov. 2005;4:1005–14. [PubMed] [Google Scholar]
84. Droogmans S, Cosyns B, D’Haenen H, et al. Possible association between 3,4-methylenedioxymethamphetamine abuse and valvular heart disease.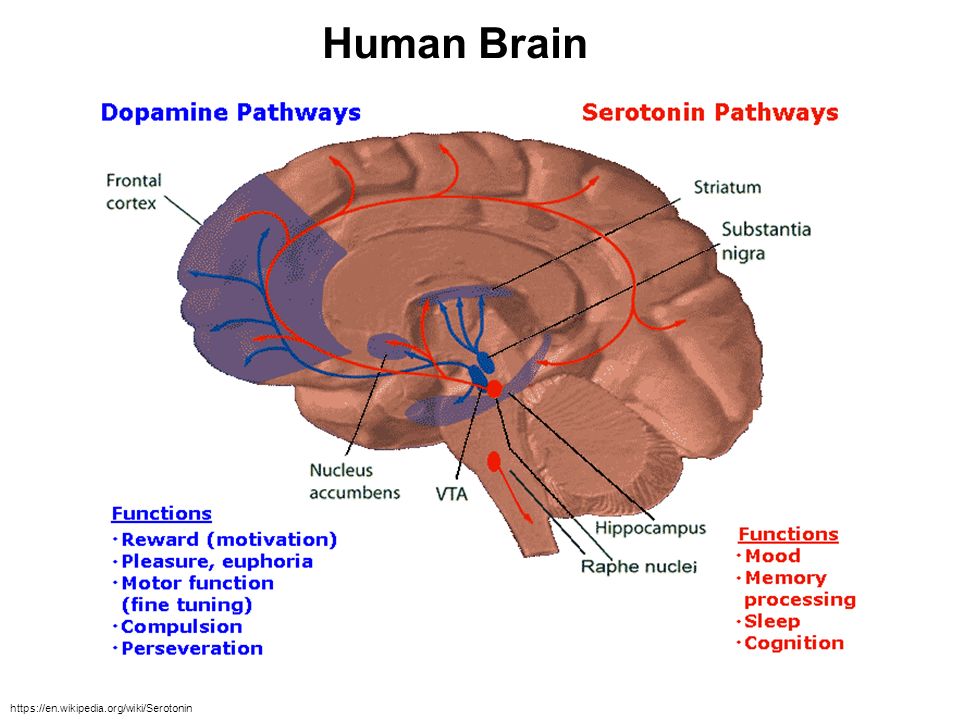 Am. J. Cardiol. 2007;100:1442–45. [PubMed] [Google Scholar]
Am. J. Cardiol. 2007;100:1442–45. [PubMed] [Google Scholar]
85. Schade R, Andersohn F, Suissa S, et al. Dopamine agonists and the risk of cardiac-valve regurgitation. N. Engl. J. Med. 2007;356:29–38. [PubMed] [Google Scholar]
86. Zanettini R, Antonini A, Gatto G, et al. Valvular heart disease and the use of dopamine agonists for Parkinson’s disease. N. Engl. J. Med. 2007;356:39–46. [PubMed] [Google Scholar]
Functions, normal range, side effects, and more
Serotonin has a wide variety of functions in the human body. People sometimes call it the “happy” chemical because it contributes to well-being and happiness.
The scientific name for serotonin is 5-hydroxytryptamine (5-HT). It is a natural chemical mainly present in the brain, bowels, and blood platelets.
Serotonin is a neurotransmitter, and some also consider it a hormone. The body uses it to send messages between nerve cells.
Serotonin appears to affect mood, emotions, appetite, and digestion.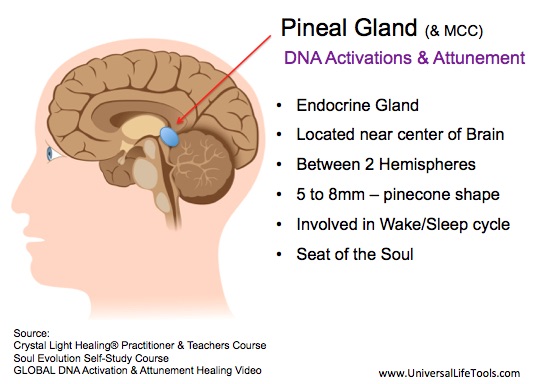 As the precursor for melatonin, it helps regulate sleep-wake cycles and the body clock.
As the precursor for melatonin, it helps regulate sleep-wake cycles and the body clock.
Many investigations have looked at serotonin and its effects, but there is much to learn.
In this article, we look at the role of serotonin in the body, drugs that affect serotonin, side effects and symptoms of serotonin deficiency, and how to boost serotonin levels.
Serotonin results from tryptophan, a component of proteins, combining with tryptophan hydroxylase, a chemical reactor. Together, they form 5-HT, or serotonin.
The intestines and the brain produce serotonin. It is also present in blood platelets and plays a role in the central nervous system (CNS).
Serotonin occurs throughout the body and appears to influence a range of physical and psychological functions.
The substance is also present in animals, plants, and fungi. For this reason, some people have looked at food as a possible source of serotonin.
However, serotonin cannot cross the blood-brain barrier. This means that the brain must produce any serotonin it needs. Treatments for depression and other mental health issues do not supply serotonin directly but trigger reactions that can boost serotonin levels in the brain.
This means that the brain must produce any serotonin it needs. Treatments for depression and other mental health issues do not supply serotonin directly but trigger reactions that can boost serotonin levels in the brain.
That said, research suggests that sources of serotonin in other areas, such as the digestive system, may work independently of serotonin in the brain. This could have implications for treating and preventing various physiological conditions, such as bone degeneration.
As a neurotransmitter, serotonin relays signals between nerve cells and regulates their intensity.
Scientists believe it plays a role in mood and the CNS and affects functions throughout the body. It may have an effect on:
- bone metabolism
- cardiovascular health
- eye health
- blood clotting
- neurological disorders
However, the relationship between serotonin and many bodily functions remains unclear.
Scientists do not precisely know what causes depression, but one theory is that it stems from an imbalance of neurotransmitters in the body.
Doctors commonly prescribe selective serotonin reuptake inhibitors (SSRIs) as antidepressants. Fluoxetine (Prozac) is one example.
Typically, the body reabsorbs a neurotransmitter after transmitting its neural impulse. SSRIs stop the body from reabsorbing serotonin, leaving higher serotonin levels to circulate.
Many people find SSRIs help relieve their symptoms, although the link between depression and serotonin remains unclear.
One problem for researchers is that, while they can measure serotonin levels in the bloodstream, they cannot measure its levels in the brain.
As a result, they do not know whether serotonin levels in the bloodstream reflect those in the brain. It is also impossible to know whether SSRIs can affect the brain.
Nevertheless, while scientists have not yet proven the serotonin theory of depression, SSRIs do appear to help many people.
Other disorders
Apart from depression, doctors may prescribe drugs that regulate serotonin levels to treat several other disorders, including:
- bipolar disorder
- post-traumatic stress disorder
- bulimia
- obsessive-compulsive disorder
- panic disorders
- migraine
As with depression, some scientists have questioned whether serotonin is the only factor affecting these conditions.
Learn more about how to stop a panic attack.
Medical professionals can measure a person’s serotonin blood levels but cannot measure serotonin levels in the brain.
Typically, treatments aim to stabilize serotonin levels between 101 and 283 nanograms per milliliter.
According to the National Institute on Drug Abuse (NIDA), low serotonin levels can lead to memory problems and a low mood.
These are symptoms of depression, although scientists have not confirmed a link between low serotonin levels and depression.
NIDA notes that when people use certain recreational drugs, such as MDMA (ecstasy), the body releases large amounts of serotonin.
This can lead to serotonin depletion, low mood, confusion, and other symptoms lasting several days.
Animal studies have suggested that these drugs may damage the nerves that contain serotonin, with possible long lasting adverse effects.
Learn more about serotonin deficiency.
Medications, foods, and other natural remedies can alter serotonin levels.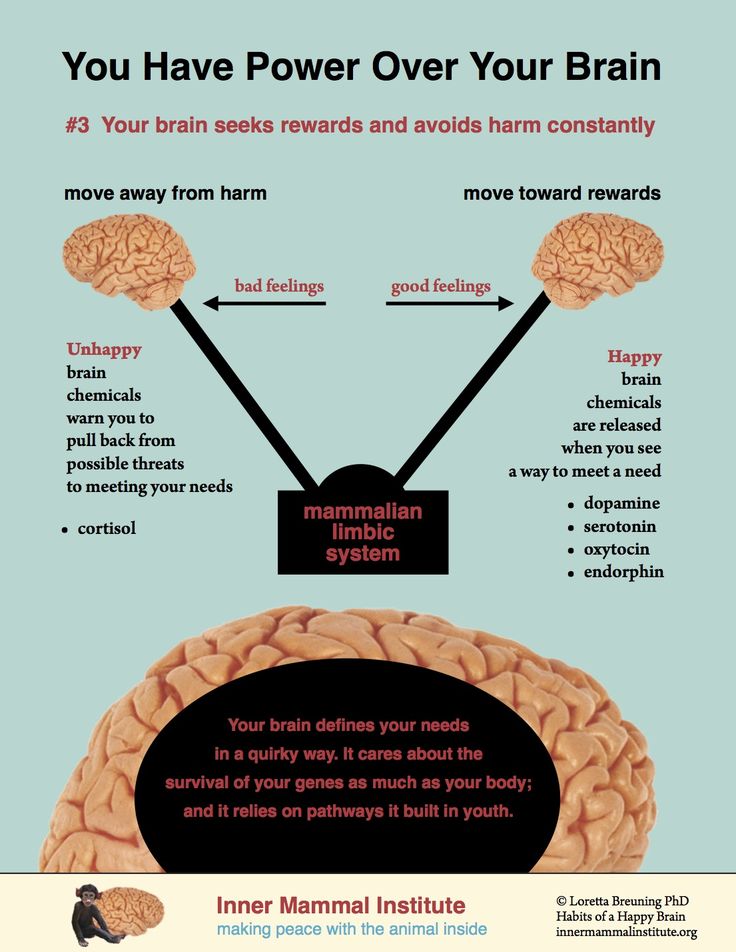
SSRIs increase serotonin levels by preventing the body from reabsorbing serotonin neurotransmitters. Serotonin levels remain high in the brain, and this may elevate a person’s mood.
SSRIs that have approval from the Food and Drug Administration (FDA) for treating depression include:
- citalopram (Celexa)
- escitalopram (Lexapro)
- Prozac
- paroxetine (Paxil, Pexeva)
- sertraline (Zoloft)
- vilazodone (Viibryd)
Learn more about SSRIs and other antidepressants.
Adverse effects of SSRIs
SSRIs have some side effects, but these usually improve with time.
They include:
- nausea and vomiting
- restlessness and agitation
- indigestion
- diarrhea or constipation
- weight or appetite loss
- increased sweating
- dizziness
- blurred vision
- sleepiness or insomnia
- feeling shaky
- dry mouth
- headache
- low sex drive
- erectile dysfunction
- suicidal thoughts
Serotonin syndrome
Rarely, taking too much of a drug that boosts serotonin levels or combining two such drugs can lead to serotonin syndrome. This is a potentially life threatening condition that may require emergency treatment.
This is a potentially life threatening condition that may require emergency treatment.
Learn more about serotonin syndrome.
SSRIs and suicide
A person who uses SSRIs for depression will not experience the benefits at once. At first, symptoms may worsen before improving. Anyone experiencing thoughts of suicide should seek help at once.
The FDA requires all antidepressants to carry a black box warning about the danger of suicide during the initial stages of treatment, especially in people under 25 years.
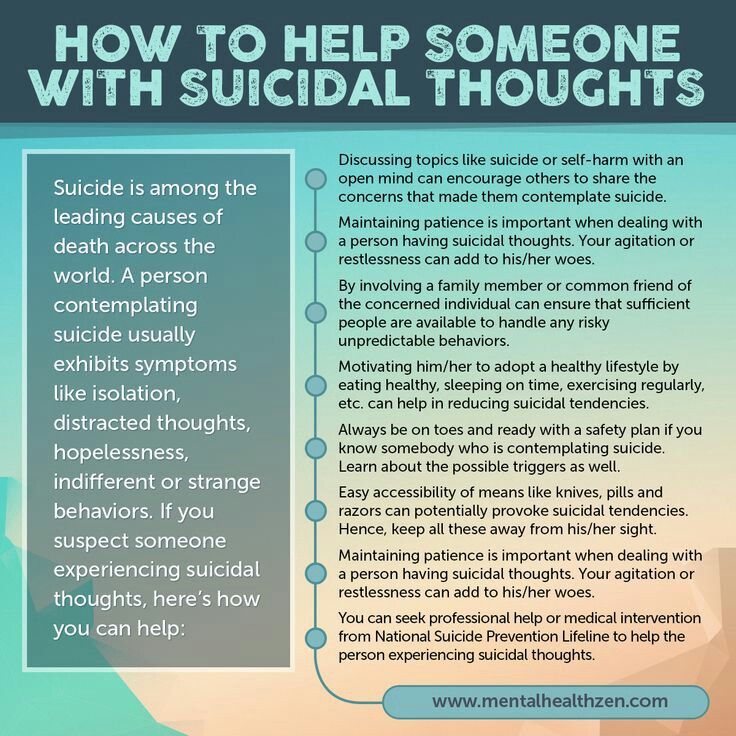
Suicide prevention
If you know someone at immediate risk of self-harm, suicide, or hurting another person:
- Ask the tough question: “Are you considering suicide?”
- Listen to the person without judgment.
- Call 911 or the local emergency number, or text TALK to 741741 to communicate with a trained crisis counselor.
- Stay with the person until professional help arrives.
- Try to remove any weapons, medications, or other potentially harmful objects.
If you or someone you know is having thoughts of suicide, a prevention hotline can help. The 988 Suicide and Crisis Lifeline is available 24 hours a day at 988. During a crisis, people who are hard of hearing can use their preferred relay service or dial 711 then 988.
Click here for more links and local resources.
Therapy
Doctors commonly recommend a combination of medication and therapy to treat depression.
Several forms of psychotherapy can help manage symptoms of depression and other mental health conditions.
Cognitive behavioral therapy and interpersonal therapy are the two main types.
Learn more about psychotherapy.
Natural remedies
Some natural remedies may help boost serotonin levels in the body. These include:
- practicing meditation
- having light therapy, already in use for seasonal affective disorder
- doing regular exercise
- consuming foods that are high in tryptophans
Though there is not enough evidence to confirm that these methods can boost serotonin levels, in moderation, they are unlikely to be harmful.
Learn more about how to boost serotonin levels.
Foods
Tryptophan is an amino acid that occurs in some foods. Some research links a higher intake of dietary tryptophan to more positive mood scores, possibly because tryptophan bolsters serotonin levels.
Foods that may contain tryptophan include:
- turkey
- eggs
- cheese
- soy products
- salmon
The body uses tryptophan to create serotonin. Eating foods that contain tryptophan may help support this process, but it does not mean that the body will necessarily absorb and use it.
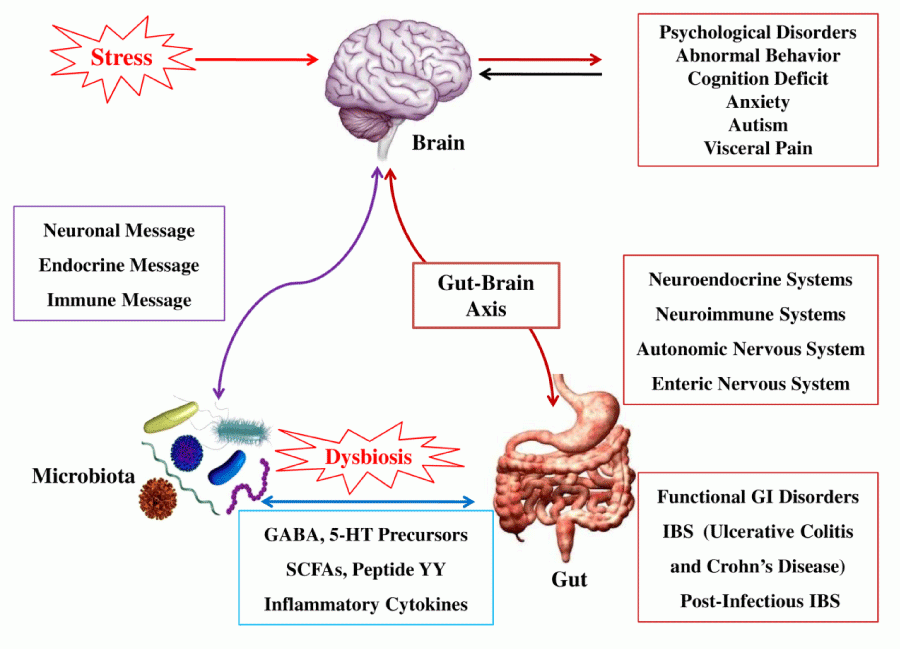
There is a growing interest among scientists in the idea that gut microbiota might influence the nervous system — including behavior, mood, and thinking — through a link known as the gut-brain axis.
If so, serotonin could provide a crucial link. This suggests that diet and gut microbiota could play a role in preventing and treating conditions such as anxiety and depression.
However, more research is necessary to confirm whether this is possible.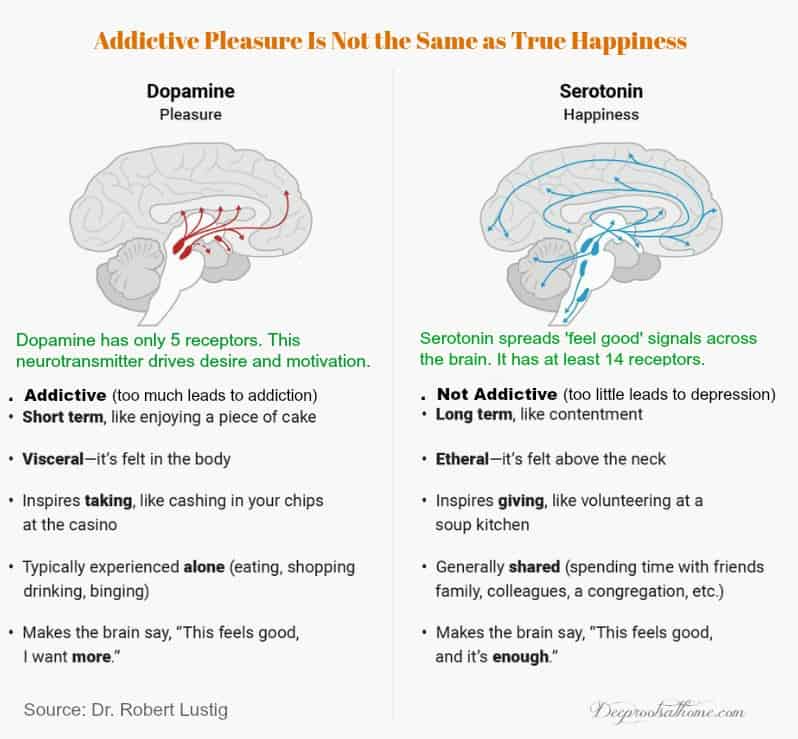
Learn more about foods that may help boost serotonin levels.
Serotonin, or the “happy” chemical, appears to play a role in various physical and psychological functions.
SSRIs are drugs that affect serotonin levels. They can help manage the symptoms of depression, although experts are still unsure exactly how it works.
Anyone considering taking a drug or supplement that affects serotonin levels should consult their doctor first to ensure it is safe for them to use.
Read the article in Spanish.
Serotonin: what is it, in simple terms
Serotonin affects almost our entire body. It acts not only in the familiar role of the “hormone of happiness”, but also plays many other important roles. Therefore, it is worth monitoring its level and helping yourself to maintain it in the normal range.
Anastasia Afanasyeva, psychiatrist, psychotherapist, clinical director of the service for the selection of psychologists Alter
Advertising on RBC www. adv.rbc.ru
adv.rbc.ru
What is serotonin
Serotonin is one of the neurotransmitters of the nervous system, molecules that act as a "negotiator" or "communicator": they move between neurons (nerve cells), helping to transmit a signal from one of them to another. Serotonin is produced from the essential amino acid tryptophan, which is found in protein foods of animal and plant origin.
Although we are accustomed to associate serotonin with mood and emotions, that is, with the activity of our nervous system, only 5% of the body's serotonin is produced in the brain. It is these 5% that affect our emotional state. The lion's share of this substance (80–95%) is actually synthesized and stored in the cells of the gastrointestinal tract. Serotonin is also produced in certain skin cells, platelets, and cells in a number of other organs. All this mass of serotonin is also in action: it turns out that this hormone performs many more important functions.
What Serotonin Does
Serotonin helps reduce depression and regulate anxiety and anxiety. But, in addition, it affects our entire body: it helps us sleep, eat, digest food and even heal wounds - not only mental, but also quite physical. (I want to say: what would we do without him!)
But, in addition, it affects our entire body: it helps us sleep, eat, digest food and even heal wounds - not only mental, but also quite physical. (I want to say: what would we do without him!)
Here is how this substance is involved in various processes and functions of the body.
Mood
It is believed that serotonin regulates the intensity of anxiety, happiness and mood background. If there is enough serotonin, then we are in a consistently good mood, and vice versa: depressive states are associated with low levels of serotonin.
Sleep
Serotonin stimulates the parts of the brain that control the sleep-wake cycle, and it is he who "decides" whether you are sleeping or not.
Blood clotting
Serotonin, which platelets collect from the blood, helps heal wounds by causing tiny arteries to narrow and may help normal blood clotting.
Strong bones
This hormone plays an important role in bone health. Too high levels of serotonin in bone tissue can lead to osteoporosis.
Too high levels of serotonin in bone tissue can lead to osteoporosis.
Intestinal regulation
As we have already said, most of the serotonin in our body is found in the stomach and intestines. This substance helps control the motility and functions of the gastrointestinal tract.
Help with food poisoning
Serotonin is one of the causes of nausea and indigestion as a reaction to toxic substances that enter the body with food. When poisoned, the production of serotonin in the intestines increases and diarrhea occurs in order to quickly displace harmful or unpleasant food. Also, serotonin increases in the blood - this stimulates the part of the brain that triggers the nausea mechanism.
Sexual function
Low levels of serotonin are associated with increased libido. And vice versa: if there is a lot of serotonin, libido decreases. And the truth is: why make extra gestures, if we feel good anyway?
© Shutterstock
Why serotonin is called the "hormone of happiness"
Serotonin regulates our mood.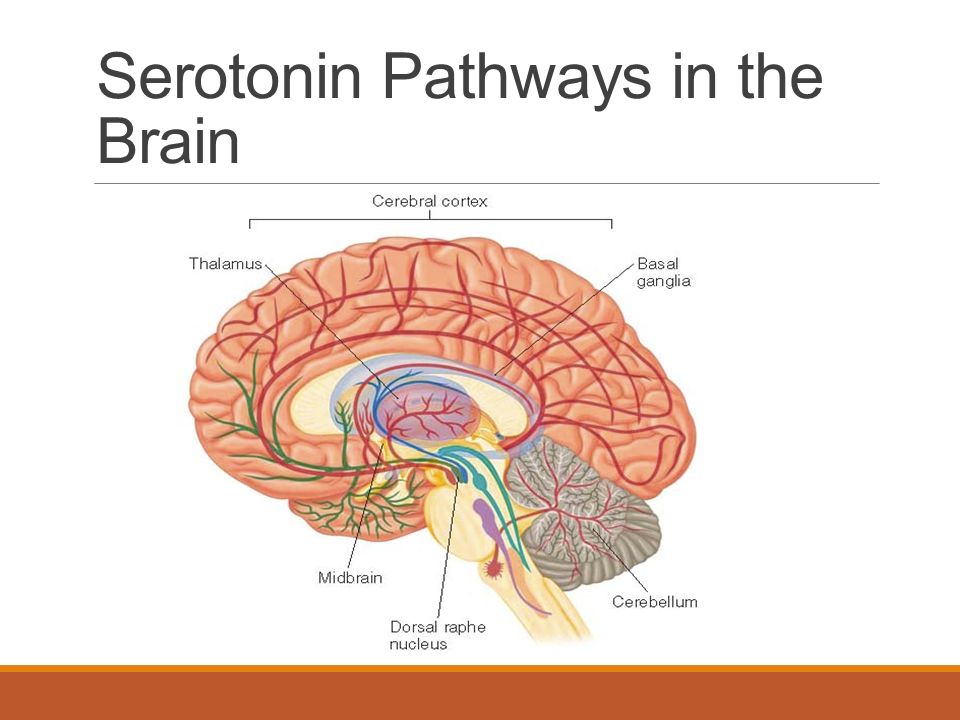 When there is enough serotonin, we feel:
When there is enough serotonin, we feel:
Since the 1980s, drugs have been actively used to treat depression, which increase the level of serotonin, blocking its natural breakdown. This group of antidepressants is called SSRIs - selective serotonin reuptake inhibitors. It was on the basis of studies of these drugs that the assumption was born that an increase in the amount of serotonin relieves the symptoms of depression and anxiety. However, this conclusion is now being questioned. The problem is that serotonin levels can only be measured in the blood, not in the brain. So, it cannot be argued that SSRIs really affect the level of this substance in the nervous system.
Still, there is a connection between the amount of serotonin and our emotional state. So, in 2016, a study was conducted on mice, in the nerve cells of which there were no receptors that inhibit the synthesis of serotonin. Accordingly, more serotonin got into their brain. The study showed that these mice experienced less anxiety and depression, and were better able to tolerate external stress [1].![]()
Thus, today scientists are inclined to believe that serotonin does not so much increase the intensity and duration of positive emotions as it reduces our susceptibility to negative ones.
How to increase serotonin without drugs
Good old healthy lifestyle will help to raise the level of serotonin. All those basic ways to prevent depression and keep yourself in good shape, which every article on these topics recommends, work precisely because they contribute to the production of serotonin in the body.
Sunshine
The sun helps increase serotonin production. Spend more time outdoors, go for walks. In autumn and winter, the lack of sun can be compensated, if not by a trip to warm islands, then by light therapy - treatment with special lamps.
Exercise
Light running, walking, swimming, cycling, cardio can all help restore serotonin levels. It is important that the load is regular, but at the same time moderate and pleasant.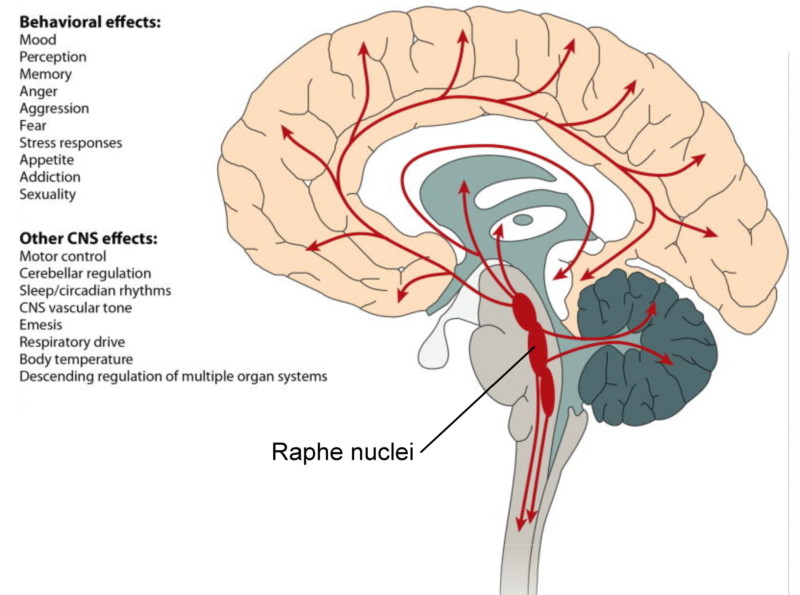 A good habit is to use at least part of the way to work or a lunch break as an opportunity to walk (and at the same time “recharge” with ultraviolet light, if the weather allows).
A good habit is to use at least part of the way to work or a lunch break as an opportunity to walk (and at the same time “recharge” with ultraviolet light, if the weather allows).
Meditation
Practicing meditation can reduce stress and promote a positive outlook on life. This, in turn, also helps keep serotonin levels high.
Normalization of sleep
Regular adequate sleep is necessary in order to stabilize the serotonin system.
Diet
Can serotonin be found in foods? Let's talk about this in more detail.
© Shutterstock
What is serotonin
Contrary to popular belief, serotonin is not found in food - it is synthesized only in our body. Food contains tryptophan, the same amino acid that is then converted into serotonin.
In order to produce more of this hormone in the body, you need to include the following foods in your diet:
- eggs;
- hard cheeses;
- turkey;
- nuts;
- salmon;
- tofu;
- pineapple.
It can be assumed that if we eat less foods containing tryptophan, this will lead to a decrease in mood. However, studies show that if you remove tryptophan from the diet, the emotional background decreases only in those people who have already had depressive episodes before. For those who did not suffer from depression in the past, a decrease in dietary tryptophan intake was not significantly affected. This seems to be due to the fact that in people with depressive disorders, the very process of serotonin metabolism changes.
As we have already found out, serotonin helps to stabilize mood, and if you actively increase it in all of the above ways, this does not mean that you will feel euphoria: your emotional background will simply become more even, you will be less prone to anxiety and more stable to stress.
© Shutterstock
Why high serotonin is dangerous
Even if you eat a lot of cheese and nuts, you don't have to worry that serotonin will exceed the norm (although you shouldn't overeat anyway).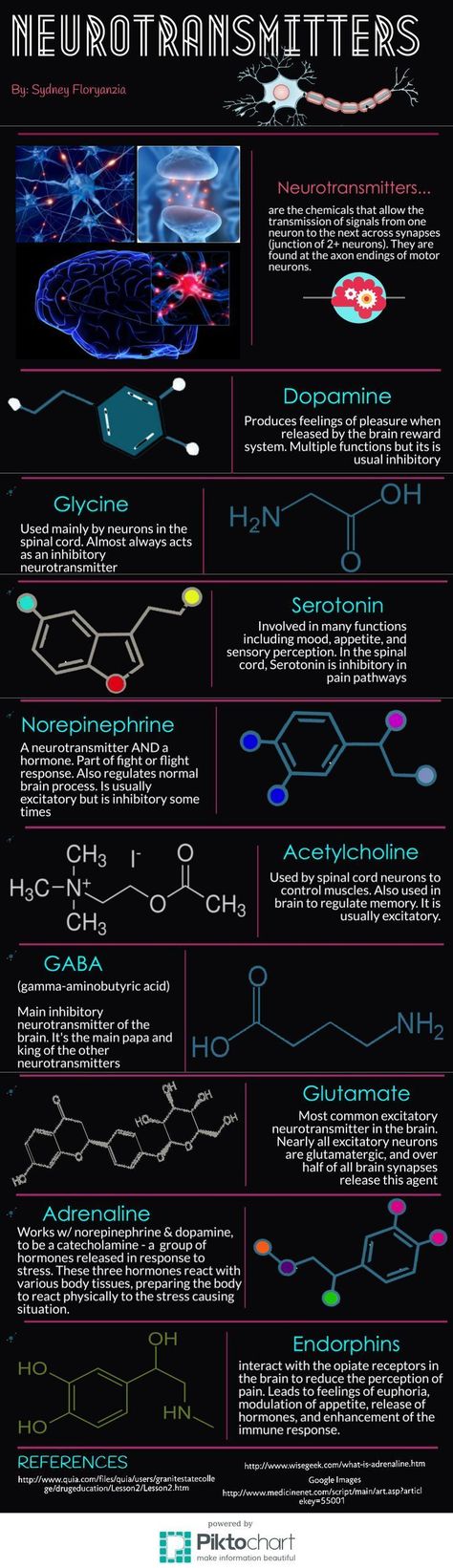 An excess of this hormone in the body can occur, for example, due to improper intake of certain medications (most often antidepressants) or their combination with drugs. This abruptly starts the "factory" for the production of serotonin in our body at full capacity - the hormone is produced too much, which can cause serotonin syndrome, in fact - "poisoning" with serotonin.
An excess of this hormone in the body can occur, for example, due to improper intake of certain medications (most often antidepressants) or their combination with drugs. This abruptly starts the "factory" for the production of serotonin in our body at full capacity - the hormone is produced too much, which can cause serotonin syndrome, in fact - "poisoning" with serotonin.
Serotonin syndrome most often develops within two hours after the first dose of the drug that provoked it, and disappears after 6-24 hours after administration. This condition may be accompanied by symptoms such as diarrhea, tachycardia, anxiety, restlessness, tremor. The temperature can rise to 41 degrees, some may experience confusion.
The most important thing in serotonin syndrome is timely and correct assistance: due to incorrect treatment of symptoms (for example, fever), serious complications can occur, even death. Therefore, the doctor needs to tell about all the drugs that the patient took. Treatment involves the abolition of drugs that increase the production of serotonin, and the use of symptomatic agents.
Too high levels of serotonin can also be a sign of serious neuroendocrine disorders. Therefore, if the amount of serotonin in the blood is significantly higher than normal (which is 101-283 nanograms / ml), you should definitely consult a doctor.
Tags: hormones , proper nutrition , psychology
How to train your brain to produce hormones of happiness.
What can we advise you?Contents of the page
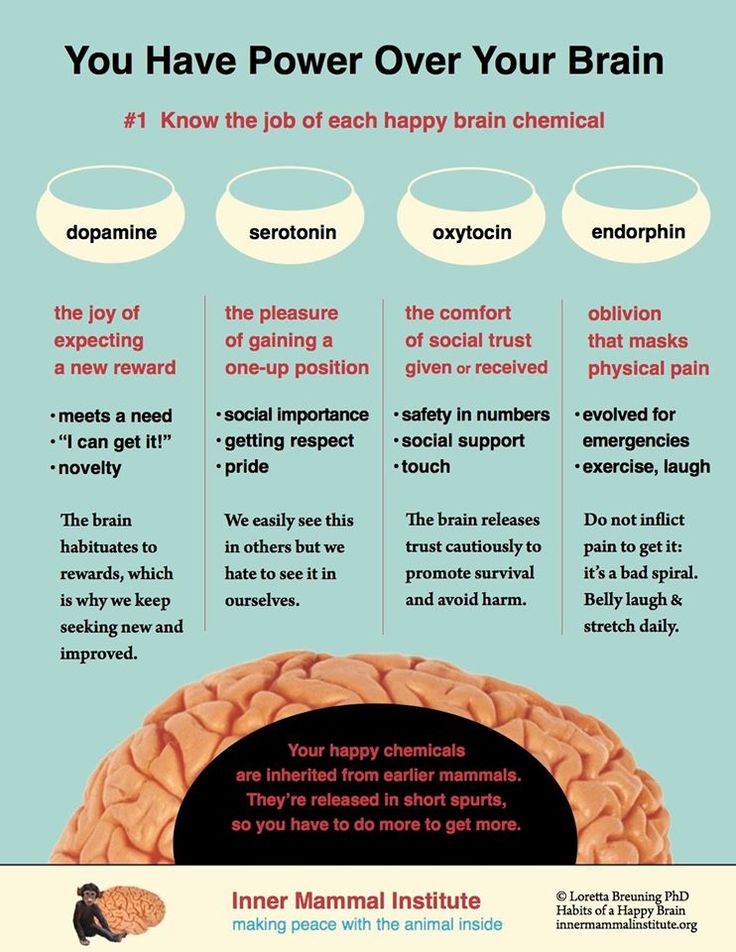
Hormones are responsible for our mood, self-confidence and satisfaction with others. Dopamine, oxytocin, serotonin, and endorphins are produced in the brain and are known as “happiness hormones.” They can also be called “success hormones” because, in addition to good mood, they give us optimism, energy, increase concentration, encourage communication with people and thus stimulate drive, leadership and confidence in ourselves and our work (work). ).
Dopamine, oxytocin, serotonin, and endorphins are produced in the brain and are known as “happiness hormones.” They can also be called “success hormones” because, in addition to good mood, they give us optimism, energy, increase concentration, encourage communication with people and thus stimulate drive, leadership and confidence in ourselves and our work (work). ).
It is under their influence that a personal psychotype is formed, motivation for active actions appears, or fear of defeat arises.
Let's briefly understand what's what and how to train your brain to produce hormones of happiness.
- Endorphins are perhaps the most famous hormone of happiness and satisfaction. Endorphins are elevated when we engage in rewarding activities such as eating, exercising, or having sex. These hormones are released during short, pleasurable, satisfying activities. Company parties, picnics, and other ways to bring employees together increase the level of endorphins in team members, helping to establish close relationships, improve employee morale, and strengthen corporate traditions.

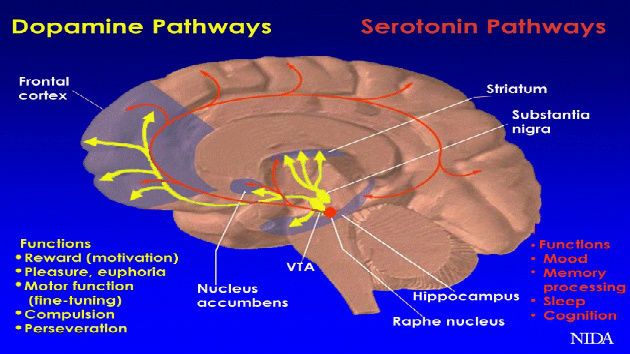
- Dopamine is a hormone of happiness, anticipation and pleasure from achieving a goal after a lot of effort has been put into it. This is the icing on the cake of your achievements. When you get a great result, the feeling of dopamine happiness will encourage you to repeat this achievement over and over again.
Dopamine is an important part of the brain's reward system. Its production is associated with pleasant sensations, learning, memory and motor functions. Dopamine helps us remember information and is a key factor in the process of associative learning. Curiosity, impulsivity, and risk-taking behavior are also heavily dependent on dopamine production. With a lack of this hormone, a person may experience lack of motivation, boredom, bad mood, anxiety or depression.
Oxytocin and serotonin can be called “hormones of vanity and selflessness”.
- Oxytocin is one of the most important hormones responsible for social interaction, human behavior in society .
 It is produced in the hypothalamus during hugs, kisses, and social interactions. It is also called the molecule of love, because thanks to him, a mother brings up her child. Oxytocin activates the release of prolactin, without which breastfeeding is impossible. No less important is oxytocin during childbirth - it stimulates uterine contractions. Oxytocin helps build trust, empathy (empathy), and bonding in relationships. This chemical stimulates the manifestation of selfless kindness and caring.
It is produced in the hypothalamus during hugs, kisses, and social interactions. It is also called the molecule of love, because thanks to him, a mother brings up her child. Oxytocin activates the release of prolactin, without which breastfeeding is impossible. No less important is oxytocin during childbirth - it stimulates uterine contractions. Oxytocin helps build trust, empathy (empathy), and bonding in relationships. This chemical stimulates the manifestation of selfless kindness and caring. - Serotonin is able to influence our well-being, increase self-esteem, help to concentrate and relax . Achievements, recognition, praise, any increase in status stimulate the production of serotonin and encourage further advancement.
Serotonin is involved in many processes: appetite control, sleep regulation, mood regulation, pain regulation, and sexual arousal.
It will not be possible to create a universal recipe for happiness, but it is quite possible to learn how to control your hormonal balance.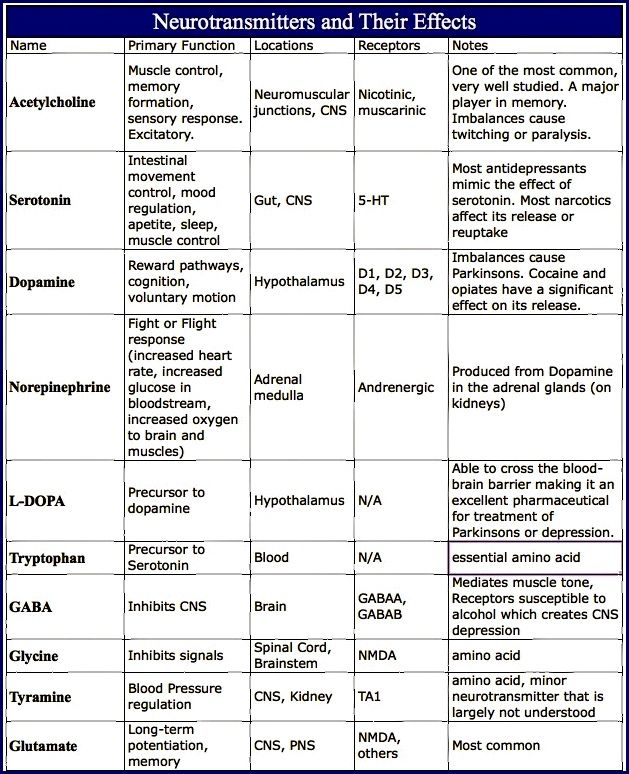
Hormones can influence our behaviour, but our behavior can also influence our hormones. In other words, the hormonal profile can be changed.
Is it possible to learn how to manage your hormones? Yes, you can.
- Start with diet. Two important things are sugar and alcohol. They disrupt the balance between estrogen and testosterone in women, increase fatigue and cortisol levels.
- Physical activity. Exercising for about 30 minutes a day will help reduce cortisol levels and overall feelings of stress.
- Set realistic goals and raise the bar every day . The pleasure of completing tasks will increase the production of dopamine.
- The best way to increase serotonin will be meditation, new experiences, hugs and laughter !
- Watch your posture and posture, do not send verbal stress signals to your body like: "I'm afraid, I'm nervous, I'm overwhelmed, it's unreal, just some kind of horror .
 ..". Such messages, being converted into a chemical signal, lead to an increase in the level of cortisol, a decrease in the level of dopamine and endorphins, testosterone. The result is an insecure posture, stuttering speech, a failed speech or a fiasco in negotiations.
..". Such messages, being converted into a chemical signal, lead to an increase in the level of cortisol, a decrease in the level of dopamine and endorphins, testosterone. The result is an insecure posture, stuttering speech, a failed speech or a fiasco in negotiations.
And the key to these changes is the art of managing your emotions. Manage stress - manage the situation!
Categories
See also:
Is it possible to get pregnant with a diagnosis of PCOS? Part 1
06/23/2022
Polycystic ovary syndrome (PCOS) is indeed one of the most common causes of female endocrine infertility. But this absolutely does not mean that there is no chance of having a desired pregnancy at all.
Azoospemia. The reasons.
 Strategy for a healthy baby.
Strategy for a healthy baby. 05/29/2022
Sad statistics say that the male factor is the cause of not getting pregnant in up to 40% of cases. One possible cause is azoospermia, which occurs in one in a hundred men.
Menopause Digest. Part 1. How to know about approaching menopause?
04/08/2021
How to find out about approaching menopause, what age of menopause is considered normal, the causes of premature and early menopause, whether it is possible to delay the onset of menopause - read in our first issue of the menopause digest. Anna Vitalievna Shargorodskaya, endocrinologist-gynecologist of our clinic, tells.
Symptoms of impaired testosterone levels
07/06/2021
Friends, in our first frequent article on testosterone, we talked about its role in a woman's life.