What causes extreme indecisiveness
Why Am I So Indecisive? 10 Methods to Help You Make Decisions
Indecisiveness has many causes. But you can get better at making decisions, big and small, with practice and time.
Whether it’s a major decision, such as choosing a life partner, or a minor decision, such as what to eat for breakfast, being indecisive can significantly impact your life.
Difficulty in making decisions can be caused by several factors, such as a fear of failure and a lack of confidence or information.
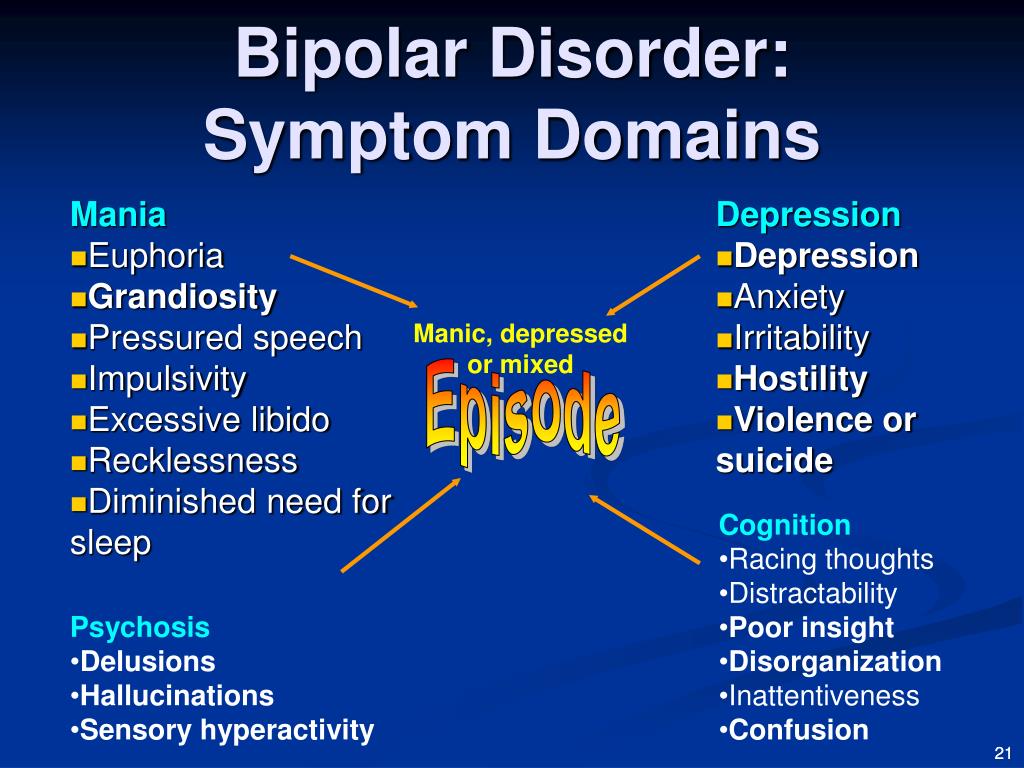
Indecisiveness can also be a symptom of mental health conditions, such as attention deficit hyperactivity disorder (ADHD), depression, and post-traumatic stress disorder (PTSD).
If you experience indecisiveness and making decisions is a constant source of stress and anxiety, you’re not alone. There are effective methods that can help with decision making.
There are many situations that may cause indecisiveness. Here are a few.
Fear of failure
Some people are inherently more hesitant when it comes to making decisions. Indecisiveness certainly can be a learned behavior.
“Those raised in environments where decision making is seen as an opportunity to learn and grow tend to feel more comfortable making choices,” says Dr. Carla Marie Manly, a clinical psychologist. “If, however, decision making becomes associated with making errors or ‘bad choices,’ indecisiveness often results.”
For example, if a parent criticizes a child for making a poor decision, the child will avoid making decisions for fear of being seen as a failure.
“These fears can carry over into adulthood and lead to the use of indecisiveness as an unconscious coping strategy,” Manly explains. “Over time, the stress and anxiety associated with making decisions leads to an avoidance of making both small and large decisions.”
In this paradigm, decision making can have a negative impact on self-worth.
“A ‘good’ decision increases self-worth, and a ‘bad’ decision leads to self-criticism,” Manly says. “In many cases, the fear and anxiety evoked at the mere thought of having to make a decision can be quite paralyzing.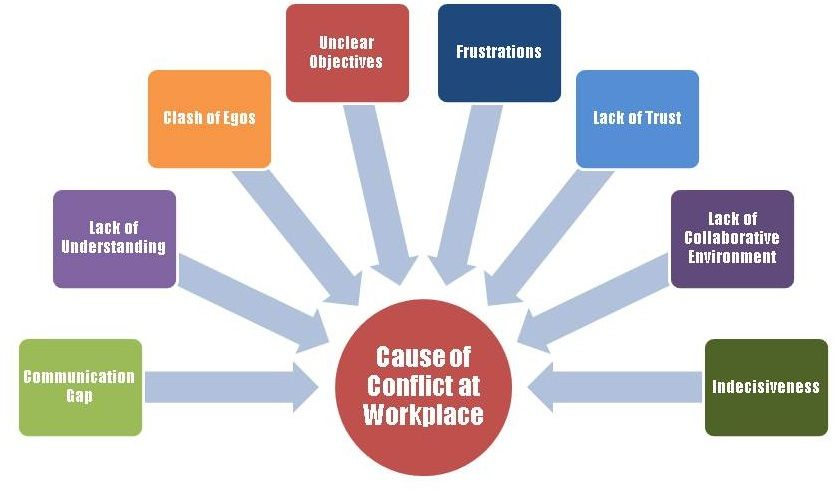 This perpetuates the tendency to default to the relative safety of indecision.”
This perpetuates the tendency to default to the relative safety of indecision.”
Parental influence
The root of your indecision may go back to parental influence.
“If someone has grown up with overbearing parents, they may not have had an opportunity to make decisions independently,” says Haley Perlus, PhD, a sport and performance psychologist. “There was never any chance for the person to fail or succeed by themselves.
“As such, once they’re given the opportunity to make a choice, they’re left looking for someone else to make that choice for them,” Perlus says.
You’re a perfectionist
Perfectionism can lead to numerous health problems, including:
- anxiety
- depression
- burnout
“When someone constantly sees their options categorized as ‘right’ and ‘wrong,’ they may find themselves paralyzed at the thought of accidentally choosing the ‘wrong’ decision,” Perlus says. “This leads to a constant back-and-forth as they struggle to figure out the correct choice. ”
”
You’re a people pleaser
Do you constantly worry about what others think?
“If you’re a people pleaser, you may find yourself continuously struggling internally between choice A (what you want) and choice B (what others want),” Perlus says.
You’ve lost sight of the bigger picture
This goes back to focusing on what matters. Many people get lost in the details and can become overwhelmed.
“Most people strive for some kind of goal, whether professionally, spiritually, or mentally,” Perlus says. “However, when one begins to lose sight of these goals, they often start to lose sight of how they’ll get to the goals as well, leaving them feeling lost and confused when it comes time to decide which direction they should take.”
You lack confidence
Self-confidence is a key component of decision making.
“Perhaps someone does know which direction they should move toward to achieve their goals,” Perlus says. “Yet if they’re insecure, they may be able to choose the decision that’s right for them but struggle with sticking to it.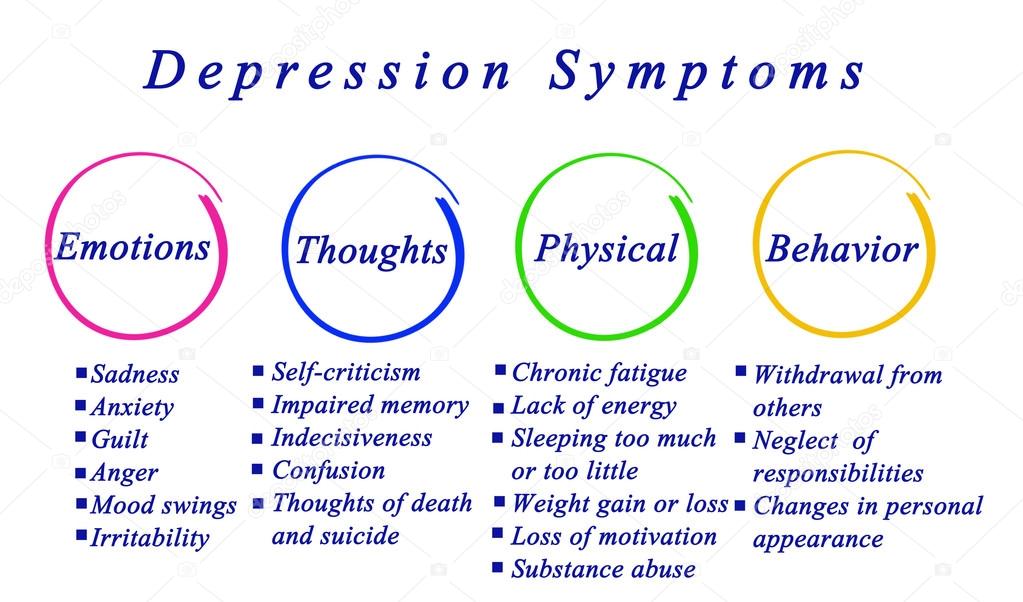 Self-doubt and a lack of confidence could even mean they procrastinate.”
Self-doubt and a lack of confidence could even mean they procrastinate.”
You lack proper knowledge of the subject
This is less internal and more due to circumstances.
“Some people may have the confidence and skills to make solid decisions promptly,” Perlus says. “If this is the case, the problem could lie in the fact that a person simply does not have enough information on the subject they need to decide on.”
You have aboulomania
This is a diagnosable mental disorder.
“Aboulomania is when a person shows signs of pathological indecisiveness,” Perlus explains. “While most people will be indecisive at some point, people with aboulomania are indecisive to the point where it is an obsession and severely affects their daily lives.”
A symptom of other mental health conditions
Indecisiveness can be a symptom of mental health conditions. In fact, indecisiveness is a prevalent symptom of major depressive disorder.
People with ADHD also experience difficulty making decisions due to factors, such as inattention, memory problems, and distractibility.
Other mental health conditions in which indecisiveness can be a symptom are:
- anxiety
- dependent personality disorder
- stress
- childhood trauma
- Alzheimer’s disease
Here are 10 methods to try that may help you become more decisive.
Make decisions for yourself
Asking 10 people about one topic will only confuse you further. Ultimately, if you trust your intuition, you will know what the right decision is.
“Nobody can give you the correct answers on what’s best for you besides yourself,” Perlus says. “Try not to allow others to be the decider between you and your goals.”
Develop your confidence
When you make a choice, trust your intuition that it’s the right decision for yourself.
“Avoid second-guessing. If you have the confidence to trust yourself, you’ll find making and sticking to decisions much easier,” Perlus says.
Let things go
The fear that comes with worrying about making the “wrong” decisions can be paralyzing.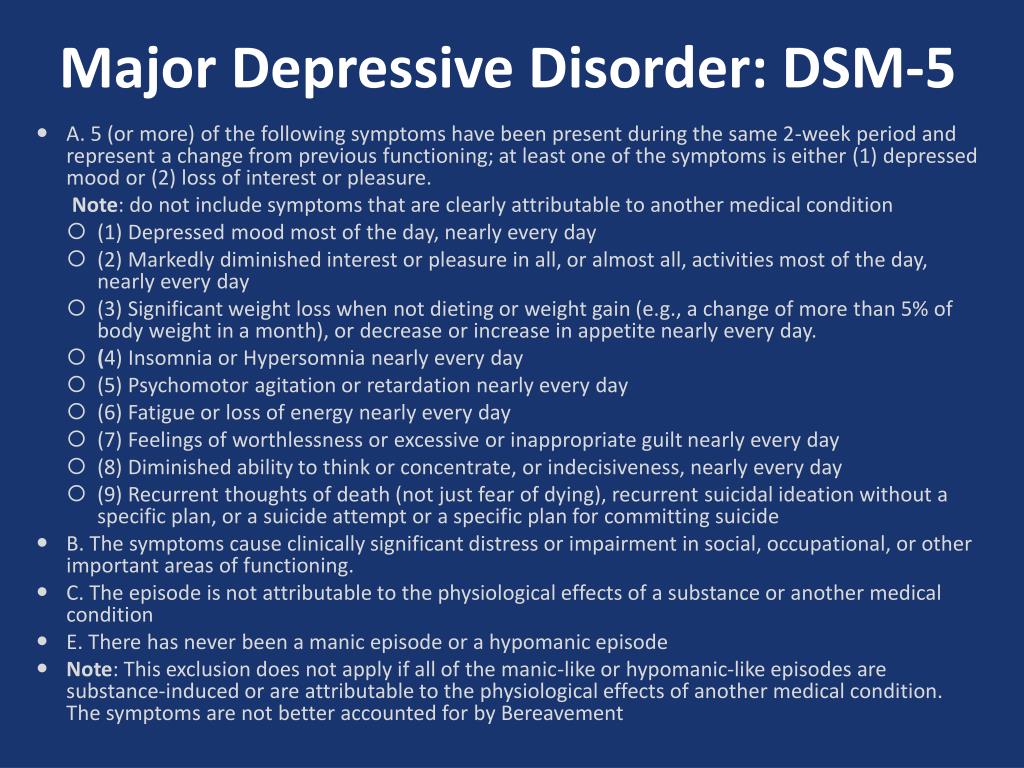
“Try not to worry about mistakes — they’re a part of life. Once you accept that things are not always in your control, making decisions will be much less threatening,” Perlus says.
Choose one person that can act as a sounding board
There will be instances when you’re truly stumped.
“When feeling stuck, ask a supportive friend or partner to weigh in,” Manly says.
Talk it out
The simple act of speaking out loud will help alleviate indecision and internal conflict.
“If it feels right, voice your thoughts out loud to a friend or partner. Decisions can become less confusing and worrisome when we voice our fears and choices out loud,” Manly says.
Narrow it down
If you’re facing a variety of options, take a practical approach.
“Narrow down your selections to three options with a ‘surgical slice.’ Don’t question yourself. Then evaluate the final three options and pick one,” Manly says.
Outline the pros and cons
If you get stuck, draft a simple pro-con list. But the important thing to remember is to write it down. Mentally weighing the pros and cons is simply adding to the indecisiveness.
But the important thing to remember is to write it down. Mentally weighing the pros and cons is simply adding to the indecisiveness.
“Pro-con lists facilitate objective and sound decision making,” Manly says.
Flip a coin
Of course, this method shouldn’t be used for big decisions, such as marriage. But this will work if it’s something as simple as what to order on the menu.
“This simple trick (which I use often) makes the decision for you,” Manly says. “And, there are times when your gut knows what it truly wants when the coin lands the ‘wrong’ way.”
What’s interesting about flipping a coin is that your reaction will actually reveal what you truly want.
Avoid questioning your final decision
Once you’ve made the decision, avoid second-guessing yourself.
“Simply embrace your selection and move forward,” Manly says.
Recognize and celebrate your decisions
Congratulate yourself for every decision you make.
“Practice a kind, validating affirmation,” Manly says. “For example, you might say, ‘I made a great decision. I’m getting better at making choices! This feels good!’ If a negative voice tries to step in to create self-doubt, simply repeat your kind, validating words.”
“For example, you might say, ‘I made a great decision. I’m getting better at making choices! This feels good!’ If a negative voice tries to step in to create self-doubt, simply repeat your kind, validating words.”
Making decisions — big and small — can sometimes be difficult. We’ve all experienced indecisiveness.
Indecisiveness can be caused by several factors, from a fear of failure and lack of information, to conditions, such as aboulomania, depression, and ADHD.
But there are steps you can take to get better at making decisions. If you feel that indecisiveness is affecting your daily life, consider talking with a doctor or mental health professional.
For more resources and support, consider the following:
- National Alliance on Mental Illness (NAMI)
- Mental Health America
- ADHD Resources: Support Groups, Books, Apps, and More
- Support Groups for Adults with ADHD
- CHADD for Adults
- ADHD Coaches Organization
Looking for a therapist but unsure where to start? Psych Central’s How to Find Mental Health Support resource can help.
What Makes People Indecisive? | Psychology Today
I invited my research colleague and friend, Dr. Reza Feyzi Behnagh, assistant professor of education at SUNY, Albany, to write this post. He and I have been collaborating on research, and I thought it was a good opportunity for me to ask him to try his hand at reaching you.
Do you ever find yourself needlessly obsessing over an important decision or avoiding making that decision altogether, by any means? You have a few (often equally attractive) options to choose from, but you obsess over only a handful, exhaustively searching for information about them, through every detail and all its minutia? Do you get easily distracted by other things and lose concentration, but ultimately end up feeling overwhelmed and avoid making that final decision?
The thought of making the final pick among the alternatives daunts us all, filling us with a multitude of “what ifs" in life. For example, “What if I moved to London instead of New York or Chicago and miss out on the cool work opportunities in NYC?”
Researchers have investigated this behavior for the past three decades and termed it indecision or decisional procrastination (see Ferrari, 2010, and Ferrari, Johnson, & McCown, 1995, for personal and professional reads, respectively). Reading this blog post, you might think that this sounds very much like procrastination. You are right, it does!
Reading this blog post, you might think that this sounds very much like procrastination. You are right, it does!
Indecision is a type of chronic procrastination, and it happens when someone has to make an important, often stressful decision, but they feel overwhelmed by the number of choices and end up searching for information and claim they never got around to making the final decision. These individuals are not lazy; they just do everything to avoid making a tough decision. An example of this situation is when one is choosing a suitable job or a mate.
Indecisiveness has been linked to neuroticism in research. Neurotic individuals tend to ponder about anything and everything that could possibly go wrong. Delaying or avoiding decision-making can be thought of as a strategy to delay or avoid the imaginary negative consequences altogether. Alas, this is only a short-term fix for the anxiety of making the decision, kicking the can down the line.
Indecision is no trivial matter, however: The impact of this type of behavior may be much greater when one is trying to make a decision about an important thing in life, like finding the right life partner, a soulmate, or “the one. ” The anxiety about and fear of making the wrong decision could be crippling.
” The anxiety about and fear of making the wrong decision could be crippling.
Indecisive people often go to great lengths to create a situation where they never put their decision-making abilities to test, often claiming they simply forgot (“I never got around to looking into all the choices I had”) and relying on and passing the buck to others to make that final important decision. Ultimately, when the outcome of the decision is a total failure, they have someone else to blame, not themselves, because it was not them who made the decision.
Even if it was them who made the final decision, indecisives find it easier to blame something external to themselves and out of their control for the outcome of the decision. This is a form of what researchers call self-handicapping, where the individual knowingly does something they know will sabotage the outcome, but deep down they think that they can use this as an excuse to explain the impending failure. A reason for this is to maintain one’s self-esteem by blaming other factors out of one’s control. A lot of this maladaptive behavior continues to sound like procrastination, where the ultimate purpose is to feel good now and avoid a stressful situation or decision by putting it off to another time (see Sirois & Pychyl, 2016).
A lot of this maladaptive behavior continues to sound like procrastination, where the ultimate purpose is to feel good now and avoid a stressful situation or decision by putting it off to another time (see Sirois & Pychyl, 2016).
Like behavioral procrastination, indecision leads to anxiety, worry, regret, shame, rumination, and ultimately negatively impacts one’s quality of life, social life, and well-being. Indecision in turn can cause procrastination, but procrastination here serves as a coping mechanism for the problem of making a difficult and important decision, and the pessimism about making a good decision that their future self will not regret. More recently, Dr. Joseph Ferrari and colleagues found that indecisiveness linked to clutter (see other Psychology Today posts) and more specifically to office clutter: People cannot decide which items to keep and which to toss, so they procrastinate in the decision to declutter.
Summary: So what? It’s out there — people are indecisive, and you can find them all over. But you are not alone, because a good 20% of the adult population is indecisive (Ferrari, 2010). We talked about what indecision is, and what it is not, plus its “causes and consequences,” and what you might do to reduce this maladaptive behavior.
But you are not alone, because a good 20% of the adult population is indecisive (Ferrari, 2010). We talked about what indecision is, and what it is not, plus its “causes and consequences,” and what you might do to reduce this maladaptive behavior.
Scholars showed that motivation to change should come from within, and external motivators will only be a Band-Aid and will not make a lasting change in the life of indecisive individuals. However, from all the research, we know that reducing this behavior will lead to a better quality of life and more positive feelings. We will talk about some effective data-based interventions in a future post. Live, based on science.
FGBNU NTsPZ. ‹‹Diagnostic seminar, 1966››
Looks like a teenager, very young. He is dissatisfied that he is called for a conversation, looks embarrassed. She smiles shyly and forcedly, looks away, and twiddles her fingers. He says that he always gets excited when he talks to someone. He reluctantly reports information about himself, sneers at the doctor's questions, sometimes he is impertinent. He puts forward timidity, "painful shyness", "extreme indecision" as the main complaints. Because of them, he cannot communicate with others, because he cannot turn to them with this or that question, everything seems to be doing wrong, there is a feeling of dissatisfaction with himself. Thinks you are weak. All this causes a bad mood, depression, a feeling of annoyance at oneself and resentment towards others. He considers himself physically unattractive, uninteresting and "dim" for others. He suggests that this may be why he constantly feels constrained when dealing with people. Because of his shyness, he lost all initiative. This explains his irritability. Due to indecision, sometimes he cannot think about anything, “thoughts disappear”, and sometimes, on the contrary, he endlessly goes over all his behavior in his mind, thoughts flow in disorder, cannot stop them. This prevents him from doing it.
He puts forward timidity, "painful shyness", "extreme indecision" as the main complaints. Because of them, he cannot communicate with others, because he cannot turn to them with this or that question, everything seems to be doing wrong, there is a feeling of dissatisfaction with himself. Thinks you are weak. All this causes a bad mood, depression, a feeling of annoyance at oneself and resentment towards others. He considers himself physically unattractive, uninteresting and "dim" for others. He suggests that this may be why he constantly feels constrained when dealing with people. Because of his shyness, he lost all initiative. This explains his irritability. Due to indecision, sometimes he cannot think about anything, “thoughts disappear”, and sometimes, on the contrary, he endlessly goes over all his behavior in his mind, thoughts flow in disorder, cannot stop them. This prevents him from doing it.
Considers shyness and indecisiveness as traits of his character, but notes that their manifestations are growing more and more. He believes that he has "sick nerves, as everything irritates him." Cries easily but calms down quickly.
He believes that he has "sick nerves, as everything irritates him." Cries easily but calms down quickly.
He is lonely in the department, mostly depressed, thoughtful. Endlessly reads the same book in English, reads slowly, notes difficulties in reading. It is difficult to focus on the book, because thoughts are busy analyzing their behavior, state. As if another person sits in him and evaluates his actions, when he does something, thinks about something. This does not particularly bother him, but he does not see the point in this, but he cannot get rid of it. Sometimes he watches patients play chess, even sits down to play it himself, but complains to the doctor that he is losing, because he feels embarrassed, thinks about it all the time and can no longer follow the game. He gets frustrated that the patients, who are weaker than he is prepared, beat him, there is a feeling of hostility towards these patients.
Tries to be more alone, because it is difficult for him to do anything in the presence of others. For example, he does not dare to sit on a chair in the presence of others if someone has sat on it before, because he is not sure that the chair is free, but he does not dare to ask about it. He is afraid that he will look pathetic and ridiculous if the chair suddenly turns out to be occupied, and he begins to be embarrassed. Therefore, he is embarrassed to ask the nanny for his towel, which was lost during cleaning, to close the window in the ward in front of everyone, etc. He draws the doctor's attention to the fact that he can never get rid of any obsessive melody, but is not burdened by this.
For example, he does not dare to sit on a chair in the presence of others if someone has sat on it before, because he is not sure that the chair is free, but he does not dare to ask about it. He is afraid that he will look pathetic and ridiculous if the chair suddenly turns out to be occupied, and he begins to be embarrassed. Therefore, he is embarrassed to ask the nanny for his towel, which was lost during cleaning, to close the window in the ward in front of everyone, etc. He draws the doctor's attention to the fact that he can never get rid of any obsessive melody, but is not burdened by this.
Detects some suspicion, hints to the doctor that he sees how the staff is watching his every step, therefore he is often rude in response to their remarks, answers offendedly, with sarcasm, every time he justifies himself by saying that they “deserve it”.
From the first days of hospitalization, he received etaperazine at a dose of up to 72 mg per day. He slept well, noted a decrease in irritability, still felt timid and shy, asked him to be discharged for outpatient treatment, said that he would walk the streets where no one cared about him and he would feel calmer.
With the addition of stelazine up to 30 mg per day, akathisia developed, there were cramps in the muscles of the body, which were not removed, despite the reduction in doses of stelazine to a minimum and the appointment of dinezin. In this regard, stelazin was canceled. Doses of etaperazine were increased to 120 mg per day in combination with chlorpromazine at night at a dose of 50 mg. There were nosebleeds, tremor of the fingers. Subsequently, he remained capricious, showed impatience when he was refused discharge, said that his head was only busy with how he could be discharged. He reluctantly spoke about his condition, tried to embellish it, declared that he himself would try to overcome his illness, that he no longer thought about it, that it entirely depended on his will.
The mood was unstable, changed during the day for no apparent reason. He was relatively calm, saying that he was aware of the need for treatment, since it was difficult for him to be and live among people in such a state, then he began to insist on being discharged, scolding himself for agreeing to go to the hospital. All the time in his thoughts he weighs all the pros and cons, cannot come to a definite conclusion. It happens that at the same time he wants to do something, and you don’t want to call it a “split of desires”.
All the time in his thoughts he weighs all the pros and cons, cannot come to a definite conclusion. It happens that at the same time he wants to do something, and you don’t want to call it a “split of desires”.
His past seems unreal to him, as if everything happened not with him, but with someone else, but he perceives the present as real.
He thinks that he has abilities, maybe even higher than the others, but he can't "give his best", he can't find a "form of contact with people." It is very burdensome. He has the feeling that he is knocked out of his knees, "life goes on by itself, by itself, and he is on his own." Life passes him by, and he can do nothing.
All the time he asks the doctor to talk to him, but during the conversation he is laconic, tries to avoid questions concerning his condition, insists on being discharged. He leaves the doctor without finishing the conversation, but immediately after the doctor says that he wants to talk more. Gently asks what disease he has. He stated several times that the doctor, “like others”, wants to do it. mentally ill, but does not cover this topic, tries to avoid talking about it or begins to deny what has just been said. He says that everyone treats him condescendingly, mockingly. He tends to talk a lot about his condition, making vague conclusions and conclusions. He is completely occupied with himself, almost never remembers his relatives, on a date with his father he is formal, dry, more accessible with his wife, but does not ask about household chores, demands that he be discharged;
He stated several times that the doctor, “like others”, wants to do it. mentally ill, but does not cover this topic, tries to avoid talking about it or begins to deny what has just been said. He says that everyone treats him condescendingly, mockingly. He tends to talk a lot about his condition, making vague conclusions and conclusions. He is completely occupied with himself, almost never remembers his relatives, on a date with his father he is formal, dry, more accessible with his wife, but does not ask about household chores, demands that he be discharged;
In this: the state was discharged by his wife from the hospital 24/24 1964.
Katamnez C and , its father 3/II 1966
Was discharged from the psychiatric hospital named after. P. P. Kashchenko in February 1964. Within a few months after discharge, he received Melleril up to 200 mg per day and indopan 15 mg per day. There was no noticeable improvement in mental state. Having received an academic leave on the certificate of a psychiatrist, I decided to pass all the "tails" during this time, but indecision and shyness interfered: I could not decide to go to college and find out what was needed to pass the exams. He endlessly analyzed his condition, was burdened by the fact that he could not "enter into life." Remained passive, “resigned”. I felt better alone when I didn’t have to “contact” with others.
P. P. Kashchenko in February 1964. Within a few months after discharge, he received Melleril up to 200 mg per day and indopan 15 mg per day. There was no noticeable improvement in mental state. Having received an academic leave on the certificate of a psychiatrist, I decided to pass all the "tails" during this time, but indecision and shyness interfered: I could not decide to go to college and find out what was needed to pass the exams. He endlessly analyzed his condition, was burdened by the fact that he could not "enter into life." Remained passive, “resigned”. I felt better alone when I didn’t have to “contact” with others.
With the help of his father, he was allowed to study at the institute, although not all subjects were passed. Remained passive; when he came to practice, he didn’t do anything there, “looked around”, taking advantage of the fact that no one pays attention to him. At the institute, I felt very lonely, could not get to know anyone, was shy, it was “somehow inconvenient” to talk to students, to ask them about something. He could not make up his mind to take a queue to the teacher for passing tests, he was seized by uncertainty, “lack of will”, he was afraid that he would ask something wrong, they would answer him wrong, etc. “Hang out” in the corridor until all the students dispersed and then "willy-nilly I had to go to the office." Sometimes, without daring to enter the office, he went home without passing the test. Tightened, thus the delivery of tests for the whole year. He found a lot of justifying reasons for his indecision and, as a result, did not go to exams, to consultations on a diploma. Often he reached the door of the teacher's office, but turned back. He was afraid of everything: that he would appear before everyone in a funny way, that they would pay attention to him, that he would again begin to be embarrassed. Sometimes even he could not explain to himself why he did not dare to do something. He was alone all the time, he did not strive to communicate with fellow students, he did not feel the need for this.
He could not make up his mind to take a queue to the teacher for passing tests, he was seized by uncertainty, “lack of will”, he was afraid that he would ask something wrong, they would answer him wrong, etc. “Hang out” in the corridor until all the students dispersed and then "willy-nilly I had to go to the office." Sometimes, without daring to enter the office, he went home without passing the test. Tightened, thus the delivery of tests for the whole year. He found a lot of justifying reasons for his indecision and, as a result, did not go to exams, to consultations on a diploma. Often he reached the door of the teacher's office, but turned back. He was afraid of everything: that he would appear before everyone in a funny way, that they would pay attention to him, that he would again begin to be embarrassed. Sometimes even he could not explain to himself why he did not dare to do something. He was alone all the time, he did not strive to communicate with fellow students, he did not feel the need for this.
From the summer of 1964, for about 4 months, I was troubled by the fear of death. Thoughts came obsessively that he might not be; at the same time, he experienced inner restlessness, vague anxiety, could not get rid of this fear, no matter how hard he tried. The fear of death was so unpleasant, so weighed down on him, that one day at the wedding of relatives he spoke about it, causing bewilderment of the listeners. Gradually, the fear passed, although the thoughts of death remained to this day, but now, he treats them without the same anxiety and anxiety, indifferently.
It was difficult to study, I could not “concentrate”: suddenly I got stuck at one point during the classes, a “jam” set in, during which some separate thoughts flashed through my head, of the most diverse content, but not related to the topic of classes. No matter how hard he tried at such moments to direct his thoughts along the right channel, he did not succeed. Because of this, combined with his "extreme indecision," progress was very slow. He felt dissatisfied with himself, thought about his inferiority, although in the depths of his soul he highly valued himself, did not consider himself incapable. I could not write my diploma on my own, half of it was done by my wife, because all the deadlines were already running out. The diploma project was defended on "4".
He felt dissatisfied with himself, thought about his inferiority, although in the depths of his soul he highly valued himself, did not consider himself incapable. I could not write my diploma on my own, half of it was done by my wife, because all the deadlines were already running out. The diploma project was defended on "4".
After graduating from the institute, together with other graduates, he served in the army as a clerk. The work was quite satisfying, since it did not require the sociability of the initiative. However, he had repeated reprimands for not following the rules prescribed by the charter: he could not make up his mind and force himself to give a report in the form, to salute a senior in rank. At the same time, he was always very embarrassed, he felt uncertainty and fear "that he would not do everything as it should; could not bring myself to do all this, despite the remarks.
Upon his return, for 2.5 months he could not bring himself to force himself to start work on distribution. Under the patronage of his father, he changed several destinations, but did not go anywhere, as he was embarrassed to go to the head of the personnel department, to the head of the enterprise, "did not imagine" what he would say there, how he would behave, "it was inconvenient." Having missed one day, he did not dare to go to the next, for he did not know how to explain his absence the day before. He deceived his family, saying every day that he was leaving for work, while he himself wandered the streets around the institution where he was supposed to work, or translated English books “for himself” in the library.
Under the patronage of his father, he changed several destinations, but did not go anywhere, as he was embarrassed to go to the head of the personnel department, to the head of the enterprise, "did not imagine" what he would say there, how he would behave, "it was inconvenient." Having missed one day, he did not dare to go to the next, for he did not know how to explain his absence the day before. He deceived his family, saying every day that he was leaving for work, while he himself wandered the streets around the institution where he was supposed to work, or translated English books “for himself” in the library.
With the help of his father, in the fall of 1965 he began working in a design workshop. Works very slowly, cannot overcome his indecision and awkwardness. He does not dare to ask the boss about anything, he is embarrassed to do something in front of everyone, for example, to get up and go for glue. Constantly insecure. Even if he does something, he sits and is silent, doing nothing else, until the leader himself comes up to him and asks. All this greatly delays his work, makes everything much slower than others. Once, for two whole days, I did nothing at work, as the boss was busy, but he himself did not dare to take the initiative and start work without pushing. Everyone at work, according to the patient, talks about his "overexpressed uncertainty." He himself calls it “absolute lack of will”, since he cannot force himself to do anything. “Goes with the flow”, scolds himself all the time, analyzes, “digs”. At these moments, it seems to “split in two” - on the one hand, he believes that something needs to be done, and on the other hand, he cannot force himself, he is looking for justifying reasons.
All this greatly delays his work, makes everything much slower than others. Once, for two whole days, I did nothing at work, as the boss was busy, but he himself did not dare to take the initiative and start work without pushing. Everyone at work, according to the patient, talks about his "overexpressed uncertainty." He himself calls it “absolute lack of will”, since he cannot force himself to do anything. “Goes with the flow”, scolds himself all the time, analyzes, “digs”. At these moments, it seems to “split in two” - on the one hand, he believes that something needs to be done, and on the other hand, he cannot force himself, he is looking for justifying reasons.
It often seems that those around him, even strangers, pay attention to him, cast a critical glance at him, seeing his inferiority, and talking about him. At work, they often find fault with him, they want to get rid of him, although they don’t talk about it directly. Distrustful of people, inclined to expect something bad from them. At times he seems to know what they are thinking, as their subsequent behavior confirms his hunches.
At times he seems to know what they are thinking, as their subsequent behavior confirms his hunches.
Became completely inactive. Has no companions. He likes to dream alone about the “unrealizable”, “in his thoughts he always wants to do something”, but in reality he remains passive, uninitiative, he has lost all his former hobbies, except for chess; gradually stopped reading even fiction. During classes, “dispersal” interferes: the thought suddenly breaks off and forgets what it was just thinking about.
At times there are obsessive thoughts and desires to hit someone for no reason, to throw themselves out the window. He understands the absurdity of these desires, with difficulty overcomes them. Such thoughts appear sporadically with no apparent connection with external events. Prone to obsessive billing.
Over the past year he has become hypochondriacal, believes that he has “poor health”, that he is “all sick”, that he may not live long.
Leads a secluded life, communicates only with his family, and even then “out of necessity”. With his father is dry, indiscreet. He often quarrels with his wife, believes that she is "prejudiced against him", tries to leave home in order to be alone. He does not feel joy from the birth of a child, he does little with him, only "when they force him."
With his father is dry, indiscreet. He often quarrels with his wife, believes that she is "prejudiced against him", tries to leave home in order to be alone. He does not feel joy from the birth of a child, he does little with him, only "when they force him."
The mood is often depressed, when you don't want to do anything, you are very irritable. This mood lasts for months, and sometimes more than a month.
He does not tell anyone except the doctor about his condition, and even then after active questioning. Passive about treatment.
Table 3
| 1. Abaskuliev A.A. | Asthenic psychopathy. | 311.6 |
| 2. | Schizophrenia. | 305.0 |
| 3. Anufriev A.K. | Schizophrenia, simple form. | 305.0 |
| 4. Volfovsky A.I. | Simple form of schizophrenia. | 305.0 |
| 5. | Schizophrenia, neurosis-like form. |
|
| 6. Detengof F.F. | Schizophrenia, simple form. | 305.0 |
| 7. Zaltsman G.I. | Simple form of schizophrenia. | 305.0 |
| 8. | Schizophrenia, simple form. | 305.0 |
| 9. Zarubashvili A.D. | Psychopathic personality of the asthenic circle. | 311.6 |
| 10. Ilyinsky Yu.A. | Asthenic psychopathy. | 311. |
| 11. Kantorovich N.V. | Schizophrenia, simple form, neurosis-like variant. | 305.0 |
| 12. Malkin P.F. | Relatively mild current schizophrenic process. | 305.9 |
| 13. Maslov E.V. | Schizophrenia neurosis-like (psychopathic), erased form. | 305.5 |
| 14. Megrabyan A.A. | Psychopathy of the asthenic circle. | 320 page 17 |
| 15. Melekhov D.E. | Schizophrenia, with neurosis-like (psychasthenic) symptoms and sluggish course. | 305.0 |
| 16. | Schizophrenia. | 305.0 |
| 17. Morozov V.M. | Sluggish psychasthenic schizophrenia. | 305.9 |
| 18. Nevzorova T.A. | Schizophrenia, sluggish current process, in form closer to a simple, neurosis-like variant. | 305 |
| 19. | Sluggish schizophrenia. | 305.5 |
| 20. Ozeretskovsky D.S. | Schizophrenia. paranoid form. | 305.3 |
| 21. Plesso G.I. | Polishchuk I.A. Developmental neurosis (psychasthenic). | 311. |
| 22. Polishchuk I.A. | Developmental neurosis (psychasthenic). | 310.3 |
| 23. Portnov A.A. | Schizophrenia (simple). | 305.0 |
| 24. Rotshtein G.A. | Schizophrenia, sluggish (neurosis-like). | 305.5 |
| 25. Saarme Yu.M. | Schizophrenia (simple form). | 305.0 |
| 26. Sluchevsky I.F. | Psychasthenic form of psychopathy. | 311.4 |
| 27. Snezhnevsky A.V. | Schizophrenia onset at puberty with reflection. | 305.0 |
| 28. Tatarenko N.P. | Schizophrenia (psychopathic or simple form). | 305.0 |
| 29. Timofeev N.N. | Schizophrenia, simple form. | 305.0 |
| 30. Ushakov G. | Slowly flowing schizophrenic process, neurosis-like form. | 305.9 |
| 31. Fridman B.D. | Sluggish form of schizophrenia. | 305.9 |
| 32. Chalisov M.A. | Schizophrenia, a simple form with a neurosis-like course. | 305. |
| 33. Chistovich A.S. | Psychasthenic development (in an organic psychopath). (Schizophrenia?). | 311.4 |
 Averbukh E.S.
Averbukh E.S.  Golodets R.G.
Golodets R.G.  Zenevich G.V.
Zenevich G.V.  6
6 
 Molokhov A.N.
Molokhov A.N.  Nadzharov R.A.
Nadzharov R.A.  4
4 
 Simple form.
Simple form.  K.
K.  9
9
Table 4
| Schizophrenia simple and unspecified | 15 |
| Paranoid schizophrenia | 1 |
| Schizophrenia psychopathic | 1 |
| Slow-flowing schizophrenia (neurosis-like) | 8 |
| Schizophrenia, total | 25 |
| Psychasthenic psychopathy (in organics) | 1 |
| Asthenic psychopathy | 6 |
| Developmental neurosis (psychoasthenic) | 1 |
The diagnosis of this observation is difficult, because there are a number of symptoms that are common to such probable diseases in this patient as schizophrenia and psychasthenia: depersonalization disorders, mood disorders, endogenous heredity (in a psychopathic personality, both children and parents may suffer obvious schizophrenia), reasoning (second-signal reasoning, according to one of the seminar participants, is characteristic of psychopathic personalities).
The patient's escape from reality, which, being characteristic of many mental illnesses, is also characteristic of neuroses and psychopathy, does not make things easier. The lack of adaptation to the environment can be not only with schizophrenia, but also with pronounced psychasthenic psychopathy. In this case, attempts to use the relationship between the individual and the environment for differential diagnosis are hardly valid either: according to the data given at the seminar, the phenomena of “incomplete home” are allegedly found even more often in schizophrenia than in psychopathy. In addition, it is not easy in this case to differentiate psychasthenicity, shyness, indecision, with ambivalence, and asthenia with a decrease in activity.
In this observation for the diagnosis of schizophrenia in its various variants (neurosis-like variant of sluggish, simple; simple sluggish; paranoid), the following considerations were made.
There was a tendency to a steady increase in painful phenomena. The psychasthenic syndrome developed with an increasing drop in energy potential. There was a development of xenophobia into pronounced delusional ideas and other features characteristic of schizophrenia. There is a permanent loss of performance.
The psychasthenic syndrome developed with an increasing drop in energy potential. There was a development of xenophobia into pronounced delusional ideas and other features characteristic of schizophrenia. There is a permanent loss of performance.
From the side of the mental status at the time of examination of the patient, a number of pronounced changes were found: disorganization and autism of thinking, complete detachment from reality, ambivalence, ambivalence, dissociation between thoughts and actions, disorder of active attention, sperrungs, manticism, hints of depersonalization, reasoning, stereotypes . A peculiar paradox of emotional life was noted: mimosa-like, a special reflection on one's own personal changes and, at the same time, emotional cooling towards relatives, adjoining direct coarsening, dullness and monotony. Pronounced personality changes were pointed out: rudeness, suspicion, lethargy, ugliness, leading to the collapse of all life endeavors, ataxia in the broadest sense of the word.
The patient's formulation “I can't force myself to do literally anything” testifies, in the opinion of one of the seminar participants, to schizophrenia, because such statements are not characteristic of psychasthenics. The present state was qualified as apathico-abulic.
Symposium participants who rejected the diagnosis of schizophrenia cited the following motives: the absence of the dynamics of the disease, which would indicate the features of the process typical of schizophrenia. It is possible to establish contact with the patient in a form in which it cannot be established with patients with schizophrenia. Violations of the associative process were denied. It was pointed out that the patient's concentration on his inner experiences is mistaken for depersonalization, and the symptoms that can be with general asthenia of mental activity are mistaken for reasoning. It was noted that the patient has extraverted compensation in fantasy - overcoming his impossibility to live in the natural world, and not autistic dreams, which are introverted in nature and are characteristic of schizophrenia. The emotional safety of the patient, his softness, positive emotional reaction to the birth of a child were stated. It was pointed out that the patient is not indifferent to his fate. It was noted that the irritability observed in the patient is not specific for schizophrenia, but is specific for asthenia of any origin, and his aggressiveness is neurotic in nature, it does not prove the presence of a schizophrenic defect.
The emotional safety of the patient, his softness, positive emotional reaction to the birth of a child were stated. It was pointed out that the patient is not indifferent to his fate. It was noted that the irritability observed in the patient is not specific for schizophrenia, but is specific for asthenia of any origin, and his aggressiveness is neurotic in nature, it does not prove the presence of a schizophrenic defect.
Participants of the seminar, who diagnosed psychopathy of the psychasthenic circle, substantiated their conclusion as follows: in the genesis of this disease, social and psychological factors play a certain role (gross mistakes in education, insufficient attention, etc.), which had a particularly pronounced effect on a biologically inferior person (asthenization, underdevelopment, - infantilism).
In the psychopathological picture of the disease, there was a large number of psychologically understandable symptoms arising from a conflict situation. It was pointed out that a particularly pronounced manifestation of psychopathic (psychasthenic) features from the moment of the patient's independent life also testifies in favor of this diagnosis. 9mood, suicidal thoughts and attempts, propensity to rationalize. Objections were raised against the diagnosis of this patient within the framework of psychopathy: the degree of emotional disturbances in him was assessed as deeper than is typical for psychiatric patients. It was noted that the patient is rude to relatives, he does not have good contact with anyone. He blames others, not himself. If psychasthenics have thoughts and desires, but no actions, then for a given patient, actions go against desires. Psychasthenics, when there is no severe neurosis of obsessions, the most reliable workers, give a high quality of work, here is a different professional adaptation. It was pointed out that this patient was characterized not by indecision, but by ambivalence, not by asthenia, but by a decrease in activity. There is no phasing during his illness.
9mood, suicidal thoughts and attempts, propensity to rationalize. Objections were raised against the diagnosis of this patient within the framework of psychopathy: the degree of emotional disturbances in him was assessed as deeper than is typical for psychiatric patients. It was noted that the patient is rude to relatives, he does not have good contact with anyone. He blames others, not himself. If psychasthenics have thoughts and desires, but no actions, then for a given patient, actions go against desires. Psychasthenics, when there is no severe neurosis of obsessions, the most reliable workers, give a high quality of work, here is a different professional adaptation. It was pointed out that this patient was characterized not by indecision, but by ambivalence, not by asthenia, but by a decrease in activity. There is no phasing during his illness.
In favor of psychopathy, but of the asthenic circle, the following arguments were made. Weak severity of obsessions, in contrast to what happens with psychasthenic psychopathy, psychopathic heredity. History of forceps delivery and asphyxia. He was brought up in an extremely unfavorable environment. The formation of personality traits over time coincided with a sharp change in the life stereotype and the difficulties of adaptation associated with it, and this happened precisely at the age at which psychopathy of the inhibited circle is usually detected (according to O. V. Kerbikov and colleagues).
History of forceps delivery and asphyxia. He was brought up in an extremely unfavorable environment. The formation of personality traits over time coincided with a sharp change in the life stereotype and the difficulties of adaptation associated with it, and this happened precisely at the age at which psychopathy of the inhibited circle is usually detected (according to O. V. Kerbikov and colleagues).
Features of the mental status include symptoms characteristic of asthenic psychopathy - irritability, inhibition, indecision and shyness.
Against this diagnosis, an opinion was expressed, according to which asthenic psychopaths are not characterized by constant poor performance.
Passive aggressive behavior. ways to stop passive-aggressive behavior and change relationships for the better. How passive-aggressive behavior manifests itself
"Yes" and "no" do not say, do not take black and white..."
children's counting.
"Whoa, no, no. " This saying epitomizes the process that psychologists call "passive aggression."
" This saying epitomizes the process that psychologists call "passive aggression."
A phrase of two contradictory processes. Passivity for us personifies an extreme form of inaction, and aggression is nothing but the embodiment of an active principle.
Thus, we are dealing with two oppositely directed processes that manage to get along together.
An acquaintance of mine told a story of how she found herself alone with a young man in a compartment of a night train and struggled all night with his harassment. Can you imagine? All night "no whoa, no well." This is how it was necessary to refuse, so that the other continued not to hear and not understand? After all, it was not about an insane rapist, but an ordinary man who showed his desire and was persistent in this.
Another example from my teaching work. A capable and intelligent listener cannot begin the practice in any way. She has everything for this. And it's not about self-doubt, it's just a superficial excuse.
In practical sessions, she demonstrates good skills and knowledge, asks the right questions, and accurately notes deep processes. She has already filed a patent and even rented an office for work. But he doesn't give advice.
To define passive aggression, I want to immediately point out the fact that it can be both a habitual psychological defense in a person and a persistent personal characteristic, an important part of the personality that determines his character and life. Therefore, you can meet the features of the described process both in yourself and in many people at different moments of life.
What are the main characteristics of a passive-aggressive personality?
Before us is a rebel, a professional revolutionary, a partisan who does not give up. He is always against. Even when it doesn't work for him. The proverb "to spite my mother, I will freeze my ears" is about them.
Entering a room (into a process, into a relationship, etc. ), he is the first to notice the shortcomings. He immediately sees that this is not the case and will not remain silent. He will say in a sharp, ironic, caustic manner. Will hook you up. True, he will do this not directly, not personally, but in an indefinite form to a third party. For example: "Well, of course, it never occurred to anyone to ventilate the room before classes."
), he is the first to notice the shortcomings. He immediately sees that this is not the case and will not remain silent. He will say in a sharp, ironic, caustic manner. Will hook you up. True, he will do this not directly, not personally, but in an indefinite form to a third party. For example: "Well, of course, it never occurred to anyone to ventilate the room before classes."
His ability to see inconsistencies might delight you if it were all presented in an ethical manner. But the task of a passive-aggressive personality is not to correct the shortcomings. She doesn't care about the outcome. She needs a process. And this process is a struggle. Not an open battle to win. Namely, the struggle, better hidden, but stubborn and endless.
He will fight everything and everyone. If not with anyone outside, then with yourself inside. The price is not important. As I said, the process is important, but not the result.
These are people of the process, fighters of invisible fronts with invisible enemies.
In contact with them, you may wonder how simple things become irresistible. How an easy step becomes impossible, and a simple action turns into an endless intricate process. You are surprised and outraged that the task was not completed, although there were no obstacles.
Why, instead of a simple decision and action, a person continues to ask clarifying questions that lead away from the meaning. Why, having agreed yesterday, nothing happened today.
You will inevitably feel angry around him. You seem to be provoked and teased. And when you break down, you are immediately pointed to a bad character or lack of proper upbringing.
Let's look at each component. Let's start with anger or aggression. It is there, but it is looking for indirect exits. Sarcasm, irony, teasing, provocation. Everything to give vent to anger is used. The main thing is to do it indirectly.
So, let's emphasize the first significant component. There is anger, and a lot of it. This means that the person has energy. There is plenty of it and enough for everything he needs. Therefore, when our character asks for support and asks for advice, help, support, be careful! Whatever you give him, it won't work.
This means that the person has energy. There is plenty of it and enough for everything he needs. Therefore, when our character asks for support and asks for advice, help, support, be careful! Whatever you give him, it won't work.
Favorite psychological game (Eric Berne, psychological game theory, Transactional Analysis) is called "Yes, but..." It looks like this: you were asked for advice, you gave, and immediately an objection follows. Yes, the asker says, but I have already tried it, done it, etc. AND NOTHING GOOD HAPPENED.
If you continue to give other advice and recommendations, then prepare for the fact that they will meet the same fate. Until a brilliant idea comes to your mind, the interlocutor does not need a result. Then what does he need? Here it is time to reveal the second component - passivity.
Passivity in the behavior of a passive-aggressive personality is rather not inaction, but resistance, which is expressed in resistance to those actions that will bring results. Outwardly, it seems that a person simply does not do anything for the sake of a goal. But in fact, there is a struggle going on inside him.
Outwardly, it seems that a person simply does not do anything for the sake of a goal. But in fact, there is a struggle going on inside him.
He wants a result (well, who doesn't?) and resists it. And all his energy, and we remember that there is a lot of it, goes to resist this action. Why, you ask, and you will be right? It's strange, to say the least.
To answer this question, we need to delve into the past of such a person, at the time when this part of the personality is being formed. We are in the age of active action from the moment we acquire our strength. But we can understand our strength and master it only through contact with another.
Case study:
Maxim grew up as an obedient boy. His mother was an extremely anxious woman, full of fears associated with her son. These fears made her active in her relationship with him. She knew what a good mother's child should be like, and that's why she didn't listen to Maxim much. Well, how can a little boy know what he needs? And mom always knows.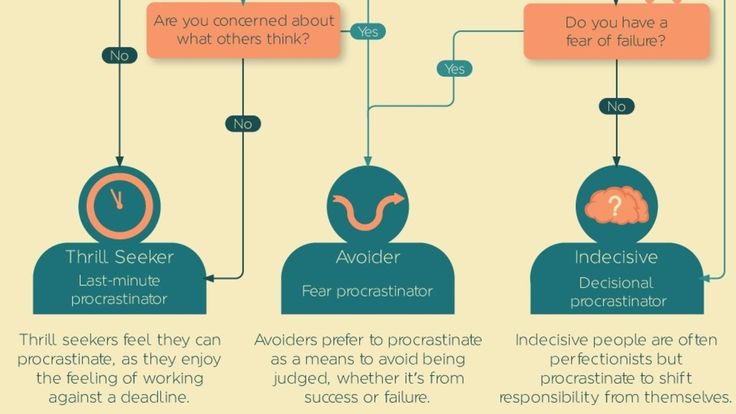
Therefore, her attitude towards the child was more like violence than care. Starting from feeding, ending with the choice of friends. Swallowing the hated porridge, and then playing the hated scales in the hated music school, Maxim began to look for ways against which his mother was powerless.
For example, he could clench his teeth or pull out. He could just sit silently over the violin without touching the strings. At these moments, my mother exploded and yelled, but Maxim clearly felt his victory. He felt his strength when the teacher almost sobbed from impotence and anger, and he just stood silent at the blackboard.
And in his childish mind he deduced the formula: "Power is not in action, but in resistance." Since he was not allowed to realize and feel his own power in what he wanted to do, the only opportunity to enjoy his own power was guaranteed to be when he resisted something. Sometimes later, in adulthood, he caught himself thinking that he was not opposed to what he opposed, but he could no longer do anything.
In childhood, the passive-aggressive personality has a dramatic experience of such "soft" and sometimes quite hard violence in the form of care and control from parents. And they decided to take revenge. Revenge by preventing the parent from seeing the result. Therefore, the best thing you can do is not reach the goal and not get the result.
To hurt a parent so that he, in secret hope, understands how bad the child is. To ask what you want, instead of forcibly stuffing what seems right to the parent. Isn't the highest aerobatics of revenge on parents - this is not to become happy? After all, one of the most important results of parenthood is a happy child. And depriving a parent of this reward becomes the very unconscious goal that a passive-aggressive personality strives for.
And the price is not important here. After all, we are talking about the inner Child, to whom he himself is not yet important. The parent is above all, he is the source of life and love. Therefore, it is not a pity to freeze your ears.
Therefore, it is not a pity to freeze your ears.
Thus, two birds with one stone become a trophy in this battle: the ability to feel one's strength (through resistance) and revenge on the parent (through failure to get a result).
Let me remind you that this process is unconscious. And a person can be sincerely surprised at the lack of results of his actions until he sees that he is his own biggest enemy. That subconsciously he builds the process of actions in such a way that the result is impossible. He chooses the wrong people, he does not feel the situation, he does not notice important details, he does not hear recommendations.
Such people are often late, miss playoffs and quarrel with the right people. And they always find excuses and explanations for their behavior. They even sound convincing. Most often, he sees the cause not in himself, but in other people, in circumstances.
Their problem is to express their needs directly, using the power of anger.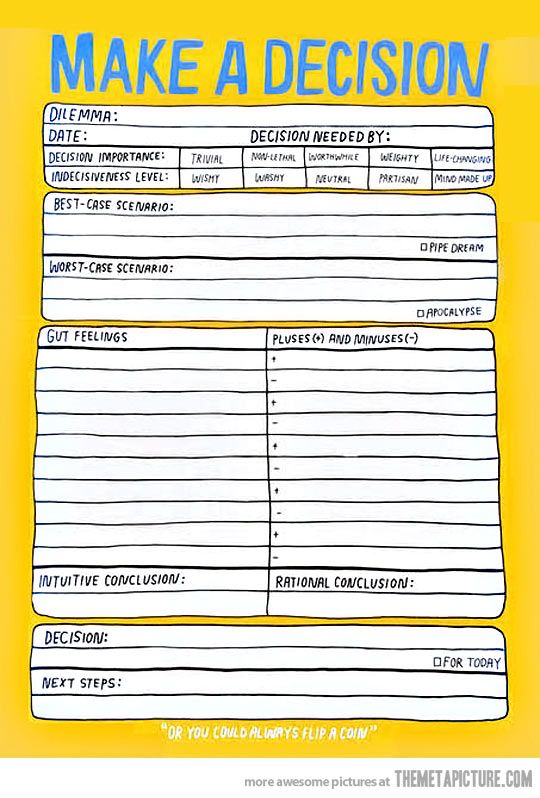 But they are afraid to show anger, because in childhood it was impossible and dangerous. Therefore, anger, and with it strength and energy, are blocked and turned 180 ", that is, against itself.
But they are afraid to show anger, because in childhood it was impossible and dangerous. Therefore, anger, and with it strength and energy, are blocked and turned 180 ", that is, against itself.
Life becomes a continuous overcoming of difficulties. Like in the famous video in which the client complains about headaches and problems, while she does not see a huge nail in her head.
Another important trait of a passive-aggressive personality is being stuck in the "either-or" trap. "Either you eat this porridge, or you are not my son," my mother said. The parent left the child no choice. Either you do as I say, or you lose my love. This trap gets stuck in the way of thinking, which makes the selection process extremely difficult.
Such individuals make good critics and detectives, investigative journalists and satirists. Their sharp eyes will not miss anything.
They are often good and loyal friends, with a subtle sense of humor and willingness to help. By the way, humor is also their hallmark. They are extremely ironic. The thing is that anger and humor have one similar function: they relieve tension. And since anger is blocked in the passive-aggressive personality, a lot of energy can come out through humor. Here they are polishing it.
They are extremely ironic. The thing is that anger and humor have one similar function: they relieve tension. And since anger is blocked in the passive-aggressive personality, a lot of energy can come out through humor. Here they are polishing it.
In social networks, a passive-aggressive personality is easy to spot. Their scope is comments. The fact is that they rarely take the initiative. They are already inclined to jump in and ride on a "foreign horse", to become noticeable at the expense of another. Their comments are critical and sarcastic. They provoke the audience and, in the end, disappear, confirming that the world and people are imperfect.
As clients, the passive-aggressive personality is a test for the consultant. The game "Yes, but" will bring anyone to hysterics. Therefore, the main principle in the work is to give the initiative in determining the goal to the client.
Don't offer anything until you get an answer to the question "What would you like?" The transference therapist will become the very parent to be avenged. And it will be extremely difficult to wait for changes and advancement in the life of a client.
And it will be extremely difficult to wait for changes and advancement in the life of a client.
The fact that a passive-aggressive person is often very capable and talented gives hope for a quick result. In the event that a person abandons the idea of revenge and begins to master his power through a direct expression of anger. Learn to say "no" directly, instead of going into ambush and building catacombs for guerrilla operations.
Instead of "either-or" will begin to use the pronoun "and". Both, instead of either-or.
I hope that this information will help you better understand people and yourself, which means it will give you the opportunity to improve the quality of life.
Passive-aggressive personality disorder is a condition in which people express anger and negative feelings covertly through their actions instead of directly venting their aggression at others. It is characterized by a tendency to obstructionism, constant procrastination, stubbornness, feigned forgetfulness, and deliberate inefficiency in all matters. People with a passive-aggressive personality type constantly complain about everything, are depressed, actively express their pessimistic attitude and are uncompromising in everything. Very often they try to realize themselves in dependent relationships, finding satisfaction in resisting all the partner's attempts to achieve adequate performance, productive independent work, equal returns in household chores, etc.
People with a passive-aggressive personality type constantly complain about everything, are depressed, actively express their pessimistic attitude and are uncompromising in everything. Very often they try to realize themselves in dependent relationships, finding satisfaction in resisting all the partner's attempts to achieve adequate performance, productive independent work, equal returns in household chores, etc.
When passive-aggressive personality disorder was first diagnosed
It was first described as a clinical case by Colonel William Menninger during World War II. He noted a peculiar deviation in some of the men, undermining their military conformity. Menninger pointed to the obviously defiant, but not contrary to direct orders, behavior of the soldiers. It was expressed in "passive opposition" such as deliberate slowness, inability to understand orders, making mistakes, general inefficiency, and passive obstruction. The colonel himself did not single out the disorder as a separate ailment and explained it as "personal immaturity" and a reaction to military stress.
For the first time, the classification of passive-aggressive personality disorder as a separate group of disorders was discussed back in the 50s of the last century, and this problem was widely discussed in the late 80s and early 90s, when, thanks to the possibilities of the World Wide Web, a mass the prevalence of such behavior in the communication of Internet users. And although not all e-mails, notes and messages with characteristic content indicate that their authors have this problem, sociological and clinical studies have shown that ~96-98% of persons belonging to the passive-aggressive personality type implement their usual behavior in network communication.
Causes of passive-aggressive personality disorder
According to most modern researchers, in most cases the roots of the problem originate in childhood. Analysis of data from different groups of subjects, depending on age, gender, race, nationality and social status, did not reveal a pronounced correlation, and the indicator varied depending on the research methods used. At the same time, there is an unambiguous relationship with a violation of the incentive system in early childhood. Most often this happens in dysfunctional families where the child does not feel safe enough to freely express frustration, anger and other feelings.
At the same time, there is an unambiguous relationship with a violation of the incentive system in early childhood. Most often this happens in dysfunctional families where the child does not feel safe enough to freely express frustration, anger and other feelings.
The same applies to overly conservative families, where the role of the dominant head of the family is clearly expressed and physical and psychological punishment is actively practiced. Under such conditions, honest expression of feelings is forbidden, and children unconsciously learn to suppress and deny their emotions, using other channels to express resentment and disappointment. Not finding opportunities for natural relaxation, the child eventually begins to consider them the norm, and in the process of growing up they become a kind of cliche, according to which a personality is formed.
Signs and main symptoms of passive-aggressive behavior
Persons with passive-aggressive personality disorder are irritable or even agitated most of the time. They have a low tolerance for disappointment and mood swings that change in very rapid succession. Such people are impatient with others, and their interest in communication, as it should be, is sharply replaced by antipathy or boredom and complete disregard.
They have a low tolerance for disappointment and mood swings that change in very rapid succession. Such people are impatient with others, and their interest in communication, as it should be, is sharply replaced by antipathy or boredom and complete disregard.
In passive-aggressive disorder, people feel dissatisfied all the time, accuse others of abuse and deceit, feel that they are underestimated, and attribute any failures to circumstances.
Individually, these signs may simply be character traits of the person and do not indicate a specific abnormality, but taken together, they often point accurately to the problem. In particular, passive-aggressive disorder is indicated by the simultaneous presence of symptoms such as:
- constant resentment towards everyone;
- opposition to any demands of other people;
- postponing work for later in order to miss the deadlines for its implementation;
- procrastination and intentional errors in any activity;
- cynical, sullen or hostile attitude towards everyone;
- frequent complaints of a person that he is betrayed, deceived and underestimated;
- unwillingness to solve their problems;
- complete rejection of criticism and cruel nit-picking in anyone who tries to give advice;
- envy and contempt for all people who are in power or generally more successful.
If they are accompanied by self-doubt, the inability to express their needs and desires directly, as well as the inability of a person to ask the necessary questions to find out what is expected of him, then this indicates the presence of this disorder with a 99% probability.
Classification of passive-aggressive personality types
Since much attention has been paid to this problem in the last two decades, today a more or less accurate classification of "negativistic" or "passive-aggressive" personality types has already been drawn up. For example, the famous American psychologist Theodore Millon identified four separate subtypes of this disorder:
| Subtype | Character traits |
| oscillating | Uncertainty and confusion; the inability to name the exact reason for their own capricious behavior; indecision both in interaction with others and as the main subjective feature of the course of all processes in the psyche. |
| dissatisfied | Grunts, petty nitpicking, irascibility over trifles, capriciousness, anger, complaints about anything, irritability, pretense to avoid open confrontation. |
| masked | Opposition is expressed in a veiled and ambiguous way. Most often, this is feigned slowness, forgetfulness, inefficiency, disregard for charters and rules, stubbornness. The person also becomes very tortuous and tries to use only indirect methods of sabotage in order to avoid direct claims of sabotage. |
| sharp (coarse) | Disputability, intransigence, uncompromisingness, capriciousness, quarrelsomeness; the character becomes caustic and irritable; a person takes pleasure in humiliating and insulting others. |
Popular is the detailed classification by category, which was proposed by the American professor Preston Ni from the University of California. The study of issues of interpersonal effectiveness, professional communication, as well as intercultural understanding and organizational change prompted him to pay attention to this issue. In total, he identifies ten general categories that people with passive-aggressive disorder fit into and, in his opinion, most exhibit at least a few of them on a regular basis.
The study of issues of interpersonal effectiveness, professional communication, as well as intercultural understanding and organizational change prompted him to pay attention to this issue. In total, he identifies ten general categories that people with passive-aggressive disorder fit into and, in his opinion, most exhibit at least a few of them on a regular basis.
- General verbal hostility . Examples : spreading gossip; unreasonable criticism of others; non-recognition of generally accepted rules and norms; condescending treatment of adults as children.
What guides : Putting others down makes you feel like you're in a dominant position. Inflicting moral suffering on others and depriving them of emotional balance is done to alleviate one's own lack of peace and security. The main desire is to support one's false sense of importance at the expense of criticizing others and make everyone suffer "for the company". In the family, this is expressed in the form of competition for power over the household and complete control in relationships.
- Ridicule. Examples : sarcasm, hostile jokes towards others, desire to tease people to the point of pissing them off. A characteristic feature is the need to humiliate a person as much as possible, avoiding an open conflict and showdown, referring to "just kidding."
What guides : Taking out one's own hidden anger and discomfort on a suitable victim. The main desire is to marginalize someone else's human dignity and authority to their own level.
- General disguised hostility . Examples : Demonstration of disdain and resentment towards people, sullenness, desire to inflict emotional pain by reproaching or ignoring.
What guides : an attempt to compensate for one's inner insecurity by deliberately creating a negative emotional background in the immediate environment and unbalancing people.
- Psychological manipulation . Examples : duplicity, a pathological tendency to intrigue, the desire to deliberately frame a person at every opportunity (for the sake of pleasure and often without any benefit to oneself), ostentatious sacrifice, twisting the same information in a conversation with different people, divulging or withholding important facts depending on the situation.
 A characteristic feature is pretense and a strong desire to protect oneself from disclosure.
A characteristic feature is pretense and a strong desire to protect oneself from disclosure.
What guides : redirecting attention away from one's own problems by endlessly interfering in someone else's life with the help of intrigue and deceit. Achieving a false sense of superiority by manipulating others.
- Bullying . Examples : unfounded accusations against someone else with an attempt to find the most vulnerable spot of the victim and cause her maximum mental pain.
What guides : Achieving a false sense of happiness and self-fulfillment against the background of the suffering of others.
- Sabotage and blaming others . Examples : ostentatious slowness, lethargy, forgetfulness, "dullness"; the desire to create a maximum of red tape around yourself and upset as many other people's plans as possible. The need is pathological and compels a person to act even without any personal gain.
What guides : creating the illusion of self-importance and authority; the desire to put everyone in a position dependent on oneself in order to block the success of other people. Often feels burning envy towards those who are more successful, which is expressed in unfounded accusations and harsh baseless criticism.
- Automatic countermeasure . Examples : stubborn intractability, rigidity, inefficiency, tendency to complicate things, habit of leaving things unfinished, attempts to sabotage the work of others.
What guides : Compensation for own insolvency. In this case, "victory" is achieved at the expense of the victim's frustration and negative emotions.
- Underhand sabotage . Examples : failure to complete any tasks, projects and activities; causing material losses or overspending resources; pathological sabotage; destruction of well-established work and personal relationships of people around; deliberate dissemination of harmful information.

What guides : obtaining moral satisfaction at the expense of revenge and "punishment" of other people; achieving emotional pleasure from observing the result of their “works”.
- Showy sacrifice . Examples : exaggeration of the importance of personal matters; manipulation of one's own health; deliberately inventing imaginary problems in order to bind the victim to himself and enjoy his sympathy and favor; taking on the role of a martyr who sacrificed his well-being for the sake of others (usually with the reproach that this sacrifice was not appreciated).
What guides : Desire to take advantage of the recipient's good will and concern and to evoke strong emotional attachment on his part to manipulate.
- Self-flagellation . Examples : intentionally creating a situation in which victim status could be achieved; groundless reproaches and reproaches; self-harm and suicide blackmail.
What guides : Desire to intimidate or cause suffering to emotionally dependent people by harming oneself. Love for creating dramas to focus attention around you.
However, in the professor's opinion, the latter sign itself cannot be considered as a separate symptom of the disorder, since it can also be a kind of cry for help, being evidence of other mental illnesses.
Treatment of passive-aggressive personality disorder
The difficulty of treating disorders of this group is that in most cases people are simply unable to get pleasure and moral satisfaction in other ways. The normal system of incentives does not work in this case, so the main program is reduced to psychotherapy and psychoanalysis, during which the patient is taught to isolate "harmful" thoughts and incentives for their conscious replacement with "useful" ones.
According to the results of clinical observations, the following set of automatic attitudes and thoughts is most often typical for passive-aggressive disorders:
- “they don't dare to tell me what to do”;
- "I will only do what I want";
- "I will do everything to spite them";
- "no one is grateful for my work";
- "everyone around is just using me";
- "I can never achieve real success";
- "people don't want to understand me";
- "my life is unhappy, and nothing can be done about it";
- "I still won't succeed";
- "being honest and frank is a weakness";
- "others want to limit and suppress my personality.
 "
"
The therapist finds out exactly what pathological thoughts and stimuli act in a person on an “automatic” level and teaches them to consciously block them. The course of treatment, as a rule, lasts at least one year, and during this time the doctor and the patient go from the stage of understanding the causes and consequences of such behavior to the development of methods of mild confrontation. The best results can be achieved if the immediate environment also participates in the process and gently, but decisively, ceases to indulge the patient's weaknesses, using the substitute templates created by the therapist. In especially advanced cases, it is allowed to eliminate acute symptoms (depression, anxiety, outbursts of anger) with medication, after which traditional therapy is carried out.
Prognosis and possible complications
In general, with adequate treatment, the prognosis is quite good. If a person has been able to open up and understand the causes of the problem, supportive psychotherapy usually brings excellent results. Of course, having been established in early childhood, this personality disorder tends to persist for a very long time. But with the patient's constant volitional efforts to overcome it, it can "burn out" with therapy and be replaced by a positive life experience.
Of course, having been established in early childhood, this personality disorder tends to persist for a very long time. But with the patient's constant volitional efforts to overcome it, it can "burn out" with therapy and be replaced by a positive life experience.
However, there is such a thing as individual tolerance, on which the success of the entire event depends greatly. Even if a positive result seems stable, a person may not fully accept new ideas and balance on the edge. The “dominant thought base” is too deeply rooted in his personality, so even the slightest push is enough for such a person to fall back into a state of chaos and dissatisfaction. Often complications arise when there is an imaginary or real lack of stability in life. This applies to any area: social, professional, spiritual, legal, financial, etc. Complications can also arise when the patient weakens control over negative thoughts, and the immediate environment does not pay attention to this and indulges his behavior or, on the contrary, expresses strong opposition . After all, the key component of psychotherapy is precisely the soft opposition to negative ideas.
After all, the key component of psychotherapy is precisely the soft opposition to negative ideas.
Character. Meanwhile, it has a number of distinguishing features. Consider further how passive aggression manifests itself.
General information
Passive-aggressive personality type is characterized by pronounced resistance to external requirements. As a rule, this is evidenced by obstructive and oppositional actions. Passive-aggressive type of behavior is expressed in procrastination, poor quality of work, "forgetting" obligations. Often do not meet generally accepted standards. Moreover, the passive-aggressive personality resists the need to follow norms. Of course, these characteristics can be observed in other people. But with passive aggression, they become a model of behavior, a pattern. Despite the fact that this form of interaction is considered not the best, it is not too dysfunctional, but until such time as it becomes a life scheme that impedes the achievement of goals.
Passive-aggressive person: features
People in this category try not to be assertive. They believe that direct confrontation is dangerous. Conducting a personality type test, you can identify the characteristic features of behavior. In particular, people in this category consider confrontation as one of the ways outsiders interfere in their affairs and control them. When such a person is approached with a request that he does not want to fulfill, the combination of indignation at existing external requirements and lack of self-confidence causes a reaction in a provocative manner. Passive-aggressive communication does not create the possibility of rejection. Obligations at school or at work, people in this category are also outraged. In general, those who are endowed with power, they see as prone to injustice and arbitrariness. Accordingly, as a rule, they blame others for their problems. Such people cannot understand that they create difficulties by their own behavior.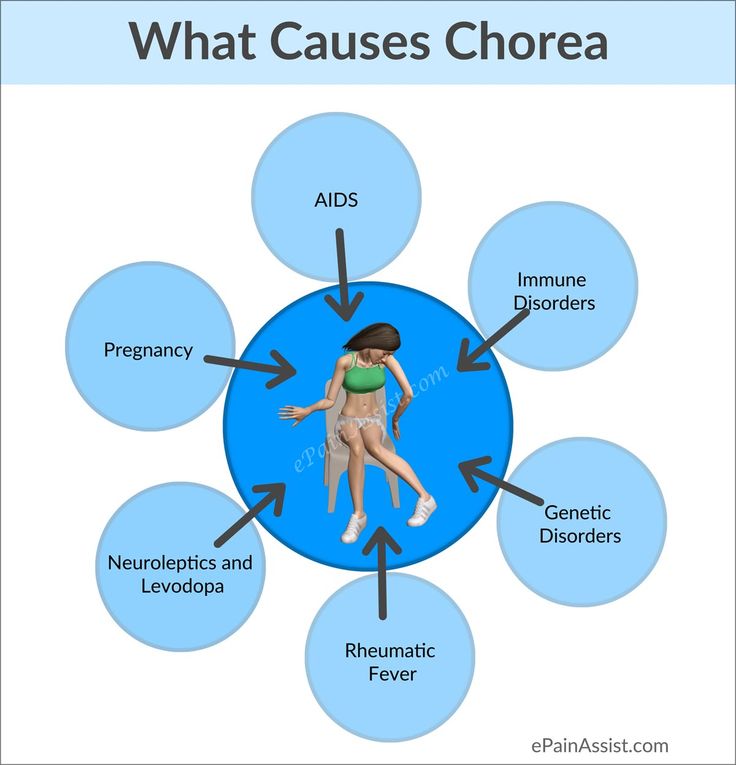 Researchers note that among other things, a passive-aggressive person is easily amenable to mood swings and tends to perceive what is happening pessimistically. Such people focus on everything negative.
Researchers note that among other things, a passive-aggressive person is easily amenable to mood swings and tends to perceive what is happening pessimistically. Such people focus on everything negative.
Personality type test
A total pattern of resistance to standards in the professional and social spheres emerges in early adulthood. It is expressed in different contexts. There are a number of signs of passive aggression. Person:
Historical information
The passive-aggressive style of behavior has been described for a long time. However, before World War II, this concept was not used. In 1945, the War Department described "an immature reaction" as a response to "a normal military stress situation." It manifested itself in inadequacy or helplessness, passivity, outbursts of aggression, obstructionism. At 19In 1949, the US Armed Forces technical bulletin used this term to describe soldiers who showed this pattern.
Classification
The DSM-I classified reactions into three categories: passive-aggressive, passive-dependent, and aggressive.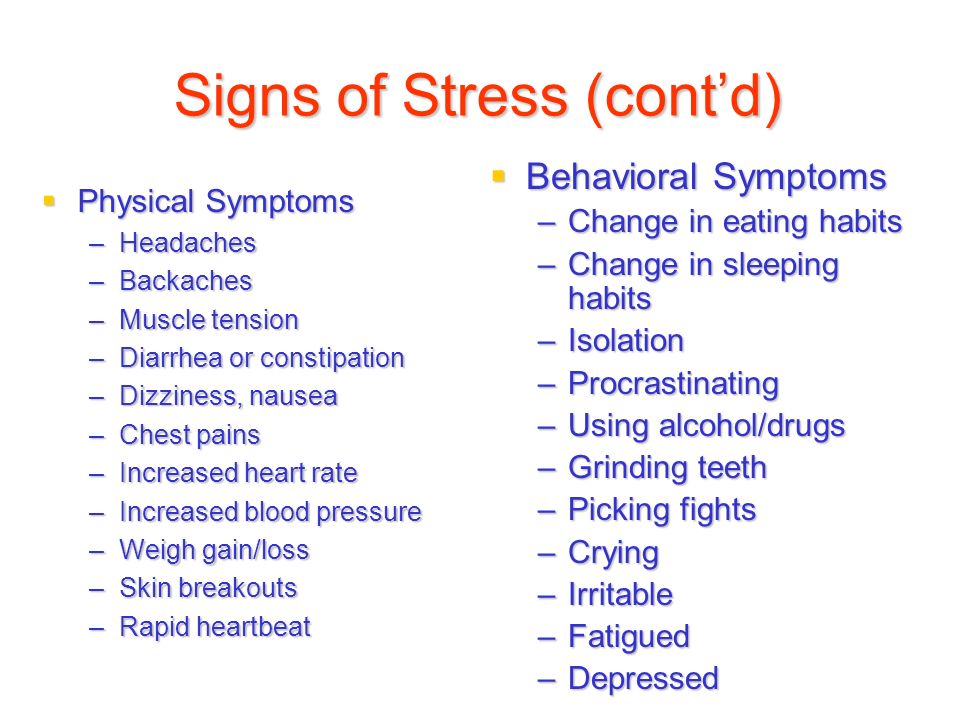 The second was characterized by helplessness, a tendency to hold on to others, indecision. The first and third categories differed in people's reaction to frustration (the inability to satisfy any need). The aggressive type, in a number of aspects having signs of antisocial, shows irritation. His behavior is destructive. A passive-aggressive person makes a disgruntled face, becomes stubborn, begins to slow down work, reduce its effectiveness. In DSM-II, such behavior is classified as a separate category. At the same time, aggressive and passive-dependent types are included in the group of "other disorders".
The second was characterized by helplessness, a tendency to hold on to others, indecision. The first and third categories differed in people's reaction to frustration (the inability to satisfy any need). The aggressive type, in a number of aspects having signs of antisocial, shows irritation. His behavior is destructive. A passive-aggressive person makes a disgruntled face, becomes stubborn, begins to slow down work, reduce its effectiveness. In DSM-II, such behavior is classified as a separate category. At the same time, aggressive and passive-dependent types are included in the group of "other disorders".
Clinical and experimental data
Despite the fact that the passive-aggressive style of behavior remains poorly understood today, at least two papers outline its key characteristics. Thus, Kening, Trossman and Whitman examined 400 patients. They found that the most common diagnosis was passive-aggressive. At the same time, 23% showed signs of a dependent category. 19% of patients fully corresponded to the passive-aggressive type.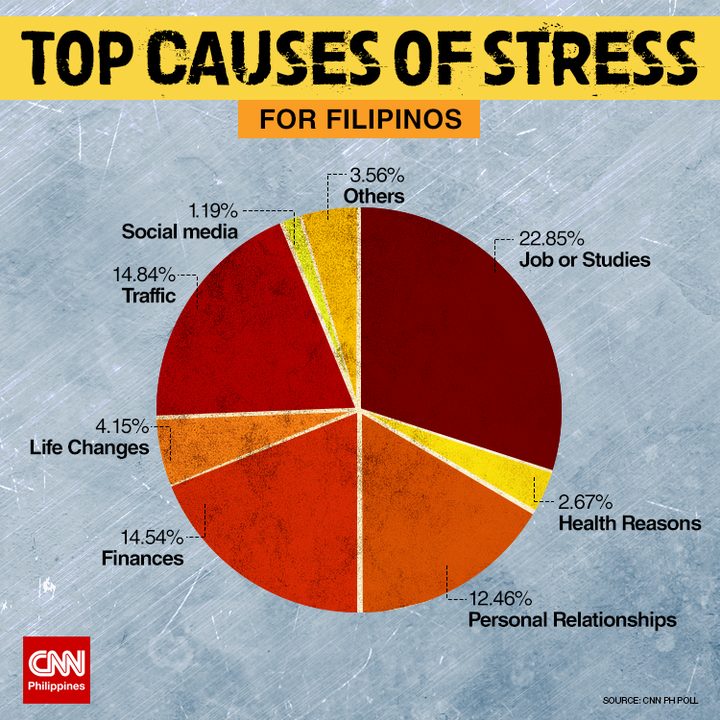 In addition, the researchers found that PARL occurs in women twice as often as in men. The traditional symptomatic picture included anxiety and depression (41% and 25%, respectively). In the passive-aggressive and dependent types, open indignation was suppressed by fear of punishment or a sense of guilt. Research has also been done by Moore, Alig and Smoly. They studied 100 patients diagnosed with passive-aggressive disorder 7 and 15 years later during inpatient treatment. The researchers found that problems in social behavior and interpersonal relationships, along with somatic and emotional complaints, were the main symptoms. The researchers also found that a significant proportion of patients suffer from depression and alcohol abuse.
In addition, the researchers found that PARL occurs in women twice as often as in men. The traditional symptomatic picture included anxiety and depression (41% and 25%, respectively). In the passive-aggressive and dependent types, open indignation was suppressed by fear of punishment or a sense of guilt. Research has also been done by Moore, Alig and Smoly. They studied 100 patients diagnosed with passive-aggressive disorder 7 and 15 years later during inpatient treatment. The researchers found that problems in social behavior and interpersonal relationships, along with somatic and emotional complaints, were the main symptoms. The researchers also found that a significant proportion of patients suffer from depression and alcohol abuse.
Automatic thoughts
The conclusions that a person with PD makes reflects his negativity, isolation and the desire to choose the path of least resistance. For example, any requests are considered as a manifestation of exactingness and importunity.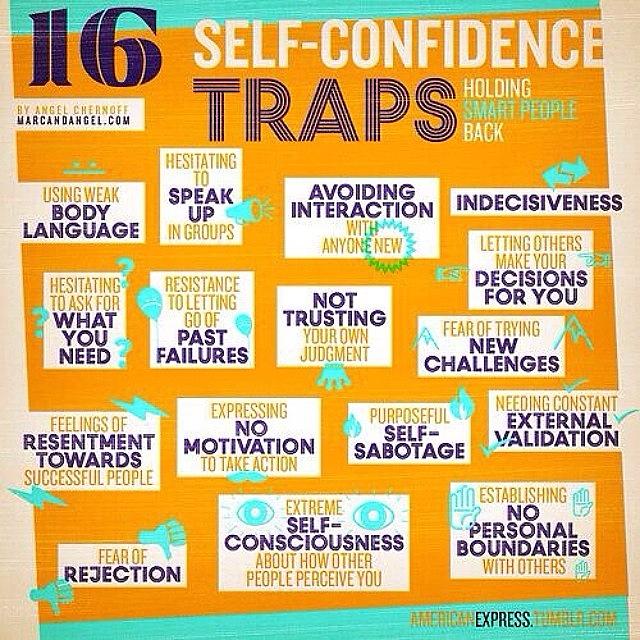 The reaction of a person is that he automatically resists instead of analyzing his desire. The patient is characterized by the belief that others are trying to use him, and if he allows it, he will become a nonentity. This form of negativism extends to all thinking. The patient is looking for a negative interpretation of most of the events. This applies even to positive and neutral phenomena. This manifestation distinguishes a passive-aggressive person from a depressed patient. In the latter case, people focus on self-judgment or negative thoughts about the future, the environment. The passive-aggressive individual believes that others are trying to control them without appreciating them. If a person receives a negative reaction in response, then he assumes that he was again misunderstood. Automatic thoughts testify to the irritation that appears in patients. They insist quite often that everything must go according to a certain pattern. Such unreasonable demands contribute to a decrease in resistance to frustration.
The reaction of a person is that he automatically resists instead of analyzing his desire. The patient is characterized by the belief that others are trying to use him, and if he allows it, he will become a nonentity. This form of negativism extends to all thinking. The patient is looking for a negative interpretation of most of the events. This applies even to positive and neutral phenomena. This manifestation distinguishes a passive-aggressive person from a depressed patient. In the latter case, people focus on self-judgment or negative thoughts about the future, the environment. The passive-aggressive individual believes that others are trying to control them without appreciating them. If a person receives a negative reaction in response, then he assumes that he was again misunderstood. Automatic thoughts testify to the irritation that appears in patients. They insist quite often that everything must go according to a certain pattern. Such unreasonable demands contribute to a decrease in resistance to frustration.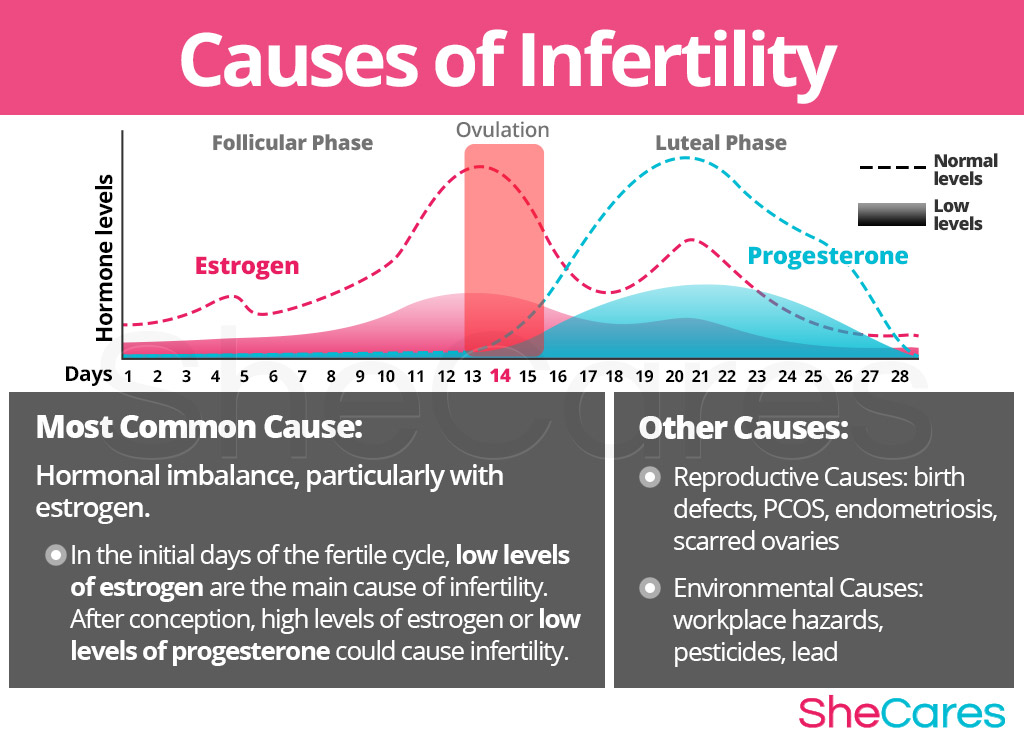
Typical attitudes
The behavior of PD patients expresses their cognitive patterns. Procrastination, poor quality of work are due to indignation at the need to fulfill duties. A person is set up to do what he does not want to do. The procrastination attitude is to follow the path of least resistance. For example, a person begins to believe that the matter can be postponed until later. Faced with the adverse consequences of not fulfilling his duties, he expresses dissatisfaction with those around him who have power. It may manifest itself in an outburst of anger, but most likely passive methods of revenge will be used. For example, sabotage. In psychotherapy, behavior may be accompanied by a refusal to cooperate in treatment.
Emotions
Annoyance will be common for PD patients and is understandable because people feel they are being asked to meet arbitrary standards, underestimated or misunderstood. Patients often fail to achieve their goals in the professional sphere, as well as in their personal lives. They are unable to understand how their behavior and existing attitudes affect the difficulties they have. This leads to further annoyance and dissatisfaction, as they again believe that circumstances are to blame. Patients' emotions are largely determined by their vulnerability to external control and the interpretation of requests as a desire to limit their freedom. When interacting with others, they constantly expect demands and, accordingly, resist.
They are unable to understand how their behavior and existing attitudes affect the difficulties they have. This leads to further annoyance and dissatisfaction, as they again believe that circumstances are to blame. Patients' emotions are largely determined by their vulnerability to external control and the interpretation of requests as a desire to limit their freedom. When interacting with others, they constantly expect demands and, accordingly, resist.
Prerequisites for therapy
The main reason patients seek help are complaints from others that these people do not live up to expectations. As a rule, co-workers or spouses turn to psychotherapists. Complaints of the latter are connected with the unwillingness of patients to provide assistance in household chores. Psychotherapists are often approached by bosses who are dissatisfied with the quality of the work performed by their subordinates. Another reason for visiting a doctor is depression. The development of this condition is caused by a chronic lack of encouragement both in the professional sphere and in personal life.