What causes autism in the brain
Autism Spectrum Disorder Fact Sheet
What is autism spectrum disorder?
What are some common signs of ASD?
What disorders are related to ASD?
How is ASD diagnosed?
What causes ASD?
What role do genes play?
Do symptoms of autism change over time?
How is autism treated?
What research is being done?
Where can I get more information?
What is autism spectrum disorder?
Autism spectrum disorder (ASD) refers to a group of neurodevelopment disorders cthat affect how people communicate, learn, behave, and socially interact. People may have repetitive and characteristic patterns of behavior or narrow interests. Not everyone who has ASD may have these symptoms, which are usually present from early childhood and affect daily functioning. Both children and adults can have ASD.
The term “spectrum” refers to the wide range of symptoms, skills, and levels of disability in functioning that can occur in people with ASD. Some children and adults with ASD are fully able to perform all activities of daily living while others require substantial support to perform basic activities. Learning and thinking can range from extremely gifted to needing severe help.The Diagnostic and Statistical Manual of Mental Disorders (DSM-5, published in 2013) includes Asperger syndrome, childhood disintegrative disorder, and pervasive developmental disorders not otherwise specified (PDD-NOS) as part of ASD rather than as separate disorders. A diagnosis of ASD includes an assessment of intellectual disability and language impairment.
ASD occurs in every racial and ethnic group, and across all socioeconomic levels. However, boys are significantly more likely to develop ASD than girls.
top
What are some common signs of ASD?
Even as infants, children with ASD may seem different, especially when compared to other children their own age. They may become overly focused on certain objects, rarely make eye contact, and fail to engage in typical babbling with their parents. In other cases, children may develop normally until the second or even third year of life, but then start to withdraw and become indifferent to social engagement.
The severity of ASD can vary greatly and is based on the degree to which social communication, insistence of sameness of activities and surroundings, and repetitive patterns of behavior affect the daily functioning of the individual.
Social impairment and communication difficulties
Many people with ASD find social interactions difficult. The mutual give-and-take nature of typical communication and interaction is often particularly challenging. Children with ASD may fail to respond to their names, avoid eye contact with other people, and only interact with others to achieve specific goals. Often children with ASD do not understand how to play or engage with other children and may prefer to be alone. People with ASD may find it difficult to understand other people’s feelings or talk about their own feelings.
People with ASD may have very different verbal abilities ranging from no speech at all to speech that is fluent, but awkward and inappropriate. Some children with ASD may have delayed speech and language skills, may repeat phrases, and give unrelated answers to questions. In addition, people with ASD can have a hard time using and understanding non-verbal cues such as gestures, body language, or tone of voice. For example, young children with ASD might not understand what it means to wave goodbye. People with ASD may also speak in flat, robot-like or a sing-song voice about a narrow range of favorite topics, with little regard for the interests of the person to whom they are speaking.
Some children with ASD may have delayed speech and language skills, may repeat phrases, and give unrelated answers to questions. In addition, people with ASD can have a hard time using and understanding non-verbal cues such as gestures, body language, or tone of voice. For example, young children with ASD might not understand what it means to wave goodbye. People with ASD may also speak in flat, robot-like or a sing-song voice about a narrow range of favorite topics, with little regard for the interests of the person to whom they are speaking.
Repetitive and characteristic behaviors
Many children with ASD engage in repetitive movements or unusual behaviors such as flapping their arms, rocking from side to side, or twirling. They may become preoccupied with parts of objects like the wheels on a toy truck. Children may also become obsessively interested in a particular topic such as airplanes or memorizing train schedules. Many people with ASD seem to thrive so much on routine that changes to the daily patterns of life — like an unexpected stop on the way home from school — can be very challenging. Some children may even get angry or have emotional outbursts, especially when placed in a new or overly stimulating environment.
Some children may even get angry or have emotional outbursts, especially when placed in a new or overly stimulating environment.
top
What disorders are related to ASD?
Certain known genetic disorders are associated with an increased risk for autism, including Fragile X syndrome (which causes intellectual disability) and tuberous sclerosis (which causes benign tumors to grow in the brain and other vital organs) — each of which results from a mutation in a single, but different, gene. Recently, researchers have discovered other genetic mutations in children diagnosed with autism, including some that have not yet been designated as named syndromes. While each of these disorders is rare, in aggregate, they may account for 20 percent or more of all autism cases.
People with ASD also have a higher than average risk of having epilepsy. Children whose language skills regress early in life — before age 3 — appear to have a risk of developing epilepsy or seizure-like brain activity. About 20 to 30 percent of children with ASD develop epilepsy by the time they reach adulthood. Additionally, people with both ASD and intellectual disability have the greatest risk of developing seizure disorder.
About 20 to 30 percent of children with ASD develop epilepsy by the time they reach adulthood. Additionally, people with both ASD and intellectual disability have the greatest risk of developing seizure disorder.
top
How is ASD diagnosed?
ASD symptoms can vary greatly from person to person depending on the severity of the disorder. Symptoms may even go unrecognized for young children who have mild ASD or less debilitating handicaps.
Autism spectrum disorder is diagnosed by clinicians based on symptoms, signs, and testing according to the Diagnostic and Statistical Manual of Mental Disorders-V, a guide created by the American Psychiatric Association used to diagnose mental disorders. Children should be screened for developmental delays during periodic checkups and specifically for autism at 18- and 24-month well-child visits.
Very early indicators that require evaluation by an expert include:
- no babbling or pointing by age 1
- no single words by age 16 months or two-word phrases by age 2
- no response to name
- loss of language or social skills previously acquired
- poor eye contact
- excessive lining up of toys or objects
- no smiling or social responsiveness
Later indicators include:
- impaired ability to make friends with peers
- impaired ability to initiate or sustain a conversation with others
- absence or impairment of imaginative and social play
- repetitive or unusual use of language
- abnormally intense or focused interest
- preoccupation with certain objects or subjects
- inflexible adherence to specific routines or rituals
If screening instruments indicate the possibility of ASD, a more comprehensive evaluation is usually indicated. A comprehensive evaluation requires a multidisciplinary team, including a psychologist, neurologist, psychiatrist, speech therapist, and other professionals who diagnose and treat children with ASD. The team members will conduct a thorough neurological assessment and in-depth cognitive and language testing. Because hearing problems can cause behaviors that could be mistaken for ASD, children with delayed speech development should also have their hearing tested.
A comprehensive evaluation requires a multidisciplinary team, including a psychologist, neurologist, psychiatrist, speech therapist, and other professionals who diagnose and treat children with ASD. The team members will conduct a thorough neurological assessment and in-depth cognitive and language testing. Because hearing problems can cause behaviors that could be mistaken for ASD, children with delayed speech development should also have their hearing tested.
top
What causes ASD?
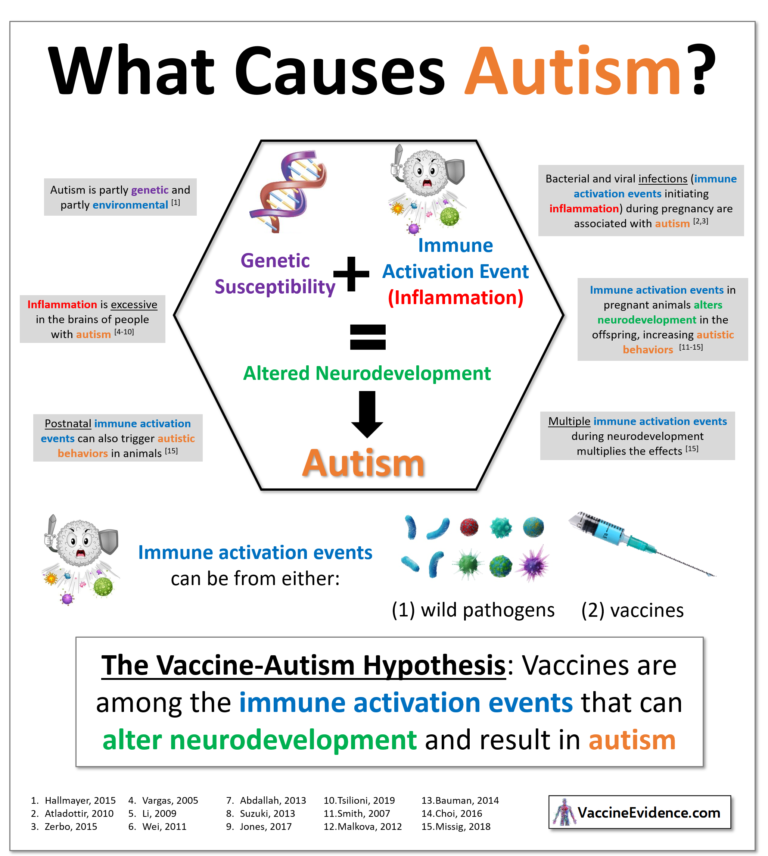
Scientists believe that both genetics and environment likely play a role in ASD. There is great concern that rates of autism have been increasing in recent decades without full explanation as to why. Researchers have identified a number of genes associated with the disorder. Imaging studies of people with ASD have found differences in the development of several regions of the brain. Studies suggest that ASD could be a result of disruptions in normal brain growth very early in development.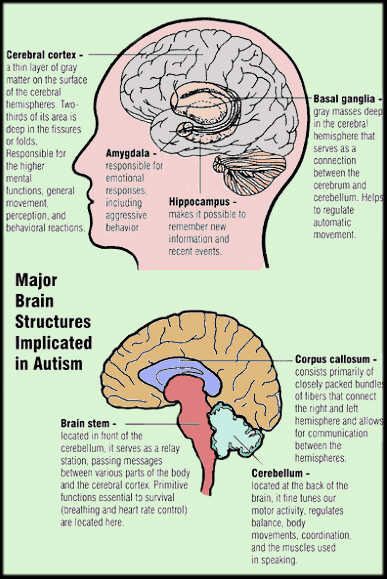 These disruptions may be the result of defects in genes that control brain development and regulate how brain cells communicate with each other. Autism is more common in children born prematurely. Environmental factors may also play a role in gene function and development, but no specific environmental causes have yet been identified. The theory that parental practices are responsible for ASD has long been disproved. Multiple studies have shown that vaccination to prevent childhood infectious diseases does not increase the risk of autism in the population.
These disruptions may be the result of defects in genes that control brain development and regulate how brain cells communicate with each other. Autism is more common in children born prematurely. Environmental factors may also play a role in gene function and development, but no specific environmental causes have yet been identified. The theory that parental practices are responsible for ASD has long been disproved. Multiple studies have shown that vaccination to prevent childhood infectious diseases does not increase the risk of autism in the population.
top
What role do genes play?
Twin and family studies strongly suggest that some people have a genetic predisposition to autism. Identical twin studies show that if one twin is affected, then the other will be affected between 36 to 95 percent of the time. There are a number of studies in progress to determine the specific genetic factors associated with the development of ASD. In families with one child with ASD, the risk of having a second child with the disorder also increases. Many of the genes found to be associated with autism are involved in the function of the chemical connections between brain neurons (synapses). Researchers are looking for clues about which genes contribute to increased susceptibility. In some cases, parents and other relatives of a child with ASD show mild impairments in social communication skills or engage in repetitive behaviors. Evidence also suggests that emotional disorders such as bipolar disorder and schizophrenia occur more frequently than average in the families of people with ASD.
Many of the genes found to be associated with autism are involved in the function of the chemical connections between brain neurons (synapses). Researchers are looking for clues about which genes contribute to increased susceptibility. In some cases, parents and other relatives of a child with ASD show mild impairments in social communication skills or engage in repetitive behaviors. Evidence also suggests that emotional disorders such as bipolar disorder and schizophrenia occur more frequently than average in the families of people with ASD.
In addition to genetic variations that are inherited and are present in nearly all of a person’s cells, recent research has also shown that de novo, or spontaneous, gene mutations can influence the risk of developing autism spectrum disorder. De novo mutations are changes in sequences of deoxyribonucleic acid or DNA, the hereditary material in humans, which can occur spontaneously in a parent’s sperm or egg cell or during fertilization. The mutation then occurs in each cell as the fertilized egg divides. These mutations may affect single genes or they may be changes called copy number variations, in which stretches of DNA containing multiple genes are deleted or duplicated. Recent studies have shown that people with ASD tend to have more copy number de novo gene mutations than those without the disorder, suggesting that for some the risk of developing ASD is not the result of mutations in individual genes but rather spontaneous coding mutations across many genes. De novo mutations may explain genetic disorders in which an affected child has the mutation in each cell but the parents do not and there is no family pattern to the disorder. Autism risk also increases in children born to older parents. There is still much research to be done to determine the potential role of environmental factors on spontaneous mutations and how that influences ASD risk.
The mutation then occurs in each cell as the fertilized egg divides. These mutations may affect single genes or they may be changes called copy number variations, in which stretches of DNA containing multiple genes are deleted or duplicated. Recent studies have shown that people with ASD tend to have more copy number de novo gene mutations than those without the disorder, suggesting that for some the risk of developing ASD is not the result of mutations in individual genes but rather spontaneous coding mutations across many genes. De novo mutations may explain genetic disorders in which an affected child has the mutation in each cell but the parents do not and there is no family pattern to the disorder. Autism risk also increases in children born to older parents. There is still much research to be done to determine the potential role of environmental factors on spontaneous mutations and how that influences ASD risk.
top
Do symptoms of autism change over time?
For many children, symptoms improve with age and behavioral treatment. During adolescence, some children with ASD may become depressed or experience behavioral problems, and their treatment may need some modification as they transition to adulthood. People with ASD usually continue to need services and supports as they get older, but depending on severity of the disorder, people with ASD may be able to work successfully and live independently or within a supportive environment.
During adolescence, some children with ASD may become depressed or experience behavioral problems, and their treatment may need some modification as they transition to adulthood. People with ASD usually continue to need services and supports as they get older, but depending on severity of the disorder, people with ASD may be able to work successfully and live independently or within a supportive environment.
top
How is autism treated?
Currently there is no cure for ASD. Therapies and behavioral interventions are designed to remedy specific symptoms and can substantially improve those symptoms. Some symptoms can be treated with medication. The ideal treatment plan coordinates therapies and interventions that meet the specific needs of the individual. Most health care professionals agree that the earlier the intervention, the better.
Educational/behavioral interventions: Early behavioral/educational interventions have been very successful in many children with ASD.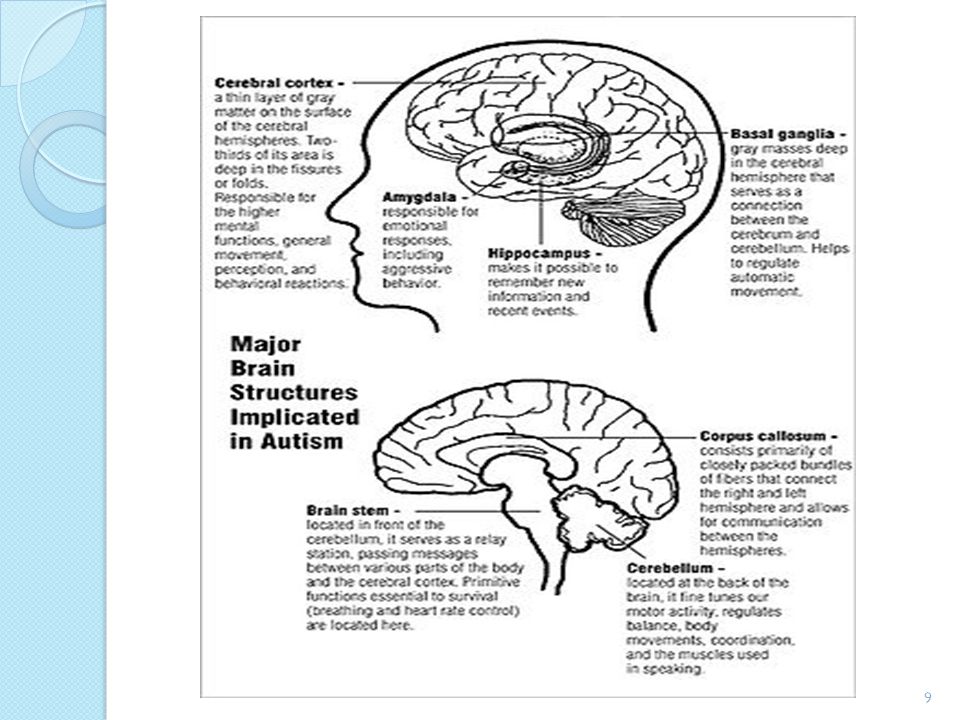 In these interventions therapists use highly structured and intensive skill-oriented training sessions to help children develop social and language skills, such as applied behavioral analysis, which encourages positive behaviors and discourages negative ones. In addition, family counseling for the parents and siblings of children with ASD often helps families cope with the particular challenges of living with a child with ASD.
In these interventions therapists use highly structured and intensive skill-oriented training sessions to help children develop social and language skills, such as applied behavioral analysis, which encourages positive behaviors and discourages negative ones. In addition, family counseling for the parents and siblings of children with ASD often helps families cope with the particular challenges of living with a child with ASD.
Medications: While medication can’t cure ASD or even treat its main symptoms, there are some that can help with related symptoms such as anxiety, depression, and obsessive-compulsive disorder. Antipsychotic medications are used to treat severe behavioral problems. Seizures can be treated with one or more anticonvulsant drugs. Medication used to treat people with attention deficit disorder can be used effectively to help decrease impulsivity and hyperactivity in people with ASD. Parents, caregivers, and people with autism should use caution before adopting any unproven treatments.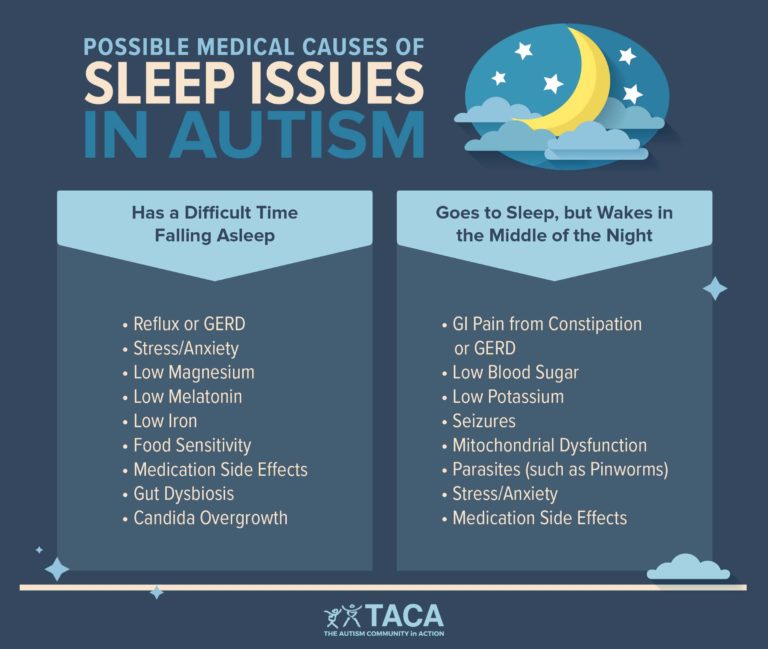
top
What research is being done?
The mission of the National Institute of Neurological Disorders and Stroke (NINDS) is to seek fundamental knowledge about the brain and nervous system and to use that knowledge to reduce the burden of neurological disease. The NINDS is a component of the National Institutes of Health (NIH), the leading supporter of biomedical research in the world. NINDS and several other NIH Institutes and Centers support research on autism spectrum disorder.
NIH participates in the Interagency Autism Coordinating Committee (IACC), a Federal advisory committee that is designed to coordinate Federal efforts and provide advice on issues related to ASD. The committee is composed of representatives from various U.S. Department of Health and Human Services agencies, the Department of Education, and other governmental organizations, as well as public members, including individuals with ASD and representatives of patient advocacy organizations. One responsibility of the IACC is to develop a strategic plan for ASD research, which guides research programs supported by NIH and other participating organizations.
NINDS funds additional research aimed at better understanding the factors that lead to ASD, including other studies on genetic disorders associated with ASD, such as TSC, Fragile X Syndrome, Phelan-McDermid syndrome (which features such autism-like symptoms as intellectual disability, developmental delays, and problems with developing functional language), and Rett syndrome (a disorder that almost exclusively affects girls and is characterized by slowing development, intellectual disability, and loss of functional use of the hands). Many of these studies use animal models to determine how specific known mutations affect cellular and developmental processes in the brain, yielding insights relevant to understanding ASD due to other causes and discovering new targets for treatments.
NINDS researchers are studying aspects of brain function and development that are altered in people with ASD. For example, NINDS-funded researchers are investigating the formation and function of neuronal synapses, the sites of communication between neurons, which may not properly operate in ASD and neurodevelopmental disorders. Other studies use brain imaging in people with and without ASD to identify differences in brain connectivity and activity patterns associated with features of ASD. Researchers hope that understanding these alterations can help identify new opportunities for therapeutic interventions. Additional NINDS researchers are studying the relationship between epilepsy and autism.
Other studies use brain imaging in people with and without ASD to identify differences in brain connectivity and activity patterns associated with features of ASD. Researchers hope that understanding these alterations can help identify new opportunities for therapeutic interventions. Additional NINDS researchers are studying the relationship between epilepsy and autism.
Through the National Center for Advancing Translational Sciences (NCATS) Rare Disease Clinical Research Network (RDCRN), NINDS and other NIH Institutes and Centers support a research consortium focused on three rare genetic syndromes associated with ASD and intellectual disability, including TSC and syndromes involving mutations in the genesSHANK3 (Phelan-McDermid syndrome) and PTEN. The goals of the consortium are to understand shared mechanisms across these syndromes, which may suggest common approaches to their treatment.
NINDS supports autism spectrum disorder research through clinical trials at medical centers across the United States to better our knowledge about ASD treatment and care.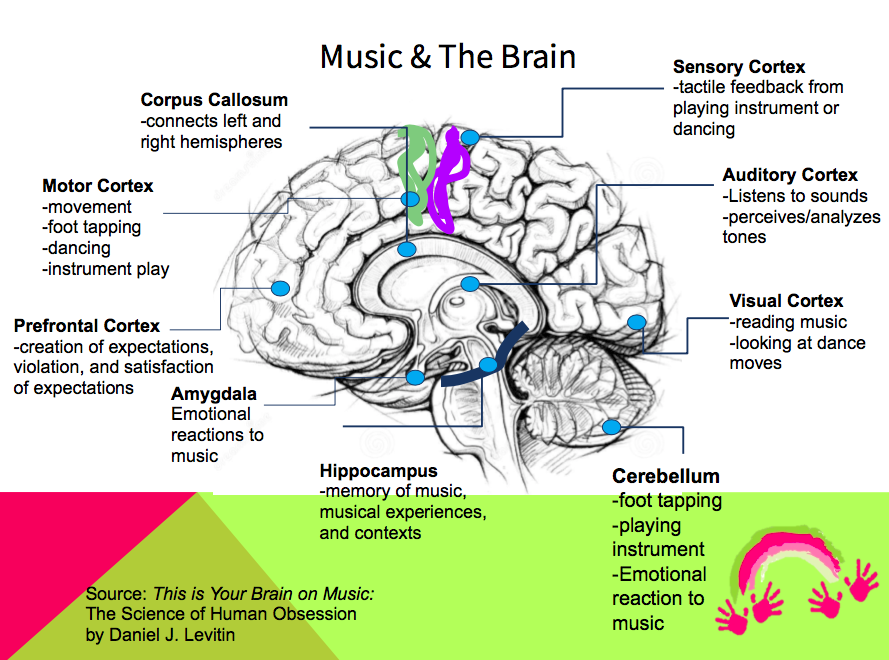 Information about participating in clinical studies can be found at the “NIH Clinical Trials and You” website at www.nih.gov/health/clinicaltrials. Additional studies can be found at www.clinicaltrials.gov. People should talk to their doctor before enrolling in a clinical trial.
Information about participating in clinical studies can be found at the “NIH Clinical Trials and You” website at www.nih.gov/health/clinicaltrials. Additional studies can be found at www.clinicaltrials.gov. People should talk to their doctor before enrolling in a clinical trial.
More information about research on ASD supported by NINDS and other NIH Institutes and Centers can be found using NIH RePORTER (projectreporter.nih.gov), a searchable database of current and past research projects supported by NIH and other federal agencies. RePORTER also includes links to publications and resources from these projects.
top
Where can I get more information?
For more information on neurological disorders or research programs funded by the National Institute of Neurological Disorders and Stroke, contact the Institute's Brain Resources and Information Network (BRAIN) at:
BRAIN
P.O. Box 5801
Bethesda, MD 20824
800-352-9424
Information also is available from the following organizations:
Centers for Disease Control and Prevention (CDC)
U. S. Department of Health and Human Services
S. Department of Health and Human Services
[email protected]
Tel: 800-311-3435; 404-639-3311; 404-639-3543
National Institute of Child Health and Human Development (NICHD)
National Institutes of Health, DHHS
Tel: 301-496-5133
Fax: 301-496-7101
National Institute on Deafness and Other Communication Disorders (NIDCD)
National Institutes of Health, DHHS
[email protected]
Tel: 301-496-7243; 800-241-1044; 800-241-1055 (TTY)
National Institute of Environmental Health Sciences (NIEHS)
[email protected]
Tel: 919-541-3345
National Institute of Mental Health (NIMH)
[email protected]
Tel: 301-443-4513; 866-415-8051; 301-443-8431 (TTY)
Fax: 301-443-4279
Association for Science in Autism Treatment
P.O. Box 1447
Hoboken, NJ 07030
[email protected]
Autism National Committee (AUTCOM)
P.O. Box 429
Forest Knolls, CA 94933
Autism Network International (ANI)
P. O. Box 35448
O. Box 35448
Syracuse, NY 13235-5448
[email protected]
Autism Research Institute (ARI)
4182 Adams Avenue
San Diego, CA 92116
Tel: 619-281-7165; 866-366-3361
Fax: 619-563-6840
Autism Science Foundation
28 West 39th Street
Suite 502
New York, NY 10018
[email protected]
Tel: 212-391-3913
Fax: 212-228-3557
Autism Society of America
4340 East-West Highway
Suite 350
Bethesda, MD 20814
Tel: 301-657-0881; 800-3AUTISM (328-8476)
Fax: 301-657-0869
Autism Speaks, Inc.
1 East 33rd Street
4th Floor
New York, NY 10016
[email protected]
Tel: 212-252-8584; 888-288-4762
Fax: 212-252-8676
MAAP Services for Autism, Asperger Syndrome, and PDD
P.O. Box 524
Crown Point, IN 46308
[email protected]
Tel: 219-662-1311
Fax: 219-662-1315
"Autism Spectrum Disorder Fact Sheet", NINDS, Publication date September 2015.
NIH Publication No. 15-1877
Back to Autism Spectrum Disorder Information Page
See a list of all NINDS disorders
Publicaciones en Español
Autismo
top
Prepared by:
Office of Communications and Public Liaison
National Institute of Neurological Disorders and Stroke
National Institutes of Health
Bethesda, MD 20892
NINDS health-related material is provided for information purposes only and does not necessarily represent endorsement by or an official position of the National Institute of Neurological Disorders and Stroke or any other Federal agency. Advice on the treatment or care of an individual patient should be obtained through consultation with a physician who has examined that patient or is familiar with that patient's medical history.
All NINDS-prepared information is in the public domain and may be freely copied. Credit to the NINDS or the NIH is appreciated.
top
What causes autism? - Queensland Brain Institute
We have learnt a great deal about the causes of autism in recent decades, but there is much more work that needs to be done. For example, we confidently know that it is not due to parentinig style, or vaccination.
For example, we confidently know that it is not due to parentinig style, or vaccination.
Both genes and environmental influences are important, and there is also evidence that the autistic brain is wired differently.
Genetics
Autism can sometimes run in families, indicating that genetics plays a key role in the disorder. Early research into the genetics of autism began with studies of twins, both identical and non-identical. Scientists studied the concordance of autism in these sets of twins – the percentage chance that if one twin had autism, the other would too. They found a significantly higher concordance in identical twins, who have largely identical DNA, suggesting that autism has a genetic basis. Under current estimates, there is a 50 to 80 per cent concordance for identical twins; this compares to an overall ~1.5 per cent chance that any two people will have autism. If parents have one child with autism, there is a 5 to 20 per cent chance that their second child will also have autism.
We now know that as with numerous other traits, including height and intelligence, autism spectrum disorder involves many different genetic variations acting together. No single gene is enough to produce autism, but the more mutations you have in specific parts of your DNA, the greater your chances of an autism diagnosis. To identify the exact regions of DNA associated with the disorder, scientists study large numbers of people affected by autism. This approach is called a genome-wide association study (GWAS). QBI Professors Naomi Wray and Peter Visscher are world leaders in such studies.
Environmental factors
As with genetics, no single environmental factor definitively causes autism. Instead, a range of environmental influences seems to exist. For example, an epidemiological study led by QBI Professor John McGrath found that women deficient in Vitamin D during pregnancy had children with an increased risk of autism.
A lack of Vitamin D is just one risk factor, but it can also interact with other environmental variables.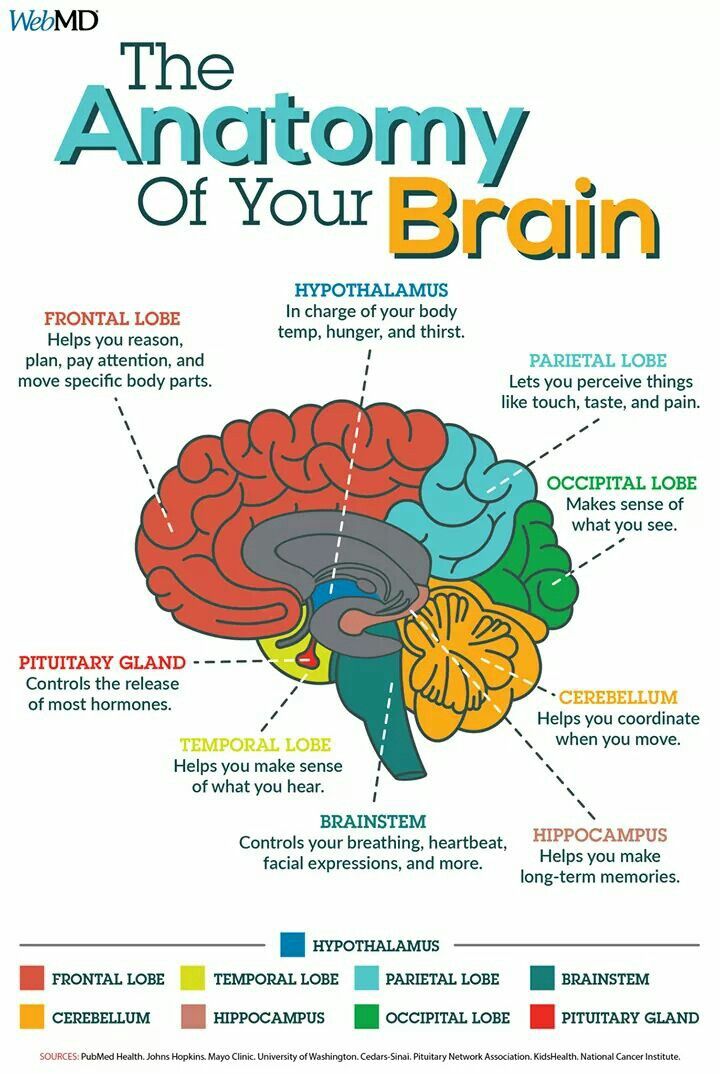 Associate Professor Thomas Burne, for example, is looking at how Vitamin D deficiency can combine with low levels of alcohol during pregnancy to raise the risk of autism-like behaviours in mice.
Associate Professor Thomas Burne, for example, is looking at how Vitamin D deficiency can combine with low levels of alcohol during pregnancy to raise the risk of autism-like behaviours in mice.
Another environmental risk is viral or bacterial infection of the pregnant mother during the first trimester, which has become a common way to study autism in model animals like mice. The laboratory of Professor Darryl Eyles has shown that the presence of Vitamin D protects against autism-like behaviours that are triggered by infections of the mother. The work of Professors McGrath, Eyles and Burne converges in the long-term hope that by supplementing pregnant mothers with Vitamin D, autism rates might be reduced.
Finally, more research by Professor McGrath has found that older fathers – particularly those over 50 at the time of conception – have a greater chance of having a child with autism, potentially as a result of new genetic mutations that affect brain development.
Brain wiring
In the developing brain, connections between and within brain regions are still being formed.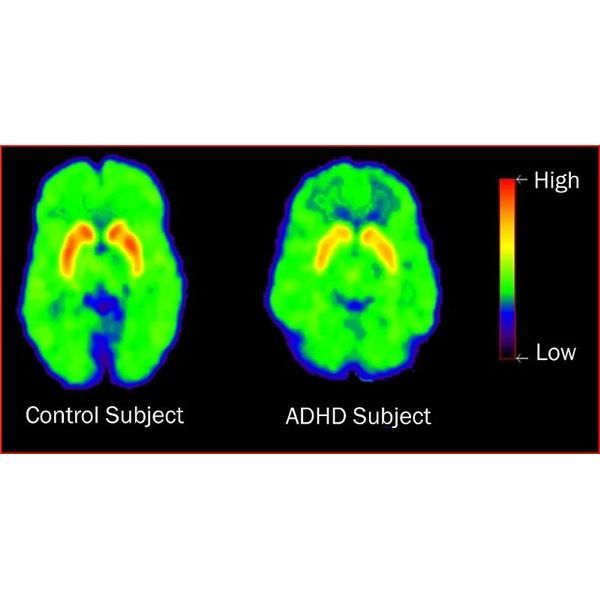 Sometimes, though, these connections don’t form in the normal way, which can produce lasting changes in behaviour.
Sometimes, though, these connections don’t form in the normal way, which can produce lasting changes in behaviour.
One example relevant to autism is a congenital condition called agenesis of the corpus callosum (AgCC). The corpus callosum is a thick bundle of nerve fibres that connects one brain hemisphere to the other. In people with AgCC, the corpus callosum is partly or even completely missing. Strikingly, one third of patients with AgCC meet the diagnostic criteria for autism. What’s more, the genes involved in AgCC and autism are similar. Other studies, however, have found the opposite profile in some people with autism – an enlarged corpus callosum.
How can these findings be reconciled? QBI’s Professor Linda Richards is working on an international project with leading paediatric neurologists to find out. According to Professor Elliott Sherr of the University of California, San Francisco, who has teamed up with Professor Richards, one possibility is that autism could result from inefficient communication between brain hemispheres, and that efficiency could be disrupted whether the corpus callosum is too big or too small.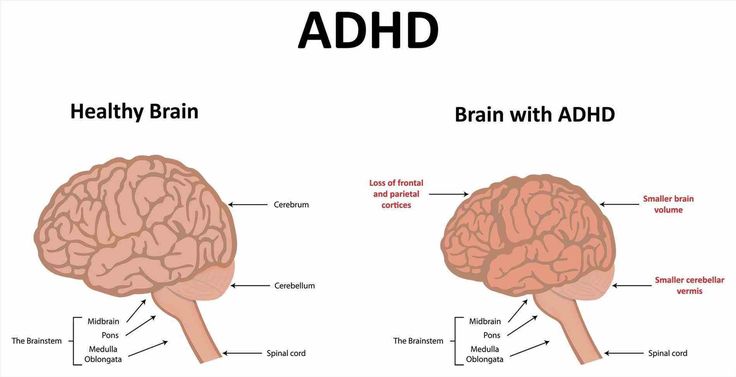
What is autism?
Autism signs and symptoms
Autism treatment
Diagnosing autism
What is autism?
Autism - a disorder of mental and speech development, accompanied by difficulty in social interactions, difficulty in mutual contact when communicating with other people, repetitive actions (stereotypes) and limitation of interests. The reasons for the development of the disease are not fully understood, most scientists suggest a connection with congenital brain dysfunction, as well as a connection with other diseases of the child (for example, diseases of the gastrointestinal tract). Autism is usually diagnosed before the age of 3-4 years, the first signs can be seen already in infancy. Full recovery is considered impossible, but at the present stage of development of medicine, the diagnosis can be removed with age.
How often do we meet children with autism?
Autism is a disease that is characterized by movement and speech disorders, as well as stereotyping of interests and behavior, accompanied by a violation of the patient's social interactions with others.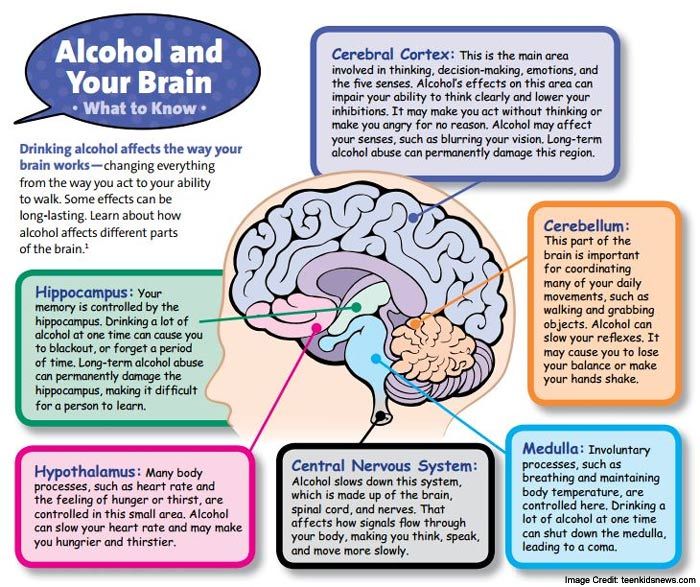 Data on the prevalence of autism vary significantly due to different approaches to the diagnosis and classification of the disease. According to various data, 0.1-0.6% of children suffer from autism without taking into account autism spectrum disorders, 1.1-2% of children suffer from autism, taking into account autism spectrum disorders. Autism is diagnosed four times less frequently in girls than in boys. In the last 25 years, this diagnosis has become much more frequent, however, it is not yet clear whether this is due to a change in diagnostic criteria or a real increase in the prevalence of the disease.
Data on the prevalence of autism vary significantly due to different approaches to the diagnosis and classification of the disease. According to various data, 0.1-0.6% of children suffer from autism without taking into account autism spectrum disorders, 1.1-2% of children suffer from autism, taking into account autism spectrum disorders. Autism is diagnosed four times less frequently in girls than in boys. In the last 25 years, this diagnosis has become much more frequent, however, it is not yet clear whether this is due to a change in diagnostic criteria or a real increase in the prevalence of the disease.
In the literature, the term "autism" can be interpreted in two ways - as autism itself (childhood autism, classic autism disorder, Kanner's syndrome) and as all other disorders of the autism spectrum, including Asperger's syndrome, atypical autism, etc. The degree of severity of individual manifestations of autism can significantly vary - from a complete inability to social contacts, accompanied by severe mental retardation to some oddities when communicating with people, pedantry of speech and narrowness of interests. The treatment of autism is long, complex, and is carried out with the participation of specialists in the field of neurology, psychologists, psychotherapists, defectologists and speech therapists.
The treatment of autism is long, complex, and is carried out with the participation of specialists in the field of neurology, psychologists, psychotherapists, defectologists and speech therapists.
What are the causes of autism?
Currently, the causes of autism have not been finally clarified, however, it has been established that the biological basis of the disease is a violation of the development of certain brain structures. In some children, the hereditary nature of autism has been confirmed, although the genes responsible for the development of the disease have yet to be determined. Children with autism have a large number of complications during pregnancy and childbirth (intrauterine viral infections, toxicosis, uterine bleeding, premature birth). It is suggested that complications during pregnancy cannot cause autism, but may increase the likelihood of its development in the presence of other predisposing factors.
Heredity. Among close and distant relatives of children with autism, 3-7% of autistic patients are detected, which is many times higher than the prevalence of the disease on average in the population.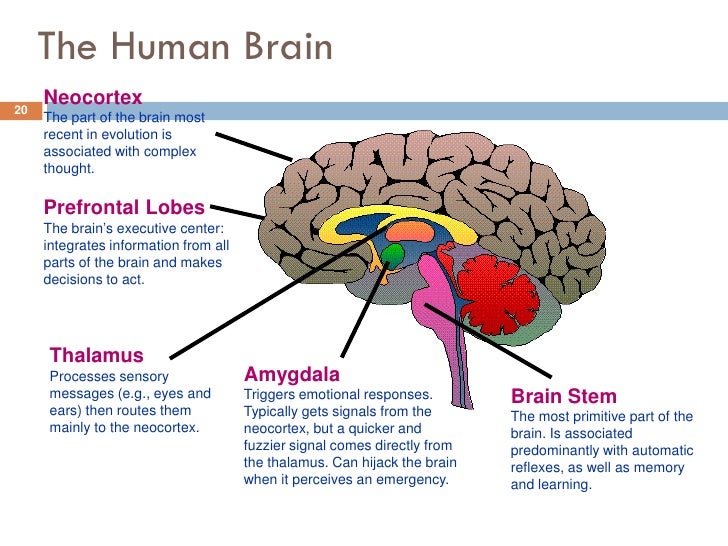 Both identical twins have a 60-90% chance of developing autism. Relatives of patients often have individual disorders characteristic of autism: a tendency to obsessive behavior, a low need for social contacts, difficulties in understanding speech, and speech disorders (including echolalia). In such families, epilepsy and delayed psycho-speech development in childhood are more often detected, which are often diagnosed with this disease. All of the above is a confirmation of the hereditary nature of autism.
Both identical twins have a 60-90% chance of developing autism. Relatives of patients often have individual disorders characteristic of autism: a tendency to obsessive behavior, a low need for social contacts, difficulties in understanding speech, and speech disorders (including echolalia). In such families, epilepsy and delayed psycho-speech development in childhood are more often detected, which are often diagnosed with this disease. All of the above is a confirmation of the hereditary nature of autism.
Scientists have been able to identify a whole group of genes predisposing to autism. The presence of these genes does not necessarily lead to the onset of autism (according to most geneticists, the disease develops as a result of the interaction of several genes). However, molecular genetic research has made it possible to objectively confirm the hereditary nature of autism. This is a serious progress in the field of studying the etiology and pathogenesis of this disease, since shortly before this discovery, some scientists considered the lack of care and attention from parents as possible causes of autism (currently this version is rejected as untrue).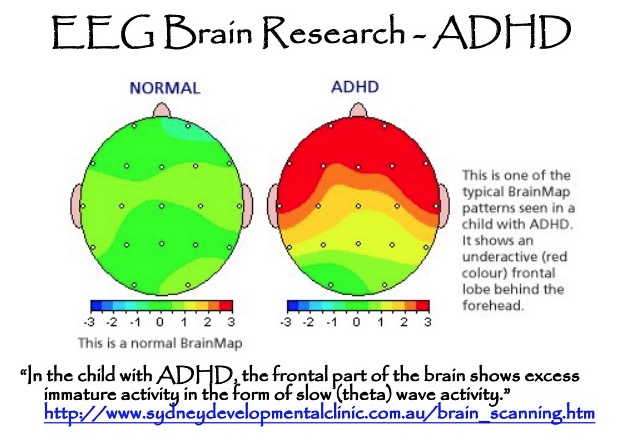
Structural disorders of the brain. Research has shown that autistic patients often show structural changes in the frontal cortex, hippocampus, median temporal lobe, and cerebellum. The main function of the cerebellum is to ensure successful motor activity, however, this part of the brain also influences speech, attention, thinking, emotions, and learning abilities. In many autistic people, some parts of the cerebellum are reduced. It is assumed that this circumstance may be due to the problems of patients with autism when switching attention.
The median temporal lobes, hippocampus, and amygdala, also commonly affected by autism, influence memory, learning, and emotional self-regulation, including the generation of pleasure in meaningful social activities. The researchers note that in animals with damage to these lobes of the brain, behavioral changes similar to autism are observed (a decrease in the need for social contacts, a deterioration in adaptation when exposed to new conditions, difficulties in recognizing danger). In addition, autistic patients often show delayed maturation of the frontal lobes.
In addition, autistic patients often show delayed maturation of the frontal lobes.
Functional disorders of the brain. Approximately 50% of patients on the EEG revealed changes characteristic of impaired memory, selective and directed attention, verbal thinking and purposeful use of speech. The degree of prevalence and severity of changes varies, while in children with high-functioning autism, EEG disturbances are usually less pronounced compared to patients suffering from low-functioning forms of the disease.
The causes of functional brain disorders in autistic symptoms can be all sorts of somatic diseases, neuroimmunological problems, metabolic disorders, latent infectious diseases.
What are the first symptoms of autism?
Mandatory signs of childhood autism are lack of social interactions , problems in building productive mutual contact with others, stereotypical behavior and interests. All of these signs appear before the age of 2-3 years, while individual symptoms indicating possible autism are sometimes detected even in infancy (low emotionality, decreased eye contact).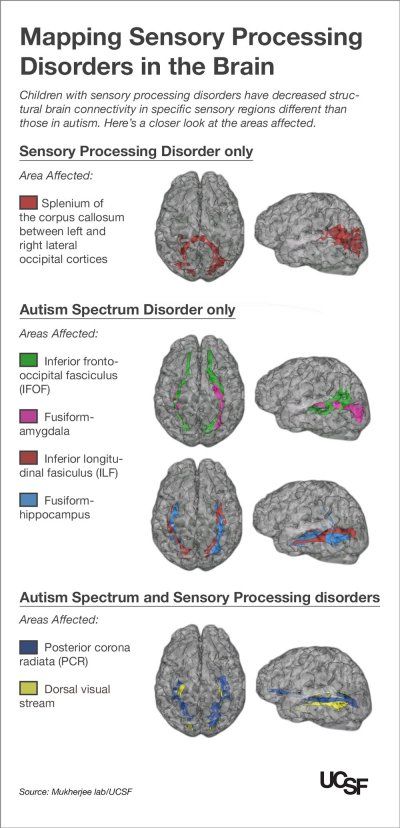
Violation of social interactions is the most striking feature that distinguishes autism from other developmental disorders. Children with autism cannot fully interact with other people. They do not feel the state of others, do not recognize non-verbal signals, do not understand the subtext of social contacts. This symptom can be detected already in infants. Such children react weakly to adults, do not look into the eyes, and are more willing to fix their eyes on inanimate objects, rather than on people around them. They do not smile, react badly to their own name, do not reach out towards an adult when trying to pick them up.
Growing up, patients do not imitate the behavior of others, do not respond to the emotions of other people, do not participate in games designed for interaction, and do not show interest in new people. They are strongly attached to loved ones, but do not show their affection like ordinary kids - they are not happy, they do not run towards them, they do not try to show toys to adults or somehow share events from their lives.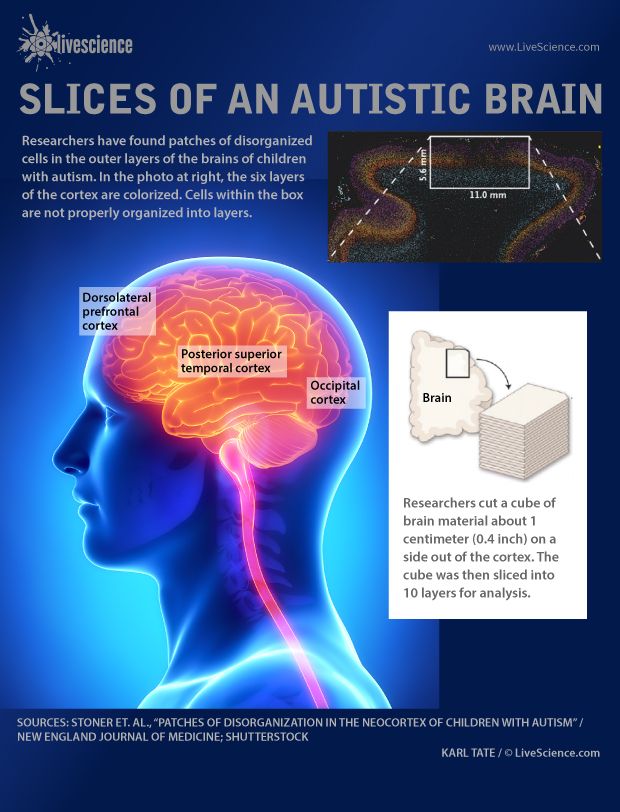 The isolation of autistic people is not due to their desire for loneliness, but to their difficulties due to the inability to build normal relationships with others.
The isolation of autistic people is not due to their desire for loneliness, but to their difficulties due to the inability to build normal relationships with others.
Patients begin to speak later, babble less and less often, and later begin to pronounce individual words and use phrase speech. They often confuse pronouns, calling themselves "you", "he" or "she". Subsequently, high-functioning autistics "gain" sufficient vocabulary and are not inferior to healthy children when passing tests for knowledge of words and spelling, but they have difficulty using images, drawing conclusions about what is written or read, etc. In children with low-functioning forms of autism speech is significantly impoverished.
Children with autism are characterized by unusual gestures and difficulties when trying to use gestures in the process of contacts with other people. In infancy, they rarely point at objects with their hands, or when trying to point to an object, they look not at it, but at their hand. As they get older, they are less likely to say words while gesturing (healthy children tend to gesticulate and speak at the same time, such as holding out their hand and saying “give”). Subsequently, it is difficult for them to play complex games, organically combine gestures and speech, move from simpler forms of communication to more complex ones.
As they get older, they are less likely to say words while gesturing (healthy children tend to gesticulate and speak at the same time, such as holding out their hand and saying “give”). Subsequently, it is difficult for them to play complex games, organically combine gestures and speech, move from simpler forms of communication to more complex ones.
Another striking sign of autism is restricted or repetitive behavior. There are stereotypes - repetitive torso swaying, head shaking, etc. It is very important for patients with autism that everything always happens in the same way: objects are placed in the right order, actions are performed in a certain sequence. A child with autism may start screaming and protesting if his mother usually puts on his right sock first, and then the left one, and today she did the opposite, if the salt shaker is not in the center of the table, but is shifted to the right, if instead of the usual cup he was given a similar one, but with a different pattern. At the same time, unlike healthy children, he does not show a desire to actively correct the state of affairs that does not suit him (reach out to his right toe, rearrange the salt shaker, ask for another cup), but by means available to him signals the wrongness of what is happening.
At the same time, unlike healthy children, he does not show a desire to actively correct the state of affairs that does not suit him (reach out to his right toe, rearrange the salt shaker, ask for another cup), but by means available to him signals the wrongness of what is happening.
The autistic's attention is focused on details, on repetitive scenarios. Children with autism often choose non-play items instead of toys for play; their games are devoid of a plot basis. They do not build castles, do not roll cars around the apartment, but lay out objects in a certain sequence, aimlessly, from the point of view of an outside observer, move them from place to place and back. A child with autism may be extremely attached to a particular toy or non-play item, may watch the same TV show at the same time every day without showing interest in other programs, and experience extremely intensely if this program is somehow That's why I couldn't see it.
Along with other forms of behavior, repetitive behavior includes auto-aggression (hitting, biting, and other self-inflicted injuries). According to statistics, about a third of autistic people during their lives show auto-aggression and the same number - aggression towards others. Aggression, as a rule, is caused by bouts of anger due to a violation of the usual life rituals and stereotypes, or due to the inability to convey one's desires to others.
According to statistics, about a third of autistic people during their lives show auto-aggression and the same number - aggression towards others. Aggression, as a rule, is caused by bouts of anger due to a violation of the usual life rituals and stereotypes, or due to the inability to convey one's desires to others.
The opinion about the obligatory genius of autists and the presence of some unusual abilities in them is not confirmed by practice. Separate unusual abilities (for example, the ability to remember details) or talent in one narrow area with deficits in other areas are observed in only 0.5-10% of patients. The level of intelligence in children with high functioning autism may be average or slightly above average. In low-functioning autism, decrease in intelligence up to mental retardation. All types of autism often have generalized learning disabilities.
Among other not obligatory, rather often occurring symptoms of autism, it is worth noting seizures (detected in 5-25% of children, more often they first occur at puberty), syndrome of hyperactivity and reduced attention , various paradoxical reactions to external stimuli: touch, sounds (closing ears), changes in lighting. Often there is a need for sensory self-stimulation (repetitive movements). More than half of autistic people have abnormal eating behavior (refusal to eat or refuse certain foods, preference for certain foods, etc.) and sleep disorders (difficulty falling asleep, nocturnal and early awakenings).
Often there is a need for sensory self-stimulation (repetitive movements). More than half of autistic people have abnormal eating behavior (refusal to eat or refuse certain foods, preference for certain foods, etc.) and sleep disorders (difficulty falling asleep, nocturnal and early awakenings).
What types of autism are there?
There are several classifications of autism, however, in clinical practice, the most widely used classification is Nikolskaya, which takes into account the severity of the manifestations of the disease, the main psychopathological syndrome and long-term prognosis. Despite the absence of an etiopathogenetic component and a high degree of generalization, teachers and other specialists consider this classification to be one of the most successful, since it makes it possible to draw up differentiated plans for psychological correction and determine treatment goals, taking into account the real capabilities of a child with autism.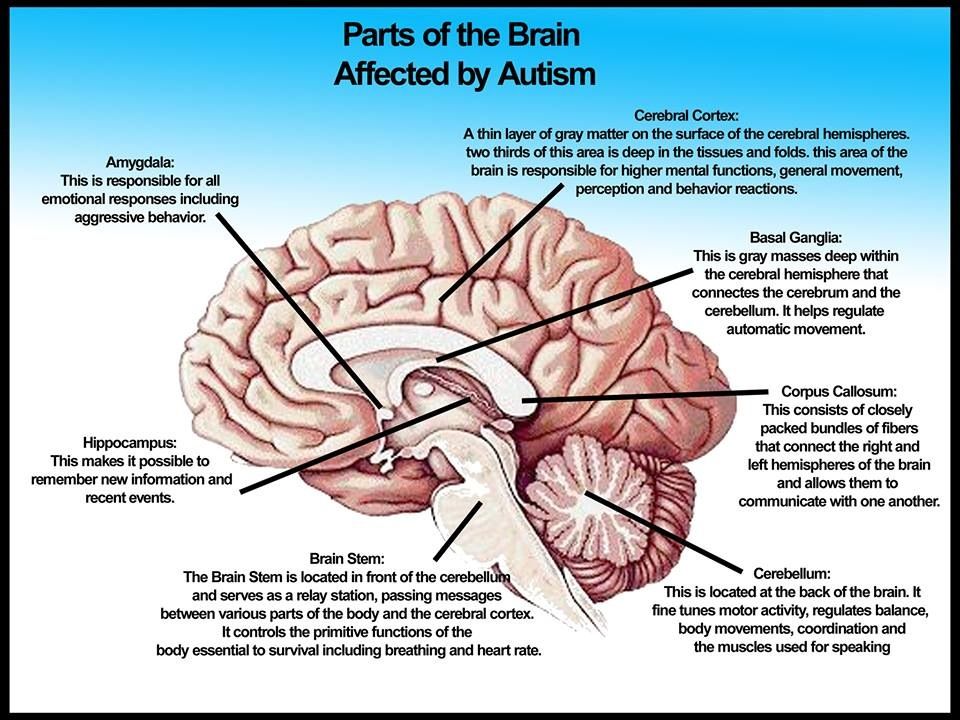
First group . The deepest violations Characterized by mutism, lack of need for interactions with others, lack of active negativism, autostimulation using simple repetitive movements and inability to self-service. The leading pathopsychological syndrome is detachment. The main goal of treatment is to establish contact, involve the child in interactions with adults and peers, as well as the development of self-service skills.
Second group . Characterized by severe restrictions in the choice of forms of behavior, a pronounced desire for immutability. Any changes can provoke a breakdown, expressed in negativism, aggression or auto-aggression. In a familiar environment, the child is quite open, capable of developing and reproducing everyday skills. Speech is stamped, built on the basis of echolalia. The leading psychopathological syndrome is the rejection of reality. The main goal of treatment is the development of emotional contacts with loved ones and the expansion of opportunities for adaptation to the environment by developing a large number of different behavioral stereotypes.
Third group. There is a more complex behavior in the absorption of one's own stereotypical interests and a weak ability to dialogue. The child strives for success, but, unlike healthy children, is not ready to try, take risks and compromise. Often, detailed encyclopedic knowledge is revealed in an abstract field, combined with fragmentary ideas about the real world. Interest in dangerous asocial impressions is characteristic. The leading psychopathological syndrome is substitution. The main goal of treatment is teaching dialogue, expanding the range of ideas and developing social behavior skills.
Fourth group . Children are capable of real voluntary behavior, but they quickly get tired, suffer from difficulties when trying to concentrate attention, follow instructions, etc. Unlike the children of the previous group, who give the impression of young intellectuals, they may look timid, shy and absent-minded, however, with adequate correction show better results compared to other groups. The leading psychopathological syndrome is vulnerability. The main goal of treatment is to teach spontaneity, improve social skills and develop individual abilities.
The leading psychopathological syndrome is vulnerability. The main goal of treatment is to teach spontaneity, improve social skills and develop individual abilities.
What is the diagnosis of autism?
Parents should consult a medical center doctor and exclude autism if the child does not respond to his own name, does not smile or make eye contact, does not notice the instructions of adults, shows atypical play behavior (does not know what to do with toys, plays with non-play objects) and can not tell adults about their desires. At the age of 1 year, the child should walk, babble, point at objects and try to grab them, at the age of 1.5 years - pronounce separate words, at the age of 2 years - use two-word phrases. If these skills are missing, you need to be examined by a specialist.
The diagnosis of autism is based on observations of the child's behavior and identification of a characteristic triad that includes lack of social interactions, lack of communication, and stereotyped behavior. To exclude speech development disorders, a consultation with a speech therapist is prescribed. Autism may or may not be combined with mental retardation, while at the same level of intelligence, the prognosis and correction schemes for oligophrenic children and autistic children will differ significantly, therefore, in the diagnostic process, it is important to distinguish between these two disorders, having carefully studied the characteristics of the patient's behavior.
To exclude speech development disorders, a consultation with a speech therapist is prescribed. Autism may or may not be combined with mental retardation, while at the same level of intelligence, the prognosis and correction schemes for oligophrenic children and autistic children will differ significantly, therefore, in the diagnostic process, it is important to distinguish between these two disorders, having carefully studied the characteristics of the patient's behavior.
An important role in the diagnosis of autism is played by neurophysiological examination (EEG, evoked potentials), as well as laboratory neuroimmunological, genetic and other types of research. Our center has developed a unique method of laboratory diagnosis of diseases accompanied by autistic stimptomology. The advantage of these studies is that the methods allow diagnosing pathological conditions not only in the early stages of development, but also as a prevention of delays in speech and mental development.
A neurophysiological examination, on the other hand, makes it possible to more accurately confirm or exclude the diagnosis of autism, as well as to predict the further development of the child.
Can a child with symptoms of autism be cured?
The main goal of treatment is to increase the level of independence of the patient in the process of self-service, the formation and maintenance of social contacts, the emergence and development of speech skills.
The basis of treatment is a unique method of pathogenetic therapy of speech disorders - biophysical activation of neuromotor structures , which is based on gentle stimulation of the conductors of the nervous system with microcurrents using modern neurophysiological equipment. The method of treatment is based both on the activation of the speech centers themselves (Broca's area, Wernicke's, the angular gyrus, etc.), and on the restoration of broken connections between the centers and hemispheres of the brain. In addition, scattered connections of speech centers with other areas of the brain involved in the implementation of the speech function are restored. In the process of treatment, a physiological, consistent interaction of all areas of the brain associated with speech production is formed. The result is speech.
In addition, scattered connections of speech centers with other areas of the brain involved in the implementation of the speech function are restored. In the process of treatment, a physiological, consistent interaction of all areas of the brain associated with speech production is formed. The result is speech.
Biophysical activation is combined with additional methods of treatment, such as - lymphocellular therapy , which is used to regulate integrative activity and compensate for the deficit of the brain energy system and allows the use of small doses of cerebroprotectors that are administered endolymphatically and enter the brain tissue bypassing the hematoencephalic barrier.
As another way to use drugs with neurotrophic and antioxidant effects, the technique of endonasal electrophoresis is used, which allows drugs to be injected directly into the brain tissue.
Studies in recent decades have revealed that the majority of children with speech and behavioral problems have impaired cerebellar and basal ganglia functions to varying degrees. It is the functioning of the cerebellum that determines the success of the child in learning. For this purpose, a unique development of the Center for Aerospace Medicine is used - plantar support load simulator "Corvit" , used for neurophysiological regulation of the stato-kinetic function of the central nervous system. The basis of the therapeutic effect of the device "Korvit" is the process of activation of the support afferentation, which is responsible for the normalization of the processes of excitation and inhibition in the central nervous system, which leads to a decrease in muscle spasticity, the development and consolidation of functional connections in the brain, contributing to the restoration of coordination of movements, and indirectly improving speech and thinking.
It is the functioning of the cerebellum that determines the success of the child in learning. For this purpose, a unique development of the Center for Aerospace Medicine is used - plantar support load simulator "Corvit" , used for neurophysiological regulation of the stato-kinetic function of the central nervous system. The basis of the therapeutic effect of the device "Korvit" is the process of activation of the support afferentation, which is responsible for the normalization of the processes of excitation and inhibition in the central nervous system, which leads to a decrease in muscle spasticity, the development and consolidation of functional connections in the brain, contributing to the restoration of coordination of movements, and indirectly improving speech and thinking.
Also, for the successful treatment of various forms of STDs, specialists use one of the achievements of modern science - the RUSTOMATIS (RULISTEN) audiovocal therapy method. The device uses sound recordings of high-frequency and low-frequency components. When alternating such music by tension and relaxation, the child trains the middle ear apparatus - the hammer and stirrup, with the help of which the range of perception of external factors expands, concentration of attention increases, new information enters the brain and, as a result, many disorders and disorders disappear.
The device uses sound recordings of high-frequency and low-frequency components. When alternating such music by tension and relaxation, the child trains the middle ear apparatus - the hammer and stirrup, with the help of which the range of perception of external factors expands, concentration of attention increases, new information enters the brain and, as a result, many disorders and disorders disappear.
Long-term behavioral therapy, play therapy, occupational therapy, and speech therapy are also used. Corrective work is carried out against the background of taking psychotropic drugs. The training program is chosen taking into account the capabilities of the child.
After a competent long-term correction, some children (3-25% of the total number of patients) go into remission, and the diagnosis of autism is eventually removed. An insufficient number of studies does not allow to build reliable long-term predictions regarding the course of autism in adulthood.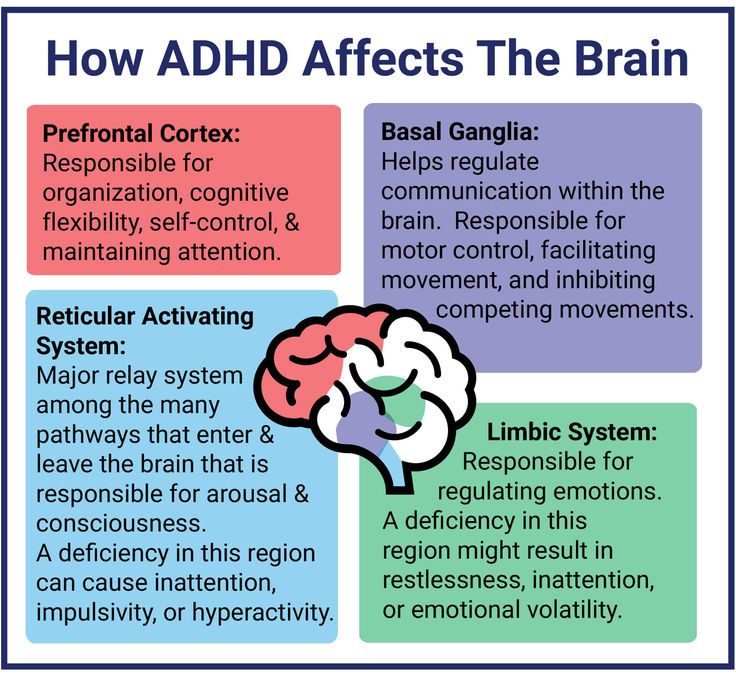 Favorable prognostic signs are an IQ above 50 and speech development before the age of 6, but only 20 percent of children in this group achieve complete or near complete independence.
Favorable prognostic signs are an IQ above 50 and speech development before the age of 6, but only 20 percent of children in this group achieve complete or near complete independence.
Autism: a reflection in a broken mirror
American psychologists came to the conclusion that the cause of autism is a malfunction of the system of mirror neurons in the brain. This leads to a lack of empathy and other symptoms of this mental illness.
When you meet a child with autism, you may not notice anything at first glance. But if you try to talk to him, you will quickly realize that something is wrong. He avoids meeting your eyes; ignores the gaze and your anxiety, sways back and forth. Even if he feels fear, anger or pleasure, he does not show this, nor does he show sincere empathy for other people, he will be distracted, avoiding manifestations of complex social interaction. Another important sign of autism is the literal perception of metaphors. (Viewers of the film "Rain Man" (Rain Man), filmed in 1988, familiar symptoms of this disease, authentically played by actor Dustin Hoffman (Dustin Hoffman)).
In the 1940s, two physicians, the American psychiatrist Leo Kanner and the Austrian pediatrician Hans Asperger, independently discovered this developmental disorder, which today affects 0.5% of American children. An amazing coincidence: neither of these scientists knew about the work of the other, and yet they both gave the same name to the discovered disease! The term "autism" comes from the Greek "autos", which means "self". The name is appropriate - after all, the most noticeable features of the violation are manifested in the fact that the patient avoids social contacts in every possible way.
According to the modern definition, childhood autism is a disorder of mental development, characterized by a special form of contact with others, speech and motor disorders, stereotypical activity and behavior, leading to impaired social interaction. It occurs in 4-5 children out of 10 thousand, differing in four types: these are the so-called Kanner, Asperger's, Rett's syndromes and autism after an attack of schizophrenia).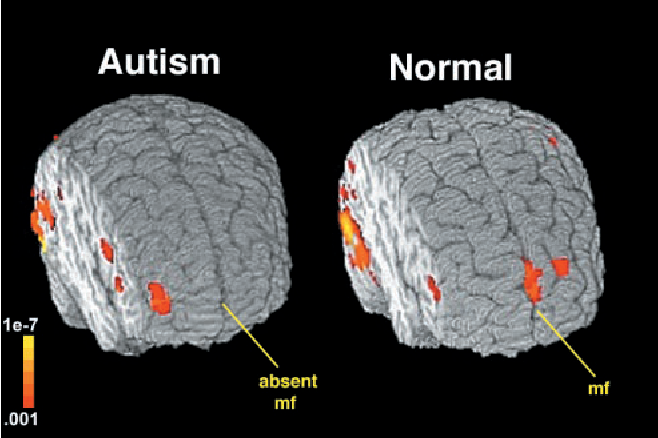
Some scientists consider autism to be a hereditary pathology caused by genetic mutations, according to other sources, the environment can negatively influence the occurrence of autism.
What causes autism? Scientific American authors Vilyanur S.Ramachandan and Lindsay M.Oberman of the Laboratory of the University of California at San Diego (Center for Brain and Cognition, University of California, San Diego - U.C.S.D), on Over the past few years, the connection between autism and a newly discovered class of brain cells called mirror neurons has been studied. Since they are responsible in our body for the ability to empathize and perceive the motivations of another person, it was logical to assume that a violation of this specific nervous activity would manifest itself in the form of symptoms of autism.
Mirror neurons are located in different parts of the human brain. Their functions are complex. Thanks to these cells, for example, we can respond to the pain of another person or imitate someone. For example, if a newborn baby is shown a tongue, he, thanks to mirror neurons, will respond in kind.
For example, if a newborn baby is shown a tongue, he, thanks to mirror neurons, will respond in kind.
However, earlier work by some anatomists (Eric Courchense of U.C.S.D) proved that autism occurs in children with characteristic anomalies of the cerebellum, the brain structure responsible for complex voluntary muscle movements. But the San Diego scientists thought it premature to conclude that damage to the cerebellum was the sole cause of the disease. And, apparently, they were right.
To understand how mirror cells work in children with autism, the parameters of the so-called mu-waves were determined on encephalograms. It turned out that when a sick child performs simple movements, his encephalogram changes in the same way as in a healthy child. But when he sees another person, unlike a healthy child, he does not react in any way - the characteristics of the mu-waves do not change. Therefore, the autistic patient's motor system is not impaired, but the mirror neuron system does not function correctly.
The main question: is it possible to "restore the mirror" by making the neurons work correctly? So far, the prospects for a cure for the disease arise in connection with the early diagnosis of autism. If you use encephalograms, then behavioral therapy will begin as early as possible, and not when the symptoms of developmental disabilities become obvious to everyone (usually this happens from two to four years). Possible drug effects are also discussed.
But how can the mirror neuron hypothesis explain such symptoms of autism as "rocking", unwillingness to meet the eyes of another person, hypersensitivity, intolerance to certain sounds? Ramachandan and his colleagues propose another theory called salience landscape theory.
When a person looks around, he is immersed in the world of sensory information - sights, sounds, smells, tactile sensations. The portal for the regulation of emotions is located in the limbic system - this is the so-called amygdala (cerebellar amygdala), which determines with what emotion to respond to a particular phenomenon.