What is the autistic spectrum scale
Autism Spectrum Rating Scales - TSLAT
Overview
The Autism Spectrum Rating Scales (ASRS; Goldstein & Naglieri, 2009) is a norm-referenced, nationally-standardized, multi-informant rating scale that helps to identify symptoms and behaviors associated with the full range of autism spectrum disorder (ASD). It can guide diagnostic decisions, treatment planning, and monitoring response to intervention. The ASRS is available in two forms- one for preschoolers and the other for elementary and high school students. It includes eight subscales, called Treatment Scales: Peer Socialization, Adult Socialization, Social/Emotional Reciprocity, Atypical Language, Stereotypy, Behavioral Rigidity, Sensory Sensitivity, Attention/Self-Regulation (ages 6-18 only), and Attention (ages 2-5 only). Using a 5-point Likert response scale, parents and teachers indicate how often they observe specific behaviors in a child being evaluated. Up to five raters can complete the ASRS for a child, and a comparative report can be generated to compare results.
There is also a 15-item Short Form that offers a convenient alternative for screening large groups or monitoring treatment. The ASRS can be scored manually or using software. The ASRS has also been updated to provide a DSM-5 scoring option (DSM-IV-TR scoring is also available). In addition, an option for obtaining ASRS scores for children and adolescents with limited or no speech is described in a technical manual available online (Goldstein & Naglieri, 2012). The ASRS is also available in Spanish.
Age: 2 years to 18 years
Time to Administer: 20 minutes (5 minutes for short form)
Method of Administration: Individually administered, norm-referenced, multi-informant rating scale to identify symptoms of ASD; completed by parent and teacher group administration of a 15-item short form is also available.
Yields T-scores (M = 50, SD = 10), percentile ranks, classifications, and interpretive guidelines
Subscales: OVERALL COMPOSITE SCORE: ASRS Total Score; DSM-5 Scale
SUBSCALE SCORES: Social/ Communication, Unusual Behaviors, Self-Regulation (6-18 years)
TREATMENT SCALE SCORES: Peer Socialization, Adult Socialization, Social/Emotional Reciprocity, Atypical Language, Stereotypy, Behavioral Rigidity, Sensory Sensitivity, Attention/Self-Regulation (ages 6-18), Attention (ages 2-5)
Screening/Diagnosis: D
Autism Related Research
Li et al.
 (2018)
(2018)Age Range: 6-18 years
Sample Size: 677
Topics Addressed:
Psychometric properties of the ASRS and SRS when used in ID and compare screening accuracy
Outcome:Li et al. (2018)Individuals with intellectual disability (ID) had higher scores on total and all subscale scores on the ASRS than typically developing (TD) peers. Gender and age did not have a significant effect on scores, but group (e.g., ASD, ID, TD) did. Total scores in the ASD group were significantly higher than in the ID group. ASRS showed good discriminant validity, suggesting that social communication deficit is the primary characteristic of ASD that can be used to identify ASD in ID. Excellent psychometric properties, both in ASD and in ASD + ID group. However, the cut-off point should be slightly higher (e.g., 67) when used to discriminate ASD from ID.
Conclusion: the ASRS can help identify ASD within persons with ID, and increasing the cut-off point is recommended when using measure in this manner.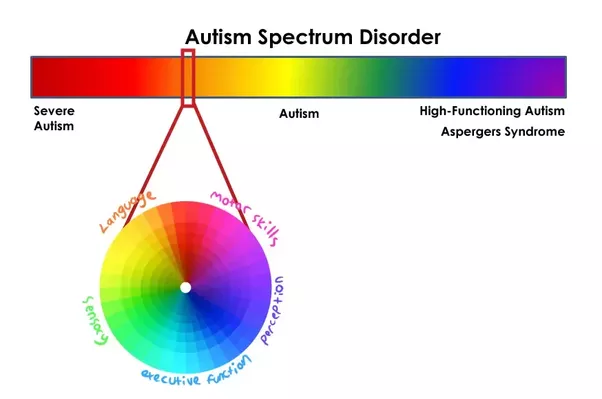
Autism Spectrum Rating Scale (ASRS)
What is the Autism Spectrum Rating Scale (ASRS)?
The Autism Spectrum Rating Scale (ASRS) is used to help identify symptoms, behaviors, and associated features of Autism Spectrum Disorder in children and adolescents aged 2-18. It is an important part of the diagnosis process because it provides a valid, reliable, and carefully crafted tool for assessment to help prevent over and under diagnosis.
What is the Autism Spectrum Rating Scale (ASRS) Used For?
The Autism Spectrum Rating Scale (ASRS) is used to quantify observations of a child that are associated with autism. This a valid and reliable tool that can be used to help guide diagnostic decisions, treatment planning, ongoing monitoring of response to intervention, and program evaluation.
How is the Autism Spectrum Rating Scale (ASRS) Administered?
The Autism Spectrum Rating Scale (ASRS) is based on reports filled out by the child’s parent(s) and teachers and/or childcare providers. The rater has to have known the child for at least four weeks and should be able to answer questions about the child’s behaviors that have occurred during the four weeks prior to the rating.
The rater has to have known the child for at least four weeks and should be able to answer questions about the child’s behaviors that have occurred during the four weeks prior to the rating.
What is Being Reported?
The parent(s) and teacher and/or childcare provider reports include 70 items related to behaviors associated with Autism, Asperger’s Disorder, and Pervasive Developmental Disorder-Not Otherwise Specified (PDD-NOS). The results of the items produce a total score which is further interpreted by three scales: ASRS Scales, DSM-5 Scale, and Treatment Scales.
What are the ASRS Scales?
The ASRS scales interpret a child’s social/communication skills and unusual behaviors.
Social/communication skills interpret whether a child has the verbal and non-verbal skills to appropriately initiate, engage in, and maintain social contact.
Unusual behaviors interpret whether a child has the ability to tolerate changes in routine, if they have purposeless or stereotypical behaviors, and if they overreact to certain sensory stimuli.
What is the DSM-5 Scale?
The DSM-5 scale compares the child’s symptoms to the diagnostic criteria for Autism Spectrum Disorder directly from the DSM-5. The Diagnostic and Statistical Manual of Mental Disorders (DSM–5) is the tool published by the American Psychiatric Association (APA) which is used to diagnose mental disorders.
What are the Treatment Scales?
The treatment scales interpret a child’s peer socialization, adult socialization, social/emotional reciprocity, atypical language, stereotypy, behavioral rigidity, sensory sensitivity, attention/self-regulation.
Peer socialization is a child’s willingness and capacity to successfully engage in activities that develop and maintain relationships with other children.
Adult socialization is a child’s willingness and capacity to successfully engage in activities that develop and maintain relationships with adults.
Social/emotional reciprocity is a child’s ability to provide an appropriate emotional response to another person in a social situation.
Atypical language is a child’s ability to utilize spoken communication in a structured and conventional way.
Stereotypy is the extent to which a child engages in purposeless and repetitive behaviors.
Behavioral rigidity is a child’s ability to tolerate changes in their environment, routines, activities, or behaviors.
Sensory sensitivity is a child’s level of tolerance for experiences through touch, sound, vision, smell, or taste.
Attention/self-regulation is a child’s ability to appropriately focus their attention on one thing while ignoring other things.
Autism Diagnosis – nakedheart.online
ASD Diagnostic Tools
Currently, there are no medical tests that confirm or refute the presence of autism in a child. Diagnostics is carried out in the form of interviews with parents and other people involved in child care. His behavior is being monitored. Structured diagnostic tests are used to evaluate behavior.
The most common screening in Russia is M-CHAT-R (The Modified Checklist for Autism in Toddlers, Revised) - a modified version of the autism screening questionnaire. It consists of 20 questions that parents need to answer and allows you to determine the possible risk of autism in a child aged 1.5–2.5 years. The test questions take a few minutes to answer.
It consists of 20 questions that parents need to answer and allows you to determine the possible risk of autism in a child aged 1.5–2.5 years. The test questions take a few minutes to answer.
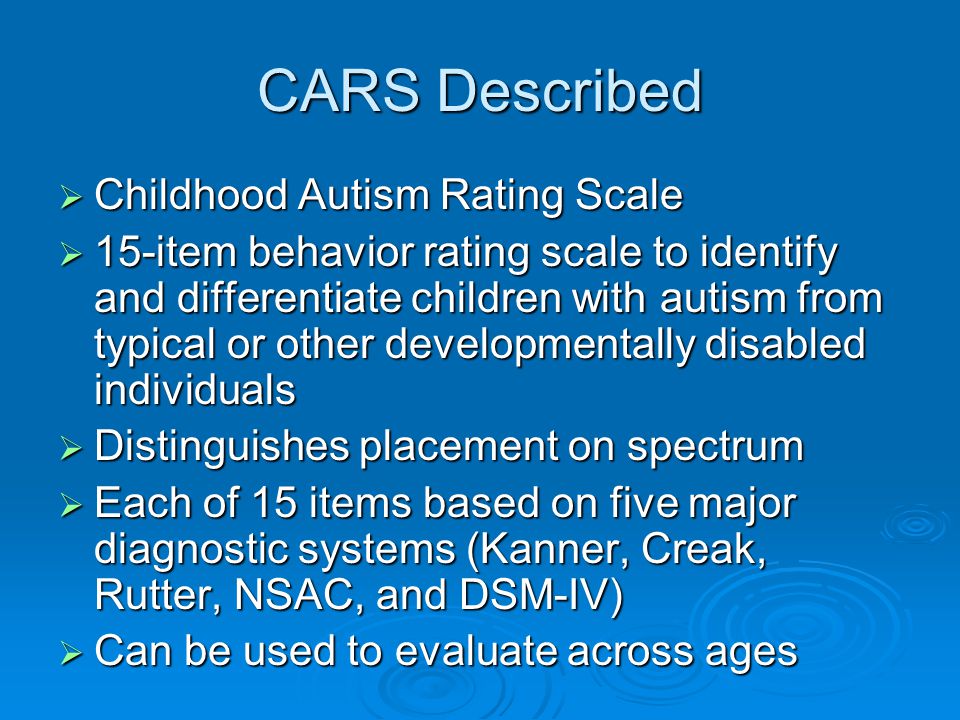
A more complex tool is CARS (Childhood Autism Rating Scale) - a rating scale for autism in a child. Typically, CARS is used by a specialist in combination with clinical observation, interaction with the child, and a structured interview with caring adults. In Russia, the translation of the previous version of CARS, available on the Internet, is widely used. This scale applies to children aged two to four years. An updated and improved version is available in English - CARS2. It has two versions: CARS2-ST for children under six years old and CARS2-HF for children over six years old with higher communication skills. The tool helps to assess the severity of impairments in different areas of a child's development and draw a conclusion about whether we really observe signs of ASD in a particular child. It should be noted that CARS is not a diagnostic tool either.
It should be noted that CARS is not a diagnostic tool either.
ADOS and ADI-R are the most reliable diagnostic tools for ASD and are often used together. These scales are available in Russian. They are used by professionals for evaluation and diagnosis.
Criteria for diagnosing ASD
Turning to a specialist for a diagnosis, you must first make sure that he owns the modern diagnostic tools listed above. In our country, for the official statement of any diagnosis, ICD-10 is used - the International Classification of Diseases of the 10th revision. Its criteria and descriptive base also make it possible to diagnose ASD. Using all of the above tools makes this task easier, and the diagnosis more accurate and reliable.
Parents have the right to insist on a correct diagnosis. If the conclusion obtained is in doubt, it is necessary to seek the opinions of other specialists with sufficient clinical experience and professional qualifications for this.
Currently, the current criteria for diagnosing ASD are based on the DSM-5 classification. It is the most up-to-date guide for diagnosing autism among professionals around the world. These criteria will also be reflected in ICD-11 when it enters into force in 2022.
It is the most up-to-date guide for diagnosing autism among professionals around the world. These criteria will also be reflected in ICD-11 when it enters into force in 2022.
DSM-5 provides the most up-to-date and comprehensive toolkit for understanding a child with autism's behavior, symptoms, and basic levels of severity for autism spectrum disorders.
In DSM-5, all components of autism spectrum disorders are divided into two main sections (“autism dyad”): (A) lack of social communication and social interaction and (B) limited, repetitive patterns of behavior, interests or activities.
The first part of the RAS (A) dyad consists of the following subsections:
- A1 - problems initiating and maintaining social interaction
- A2 - problems with nonverbal communication
- A3 - problems understanding social situations and social relationships
The second part of the RAS dyad (B) consists of the following subsections:
- B1 - atypical speech, movement and play
- B2 - rituals and resistance to change
- B3 - over-obsession with objects or interests
- B4 - atypical sensory behavior
At the same time, the diagnosis of "autism spectrum disorder" should be made only in cases where the manifestations of the "dyad of autism" affect daily behavior: if a person finds it difficult to interact with family, peers and other people, develop skills, including speech, be flexible and switch from one task to another. If there are no difficulties in everyday life, then there is no violation. The point of making a diagnosis should not be to put a label on a person, but to help him cope with the difficulties caused by the violation, help him realize his potential and live in society together with other people.
If there are no difficulties in everyday life, then there is no violation. The point of making a diagnosis should not be to put a label on a person, but to help him cope with the difficulties caused by the violation, help him realize his potential and live in society together with other people.
Associated problems
Most often, autism manifests itself in the form of difficulties with social communication and limited repetitive behavior. But, in addition to this, the child may have poorly developed speech and other cognitive impairments may be observed. Also, the main symptoms can be accompanied by completely different health problems. They make diagnosing autism even more difficult. For example, autism is often associated with disorders such as epilepsy, genetic syndromes, gastrointestinal disorders, ADHD. That is, they coexist side by side, but do not cause each other (in the scientific literature, this is called comorbidity).
Another important aspect is that behavioral disorders, manifestations of aggression, self-aggression and other forms of unwanted behavior are not related to the diagnostic criteria for ASD. In most cases, these manifestations are due to the insufficient development of the child's communication, as well as the peculiarities of his environment. Understanding children's communication needs and an appropriate program of assistance can help reduce problem behaviors and develop academic and social skills in a less restrictive environment.
In most cases, these manifestations are due to the insufficient development of the child's communication, as well as the peculiarities of his environment. Understanding children's communication needs and an appropriate program of assistance can help reduce problem behaviors and develop academic and social skills in a less restrictive environment.
UDC 616.89-007.12-053.2
Evaluation of the severity of autistic spectrum disorders in children with general developmental development Bizyukevich S. AT.
Supervisor - Candidate of Medical Sciences, Associate Professor Karpyuk V.A.
Grodno State Medical University, Belarus, 230009, Grodno, st. Gorky, 80
[email protected] - Bizyukevich Svetlana Viktorovna
Resume. Autism spectrum disorders are a topical issue in child psychiatry.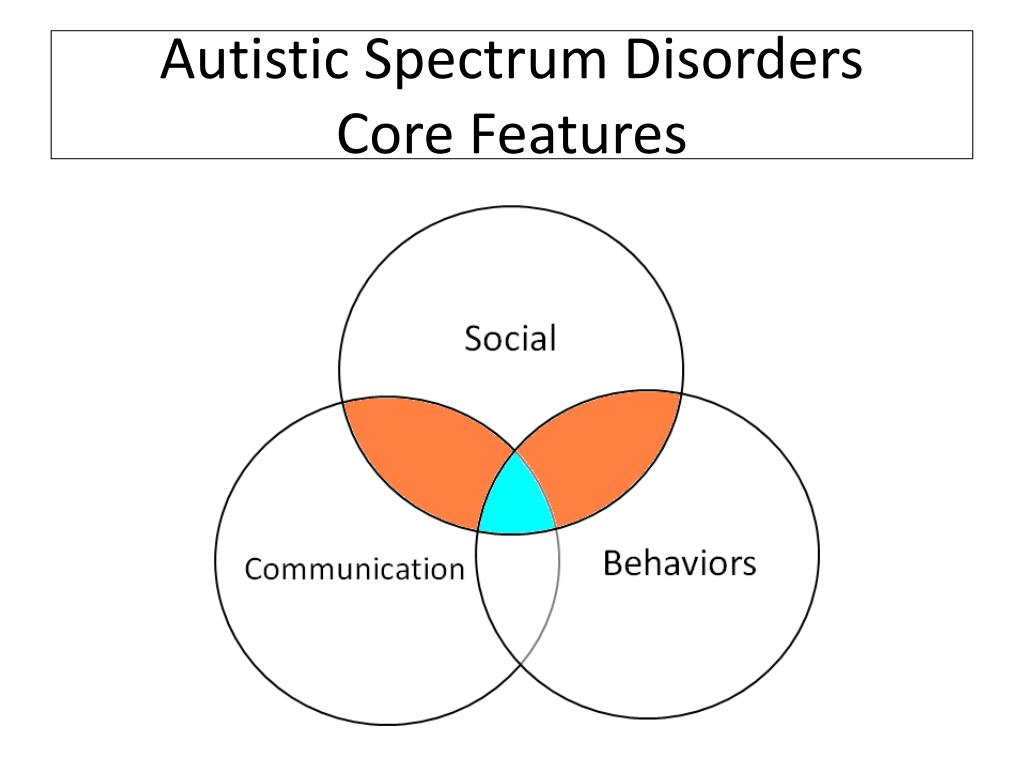 There is an acute problem of the earliest diagnosis of autism spectrum disorders, differential diagnosis, dynamic monitoring of children with autism spectrum disorders (ASD). The purpose of this article is to quantify the severity of autism spectrum disorders using the Childhood Autism Rating Scale (CARS). The results of applying the rating scale to assess the severity of ASD are presented. The scale showed high efficiency for quantitative assessment of the severity of autism spectrum disorders, which may allow individualizing the approach to the use of treatment and correction measures in children with ASD.
There is an acute problem of the earliest diagnosis of autism spectrum disorders, differential diagnosis, dynamic monitoring of children with autism spectrum disorders (ASD). The purpose of this article is to quantify the severity of autism spectrum disorders using the Childhood Autism Rating Scale (CARS). The results of applying the rating scale to assess the severity of ASD are presented. The scale showed high efficiency for quantitative assessment of the severity of autism spectrum disorders, which may allow individualizing the approach to the use of treatment and correction measures in children with ASD.
Key words: autism spectrum disorders, diagnostics, rating scale, children.
ASSESSMENT OF THE SEVERITY OF AUTISM SPECTRUM DISORDERS IN CHILDREN WITH GENERAL DEVELOPMENTAL DISORDERS Biziukevich S.V.
Scientific advisor — associate professor Karpiuk V.A., Candidate of Medicine
Grodno state medical university, Belarus, 230009, Grodno, Gorkogo St., 80.
Summary. Autism spectrum disorder is a challenging problem in pediatric psychiatry. An urgent task is the earliest diagnosis of autism spectrum disorders, differential diagnosis, dynamic monitoring of children with autism spectrum disorders (ASD). The aim of this study is to quantify the severity of autism spectrum disorders using the rating scale for the assessment of childhood autism (CARS). The results of the application of the rating scale to assess the severity of the ASD are presented. The scale revealed a high efficiency of the severity of autism spectrum disorders for the quantitative assessment, which make it possible to individualize the approach to the application of therapeutic and rehabilitative measures in children with ASD. Key words: autism spectrum disorders, diagnosis, rating scale, children.
Introduction. The problem of autism spectrum disorders is one of the most urgent in modern psychiatry, due to the steady increase in the number of children with autism spectrum disorders. Due to ambiguous approaches to the assessment of autistic disorders in different countries, the prevalence of autism is different and ranges from 4 to 26 cases per 10,000 children. The average male to female ratio in autism spectrum disorders (ASD) is 4.3:1 [3].
Due to ambiguous approaches to the assessment of autistic disorders in different countries, the prevalence of autism is different and ranges from 4 to 26 cases per 10,000 children. The average male to female ratio in autism spectrum disorders (ASD) is 4.3:1 [3].
In the Republic of Belarus from 2005 to 2012, the total number of children under the supervision of psychiatrists due to general developmental disorders, including autism spectrum disorders (ASD), increased by 2.8 times (from 251 to 699 cases) [1].
Autism Spectrum Disorders are developmental disorders characterized by marked and pervasive deficits in social interaction and communication, as well as limited interests and repetitive activities. The etiology and pathogenesis of ASD is not fully understood. Have
place different hypotheses on the etiology of autism spectrum disorders. It should be borne in mind that the existing hypotheses are not mutually exclusive and rather describe violations in different systems. In addition, the cause or causes of ASD may lie in the simultaneous influence of various etiological factors at a certain stage of intrauterine development [2].
In addition, the cause or causes of ASD may lie in the simultaneous influence of various etiological factors at a certain stage of intrauterine development [2].
Pronounced polymorphism
of clinical manifestations of autism spectrum disorders makes it difficult to accurately diagnose certain types of ASD. Based on diagnostic criteria,
presented in the International Classification of Diseases of the Tenth Revision (ICD-10): qualitative deviations in social
interactions, in terms of
sociability, as well as
limited stereotypical interests and behavioral reactions, the severity of signs of autism spectrum disorders is reduced to a subjective interpretation which often leads to overdiagnosis.
The subjectivism of such assessments is especially pronounced in the differential diagnosis of autism spectrum disorders with other mental disorders accompanied by hyperactivity, stereotypical
movements, limited interests, intellectual decline.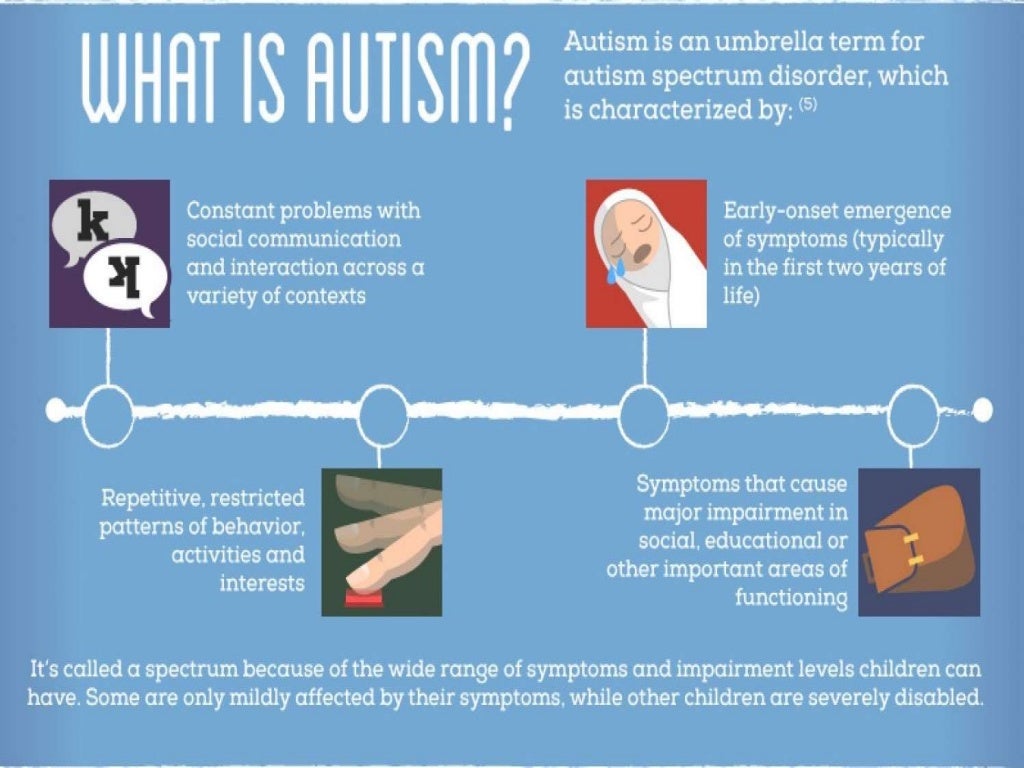
In Russian-speaking countries, including the Republic of Belarus, isolated cases of using diagnostic tools to quantify the severity of signs of autism spectrum disorders are described. This suggests that the diagnosis of the severity of signs of autism spectrum disorders is not accurate enough.
Thus, in order to develop individual programs of treatment and correction measures for children with autism spectrum disorders, it is important to establish the severity of autism spectrum disorders.
The aim of this work is to evaluate the severity of autistic manifestations in children using the Childhood Autism Rating Scale (CARS).
Method. The study was carried out with the participation of 37 children who underwent inpatient examination and treatment in the children's department of the GOCC "Psychiatry-Narcology" for the period from January to December 2016. Of these, boys accounted for - 62.2% (23 people), girls - 37.8 % (14 people), aged 3 to 8 years. The study group included patients who, in accordance with the ICD-10 research diagnostic criteria, were diagnosed with "autism spectrum disorders".
To quantify the severity of ASD, an adapted (translation and adaptation of Morozova T.Yu., Dovbnya S.V., 2011) rating scale for assessing childhood autism (CARS) was used. The scale is a standardized tool for assessing the severity of autistic behavior based on clinical observations of the child's behavior. It consists of 15 functional areas. The assessment of individual areas includes 4 degrees - from signs corresponding to age to signs that are very "deviating from the usual".
Results of the study and discussion: The distribution of the examined children by gender and depending on the diagnosis is presented in Table 1.
Table 1. Distribution of children by sex and diagnosis
Diagnosis General Boys Girls
number
Childhood autism (F 84.0) 16 11 5
Atypical autism (F 84.1) 4 3 1
Asperger's syndrome (B 84.5) 4 3 1
Rett's syndrome (B 84.2) 1 0 1
90.3 6 3 3 Hyperactive disorder associated with mental retardation and stereotyped movements (B 84.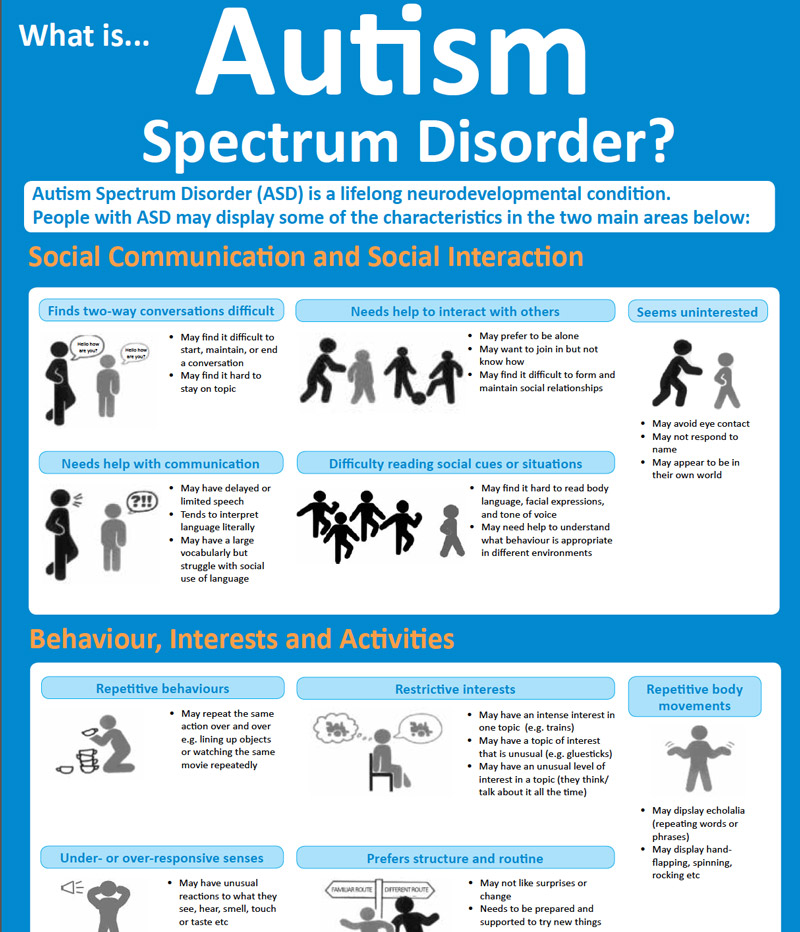 4) 6 3 3
4) 6 3 3
Total: 37 23 14
%. Atypical autism was detected in 10.8% of cases. Of the total number of children, 10.8% have Asperger's syndrome, 1 child (2.7%) has Rett's syndrome.
another disintegrative disorder of childhood, as well as a hyperactive disorder, combined with mental retardation and stereotyped
movements.
The largest number of children with autism spectrum disorders at the age of 5 years - 10 people (27%),
the smallest - at the age of 3 years - 4 people (11%). At the age of 4 years - 9 children (24%), at 6 years old - (22%), 7 years old - 13%, at 8 years old - 3%. The average age of the examined children is 5 years. The peak of the number of surveyed falls on the primary school age - 5-7 years, which reflects the rather late detection of ASD.
The Childhood Autism Rating Scale (CARS) was used to quantify the severity of autism spectrum disorders. The distribution of children depending on the severity of ASD on a scale (CARS) is presented in Table 3.
Table 3. Distribution of children depending on the severity of ASD on a scale _(CARS)_
Diagnosis Total number of children 15-29.5 points - no signs of ASD 30-36.6 points - mild - moderate signs of ASD 37-60 points - severe signs of ASD
Childhood autism (B 84.0) 16 0 4 12
Atypical autism (B 84.1) 4 1 1 2
Asperger's syndrome (B 84.5) 4 2 2 0 Rett syndrome (B0
84.2) 1 0 0 1Disintegrative disorder of childhood (B 84.3) 6 2 2 2
Hyperactive disorder associated with mental retardation and stereotypical movements (B 84.4) 6 0 3 3
Total: 37 5 12 20
severe features of autism spectrum disorder. Children diagnosed with childhood autism, atypical
autism, Rett syndrome in most cases showed severe signs of ASD. In the group of children with hyperactive disorder,
combined with mental retardation and stereotyped movements, severe and moderate signs of autism spectrum disorders were detected to the same extent. Severe signs of autism spectrum disorders in children diagnosed with childhood disintegrative disorder were found only in half of the cases. With Asperger's syndrome, half of the subjects had mild signs of ASD. Moderately pronounced signs of autism spectrum disorders were found in 12 people (29.7%) among all examined children. In 13.5% (5 people) of cases, signs of autism spectrum disorders were not detected or did not reach the value of mild severity.
Severe signs of autism spectrum disorders in children diagnosed with childhood disintegrative disorder were found only in half of the cases. With Asperger's syndrome, half of the subjects had mild signs of ASD. Moderately pronounced signs of autism spectrum disorders were found in 12 people (29.7%) among all examined children. In 13.5% (5 people) of cases, signs of autism spectrum disorders were not detected or did not reach the value of mild severity.
Conclusion. An analysis of the results obtained and their correlation with individual groups of general developmental disorders allows us to draw a number of conclusions. Severe signs of autism spectrum disorders in the vast majority of cases are detected in children diagnosed with "Children's autism", "Atypical autism", but among the examined, in 5 children, significant severity of autistic manifestations was not found, which may indicate the absence of ASD.
Thus, the use of the rating scale (CARS) to assess the severity of autistic manifestations improves the quality of diagnosis verification and differential diagnosis of
ASD with other mental disorders, and also provides an opportunity to develop individual programs for the medical, psychological and pedagogical rehabilitation of patients with ASD.